Embed Size (px)
Citation preview
Jayp
ee B
rothe
rs
DiagnosticProcedures in
OPHTHALMOLOGY
Jayp
ee B
rothe
rsThird Edition
Diagnostic Procedures in
OPHTHALMOLOGY
JAYPEE BROTHERS MEDICAL PUBLISHERS (P) LTDNew Delhi • London • Philadelphia • Panama
HV Nema MSFormer Professor and Head
Department of OphthalmologyInstitute of Medical Sciences
Banaras Hindu UniversityVaranasi, Uttar Pradesh, India
Nitin Nema MS DNBProfessor
Department of OphthalmologySri Aurobindo Institute of Medical Sciences
Indore, Madhya Pradesh, India
Jayp
ee B
rothe
rs
HeadquartersJaypee Brothers Medical Publishers (P) Ltd4838/24, Ansari Road, DaryaganjNew Delhi 110 002, IndiaPhone: +91-11-43574357Fax: +91-11-43574314Email: [email protected]
Website: www.jaypeebrothers.comWebsite: www.jaypeedigital.com
© 2014, Jaypee Brothers Medical Publishers
The views and opinions expressed in this book are solely those of the original contributor(s)/author(s) and do not necessarily represent those of editor(s) of the book.
All rights reserved. No part of this publication may be reproduced, stored or transmitted in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, without the prior permission in writing of the publishers.
All brand names and product names used in this book are trade names, service marks, trademarks or registered trademarks of their respective owners. The publisher is not associated with any product or vendor mentioned in this book.
Medical knowledge and practice change constantly. This book is designed to provide accurate, authoritative information about the subject matter in question. However, readers are advised to check the most current information available on procedures included and check information from the manufacturer of each product to be administered, to verify the recommended dose, formula, method and duration of administration, adverse effects and contraindications. It is the responsibility of the practitioner to take all appropriate safety precautions. Neither the publisher nor the author(s)/editor(s) assume any liability for any injury and/or damage to persons or property arising from or related to use of material in this book.
This book is sold on the understanding that the publisher is not engaged in providing professional medical services. If such advice or services are required, the services of a competent medical professional should be sought.
Every effort has been made where necessary to contact holders of copyright to obtain permission to reproduce copyright material. If any have been inadvertently overlooked, the publisher will be pleased to make the necessary arrangements at the first opportunity.
Inquiries for bulk sales may be solicited at: [email protected]
Diagnostic Procedure in Ophthalmology
First Edition: 2002Second Edition: 2009Third Edition: 2014
ISBN: 978-93-5090-852-5
Printed at
Overseas OfficesJ.P. Medical Ltd 83 Victoria Street, LondonSW1H 0HW (UK)Phone: +44-2031708910Fax: +02-03-0086180Email: [email protected]
Jaypee Brothers Medical Publishers (P) Ltd17/1-B Babar Road, Block-B, ShaymaliMohammadpur, Dhaka-1207BangladeshMobile: +08801912003485Email: [email protected]
Jaypee-Highlights Medical Publishers Inc.City of Knowledge, Bld. 237, ClaytonPanama City, PanamaPhone: +1 507-301-0496Fax: +1 507-301-0499Email: [email protected]
Jaypee Brothers Medical Publishers (P) LtdBhotahity, KathmanduNepalPhone: +977-9741283608Email: [email protected]
Jaypee Medical Inc.The Bourse111 South Independence Mall EastSuite 835, Philadelphia, PA 19106, USAPhone: +1 267-519-9789Email: [email protected]
Jaypee Brothers Medical Publishers (P) Ltd
Jayp
ee B
rothe
rsDedicated to
Ma
Jayp
ee B
rothe
rsMohammad Javed Ali MS FRCSConsultantLV Prasad Eye InstituteHyderabad, Andhra Pradesh, India
Jorge L Alió MD PhDDirectorVissum, Institute of Ophthalmology AlicanteAlicante, Spain
Francisco Arnalich MDVissum, Institute of Ophthalmology AlicanteAlicante, Spain
Jayamuruga Pandian Arunachalam PhDReaderDepartment of GeneticsSankara NethralayaChennai, Tamil Nadu, India
Sreedharan Athmanathan MD DNBVirologist, LV Prasad Eye InstituteHyderabad, Andhra Pradesh, India
RV Azad MDChiefDr RP Center for Ophthalmic SciencesAIIMS, New Delhi, India
Shaloo Bageja MSConsultantDepartment of OphthalmologySir Ganga Ram HospitalNew Delhi, India
Mandeep S Bajaj MDProfessorDr RP Center for Ophthalmic SciencesAIIMS, New Delhi, India
Vanuli Bajpai MS FICOFellow, Sankara NethralayaChennai, Tamil Nadu, India
Contributors
Tinku Bali MSConsultantDepartment of OphthalmologySir Ganga Ram HospitalNew Delhi, India
Rituraj Baruah MSSenior RegistrarLady Hardinge Medical CollegeNew Delhi, India
Muna Bhende MSConsultantSankara NethralayaChennai, Tamil Nadu, India
Jyotirmay Biswas MS FAMSHead, Ocular Pathology and UveitisSankara NethralayaChennai, Tamil Nadu, India
Parijat Chandra MDAssociate ProfessorDr RP Center for Ophthalmic SciencesAIIMS, New Delhi, India
Shivcharan L Chandravanshi MSAssistant ProfessorMedical CollegeRewa, Madhya Pradesh, India
Nikhil S Choudhary MSConsultantLV Prasad Eye InstituteHyderabad, Andhra Pradesh, India
Taraprasad Das MSDirectorLV Prasad Eye InstituteBhubaneswar, Odisha, India
Sudha Dhandayuthapani MScDepartment of GeneticsSankara NethralayaChennai, Tamil Nadu, India
Jayp
ee B
rothe
rs
viii Diagnostic Procedures in Ophthalmology
Ronnie Jacob George MSHead, Glaucoma ServiceSankara NethralayaChennai, Tamil Nadu, India
Lingam Gopal MS FRCSChairmanMedical Research FoundationSankara NethralayaChennai, Tamil Nadu, India
AK Grover MD FRCSChairmanDepartment of OphthalmologySir Ganga Ram HospitalNew Delhi, India
Sanjiv Gupta MDConsultantDr RP Center for Ophthalmic SciencesAIIMS, New Delhi, India
Santosh Honavar MD FAMSDirectorSuper Specialty Hospital Center for SightHyderabad, Andhra Pradesh, India
Anjali Hussain MSConsultantLV Prasad Eye InstituteHyderabad, Andhra Pradesh, India
Subhadra Jalali MSHeadSmt Kanuri Santhamma Retina-Vitreous CenterLV Prasad Eye InstituteHyderabad, Andhra Pradesh, India
Navin Jayakumar MBBS DO FRCS (Ed)Honorable DirectorDarshan Eye ClinicConsultant, Vasan Eye Care HospitalsChennai, Tamil Nadu, India
Sripathi Kamath MSFellowLV Prasad Eye InstituteHyderabad, Andhra Pradesh, India
Sadao Kanagami FOPSProfessorKitasato University School of MedicineTeikyo, Japan
Sanghmitra Kanungo MD FRCSConsultantLV Prasad Eye InstituteHyderabad, Andhra Pradesh, India
R Kim DOHeadRetina-Vitreous ServiceAravind Eye Hospital and Postgraduate Institute of OphthalmologyMadurai, Tamil Nadu, India
Reesha KR MSFellowSankara NethralayaChennai, Tamil Nadu, India
S Manoj MSConsultantRetina-Vitreous ServiceAravind Eye Hospital and PostgraduateInstitute of OphthalmologyMadurai, Tamil Nadu, India
Arijit Mitra MSConsultantAravind Eye HospitalTirunelveli, Tamil Nadu, India
R Muralidhar MSConsultantPediatric OphthalmologyAravind Eye Hospital and PostgraduateInstitute of OphthalmologyMadurai, Tamil Nadu, India
Amit Nagpal MSConsultantSankara NethralayaChennai, Tamil Nadu, India
A Narayanaswamy MSResearch AssociateSingapore Eye HospitalSingapore
Rajiv Nath MSFormer ProfessorDepartment of OphthalmologyKG Medical UniversityLucknow, Uttar Pradesh, India
Jayp
ee B
rothe
rs
Contributors ix
Nitin Nema MS DNBProfessorDepartment of OphthalmologySri Aurobindo Institute of Medical SciencesIndore, Madhya Pradesh, India
Rajeeve R Pappuru MSConsultant, Retina ServiceLV Prasad Eye InstituteHyderabad, Andhra Pradesh, India
Rajul Parikh MSConsultantShreeji Eye ClinicMumbai, Maharashtra, India
Shefali Parikh MSConsultantShreeji Eye ClinicMumbai, Maharashtra, India
A Parivadhini MSConsultantSankara NethralayaChennai, Tamil Nadu, India
David Pinero ODVissumInstitute of Ophthalmology AlicanteAlicante, Spain
LS Mohan Ram D Opt BSLV Prasad Eye InstituteHyderabad, Andhra Pradesh, India
R Ramakrishnan MSChief Medical OfficerAravind Eye HospitalTirunelveli, Tamil Nadu, India
NR Rangaraj MS DODirectorPremier Eye Care and Surgical CentreChennai, Tamil Nadu, India
Manotosh Ray MD FRCSAssociate ConsultantNational University HospitalSingapore
Pukhraj Rishi MDConsultant Retina ServiceSankara NethralayaChennai, Tamil Nadu, India
Monica Saha MBBSDepartment of OphthalmologyKG Medical UniversityLucknow, Uttar Pradesh, India
Virender Sangwan MSAssociate DirectorLV Prasad Eye InstituteHyderabad, Andhra Pradesh, India
G Chandra Sekhar MS FRCSDirectorLV Prasad Eye InstituteHyderabad, Andhra Pradesh, India
Harinder Singh Sethi MS FRCSAssociate ProfessorVardhman Mahavir Medical CollegeNew Delhi, India
Jay Shah DNBLV Prasad Eye InstituteHyderabad, Andhra Pradesh, India
Pradeep Sharma MDProfessorDr RP Center for Ophthalmic SciencesAIIMS, New Delhi, India
Rajni Sharma MDAssistant ProfessorDepartment of PediatricsLady Hardinge Medical CollegeNew Delhi, India
Savitri Sharma MD FAMSHeadJhaveri Microbiological CenterLV Prasad Eye InstituteHyderabad, Andhra Pradesh, India
Tarun Sharma MD FRCSDirector, Retina ServiceSankara NethralayaChennai, Tamil Nadu, India
Yog Raj Sharma MDProfessor and HeadRetina UnitDr RP Center For Ophthalmic SciencesAIIMS, New Delhi, India
Jayp
ee B
rothe
rs
x Diagnostic Procedures in Ophthalmology
Himanshu Shekhar MDSenior RegistrarDr RP Center for Ophthalmic SciencesAIIMS, New Delhi, India
Rohit Shetty DNB FRCSVice PresidentSankara NethralayaBengaluru, Karnataka, India
Ashwin Shetty DOMS DNBSankara NethralayaBengaluru, Karnataka, India
Digvijay Singh MDDr RP Center for Ophthalmic SciencesAIIMS, New Delhi, India
Rajesh Sinha MD FRCSAssociate ProfessorDr RP Center for Ophthalmic SciencesAIIMS, New Delhi, India
Devindra Sood MSDirectorEye-Q Institute of GlaucomaNew Delhi, India
Nagasamy Soumittra MSc PhDDepartment of GeneticsSankara NethralayaChennai, Tamil Nadu, India
Sarangapani Sripriya MSc PhDDepartment of GeneticsSankara NethralayaChennai, Tamil Nadu, India
Kallakuri Sumasri B OptLV Prasad Eye InstituteHyderabad, Andhra Pradesh, India
Jeewan S Titiyal MDProfessorDr RP Center for Ophthalmic SciencesAIIMS, New Delhi, India
Garima Tyagi B OptLV Prasad Eye InstituteHyderabad, Andhra Pradesh, India
Jayesh Vazirani MSConsultantLV Prasad Eye InstituteHyderabad, Andhra Pradesh, India
Vasumathy Vedantham MS DNB FRCSConsultantRetina-Vitreous ServiceAravind Eye Hospital and PostgraduateInstitute of OphthalmologyMadurai, Tamil Nadu, India
Arulmozi Verman MSDirectorUma Eye ClinicChennai, Tamil Nadu, India
L Vijaya MSConsultantSingapore Eye HospitalSingapore
P Vijayalakshami MSHead, Pediatic OphthalmologyAravind Eye Hospital and PostgraduateInstitute of OphthalmologyMadurai, Tamil Nadu, India
P Vrushali DNBAravind Eye Hospital and PostgraduateInstitute of OphthalmologyMadurai, Tamil Nadu, India
Jayp
ee B
rothe
rsThe second edition of the Diagnostic Procedures in Ophthalmology was well-received by readers and was also translated in Spanish for the benefit of readers in the Spanish speaking countries. The third edition of the book is further expanded by adding eight more chapters and like its earlier two editions, is a rich source of material on routine and advanced diagnostic investigations and procedures for the accurate and speedy diagnosis of eye diseases.
The routine tests required for examination of the ophthalmic patients include recording of visual acuity, color vision and color defects, slit-lamp examination, tonometry, gonioscopy, optic disc assessment, ophthalmoscopy, and perimetry. In the present edition, the chapter on perimetry is updated and both Octopus and Humphrey perimetry are described.
Fundus fluorescence angiography and Indocyanine green angiography are invaluable tools in the diagnosis, documentation and follow-up of chorioretinal disorders. Both types of angiography help in monitoring treatment of the macular diseases. A-scan and B-scan ultrasonography are well-established and essential procedures. A-scan is largely used for biometry and supplementing findings of B-scan. Three-dimensional ultrasound tomography has improved visualization of the posterior segment pathology. It can measure the volume, surface and boundaries of the intraocular tumors. Ultrasound biomicroscopy (UBM) can imagine the anatomy and pathology of the anterior segment of the eye both qualitatively and quantitatively. The images are helpful in understanding the mechanism of different types of glaucoma and identifying lesions of the ciliary body.
Confocal microscopy is an advanced imaging technology that facilitates examination of microstructure of the cornea for identifying diseases like keratoconus, corneal dystrophies and corneal degeneration. Corneal topography is a useful tool for the diagnosis of corneal curvature pathologies. However, it is more often applied in planning appropriate refractive surgery.
Separate chapters have been devoted for the diagnosis of infective keratitis, uveitis, retinopathy of prematurity, localization of intraocular foreign body, concomitant and incomitant strabismus, dry eye disease, epiphora and proptosis.
Like other branches of medicine, ophthalmology is an ever-expanding discipline. With inroads of technology, new diagnostic tools have been introduced in the ophthalmology. New chapters based on recent development include Imaging in Glaucoma, Spectrum Domain Optical Coherence Topography, Anterior Segment Optic Coherence Topography, Pentacam, and IOL Power Calculation. Additionally, Diagnostic Procedures for Genetically Transmitted Eye Diseases, Diagnostic Modalities of Intraocular Malignancies, Ptosis Evaluation, and Ocular Motor Nerve Palsies have been included.
Optic coherence tomography (OCT) has emerged to the forefront of ocular imaging as it can measure the thickness of retina, RNFL, optic cup depth and can produce the maps of internal limiting membrane and retinal pigment epithelium. It has significant utility in the diagnosis of glaucoma and retinal diseases. Earlier, time domain OCT was used in ophthalmic clinics. It is now being replaced by the Spectrum domain OCT because it provides a superior image quality with larger field and reduced motion artifacts, faster acquisition of images and higher detection rate of ocular disorders.
Pentacam and anterior segment optical coherence tomography (ASOCT) are used for imaging of cornea and anterior chamber. Pentacam can produce anterior and posterior corneal curvature maps and diagnose forme fruste keratoconus. It measures corneal power and thus guides in refractive surgery. It can assess grades of cataract and IOL power and facilitates refractive cataract surgery.
Anterior segment optical coherence tomography (ASOCT) is a relatively new modality to directly visualize cornea, anterior chamber and measures anterior chamber depth, angle width, and can imagine scleral spur, ciliary body, ciliary sulcus and canal of Schlemm. Application of ASOCT has improved the results of refractive surgery, phakic IOL implantation, and glaucoma surgery.
With the completion of Human Genome Project in 2003, data, devices and molecular techniques have progressed remarkably. It has been reported that out of 4,000 genetic disorders, about one-third are ocular diseases. Cytogenetics provides the broad overview of genetic landscapes. It detects abnormalities in the number, and structure of chromosomes. Several methods for detection of mutation of genes are comprehensively described in the chapter on Diagnostic Procedures for Genetically Transmitted Eye Diseases. Early diagnosis of gene defect is likely to open possibilities of the gene therapy in some ophthalmic disorders.
Three chapters—Electrophysiological Tests for Visual Function Assessment, Pupil and Ocular Nerve Palsies included in this edition of the book are likely to assist readers in the diagnosis of neuro-ophthalmic problems. Electrophysiological tests can assess the functional integrity of visual pathway. They not only help in detecting the cause of visual loss but also the site
Preface to the Third Edition
Jayp
ee B
rothe
rs
xii Diagnostic Procedures in Ophthalmology
of the lesion. A detailed chapter has been devoted to cover the EOG, ERG, Pattern ERG, Multifocal ERG, VEP and Multifocal VEP, and their utility in the diagnosis of neurological and retinal disorders and drug toxicity. Similarly, testing of ocular motor nerves may localize lesions of the central nervous system. Proper examination of pupil and its reflexes cannot be overemphasized as they reveal a wealth of information on the diseases of the nervous system.
Newer investigative procedures in ophthalmology have revolutionized the diagnosis of the eye diseases. The early diagnosis is a key to early treatment, better prognosis and ultimate improved quality of the life of the eye patients. We hope that residents and ophthalmic practitioners will continue to find the 3rd edition of the book more useful in the investigations of eye patients in their clinical practices.
HV NemaNitin Nema
Jayp
ee B
rothe
rsThe word diagnosis comes from the Greek word diagignoskein meaning to distinguish or discern. Besides history and clinical examination of the patient, diagnostic tests are required to aid in making correct diagnosis of eye diseases. The role of diagnostic technology is not inferior to that of a clinician’s acumen. A correct diagnostic report helps in differentiating functional from organic and idiopathic from non-idiopathic diseases. The number of diagnostic tests available to an ophthalmologist has increased significantly in the last two decades. Both selective and non-selective tests are presently used for the clinical and research purposes. Non-selective approach to testing is costly and does not provide useful information. In order to be useful, diagnostic tests have to be properly performed, accurately read, and correctly interpreted. The ordering oculist should always compare the results of test with the clinical features of the eye disease. The main aim of the book—Diagnostic Procedures in Ophthalmology is to provide useful information on diagnostic tests, which an ophthalmologist intends to perform or order during his clinical practice. Some of the procedures described in the book, assessment of visual acuity, slit-lamp examination, tonometry, gonioscopy, perimetry, and ophthalmoscopy, are routine examinations. However, the technique of proper examination and interpretation of findings to arrive at a correct diagnosis must be known to the practicing ophthalmologist or optometrist. Procedures such as ophthalmic photography, evaluation of optic nerve head, fundus fluorescein angiography, and indocyanine green angiography are invaluable because they not only help in the diagnosis and documentation but also help in monitoring the management of eye disease. Corneal topography gives useful data about corneal surface and curvature and contributes to the success of Lasik surgery to a great extent. The role of A-scan ultrasonography in the measurement of axial length of the eye and biometry cannot be overemphasized. B-scan ultrasonography is needed to explore the posterior segment of the eye when media are opaque or an orbital mass is suspected. Ultrasound biomicroscopy (UBM) and optical coherence tomography (OCT) are relatively new noninvasive tools to screen the eye at the microscopic level. UBM helps in understanding the pathogenesis of various forms of glaucoma and their management. OCT obtains a tomograph of the retina showing its microstructure incredibly similar to a histological section. It helps in the diagnosis and management of the macular and retinal diseases. Electrophysiological tests allow objective evaluation of visual system. They are used in determination of visual acuity in infants and in the diagnosis of the macular and optic nerve disorders. What diagnostic tests should be ordered in the evaluation of the patients with infective keratitis or uveitis? Chapters on Diagnostic Procedures in Infective Keratitis and Diagnostic Procedures in Uveitis provide an answer. The experts who have credibility in their fields have contributed chapters to the book. Not only the procedures of diagnostic tests are described but to make the reader conversant, characteristic findings in the normal and the diseased eye are also highlighted with the help of illustrations. The book should be of great help to the practicing ophthalmologists, resident ophthal mologists, optometrists and technicians as it provides instant access to the diagnostic procedures in ophthalmology. We are indebted to all contributors for their excellent contributions in short time in spite of their busy schedule. Mr JP Vij deserves our sincere thanks for nice publication of the book.
HV Nema Nitin Nema
Preface to the First Edition
Jayp
ee B
rothe
rsWe would like to record our grateful thanks to all contributing authors of the book for sparing valuable time from their busy schedule to write the chapters for the book. Dr Savitri Sharma, Dr Devindra Sood and Dr J Biswas have updated their earlier chapters.
Our special appreciation goes to Dr R Ramakrisnan, Dr P Vijayalakshmi, Dr Rajul Parikh, Dr S Honavar, Dr Jayamuruga Pandian and Dr Rajeev Pappuru for submitting their write-up on a short notice and enabling us to maintain the schedule of publication.
Shri Jitendar P Vij (Group Chairman), Mr Ankit Vij (Managing Director) and Mr Tarun Duneja (Director Publishing) of M/s Jaypee Brothers Medical Publishers (P) Ltd, New Delhi, India, deserve our sincere thanks for their cooperation and meticulous publication of the third edition of the Diagnostic Procedures in Ophthalmology.
Acknowledgments
Jayp
ee B
rothe
rs
Contents
1. ASSESSMENT OF VISUAL ACUITY 1 Nitin Nema
History 1Principle 1Recording of distant visual acuity 2Bailey-Lovie chart 2Normal vision 3Near visual acuity 4Factors affecting visual acuity 4Visual acuity assessment in infants and children 7Procedure for testing visual acuity 9Near vision in children 10
2. COLOR VISION AND COLOR BLINDNESS 11 Harinder Singh Sethi
Color vision 11Factors affecting color vision 11Illumination 12Theories of color vision 12Anatomy of color vision 13Anomalies of color vision 14Color vision testing 16Other tests 23
3. SLIT-LAMP EXAMINATION 26Arulmozhi Verman
History of slit-lamp development 26Types of illumination used in slit–lamp examination 27Gonioscopy 34
4. CORNEAL TOPOGRAPHY 38Francisco Arnalich, David Piñero, Jorge L Alió
History of corneal measurement 38Shape of the normal cornea 39Fundamentals and technological approaches to corneal topography 40How to interpret a corneal topography map 42A good topography examination 45Quantitative descriptors of corneal topography: corneal indexes 46Corneal aberrometry: fundamentals and clinical applications 48Clinical uses of corneal topography 51
Jayp
ee B
rothe
rs
xviii Diagnostic Procedures in Ophthalmology
5. CORNEAL CONFOCAL MICROSCOPY 60Manotosh Ray
Optics 60Confocal microscopy in corneal pathologies 63
6. TONOMETRY 69Shefali Parikh, Rajul Parikh
What is intraocular pressure? 69
7. GONIOSCOPY 77Ronnie Jacob George, A Parivadhini, A Narayanaswamy, L Vijaya
Optical principles 77
8. OPTIC DISC ASSESSMENT IN GLAUCOMA 87Nikhil S Choudhari, G Chandra Sekhar
Methods of optic disc examination 87Features of glaucomatous disc damage 87
9. PERIMETRY 96Devindra Sood, NR Rangaraj
Evolution of octopus perimeter 96Basic terminologies in perimetry 98Measurement strategies 99Humphrey visual field analyzer 102Humphrey field analyzer 109
10. IMAGING IN GLAUCOMA 118Rajul Parikh, Shefali Parikh
Heidelberg retinal tomogram (HRT II/HRT III) 118Scanning laser polarimetry 123Optical coherence tomography 124
11. OPHTHALMOSCOPY 129Pukhraj Rishi, Tarun Sharma
Principles of ophthalmoscopy 129Indirect ophthalmoscopy 129Head mounted binocular indirect ophthalmoscopy 130Monocular indirect ophthalmoscopy 134Modified monocular indirect ophthalmoscopy 135Penlight ophthalmoscopy 136Direct ophthalmoscopy 136Hruby lens direct ophthalmoscopy 137Wide angle viewing system 137
12. OPHTHALMIC PHOTOGRAPHY 140Sadao Kanagami
35-mm camera 140Fundus camera 140Photo slit-lamp (Kowa attachment) 142Photography in operating theater 143
Jayp
ee B
rothe
rs
Contents xix
Specular microscopy 143Imaging system 143Photography of face and skin 145Photography of pupil 145External photography 146Optical system of fundus camera 147Fundus photography 147Fluorescein angiography 148Monochromatic fundus photography 150Photo slit-lamp biomicrography of anterior segment 151
13. FLUORESCEIN ANGIOGRAPHY 152R Kim, S Manoj
History 152Basic principles 152Properties of sodium fluorescein 152Technique and equipment 153Digital angiography 153Procedure for fundus fluorescein angiography 154Stereophotography 155Side effects and complications 155Basic anatomic considerations 156Normal fundus fluorescein angiography 156Abnormal fluorescence angiography 158Iris fluorescein angiography 165
14. INDOC YANINE GREEN ANGIOGRAPHY 167Vasumathy Vedantham
Indocyanine green angiography vs fluorescein angiography 167Indocyanine green 167
15. A-SCAN ULTRASONOGRAPHY 179Rajiv Nath, Tinku Bali, Monica Saha
History 179Physics of ultrasound 179Instrumentation 180Vector A-scan display 181Basic screening examination 181A-scan in common ocular pathologies 184Biometry 189Biometry in ocular pathologies 191Limitations and pitfalls of A-scan 191
16. B-SCAN ULTRASONOGRAPHY 195Taraprasad Das, Vasumathy Vedantham, Anjali Hussain, Sanghamitra Kanungo, LS Mohan Ram
Physics and basic technology 195Ultrasound unit 195Screening techniques 196Structural anomalies 207Immersion B-scan 208
Jayp
ee B
rothe
rs
xx Diagnostic Procedures in Ophthalmology
17. ULTRASOUND BIOMICROSCOPY 211Muna Bhende, Vanuli Bajpai
Basic physics 211Instrumentation 211Technique 211
18. ELECTROPHYSIOLOGICAL TESTS FOR VISUAL FUNCTION ASSESSMENT 218Subhadra Jalali, LS Mohan Ram, Garima Tyagi, Kallakuri Sumasri
Visual electrophysiology tests 218Electro-oculogram 219Electroretinogram 221
19. PENTACAM 251Rohit Shetty, Ashwin Shetty
Output 252Topography 253
20. ANTERIOR SEGMENT OPTICAL COHERENCE TOMOGRAPHY 263R Ramakrishnan, Arijit Mitra
Principle of optical coherence tomography 263Measurement tools 265
21. SPECTRAL DOMAIN OPTICAL COHERENCE TOMOGRAPHY 280Sripathi Kamath, Rajeev R Pappuru
Spectral domain optical coherence tomography vIz time domain optical coherence tomography 289
22. INTRAOCULAR LENS POWER CALCULATION 291Himanshu Shekhar, Rajesh Sinha, Jeewan S Titiyal
Intraocular lens power formulas 291Optical biometry 295Intraocular lens power calculation in special situations 296
23. DIAGNOSTIC PROCEDURES IN INFECTIOUS KERATITIS 299Savitri Sharma, Sreedharan Athmanathan
Corneal confocal microscopy 299Molecular methods 308Protocol for viral keratitis 308
24. DIAGNOSTIC PROCEDURES IN UVEITIS 314Jyotirmay Biswas, Reesha KR
Anterior chamber paracentesis 314Vitreous tap and diagnostic vitrectomy 316Vitrectomy 317Handling and testing of aqueous and vitreous specimen 317
25. RETINOPATHY OF PREMATURITY: DIAGNOSTIC PROCEDURES 321Yog Raj Sharma, Parijat Chandra, Rajni Sharma, Raj Vardhan Azad
Etiology 321
Jayp
ee B
rothe
rs
Contents xxi
International classification of retinopathy of prematurity 321Fluorescein angiography 324Ultrasound biomicroscopy 325Ultrasonography 326
26. LOCALIZATION OF INTRAOCULAR FOREIGN BODY 328Amit Nagpal, Lingam Gopal
Types of intraocular foreign bodies 328Ultrasound biomicroscopy 330
27. CONCOMITANT STRABISMUS: DIAGNOSTIC METHODS 333Digvijay Singh, Harinder Singh Sethi, Pradeep Sharma
Diagnostic method 333Qualitative tests 334Quantitative tests 335
28. INCOMITANT STRABISMUS: DIAGNOSTIC PROCEDURES 343P Vijayalakshmi, P Vrushali, R Muralidhar
Paralytic strabismus 343Restrictive strabismus 355
29. DIAGNOSTIC PROCEDURES IN DRY EYE DISEASE 360Jayesh Vazirani, Virender Sangwan
Definition 360Dry eye diagnosis 360Slit-lamp examination 360
39. EVALUATION OF EPIPHORA 364AK Grover, Rituraj Baruah, Shaloo Bageja
Applied anatomy and physiology of the lacrimal apparatus 364Tear secretion and elimination 366Evaluation of epiphora 366
31. DIAGNOSTIC TECHNIQUES IN PROPTOSIS 376Mandeep S Bajaj, Sanjiv Gupta
Diagnostic techniques 377Imaging techniques 377Blood tests 383Biopsy techniques 384Pathology techniques 385Additional investigations 386
32. DIAGNOSTIC PROCEDURES FOR GENETICALLY TRANSMITTED EYE DISEASES 388Sudha Dhandayuthapani, Sarangapani Sripriya, Nagasamy Soumittra, Jayamuruga Pandian Arunachalam
DNA-based gene screening (or) molecular diagnostics 388Chromosomal study/cytogenetics 396Genetic counseling 399Quality management in a genetic laboratory 401Safety in a genetic laboratory 401
Jayp
ee B
rothe
rs
xxii Diagnostic Procedures in Ophthalmology
33. DIAGNOSTIC MODALITIES IN INTRAOCULAR MALIGNANCIES 404Mohammad Javed Ali, Sneha Jay Shah, Santosh G Honavar
Ultrasonography 404Fundus fluorescein and indocyanine green angiography 406Computed tomography 407Magnetic resonance imaging 409Fine needle aspiration biopsy/cytology (FNAB/FNAC) 410
34. PUPIL 413Navin Jayakumar
Functional anatomy and physiology of the pupil reflexes 413Principles and techniques of pupil examination 416Disorders of pupil function 423
35. PTOSIS EVALUATION 432AK Grover, Shaloo Bageja
Classification 432Clinical evaluation 432Laboratory studies 438
36. OCULAR MOTOR NERVE PALSIES 440Shivcharan L Chandravanshi, Nitin Nema
Oculomotor nerve palsy 440Trochlear nerve palsy 443Abducens nerve palsy 446
Index 451
Jayp
ee B
rothe
rsINTRODUCTION
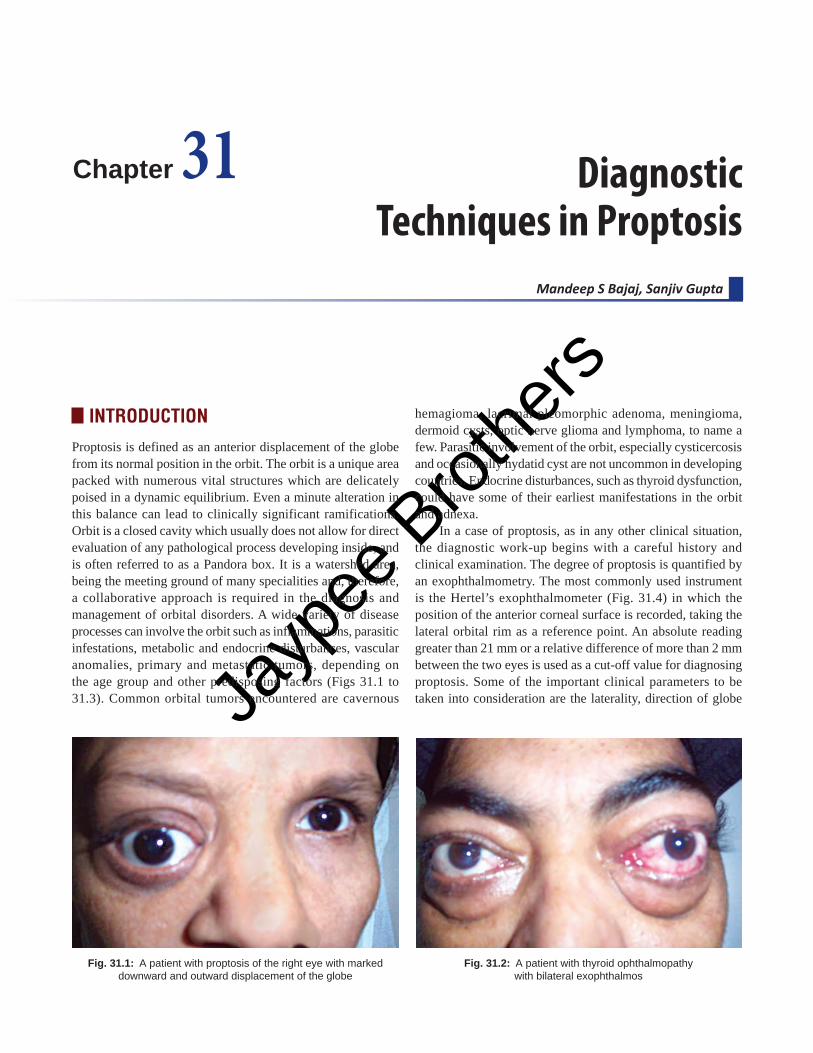
Proptosis is defined as an anterior displacement of the globe from its normal position in the orbit. The orbit is a unique area packed with numerous vital structures which are delicately poised in a dynamic equilibrium. Even a minute alteration in this balance can lead to clinically significant ramifications. Orbit is a closed cavity which usually does not allow for direct evaluation of any pathological process developing inside, and is often referred to as a Pandora box. It is a watershed area, being the meeting ground of many specialities and, therefore, a collaborative approach is required in the diagnosis and management of orbital disorders. A wide variety of disease processes can involve the orbit such as inflammations, parasitic infestations, metabolic and endocrine disturbances, vascular anomalies, primary and metastatic tumors, depending on the age group and other predisposing factors (Figs 31.1 to 31.3). Common orbital tumors encountered are cavernous
Mandeep S Bajaj, Sanjiv Gupta
Diagnostic Techniques in Proptosis
Chapter 31
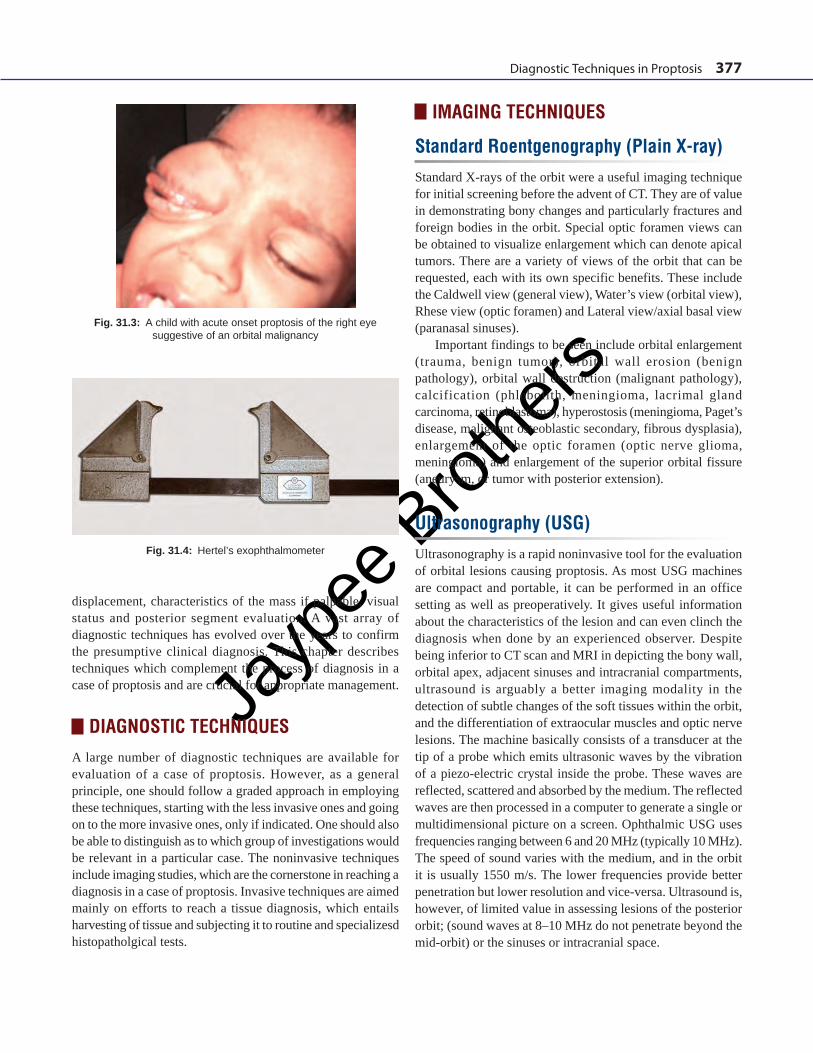
Fig. 31.2: A patient with thyroid ophthalmopathy with bilateral exophthalmos
Fig. 31.1: A patient with proptosis of the right eye with marked downward and outward displacement of the globe
hemagioma, lacrimal pleomorphic adenoma, meningioma, dermoid cysts, optic nerve glioma and lymphoma, to name a few. Parasitic involvement of the orbit, especially cysticercosis and occasionally hydatid cyst are not uncommon in developing countries. Endocrine disturbances, such as thyroid dysfunction, could have some of their earliest manifestations in the orbit and adnexa.
In a case of proptosis, as in any other clinical situation, the diagnostic work-up begins with a careful history and clinical examination. The degree of proptosis is quantified by an exophthalmometry. The most commonly used instrument is the Hertel’s exophthalmometer (Fig. 31.4) in which the position of the anterior corneal surface is recorded, taking the lateral orbital rim as a reference point. An absolute reading greater than 21 mm or a relative difference of more than 2 mm between the two eyes is used as a cut-off value for diagnosing proptosis. Some of the important clinical parameters to be taken into consideration are the laterality, direction of globe
Jayp
ee B
rothe
rs
Diagnostic Techniques in Proptosis 377
displacement, characteristics of the mass if palpable, visual status and posterior segment evaluation. A vast array of diagnostic techniques has evolved over the years to confirm the presumptive clinical diagnosis. This chapter describes techniques which complement the process of diagnosis in a case of proptosis and are crucial for appropriate management.
DIAGNOSTIC TECHNIQUESA large number of diagnostic techniques are available for evaluation of a case of proptosis. However, as a general principle, one should follow a graded approach in employing these techniques, starting with the less invasive ones and going on to the more invasive ones, only if indicated. One should also be able to distinguish as to which group of investigations would be relevant in a particular case. The noninvasive techniques include imaging studies, which are the cornerstone in reaching a diagnosis in a case of proptosis. Invasive techniques are aimed mainly on efforts to reach a tissue diagnosis, which entails harvesting of tissue and subjecting it to routine and specializesd histopatholgical tests.
IMAGING TECHNIQUES
Standard Roentgenography (Plain X-ray)Standard X-rays of the orbit were a useful imaging technique for initial screening before the advent of CT. They are of value in demonstrating bony changes and particularly fractures and foreign bodies in the orbit. Special optic foramen views can be obtained to visualize enlargement which can denote apical tumors. There are a variety of views of the orbit that can be requested, each with its own specific benefits. These include the Caldwell view (general view), Water’s view (orbital view), Rhese view (optic foramen) and Lateral view/axial basal view (paranasal sinuses).
Important findings to be seen include orbital enlargement (trauma, benign tumor), orbital wall erosion (benign pathology), orbital wall destruction (malignant pathology), calcification (phlebolith, meningioma, lacrimal gland carcinoma, retinoblastoma), hyperostosis (meningioma, Paget’s disease, malignant osteoblastic secondary, fibrous dysplasia), enlargement of the optic foramen (optic nerve glioma, meningioma) and enlargement of the superior orbital fissure (aneurysm, or tumor with posterior extension).
Ultrasonography (USG)Ultrasonography is a rapid noninvasive tool for the evaluation of orbital lesions causing proptosis. As most USG machines are compact and portable, it can be performed in an office setting as well as preoperatively. It gives useful information about the characteristics of the lesion and can even clinch the diagnosis when done by an experienced observer. Despite being inferior to CT scan and MRI in depicting the bony wall, orbital apex, adjacent sinuses and intracranial compartments, ultrasound is arguably a better imaging modality in the detection of subtle changes of the soft tissues within the orbit, and the differentiation of extraocular muscles and optic nerve lesions. The machine basically consists of a transducer at the tip of a probe which emits ultrasonic waves by the vibration of a piezo-electric crystal inside the probe. These waves are reflected, scattered and absorbed by the medium. The reflected waves are then processed in a computer to generate a single or multidimensional picture on a screen. Ophthalmic USG uses frequencies ranging between 6 and 20 MHz (typically 10 MHz). The speed of sound varies with the medium, and in the orbit it is usually 1550 m/s. The lower frequencies provide better penetration but lower resolution and vice-versa. Ultrasound is, however, of limited value in assessing lesions of the posterior orbit; (sound waves at 8–10 MHz do not penetrate beyond the mid-orbit) or the sinuses or intracranial space.
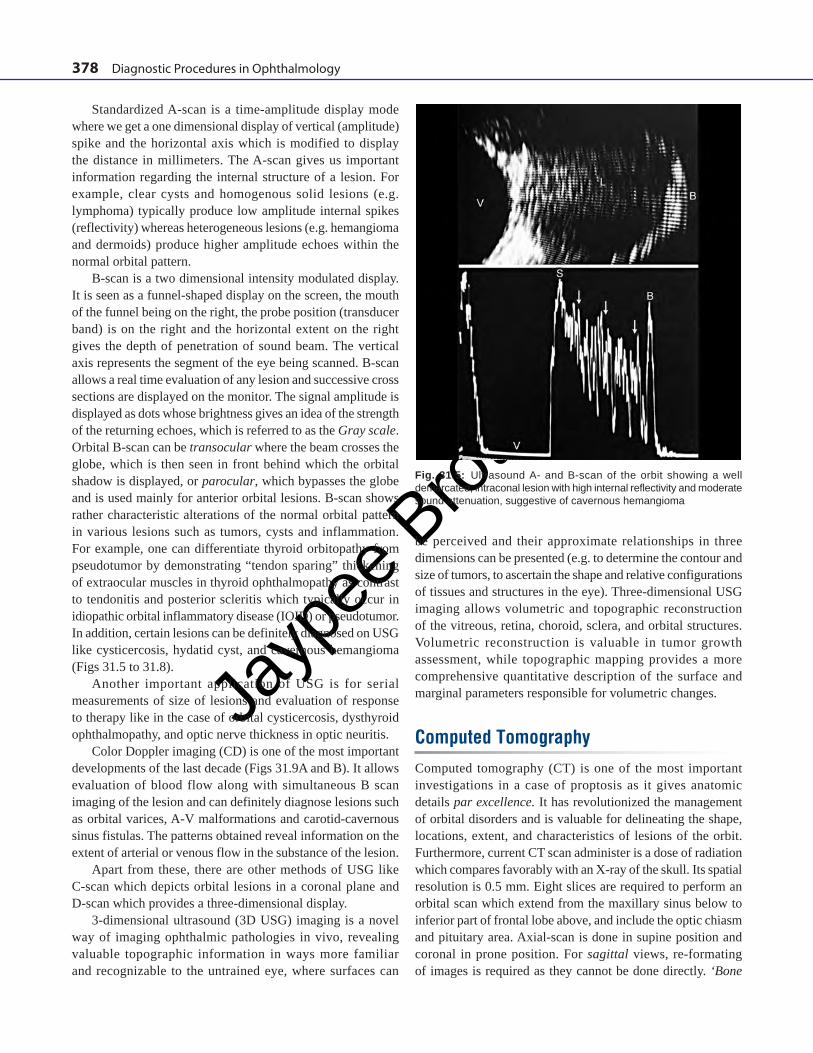
Fig. 31.3: A child with acute onset proptosis of the right eye suggestive of an orbital malignancy
Fig. 31.4: Hertel’s exophthalmometer
Jayp
ee B
rothe
rs
378 Diagnostic Procedures in Ophthalmology
Standardized A-scan is a time-amplitude display mode where we get a one dimensional display of vertical (amplitude) spike and the horizontal axis which is modified to display the distance in millimeters. The A-scan gives us important information regarding the internal structure of a lesion. For example, clear cysts and homogenous solid lesions (e.g. lymphoma) typically produce low amplitude internal spikes (reflectivity) whereas heterogeneous lesions (e.g. hemangioma and dermoids) produce higher amplitude echoes within the normal orbital pattern.
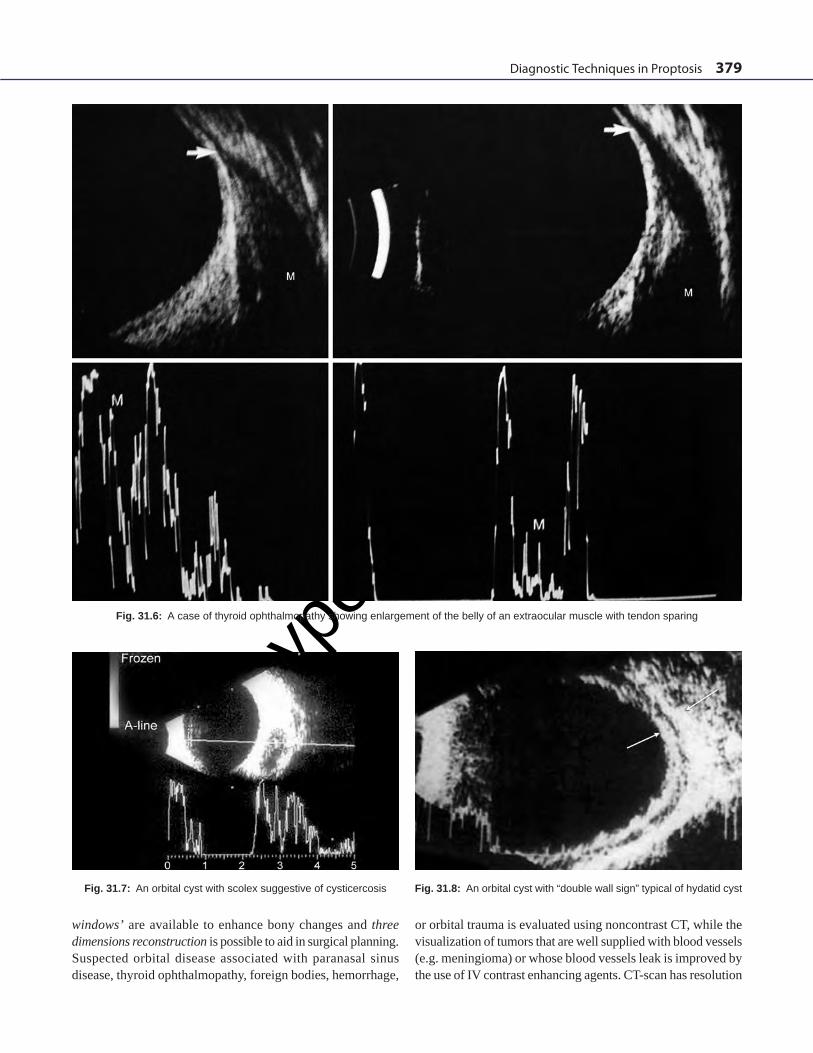
B-scan is a two dimensional intensity modulated display. It is seen as a funnel-shaped display on the screen, the mouth of the funnel being on the right, the probe position (transducer band) is on the right and the horizontal extent on the right gives the depth of penetration of sound beam. The vertical axis represents the segment of the eye being scanned. B-scan allows a real time evaluation of any lesion and successive cross sections are displayed on the monitor. The signal amplitude is displayed as dots whose brightness gives an idea of the strength of the returning echoes, which is referred to as the Gray scale. Orbital B-scan can be transocular where the beam crosses the globe, which is then seen in front behind which the orbital shadow is displayed, or parocular, which bypasses the globe and is used mainly for anterior orbital lesions. B-scan shows rather characteristic alterations of the normal orbital pattern in various lesions such as tumors, cysts and inflammation. For example, one can differentiate thyroid orbitopathy from pseudotumor by demonstrating “tendon sparing” thickening of extraocular muscles in thyroid ophthalmopathy as contrast to tendonitis and posterior scleritis which typically occur in idiopathic orbital inflammatory disease (IOID) or pseudotumor. In addition, certain lesions can be definitely diagnosed on USG like cysticercosis, hydatid cyst, and cavernous hemangioma (Figs 31.5 to 31.8).
Another important application of USG is for serial measurements of size of lesions and evaluation of response to therapy like in the case of orbital cysticercosis, dysthyroid ophthalmopathy, and optic nerve thickness in optic neuritis.
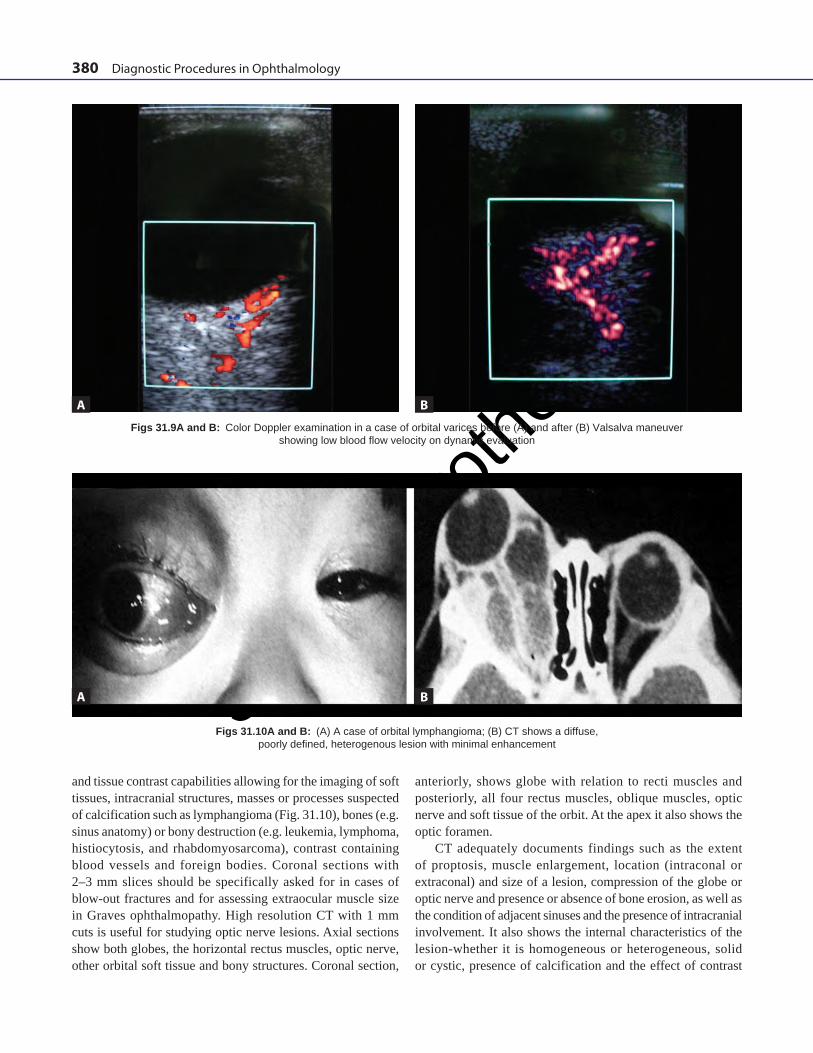
Color Doppler imaging (CD) is one of the most important developments of the last decade (Figs 31.9A and B). It allows evaluation of blood flow along with simultaneous B scan imaging of the lesion and can definitely diagnose lesions such as orbital varices, A-V malformations and carotid-cavernous sinus fistulas. The patterns obtained reveal information on the extent of arterial or venous flow in the substance of the lesion.
Apart from these, there are other methods of USG like C-scan which depicts orbital lesions in a coronal plane and D-scan which provides a three-dimensional display.
3-dimensional ultrasound (3D USG) imaging is a novel way of imaging ophthalmic pathologies in vivo, revealing valuable topographic information in ways more familiar and recognizable to the untrained eye, where surfaces can
be perceived and their approximate relationships in three dimensions can be presented (e.g. to determine the contour and size of tumors, to ascertain the shape and relative configurations of tissues and structures in the eye). Three-dimensional USG imaging allows volumetric and topographic reconstruction of the vitreous, retina, choroid, sclera, and orbital structures. Volumetric reconstruction is valuable in tumor growth assessment, while topographic mapping provides a more comprehensive quantitative description of the surface and marginal parameters responsible for volumetric changes.
Computed Tomography Computed tomography (CT) is one of the most important investigations in a case of proptosis as it gives anatomic details par excellence. It has revolutionized the management of orbital disorders and is valuable for delineating the shape, locations, extent, and characteristics of lesions of the orbit. Furthermore, current CT scan administer is a dose of radiation which compares favorably with an X-ray of the skull. Its spatial resolution is 0.5 mm. Eight slices are required to perform an orbital scan which extend from the maxillary sinus below to inferior part of frontal lobe above, and include the optic chiasm and pituitary area. Axial-scan is done in supine position and coronal in prone position. For sagittal views, re-formating of images is required as they cannot be done directly. ‘Bone
Fig. 31.5: Ultrasound A- and B-scan of the orbit showing a well demarcated, intraconal lesion with high internal reflectivity and moderate sound attenuation, suggestive of cavernous hemangioma
Jayp
ee B
rothe
rs
Diagnostic Techniques in Proptosis 379
Fig. 31.6: A case of thyroid ophthalmopathy showing enlargement of the belly of an extraocular muscle with tendon sparing
Fig. 31.7: An orbital cyst with scolex suggestive of cysticercosis Fig. 31.8: An orbital cyst with “double wall sign” typical of hydatid cyst
windows’ are available to enhance bony changes and three dimensions reconstruction is possible to aid in surgical planning. Suspected orbital disease associated with paranasal sinus disease, thyroid ophthalmopathy, foreign bodies, hemorrhage,
or orbital trauma is evaluated using noncontrast CT, while the visualization of tumors that are well supplied with blood vessels (e.g. meningioma) or whose blood vessels leak is improved by the use of IV contrast enhancing agents. CT-scan has resolution
Jayp
ee B
rothe
rs
380 Diagnostic Procedures in Ophthalmology
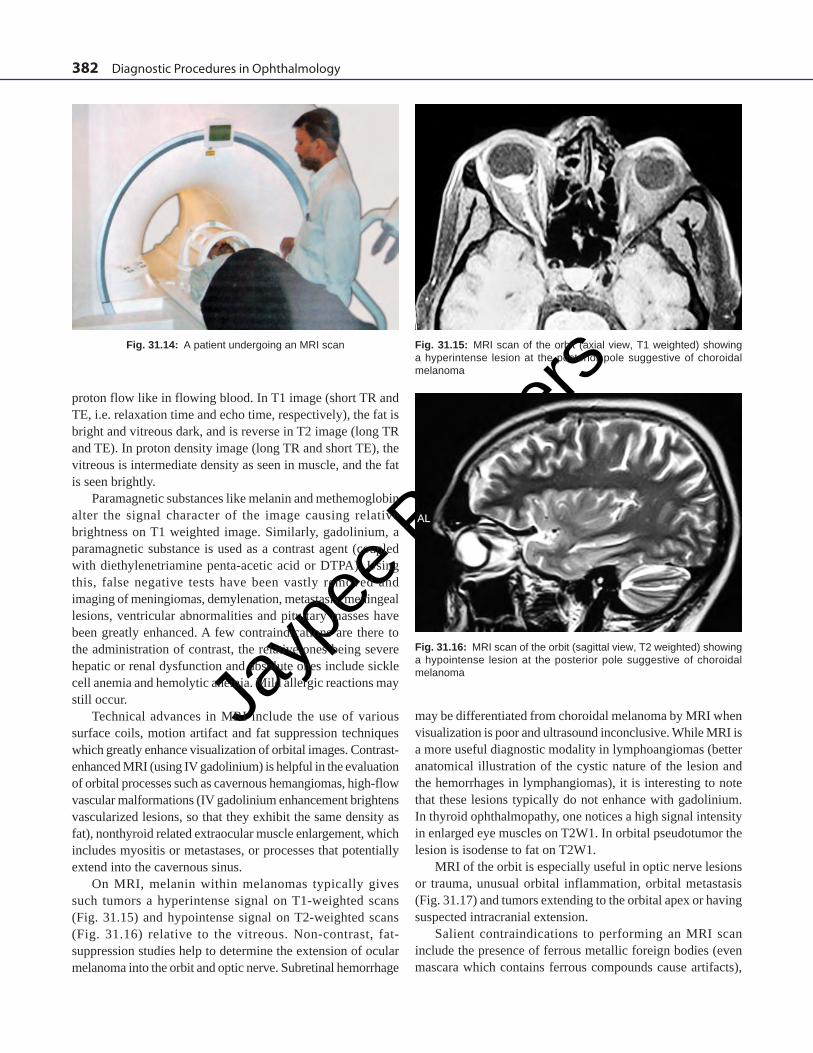
Figs 31.10A and B: (A) A case of orbital lymphangioma; (B) CT shows a diffuse, poorly defined, heterogenous lesion with minimal enhancement
and tissue contrast capabilities allowing for the imaging of soft tissues, intracranial structures, masses or processes suspected of calcification such as lymphangioma (Fig. 31.10), bones (e.g. sinus anatomy) or bony destruction (e.g. leukemia, lymphoma, histiocytosis, and rhabdomyosarcoma), contrast containing blood vessels and foreign bodies. Coronal sections with 2–3 mm slices should be specifically asked for in cases of blow-out fractures and for assessing extraocular muscle size in Graves ophthalmopathy. High resolution CT with 1 mm cuts is useful for studying optic nerve lesions. Axial sections show both globes, the horizontal rectus muscles, optic nerve, other orbital soft tissue and bony structures. Coronal section,
anteriorly, shows globe with relation to recti muscles and posteriorly, all four rectus muscles, oblique muscles, optic nerve and soft tissue of the orbit. At the apex it also shows the optic foramen.
CT adequately documents findings such as the extent of proptosis, muscle enlargement, location (intraconal or extraconal) and size of a lesion, compression of the globe or optic nerve and presence or absence of bone erosion, as well as the condition of adjacent sinuses and the presence of intracranial involvement. It also shows the internal characteristics of the lesion-whether it is homogeneous or heterogeneous, solid or cystic, presence of calcification and the effect of contrast
Figs 31.9A and B: Color Doppler examination in a case of orbital varices before (A) and after (B) Valsalva maneuver showing low blood flow velocity on dynamic evaluation
A
A
B
B

Jayp
ee B
rothe
rs
Diagnostic Techniques in Proptosis 381
enhancement. Benign tumors such as cavernous hemangioma, neurilemoma, dermoids and gliomas usually have rounded well circumscribed borders (Fig. 31.11). Malignant lesions on the other hand have diffuse, irregular boundaries. Important features of thyroid ophthalmopathy include swelling of muscles maximally in the mid-portion (relative sparing of the tendons), slight uveo-scleral thickening, apical crowding, increase in the diameter of the retrobulbar optic nerve sheath, increased density of orbital fat, and anterior displacement of the lacrimal gland (Fig. 31.12). CT is a useful modality for the evaluation of lacrimal fossa masses, especially epithelial tumors (Fig. 31.13). CT can adequately depict osseous alterations and calcifications, and can differentiate a group of epithelial tumors from inflammatory and lymphoproliferative conditions. Features specific of orbital pseudotumor include a poorly defined intra-extraconal mass close to the surface margin of the globe. In the myositic type one may get enlargement of one or more muscles close to their insertion, with ill-defined margins. Other features of orbital pseudotumor are that it typically involves muscles and tendon insertions. There is increased density of retro-orbital
fat, thickening and enhancement of sclera near Tenon’s capsule and enlargement of the lacrimal gland. Lymphangioma may be diagnosed if there is a multi-lobulated pattern on CT-scan (Fig. 31.10) and a cystic internal structure in standardized ultrasound evaluation. Cavernous hemangiomas show as well circumscribed, solid, masses involving the intra or extraconal compartment. On CT-scan lymphoproliferative tumors typically show up as a localized or diffuse mass with moulding to the orbital structures.
Magnetic Resonance Imaging Magnetic resonance imaging (MRI) is a noninvasive imaging technique which does not employ ionizing radiation and has no known adverse biological effects. The process involves a strong magnetic field which is applied to the body (Fig. 31.14). It excites protons in the body tissues and causes them to align in a particular orientation in relation to the magnetic field. When the magnetic field is switched off, the protons relax to their original alignment and re-emit the energy gained. The signal is recorded in terms of intensity and location. T1 weighting and T2 weighting refers to two methods of measuring the relaxation times of the excited protons after the magnetic field is switched off. The various body tissues have different relaxation times and a given tissue may be T1 or T2 weighted, implying that is best visualized on that particular type of image. Coronal, sagittal and axial images can be directly obtained. A surface coil is used for ophthalmic purposes to enhance spatial resolution. Four basic parameters can be adjusted to identify different tissues: proton density of tissue, bulk motion of protons (flow), spin lattice relaxation time (T1) and spin-spin relaxation time (T2).
Tissues with high proton (hydrogen nuclei) density (e.g. fat) emit a high signal as does low proton flow (coagulated blood). Low signal is produced by bone, sclera and sinus air and faster
Fig. 31.11: CT scan (axial view) showing a well-delineated, fusiform, intraconal mass isodense to the optic nerve, suggestive of glioma
Fig. 31.12: CT scan (coronal view) showing an infiltrative lesion in the lacrimal gland fossa with irregular internal structure suggestive of a malignant lacrimal gland tumor
Fig. 31.13: CT scan (axial view) showing significant enlargement of extraocular muscles with sparing of tendons in a case of thyroid exophthalmos
Jayp
ee B
rothe
rs
382 Diagnostic Procedures in Ophthalmology
proton flow like in flowing blood. In T1 image (short TR and TE, i.e. relaxation time and echo time, respectively), the fat is bright and vitreous dark, and is reverse in T2 image (long TR and TE). In proton density image (long TR and short TE), the vitreous is intermediate density as seen in muscle, and the fat is seen brightly.
Paramagnetic substances like melanin and methemoglobin alter the signal character of the image causing relative brightness on T1 weighted image. Similarly, gadolinium, a paramagnetic substance is used as a contrast agent (coupled with diethylenetriamine penta-acetic acid or DTPA). Using this, false negative tests have been vastly removed and imaging of meningiomas, demylenation, metastasis, meningeal lesions, ventricular abnormalities and pituitary masses have been greatly enhanced. A few contraindications are there to the administration of contrast, the relative ones being severe hepatic or renal dysfunction and absolute ones include sickle cell anemia and hemolytic anemia. Mild allergic reactions may still occur.
Technical advances in MRI include the use of various surface coils, motion artifact and fat suppression techniques which greatly enhance visualization of orbital images. Contrast-enhanced MRI (using IV gadolinium) is helpful in the evaluation of orbital processes such as cavernous hemangiomas, high-flow vascular malformations (IV gadolinium enhancement brightens vascularized lesions, so that they exhibit the same density as fat), nonthyroid related extraocular muscle enlargement, which includes myositis or metastases, or processes that potentially extend into the cavernous sinus.
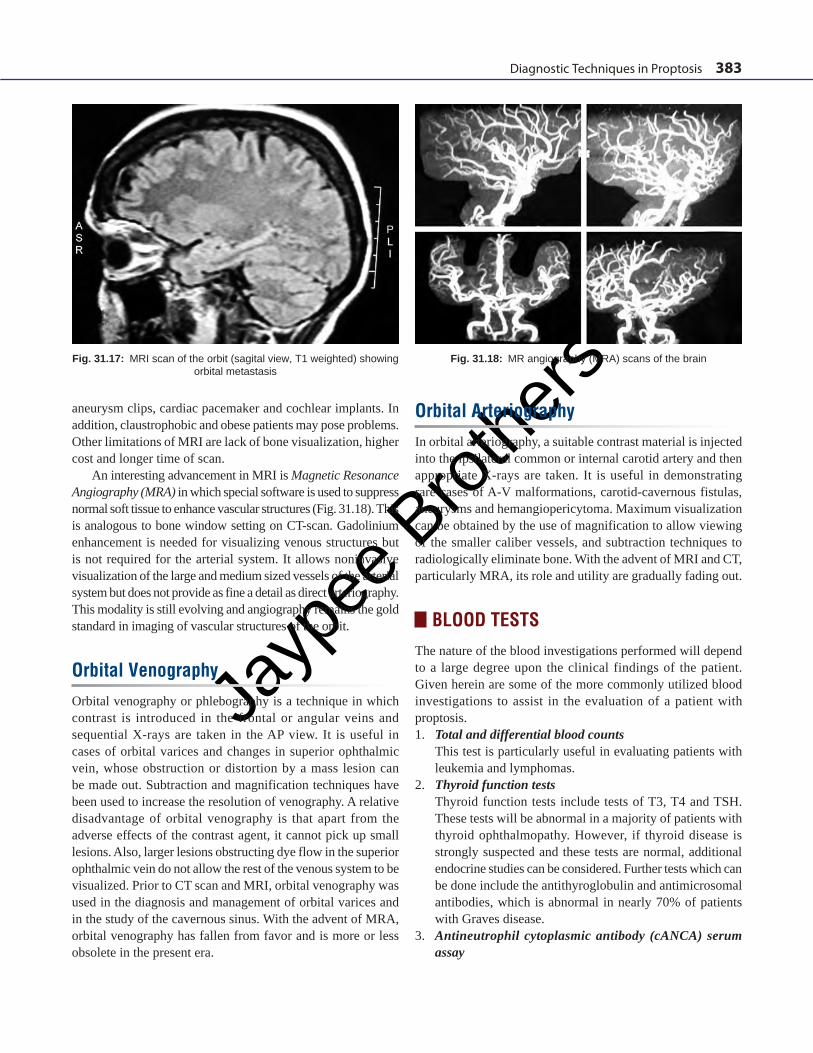
On MRI, melanin within melanomas typically gives such tumors a hyperintense signal on T1-weighted scans (Fig. 31.15) and hypointense signal on T2-weighted scans (Fig. 31.16) relative to the vitreous. Non-contrast, fat-suppression studies help to determine the extension of ocular melanoma into the orbit and optic nerve. Subretinal hemorrhage
Fig. 31.14: A patient undergoing an MRI scan Fig. 31.15: MRI scan of the orbit (axial view, T1 weighted) showing a hyperintense lesion at the posterior pole suggestive of choroidal melanoma
Fig. 31.16: MRI scan of the orbit (sagittal view, T2 weighted) showing a hypointense lesion at the posterior pole suggestive of choroidal melanoma
may be differentiated from choroidal melanoma by MRI when visualization is poor and ultrasound inconclusive. While MRI is a more useful diagnostic modality in lymphoangiomas (better anatomical illustration of the cystic nature of the lesion and the hemorrhages in lymphangiomas), it is interesting to note that these lesions typically do not enhance with gadolinium. In thyroid ophthalmopathy, one notices a high signal intensity in enlarged eye muscles on T2W1. In orbital pseudotumor the lesion is isodense to fat on T2W1.
MRI of the orbit is especially useful in optic nerve lesions or trauma, unusual orbital inflammation, orbital metastasis (Fig. 31.17) and tumors extending to the orbital apex or having suspected intracranial extension.
Salient contraindications to performing an MRI scan include the presence of ferrous metallic foreign bodies (even mascara which contains ferrous compounds cause artifacts),
Jayp
ee B
rothe
rs
Diagnostic Techniques in Proptosis 383
Fig. 31.17: MRI scan of the orbit (sagital view, T1 weighted) showing orbital metastasis
aneurysm clips, cardiac pacemaker and cochlear implants. In addition, claustrophobic and obese patients may pose problems. Other limitations of MRI are lack of bone visualization, higher cost and longer time of scan.
An interesting advancement in MRI is Magnetic Resonance Angiography (MRA) in which special software is used to suppress normal soft tissue to enhance vascular structures (Fig. 31.18). This is analogous to bone window setting on CT-scan. Gadolinium enhancement is needed for visualizing venous structures but is not required for the arterial system. It allows noninvasive visualization of the large and medium sized vessels of the arterial system but does not provide as fine a detail as direct arteriography. This modality is still evolving and angiography remains the gold standard in imaging of vascular structures of the orbit.
Orbital VenographyOrbital venography or phlebography is a technique in which contrast is introduced in the frontal or angular veins and sequential X-rays are taken in the AP view. It is useful in cases of orbital varices and changes in superior ophthalmic vein, whose obstruction or distortion by a mass lesion can be made out. Subtraction and magnification techniques have been used to increase the resolution of venography. A relative disadvantage of orbital venography is that apart from the adverse effects of the contrast agent, it cannot pick up small lesions. Also, larger lesions obstructing dye flow in the superior ophthalmic vein do not allow the rest of the venous system to be visualized. Prior to CT scan and MRI, orbital venography was used in the diagnosis and management of orbital varices and in the study of the cavernous sinus. With the advent of MRA, orbital venography has fallen from favor and is more or less obsolete in the present era.
Orbital ArteriographyIn orbital arteriography, a suitable contrast material is injected into the ipsilateral common or internal carotid artery and then appropriate X-rays are taken. It is useful in demonstrating rare cases of A-V malformations, carotid-cavernous fistulas, aneurysms and hemangiopericytoma. Maximum visualization can be obtained by the use of magnification to allow viewing of the smaller caliber vessels, and subtraction techniques to radiologically eliminate bone. With the advent of MRI and CT, particularly MRA, its role and utility are gradually fading out.
BLOOD TESTSThe nature of the blood investigations performed will depend to a large degree upon the clinical findings of the patient. Given herein are some of the more commonly utilized blood investigations to assist in the evaluation of a patient with proptosis.1. Total and differential blood counts This test is particularly useful in evaluating patients with
leukemia and lymphomas.2. Thyroid function tests Thyroid function tests include tests of T3, T4 and TSH.
These tests will be abnormal in a majority of patients with thyroid ophthalmopathy. However, if thyroid disease is strongly suspected and these tests are normal, additional endocrine studies can be considered. Further tests which can be done include the antithyroglobulin and antimicrosomal antibodies, which is abnormal in nearly 70% of patients with Graves disease.
3. Antineutrophil cytoplasmic antibody (cANCA) serum assay
Fig. 31.18: MR angiography (MRA) scans of the brain
Jayp
ee B
rothe
rs
384 Diagnostic Procedures in Ophthalmology
Diagnosis of Wegener’s granulomatosis should be considered in patients with scelokeratitis or coexisting sinus disease and orbital mass lesions. The antineutrophil cytoplasmic antibody (cANCA) serum assay is a very sensitive test for the presence of this rare disease.
4. Serum Angiotensin Converting Enzyme The diagnosis of sarcoidosis may be assisted by testing for
serum angiotensin converting enzyme (ACE). This multi-system granulomatous inflammatory condition may present with lacrimal gland enlargement.
5. ELISA for Cysticercosis Elisa test is used for evaluating the presence of an orbital
cyst, if cysticercosis is suspected. However, it needs to be corroborated with clinical and imaging findings due to a high percentage of both false positive and false negative results.
BIOPSY TECHNIQUESAlthough imaging techniques can help us in making a provisional diagnosis and are indicative in nature, a definitive diagnosis can only be made by obtaining a tissue specimen and subjecting it to routine and specialized histopathological techniques. Biopsy techniques which are commonly employed are described below:1. Fine Needle Aspiration Cytology Fine needle aspiration cytology (FNAC) is employed for
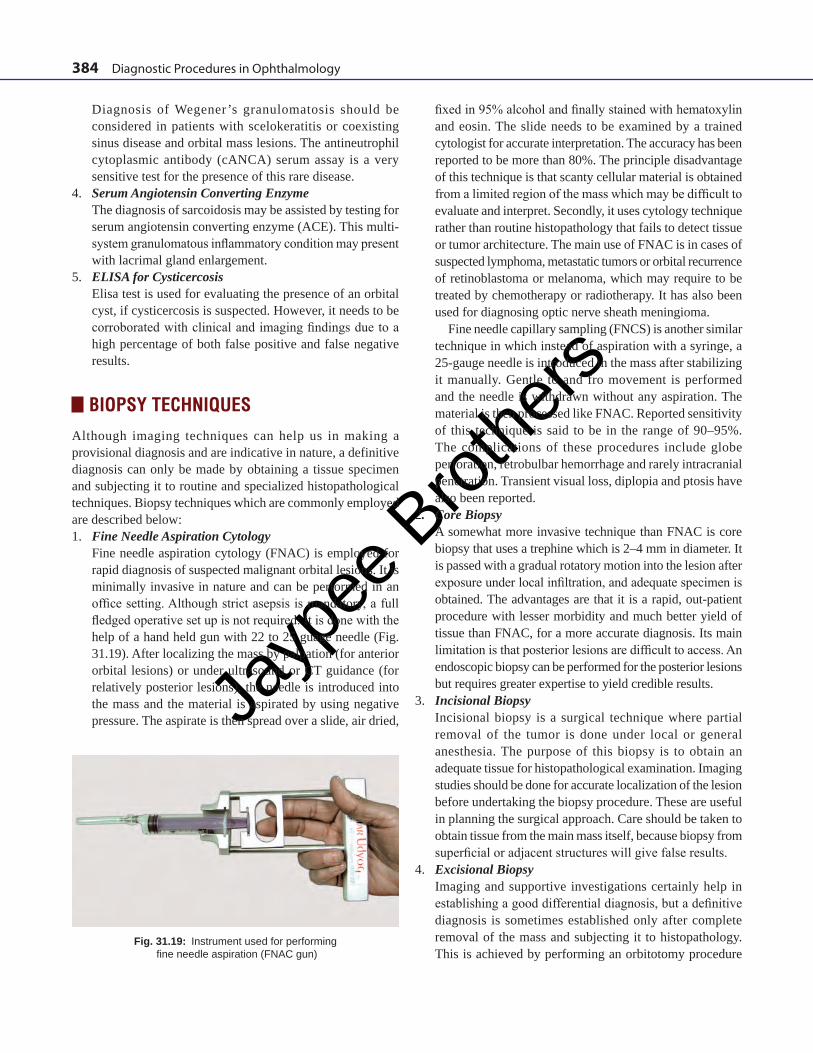
rapid diagnosis of suspected malignant orbital lesions. It is minimally invasive in nature and can be performed in an office setting. Although strict asepsis is mandatory, a full fledged operative set up is not required. It is done with the help of a hand held gun with 22 to 25 guage needle (Fig. 31.19). After localizing the mass by palpation (for anterior orbital lesions) or under ultrasound or CT guidance (for relatively posterior lesions), the needle is introduced into the mass and the material is aspirated by using negative pressure. The aspirate is then spread over a slide, air dried,
fixed in 95% alcohol and finally stained with hematoxylin and eosin. The slide needs to be examined by a trained cytologist for accurate interpretation. The accuracy has been reported to be more than 80%. The principle disadvantage of this technique is that scanty cellular material is obtained from a limited region of the mass which may be difficult to evaluate and interpret. Secondly, it uses cytology technique rather than routine histopathology that fails to detect tissue or tumor architecture. The main use of FNAC is in cases of suspected lymphoma, metastatic tumors or orbital recurrence of retinoblastoma or melanoma, which may require to be treated by chemotherapy or radiotherapy. It has also been used for diagnosing optic nerve sheath meningioma.
Fine needle capillary sampling (FNCS) is another similar technique in which instead of aspiration with a syringe, a 25-gauge needle is introduced in the mass after stabilizing it manually. Gentle to and fro movement is performed and the needle is withdrawn without any aspiration. The material is then processed like FNAC. Reported sensitivity of this technique is said to be in the range of 90–95%. The complications of these procedures include globe perforation, retrobulbar hemorrhage and rarely intracranial penetration. Transient visual loss, diplopia and ptosis have also been reported.
2. Core Biopsy A somewhat more invasive technique than FNAC is core
biopsy that uses a trephine which is 2–4 mm in diameter. It is passed with a gradual rotatory motion into the lesion after exposure under local infiltration, and adequate specimen is obtained. The advantages are that it is a rapid, out-patient procedure with lesser morbidity and much better yield of tissue than FNAC, for a more accurate diagnosis. Its main limitation is that posterior lesions are difficult to access. An endoscopic biopsy can be performed for the posterior lesions but requires greater expertise to yield credible results.
3. Incisional Biopsy Incisional biopsy is a surgical technique where partial
removal of the tumor is done under local or general anesthesia. The purpose of this biopsy is to obtain an adequate tissue for histopathological examination. Imaging studies should be done for accurate localization of the lesion before undertaking the biopsy procedure. These are useful in planning the surgical approach. Care should be taken to obtain tissue from the main mass itself, because biopsy from superficial or adjacent structures will give false results.
4. Excisional Biopsy Imaging and supportive investigations certainly help in
establishing a good differential diagnosis, but a definitive diagnosis is sometimes established only after complete removal of the mass and subjecting it to histopathology. This is achieved by performing an orbitotomy procedure
Fig. 31.19: Instrument used for performing fine needle aspiration (FNAC gun)
Jayp
ee B
rothe
rs
Diagnostic Techniques in Proptosis 385
through one of the surgical approaches to the orbit. The principles of localization and surgical planning are similar to the ones described above. This, along with incisional biopsy, is the gold standard for diagnosis and has the added advantage of being therapeutic in benign encysted lesions like dermoids, cavernous hemangioma, pleomorphic adenoma of lacrimal gland, neurilemoma and fibrous histiocytoma.
PATHOLOGY TECHNIQUESThis area is the most important part of any diagnostic process as it provides actual tissue diagnosis, which may have therapeutic and medico-legal importance. It is imperative to have proper communicaton with the pathologist preoperatively, to facilitate and plan the appropriate histopathologic technique for a given case.1. Cytology: As already stated under the section on FNAC,
cytology is a low cost technique for rapid diagnosis. The aspirate is spread over a slide and air dried followed by alcohol fixation and stained by Papanicolaou technique and H&E or May-Grunwald-Giemsa stain; mainly used for suspected malignant lesions. Cytology has its limitations as discussed earlier.
2. Gross Examination: The gross excised specimen is inspected for shape, size, consistency (firm/hard/cystic/nodular), and whether the capsule is intact or broken. Measurements are made in three dimensions. Then it is cut to see the internal architecture– color, areas of necrosis, calcification and inner structure (solid or cystic). For example, on gross examination, pleomorphic adenoma of the lacrimal gland displays an intact capsule, with firm, bosselated appearance, and on cut section it has whitish, firm solid areas with some interspersed friable areas.
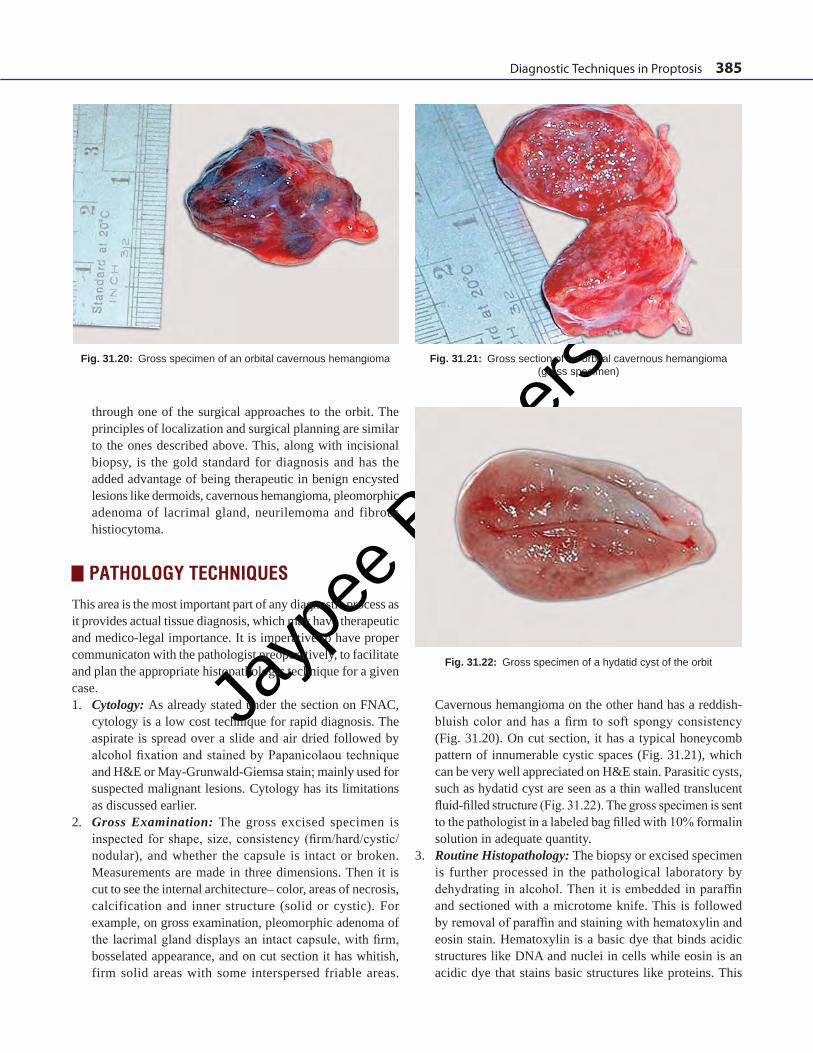
Fig. 31.20: Gross specimen of an orbital cavernous hemangioma Fig. 31.21: Gross section of an orbital cavernous hemangioma (gross specimen)
Fig. 31.22: Gross specimen of a hydatid cyst of the orbit
Cavernous hemangioma on the other hand has a reddish-bluish color and has a firm to soft spongy consistency (Fig. 31.20). On cut section, it has a typical honeycomb pattern of innumerable cystic spaces (Fig. 31.21), which can be very well appreciated on H&E stain. Parasitic cysts, such as hydatid cyst are seen as a thin walled translucent fluid-filled structure (Fig. 31.22). The gross specimen is sent to the pathologist in a labeled bag filled with 10% formalin solution in adequate quantity.
3. Routine Histopathology: The biopsy or excised specimen is further processed in the pathological laboratory by dehydrating in alcohol. Then it is embedded in paraffin and sectioned with a microtome knife. This is followed by removal of paraffin and staining with hematoxylin and eosin stain. Hematoxylin is a basic dye that binds acidic structures like DNA and nuclei in cells while eosin is an acidic dye that stains basic structures like proteins. This
Jayp
ee B
rothe
rs
386 Diagnostic Procedures in Ophthalmology
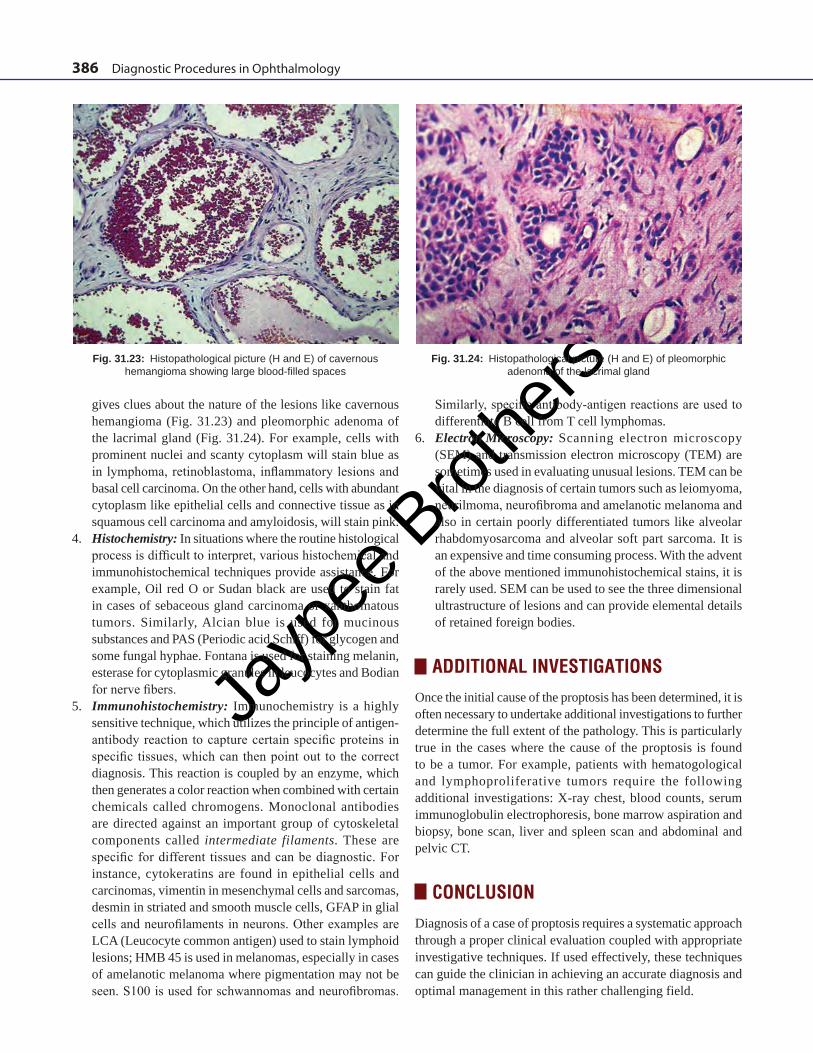
Fig. 31.23: Histopathological picture (H and E) of cavernous hemangioma showing large blood-filled spaces
Fig. 31.24: Histopathological picture (H and E) of pleomorphic adenoma of the lacrimal gland
gives clues about the nature of the lesions like cavernous hemangioma (Fig. 31.23) and pleomorphic adenoma of the lacrimal gland (Fig. 31.24). For example, cells with prominent nuclei and scanty cytoplasm will stain blue as in lymphoma, retinoblastoma, inflammatory lesions and basal cell carcinoma. On the other hand, cells with abundant cytoplasm like epithelial cells and connective tissue as in squamous cell carcinoma and amyloidosis, will stain pink.
4. Histochemistry: In situations where the routine histological process is difficult to interpret, various histochemical and immunohistochemical techniques provide assistance. For example, Oil red O or Sudan black are used to stain fat in cases of sebaceous gland carcinoma or xanthomatous tumors. Similarly, Alcian blue is used for mucinous substances and PAS (Periodic acid Schiff) for glycogen and some fungal hyphae. Fontana is used for staining melanin, esterase for cytoplasmic granules in leucocytes and Bodian for nerve fibers.
5. Immunohistochemistry: Immunochemistry is a highly sensitive technique, which utilizes the principle of antigen-antibody reaction to capture certain specific proteins in specific tissues, which can then point out to the correct diagnosis. This reaction is coupled by an enzyme, which then generates a color reaction when combined with certain chemicals called chromogens. Monoclonal antibodies are directed against an important group of cytoskeletal components called intermediate filaments. These are specific for different tissues and can be diagnostic. For instance, cytokeratins are found in epithelial cells and carcinomas, vimentin in mesenchymal cells and sarcomas, desmin in striated and smooth muscle cells, GFAP in glial cells and neurofilaments in neurons. Other examples are LCA (Leucocyte common antigen) used to stain lymphoid lesions; HMB 45 is used in melanomas, especially in cases of amelanotic melanoma where pigmentation may not be seen. S100 is used for schwannomas and neurofibromas.
Similarly, specific antibody-antigen reactions are used to differentiate B cell from T cell lymphomas.
6. Electron Microscopy: Scanning electron microscopy (SEM) and transmission electron microscopy (TEM) are sometimes used in evaluating unusual lesions. TEM can be vital in the diagnosis of certain tumors such as leiomyoma, neurilmoma, neurofibroma and amelanotic melanoma and also in certain poorly differentiated tumors like alveolar rhabdomyosarcoma and alveolar soft part sarcoma. It is an expensive and time consuming process. With the advent of the above mentioned immunohistochemical stains, it is rarely used. SEM can be used to see the three dimensional ultrastructure of lesions and can provide elemental details of retained foreign bodies.
ADDITIONAL INVESTIGATIONSOnce the initial cause of the proptosis has been determined, it is often necessary to undertake additional investigations to further determine the full extent of the pathology. This is particularly true in the cases where the cause of the proptosis is found to be a tumor. For example, patients with hematogological and lymphoproliferative tumors require the following additional investigations: X-ray chest, blood counts, serum immunoglobulin electrophoresis, bone marrow aspiration and biopsy, bone scan, liver and spleen scan and abdominal and pelvic CT.
CONCLUSIONDiagnosis of a case of proptosis requires a systematic approach through a proper clinical evaluation coupled with appropriate investigative techniques. If used effectively, these techniques can guide the clinician in achieving an accurate diagnosis and optimal management in this rather challenging field.
Jayp
ee B
rothe
rs
Diagnostic Techniques in Proptosis 387
BIBLIOGRAPHY 1. Aburn NS, Sergott RC. Orbital Color Doppler Imaging. Eye.
1993;7:639-47. 2. Aviv RI, Miszkiel K. Orbital imagig : Part 2. Intraorbital
pathology. Clin Radiol. 2005;60:288-307. 3. Bartley GB, Gorman CA. Diagnostic criteria for Graves
ophthalmopathy. Am J Ophthalmol. 1995;119:792-5. 4. Bilaniuik CT. Vascular lesions of the orbit in children.
Neuoimaging Clin N Am. 2005;15:107-20. 5. Devis PC, Newman NJ. Advances in neuroimaging of visual
pathways. Am J Ophthalmol. 1996;121:690-705. 6. Dutton JJ, Byrne SF, Proia AD. Diagnostic Atlas of Orbital
Diseases. Philadelphia, Saunders. 2000.
7. Newton TH, Bilaniuk LT. (Eds). Radiology of Eyes and Orbit. New York, Raven. 1990.
8. Rootman J. (Ed). Diseases of Orbit: A Multidisciplinary approach. Philadelphia, Lippincott William & Wilkins. 2003.
9. Shields JA, Shields CL. Atlas of Orbital Tumors. New York, William & Wilkins. 1999.
10. Shields JL, Shields JA, Honavar, SG, et al. Clinical spectrum of primary ophthalmic rhabdomyosarcoma. Ophthalmology. 2001; 108:2284-92.
11. Wiersinga,WM, Prummel MF. Pathogenesis of Graves ophthalmopathy—current understanding (Editorial). J Clin Endocrinol Metab. 2001;86:501-3.