Diastolic LV function and HFNEF FRIJO JOSE A Slide 2
Approximately 50% of pts with HF have a normal or near normal LVEF
Mayo Clinic registry Slide 3 Women Hypertension (up to 88%) Obesity
(BMI >30 kg/m2 40%) Renal failure Anemia AF Diabetes (30%) CAD
(40%-50%) similar to that in HF patients with impaired LVEF Slide 4
Lower overall mortality in HFNEF v/s SHF patients (2.8% vs 3.9%; P
= 0.005) Symptom burden, duration of ICU stay & hospital stay,
long-term mortality similar ADHERE database- 52,187 patients Slide
5 Clinical of HF (Framingham criteria) and an LVEF > 50% True-
typically excluded significant CAD(most often clinically assessed)
Hypertrophic cardiomyopathy Valvular heart disease Slide 6
Morphologic Features Higher cardiomyocyte diameter Higher
myofibrillar density Collagen volume fraction was similar Slide 7
Slide 8 SHF HFNEF Slide 9 D/D to the Syndrome of HFNEF Slide 10
Diastolic function Major factors influencing relaxation Cytosolic
Ca level must fall- requires ATP & phosphorylation of
phospholamban Inherent viscoelastic properties of myocard
(hypertrophied heart -fibrosis, relaxation slower) phosphorylation
of troponin I Influenced by systolic load- the systolic load, the
faster the rate of relaxation Slide 11 Diastolic function SHF pts
LV pressurevolume analysis less steep slope of end-systolic LV
pressure volume relationship HFNEF pts Upward and leftward shifted
end-diastolic pressurevolume relationship End-systolic
pressurevolume relationship- unaltered or even steeper Slide 12
Slide 13 Slide 14 HFNEF LV stiffness Very small changes in LVEDV
Marked in LVEDP & pulm venous P dyspnea during exercise, even
pulm edema Impaired LV filling and inability to use Frank- Starling
mech Failure to CO during exercise Exercise intolerance Slide 15 Is
diastolic dysfunction the only explanation? TDI - systolic mitral
annular amplitudesin HFNEF pts V/S controls These changes not as
pronouncd as in SHF pts ? initial abn compensated for by ventri
hypertrophy & neurohormonal activation hypercontractile LV
state with abn relaxation resistance to LV filling progress
phenotype characteristic of SHF However, data lacking &
progression have been shown to occur rarely Slide 16 2,042
participants Incidence of mod-sev LV diast dysf in presence of an
LVEF >50% - 5.6% Only ~ 1% of study population had symptoms of
HF & an LVEF >50%. Redfield MM et al. JAMA 2003;289:194 202.
Slide 17 37 HFNEF pts (prev pulm edema, LVEF >50%) 40 pts with
hypertensive LVH without HF 56 control subjects HFNEF V/S HTN LVH
and control - LV mass index, conc LV geometry, E/E ratio, LA volume
Distinguished HFNEF pts very well from control but not from
asymptomatic hypertensive LVH Product of LV mass index and LA
volume - highest accuracy for predicting HFNEF Melenovsky V et al.
J Am Coll Cardiol 2007;49:198207 Slide 18 Anemia, renal dysf ?
Volume overload rather than an intrinsic abn of LV diastolic
function -pathophysio of HFNEF Slide 19 LV systolic function LVEF
as a measure of LV systolic function - questioned-load dependence
Annular peak syst velocity (TDI) in HFNEF Still controversial-
whether LV syst function is N in HFNEF Slide 20 Ventriculovascular
coupling in HFNEF Effective art elastance- global measure of art
stiffness- (LVESP/SV)- HFNEF pts Combined ventri-art stiffening
contributes to HFNEF Mechanisms 1) exaggerated SBP after small in
LVEDV 2) a marked SBP after a further in art elastance in presence
of a high ES elastance 3) limited systolic reserve due to baseline
ES elastance 4) cardiac work to deliver a given CO 5) a direct
influence of art elastance on LV diast functn First 2 also explain
sensitivity of these pts to overdiuresis & aggr vasodilator
therapy Slide 21 Role of Atrial Fibrillation Atria Blood-receiving
reservoir chamber Contractile chamber Conduit Volume sensor of the
heart, releasing ANP in response to intermittent stretch Contains
receptors for afferent arms of various reflexes mechanoreceptors
that sinus discharge rate, thereby contributing to the tachycardia
of exercise as the venous return increases (Bainbridge reflex)
Slide 22 Role of Atrial Fibrillation The prevalence of AF in HFNEF
20% to 30% Slide 23 Fung et al- HFNEF pts with AF (29%) had
functional class & quality of life than without AF CHARM - AF
adv CV outcomes irrespective of baseline LVEF High HR, loss of
atrial systole, irr cycle length with implications of the
Frank-Starling mechanism, episodic nature Echocardiographic assess
challenging Fung et al - similar E/E ratios in HFNEF with and
without AF but larger LA size in AF Melenovsky et al - LA emptying
fraction in HFNEF pts than hypertensive LVH & during handgrip,
late diastolic annular tissue velocity - unchanged in HFNEF but in
control (5% vs. 35%) Slide 24 Role of Coronary Artery Disease
Ischemia affects early diastole by Tau Reversed after removal of
ischemic burden by CABG ?Considerable no of pts with atypical
presentation of ischemia (silent/dyspnea) labeled as HFNEF 15%
incidence of hospital admission due to UA in pts previously with
HFNEF -38/12 Slide 25 Volume overload HF with either /N EF is a
Na-sensitive condition HFNEF- likely to have multiple comorbidities
that may contribute to volume overload Renovascular disease,
obesity, OSAHS, anemia Plasma volumes of HTN HFNEF - by an average
of 16% compared with N controls despite daily diuretic use Slide 26
UNLOAD -ultrafiltration -186 pts -45 NEF ultrafiltration, other IV
diuretics Volume expansion precedes sympt, volume removal
alleviates sympt without inducing hypotension/end-organ dysf HFNEF
risk of recur of fluid overload A/c pulm edema - common
manifestation of HFNEF diuretics remain mainstay Diuretics &
dietary salt restrict- paramount to care of HFNEF pts Slide 27
Venoconstriction/volume redistribution 85% of blood vol- venous
circulation Small alterations in venous tone & capacitance (esp
splanchnic bed) impact the distri of intravasc vol - imp
determinant of LVED filling P Data lacking Most imp drugs used in
a/c pulm edema venodilators & diuretics ? Improvements-at least
partly due to autonomic tone & resulting in venous capacitance
Slide 28 Diagnosis of HFNEF 2007- European Working Group on HFNEF 3
conditions must be fulfilled 1) symptoms & signs of HF 2) LVEF
>50% in a nondilated LV (LVEDV Slide 29 Symptoms & Signs of
HF Slide 30 Slide 31 Invasive Diagnostics Prolonged & Tau-
require sophist measurement LVEDP /PCWP - suggested to be
appropriate for of HFNEF in the presence of HF sympts &
LVEF>50% Slide 32 Slide 33 Slide 34 Slide 35 Slide 36 Slide 37
The rate of isovolumic relaxation - best measured by negative dP/dt
max at invasive catheterization The -dP/dt max, which gives the
isovolumic relaxation rate- measured either invasively or by a CW
Doppler velocity spectrum in AR Isovolumic relaxation is when rate
of Ca uptake into the sarcoplasmic reticulum (SR) is Tau- time
constant of relaxation- describes rate of fall of LV pressure
during isovolumic relaxation -also req invasive for precise
determination Slide 38 Slide 39 Isovolumic pressure decay Simplest
way of quantifying the time course of LV pressure decline - peak
-dp/dt Peak -dp/dt - altered by myo relaxation & changes in
loading conditions For eg, LV peak -dp/dt when Ao pressure - ie, in
LV peak -dp/dt from -1,500 to -1,800 mm Hg/sec could be caused by
an in rate of myo relaxation, a rise in Ao pressure, or both LV
peak -dp/dt is during myo ischemia & is in response to adr
stimulation & phosphodiesterase inhibitor milrinone It is not
by digitalis glycosides Slide 40 Echocardiography Currently most
sensitive & widely available technique for assessment of LV
diastolic function TDI Whereas the ratio of early to late diastolic
peak mitral inflow velocities exhibits a J-shaped relationship with
LVEDP, TDI velocities continuously decline from N to advanced LV
diastolic dysfunction As a consequence, E & E/E ratio
continuously with advanced LV diastolic dysfunction Slide 41 E/E
ratio >15 mean diastolic LV pressure >12 mm Hg E/E ratio
>15 - of LV filling pressure and thus HFNEF An E/E ratio 8 15-
asso with very wide range of mean LV diastolic pressures, thus,
further measurements suggested Slide 42 Values for E at the lateral
annulus are generally higher than at medial annulus, resulting in
lower E/E ratios at the lateral annulus Slide 43 Slide 44 Slide 45
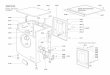
Diastolic Dysfunction LV pressure Grade 1 Grade 2 Grade 3 Grade 4
Mitral flow Tissue Doppler Pulmonary vein E/e E e < 10 10 -15
>15>15 Slide 46 Nagueh et al: JACC, 1997 Ommen et al: Circ,
2000 Annulus e Mitral E E/e As LV filling pressure Slide 47 Slide
48 Slide 49 Measurement of velocity of mitral annular ascent during
early diastole (e vel ) with TDI relatively preload-independent
measure of LV relaxation that correlates inversely with tau E/e
ratio is a fairly accurate predictor of the presence of elevated
filling pressures Slide 50 Slide 51 Area-length method for
calculation of LV mass LVmass=1.05[5/6(A1xL1)-5/6(A2xL2)] Divide by
body surface area to get LV mass index Reichek et al. Circulation
1983;67:348-52 Slide 52 Natriuretic peptides BNP & NT-proBNP-
established tools for exclusion of possible HF in patients
presenting to the emergency room with dyspnea of unclear origin
Among patients with preserved LVEF but not necessarily HF, BNP
& NT-proBNP levels related to severity of LV diastolic
dysfunction Used to distinguish a N from a pseudonormal LV filling
pattern Slide 53 Treatment Aggressive treatment of hypertension and
diabetes Diuretic therapy & dietary salt restrictions is
paramount Compelling indication for ACEI/ARBs in many patients (DM
+LVH), But, Candesartan (the CHARM-PRESERVED trial) Irbesartan (the
I-PRESERVED) Perindopril (the PEP-CHF) Did not reveal a survival
benefit Slide 54 VALIDD [VALsartan In Diastolic Dysfunction] study)
SBP lowering in pts with HTN & LV diastolic dysfunction Either
with a valsartan-based regimen or a regimen not including
inhibitors of the RAAS Similar reduction in BP & an diastolic
relaxation Suggests that BP control may be a key factor in
determining the response to treatment Solomon SD et al. Lancet
2007;369:207987 Slide 55 The Digitalis Investigation Group
Evaluated effects of digoxin on all-cause mortality and HF
hospitalization in patients with HF regardless of EF LVEF >45%
(n = 988) ancillary study parallel to main trial Digoxin - no
effect on all-cause mortality/CV hospitalization Trend toward a in
HF related hospitalizations in hospitalizations for UA Ahmed A et
al. Circulation 2006, 114:397403. Slide 56 TOPCAT trial A trial for
HF pts with preserved systolic function Multi-center,
international, randomized, double blind placebo-controlled trial
Spironolactone 4500 adults with HF &LVEF >45% Enrollment
started -Aug 2006 & is ongoing Slide 57 ACC/AHA Guidelines for
Treatment of Patients with Heart Failure and Normal Left
Ventricular Ejection Fraction-2005 update Class l Control systolic
& diastolic HTN Control ventricular rate in pts with AF
Diuretics to control pulm congestion & periph edema Slide 58
Class lla Cor revascularization in pts with CAD in whom
sympt/demonstrable myo ischemia is judged to be having an adverse
effect on cardiac function Restoration & maintenance of SR in
pts with AF might be useful to improve symptoms Slide 59 Class llb
Use of -blockade, ACEIs, ARBs, or CCA may minimize heart failure
sympt Use of digitalis to minimize sympt is not well established
Slide 60 HFNEFthe Future? Elucidate the mech responsible for HFNEF
Ischemia, uncontrolled HTN, AF must be clearly defined In
particular, inducible ischemia must be searched actively Slide 61
Possible therapeutic strategies Active relaxation - Ca uptake into
the sarc reticulum - sarc reticulum Ca ATP-ase type 2 Gene transfer
suggested possible strategy Percutaneous delivery of a modified
phospholamban encoded in an adenovirus Studeli R et al. Am J
Transplant 2006;6:775 82 Slide 62 Passive LV stiffness - Advanced
glycation end products cross-links breaker, Alagebrium- Pilot study
in 23 HFNEF pts - LV mass & an in E -currently evaluated in a
multicenter study Little WC et al. J Card Fail 2005;11:1915. Slide
63 Role of Sympath nervous system & RAAS in HFNEF is largely
unknown given that LVH is asso with sympath activity & more
severe LVH seems to be asso with likelihood of HFNEF Sympathetic NS
may play a role in the pathogenesis of HFNEF Candesartan has been
shown to the sympath activity Slide 64 -blockers & negatively
chronotropic CCBs HR lowering & prolongation of diastole
results in better LV filling and output Study evaluating purely
HR-lowering agent ivabradine in HFNEF is currently ongoing Slide
65