Embed Size (px)
Citation preview
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
1
SH CP 21
Diarrhoea and Vomiting
(Infection Prevention and Control Policy: Appendix 13)
This Appendix must be read in conjunction with the Infection Prevention and Control Policy
Version: 2
Summary:
The Health Act (2008) stipulates that NHS bodies must, in relation to preventing and controlling the risk of Health Care Associated Infections (HCAI) have in place core policies. This document provides staff with clear guidelines on the actions they must take in order to manage case/s of diarrhoea and vomiting within the community. Implementation of this policy will contribute to the achievement of compliance with the Health Act (2008)
Keywords (minimum of 5): (To assist policy search engine)
Diarrhoea, vomiting, outbreak, isolation, norovirus, Bristol Stool chart, ward closure
Target Audience:
All staff of all disciplines, Non-Executive Directors, Volunteers, Governors and Contractors
Next Review Date: August 2018
Approved & Ratified by:
IP&C Group Date of meeting: 1st May 2014
Date issued:
May 2014
Author:
Mary Pilgrim Infection Prevention & Control Nurse
Sponsor:
Jude Diggins Executive Director of Nursing, AHP &Quality and Director of Infection Prevention and Control
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
2
Version Control
Change Record
Date Author Version Page Reason for Change
01.04.14 Mary Pilgrim & Louise Piper
2 1 Review due to updated version
22.10.14 Mary Pilgrim & Louise Piper
2 9 & 27 Technical Amendment - Infected linen bag change of outer bag cover from red to white
13.3.17 Angela Roberts 2 27 Technical Amendment - Appendix 13.6 terminal clean of isolation room has been strengthened to include advice on radiator cleaning and separate instruction is now available for microfibre and mop and bucket cleaning.
19.9.17 Ann Hammond 2 Ward Outbreak Pack page 8 and 9 & 18
Technical Amendment to Outbreak Pack on page 8– IP&CT contact details amendment and of risk of infection poster added. Amendments made to pages 9 and 18 of actual policy re ward closure and risk of infection posters
7.3.18 Review date extended from April to May 2018
4.5.18 2 Review date extended for 3 months to August 2018 to allow for wider consultation
Reviewers/contributors
Name Position Version Reviewed & Date
IP& C Group members April 2014
IP&C Team April 2014
Liz Taylor Modern Matron, Children’s Division, SHFT April 2014
Carol Cleary TQtwentyone April 2014
Sarah Underwood Ward Manager, Rowan ward, Petersfield Hospital
April 2014
Angela Wilson Ward Manager, Sultan ward, GWMH April 2014
Julie Redman Modern Matron, The Becton Centre, Barton-on-Sea
April 2014
Shelley Mason Modern Matron, Parklands Hospital, Aldermaston Road, Basingstoke
April 2014
Toni Scammell Modern Matron, SE, SHFT (GWMH & Petersfield Hospitals)
April 2014
Brian Murtagh Modern Matron for Hampshire and Southampton
April 2014
Tim Coupland Head of Nursing, AHP & Quality – Mental Health Division
April 2014
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
3
Contents
Page
1. Introduction
4
2. Definitions
4
3. Process (including Ward Outbreak Pack)
6 8
4. Training
16
5. References
16
Appendices:
13.1 Infection Control Action Card – Diarrhoea and Vomiting Outbreak
18
13.2 Disease and/or infective agent and clinical features
19
13.3 Bristol Stool Chart
23
13.4 Summary Flowchart
24
13.5 Daily cleaning procedure for a single isolation room/bed space
25
13.6 Infectious terminal clean of isolation room / bay Microfibre cleaning method Mop and bucket cleaning method
27 32
13.7 Decontamination of Air Mattresses
37
13.8 Clostridium difficile fact sheet
38
13.9 Gastroenteritis fact sheet
40
13.10 Personal Protective Equipment for relatives and visitors
42
13.11 Norovirus Checklist
45
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
4
Diarrhoea and Vomiting
1. Introduction 1.1 For a quick reference guide to managing a potential outbreak please refer to
Appendix 1 (Infection Control Action Card – Diarrhoea and Vomiting) of this document (page number 18) which outlines the key actions to follow.
1.2 This appendix to the overarching Infection Prevention and Control Policy has been
developed to provide a practical document to equip all care staff in the Trust with necessary information on the recognition, management and treatment of outbreaks and/or incidents of diarrhoea and vomiting in inpatient and community settings. Appropriate management of the service user(s) presenting with symptoms of infectious diarrhoea is paramount to reducing the incidence of an outbreak. The two main causes of an outbreak of diarrhoea and/or vomiting in a care setting are either Clostridium difficile and/or gastro-enteritis due to small round structured viruses such as Norovirus (2.14). Another cause for consideration is food poisoning and a food history should always be obtained and investigated for possible links.
Background - there can be many causes of gastroenteritis (diarrhoea and vomiting), such as overeating, excess alcohol, aperients, antibiotics, underlying medical condition and food poisoning, bacterial or viral infection. Symptoms can be varied such as nausea, cramps, headaches, diarrhoea and vomiting. They can range from quite mild to extremely severe. Until investigated, all forms of diarrhoea and vomiting should be treated as potentially infectious.
2. Definitions
2.1 Clostridium difficile is an anaerobic, gram positive spore forming Bacillus that can
cause an infection in the gut (refer to Appendix 13.7 of this document - Patient and Staff Information leaflet).
These spores are resistant to heat, alcohol and acids in the stomach, and can survive in patients and the surrounding environment for long periods of time. (Healthcare Commission: Management, prevention and surveillance of Clostridium difficile 2005). Following antibiotic therapy the intestinal flora is altered which allows any Clostridium difficile bacteria to proliferate. The bacteria produce two toxins, Toxin A and Toxin B. For further information please refer to Clostridium Difficile Appendix 15 Infection Prevention and Control Policy.
2.2 Cohort nursing – a group of service users with a disease or infection who are
separated from service users who do not harbour the disease or infection and who are nursed in a geographically distinct area e.g. bay.
2.3 Confirmed outbreak – results from laboratory specimens to identify cause of
symptoms and/or pattern of outbreak which suggests transmission of infection
2.4 Decant Ward – if two or more wards are affected by a norovirus outbreak, in the
later stages of the outbreak there may be value in moving all affected patients and recovered patients to one ward to allow earlier cleaning and re-opening of an empty ward. (HPA 2011 Guidelines for the management of norovirus outbreaks)
2.5 Diarrhoea – frequent episodes of loose stools type 6/7 (see Appendix 13.2 of this
document - Bristol Stool Chart) this implies more than 3 episodes per day or more
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
5
than is usually experienced by the symptomatic person.
2.6 Environmental Contamination – the area around the service user is
contaminated with microbes capable of causing infection, e.g. norovirus infectivity can last for 48 hours after resolution of symptoms. Contaminated hands can transfer norovirus sequentially to up to seven clean surfaces. (HPA 2011 Guidelines for the management of norovirus outbreaks). Soft furnishings should be steam cleaned or laundered. Soiling with vomit should ideally be cleaned to a radius of two metres and people taken out of the area until it is done. (Working party of former PHLS Advisory Committee on GI Infections 2004).
2.7 Exclusion Rule – staff should be excluded from the workplace for 48 hours after
all symptoms of diarrhoea and/or vomiting have ceased. Symptomatic service users are required to be clear of symptoms for 48 hours prior
to being deemed fully recovered. For further advice on an individual basis please contact the IPCT
2.8 Hand Hygiene – before and after each patient contact, after environmental
contact and when moving between “clean” and “dirty” sites on the same patient World Health Organisation (WHO 2006) Five moments for Hand Hygiene (refer to Hand Hygiene Appendix 6 Infection Prevention and Control Policy).
2.9 Infectious diarrhoea - can be caused by many organisms including Escherichia
coli sp, Salmonella sp, Shigella sp, Campylobacter sp, rotavirus to name but a few. Other causes of diarrhoea to consider are Clostridium difficle (bacteria) and Norovirus (viral diarrhoea), (refer to Appendix 13.1 of this document for further details).
2.10 Isolation room – a single room often with its own hand washing and toilet facilities.
2.11 Major Outbreak – an outbreak may be classed MAJOR after consideration of its
complexity, the number of people affected, the pathogenicity of the organism involved, the potential for transmission and any other unusual or exceptional features. The DIPC (Director of Infection Prevention and Control) or CCDC (Consultant of Communicable Disease Control) will make this decision. A significant number of cases of diarrhoea and vomiting involving several wards at the same site may be classed a major outbreak (refer to Outbreak of Infection & Major Outbreak Appendix 8 Infection Prevention and Control Policy)
2.12 Outbreak of diarrhoea and/or vomiting – when two or more service users
present with the same symptoms of diarrhoea and/or vomiting not associated with any underlying clinical condition in the same clinical setting. May also be used to refer to a local cluster of cases.
2.13 Outbreak resolved - an outbreak will be considered to be over when there has
been a period of 48 hours after the resolution of vomiting and/or diarrhoea in the last known case and at least 72 hours after the presentation of the last new case.
Often there can be a small number of patients with persistent symptoms these will be isolated or cohorted in order to facilitate the return to normal activity.
2.14 Small round structured virus (SRSV e.g. Norovirus or Rotavirus). - Norwalk -
like virus, are the most common causes of outbreaks in hospitals and can also cause outbreaks in other settings such as schools, hotels, residential and nursing homes and cruise ships (HPA 2011 Guidelines for the management of norovirus
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
6
outbreaks). (Refer to Appendix 13.8 of this document - Patient and Staff Information leaflet).
2.15 Serious Incident (SI) – an episode that requires reporting and investigating in view
of Patient Safety and Quality. Any ward closure is classified as an SI. 2.16 Serious Incident Panel - a panel involving all parties to investigate the outbreak
and put in place an action plan for future learning.
2.17 Ward/ Service closure – if a ward/unit is closed due to an outbreak of diarrhoea
and/or vomiting it will be considered a Serious Incident (SI) and will require a report on the Trust reporting system by ward staff.
2.18 Ward Outbreak Pack – this is a separate pack of instructions to be used as an aide
memoire to the local management of the outbreak and includes closure signs and checklists etc. (inpatient areas only) – see page 8 for pack.
3. Process
3.1 The management of diarrhoea and/or vomiting requires commitment and adherence from the Trust and all staff involved. The effect on a service user and/or member of staff involved in an incident and/or outbreak of this kind can be far reaching. Therefore the management of the situation should be led by the Infection Prevention and Control Team and supported by the key personnel in the Trust responsible for the service user stay and their holistic care. Infection control provide advice based on experience, research and evidence and follow procedures in place to safeguard all involved and to bring the situation to a safe conclusion.
3.2 Methods of Transmission of Infection - transmission of organisms, which cause
diarrhoea and/or vomiting, is mainly by the faecal-oral route (unwashed hands after visiting the toilet and handling patient’s soiled clothing, bed linen etc). Some organisms are spread by direct contact or through aerosoled viruses in vomit droplets. Widespread environmental contamination during bouts of diarrhoea and/or vomiting occurs. Food borne illness can occur directly through environmental contamination as above and also ingestion. Norovirus’s mode of transmission is contact via the faecal-oral route and airborne via inhalation followed by ingestion of norovirus – contaminated aerosolised vomit. NB 30 mls of vomit =30,000,000 virus particles which are considered highly infectious only 50-100 particles are required for an infection to occur. (HPS 2013).
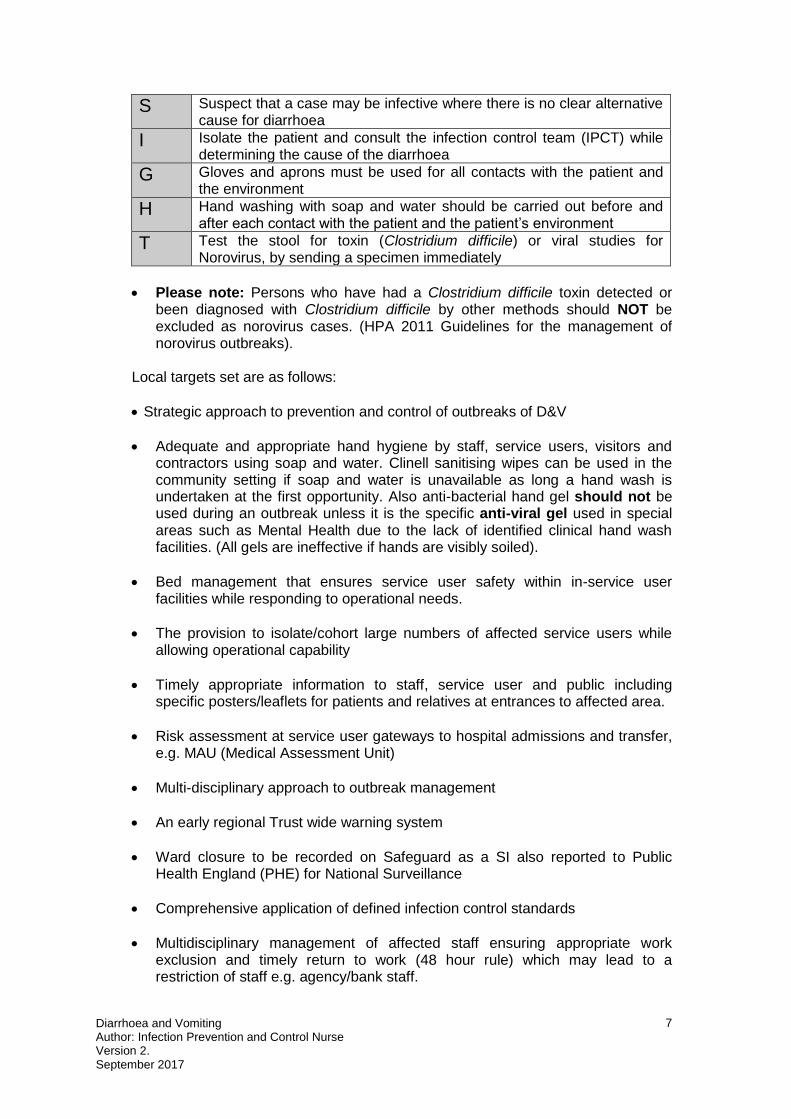
3.3 Local Management of Diarrhoea and Vomiting within the Trust Key recommendations: Clinicians (doctors and nurses) should apply the following mnemonic protocol (SIGHT) when managing suspected potentially infectious diarrhoea (DH
Clostridium difficile infection: How to deal with the problem 2009).
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
7
S Suspect that a case may be infective where there is no clear alternative cause for diarrhoea
I Isolate the patient and consult the infection control team (IPCT) while determining the cause of the diarrhoea
G Gloves and aprons must be used for all contacts with the patient and the environment
H Hand washing with soap and water should be carried out before and after each contact with the patient and the patient’s environment
T Test the stool for toxin (Clostridium difficile) or viral studies for Norovirus, by sending a specimen immediately
Please note: Persons who have had a Clostridium difficile toxin detected or been diagnosed with Clostridium difficile by other methods should NOT be excluded as norovirus cases. (HPA 2011 Guidelines for the management of norovirus outbreaks).
Local targets set are as follows:
Strategic approach to prevention and control of outbreaks of D&V
Adequate and appropriate hand hygiene by staff, service users, visitors and contractors using soap and water. Clinell sanitising wipes can be used in the community setting if soap and water is unavailable as long a hand wash is undertaken at the first opportunity. Also anti-bacterial hand gel should not be used during an outbreak unless it is the specific anti-viral gel used in special areas such as Mental Health due to the lack of identified clinical hand wash facilities. (All gels are ineffective if hands are visibly soiled).
Bed management that ensures service user safety within in-service user facilities while responding to operational needs.
The provision to isolate/cohort large numbers of affected service users while allowing operational capability
Timely appropriate information to staff, service user and public including specific posters/leaflets for patients and relatives at entrances to affected area.
Risk assessment at service user gateways to hospital admissions and transfer, e.g. MAU (Medical Assessment Unit)
Multi-disciplinary approach to outbreak management
An early regional Trust wide warning system
Ward closure to be recorded on Safeguard as a SI also reported to Public Health England (PHE) for National Surveillance
Comprehensive application of defined infection control standards
Multidisciplinary management of affected staff ensuring appropriate work exclusion and timely return to work (48 hour rule) which may lead to a restriction of staff e.g. agency/bank staff.
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
8
Ensure all staff (including bank and agency) who have been exposed to an outbreak situation are not transferred/moved to non-affected areas to work and remain in the area for the duration of their shift.
Daily communication is required during an outbreak with the ward/unit representative, Infection Prevention and Control Team and facilities management. If a face to face meeting is not possible Trust teleconferencing facilities may be used.
Visitor restriction may be required
Communication Team may need to be informed due to possible Press coverage.
3.4 Communication - It is important that everyone is aware of the infection prevention
and control precautions that need to be in place to manage D&V. Appropriate/relevant staff involved in service user care/interventions must be informed of the potential risks of the service user’s infective diarrhoea. In addition to this, daily outbreak updates are available from the Infection Prevention and Control Team.
Care staff must be empowered to provide the individual with appropriate information about D&V. This must be supported with the use of information leaflets (refer to Appendices 13.7 and 13.8 of this document). The care staff must explain to the service user and relatives that the service user has potentially infective diarrhoea and the rationale for further management e.g. the need for isolation/cohort until 48 hours clear from symptoms.
If service users and/or carers require adapted communication please contact the IP&C team for support. 3.5 Outbreak management Please print a copy of the outbreak pack embedded in this document (see
associated documents), this will guide you through the actions you need to manage on a daily basis.
Ward Outbreak Pack March 2014 revised.doc
Immediate Action – Community Hospital and Mental Health Settings (refer to
Appendix 13.3 of this document) The Ward/Clinical Manager or deputy (Nurse in charge) will coordinate the initial
response to the outbreak in consultation with the Infection Prevention and Control Team (IPCT)
This will involve:
Informing the IPCT immediately by telephone during core hours. Outside these periods the on call Modern Matron/Manager should be informed.
Set up daily communications between IPCT and the unit ward managers
Informing Facilities Management to provide continuity of cleaning. This is to: a) provide reassurance that an enhanced clean is taking place daily and a
terminal clean when situation is resolved
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
9
b) ensure levels of cleaning are increased in cases of infection and/or colonisation when a suspected or known pathogen can survive in the environment. Environmental contamination may contribute to the spread of infection ( sp1 epic 3 2014)
Identifying whether there is an alternative reason for diarrhoea and/or vomiting, such as an underlying disease or medication.
All patients and staff presenting with symptoms having their details and symptom history recorded on the outbreak reporting form (Ward Outbreak Pack available from Infection Control also embedded in this document 2.18). Staff must be made aware of the 48 hour rule which means that they must remain off duty for 48 hours after their last known symptom to reduce the risk of transmission to others on their return to work. Staff should always maintain excellent hand hygiene.
Closure of the bay/ward The decision to close the ward will be made by the IP&C Team with the ward manager and the DIPC and Professional lead will subsequently be informed.
Arranging stool specimens to be taken from all symptomatic individuals, for definitions of diarrhoea please refer to the Bristol Stool Chart (refer to Appendix 13.2 of this document). The stool must be type 6 or 7 and take up the shape of the container. If samples are contaminated with urine they can still be processed. The laboratory should be asked for a viral screen on all samples, this should be also identified on the specimen request form e.g. Stool for viral studies/ Clostridium difficile screen. Up to a maximum of six specimens of faeces from the group of affected patients should be submitted for Norovirus detection in the first instance. (HPA 2011 Guidelines for the management of norovirus outbreaks) NB Stool samples collected over a weekend should be sent to the local Laboratory by taxi, so they are not delayed.
Instigate the Ward Outbreak Pack (embedded in 2.18 of this document) including risk of infection and ward closure posters at all entrances/ward reporting form etc.
Ensure orange bags are available for the disposal of clinical waste and to replace tiger stream bags during the outbreak period.
Ensure safe disposal of linen to include use of alginate bags (as per manufacturer’s guidance) as well as white outer bags. Please make sure that the bags are not overfilled as this will reduce the risk of cross infection.
Relay all relevant information concerning affected patients during subsequent change over of clinical staff and include the status of the ward i.e. open or closed. This is aimed at preventing complications such as dehydration. Escalate outbreak information to microbiologist/laboratory for results and advice. (Usually undertaken by IPCN).
Hand Hygiene – as a minimum hands should be washed with soap and water at the start and end of clinical duties, when hands are visibly soiled or potentially contaminated, following removal of gloves and before and after any clinical intervention, (refer to Hand Hygiene Appendix 6 IP&C Policy).
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
10
3.6 Isolation
The isolation of cases within single rooms and bays ideally with an en-suite facility as opposed to the early closure of complete wards allows flexibility of response and the early terminal cleaning and re-opening of affected bays. Only when there is evidence of failure of containment within all available single-occupancy rooms and bays should whole ward closure be considered. This is an important change to previous guidance which advised the early closure of whole wards. (HPA 2011 Guidelines for the management of norovirus outbreaks) Symptomatic patients should be nursed in isolation where possible and a risk assessment should be done if the patient presents with any other clinical need or to avoid compromising the patient/service users medical and psychological welfare by unnecessary restrictive infection control measures. Patients in shared facilities/rooms/bays presenting with symptoms may be nursed together (cohort) and should be cared for by a designated team to avoid transmission to non-affected patients. Avoid cohort nursing individuals with diarrhoea of different aetiologies (causes or diagnosis) The clinical needs of the service user are of paramount importance if neither a single room or cohort nursing is available then single bed barrier nursing with strictly enforced source isolation must be adhered too following discussion with IP&C Team only.
Risk Assessment prior to isolation must be undertaken, e.g. risk of falls, confusion etc. Be aware that patients may present with similar symptoms but may in fact be identified as having different aetiologies ( Clostridium difficile or norovirus)
3.7 Service user Admission/Movement and Transfers
Prior to admission/transfer of a service user the following questions should be considered:
Is the service user known to be currently suffering from diarrhoea and/or vomiting?
Has the service user had a history of diarrhoea and/or vomiting in the past?
Has the service user come from a known outbreak/infectious care setting
Has the service user recently had an inpatient stay in a healthcare institution?
Has the service user an existing contributing condition that may present with diarrhoea and/or vomiting?
Priority order
Service users with viral gastroenteritis / diarrhoea
1 Single room or cubicle within the specialty, ensuite- toilet if possible or a dedicated commode
2 To a cohort nursing area – refer to Isolation - Appendix 9 of the Infection Prevention and Control Policy
3 A single bed isolation area close to a clinical washbasin within an existing bay. Strict source isolation nursing MUST be enforced refer to Isolation procedure (viral diarrhoea) and discussion with IP&C Team
4 Consider reverse barrier nursing if minority of service users are affected, removing immunocompromised non affected service users into side rooms
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
11
Has the service user been prescribed antibiotics?
Has the service user an alternative method of feeding, e.g. PEG, Naso-gastric tube?
Has the service user provided a recent stool specimen?
Has the service user a known history of Clostridium difficile, with a positive stool in the past 28 days?
Consider food poisoning if patient/service user shows symptoms within 3 days of admission and of duration of more than 3 days?
Has the service user been prescribed any laxatives?
Is there an accurate documentation and reporting of symptoms, fluid balance and bowel movements? Does the Nurse in charge have an in-depth knowledge of the service user involved in the outbreak so as to be able provide a comprehensive update on a daily basis?
The movement of service users with diarrhoea and/or vomiting or their contacts
(when dealing with viral diarrhoea) within the Trust or to other health care settings or communal residences should be minimised to reduce the risk of cross infection, and any potential embarrassment for the service user.
If any informal service users wish to go on leave, staff are required to escort them to the reception area of the building and then to collect them on their return. Any informal service users who are experiencing symptoms are requested to remain on the ward to prevent the spread of infection to the wider hospital. All discussions with the service user should be documented in their record.
Where service users need to attend departments for essential lifesaving investigations the receiving area should be notified of the service user’s D&V status in advance of transfer, and arrangements should be put in place to minimise the contact with other service users. Staff should take standard precautions whilst in contact with the service user. Arrangements for transfer to other healthcare facilities, e.g. hospitals, should include notification of the individual’s D&V status, as appropriate and be made following advice from the Infection Prevention and Control Team. (Refer to Admission, Discharge and Transfer Policy) Non-essential treatments e.g. visits to physiotherapy gyms, OT assessments should be postponed until the service user is symptom free for 48 hours
Staff who are transferring service users who require an enhanced level of care must ensure that:
The receiving area is aware of the service user’s D&V status
If the service user is being moved to another ward/unit the receiving area has the appropriate level of isolation nursing available
If the service user is on antibiotics and/or stool charts these MUST be sent with the service user.
Portering staff who are transferring service users should wear appropriate PPE (gloves and/or aprons depending on contact risk) only when in contact with service user; however they MUST cleanse their hands before and after the job using soap and water.
The service user is transferred to a clean bed with clean linen or if a trolley or chair is used this must be cleaned with detergent followed by a chlorine based
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
12
disinfectant e.g. Actichlor Plus solution that contains both components before being used on another service user.
Ambulance staff MUST adhere to their own policy.
3.8 During the Service Users Stay
The service user:
Must be actively encouraged to keep the bed space free from clutter to enable cleaning to be carried out to a high standard.
Must be discouraged from keeping open food stuff at bedside.
Must be actively encouraged to inform nursing staff of bowel movements to ensure the accurate recording of a stool chart and provide a stool specimen (stool specimen forms should indicate if viral and/or bacterial screen is required).
Must be actively encouraged to observe good hand hygiene at every opportunity preferably with soap and water.
Must be encouraged to follow instructions from healthcare staff to limit any cross transmission e.g. this may include the restriction on staff movement between clinical areas.
If compliant and not detrimental to mental health the service user must remain in isolation as advised by IP&C team.
If identified as Clostridium difficile positive must be encouraged to wash using soap and water as alcohol gel is not affective against spores. (Appendix 15 of the IP&C Policy).
The staff.
Personal Protective Equipment (PPE) should be worn by staff carrying out clinical care or cleaning of the environment/equipment (gloves and/or aprons depending on the task/risk), (refer to Appendix 13.9 of this document).
Service user’s water jugs should be renewed by staff as required ensuring that one member of the team remains in the infected bay and is supported to deliver meal trays and/or jugs by a member who presides in the unaffected area.
Hand washing with a liquid soap should be undertaken before and after service user contact by staff and following removal of PPE.
The nurse in charge of the shift is to ensure documentation of service users stool history is accurate and up to date.
The visitor
Visitors should be restricted and children of school age should be discouraged for the duration of the outbreak because of the risk of sudden symptoms developing without warning in school. (HPA 2011 Guidelines for the management of norovirus outbreaks)
Signage should be on display to inform visitors if there is an outbreak or ward closure.
3.9 Surgical Interventions
Every effort should be made to eliminate D&V before surgery if this is not possible then the following strategy must be adopted
D&V service users should be scheduled for surgery (only if lifesaving) for further advice consult the Infection Prevention and Control Team.
Bathe/shower the service user with antiseptic detergent e.g. chlorhexidene
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
13
gluconate 4% prior to surgery to reduce risk of transmission.
All theatre surfaces in contact with the service user should be decontaminated post operation according to theatre policy
D & V service users in recovery must be segregated wherever feasible and nursed by dedicated staff adhering to isolation procedures
At the end of every operating session the table and any other equipment must be cleaned using detergent solution, followed by hypochlorite solution (Actichlor plus) and dried.
3.10 Service User Discharge
D&V service users should be discharged promptly from hospital when their clinical condition allows.
The General Practitioner and other healthcare agencies, including if appropriate, Community Infection Prevention and Control Teams (IPCT), involved in the service user’s care should be informed.
D & V service users will not normally require special treatment after discharge from hospital. If a treatment course needs to be completed in particular circumstances the IPCT team should advise about this.
If the service user is discharged to a residential care facility the medical and/or nursing staff should be informed in advance. The service user should be 48 hours free from symptoms in order to reduce the risk to the other residents of transmission of infection. However, discharge to a home (nursing or residential) known to be affected by an outbreak at the time of discharge should not be delayed providing the home can safely meet the individual’s needs. Those that have been exposed but are not symptomatic maybe discharged only on the advice of the local Public Health England office or IPCT (Infection Prevention and Control Team).
Carers must be alerted to the risk of diarrhoea and/or vomiting infection. If visiting in a care facility or clients own home and they themselves have been symptomatic they should be discouraged from contact until 48 hours clear.
If a service user has been identified as medically fit for an early facilitated discharge under the care of the Community Care team (CCT), Outreach team or CPN, they should ideally be 48 hours free from symptoms. This is because despite being discharged to their own homes they will be receiving for example, visits from members of staff from the CCT 2-3 times each day, who will also be visiting other service users in between.
3.11 Deceased Service User
The Infection Prevention and Control precautions for handling the deceased service users are the same as those used in life. Any lesions should be covered with impermeable dressings. Black body bags may be used as part of general practice in accordance with standard precautions for all service users. There is a negligible risk to mortuary staff and/or undertakers, provided standard precautions are employed. It is not necessary to inform the mortuary that the service user had D&V. (Refer to the Care of the Deceased Patient Appendix 19 Infection Prevention and Control Policy)
3.12 Visitors
During an outbreak of gastroenteritis, the service manager in consultation with the IPCT should advise restricted visiting. Visitors should therefore be advised of the situation and warned that they may be at risk of illness. This should occur prior to them entering the ward in order that they can make an informed decision to visit.
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
14
All visitors should be encouraged to wash their hands with soap and water when visiting.
3.13 Staff Movement
Due to the risk to staff of certain conditions, even if correct personal protective equipment (PPE) has been used, staff movement from one clinical area to another must be avoided for the duration of the shift. Ideally staff working in an outbreak area should remain there for the duration of the outbreak. It is very important that this advice includes housekeeper and facilities staff as they are frequently expected to work across more than one clinical area and therefore may spread the virus to an non-affected ward/unit.. Consideration should be given to pregnant staff who should avoid working in a closed unit/ward until the causative organism is identified and following advice from Occupational Health. Other staff including doctors, physiotherapists, radiographers and social workers can continue to work in affected and unaffected areas, however outbreak areas should be visited last if necessary and meticulous hand hygiene should be undertaken and appropriate PPE worn.
3.14 Patients/Service Users in the Community (e.g. Supported Living) with
Diarrhoea and Vomiting These service users are under the care of their own General Practitioners who
should be advised of the patient’s debility if the symptoms are severe as well as review any current medications.
Members of healthcare staff who work with the affected service users must adopt Standard Infection Control Precautions particularly in regards to hand hygiene.
Service users and carers in these settings should have the importance of hand hygiene and all other precautions explained. Service users in the community who are symptomatic should not attend community day care clinics / facilities until 48 hours after their symptoms have resolved
Service users who are symptomatic must be encouraged to stay out of the kitchen and not be involved in food handling and/or preparation.
Service users must be encouraged to stay in their own bedrooms if possible while symptomatic.
During the outbreak enhanced daily cleaning of bedrooms and bathrooms should be undertaken.
3.15 Patient/Service Users Community Respite Facilities
Unless clinically imperative patients/service users who have symptoms should not be admitted for respite care until 48 hours after symptoms have resolved. However, if symptomatic patients require admission they should be admitted into an isolation room and all precautions taken.
3.16 Cleaning in the Environment and Equipment
The management of the environment and equipment should be considered as central to minimising the spread of D &V. Cleaning regimens for isolation facilities should focus on removal of dust and infectious organisms from frequently touched surfaces as dust contains spores and harmful organisms, therefore dust must be kept to a minimum. For example, the ability of Clostridium difficile spores to survive for long periods demonstrates the need for dust minimalisation and the requirement for the appropriate disposal of contaminated waste and linen. Trust policies, environmental
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
15
cleaning and equipment decontamination, waste and linen management should state necessary standards, and must be rigorously applied. (Refer to EPIC 3 2014) There should be a two-fold approach;
firstly, the management of the occupied facility
secondly, terminal clean of the facility after the discharge of the service user or resolution of the outbreak.(A sign off sheet should be kept as evidence that a terminal clean has been carried out after discharge of the service user or at the end of the outbreak), (refer to Appendix 13.6 of this document)
When there is diarrhoea or vomiting present within a supported living home, a chlorine cleaning product is necessary to clean the affected areas, in particular toilets and bathrooms. Detergent alone is not sufficient to clean. 1) Household bleach needs to be diluted as per manufacturer’s instructions to avoid personal injury (Domestos or equivalent may be the only product available so can be used as required). 2) Service user equipment e.g. wheelchairs, hoists, slings, sphygmomanometer cuffs etc. should be capable of being decontaminated before use by other service users, or should be single service user use and discarded as clinical waste at the end of the period of usage.
3.17 Routine Cleaning of the Occupied Facility (refer to Appendix 13.4 of this
document)
Instruments or equipment (e.g. sphygmomanometers, stethoscopes, lifting slings, and physiotherapy exercise machines) should preferably be single service user use, or designated for D&V service users, these should be cleaned daily with detergent and chlorine containing solution e.g. Actichlor plus.
Multiple-service user use items should be decontaminated appropriately before use on another service user in accordance with Trust policy or manufacturer’s instructions e.g. toilets, commodes etc.
It is essential that clutter around the bed space is kept to a minimum to aid good nursing practice and facilitate cleaning.
Stains, soiling, food residue etc. should be removed with a detergent solution – disinfectants on their own do not clean
Enhanced daily clean, lockers, over-bed tables and chairs should be cleaned daily with detergent and a chlorine based disinfectant e.g. Actichlor plus. The mattress and bed frame should be wiped over daily with detergent. If the admission is more than two weeks wherever possible the service user should be given a clean bed and the current bed thoroughly cleaned with detergent.
In some settings where isolation of the affected patient cannot be managed i.e. in Adult mental health settings, the IP&C team will recommend that communal areas are included in the daily clean with Actichlor plus. In addition healthcare workers will be advised to clean commonly touched objects e.g. door handles and light switches at least twice daily with Clinell sanitising wipes.
3.18 Terminal Cleaning on Service User/Inpatient Discharge following resolution
of the outbreak/Transfer/Death (refer to Appendix 13.5 of this document) Enhanced levels of cleaning requiring additional time to enable the removal of all reservoirs of dust, e.g. ventilation ducts, radiators, equipment etc. are required. Infected diarrhoea service user areas should be cleaned after the service user’s discharge according to Trust policy, this includes; (refer to Appendix 13.4 for guidance and Appendix 13.5 for cleaning schedule checklist sign off sheet).
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
16
* Steam cleaning is highly effective in the removal of organic matter but may not inactivate norovirus. Therefore hypochlorite disinfection is still required for areas which have been previously steam cleaned. Disposable cloths should be used for each bed space. (HPA 2011 Guidelines for the management of norovirus outbreaks).
Additionally there should be planned, periodic and thorough cleaning of the whole ward, including bedding, soft furnishings and curtains
3.19 Defining the end of an outbreak This also serves two purposes which, again, may have two different
approaches: a) Declaration of the end of an outbreak for Infection Prevention and
Control (IPC) The definition is usually set, on the basis of experience, as 48hr after the resolution of vomiting and/or diarrhoea in the last known case and at least 72hr after the initial onset of the last new case. This is also the point at which terminal cleaning has been completed. Often, there are a small number of patients with persistent symptoms and it is advisable to segregate those patients in order to facilitate a return to normal activity. Symptomatic patients may be moved into single rooms or otherwise within a cohort away from the area to be cleaned. There is thought to be little risk of prolonged airborne persistence of virus and terminal cleaning of an area such as a ward can commence immediately after the removal of the symptomatic patients.
b) Epidemiological surveillance. The end of an outbreak is defined as no new cases recognised within the previous 7 days. (HPA Guidelines 2011).
4. Training: Refer to Training Needs Analysis (TNA) in IP&C Policy
5. References Department of Health 2009, Clostridium difficile infection: How to deal with the problem. epic 3 :National Evidence-Based Guidelines for Preventing Healthcare-Associated Infections in NHS Hospitals in England. 2014 H.P.Loveday, JA Wilson, RJ Pratt, M Golsorki, A Tingle, A Bak, J Browne , J Prieto, M Wilcox Healthcare Commission 2005: Management, prevention and surveillance of Clostridium difficile.
Health Protection Agency, November 2011: Guidelines for the Management of norovirus outbreaks in acute and community health and social care settings. Norovirus Working Party 2010 .
Health Protection Scotland, 2013: HPS Norovirus Outbreak Guidance
Preparedness, control measures & practical considerations for optimal patient safety and service continuation in hospitals. Version 2 September 2013.
Solent NHS Trust, 2011. Policy for the Management of Diarrhoea and Vomiting Outbreaks
Working Party of former PHLS Advisory Committee on GI Infections 2004:

Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
17
Preventing person to person spread following gastrointestinal infections: guidelines for public health physicians and environmental health officers. Communicable Disease and Public Health vol7 no 4 pages 362-384
World Health Organisation (2009) WHO Guidelines on Hand Hygiene in Healthcare - First Global Patient Safety Challenge Clean Care is safe care.
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
18
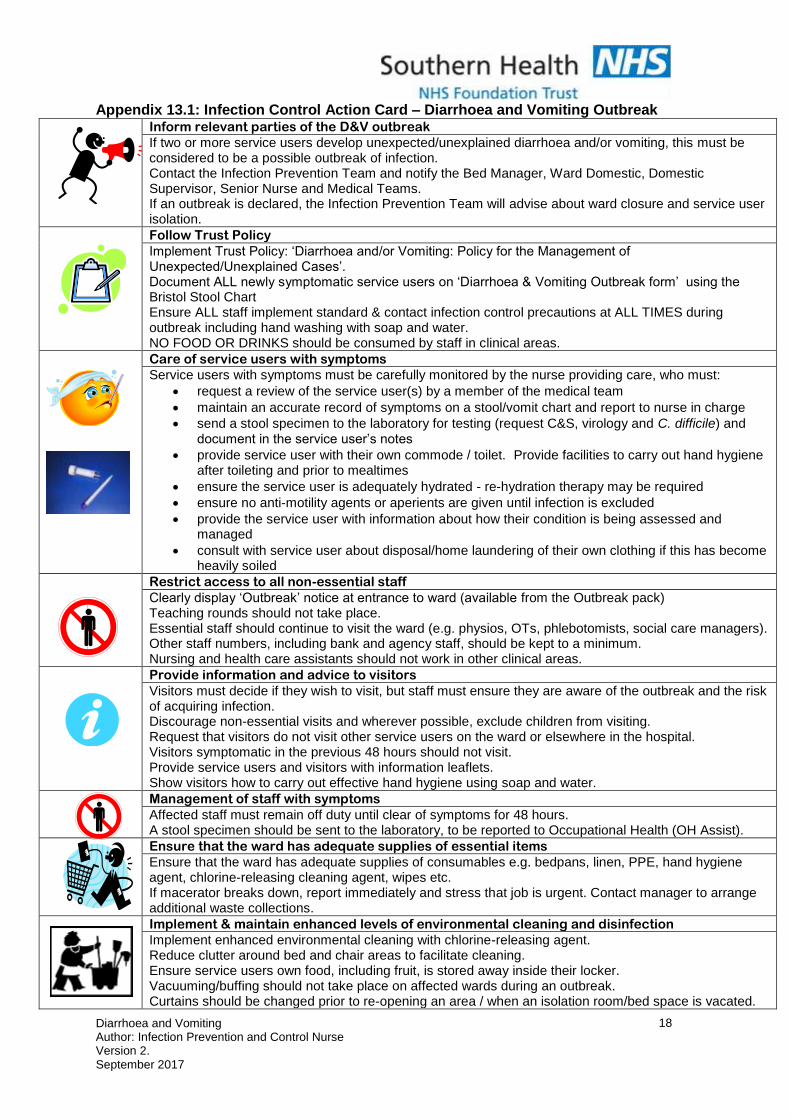
Appendix 13.1: Infection Control Action Card – Diarrhoea and Vomiting Outbreak Inform relevant parties of the D&V outbreak
If two or more service users develop unexpected/unexplained diarrhoea and/or vomiting, this must be considered to be a possible outbreak of infection. Contact the Infection Prevention Team and notify the Bed Manager, Ward Domestic, Domestic Supervisor, Senior Nurse and Medical Teams. If an outbreak is declared, the Infection Prevention Team will advise about ward closure and service user isolation.
Follow Trust Policy
Implement Trust Policy: ‘Diarrhoea and/or Vomiting: Policy for the Management of Unexpected/Unexplained Cases’. Document ALL newly symptomatic service users on ‘Diarrhoea & Vomiting Outbreak form’ using the Bristol Stool Chart Ensure ALL staff implement standard & contact infection control precautions at ALL TIMES during outbreak including hand washing with soap and water. NO FOOD OR DRINKS should be consumed by staff in clinical areas.
Care of service users with symptoms
Service users with symptoms must be carefully monitored by the nurse providing care, who must:
request a review of the service user(s) by a member of the medical team
maintain an accurate record of symptoms on a stool/vomit chart and report to nurse in charge
send a stool specimen to the laboratory for testing (request C&S, virology and C. difficile) and document in the service user’s notes
provide service user with their own commode / toilet. Provide facilities to carry out hand hygiene after toileting and prior to mealtimes
ensure the service user is adequately hydrated - re-hydration therapy may be required
ensure no anti-motility agents or aperients are given until infection is excluded
provide the service user with information about how their condition is being assessed and managed
consult with service user about disposal/home laundering of their own clothing if this has become heavily soiled
Restrict access to all non-essential staff
Clearly display ‘Outbreak’ notice at entrance to ward (available from the Outbreak pack) Teaching rounds should not take place. Essential staff should continue to visit the ward (e.g. physios, OTs, phlebotomists, social care managers). Other staff numbers, including bank and agency staff, should be kept to a minimum. Nursing and health care assistants should not work in other clinical areas.
Provide information and advice to visitors
Visitors must decide if they wish to visit, but staff must ensure they are aware of the outbreak and the risk of acquiring infection. Discourage non-essential visits and wherever possible, exclude children from visiting. Request that visitors do not visit other service users on the ward or elsewhere in the hospital. Visitors symptomatic in the previous 48 hours should not visit. Provide service users and visitors with information leaflets. Show visitors how to carry out effective hand hygiene using soap and water.
Management of staff with symptoms
Affected staff must remain off duty until clear of symptoms for 48 hours. A stool specimen should be sent to the laboratory, to be reported to Occupational Health (OH Assist).
Ensure that the ward has adequate supplies of essential items
Ensure that the ward has adequate supplies of consumables e.g. bedpans, linen, PPE, hand hygiene agent, chlorine-releasing cleaning agent, wipes etc. If macerator breaks down, report immediately and stress that job is urgent. Contact manager to arrange additional waste collections.
Implement & maintain enhanced levels of environmental cleaning and disinfection
Implement enhanced environmental cleaning with chlorine-releasing agent. Reduce clutter around bed and chair areas to facilitate cleaning. Ensure service users own food, including fruit, is stored away inside their locker. Vacuuming/buffing should not take place on affected wards during an outbreak. Curtains should be changed prior to re-opening an area / when an isolation room/bed space is vacated.
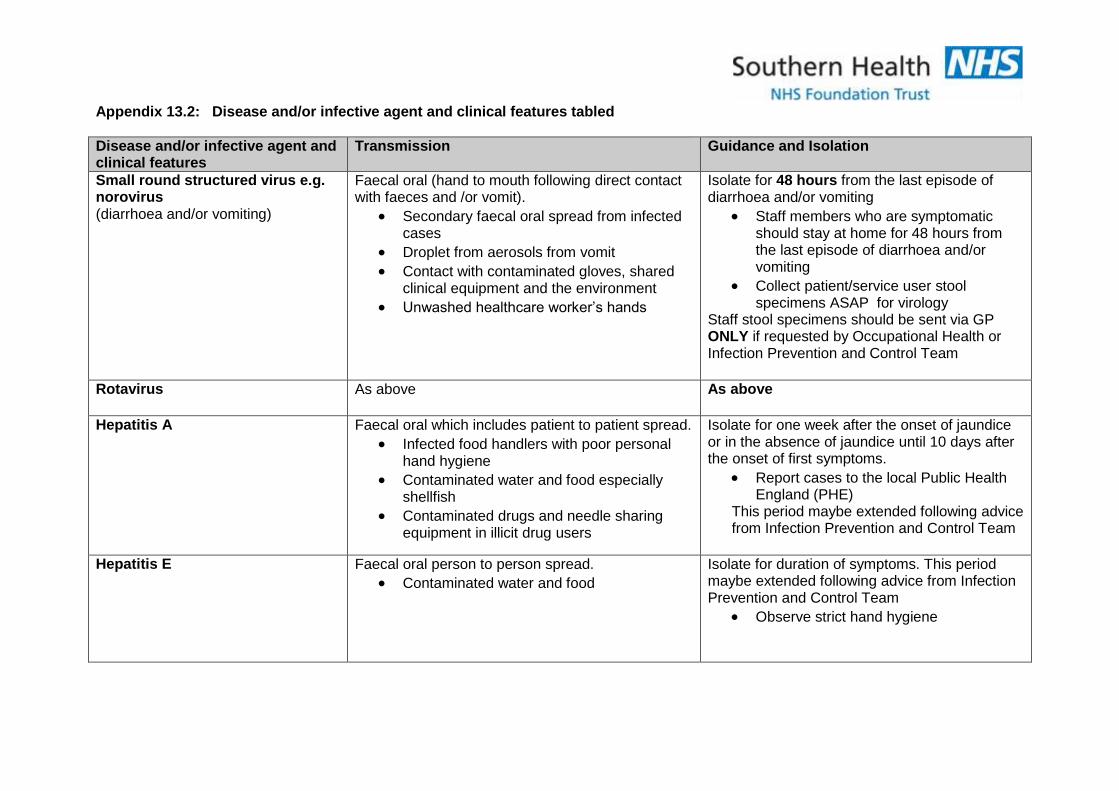
Appendix 13.2: Disease and/or infective agent and clinical features tabled
Disease and/or infective agent and clinical features
Transmission Guidance and Isolation
Small round structured virus e.g. norovirus (diarrhoea and/or vomiting)
Faecal oral (hand to mouth following direct contact with faeces and /or vomit).
Secondary faecal oral spread from infected cases
Droplet from aerosols from vomit
Contact with contaminated gloves, shared clinical equipment and the environment
Unwashed healthcare worker’s hands
Isolate for 48 hours from the last episode of diarrhoea and/or vomiting
Staff members who are symptomatic should stay at home for 48 hours from the last episode of diarrhoea and/or vomiting
Collect patient/service user stool specimens ASAP for virology
Staff stool specimens should be sent via GP ONLY if requested by Occupational Health or Infection Prevention and Control Team
Rotavirus As above As above
Hepatitis A Faecal oral which includes patient to patient spread.
Infected food handlers with poor personal hand hygiene
Contaminated water and food especially shellfish
Contaminated drugs and needle sharing equipment in illicit drug users
Isolate for one week after the onset of jaundice or in the absence of jaundice until 10 days after the onset of first symptoms.
Report cases to the local Public Health England (PHE)
This period maybe extended following advice from Infection Prevention and Control Team
Hepatitis E Faecal oral person to person spread.
Contaminated water and food
Isolate for duration of symptoms. This period maybe extended following advice from Infection Prevention and Control Team
Observe strict hand hygiene
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
20
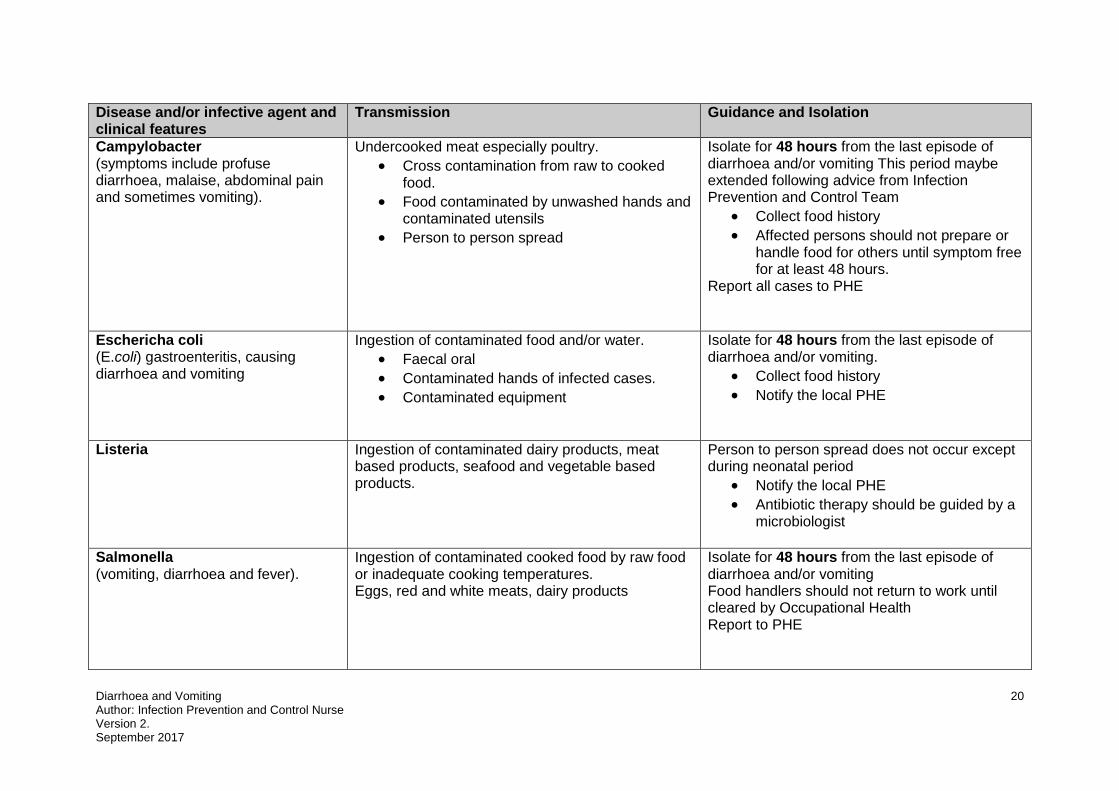
Disease and/or infective agent and clinical features
Transmission Guidance and Isolation
Campylobacter (symptoms include profuse diarrhoea, malaise, abdominal pain and sometimes vomiting).
Undercooked meat especially poultry.
Cross contamination from raw to cooked food.
Food contaminated by unwashed hands and contaminated utensils
Person to person spread
Isolate for 48 hours from the last episode of diarrhoea and/or vomiting This period maybe extended following advice from Infection Prevention and Control Team
Collect food history
Affected persons should not prepare or handle food for others until symptom free for at least 48 hours.
Report all cases to PHE
Eschericha coli (E.coli) gastroenteritis, causing diarrhoea and vomiting
Ingestion of contaminated food and/or water.
Faecal oral
Contaminated hands of infected cases.
Contaminated equipment
Isolate for 48 hours from the last episode of diarrhoea and/or vomiting.
Collect food history
Notify the local PHE
Listeria Ingestion of contaminated dairy products, meat based products, seafood and vegetable based products.
Person to person spread does not occur except during neonatal period
Notify the local PHE
Antibiotic therapy should be guided by a microbiologist
Salmonella (vomiting, diarrhoea and fever).
Ingestion of contaminated cooked food by raw food or inadequate cooking temperatures. Eggs, red and white meats, dairy products
Isolate for 48 hours from the last episode of diarrhoea and/or vomiting Food handlers should not return to work until cleared by Occupational Health Report to PHE
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
21
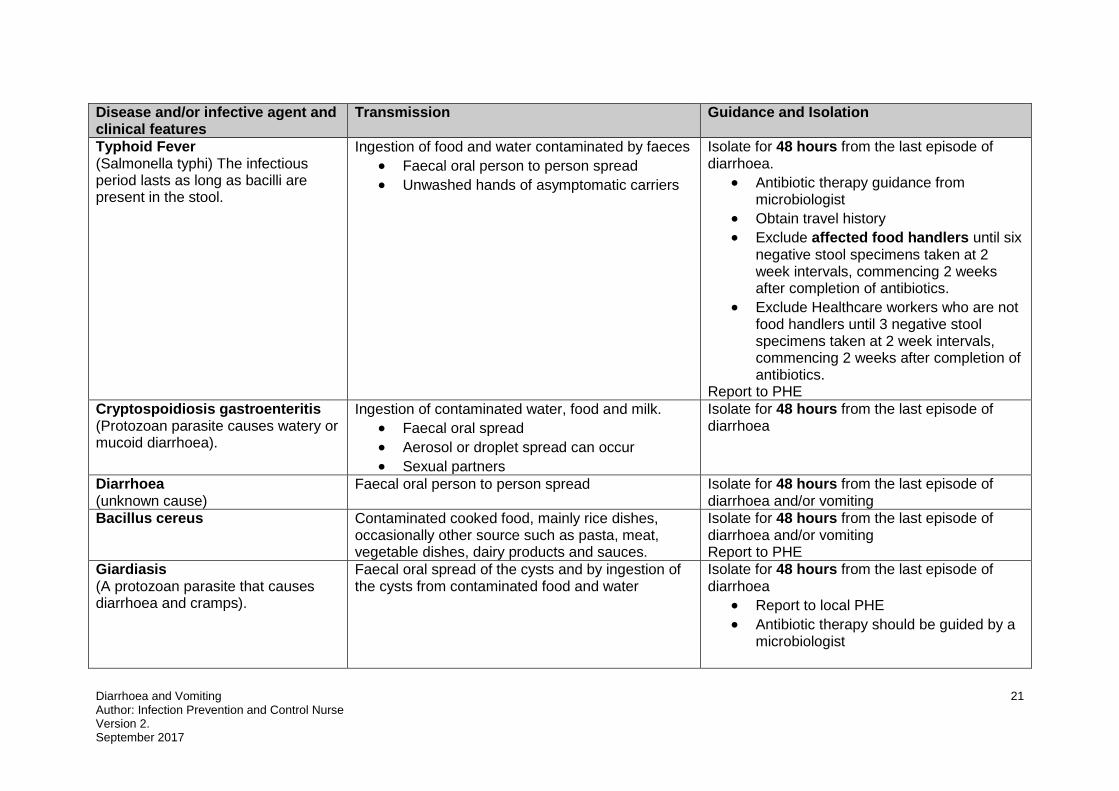
Disease and/or infective agent and clinical features
Transmission Guidance and Isolation
Typhoid Fever (Salmonella typhi) The infectious period lasts as long as bacilli are present in the stool.
Ingestion of food and water contaminated by faeces
Faecal oral person to person spread
Unwashed hands of asymptomatic carriers
Isolate for 48 hours from the last episode of diarrhoea.
Antibiotic therapy guidance from microbiologist
Obtain travel history
Exclude affected food handlers until six negative stool specimens taken at 2 week intervals, commencing 2 weeks after completion of antibiotics.
Exclude Healthcare workers who are not food handlers until 3 negative stool specimens taken at 2 week intervals, commencing 2 weeks after completion of antibiotics.
Report to PHE Cryptospoidiosis gastroenteritis (Protozoan parasite causes watery or mucoid diarrhoea).
Ingestion of contaminated water, food and milk.
Faecal oral spread
Aerosol or droplet spread can occur
Sexual partners
Isolate for 48 hours from the last episode of diarrhoea
Diarrhoea (unknown cause)
Faecal oral person to person spread Isolate for 48 hours from the last episode of diarrhoea and/or vomiting
Bacillus cereus Contaminated cooked food, mainly rice dishes, occasionally other source such as pasta, meat, vegetable dishes, dairy products and sauces.
Isolate for 48 hours from the last episode of diarrhoea and/or vomiting Report to PHE
Giardiasis (A protozoan parasite that causes diarrhoea and cramps).
Faecal oral spread of the cysts and by ingestion of the cysts from contaminated food and water
Isolate for 48 hours from the last episode of diarrhoea
Report to local PHE
Antibiotic therapy should be guided by a microbiologist
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
22
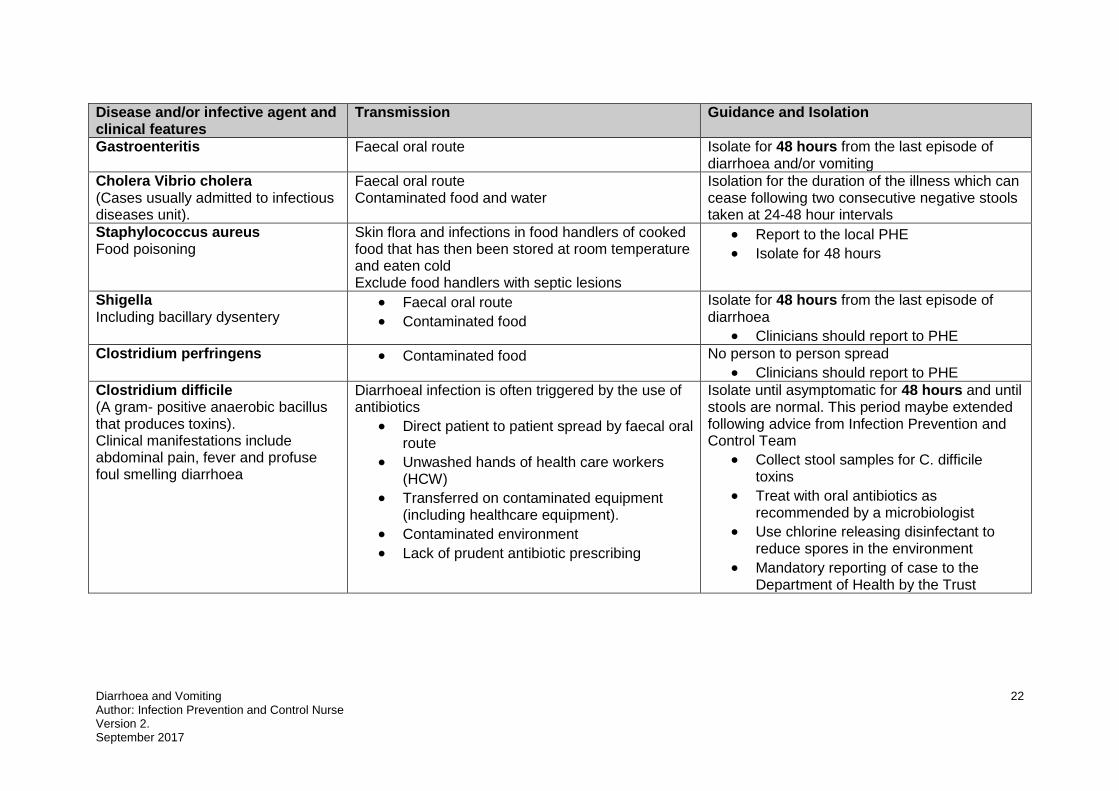
Disease and/or infective agent and clinical features
Transmission Guidance and Isolation
Gastroenteritis Faecal oral route Isolate for 48 hours from the last episode of diarrhoea and/or vomiting
Cholera Vibrio cholera (Cases usually admitted to infectious diseases unit).
Faecal oral route Contaminated food and water
Isolation for the duration of the illness which can cease following two consecutive negative stools taken at 24-48 hour intervals
Staphylococcus aureus Food poisoning
Skin flora and infections in food handlers of cooked food that has then been stored at room temperature and eaten cold Exclude food handlers with septic lesions
Report to the local PHE
Isolate for 48 hours
Shigella Including bacillary dysentery
Faecal oral route
Contaminated food
Isolate for 48 hours from the last episode of diarrhoea
Clinicians should report to PHE Clostridium perfringens Contaminated food No person to person spread
Clinicians should report to PHE Clostridium difficile (A gram- positive anaerobic bacillus that produces toxins). Clinical manifestations include abdominal pain, fever and profuse foul smelling diarrhoea
Diarrhoeal infection is often triggered by the use of antibiotics
Direct patient to patient spread by faecal oral route
Unwashed hands of health care workers (HCW)
Transferred on contaminated equipment (including healthcare equipment).
Contaminated environment
Lack of prudent antibiotic prescribing
Isolate until asymptomatic for 48 hours and until stools are normal. This period maybe extended following advice from Infection Prevention and Control Team
Collect stool samples for C. difficile toxins
Treat with oral antibiotics as recommended by a microbiologist
Use chlorine releasing disinfectant to reduce spores in the environment
Mandatory reporting of case to the Department of Health by the Trust
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
23
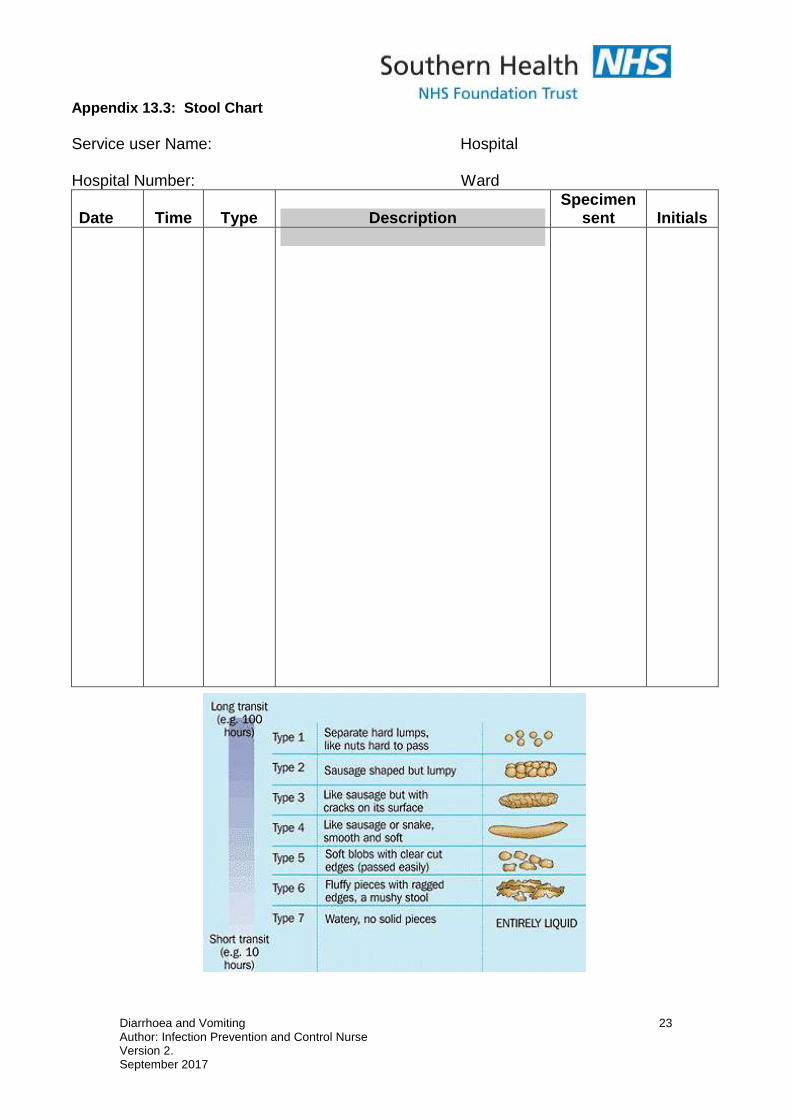
Appendix 13.3: Stool Chart
Service user Name: Hospital Hospital Number: Ward
Date
Time
Type
Description
Specimen sent
Initials
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
24
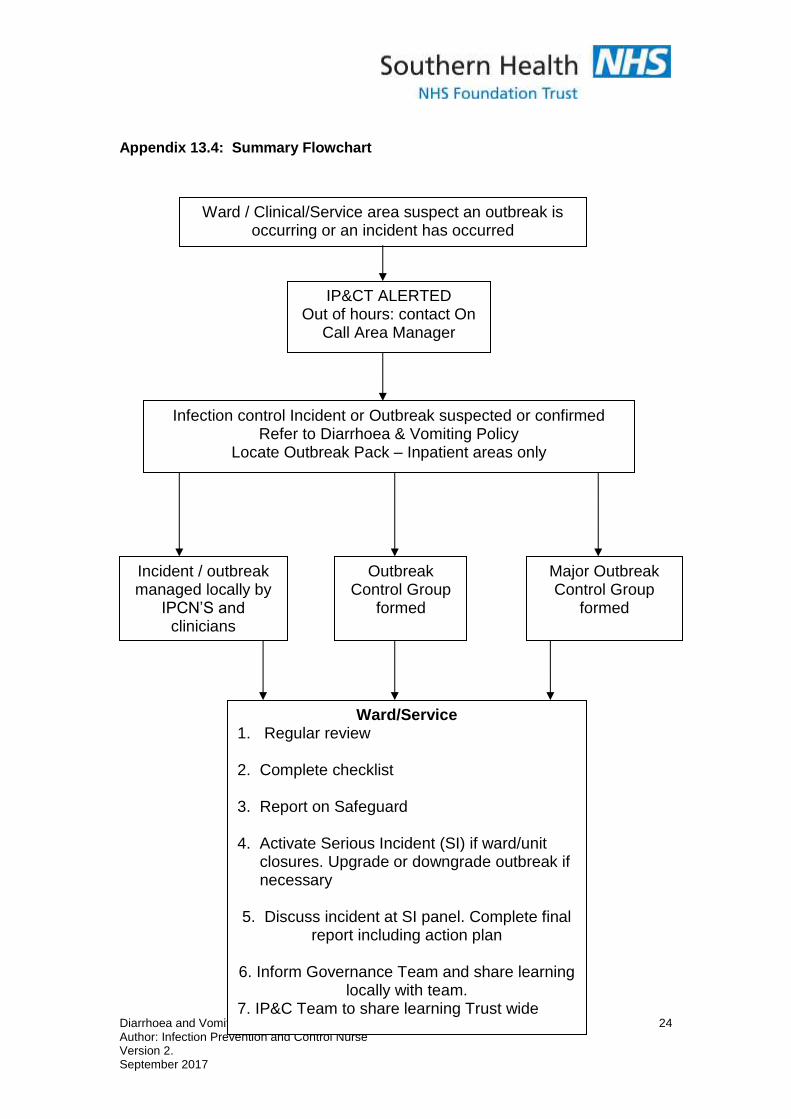
Appendix 13.4: Summary Flowchart
Ward / Clinical/Service area suspect an outbreak is occurring or an incident has occurred
IP&CT ALERTED Out of hours: contact On
Call Area Manager
Outbreak Control Group
formed
Infection control Incident or Outbreak suspected or confirmed Refer to Diarrhoea & Vomiting Policy
Locate Outbreak Pack – Inpatient areas only
Incident / outbreak managed locally by
IPCN’S and clinicians
Major Outbreak Control Group
formed
Ward/Service 1. Regular review
2. Complete checklist
3. Report on Safeguard
4. Activate Serious Incident (SI) if ward/unit closures. Upgrade or downgrade outbreak if necessary
5. Discuss incident at SI panel. Complete final
report including action plan
6. Inform Governance Team and share learning locally with team.
7. IP&C Team to share learning Trust wide .
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
25
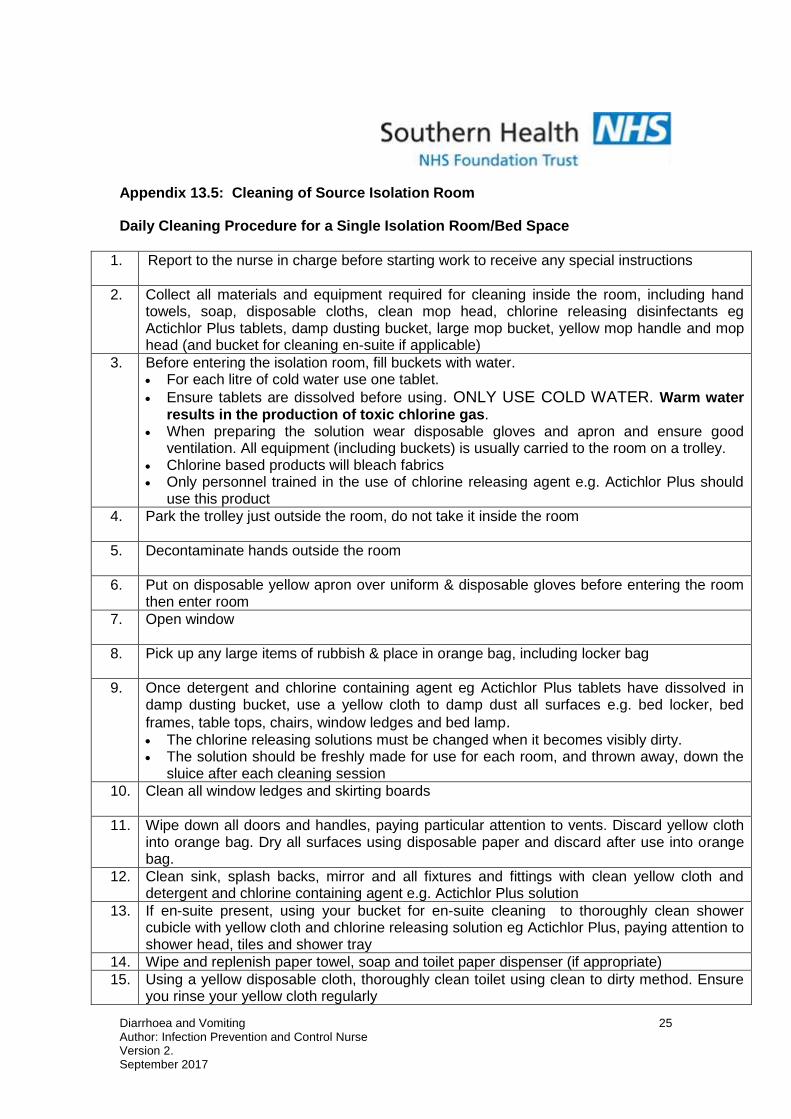
Appendix 13.5: Cleaning of Source Isolation Room
Daily Cleaning Procedure for a Single Isolation Room/Bed Space
1. Report to the nurse in charge before starting work to receive any special instructions
2. Collect all materials and equipment required for cleaning inside the room, including hand towels, soap, disposable cloths, clean mop head, chlorine releasing disinfectants eg Actichlor Plus tablets, damp dusting bucket, large mop bucket, yellow mop handle and mop head (and bucket for cleaning en-suite if applicable)
3. Before entering the isolation room, fill buckets with water. For each litre of cold water use one tablet.
Ensure tablets are dissolved before using. ONLY USE COLD WATER. Warm water results in the production of toxic chlorine gas.
When preparing the solution wear disposable gloves and apron and ensure good ventilation. All equipment (including buckets) is usually carried to the room on a trolley.
Chlorine based products will bleach fabrics Only personnel trained in the use of chlorine releasing agent e.g. Actichlor Plus should
use this product
4. Park the trolley just outside the room, do not take it inside the room
5. Decontaminate hands outside the room
6. Put on disposable yellow apron over uniform & disposable gloves before entering the room then enter room
7. Open window
8. Pick up any large items of rubbish & place in orange bag, including locker bag
9. Once detergent and chlorine containing agent eg Actichlor Plus tablets have dissolved in damp dusting bucket, use a yellow cloth to damp dust all surfaces e.g. bed locker, bed
frames, table tops, chairs, window ledges and bed lamp. The chlorine releasing solutions must be changed when it becomes visibly dirty. The solution should be freshly made for use for each room, and thrown away, down the
sluice after each cleaning session
10. Clean all window ledges and skirting boards
11. Wipe down all doors and handles, paying particular attention to vents. Discard yellow cloth into orange bag. Dry all surfaces using disposable paper and discard after use into orange bag.
12. Clean sink, splash backs, mirror and all fixtures and fittings with clean yellow cloth and detergent and chlorine containing agent e.g. Actichlor Plus solution
13. If en-suite present, using your bucket for en-suite cleaning to thoroughly clean shower cubicle with yellow cloth and chlorine releasing solution eg Actichlor Plus, paying attention to shower head, tiles and shower tray
14. Wipe and replenish paper towel, soap and toilet paper dispenser (if appropriate) 15. Using a yellow disposable cloth, thoroughly clean toilet using clean to dirty method. Ensure
you rinse your yellow cloth regularly
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
26
16. Discard used cloths into orange waste bag. 17. Dry mop the floor working from the furthest point towards the door.
Alternatively an (exhaust filtered) vacuum cleaner can be used. Wipe the casing of the vacuum cleaner with a Clinell sanitising wipe, after vacuuming before moving to another room
18. If floor not carpeted wet mop the floor working from the furthest point towards the door. Display floor signs.
19. Leave room and shut door
20. Go directly (whilst still wearing your aprons and gloves) to the sluice area.
21. Empty floor buckets, damp dusting bucket and en-suite bucket in sluice /cleaning cupboard
sink (never use a hand washing sink or a sink in the isolation room)
22. Wash the bucket with detergent and water and rinse and dry the bucket whilst in the sluice/or if applicable decontaminate in a ward washer disinfector
23. Remove mop heads and send for laundry in a plastic bag
24. Store mop handle and buckets in the cleaning cupboard or isolation room
25. Remove disposable gloves and apron whilst still in the sluice and thoroughly wash hands using soap and water, in the hand washing sink
.
Appendix 13.6: Infectious Terminal Clean of Isolation room/bay
Microfibre cleaning method Site: …………………………….. Ward/Dept: ……………………………………. Room number/name: ………………………………………………………………. Date requested: …………………………… Time requested:…………………… Requested by: ………………………………………………………………………. Requirement to remove radiator covers prior to terminal cleaning Remove if:-
Ward closure due to infection (e.g. D&V, MRSA, FLU outbreak) Single case of Clostridium difficile and C.diff carrier case if advised by IPCT On request of IPCT as part of management of a resistant organism
Removal not required if:- Bay closures due to infection e.g. D&V Single case of resistant organism e.g. MRSA or ESBL
Actions Y N Signature
Radiator cleaning if covers removed:- Estates department to be contacted in advance of infectious terminal cleaning by the nurse in charge to remove radiator covers. Estates helpline telephone number: 0300 300 3636 (Mon - Fri 08:30 – 5pm) Arrange the date and time to coincide with terminal cleaning. Estates department to replace radiator covers when infectious terminal cleaning process completed.
Cleaning of radiators: Outside & Inside (if required) Facility staff to clean using a damp disposable cloth soaked in detergent and chlorine containing solution (e.g. Actichlor Plus).
Nursing staff Responsibility (ideally nursing tasks to be completed prior to housekeeping tasks)
Actions Y N Signature
The patient must have vacated the bed space before cleaning commences.
Wash hands before entering the isolation area.
Put on single use gloves and yellow apron before entering the isolation area.
Ensure good ventilation.
The room or area should be cleared of miscellaneous items (e.g. discard magazines, used toiletries into an orange hazardous waste bag).
Remove all linen from bed and place in an alginate bag, followed by infectious outer laundry bag, and tie securely.
All disposable fittings and single use medical devices should be disposed of into an orange hazardous waste bag, e.g. oxygen tubing, suction tubing & suction drainage bags.
All reusable medical equipment must be decontaminated according to manufacturer’s instructions. Following decontamination, remove the equipment from the area.
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
28
Cleaning: Use a detergent and chlorine containing solution eg Actichlor Plus, 1000ppm. Ensure tablets are dissolved before using. Always ensure good ventilation and correct personal protective clothing is worn when handling the chlorine releasing solution. (Refer to Actichlor Plus dilution poster for the general environment and for cleaning up any blood spillage).
Actichlor Plus BS Solution Only Southern Health NHS V1.pdf
Actichlor Plus GE Southern Health NHS V1.pdf
If commode or raised toilet seat present, thoroughly clean all areas with a detergent and chlorine solution, rinse and then dry.
Thoroughly wipe the mattress, upper bed frame, bed head, bed rails, and plastic pillow cover with detergent and chlorine solution eg Actichlor Plus and dry with disposable paper towels. Discard paper towels into orange hazardous waste bag. Ensure good ventilation whilst cleaning within the room.
Clean the patient wash bowl if non-disposable with detergent and chlorine solution e.g. Actichlor Plus and dry with disposable paper towels. If bedside entertainment system present, remove headset earpiece covers and discard into orange hazardous waste bag. Arrange for cleaning and replacement earpieces.
Name of nurse (print): Date completed: Time:
Signature:
Housekeeping Staff Responsibility (Ideally nursing tasks should be completed prior to housekeeping tasks)
Housekeeping Team to use detergent and chlorine containing agent eg Actichlor Plus 1000ppm for all cleaning tasks during this procedure.
Actions Y N Signature
Before starting: report to clinical staff to receive any specific instructions.
Make up Chlorine based disinfectant solution: In the cleaning room, prepare all equipment needed.
Wearing gloves and aprons make up a chlorine solution by adding one tablet of Chlorine releasing agent e.g. Actichlor Plus to one litre of cold water.
When the tablet has fully dissolved, dose cloths and mops as per microfibre set up on trolley in yellow buckets.
NB: Only personnel trained in use of Chlorine releasing agent e.g. Actichlor Plus, should use this product.
Collect all materials and equipment: e.g. hand towels, toilet rolls, soap, pre-dosed yellow microfibre cloths or disposables & pre-dosed yellow microfibre mops, high dusting tool.
Park cleaning trolley outside: Within reach of the door. Do not take the trolley inside the room.
Clean hands before entering the isolation area.
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
29
PPE: Put on single use gloves and yellow apron before entering the isolation area (discuss with nursing staff if any additional PPE is required).
Ensure good ventilation e.g. open a window
Remove dirty curtains: Place into an alginate bag, then outer infectious linen stream bag.
Damp dust: Using the pre-dosed yellow micro fibre 8 sided cloth technique. Clean all horizontal surfaces from:- High to low Clean to dirty Top to bottom Far end of room to the door
Damp dust: Using the pre-dosed yellow micro fibre 8 sided cloth technique.
High Dust - Damp dust all areas to hand height level regularly rinsing cloth, allow to air dry.
Bedside Lamp - Extend the lamp, damp dust all areas, return to original position, allow to air dry.
Hand held ‘nurse call’ device, careful to clean around idented button, allow to air dry.
Bedside Locker - Thoroughly clean all areas inside and outside, and allow to air dry.
Bedside Table - Thoroughly clean all areas of table top, underside & stand, allow to air dry.
Bedside Chair - Thoroughly clean all wipeable areas of chair seat, back, top, underside and legs, allow to air dry.
Bed Frame (below top frame) - Raise bed and thoroughly clean all areas of underside and stand areas working from the top to the bottom, allow to air dry.
Window Ledges - Damp dust all areas, and allow to air dry.
All Doors, Door Handles & Door Vents - Thoroughly clean all areas paying attention to hand contact surfaces, allow to air dry.
Skirting Boards - Damp dust all areas, allow to air dry.
Clinical Hand Wash Sink, Taps & Splash Back Use two cloths one for taps and dispensers the other for the Basin.
Taps should be cleaned first before the rest of the CHWB (ref HTM 04:01 2016).
Tiles -Thoroughly clean the area working from the outside inwards, Allow to air dry.
Mirrors - Thoroughly clean the area then dry and buff with a second cloth/disposable paper towel to remove any smears.
Bathroom facilities/ En Suite: Using a fresh cloth, clean the basin and shower cubicle paying attention to taps, shower heads, tiles and shower tray. For any wash hand basins: Use two cloths one for taps and dispensers the other for the basin Taps should be cleaned first before the rest of the CHWB (ref HTM 04:01 2016) Clean the areas working from the outside inwards, allow to air dry. Shower Cubicle, Shower Tray & Wall Tiles/Cladding (if present) - Thoroughly clean the area working from shower head/hose/controls
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
30
outwards to the tiles and tray, allow to air dry.
Hand Towel, soap & Toilet Roll Dispensers - Damp dust all areas, allow to air dry. Replacement Consumables - Replenish hand soap, toilet roll, paper hand towels and opened packets of Clinell wipes. (No need to replace hand towels or toilet rolls that are in an enclosed dispenser, just clean/wipe over the external container). Throw away toilet brushes.
Toilet & Toilet Seat - Flush then apply descaler if required. Using a fresh yellow microfibre cloth thoroughly clean all areas with a chlorine releasing solution eg Actichlor plus, working from the highest point to the lowest and from the outside inwards (clean to dirty method), scrub toilet bowl and finish with toilet seat and a final flush.
Damp dust: Using the pre-dosed yellow micro fibre 8 sided cloth technique. Floors Hard floors: Damp mop (using yellow mop heads or disposable), working from the furthest point to the door. Display floor signs. Soft floors: Vacuum debris using an exhaust filtered vacuum cleaner then carpeted floors’/ any rugs to be steam cleaned.
Soft furnishings e.g. chairs or sofas: Steam clean any non wipeable surfaces within the room.
Discard all disposable cleaning cloths / mop heads into the orange bag for infectious waste. Ensure used microfibre cloths and mop heads have been placed into linen bags directly on the cleaning trolley ready for laundry.
Waste Bin/Bags – Pick up any items of rubbish e.g. locker bag, discard in orange waste bag. Remove Orange healthcare waste bags, and clean the bin.
Replace waste bags as appropriate in the lidded bins for the next patient.
Before leaving the room: Remove PPE and discard into orange waste bag. Swan neck tie and secure orange bag with ward identification tape. Thoroughly clean hands with soap and water Close door as you leave the room.
Outside of room:
Clean hands with alcohol sanitizer
Store mop handle and buckets in the cleaning cupboard
Place microfibre laundry bags into dedicated washing machine, on hot wash
Take orange waste bag to storage area
Replace curtains with clean ones, if no available curtains please discuss steam cleaning with the IPCT before the infectious terminal clean commences. Blinds - Clean /Steam / Actichlor blinds as appropriate.
Comments from housekeeping staff
Comments from nursing staff
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
31
On completion of the Terminal Clean please sign the box below confirming that you are satisfied with the standard of cleanliness.
Ward Manager/shift leader Name: (print) Date completed: Time:
Housekeeping supervisor Name: (print) Date completed: Time:
Signature:
Signature:
Retain copies of this form:- 1. The person requesting final isolation clean must ensure that a copy is to be retained on the ward 2. One copy to be retained by Housekeeping
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
32
Appendix 13.6: Infectious Terminal Clean of Isolation room/bay
Mop and Bucket cleaning method Site: …………………………….. Ward/Dept: ……………………………………. Room number/name: ………………………………………………………………. Date requested: …………………………… Time requested:…………………… Requested by: ………………………………………………………………………. Requirement to remove radiator covers prior to terminal cleaning Remove if:-
Ward closure due to infection (e.g. D&V, MRSA, FLU outbreak) Single case of Clostridium difficile and C. diff carrier case if advised by IPCT On request of IPCT as part of management of a resistant organism
Removal not required if:-
Bay closures due to infection e.g. D&V Single case of resistant organism e.g. MRSA or ESBL
Actions Y N Signature
Radiator cleaning if covers removed:- Estates department to be contacted in advance of infectious terminal cleaning by the nurse in charge to remove radiator covers. Estates helpline telephone number: 0300 300 3636 (Mon - Fri 08:30 – 5pm) Arrange the date and time to coincide with terminal cleaning. Estates department to replace radiator covers when infectious terminal cleaning process completed.
Cleaning of radiators: Outside and inside (if required) Facility staff to clean using a damp disposable cloth soaked in detergent and chlorine containing solution (e.g. Actichlor Plus).
Nursing staff Responsibility (ideally nursing tasks to be completed prior to housekeeping tasks)
Actions Y N Signature
The patient must have vacated the bed space before cleaning commences.
Wash hands before entering the isolation area.
Put on single use gloves and yellow apron before entering the isolation area.
Ensure good ventilation e.g. open a window
The room or area should be cleared of miscellaneous items (e.g. discard magazines, used toiletries into an orange hazardous waste bag).
Remove all linen from bed and place in an alginate bag, followed by infectious outer laundry bag, and tie securely.
All disposable fittings and single use medical devices must be disposed of into an orange hazardous waste bag, e.g. oxygen tubing, suction tubing & suction drainage bags.
All reusable medical equipment must be decontaminated according to manufacturer’s instructions. Following decontamination, remove the equipment from the area.
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
33
Actions Y N Signature
Cleaning: Use a detergent and chlorine containing solution eg Actichlor Plus 1000ppm, Ensure tablets are dissolved before using. Always ensure good ventilation and correct personal protective clothing is worn when handling the chlorine releasing solution. (Refer to Actichlor Plus dilution poster for the general environment and for cleaning up any blood spillage).
Actichlor Plus BS Solution Only Southern Health NHS V1.pdf
Actichlor Plus GE Southern Health NHS V1.pdf
If commode or raised toilet seat present, thoroughly clean all areas with a detergent and chlorine solution, rinse and then dry.
Thoroughly wipe the mattress, upper bed frame, bed head, bed rails, and plastic pillow cover with detergent and chlorine solution eg Actichlor Plus and dry with disposable paper towels. Discard paper towels into orange hazardous waste bag. Ensure good ventilation whilst cleaning within the room.
Clean the patient wash bowl if non-disposable with detergent and chlorine solution e.g. Actichlor Plus and dry with disposable paper towels. If bedside entertainment system present, remove headset earpiece covers and discard into orange hazardous waste bag. Arrange for cleaning and replacement earpieces.
Name of nurse (print): Date completed: Time:
Signature:
Housekeeping Staff Responsibility (ideally nursing tasks should be completed prior to housekeeping tasks)
Housekeeping Team to use detergent and chlorine containing agent eg Actichlor Plus 1000ppm for all cleaning tasks during this procedure. Ensure tablets are dissolved before using. Always ensure good ventilation and correct personal protective clothing is worn when handling the chlorine releasing solution. (Refer to Actichlor Plus dilution poster for the general environment and for cleaning up any blood spillage).
Actions Y N Signature
Prepare all equipment needed. Park cleaning trolley outside infection room/bay.
Wash hands before entering the isolation area.
Put on single use gloves and yellow apron before entering the isolation area (discuss with nursing staff if any additional PPE is required).
Ensure good ventilation.
Whilst the chlorine containing tablets are dissolving, remove dirty curtains, place into alginate then outer infectious laundry bag.
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
34
Actions Y N Signature
Use a detergent and chlorine containing solution eg Actichlor Plus, clean the following using a yellow disposable cloth and damp dusting bucket:
High Dust - Damp dust all areas to hand height level regularly rinsing cloth, allow to air dry.
Bedside Lamp - Extend the lamp, damp dust all areas, return to original position, allow to air dry.
Hand held ‘nurse call’ device, be careful to clean around idented button.
Bedside Locker - Thoroughly clean all areas inside and outside, and allow to air dry.
Bedside Table - Thoroughly clean all areas of table top, underside and stand area regularly rinsing cloth, allow to air dry.
Bedside Chair - Thoroughly clean all wipeable areas of chair seat, back top, underside and legs, allow to air dry.
Bed Frame (below top frame) - Raise bed and thoroughly clean all areas of underside and stand areas working from the top to the bottom, regularly rinsing cloth, allow to air dry.
Window Ledges - Damp dust all areas, and allow to air dry.
All Doors, Door Handles & Door Vents - Thoroughly clean all areas paying attention to hand contact surfaces, regularly rinsing cloth, allow to air dry.
Skirting Boards - Damp dust all areas, allow to air dry.
Clinical Hand Wash Sink, Taps & Splash Back Use two cloths one for taps and dispensers the other for the basin. Taps should be cleaned first before the rest of the CHWB
(ref HTM 04:01 2016)
Tiles -Thoroughly clean the area working from the outside inwards, allow to air dry.
Mirrors - Thoroughly clean the area then dry and buff with a second cloth/disposable paper towel to remove any smears.
Bathroom facilities/ En Suite, use detergent and chlorine releasing solution contained in the ‘Ensuite Cleaning Bucket’ and disposable yellow cloths and clean taps & splash back tiles thoroughly. Clean the area working from the outside inwards, regularly rinsing cloth, allow to air dry.
For any wash hand basins: Use two cloths one for taps and dispensers the other for the basin. Clean the areas working from the outside inwards, allow to air dry.
Taps should be cleaned first before the rest of the CHWB (ref HTM 04:01 2016)
Shower Cubicle, Shower Tray & Wall Tiles/Cladding (if present) - Thoroughly clean the area working from shower head/hose/controls outwards to the tiles and tray, allow to air dry.
Hand Towel & Toilet Roll Dispensers:
Damp dust all areas, allow to air dry. (No need to replace hand towels or towel rolls that are in an enclosed dispenser, just clean/wipe over the external container).
Throw away toilet brushes into infectious waste stream bag.
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
35
Actions Y N Signature
Toilet & Toilet Seat - Flush then apply descaler if required, thoroughly clean all areas using a yellow cloth and chlorine releasing solution eg Actichlor plus, working from the highest point to the lowest and from the outside inwards, scrub toilet bowl and finish with toilet seat and a final flush.
Floors – Remove debris using an exhaust filtered vacuum cleaner OR dry mop. Follow this with, wet mopping using a yellow handled mop and chlorine releasing agent eg Actichlor plus from the yellow mop bucket (dispose/launder mop heads after use). If areas are carpeted, steam clean carpet and launder any rugs.
Soft furnishings e.g. chairs or sofas: Steam clean any non wipeable surfaces within the room.
Waste: Discard all disposable cleaning cloths in the orange bag for infectious waste. Pick up any items of rubbish e.g. locker bags, discard into orange waste bag Remove orange waste bag to clean the bin. Replace waste bags as appropriate in the lidded bin for the next patient.
Replacement Consumables - Replenish hand soap, toilet roll, hand towels and opened packets of Clinell wipes. (No need to replace hand towels or toilet rolls that are in an enclosed dispenser, just clean/wipe over the external container). Throw away toilet brushes.
Before leaving the room: Remove PPE and discard into the orange waste bag. Swan neck tie and secure with ward identification tag / tape. Thoroughly clean hands with soap and water. Close door as you leave the room.
Outside the room: Clean hands with alcohol sanitiser Store cleaned and dry cleaning trolley, mop handle and bucket in the cleaning cupboard. Take orange bag waste to storage area.
Replace curtains with clean ones, if no available curtains please discuss steam cleaning with the IPCT before the Infectious terminal cleaning process.. Blinds – Clean / Steam / Actichlor blinds as appropriate.
Comments from housekeeping staff
Comments from nursing staff
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
36
On completion of the Terminal Clean please sign the box below confirming that you are satisfied with the standard of cleanliness.
Ward Manager/shift leader Name: (print) Date completed: Time:
Housekeeping supervisor Name: (print) Date completed: Time:
Signature:
Signature:
Retain copies of this form:- 1. The person requesting final isolation clean must ensure that a copy is to be retained on the ward 2. One copy to be retained by Housekeeping
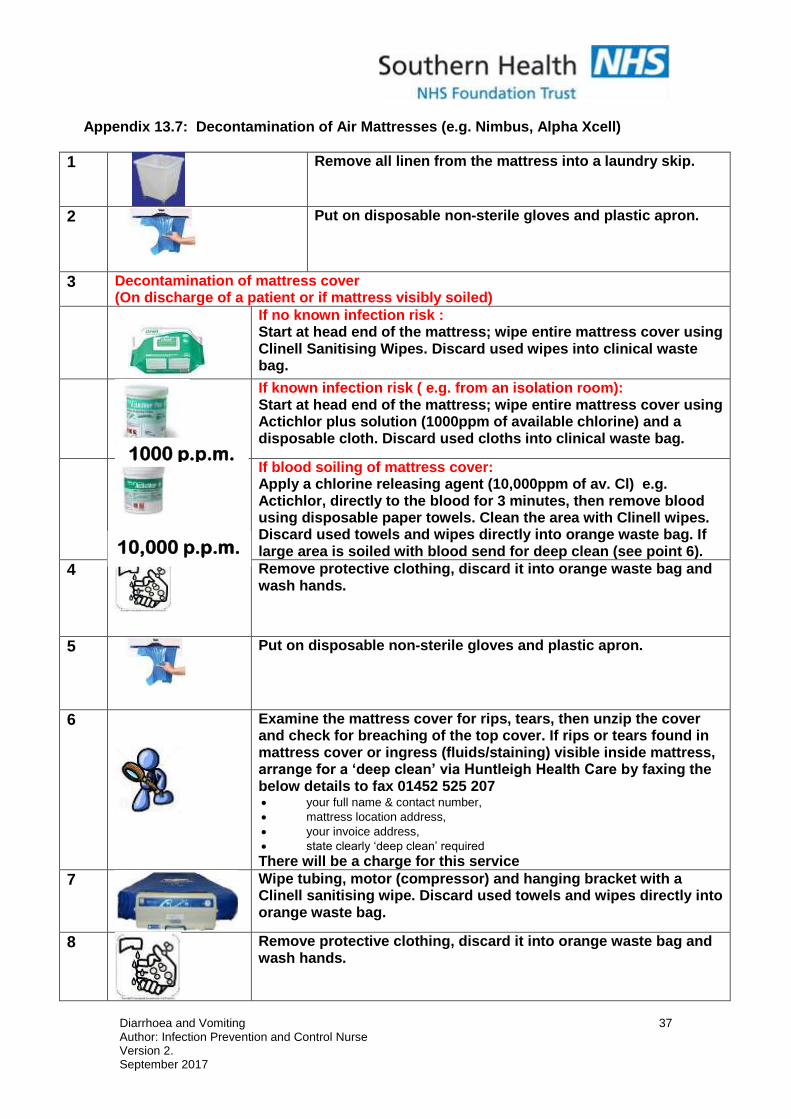
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
37
Appendix 13.7: Decontamination of Air Mattresses (e.g. Nimbus, Alpha Xcell)
1
Remove all linen from the mattress into a laundry skip.
2
Put on disposable non-sterile gloves and plastic apron.
3 Decontamination of mattress cover (On discharge of a patient or if mattress visibly soiled)
If no known infection risk : Start at head end of the mattress; wipe entire mattress cover using Clinell Sanitising Wipes. Discard used wipes into clinical waste bag.
If known infection risk ( e.g. from an isolation room): Start at head end of the mattress; wipe entire mattress cover using Actichlor plus solution (1000ppm of available chlorine) and a disposable cloth. Discard used cloths into clinical waste bag.
If blood soiling of mattress cover: Apply a chlorine releasing agent (10,000ppm of av. Cl) e.g. Actichlor, directly to the blood for 3 minutes, then remove blood using disposable paper towels. Clean the area with Clinell wipes. Discard used towels and wipes directly into orange waste bag. If large area is soiled with blood send for deep clean (see point 6).
4
Remove protective clothing, discard it into orange waste bag and wash hands.
5
Put on disposable non-sterile gloves and plastic apron.
6
Examine the mattress cover for rips, tears, then unzip the cover and check for breaching of the top cover. If rips or tears found in mattress cover or ingress (fluids/staining) visible inside mattress, arrange for a ‘deep clean’ via Huntleigh Health Care by faxing the below details to fax 01452 525 207 your full name & contact number,
mattress location address,
your invoice address,
state clearly ‘deep clean’ required There will be a charge for this service
7
Wipe tubing, motor (compressor) and hanging bracket with a Clinell sanitising wipe. Discard used towels and wipes directly into orange waste bag.
8
Remove protective clothing, discard it into orange waste bag and wash hands.
1000 p.p.m.
10,000 p.p.m.
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
38
Appendix 13.8: Clostridium difficile fact sheet – information for patients, visitors and relatives
Clostridium difficile fact sheet:
Information for patients, visitors and relatives.
What is Clostridium difficile (C. diff)? A germ (bacteria),which is present in the gut of approx 3% of healthy adults. It is more common in babies/infants, but rarely causes problems. People over the age of 65 are more susceptible to contracting infection. How do you catch it? It is possible for this infection to spread from person to person because C. diff spores are shed in the faeces they can survive for long periods of time in the environment (bedpans, toilets, surfaces etc.) and can be transported on hands and contaminated equipment. Clostridium difficile may be acquired by transferring the bacteria from contaminated hands or equipment to the mouth (faecal oral spread). In most healthy people the C. diff will not cause disease, however more vulnerable people particularly those whose normal gut bacteria have been disrupted by antibiotic treatment, may go on to develop C. diff infection. What are the symptoms? The effects of C. diff can vary from no symptoms to diarrhoea (mild to severe) and more unusually severe inflammation of the intestines which can cause death. Other symptoms can include fever, loss of appetite, nausea and abdominal pain or tenderness. You should report any diarrhoea and or vomiting to health care staff immediately. Who does this affect? Are some people more at risk?
Advanced age, 80% of cases reported are in the over 65 age group. Those with a lowered immunity Those patients with underlying medical conditions Patients who have had long length of stay in healthcare settings Antibiotic treatment Repeated enemas and or gut surgery increases a person’s risk.
How is Clostridium difficile diagnosed? Initial diagnosis can be on the symptoms and patient history (e.g. previously taken a course of antibiotics). Followed up with carrying out laboratory testing of a faecal
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
39
specimen which shows the presence of the C. diff toxins, (poisons produced by the bacteria). How can it be treated? In most patients the C. diff can be treated with specific antibiotics. There is a relapse rate of 20 – 30% of patients; other treatments may be tried with the aim of re-establishing the balance of flora in the gut. Most cases make a full recovery. More complex cases, associated with other underlying medical conditions may have a more severe infection. Occasionally, infection in these circumstances may be life threatening. If I have Clostridium difficicle, what should I do to prevent the spread to others? In order to reduce the chance of spreading the infection to others it is advisable to wash hands with soap and water, especially after using the toilet/commode and before eating. Keep surfaces in bathrooms clean, using a household disinfectant e.g. bleach type agent, (bleach can dis-colour/damage certain fabrics – use with caution) Encourage your visitors to wash their hands before they leave. How can hospitals prevent the spread of Clostridium difficile? Ensure antibiotics are used only when really necessary. Clinical staff will identify patients in the early stages of this disease and introduce enhanced infection control measures such as;-
Isolation in a single room with en-suite or dedicated toilet/commode, which helps to limit the spread of infection.
Clinical staff will wear disposable gloves and aprons when caring for infected patients
Performing hand hygiene using soap and water prior to and after contact with the patient who has the infection.
Clostridium difficile contamination should be removed from the environment by daily thorough cleaning using a chlorine based cleaning agent.
Visitors will be asked to wear disposable aprons and gloves if participating in the care of their relatives.
Additional infection control measures may be introduced for staff, patients and relatives if an outbreak (2 or more patients) with Clostridium difficile infection is suspected. Does somebody who has had a Clostridium difficile infection pose a risk to others after they have been discharged? There should be no restriction on the discharge or transfer of patients’ to other healthcare facilities when recovered from C. diff diarrhoea. Once recovered there is no clinical risk to others even though they continue to carry the organism in their gut provided they observe normal personal hygiene precautions e.g. hand washing with soap and water after using the toilet.
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
40
Appendix 13.9: Gastroenteritis caused by Norovirus and other viruses factsheet
Gastroenteritis caused by Norovirus and other viruses factsheet.
Information for patients, visitors and relatives.
What is viral gastroenteritis? An infection of the gut (intestines) which usually causes vomiting and/or diarrhoea. It is most commonly caused by Norovirus, other small round structured viruses or Rotavirus. What is Norovirus? The most common cause of gastroenteritis (stomach bugs) also called “winter vomiting virus or Norwalk-like virus. It is estimated that Norovirus affects between 600 thousand and a million people in the UK each year, most of these are people in their own homes. This virus is responsible for causing outbreaks of gastroenteritis in institutions like hospitals, residential/nursing homes, schools and cruise ships. How is viral gastroenteritis including Norovirus caught? Viral gastroenteritis is easily transmitted from one person to another.
By contact with an infected person. By contact with surfaces or objects that have been contaminated with viral
particles. By swallowing the virus dispersed in the air after someone has had projectile
vomiting. By consuming food or water contaminated with viral particles Also rarely from raw or undercooked food, particularly shell fish, as this may
be contaminated with raw sewage. Who is at risk of getting Norovirus or other viral gastroenteritis? It affects people of all ages. The very young and elderly should take extra care if infected, as dehydration is more common in these age groups. Outbreaks usually affect people who are in semi-closed environments, or where large numbers of people congregate for several days, providing an ideal environment for the spread of the disease. What are the symptoms? The following symptoms will usually begin around 12 – 48 hours after becoming infected with gastroenteritis/Norovirus:-
Sudden onset of nausea followed by vomiting – which may be projectile.
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
41
Watery diarrhoea. Stomach pains/cramps. Some people may have a raised temperature, headache and aching limbs.
Symptoms may last 12 – 48 hours. Most people will make a full recovery within 2 days. The very young, elderly or people with a weakened immune system may become dehydrated and require hospital treatment. If unwell at home and in doubt about the cause of symptoms, contact your GP. Why does Norovirus often cause outbreaks? It is easily spread from one person to another and the virus is able to survive in the environment for many days, more than 50% of people who are exposed to Norovirus will be affected. There are many different strains and once infected immunity is short-lived. How can these outbreaks be controlled? Outbreaks can be difficult to control. The most effective way to control an outbreak is to isolate/nurse together patients who have become infected usually isolation lasts for 48 hours after symptoms have ceased. Close the ward to new admissions who may be susceptible. Enhance cleaning regimes using a bleach type agent to remove the viruses from surfaces/objects. Please NB. Bleach will discolour/damage certain fabrics – use with caution. Institute good hygiene measures including hand washing using soap and water. Provide advice on food handling. Affected staff, relatives or visitors should not work/visit until they have been free from symptoms for 48 hours. How is Norovirus and other viral gastroenteritis treated? There is no specific treatment, apart from letting the illness run its course. It is important to drink plenty of fluids to prevent dehydration. This is particularly important for young children and the elderly. If I am suffering from Norovirus or other viral gastroenteritis, how can I prevent others from becoming infected? Good hygiene is important in preventing others from becoming infected – this includes thorough hand washing with soap and water before and after contact with others and after using the toilet. Soap and water is more effective against the viruses than alcohol gel, when cleaning your hands. Food preparation should be avoided until 48 hours after symptoms have gone altogether. You should report any diarrhoea and /or vomiting to staff immediately if you are in hospital.
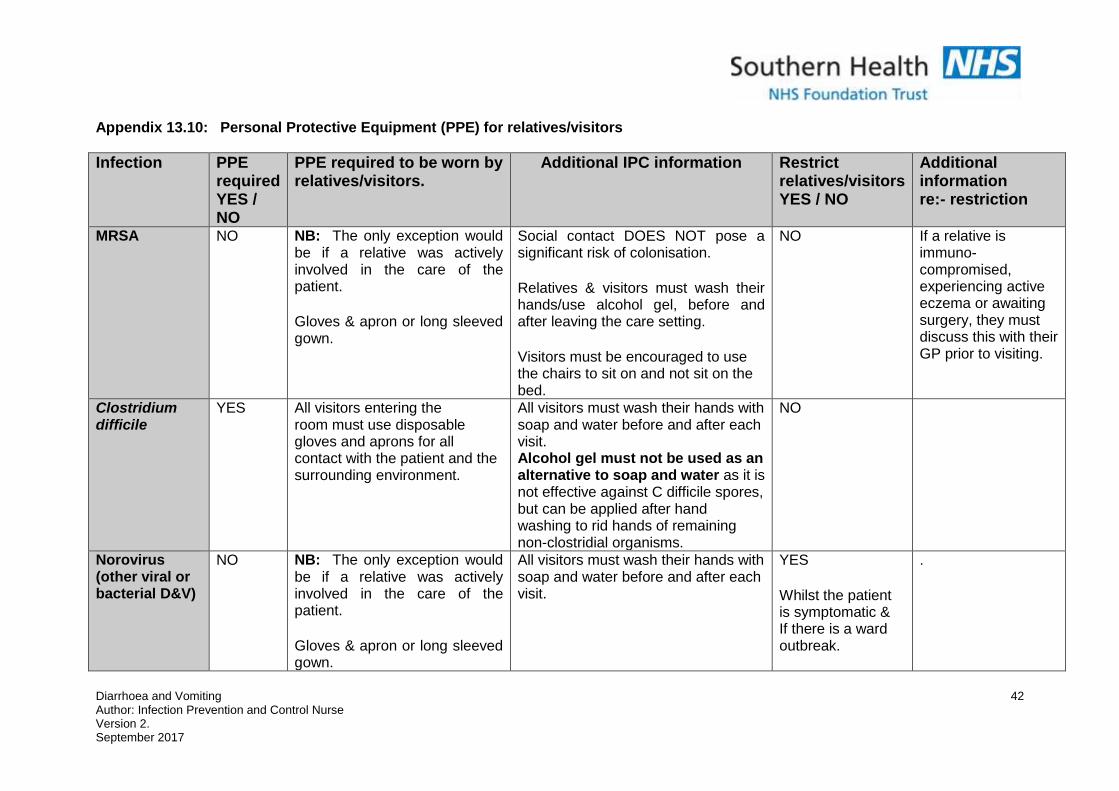
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
42
Appendix 13.10: Personal Protective Equipment (PPE) for relatives/visitors
Infection
PPE required YES / NO
PPE required to be worn by relatives/visitors.
Additional IPC information Restrict relatives/visitors YES / NO
Additional information re:- restriction
MRSA
NO
NB: The only exception would be if a relative was actively involved in the care of the patient. Gloves & apron or long sleeved gown.
Social contact DOES NOT pose a significant risk of colonisation. Relatives & visitors must wash their hands/use alcohol gel, before and after leaving the care setting. Visitors must be encouraged to use the chairs to sit on and not sit on the bed.
NO If a relative is immuno-compromised, experiencing active eczema or awaiting surgery, they must discuss this with their GP prior to visiting.
Clostridium difficile
YES All visitors entering the room must use disposable gloves and aprons for all contact with the patient and the surrounding environment.
All visitors must wash their hands with soap and water before and after each visit. Alcohol gel must not be used as an alternative to soap and water as it is not effective against C difficile spores, but can be applied after hand washing to rid hands of remaining non-clostridial organisms.
NO
Norovirus (other viral or bacterial D&V)
NO
NB: The only exception would be if a relative was actively involved in the care of the patient. Gloves & apron or long sleeved gown.
All visitors must wash their hands with soap and water before and after each visit.
YES Whilst the patient is symptomatic & If there is a ward outbreak.
.
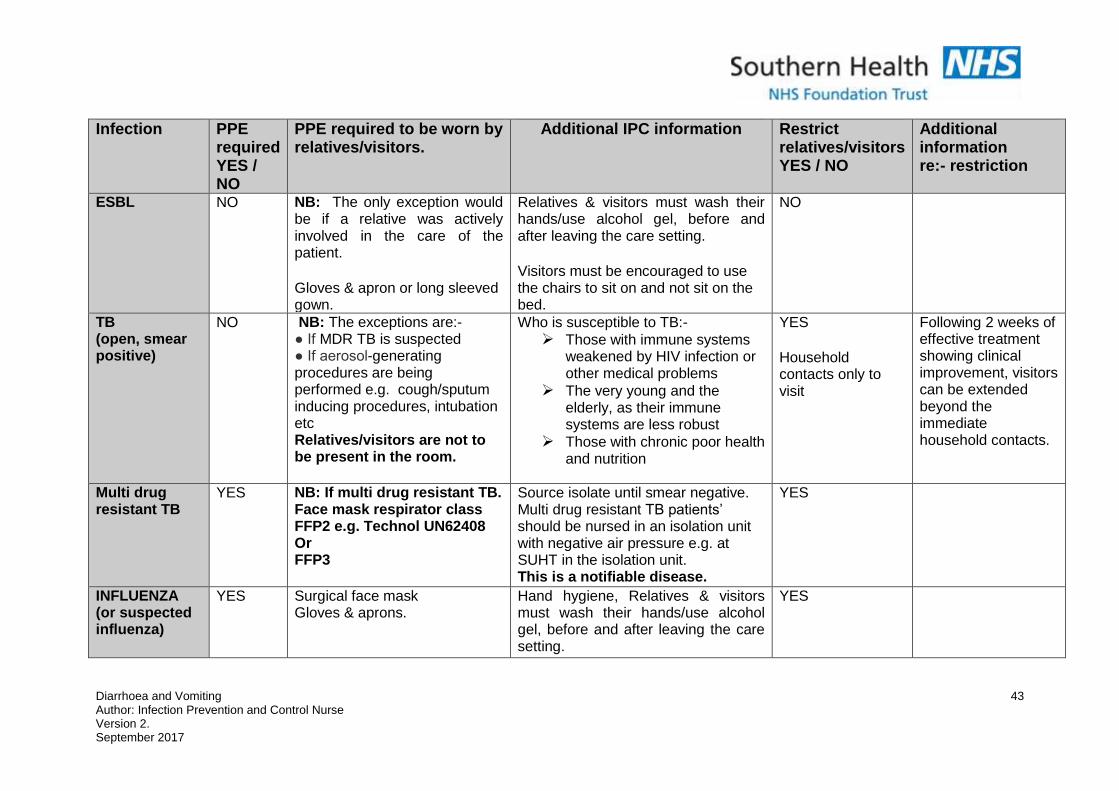
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
43
Infection
PPE required YES / NO
PPE required to be worn by relatives/visitors.
Additional IPC information Restrict relatives/visitors YES / NO
Additional information re:- restriction
ESBL
NO NB: The only exception would be if a relative was actively involved in the care of the patient. Gloves & apron or long sleeved gown.
Relatives & visitors must wash their hands/use alcohol gel, before and after leaving the care setting. Visitors must be encouraged to use the chairs to sit on and not sit on the bed.
NO
TB (open, smear positive)
NO NB: The exceptions are:- ● If MDR TB is suspected ● If aerosol-generating procedures are being performed e.g. cough/sputum inducing procedures, intubation etc Relatives/visitors are not to be present in the room.
Who is susceptible to TB:- Those with immune systems
weakened by HIV infection or other medical problems
The very young and the elderly, as their immune systems are less robust
Those with chronic poor health and nutrition
YES Household contacts only to visit
Following 2 weeks of effective treatment showing clinical improvement, visitors can be extended beyond the immediate household contacts.
Multi drug resistant TB
YES NB: If multi drug resistant TB. Face mask respirator class FFP2 e.g. Technol UN62408 Or FFP3
Source isolate until smear negative. Multi drug resistant TB patients’ should be nursed in an isolation unit with negative air pressure e.g. at SUHT in the isolation unit. This is a notifiable disease.
YES
INFLUENZA (or suspected influenza)
YES Surgical face mask Gloves & aprons.
Hand hygiene, Relatives & visitors must wash their hands/use alcohol gel, before and after leaving the care setting.
YES
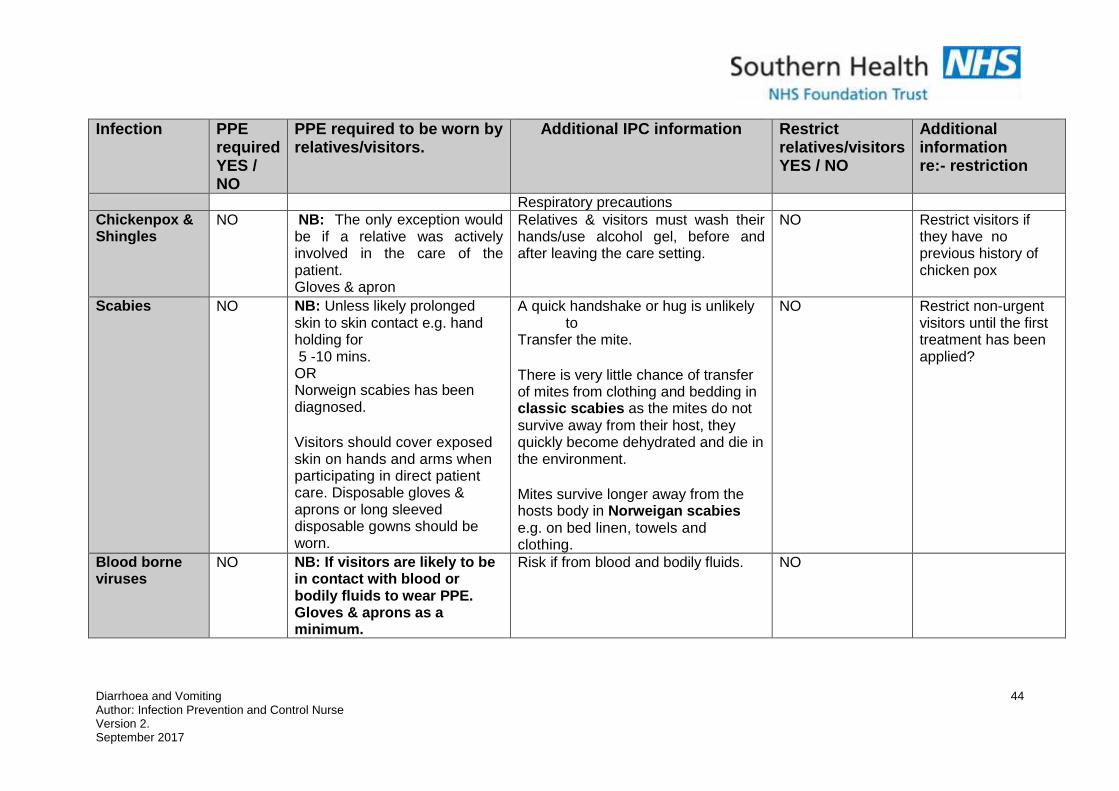
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
44
Infection
PPE required YES / NO
PPE required to be worn by relatives/visitors.
Additional IPC information Restrict relatives/visitors YES / NO
Additional information re:- restriction
Respiratory precautions Chickenpox & Shingles
NO NB: The only exception would be if a relative was actively involved in the care of the patient. Gloves & apron
Relatives & visitors must wash their hands/use alcohol gel, before and after leaving the care setting.
NO
Restrict visitors if they have no previous history of chicken pox
Scabies
NO NB: Unless likely prolonged skin to skin contact e.g. hand holding for 5 -10 mins. OR Norweign scabies has been diagnosed. Visitors should cover exposed skin on hands and arms when participating in direct patient care. Disposable gloves & aprons or long sleeved disposable gowns should be worn.
A quick handshake or hug is unlikely to
Transfer the mite. There is very little chance of transfer of mites from clothing and bedding in classic scabies as the mites do not survive away from their host, they quickly become dehydrated and die in the environment. Mites survive longer away from the hosts body in Norweigan scabies e.g. on bed linen, towels and clothing.
NO Restrict non-urgent visitors until the first treatment has been applied?
Blood borne viruses
NO NB: If visitors are likely to be in contact with blood or bodily fluids to wear PPE. Gloves & aprons as a minimum.
Risk if from blood and bodily fluids. NO
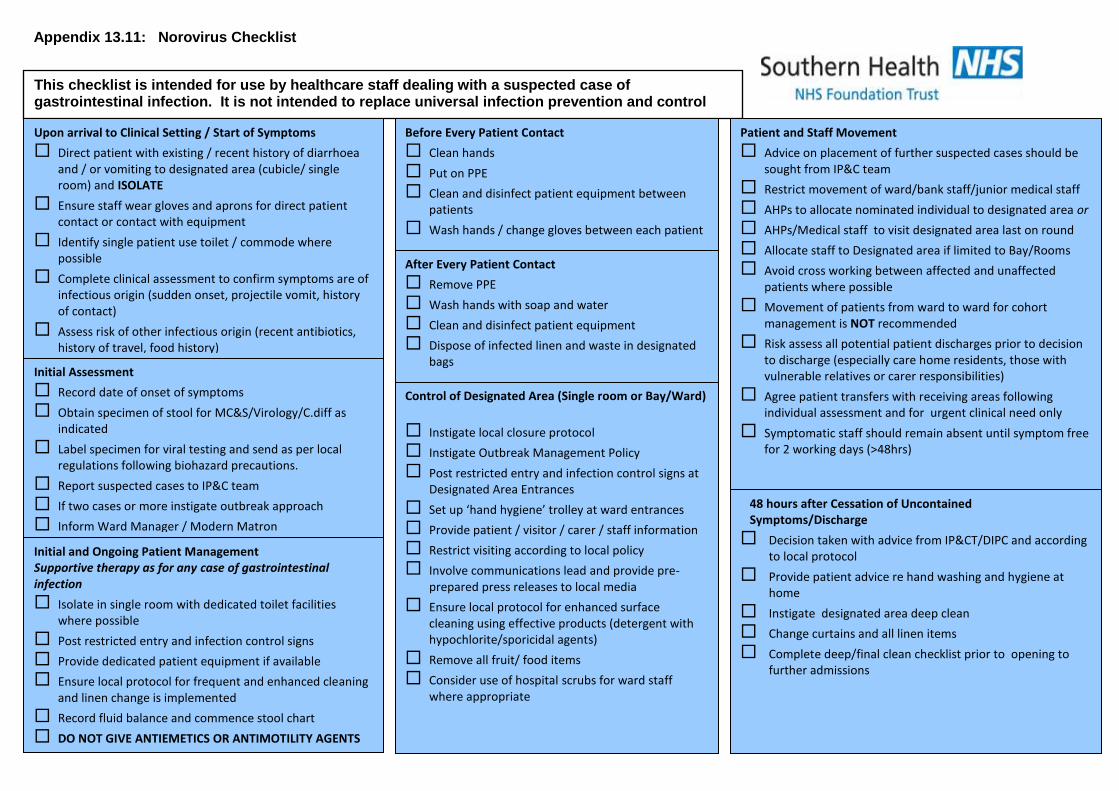
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
45
Appendix 13.11: Norovirus Checklist
This checklist is intended for use by healthcare staff dealing with a suspected case of gastrointestinal infection. It is not intended to replace universal infection prevention and control measures.
Upon arrival to Clinical Setting / Start of Symptoms
Direct patient with existing / recent history of diarrhoea and / or vomiting to designated area (cubicle/ single room) and ISOLATE
Ensure staff wear gloves and aprons for direct patient contact or contact with equipment
Identify single patient use toilet / commode where possible
Complete clinical assessment to confirm symptoms are of infectious origin (sudden onset, projectile vomit, history of contact)
Assess risk of other infectious origin (recent antibiotics, history of travel, food history)
Initial Assessment
Record date of onset of symptoms
Obtain specimen of stool for MC&S/Virology/C.diff as indicated
Label specimen for viral testing and send as per local regulations following biohazard precautions.
Report suspected cases to IP&C team
If two cases or more instigate outbreak approach
Inform Ward Manager / Modern Matron
Before Every Patient Contact
Clean hands
Put on PPE
Clean and disinfect patient equipment between patients
Wash hands / change gloves between each patient
After Every Patient Contact
Remove PPE
Wash hands with soap and water
Clean and disinfect patient equipment
Dispose of infected linen and waste in designated bags
Control of Designated Area (Single room or Bay/Ward)
Instigate local closure protocol
Instigate Outbreak Management Policy
Post restricted entry and infection control signs at Designated Area Entrances
Set up ‘hand hygiene’ trolley at ward entrances
Provide patient / visitor / carer / staff information
Restrict visiting according to local policy
Involve communications lead and provide pre-prepared press releases to local media
Ensure local protocol for enhanced surface cleaning using effective products (detergent with hypochlorite/sporicidal agents)
Remove all fruit/ food items
Consider use of hospital scrubs for ward staff where appropriate
Patient and Staff Movement
Advice on placement of further suspected cases should be sought from IP&C team
Restrict movement of ward/bank staff/junior medical staff
AHPs to allocate nominated individual to designated area or
AHPs/Medical staff to visit designated area last on round
Allocate staff to Designated area if limited to Bay/Rooms
Avoid cross working between affected and unaffected patients where possible
Movement of patients from ward to ward for cohort management is NOT recommended
Risk assess all potential patient discharges prior to decision to discharge (especially care home residents, those with vulnerable relatives or carer responsibilities)
Agree patient transfers with receiving areas following individual assessment and for urgent clinical need only
Symptomatic staff should remain absent until symptom free for 2 working days (>48hrs)
48 hours after Cessation of Uncontained Symptoms/Discharge
Decision taken with advice from IP&CT/DIPC and according to local protocol
Provide patient advice re hand washing and hygiene at home
Instigate designated area deep clean
Change curtains and all linen items
Complete deep/final clean checklist prior to opening to further admissions
Initial and Ongoing Patient Management Supportive therapy as for any case of gastrointestinal infection
Isolate in single room with dedicated toilet facilities where possible
Post restricted entry and infection control signs
Provide dedicated patient equipment if available
Ensure local protocol for frequent and enhanced cleaning and linen change is implemented
Record fluid balance and commence stool chart
DO NOT GIVE ANTIEMETICS OR ANTIMOTILITY AGENTS
Diarrhoea and Vomiting Author: Infection Prevention and Control Nurse Version 2. September 2017
46
ABOUT THIS CHECKLIST The NHS Norovirus Management Checklist is intended for use by hospital staff treating a suspected or confirmed case of gastrointestinal infection that may be attributed to Norovirus. This checklist combines two aspects of management:
i) clinical assessment of possible cases ii) infection control measures to limit the spread of cases thus reducing the
duration of an outbreak
The checklist is not a comprehensive tool but follows the approach of WHO Patient Safety Checklists in highlighting actions to be taken at critical points in the patient’s care pathway. They are produced in a format that can be referred to readily and repeatedly by staff to ensure that all essential actions are performed. They are not comprehensive protocols and do not replace routine care.
How to Use the Checklist Staff can use this checklist in a variety of ways – ticking the boxes is optional. The objective is to ensure that no critical patient care items are missing during or immediately following care The checklist can be:
- Used as part of the patient care record - Reproduced as wall posters - Printed as individual staff aide memoirs - Included in outbreak kits - Adapted and revised for local use
This checklist does not replace clinical guidance or clinical judgment.
Related Guidance and Advice Incubation Duration Low infectious dose Wards closed within 3 days of onset of cases are reported to have: 10-72 hours 24-48 hours asymptomatic carriage common Sources - contaminated food/water, infected food handlers, infected people
Outbreaks of shorter duration Transmission - aerosols, contaminated hands/surfaces
Lower patient attack rates Patient Recovery - 75% will recover within 3 days
Lower staff attack rates - 10% of hospitalised cases will remain symptomatic at Day 10 Testing PCR testing is recommended for sensitivity and specificity Estimated Outbreak Costs per NHS Trust (Acute and Community) Electron microscopy detects only reasonable levels of viral load £635,000
References Lopman, B. et al (2004) Epidemiology and cost of nosocomial gastroenteritis, Avon, England, 2002-2003 Emerging Infectious Diseases, 2004; 10(10):1827
WHO (2009) Patient Care Checklist: new influenza A(H1N1) Available at www.who.int
Lopman B. et al Clinical manifestation of norovirus gastroenteritis in health care settings Clinical Infectious Diseases,
2004; 39(3):318-24
This checklist was devised by members of the NHS Southwest Norovirus Working Group and has been adapted for use by HCHC. October 2009













![Evidence-Based Complementary and AlternativeMedicine · 2019. 7. 31. · Evidence-Based Complementary and AlternativeMedicine vomiting, diarrhoea, ulceration, and bleeding [ ]. Gas-trointestinal](https://img.pdfslide.us/doc/110x75/613baed6f8f21c0c826922b1/evidence-based-complementary-and-alternativemedicine-2019-7-31-evidence-based.jpg)

![GIS - K21 DIARRHOEA .ppt [Read-Only]ocw.usu.ac.id/course/download/1110000120...diarrhoea - freq. ≥3 x /day - changing of consistency - with/ without vomiting - with/without bloody](https://img.pdfslide.us/doc/110x75/5ea22a74b6bee67fea1b7254/gis-k21-diarrhoea-ppt-read-onlyocwusuacidcoursedownload1110000120.jpg)













