Embed Size (px)
Citation preview

Contents lists available at ScienceDirect
J Ped Surg Case Reports 11 (2016) 31e34
Journal of Pediatric Surgery CASE REPORTS
journal homepage: www.jpscasereports .com
DICER1 syndrome and thyroid disease
Michael Canfarotta a,1, Rebecca Riba-Wolman b,2, Andrea D. Orsey c,3,Fabiola Balarezo d,4, Christine Finck e,*
aUniversity of Connecticut School of Medicine, 263 Farmington Avenue, Farmington, CT 06032, USAbDepartment of Pediatrics and Endocrinology, Connecticut Children’s Medical Center, Multidisciplinary Thyroid Center, 282 Washington Street,Hartford, CT 06106, USAcDepartment of Pediatrics and Hematology/Oncology, Connecticut Children’s Medical Center, 282 Washington Street, Hartford, CT 06106, USAdDepartment of Pathology and Laboratory Medicine, Hartford Hospital, 80 Seymour Street, P.O. Box 5037, Hartford, CT 06102, USAeDepartment of Surgery, Connecticut Children’s Medical Center, Multidisciplinary Thyroid Center, 282 Washington Street, Hartford, CT 06106, USA
a r t i c l e i n f o
Article history:Received 13 May 2016Received in revised form25 May 2016Accepted 26 May 2016
Key words:DICER1Multinodular goiterOvarian Sertoli-Leydig cell tumorCancer predisposition syndromePediatric onset tumors
* Corresponding author. Tel.: þ1 860 545 9520; fax:E-mail address: [email protected] (C
1 Tel.: þ1 860 679 7845; fax: þ1 860 679 1201.2 Tel.: þ1 860 837 6700.3 Tel.: þ1 860 545 9630.4 Tel.: þ1 860 972 2249.
2213-5766/� 2016 The Authors. Published by Elsevierhttp://dx.doi.org/10.1016/j.epsc.2016.05.014
a b s t r a c t
DICER1, a member of the ribonuclease III (RNase III) family, is known to play an important role in thepost-transcriptional regulation of gene expression and germline mutations have been associated with afamilial tumor susceptibility syndrome. In this report, we describe an 11-year-old female with a historyof ovarian Sertoli-Leydig cell tumor resection and known DICER1 mutation (c.325C>T, p.Gln109*). Shepresented with multiple thyroid nodules on screening ultrasound. On fine needle aspiration she wasfound to have cytologic atypia, which in the general adult population confers a 5e15% risk of malignancy.Herein, we review the literature on DICER1 phenotype and pediatric thyroid disease and discussmanagement options.� 2016 The Authors. Published by Elsevier Inc. This is an open access article under the CC BY-NC-ND
license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
DICER1 is amember of the ribonuclease III (RNase III) family thatis involved in cleaving double stranded pre-microRNAs into maturemicro-ribonucleic acids (miRNAs) [1]. Mature miRNAs are 22nucleotide, single stranded, noncoding small RNAs that bind to the30-untranslated region of target mRNAs to suppress their trans-lation by either silencing or degradation [2]. These moleculesregulate the expression of many cellular proteins. Dysregulation ofmiRNAs has been related to cancer initiation and progression forseveral tumor types, including all variants of thyroid cancer [2].DICER1 germline mutations also have been described in associationwith multinodular goiter (MNG), Sertoli-Leydig cell tumors (SLCT),cystic nephroma, pleuropulmonary blastoma, primitive neuro-ectodermal tumor, cervical embryonal rhabdomyosarcoma, andWilms tumor [3e10]. We present a pediatric case of MNG withatypia of undetermined significance on fine needle aspiration (FNA)
þ1 860 545 9545.. Finck).
Inc. This is an open access article u
in a patient with a history of ovarian SLCT and confirmed DICER1syndrome and review the literature on work up and management.
1. Case report
An 11-year-old female presented with nine nodules, the largestbeing 1 � 0.8 � 0.9 cm (Fig. 1), on her thyroid screening ultrasoundfollowing confirmation of a DICER1 mutation (c.325C>T,p.Gln109*).
Four years previously, she was diagnosed with SLCT of the rightovary. She underwent an oophorectomy and completed chemo-therapy including six cycles of PEB (cisplatin, etoposide and bleo-mycin) as per AGCT0132. She did not receive radiation therapy. Shedeveloped autoimmune hypothyroidism shortly after treatment forher SLCT and had been maintained on levothyroxine. She had nofamily history of thyroid disease and no complaints suggestive ofhyper or hypothyroidism while on levothyroxine. Her physicalexam was unremarkable with no palpable thyroid nodules orcervical adenopathy. The patient underwent FNA biopsy of thethyroid nodules, which demonstrated atypia of undetermined sig-nificance (Bethesda class III). With the reported 5e15% risk formalignancy, case reports of differentiated thyroid cancer in DICER1
nder the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
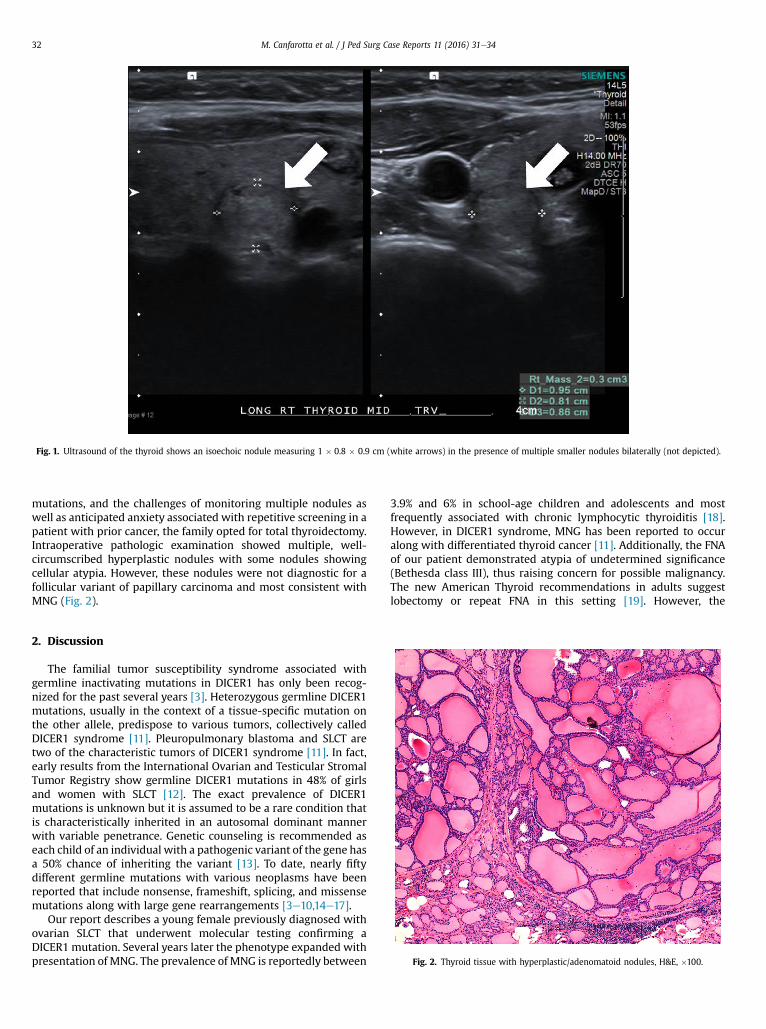
Fig. 1. Ultrasound of the thyroid shows an isoechoic nodule measuring 1 � 0.8 � 0.9 cm (white arrows) in the presence of multiple smaller nodules bilaterally (not depicted).
M. Canfarotta et al. / J Ped Surg Case Reports 11 (2016) 31e3432
mutations, and the challenges of monitoring multiple nodules aswell as anticipated anxiety associated with repetitive screening in apatient with prior cancer, the family opted for total thyroidectomy.Intraoperative pathologic examination showed multiple, well-circumscribed hyperplastic nodules with some nodules showingcellular atypia. However, these nodules were not diagnostic for afollicular variant of papillary carcinoma and most consistent withMNG (Fig. 2).
Fig. 2. Thyroid tissue with hyperplastic/adenomatoid nodules, H&E, �100.
2. Discussion
The familial tumor susceptibility syndrome associated withgermline inactivating mutations in DICER1 has only been recog-nized for the past several years [3]. Heterozygous germline DICER1mutations, usually in the context of a tissue-specific mutation onthe other allele, predispose to various tumors, collectively calledDICER1 syndrome [11]. Pleuropulmonary blastoma and SLCT aretwo of the characteristic tumors of DICER1 syndrome [11]. In fact,early results from the International Ovarian and Testicular StromalTumor Registry show germline DICER1 mutations in 48% of girlsand women with SLCT [12]. The exact prevalence of DICER1mutations is unknown but it is assumed to be a rare condition thatis characteristically inherited in an autosomal dominant mannerwith variable penetrance. Genetic counseling is recommended aseach child of an individual with a pathogenic variant of the gene hasa 50% chance of inheriting the variant [13]. To date, nearly fiftydifferent germline mutations with various neoplasms have beenreported that include nonsense, frameshift, splicing, and missensemutations along with large gene rearrangements [3e10,14e17].
Our report describes a young female previously diagnosed withovarian SLCT that underwent molecular testing confirming aDICER1 mutation. Several years later the phenotype expanded withpresentation of MNG. The prevalence of MNG is reportedly between
3.9% and 6% in school-age children and adolescents and mostfrequently associated with chronic lymphocytic thyroiditis [18].However, in DICER1 syndrome, MNG has been reported to occuralong with differentiated thyroid cancer [11]. Additionally, the FNAof our patient demonstrated atypia of undetermined significance(Bethesda class III), thus raising concern for possible malignancy.The new American Thyroid recommendations in adults suggestlobectomy or repeat FNA in this setting [19]. However, the
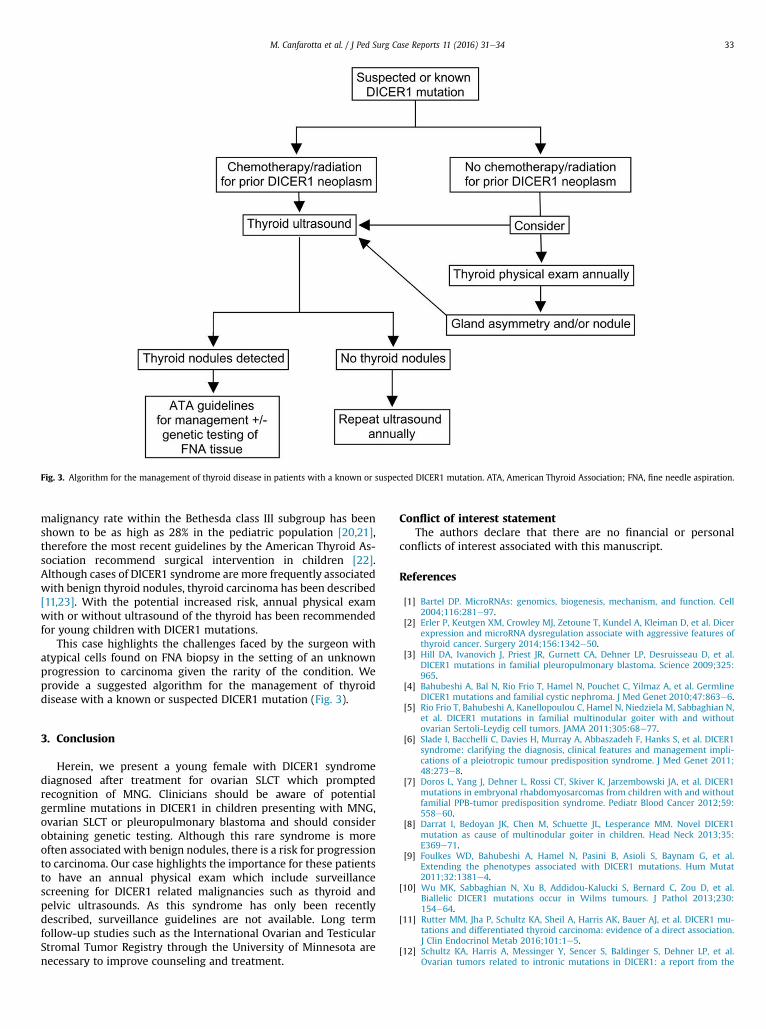
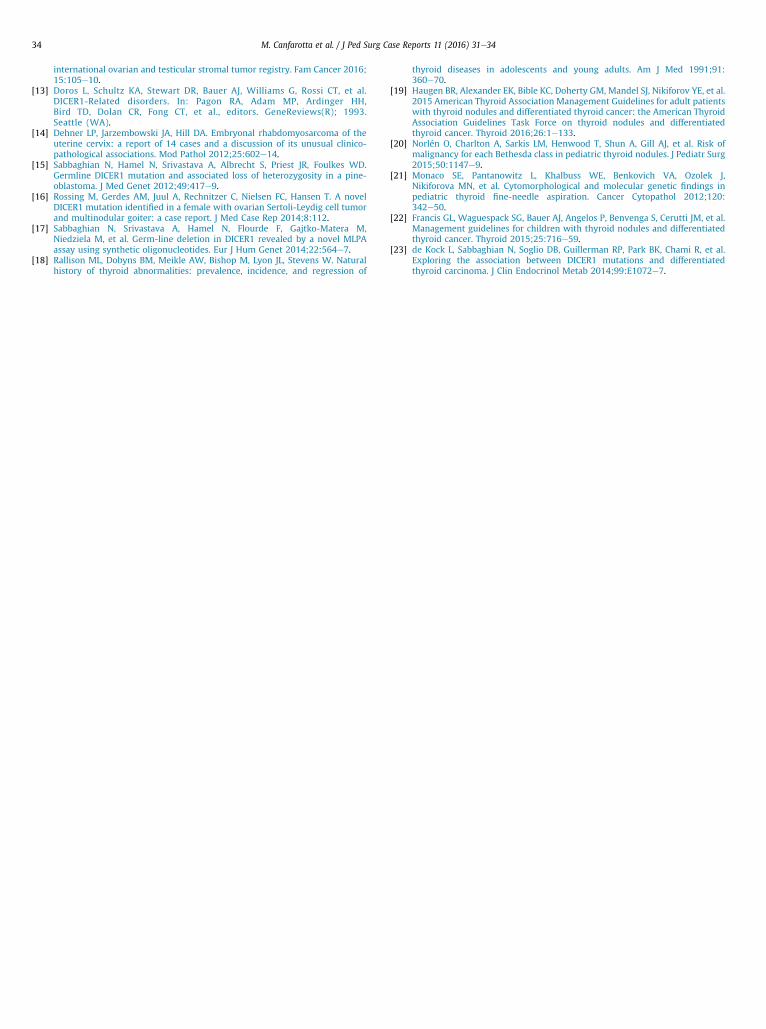
Fig. 3. Algorithm for the management of thyroid disease in patients with a known or suspected DICER1 mutation. ATA, American Thyroid Association; FNA, fine needle aspiration.
M. Canfarotta et al. / J Ped Surg Case Reports 11 (2016) 31e34 33
malignancy rate within the Bethesda class III subgroup has beenshown to be as high as 28% in the pediatric population [20,21],therefore the most recent guidelines by the American Thyroid As-sociation recommend surgical intervention in children [22].Although cases of DICER1 syndrome are more frequently associatedwith benign thyroid nodules, thyroid carcinoma has been described[11,23]. With the potential increased risk, annual physical examwith or without ultrasound of the thyroid has been recommendedfor young children with DICER1 mutations.
This case highlights the challenges faced by the surgeon withatypical cells found on FNA biopsy in the setting of an unknownprogression to carcinoma given the rarity of the condition. Weprovide a suggested algorithm for the management of thyroiddisease with a known or suspected DICER1 mutation (Fig. 3).
3. Conclusion
Herein, we present a young female with DICER1 syndromediagnosed after treatment for ovarian SLCT which promptedrecognition of MNG. Clinicians should be aware of potentialgermline mutations in DICER1 in children presenting with MNG,ovarian SLCT or pleuropulmonary blastoma and should considerobtaining genetic testing. Although this rare syndrome is moreoften associated with benign nodules, there is a risk for progressionto carcinoma. Our case highlights the importance for these patientsto have an annual physical exam which include surveillancescreening for DICER1 related malignancies such as thyroid andpelvic ultrasounds. As this syndrome has only been recentlydescribed, surveillance guidelines are not available. Long termfollow-up studies such as the International Ovarian and TesticularStromal Tumor Registry through the University of Minnesota arenecessary to improve counseling and treatment.
Conflict of interest statementThe authors declare that there are no financial or personal
conflicts of interest associated with this manuscript.
References
[1] Bartel DP. MicroRNAs: genomics, biogenesis, mechanism, and function. Cell2004;116:281e97.
[2] Erler P, Keutgen XM, Crowley MJ, Zetoune T, Kundel A, Kleiman D, et al. Dicerexpression and microRNA dysregulation associate with aggressive features ofthyroid cancer. Surgery 2014;156:1342e50.
[3] Hill DA, Ivanovich J, Priest JR, Gurnett CA, Dehner LP, Desruisseau D, et al.DICER1 mutations in familial pleuropulmonary blastoma. Science 2009;325:965.
[4] Bahubeshi A, Bal N, Rio Frio T, Hamel N, Pouchet C, Yilmaz A, et al. GermlineDICER1 mutations and familial cystic nephroma. J Med Genet 2010;47:863e6.
[5] Rio Frio T, Bahubeshi A, Kanellopoulou C, Hamel N, Niedziela M, Sabbaghian N,et al. DICER1 mutations in familial multinodular goiter with and withoutovarian Sertoli-Leydig cell tumors. JAMA 2011;305:68e77.
[6] Slade I, Bacchelli C, Davies H, Murray A, Abbaszadeh F, Hanks S, et al. DICER1syndrome: clarifying the diagnosis, clinical features and management impli-cations of a pleiotropic tumour predisposition syndrome. J Med Genet 2011;48:273e8.
[7] Doros L, Yang J, Dehner L, Rossi CT, Skiver K, Jarzembowski JA, et al. DICER1mutations in embryonal rhabdomyosarcomas from children with and withoutfamilial PPB-tumor predisposition syndrome. Pediatr Blood Cancer 2012;59:558e60.
[8] Darrat I, Bedoyan JK, Chen M, Schuette JL, Lesperance MM. Novel DICER1mutation as cause of multinodular goiter in children. Head Neck 2013;35:E369e71.
[9] Foulkes WD, Bahubeshi A, Hamel N, Pasini B, Asioli S, Baynam G, et al.Extending the phenotypes associated with DICER1 mutations. Hum Mutat2011;32:1381e4.
[10] Wu MK, Sabbaghian N, Xu B, Addidou-Kalucki S, Bernard C, Zou D, et al.Biallelic DICER1 mutations occur in Wilms tumours. J Pathol 2013;230:154e64.
[11] Rutter MM, Jha P, Schultz KA, Sheil A, Harris AK, Bauer AJ, et al. DICER1 mu-tations and differentiated thyroid carcinoma: evidence of a direct association.J Clin Endocrinol Metab 2016;101:1e5.
[12] Schultz KA, Harris A, Messinger Y, Sencer S, Baldinger S, Dehner LP, et al.Ovarian tumors related to intronic mutations in DICER1: a report from the
M. Canfarotta et al. / J Ped Surg Case Reports 11 (2016) 31e3434
international ovarian and testicular stromal tumor registry. Fam Cancer 2016;15:105e10.
[13] Doros L, Schultz KA, Stewart DR, Bauer AJ, Williams G, Rossi CT, et al.DICER1-Related disorders. In: Pagon RA, Adam MP, Ardinger HH,Bird TD, Dolan CR, Fong CT, et al., editors. GeneReviews(R); 1993.Seattle (WA).
[14] Dehner LP, Jarzembowski JA, Hill DA. Embryonal rhabdomyosarcoma of theuterine cervix: a report of 14 cases and a discussion of its unusual clinico-pathological associations. Mod Pathol 2012;25:602e14.
[15] Sabbaghian N, Hamel N, Srivastava A, Albrecht S, Priest JR, Foulkes WD.Germline DICER1 mutation and associated loss of heterozygosity in a pine-oblastoma. J Med Genet 2012;49:417e9.
[16] Rossing M, Gerdes AM, Juul A, Rechnitzer C, Nielsen FC, Hansen T. A novelDICER1 mutation identified in a female with ovarian Sertoli-Leydig cell tumorand multinodular goiter: a case report. J Med Case Rep 2014;8:112.
[17] Sabbaghian N, Srivastava A, Hamel N, Flourde F, Gajtko-Matera M,Niedziela M, et al. Germ-line deletion in DICER1 revealed by a novel MLPAassay using synthetic oligonucleotides. Eur J Hum Genet 2014;22:564e7.
[18] Rallison ML, Dobyns BM, Meikle AW, Bishop M, Lyon JL, Stevens W. Naturalhistory of thyroid abnormalities: prevalence, incidence, and regression of
thyroid diseases in adolescents and young adults. Am J Med 1991;91:360e70.
[19] Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al.2015 American Thyroid Association Management Guidelines for adult patientswith thyroid nodules and differentiated thyroid cancer: the American ThyroidAssociation Guidelines Task Force on thyroid nodules and differentiatedthyroid cancer. Thyroid 2016;26:1e133.
[20] Norlén O, Charlton A, Sarkis LM, Henwood T, Shun A, Gill AJ, et al. Risk ofmalignancy for each Bethesda class in pediatric thyroid nodules. J Pediatr Surg2015;50:1147e9.
[21] Monaco SE, Pantanowitz L, Khalbuss WE, Benkovich VA, Ozolek J,Nikiforova MN, et al. Cytomorphological and molecular genetic findings inpediatric thyroid fine-needle aspiration. Cancer Cytopathol 2012;120:342e50.
[22] Francis GL, Waguespack SG, Bauer AJ, Angelos P, Benvenga S, Cerutti JM, et al.Management guidelines for children with thyroid nodules and differentiatedthyroid cancer. Thyroid 2015;25:716e59.
[23] de Kock L, Sabbaghian N, Soglio DB, Guillerman RP, Park BK, Chami R, et al.Exploring the association between DICER1 mutations and differentiatedthyroid carcinoma. J Clin Endocrinol Metab 2014;99:E1072e7.