Embed Size (px)
Citation preview

Diagnostic Tests for Cardiovascular System

Diagnostic Tests What you need to know
• Client Teaching and Nursing Care–Explain procedure to client–Know what assessments and
interventions nursing may need to do• Allergies, Mobility, Nutrition Status
–Physically, prepare the client

DIAGNOSTIC IMAGING
• RADIOGRAPH EXAMS– Show heart size, shape, position and outline of
shadow– Show lung congestion• Heart failure: pleural effusion from L heart failure
– FLOUROSCOPY• An action picture radiograph• Allows observation of movement

Chest X-ray• 1 or 2 views (AP and Lateral)

DIAGNOSTIC IMAGING
• ANGIOGRAM– A series of radiographs taken after injection with
contrast medium– Visualizes: heart, aorta, inferior vena cava,
pulmonary artery and vein; coronary arteries– Aids in diagnosing vascular occlusions, pooling in
the heart chambers, congenital abnormalities

DIAGNOSTIC IMAGING
• ANGIOGRAM (cont.)
– Angiography/Cardiac Catheterization/ EP Study• Procedure: involves passage of a catheter through a
peripheral vessel heart chamber in order to:– Measure pressure within the heart– Measure blood volume related to cardiac competence– Valvular defects; congenital abnormalities

DIAGNOSTIC IMAGING
• Angiogram (cont.)– IV site required– Moderate sedation used, so NPO status for 6-8 hours
required.– Intravascular contrast used, all precautions apply– “Recovery Period” after sedation with frequent vital
signs– If femoral artery used- bed rest- HOB flat, head on the
pillow, movement of affected leg prohibited– Bleeding from puncture site and/or arterial clot are risks– Full day or overnight hospital stay
DIAGNOSTIC IMAGING
• Aortogram– Abdominal Aorta + major leg arteries– Viewed after contrast medium administered– Can diagnose aneurysms and other abnormalities

Computed Tomographyaka CT or CAT Scan
• X-ray that uses cross-sectional views to image tissue density differences
• May use IV contrast to view vascular structures and enhancement of tumors

CT Angiography
• 3D reconstruction of CT with contrastAsk about allergies to injectable contrast or shellfish
• Used for vascular structures including coronary arteries
Radiation exposure is considerable

Cardiac Catheterization

Cardiac Catheterization
• Right Heart Catheterization– Catheter in inserted into a central vein and
advanced until enters the Right Atrium,– Pressures are measured in the RA, RV, Pulmonary
Artery and Pulmonary Capillaries

Right-heart Catheterization

Left-heart Catheterization
• Left Heart Catheterization– Catheter is inserted into
an artery and advance until enters the Left Atrium
– Pressures are measured in the LA and LV
– A Ventriculogram is done to measure the ejection fraction

Coronary Angiography
• During a Left Heart Catheterization, the Coronary Arteries are engaged by the catheter and contrast is injected to determine blood flow through the artery

Electrophysiology Studies(EP Studies)
Maps electrical pathways and foci of abnormal heart rhythms• Multiple catheters are inserted in to different
veins and sometimes arteries to reach the chambers of the heart and induce dysrhythmias
• If the focus of the dysrhythmia is determined, it is then ablated (burned)

EP Study

Other Tests
MRI/MRA
• Soft tissue discrimination• MRI (Magnetic Resonance Imaging)– Looks at structure (Heart defects), function (EF,
contractility, relaxation), and areas of scarring in 2D in the heart using Gadolinium contrast
• MRA (Magnetic Resonance Angiography)– Looks at the lumen of arteries using GAD to reconstruct
vascular structures in 3D

Nuclear Medicine
• PET Scan– Viable cardiac tissue will have more glucose (fluorodeoxy)
uptake than scarred non-viable areas
• Thallium Imaging– Perfusion imaging agent used during exercise or
pharmacological stress testing to look for areas of decreased perfusion
• Persantine/Adenosine/Dobutamine– Pharmacological stress testing by causing vasodilatation.
Perfusion imaging agents Technetium or Thallium. Normal segments will vasodilate more than diseased areas
DIAGNOSTIC IMAGING
• ELECTROCARDIOGRAPHY– EKG, ECG– A graphic study of the electrical activity of the
heart muscleTo determine transmission of cardiac impulses through the muscle and conductive tissues

DIAGNOSTIC IMAGING
• ELECTROCARDIOGRAPHY cont.– 3 distinct waves or deflections• P Wave• QRS Complex• T Wave
– Depolarization = heart contraction– Repolarization = heart relaxation


Electrocardiography (ECG/EKG)• 12 Leads – 12 different angles of
the heart can be viewed at once for comparison
– Can be used to see• Myocardial
ischemia/infarction• Hypertrophy of the
myocardium• Dysrhythmias• Drug toxicity• Electrolyte imbalances
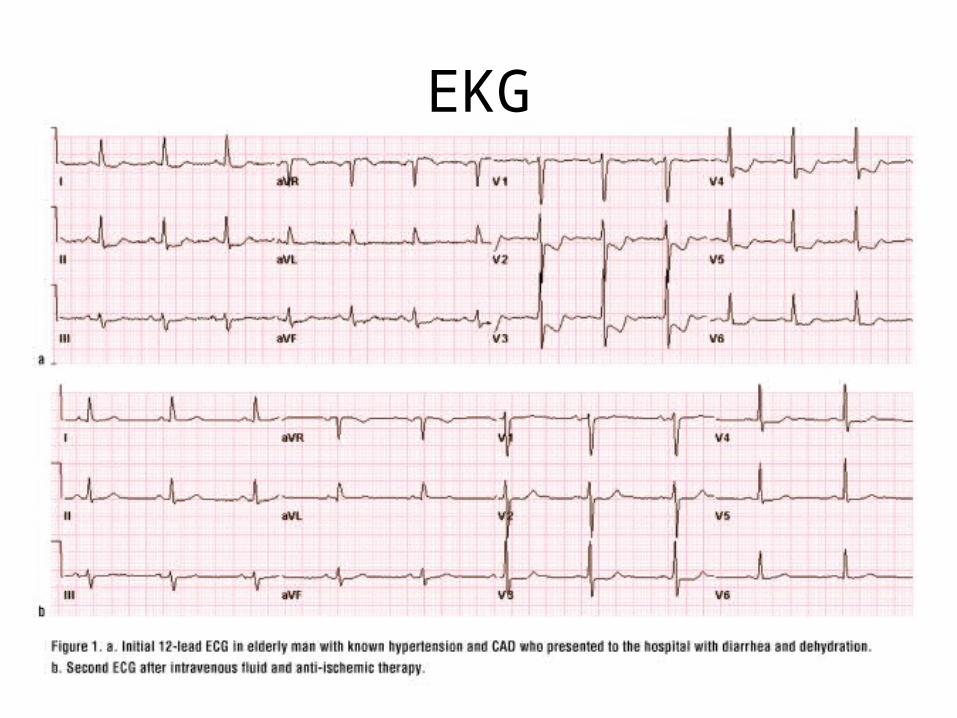
EKG

Holter Monitoring/ Event Monitoring
• A Holter Monitor is an EKG monitor worn by the patient for 24 hours to evaluate for cardiac dysrrhythmias– No Showers!– A journal is kept to match symptoms with
dysrrhythmias

Holter Monitor

Holter Monitor
• An Event Monitor may be worn for longer periods of time and has a record button for the patient to push when they feel symptomatic
• A Loop Recorder is a monitor which is surgically implanted in the patient to monitor the EKG for longer periods of time
Pacemaker Interrogation• Machine reads pacemaker
activity and pacemaker settings to ensure proper timing and strength of electrical impulses
• Also used to determine how many “shocks” an internal defibrillator has given and whether or not the “shocks” were appropriate

Echocardiography
• Transcutaneous Echocardiography– Probe is used on the skin of the anterior chest to
image the heart by ultrasound
• Transesophageal Echocardiography (TEE)– Endoscopic probe is inserted into the esophagus
and doppler is used to image the heart from the posterior angle, moderate sedation is required

Echo
http://depts.washington.edu/anesth/tips/tee_pictures/2009_03_1.gif

Echocardiography
• Echo is used to evaluate Left Ventricular function (ejection fraction*), Right Ventricular function, heart valve function, heart wall motion, pericardial sac.
*Ejection Fraction is the percentage of Left Ventricular volume the LV ejects with each contraction

Echocardiography
• Also used to:– Detect collection of blood or fluid in pericardial
sac– Cardiac chamber(s) size and contents– Septum: motion and thickness– Congenital heart disorder– Valve function

Exercise/Stress Test• Pt is asked to exercise using a treadmill or exercise
bike, OR• Pt is given a pharmacological agent to induce stress
on the heart
• EKG and possibly Transcutaneous Echo are monitored as well as vital signs and subjective data from the pt
• A positive (symptomatic) stress test will require more evaluation for heart disease

Exercise Stress Test

Ankle-Brachial Index

Understanding the ABI
The ratio of the higher brachial systolic pressure and the higher ankle systolic pressure for each
leg:
Ankle systolic pressure
Higher brachial artery systolic pressure
ABI =

http://www.nhlbi.nih.gov/health/dci/Diseases/pad/pad_diagnosis.html
ABI Procedure

Calculate the ABI
Hiatt WR. N Engl J Med. 2001;344:1608-1621; TASC Working Group. J Vasc Surg. 2000;31(1Suppl):S1-S296.
ABI Interpretation≤ 0.90 is diagnostic of peripheral arterial disease
Right Leg ABI
Right Ankle PressureHighest Arm Pressure
Highest Arm Pressure
Left Ankle Pressure
1. For the left side, divide the left ankle pressure by the highest brachial pressure and record the result.
2. Repeat the steps for the right side. 3. Record the ABIs and place the results in the medical
record.
Left Leg ABI
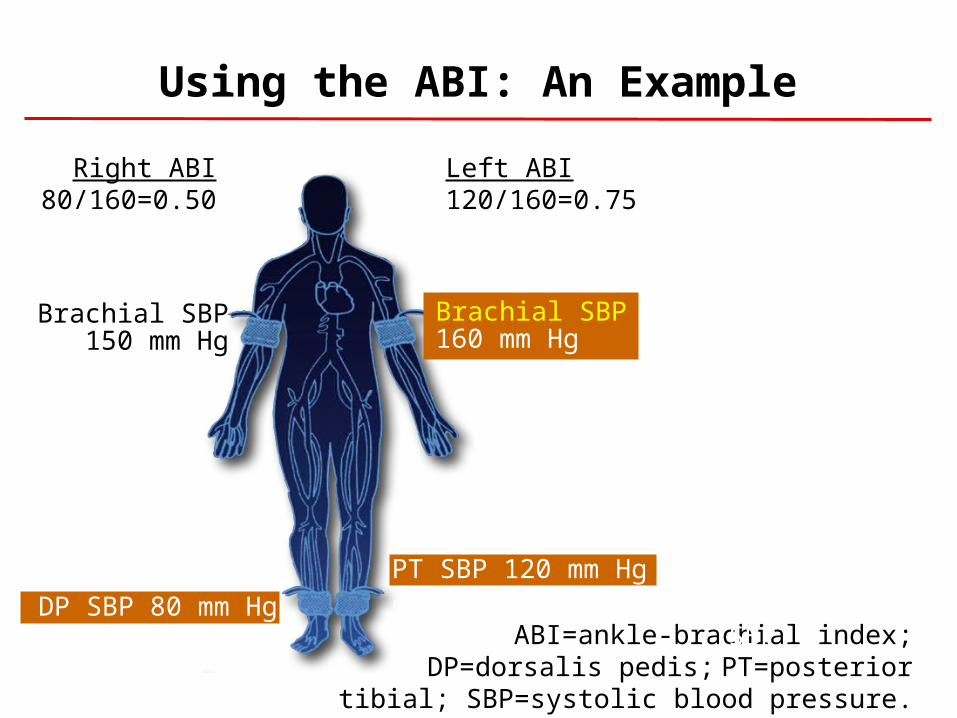
Using the ABI: An Example
ABI=ankle-brachial index; DP=dorsalis pedis; PT=posterior tibial; SBP=systolic blood pressure.
Right ABI80/160=0.50
Brachial SBP160 mm Hg
PT SBP 120 mm Hg
DP SBP 80 mm Hg
Brachial SBP150 mm Hg
PT SBP 40 mm HgDP SBP 80 mm Hg
Left ABI120/160=0.75
Highest brachial SBP
Highest of PT or DP SBP
ABI(Normal >0.90)

Interpreting the Ankle-Brachial Index
Adapted from Hirsch AT, et al. J Am Coll Cardiol. 2006;47:e1-e192. Figure 6.

Ultrasound

Bone Marrow Aspiration• Occasionally pt will take a
sedative• Pt will lay prone or on their
side • The skin over the bone to
be sampled is cleaned with antiseptic
• Local anesthetic is then injected into a small area of skin and tissues just over the bone.
• A long, large bore needle is used to aspirate samples

Bone Marrow Aspiration

Serum Tests

Serum (blood) Tests
• Cardiac Enzymes• Complete Blood Count (CBC)• Coagulation Studies• Lipids• Metabolic Panel (BMP or CMP)• Electrolytes• Miscellaneous Tests

Serum Cardiac Markers
• Proteins released into the blood in large quantities from necrotic heart muscle after an MI.
• Include Cardiac Enzymes + Troponin IImportant screening diagnostic criteria for an MI
Cardiac Enzymes
• Include:– Creatine Kinase (CK)– Creatine Phosphokinase (isoenzyme of CK) (CK-
MB)• Normal Range:– CPK or CK (Myoglobin)– Normal 26-174 units/L
– CK-MB (Creatine Kinase, myocardial muscle)– Normal < 5% of total CK– 1.3 to 8.7 units/L

Cardiac Enzymes
• Start to rise 2-3 hrs after the beginning of an MI peak in 24hrs return to nml. within 24-40 hrs– Note: CK-MB can be elevated in skeletal muscle
damage r/t surgery, trauma, or disease process

Serum Cardiac Markers
• Other: Troponin I – a myocardial muscle protein released into circulation after myocardial injury– 2 subtypes: Troponin T and Troponin I– Can identify small amts of myocardial damage

Serum Cardiac Markers
– Troponin T appears in the blood 3-5hrs after MI; may remain elevated for up to 21 days• Note: affected by skeletal muscle injury and renal disease
– Troponin I – rises 3 hrs after MI peaks at 14-18 hrs. returns to nml in 5-7 days• Not affected by skeletal muscle injury or renal disease
• Normal Range:– Troponin (Troponin I)
• Normal 0.0 to 0.5 ng/mL

Cardiac Enzymes

Complete Blood Count
• CBC or ABC (Automated Blood Count)– RBC– WBC– Hemoglobin– Hematocrit– CBC includes: • Differential of
WBC

Coagulation Studies
• PT (Prothrombin Time or Protime)• INR (International Ratio)• aPTT (Activated Partial Thromboplastin Time)• ACT (Activated Clotting Time)• Fibrinogen• Plasminogen Activator Inhibitor

Lipid Profile• Cholesterol– <200
• Triglycerides– <150
• Lipoproteins– LDL <130– HDL >40

Metabolic Panel
• Basic Metabolic Panel– Glucose– BUN (Blood Urea Nitrogen) – Creatinine– Sodium– Calcium– Potassium– CO2– Chloride– *Magnesium– *Phosphorus
Metabolic Panel
• Complete Metabolic Panel– CMP + Liver Enzymes and liver function• AST• ALT• Bilirubin• Alkaline phosphatase

Metabolic Panel
• CMP +Liver enzymes and liver function:• AST = Aspartate Aminotransferase– An enzyme found primarily in heart muscle and
liver with moderate amts, found in skeletal muscle, kidney, and pancreas
– Blood concentration is low except with cellular damage. High levels post acute MI.• Norm: Adult men = 8-46 u/L
»Women = 7-31 u/L

Metabolic Panel
• ALT = Alanine Aminotransferase– Previously known as: GPT and SGPT– Primarily a liver enzyme that also rises with
cardiac damage• Bilirubin– A substance produced in the liver, spleen and
bone marrow– A by-product of hemoglobin– Levels may rise with MI

Miscellaneous Tests
• Erythrocyte Sedimentation Rate (ESR)• Homocysteine• C-reactive Protein (CRP)• Thyroid Studies• Glucose Tolerance• Fasting Serum Insulin Level

ESR
• Erythrocyte Sedimentation Rate– Used to r/o inflammatory or infective conditions– ↑ with MI and infective endocarditis– Decreases when healing begins– Normal Range:• Males (< 50 yrs. Old) = 0-15 mm/hr• Over 50 yrs. Old = 0-20 mm/hr• Females (< 50 yrs. Old) = 0-20 mm/hr• > 50 yrs old = 0-30 mm/hr

Homocysteine
• An amino acid produced during protein digestion.
• ↑ blood levels may act as an independent risk factor for ischemic heart disease, cerebrovascular disease, peripheral arterial disease and venous thrombosis
• Promotes the progression of atherosclerosis

Homocysteine
• Also plays an important role in blood clotting.• ↑ level results in increased platelet
aggregation
C-Reactive Protein
• CRP• Produced by the liver during periods of acute
inflammation• The presence of CRP is a predictor of cardiac
events • Emerging as an independent risk factor for
CAD