Embed Size (px)
Citation preview

UC 577,1; 61 ISSN 0354-3447
Jugoslov Med Biohem 25: 381–390, 2006 Revijski radReview paper
Jugoslov Med Biohem 2006; 25 (4): 381 DOI: 10.2298/JMB0604381S
Introduction
It has already been demonstrated that geno-mics have indeed begun to change the practice ofmedicine. If the genomic era can be said to have aprecise birth date, it was on April 14, 2003. That waswhen the international effort known as the HumanGenome Project put a close to the pre-genomic erawith its announcement (available at http://www.ge-nome.gov) that it had achieved the last of the pro-ject’s original goals, the complete sequencing of thehuman genome. The extent and pace of progress ingenomics are suggested by the fact that this achieve-ment occurred 11 days before the 50th anniversary ofthe publication of Watson and Crick’s description ofthe DNA double helix. If science, technology, andmedicine have consistently demonstrated anything, itis that they proceed at an ever-quickening pace. Thatwe have gone in the past 50 years from the firstdescription of the structure of our DNA to its com-plete sequencing gives some indication of how muchthe impact of genomic medicine on the health care oftoday’s neonates will increase by the time they turn50 years of age (1, 2).
The discovery of inherited mutations of genesassociated with increased risk of cancer has openeda new field of cancer medicine. As these genes havebeen identified and characterized over the pastdecade, cancer genetics has become intrinsic to thecancer risk assessment that is an essential compo-nent of the practice of preventive oncology. Syndro-mes have generally been identified based on obser-vation by clinicians. Once the underlying genes havebeen identified, further research must define the fullspectrum of the syndrome, including the gene pene-trance (associated cancer risk), identification of anydistinguishing histologic, immunohistochemical, ormolecular features of the component tumours,details of other associated findings and, ultimately,effective strategies for surveillance and prevention.This process can take many years. The resultinginformation is essential for individuals and families asthey consider whether or when to undergo genetictesting, and the implications of the test result formutation carriers. Recent guidelines have also emp-hasized that, in order to competently offer a genetictest to a patient or family, the provider must be pre-pared to deal with a spectrum of medical, psycholog-ical, and social consequences of a positive, negative,or ambiguous result. Some courts have already de-monstrated their belief that health care providers bearresponsibility for informing patients that their cancermay have an inherited basis, with specific implica-tions for their children (1).
DIAGNOSTICS OF HEREDITARY MALIGNANCIES
Karmen Stankov
Department of Biochemistry, Clinical Center »Novi Sad«, Novi Sad, Serbia
Summary: Significant advances have occurred in our understanding of the cancer etiology in the lastdecade, as a consequence of the generalized use of molecular biology techniques in human genetics. Canceris a form of a complex genetic disease. Most forms of cancer are characterised by the accumulation of diffe-rent genetic alterations affecting genes from a set of genes with pathogenic potential, which is specific for eachtumour entity. While in the majority of malignant tumours these changes are somatically acquired, some muta-tions are transmitted through the germline and account for an inherited tumour predisposition. The next fron-tier in cancer genetics is to find genes with high prevalence alleles conferring a low increase or decrease of can-cer risk.
Key words: diagnostics, cancer, hereditary malignancies
Address for correspondence:
Assistant Professor Dr Karmen StankovDepartment of BiochemistryClinical Center ’ Novi SadHajduk Veljkova 321000 Novi Sad, SerbiaFax: 021/662’41’53

This review is intended to provide a brief sum-mary of the major inherited cancer syndromes, co-vering recommendations for genetic diagnostics. Thedata emphasize some of the most important obser-vations in the last two decades, during which manycancer susceptibility genes have been identified(Table I) (3). Epidemiologic studies have elucidatedthe underlying genetic heterogeneity of even raretumours: that is, susceptibility to specific tumoursmay be attributable to mutations in different genes.Conversely, some syndromes that appeared to beindependent have been found to be manifestations ofdifferent mutations in the same gene. Alternate clas-sifications are surely possible based on gene func-tion, specific tumours, and other factors. Theincreasing ability to identify individuals at remarkablerisk for particular cancers, generally at early ages, hasbrought with it the responsibility to devise effectivesurveillance and prevention strategies for these indi-viduals. It is important, therefore, that cancer gene-tics be included under the aegis of cancer preventionas an area that has become an essential componentof medical oncology.
Cancer as a genetic disease
Cancer can be considered a genetic disease for itis caused by alterations affecting the DNA of somaticcells. However, the definition of cancer as a hereditarydisease implies that mutations are already present in
the germline and transmitted into families. Pedigreeanalysis identifies the familial forms of cancer, whichare rarer than sporadic forms and are described foralmost every type of tumour. These forms may segre-gate into families as simple Mendelian disorders, but aless penetrant predisposition to develop cancer mayalso be transmitted as a complex genetic trait (4).
Numerous studies have demonstrated that bothsomatic genetic changes and hereditary factors areinvolved in the etiology of many cancers (4, 5). Thefamilial forms are very helpful for the discovery of thegenes that increase the susceptibility to cancer andmay elucidate on the contribution of a single gene tothe disease predisposition. Since very often two ormore genetic loci with variable contribution fromenvironmental factors are implicated in tumour pre-disposition, cancer falls within the category of multi-factorial diseases (5).
Polygenic determination may involve: (a) a smallnumber of loci (oligogenic); (b) many loci, each locushaving only a small effect (polygenic); (c) a singlemajor locus with a multifactorial background.
Two theories on inherited predisposition to can-cer are to be taken into account in order to explainhow cancer may be genetically determined. More-over, genetic heterogeneity is to be considered, inthat it may underlie an apparent polygenic determi-nation.
Table I The genes involved in the predisposition to hereditary malignant syndromes (8)
Syndrome Gene Chromosomal localisation Localisation/tumour type
MEN2 RET 10q11 Medullar thyroid, pheochromocytoma
Hereditary breast/ovarian cancer BRCA1 17q21 Breast, ovaries, colon, prostate
Hereditary breast cancer BRCA2 13q12 Breast, male breast cancer
Hereditary melanoma CDKN2 9p21 Melanoma, pancreas
Hereditary colon polyposis APC 5q21 Intestinal polyps, colon cancer
Hereditary retinoblastoma RB 13q14 Retinoblastoma, osteosarcoma
Hereditary Wilms tumours WT1 11q13 Wilms tumour, aniridia, genitourinary abnormalities, mental retardation
Li-Fraumeni syndrome p53 17p13 Sarcoma, breast cancer
Neurofibromatosis NF1 17q11.2 Neurofibroma, neurofibrosarcoma
Tuberose sklerosis TSC2 16p13.3 Angiofibroma, renal angiomyolypoma
Von Hippel-Lindau VHL 3p25-26 Kidney cancer, pheochromocitoma
382 Stankov: Diagnostics of hereditary malignancies

Jugoslov Med Biohem 2006; 25 (4) 383
The two-hit hypothesis
In 1971 a predictive study on retinoblastoma(RB) by Knudson (6) hypothesized that two succes-sive mutations (’hits’) were required to turn a normalcell into a tumour cell. In familial RB the first hit is aninherited mutation occurring in the germline thatgives tumour susceptibility, and the second is a so-matic mutation occurring in the target tissue (retina),which promotes tumour formation. According to thismodel, sporadic tumours arise from two successivemutations occurring in the same somatic cell. Thistheory also explains why hereditary cases are morelikely to be bilateral and diagnosed earlier. Succes-sively, it was suggested that this model could beapplied to other types of hereditary cancer. The iden-tification of the RB gene proved the inactivation ofrecessive genes as tumour suppressor genes (TSG)via a two-hit mechanism (7).
The polygenic model
The polygenic theory was postulated to describethe quantitative traits governed by the simultaneousaction of many loci as polygenic in Mendelian terms.Since many families show diseases and malforma-tions which cannot be defined as Mendelian traits,the polygenic theory was extended to the so-calleddiscontinuous characters by postulating a continu-ously variable susceptibility following a Gaussian dis-tribution in the population and the existence of athreshold superimposed on the developmental pro-cess. Affected people inherit an unfortunate combi-nation of high-susceptibility genes and their relativesmay have a raised susceptibility diverging from thepopulation mean at rate of shared gene proportion. Apolygenic inheritance of predisposition to cancer isdemonstrated in experimental animals and suggest-ed in humans for different tumours. The polygenicmodel of cancer predisposition explains the low pe-netrance through the allele assortment of multiplegenes, each having two alleles: ’r’ for resistance tocancer and ’s’ for susceptibility, where ’s’ is dominantover ’r’. For example, if three genes control tumourpredisposition, the risk of cancer would be high inindividuals carrying the three ’s’ alleles, intermediatein individuals with two ’s’ alleles and low in those withone ’s’ allele (8).
Genetic heterogeneity
A disease may also appear genetically complexbecause of genetic heterogeneity. Genetic hetero-geneity is defined as the occurrence of independentmutations at the same locus (allelic heterogeneity) orat more different loci (locus heterogeneity), all caus-ing the same disease phenotype. In case of geneticheterogeneity for a given trait linkage of the diseaseto markers located in a given chromosomal region
will be found in some families, but not in others withthe same disease (4).
General aspects of hereditary cancer risk assessment
Identifying individuals at increased risk
Dramatic advances in our understanding of thegenetic basis of cancer have led to new forms of tech-nology and new tools for assessing the genetic risk ofcancer. Although inherited forms of cancer are rare ’representing only about 5 percent of many types ofadult onset cancer ’ the risks conferred by the inher-ited cancer-susceptibility genes are high and the can-cers frequently appear at a young age. A commonperception of familial cancer is that it is a matter notof whether cancer will develop but of when. Yet sincemost hereditary cancer syndromes are autosomaldominant, the laws of Mendelian genetics dictate thatthere is only a 50% chance of inheriting the familialpredisposition to cancer. This is where genetic testingcan help. When informative, it presents an unprece-dented opportunity to prevent the development ofcancer (Table II) (9).
The majority of patients who develop cancer doso sporadically, that is, there is no familial or heredi-tary risk. The small percentage of patients with ahereditary cancer syndrome may be suspected on the
Table II Identifying and testing for hereditary susceptibility to common cancers (9)
1. Pedigree construction
2. Genetic counselling and testing
3. Components of informed consent
A description of the purpose and type of test being performed
Technical accuracy of the test
Implications of a positive and negative result and possibility that the test will not be informative
Options for risk estimation without genetic testing
Risk of passing mutation to children
Fees involved in testing and counselling
Psychological implications of test results
Risks of insurance and employer discrimination
Confidentiality issues
Importance of sharing genetic test results with at-riskrelatives so that they may benefit from this information
4. Result reporting and post-test counselling

384 Stankov: Diagnostics of hereditary malignancies
basis of personal and family medical history. Unfor-tunately, data gathering around family history is oftenincomplete. When a family history of cancer is obtai-ned, critical details needed for risk assessment, suchas the cancer site and age of diagnosis, are oftenlacking. This occurs in both primary care and spe-cialty settings. One study showed that the age ofdiagnosis was documented in only 7% of relativesidentified as having cancer. Tools to help facilitatefamily history gathering, such as medical intake ques-tionnaires, have been in use for many years, but datashowing their effectiveness are lacking.
Hereditary cancer syndromes are estimated toaccount for 5% of diagnosed breast, ovarian, andcolon cancers. Although uncommon, they are impor-tant to recognize because they confer a high risk ofmultiple primary cancers occurring at younger ages,affecting multiple members of a family who inheritthe cancer-predisposing genetic mutation. More im-portantly, patients and providers are recognizing thepotential therapeutic advantages of identifying he-reditary cancer risk. With a growing number of pre-ventive care options available to patients and familieswith hereditary cancer syndromes, the process of sys-tematically assessing risk is becoming increasinglyimportant. Both provider and patient forces are con-tributing to the development of hereditary cancer riskassessment. Patients are becoming increasingly awa-re of cancer genetics through media exposure and,more recently, through direct advertising to consu-mers of commercially available testing. Patient inter-est and awareness of testing have in turn affected de-livery of genetic services. In fact, patient inquiry aboutcancer genetic testing is one of the strongest predic-tors of providers ordering or referring for testing.
Identification of the cancer susceptibilitygene(s) through positional cloning
As shown in numerous studies, there is a highlikelihood that cancer has a familial component (10,11). There are two main ways in which such suscep-tibility genes may be identified. The first is the identi-fication of a biological or biochemical anomaly asso-ciated with the disease ’ due to the identification ofthe biochemical change, the causative gene maythen be identified. The second technique is reversegenetics, which allows the identification of the cau-sative gene without prior knowledge of its biologicalfunction. Therefore, as the majority of genetic disea-ses identified cannot be associated with an obviousbiochemical change, reverse genetics has been thetechnique of choice for identification of susceptibilitygenes. Reverse genetics uses the fact that the diseasein question is familial, and hence members of anaffected family will share a common inherited factorthat is causing the disease. As reverse genetics isreliant on this fact, the first step is to identify that thetrait of interest is a genetic trait.
Some inherited traits can be the result of soma-tic translocations of chromosomes which are segre-gated through the affected family, for example, theFHIT:TRC8 translocation which was shown to causesusceptibility to renal cancer, and, to a lesser extent,PTC (papillary thyroid carcinoma) (12), and, as statedabove, 5q21 was identified as the candidate area forFAP (familial adenomatous polyposis) through aninterstitial deletion in a patient with Gardner syn-drome (13). Such a rearrangement should be obser-ved through standard cytogenetic techniques, andtherefore in families with the inherited trait of interestshould be a kariotype of the affected patients. How-ever, in the majority of cases the genetic defect isonly the alteration of one nucleotide base, which, ofcourse, will not be detected under g-banding stainingtechniques.
If cytogenetics is unable to identify the region ofthe genome in which the susceptibility gene is loca-ted, the next step in positional cloning is to use thetechnique of linkage analysis to identify the region ofthe genome in which the susceptibility gene is posi-tioned. Linkage analysis works on the premise thateach affected patient from each family shares a sus-ceptibility gene. As the susceptibility gene segregatesthrough the family, the process of independent seg-regation of the chromosomes and recombinationalong the chromosome will mean that, in addition tothe susceptibility gene, the affected patients fromeach family will also share the genomic area surroun-ding the gene. Using one large, or large sets of fami-lies, linkage analysis allows the identification of thisshared genomic region and hence the approximateposition of the susceptibility gene. When such aregion has been identified and results confirmed bysubsequent studies, the position of the susceptibilitygene in the genome is determined, which is named asusceptibility locus. Linkage analysis has been verysuccessful in localising a large number of simpleMendelian traits. However, as the complexity of thegenetic trait increases, the effectiveness of linkageanalysis to detect susceptibility loci decreases. Fa-milial prostate cancer is the example of how a com-plex genetic trait can significantly impact on the po-wer of linkage analysis to identify susceptibility (8).Using large sample sets, a number of prospective locihave been identified, however, due to the high phe-nocopy rate, late age of onset, lack of a means tostratify patients into more homogenous groups andconsiderable genetic heterogeneity, confirmation ofthe linkage results has proven arduous.
By examination of the families that are linked tothis susceptibility locus, recombinant events will allowthe identification of an area in which all the linkedfamilies share a region of DNA. In the genetic insta-bility in cancer, loss of heterozygosity (LOH) hasgreatly aided the identification of tumour suppressorsand gains, through techniques such as comparativegenomic hybridisation (CGH), offering the same po-

tential in identifing protooncogenes. A novel appro-ach was used by Hemminki et al (14) to map a locuson chromosome 19 in Peutz-Jeghers syndrome. Thisapproach used CGH and LOH to identify the chro-mosome 19 region, and then used targeted linkageanalysis in affected families to confirm the result. Asmentioned above, the susceptibility gene was subse-quently identified as STK11 (15, 16). A similar appro-ach was applied in the search for prospective BRCA3loci, and a possible locus on chromosome 13 usingCGH and targeted linkage analysis (17), however, todate this linkage result has not been confirmed.
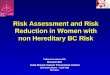
Through the examination of LOH or recombi-nant events, if this region is sufficiently small in size,if no obvious candidate gene exists, then a physicalmap of the area is constructed. Previously, this in-volved the tedious task of assembling a physical mapof the region, using Southern blot, to identify the cor-rect area followed by construction of the physicalmap, by sequencing overlaying Bacterial ArtificialChromosome (BAC) clones. Once the physical maphas been constructed, the genes contained in theregion can be identified. Techniques such as exontrapping allow the identification of genes in the areaand, once identified, these genes can be screened formutations that segregate with the disease. However,the completion of the Human Genome Project (18),and in addition the availability of the privately fundedCelera raw sequence (19), have greatly facilitated theconstruction of such physical maps, making the con-struction of overlapping BAC clones and sequencingredundant. The availability of the raw sequence addi-tionally offers a larger number of markers to allow fur-ther and finer restriction of an area of interest throughthe exploitation of the informative recombinationsand LOH or CGH. Subsequently to the identification,the genes in that area can be identified, either byidentification of known genes that map to that area orby prediction through computer programs, by identi-fication of Expressed Sequence Tags (ESTs) whichmatch the sequence, gene prediction programs, andmore recently, comparative sequencing betweenmouse and human genomes allows areas that arehighly conserved to be identified (highly conservedareas are under greater evolutionary pressure andtherefore are more likely to be functionally significanti.e. genes). Once the genes in that area are identified,screening the coding region in patients identifiesmutations that segregate in affected families andallow the identification of the causative gene. Positio-nal cloning has been successful in identifying genesimplicated in human disease, notably in the field ofcancer research, PTEN, APC, BRCA1, BRCA2, ME-NIN, PKA, and STK11 (20, 21) (Figure 1).
All of the steps in positional cloning strategyinvolve the utilization of molecular biology methods(such as cDNA library screening, cDNA selection,CpG island identification, exon trapping, sequenceanalysis, STSs, ESTs, linkage, loss of heterozygosity,
etc.) and bioinformatics methods. Our ability to findthe genes involved in genetic susceptibility to manydiseases, including the cancer, is increasing rapidly.The utilization of bioinformatic methods in cancerresearch already became a routine, owing to power-ful analytical tools and the completed human ge-nome sequence information (22, 23).
Contribution of molecular biology in hereditary cancer diagnostics and treatment
The methods involved in molecular geneticsscreening in hereditary nonpolyposis colorectal can-cer (HNPCC) patients involve: DNA isolation fromblood and normal colon samples, microsatelliteinstability testing (MSI), direct sequencing of predis-posing genes (MLH1, MSH2, MSH6), Western blotprotein detection and immunohistochemistry (24).
DNA replication errors characterize tumourswith loss-of-function mutations in mismatch repair(MMR) genes. These can be detected as microsatel-lite instability testing (MSI), which is the finding that,in the same individual, the number of repeats in agiven repeating sequence of DNA varies from cell tocell instead of being constant. Several (usually five orsix) such repeating sequences’called microsatellitemarkers ’ can be examined for variability (termed»instability«), indicating errors in DNA replication.MSI is termed »low« if zero or one of the markersshow instability, and »high« if a high proportion of themarkers is unstable. More than 90% of colorectalcancers (CRCs) in people with DNA mismatch repairgene mutations have high MSI, whereas less than15% of sporadic CRCs do. A recent economic analy-sis compared the cost per year of life gained for threestrategies for identifying cases of HNPCC: (1) geno-
Jugoslov Med Biohem 2006; 25 (4) 385
Figure 1 Summary of transcription regulatory functions of BRCA1. This figure shows the range of transcriptional
pathways and individual target genes that may be regulated,in part, through BRCA1. Some of these pathways may
contribute to the tumour suppressor function of BRCA1.They may also relate to normal functions of the BRCA1
protein that are not directly linked to tumourigenesis (21).
BRCA 1
Steroid HormoneReceptor Signaling
(ER-a, AR)Stress Response
Antioxidant Response(ATF1, NFE2L2, GSTs,
Oxidoreductases
Growth InhibitionDNA Damage Response
(p21WAF1, p27Kip1
Gadd45a, Gass153)
Transcriptional Repression(ZBRK1/2, RbAp46/48)
Transcriptional ActivationMediator, Chromatin Modification
(RNA Pol II, RHA, NUFIP,P300, P-TEFb, TRAP220,
SWI/SNF, COBRA1)
Tumour Suppressor(p53, RB1,
BRCA2, BARD1)
Oncogene(c-Myc, hTERT,
IGF1R)

typing everyone with colon cancer for MMR genemutations (the most expensive); (2) testing every can-cer for MSI and genotyping those with high MSI; or(3) applying the Bethesda criteria (family history, age,and histology) to all cases of CRC, testing for MSI onthose meeting the criteria, and genotyping the subsetwith high MSI. Given the expense of genotyping,strategy 3 was the most cost-effective. This analysisalso pointed out that the cost’benefit ratio for MMRgene mutation testing decreases dramatically if oneassumes that identifying one person with MMR genemutations leads to the offer of testing and institutionof preventive measures in siblings, sons, and daugh-ters rather than the tested individual alone (25).
DNA microarrays as diagnosticand prognostic tools
In diseases such as cancer, many biologicalpathways and cell functions are irreversibly altered atthe transcriptional, translational and protein level.Various technologies exist in order to investigate can-cer-related modifications in the cells. One promisingapproach relies on microarray expression profiling.Microarrays enable a precise analysis of multipleparameters in a miniaturised format (26).
The successful clinical management of humanmalignancies requires an ever-evolving arsenal ofboth diagnostic and prognostic methods, and mi-croarray analysis may be able to serve as a new toolthat provides useful information for both. Currently,histopathologic evaluation of tumour type and grade,and pathologic and clinical assessment of a cancer’sstage are the mainstays for guiding therapeutic inter-ventions and predicting outcomes. These data areusually supplemented with information from the pa-tient’s history, the physical exam, imaging tests, andclinical laboratory assays of tumour markers (26’28).
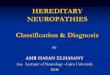
However, even the combined use of all availableclinical and laboratory information remains subopti-mal for diagnosis, for predicting prognosis, and forpredicting patient response to specific therapies.Tumours with identical histopathologies mayprogress differently, may respond differently to thera-py, and may be associated with widely divergent clin-ical outcomes, suggesting that additional factors maybe directing disease outcomes. DNA microarraytechnology may be a more comprehensive determi-nant for guiding therapeutic interventions in thefuture (Figure 2) (28).
The potential for microarray analysis to assumea significant role in cancer diagnosis and treatmentselection is excellent. The importance of microarraysto future progress in oncology and other fields ofmedicine is supported by the recent appearance ofreview articles in several clinical journals (26’29).Although the technology is still evolving and its usesare still being explored, the promise demonstrated
thus far from research findings on microarrays’ abili-ty to predict prognosis of some diseases is astoun-ding. Microarray-based studies have already identifiedmany genes whose protein products might serve aseffective biomarkers for cancer diagnoses, prognosis,and individualized treatment selection. These studieshave also identified genes whose protein productsmay provide therapeutic targets for the progressivedevelopment of novel, more effective, and less toxicchemotherapeutic agents (29).
The gene expression profiles obtained by cDNAmicroarrays may help ascertain the key geneticevents underlying tumour initiation, promotion, andprogression. This type of genetic information mayprovide the foundation for the development of eitheruniversal or tumour-specific chemopreventive agents.In any event, illumination of DNA transcriptionalevents that are perturbed during tumourigenesis asuncovered by microarray analysis will unquestionablypave the way toward more protein-based researchefforts to reveal the myriad interplay of protein func-
386 Stankov: Diagnostics of hereditary malignancies
Figure 2 cDNA microarray schema: templates for genes of interest are obtained and amplified by PCR.Following purification and quality control, cDNAs are printed onto coated glass microscope slides using a
computer-controlled high-speed robot. Total RNA fromboth the test and reference sample are fluorescentlylabelled using a single round of reverse transcription.
The fluorescent targets are pooled and allowed to hybridizeunder stringent conditions to the clones on the array. Laser excitation of the incorporated targets yields an
emission with a characteristic spectra, which is measuredusing a laser scanning instrument. Information about the
clones, including gene name, clone identifier, intensity values, intensity ratios, normalization constant, and
confidence intervals, is attached to each target. Data from a single hybridization experiment are viewed as a normalizedratio (that is, Cy5/Cy3) in which significant deviations from
1 (no change) are indicative of increased (> 1) ordecreased (< 1) levels of gene expression relative
to the reference sample. In addition, data from multipleexperiments can be examined using any number
of data mining tools (28).
DNA clonestest
PCR amplificationpurification
referencelaser 1 laser 2
excitation
emission
computeranalysis
hybridize targetto microarray
reversetranscription
label withfluor dyes
robotic printing

tions and protein-protein interactions that ultimatelycontribute to human tumour development (27).
Molecular markers in clinical oncology:assays, tissues, progress and pitfalls
The promise of molecular diagnostics for can-cer prevention in terms of early detection rests on twopremises: assays can be developed to measure pro-teins, DNA, RNA or metabolites that accurately andreproducibly detect incipient neoplasias; and that thisearly detection will eventually result in a decrease inmorbidity and mortality, and therefore benefit pa-tients. Novel molecular technologies, including lasercapture microdissection, time-of-flight mass spectro-metry, DNA microarrays, tissue arrays, protein micro-arrays and antibody microarrays, are being developedto investigate the molecular differences between di-sease and normal cells and detect cancer-specificalterations in proteins, DNA and RNA in body fluids.Although literally hundreds of articles are publishedeach year describing alterations in genes or proteinsthat are associated with cancer, very few result in use-ful molecular diagnostics for early cancer detection.Thus, there remains a critical need for new biomark-ers for use in early detection and for assay methodsthat allow the translation of these biomarkers fromthe laboratory to the clinic (30, 31).
In spite of advances in diagnostics and thera-peutics, cancer remains the second leading cause ofdeath in the western countries. Successful cancertreatment depends not only on better therapies butalso on improved methods to assess an individual’srisk of developing cancer and to detect cancers atearly stages when they can be more effectively trea-ted. Current cancer diagnostic imaging methods arelabour-intensive and expensive, especially for scree-ning large asymptomatic populations. Effective scree-ning strategies depend on methods that are non-invasive and detect cancers in their early stages ofdevelopment. There is increasing interest in andenthusiasm about molecular markers as tools forcancer detection and prognosis. It is hoped that ne-wly discovered cancer biomarkers and advances inhigh-throughput technologies would revolutionizecancer therapies by improving cancer risk assess-ment, early detection, diagnosis, prognosis, and mo-nitoring therapeutic response. These biomarkers willbe used either as stand-alone tests or to complementexisting imaging methods (30, 31).
Molecular markers in clinical oncology can bedivided into diagnostic markers, which distinguishone disease from another; prognostic markers, whichare associated with the clinical behaviour of a tu-mour; and predictive markers, which are used to pre-dict outcome of therapy and to aid in the selection ofoptimal treatment.
Diagnostic and prognostic markers, thoughimportant in clinical management, are deterministicin nature, in that the natural course of a cancer is notlikely to be changed because of knowledge of thatmarker status. However, more excitement within thelast decade has been centred on predictive markers,many of which are also the targets for specific the-rapeutics. What is important, of course, is that theascertainment of these predictive markers may guidetreatment selection that can change the course of adisease (31).
A troubling aspect of molecular cancer diag-nostics has been previously recognized, but is still notarticulated very well. Quality control, cut-off criteria,and consistent analytic formats may seem pedestrian,but are critical to achieving practical clinical impact.Unfortunately, the absence of accepted standardsmay lead to disturbingly high rates of false calls or, atleast, uncertainty in the results. Using a variety ofaccepted methods for the detection of molecular per-turbations, the analytical study was performed (31).Analytical results show that data discrepancies thatwould change clinical interpretation occurred in therange of 7% to 8%, and that the majority of the inac-curacies may be due to the clinician’s not consideringsomething as simple as the proportion of tumourcells in the sample. If significant clinical decisions aremade on any one test, then this range of technicalerror is a source of great concern.
Although the initial reaction to these data maybe one of alarm, it is actually surprising that the errorrate is as low as documented given the different ana-lytic platforms (fluorescent in situ hybridization[FISH], Southern blot, polymerase chain reaction[PCR]) used. Clinicians, accustomed to the repro-ducibility of routine laboratory tests such as serumsodium and quantitative immunoglobulin levels, areoften surprised at the qualitative and relatively inexactnature of molecular diagnostics (31).
Results from molecular technologies are met-hod-, reagent-, and operator-sensitive. For example,Southern blot analysis for MYCN amplificationdetects a band of a specific molecular weight and issensitive to DNA degradation. Although PCR is sub-ject to PCR amplification bias and detects only thepresence of a specific fragment of the gene, it ismuch less sensitive to DNA degradation. A resultfrom either PCR or Southern blot hybridization is anaverage of the DNA in the tumour, which includesstromal and inflammatory cells. FISH, however, likeimmunohistochemical analysis of tissue sections,detects single cell events in a population of cells with-in a tumour. Despite the fact that all techniques seekto identify gene amplification, the data outputs aresufficiently different so that the results are not alwaysreadily comparable. The most rational approachwould then be to standardize one technical platformand enforce its use as the gold standard. Unfortu-
Jugoslov Med Biohem 2006; 25 (4) 387

nately, sometimes even economics impede the adop-tion of standards. The low profit margins for somediagnostics hinder the development of standardizedkits tested in rigorous (and expensive) clinical trials.Nevertheless, these issues can still be adequatelyaddressed by organization and consensus. However,even if standardization were simple, the practical rea-lities are much more complicated. First, moleculartechnologies are not stable and are highly fluid: new,more robust, more exact, and cheaper approachesemerge frequently. The evolution of the bcr-abltranslocation assay from one based on cytogeneticsto Southern blot hybridization and reverse transcrip-tase PCR is an excellent example of this improvementcycle. This raises the question of whether each tech-nical improvement of a molecular test needs to bevalidated in a completely independent clinical trial. Ifthis principle were applied to predictive markers instudies where the outcome may require 5 to 10 yearsof follow-up, few advances would be made. Second,even if tests could be standardized, biologic variabili-ty limits the convertibility of one analytic platform toanother. For example, protein levels and gene ampli-fication measure are related, but clearly different tar-gets. Immunohistochemical analysis for HER-2 over-expression correlates with gene amplification 70% to80% of the time, at best. Does the 20% to 30% dis-crepancy nullify the utility of this test as a predictivemarker? Investigators have found that, despite thesediscrepancies, HER-2 overexpression by immunohis-tochemical analysis and HER-2 amplification byeither differential PCR or FISH were both able to dis-tinguish the subset of node-positive patients benefi-ting from dose-intense chemotherapy (31).
Moreover, it is questionable what can be con-sidered the gold standard. Biologic reality would sug-gest that the protein product represented by theimmunohistochemical result should be more associ-ated with tumour behaviour than gene amplification,and should therefore be considered the biochemicalgold standard. For the HER-2 marker, however, re-cent data suggest that FISH analysis for gene ampli-fication is more likely to predict response to trast-uzumab than the standardized immunohistochemicaltest. These results seem counterintuitive, but perhapscan be explained by the fact that immunohistoche-mistry is a less quantitative and potentially less con-sistent analytic test than the FISH (31).
The many ways in which a molecular markercan be defined as abnormal, when compared withnormal, can also confuse the clinical interpretation ofmolecular results. For example, P53 mutations withbiologic consequences can be found as missensemutations anywhere in the gene that give rise to anabnormal protein, or as deletion-insertion or splicemutants that render the transcript unstable andshort-lived. In addition, the same biologic outcomecan be achieved by alternative abnormalities that alterdownstream p53 biology or biochemistry such as
murine double minute 2 (MDM2) amplification, orthe presence of human papilloma viral oncoproteinE6 that enhances the degradation of the p53 onco-protein. For the p53 status of a cancer, no singlemolecular test will completely define the functionalabnormality and will therefore always be incomplete.This will become an important issue when therapeu-tics directed at abnormal p53 pathways are develo-ped (30, 31).
The conclusion that molecular tests are impre-cise or technically unstable and should not be usedis, however, inappropriate. Nevertheless, the exam-ples discussed here should force us to develop morestructured strategies in marker development and ininforming the clinical community about how best tointerpret these markers. Several groups have sug-gested standards in marker development that arereasonable and should be heeded.
The foundations of these recommendationsare: precision in the detection of a valid target, repro-ducibility of the test, and stable access to necessaryreagents over time. The work by Ambros et al (30)also highlights the importance of standardized tissueprocessing and the need to assess tumour and nor-mal-tissue content (Table III) (30). But given the pro-gressive importance of tumour markers in guidingtherapeutic options, we should consider different waysof interpreting marker data and new approaches tospeed their development and validation.
Marker development and the new realities
The new molecular reality is that scientists arenow able to generate a large number of potentialdiagnostic and prognostic markers with remarkablespeed. The high-throughput capabilities of new tech-nologies, such as expression and tissue arrays and
388 Stankov: Diagnostics of hereditary malignancies
Table III Qualifications of a molecular test (30)
Attribute Questions asked
Precision in the detectionof a valid target
Does it detect the appropriatemolecular target?
Reproducibility of the test
How stable are the results?
Access to the necessaryreagents over time
Are the reagents exhaustible?
Tissue composition Is the analytical technologyobsolete?
Are we testing the right tissue?
What is the fraction of tumour cells?

proteomic approaches, identify definitive diseasemarkers, often without obvious mechanistic associa-tions. In this scenario, our approach of picking onemarker at a time for development is unacceptablyslow. Instead, it is suggested that the following modelfor marker development should be considered(Figure 3) (31). Marker genes associated with diseaseor prognosis identified by high-throughput proce-dures or database searches (as in the CancerGenome Anatomy Project) and then validated on aseparate tissue set will need to be identified. First, theassociated full-length cDNAs are cloned and recom-binant proteins expressed to generate antibodies. Acollection of these will be made available for any cli-nical trials group for testing on therapeutic trials, withan understanding that the raw data will be retained in
a central data repository for later use in meta-analy-ses. It is estimated that for breast cancer alone theremay be between 50 and 300 such markers, depen-ding on the stringency of selection. Conceivably, allcancers can be studied in this fashion. As recently as10 years ago, the absence of technologies such asmicroarrays, cDNA libraries, and antibody productionwould have made such a sweeping oncodiagnosticproject unimaginable. Now, it is hard to imagine howcancer diagnostics can adequately be exploited with-out such a plan (31).
Molecular genetic testing offers importantopportunities for diagnosis and assessment of geneticrisk for cancer. The sensitivity of tests for rare condi-tions will continue to improve as additional causativemutations are identified. Genetic tests are available todetermine the risk of common diseases, but theseoften have limited predictive value. Evaluation of theclinical usefulness of these tests will require a carefulassessment of the risks and benefits of testing; theavailability of specific measures to reduce risk in gene-tically susceptible people will be a major consideration(32).
One of the difficult challenges in the use of ge-netic tests is a constantly changing knowledge base.Research to evaluate interventions based on geneticrisk will assume increasing importance as new testsbecome available. Because the development of teststo assess risk is likely to outpace the ability to reducethe risk, an ongoing dialogue involving clinicians andpolicymakers will be needed to develop a consensusabout their appropriate clinical use (32).
Jugoslov Med Biohem 2006; 25 (4) 389
DIJAGNOSTIKA NASLEDNIH MALIGNITETA
Karmen Stankov
Zavod za biohemiju, Klini~ki centar ’ Novi Sad, Srbija
Kratak sadr`aj: Na{e razumevanje etiologije nastanka predispozicije za nasledna oboljenja je poslednjihgodina izuzetno napredovalo. Taj napredak omogu}en je pre svega naglim razvojem molekularne genetike iispitivanja genoma, kao i njihovom primenom u humanoj genetici. Malignitet je specifi~an oblik kompleksnoggenetskog oboljenja. Ve}inu tipova malignih oboljenja karakteri{e akumulacija razli~itih genetskih alteracija kojeuti~u na gene sa specifi~nim patogenim potencijalom, koji su specifi~ni za svaki tip maligniteta. Kod ve}inemalignih tumora te genetske alteracije odvijaju se na nivou somatskih }elija, me|utim neke od njih se prenosepreko germinativnog epitela i imaju ulogu u naslednoj predispoziciji za nastanak maligniteta. Budu}i izazov ugenetici maligniteta predstavlja identifikacija gena sa visokom prevalencijom alela koji doprinose smanjenju ilipove}anju rizika za nastanak maligniteta.
Klju~ne re~i: dijagnostika, karcinom, nasledni malignitet
Diagnostic trials
In vitro cell biology
Antibodies
Full length cDNA Candidate marker gene confirmation
Microarray data
Marker databases: CGAP
Figure 3 A model for marker development (31)

References
1. Godard B, Hurlimann T, Letendre M, Egalite N. Gui-delines for disclosing genetic information to family mem-bers: from development to use. Familial Cancer 2006; 5:103’16.
2. Guttmacher AE, Collins FS. Welcome to the genomicera. N Engl J Med 2003; 349: 996’8.
3. Lynch HT, Lynch JF. Hereditary cancer: family history,diagnosis, molecular genetics, ecogenetics, and man-agement strategies. Biochimie 2003; 84: 3 ’17.
4. Harrison's principles of internal medicine, 15th ed. Eds:Eugene Braunwald et al. 2001.
5. Knudson AGJ. Mutation and cancer: statistical study ofretinoblastoma. Proc Natl Acad Sci USA 1971; 68:820’3.
6. Cavenee WK, Dryja TP, Phillips RA, Benedict WF,Godbout R, Gallie BL, et al. Expression of recessive alle-les by chromosomal mechanisms in retinoblastoma.Nature 1983; 305: 779’84.
7. Dragani TA, Canzian F, Pierotti M. A polygenic model ofinherited predisposition to cancer. FASEB J 1996; 10:865’70.
8. Garber JE, Offit K. Hereditary cancer predisposition syn-dromes. J Clin Oncol 2005; 2: 276’92.
9. Sifri R, Gangadharappa S, Acheson LS. Identifying andtesting for hereditary susceptibility to common cancers.CA Cancer J Clin 2004; 54: 309’26.
10. Balmain A, Gray J, Ponder B. The genetics and genomicsof cancer. Nature Genetics 2003; 33: 238’44.
11. Bardelli A, Velculescu VE. Mutational analysis of genefamilies in human cancer. Curr Opin Genet Dev 2005; 15:5 ’12.
12. Gemmill RM, West JD, Boldog F, Tanaka N, Li F,Drabkin HA, et al. The hereditary renal cell carcinoma 3;8translocation fuses FHIT to a patched-related gene,TRC8. Proc Natl Acad Sci U S A 1998; 95: 9572’7.
13. Herrera L, Kakati S, Gibas L, Pietrzak E, Sandberg AA, etal. Gardner syndrome in a man with an interstitial deletionof 5q. Am J Med Genet 1986; 25: 473’6.
14. Hemminki A, Tomlinson I, Markie D, Shibata D, De laChapelle A, Aaltonen LA, et al. Localization of a suscep-tibility locus for Peutz-Jeghers syndrome to 19p usingcomparative genomic hybridization and targeted linkageanalysis. Nat Genet 1997; 15: 87’ 90.
15. Jenne DE, Reimann H, Nezu J, Muller O, Back W,Zimmer M, et al. Peutz-Jeghers syndrome is caused bymutations in a novel serine threonine kinase. Nat Genet1998; 18: 38’43.
16. Hemminki A, Markie D, Tomlinson I, Stratton MR, De laChapelle A, Aaltonen LA, et al. A serine/threonine kinasegene defective in Peutz-Jeghers syndrome. Nature 1998;391: 184’7.
17. Kainu T, Juo SH, Desper R, Heikkila P, Pyrhonen S,Nevanlinna H, et al. Somatic deletions in hereditary breastcancers implicate 13q21 as a putative novel breast can-cer susceptibility locus. Proc Natl Acad Sci U S A 2000;97: 9603’8.
18. Lander ES, Linton LM, Birren B, Nusbaum C, Zody MC,Baldwin J, et al. Initial sequencing and analysis of thehuman genome. Nature 2001; 409: 860’921.
19. Venter JC, Adams MD, Myers EW, Li PW, Mural RJ,Sutton GG, et al. The sequence of the human genome.Science 2001; 291: 1304’51.
20. Liaw D, Marsh DJ, Li J, Peacocke M, Eng C, Parsons R,et al. Germline mutations of the PTEN gene in Cowdendisease, an inherited breast and thyroid cancer syn-drome. Nat Genet 1997; 16: 64’7.
21. Rosen EM, Fan S, Ma Y. BRCA1 regulation of transcrip-tion. Cancer Letters 2005; 195: 322’32.
22. Stankov K, Pastore A, Toschi L, Volante M, Papotti M,Romeo G, et al. Allelic loss on chromosomes 2q21 and19p13.2 in Hürthle thyroid tumours. Intl J Cancer 2004;111: 463’7.
23. McKay JD, Thompson D, Lesueur F, Stankov K, RomeoG, Goldgar DE, et al. Evidence for interaction between theTCO and NMTC1 loci in familial non-medullary thyroidcancer. J Med Genet 2004; 41: 407’12.
24. Hampel H, Frankel WL, Martin E, Lockman J, ComerasI, De la Chapelle A, et al. Screening for the Lynch Syn-drome (Hereditary Nonpolyposis Colorectal Cancer). NEngl J Med 2005; 352: 1851’ 60.
25. De la Chapelle A. Microsatellite instability. N Engl J Med2003; 349: 209 ’10.
26. Macoska JA. The progressing clinical utility of DNAmicroarrays. CA Cancer J Clin 2002; 52; 50’9.
27. Gillet JP, De Longueville F, Remacle J. DualChip micro-array as a new tool in cancer research. Expert Rev MolDiagn 2006; 6: 295’306.
28. Duggan DJ, Bittner M, Chen Y, Meltzer P, Trent JM.Expression profiling using cDNA microarray. Nat Genet1999; 21: 10 ’14.
29. Tinker AV, Boussioutas A, Bowtell DDL. The challengesof gene expression microarrays for the study of humancancer. Cancer Cell 2006; 9; 333’9.
30. Ambros IM, Benard J, Boavida M, et al. Quality assess-ment of genetic markers used for therapy stratification. JClin Oncol 2003; 21: 2077’84.
31. Liu ET. Molecular oncodiagnostics: where we are andwhere we need to go. Clin Oncol 2003; 21: 2052’5.
32. Burke W. Genetic testing. N Engl J Med 2002; 347:1867’75.
390 Stankov: Diagnostics of hereditary malignancies
Received: July 15, 2006
Accepted: August 23, 2006