Embed Size (px)
Citation preview
Diagnostic Injection of Xylocaine into Extraocular Muscles ELBERT MAGOON, MD, MARC CRUCIGER, MD, ALAN B. SCOTT, MD, ARTHUR JAMPOLSKY, MD
Abstract: In situations where it is unclear which extraocular muscle is causing anomalous eye movement or to what extent one of two muscles is responsible, temporary paralysis of the muscle with Xylocaine may provide the answer. The procedure is to inject 0.2 to 0.5 cc 2% Xylocaine directly into the muscle using electromyography (EMG) for precise localization, a technique similar to that of therapeutic injections of botulinum toxin (Oculinum). The procedure is especially useful for Duane's syndrome, superior oblique palsy, and other situations where abnormal muscle insertions or innervations make diagnosis ofthe muscle responsible for an eye movement anomaly difficult and surgery unpredictable. [Key words: botulinum toxin, eye muscle injection, Strabismus diagnosis, Xylocaine.] Ophthalmology 89:489-491, 1982
The contribution of each extraocular muscle, especially for vertical and torsional movements, is not straightforward. Even between normal subjects there is some variability; in strabismus patients, these interactions of eye muscles may be quite unpredictable. Although good surgical results are obtained in most cases of strabismus by assuming normal muscle action, better results could be achieved if the effects of individual muscles could be quantitatively known before surgery. In patients who have abnormal innervation or anomalous muscle insertions, it is even more difficult to predict the effect of surgery using classic normal physiology guidelines.
Injections of 2% Xylocaine into extraocular muscles have been used in the past as a research tool to study muscle mechanics.1.2 Advanced techniques and instrumentation developed for therapeutic injections of botulinum toxin (Oculinum)3 have made practical the diagnostic injection of Xylocaine directly into ex-
From the Smith-Kettlewell Institute of Visual Sciences, San Francisco, California.
Presented at the Eighty-sixth Annual Meeting of the American Academy of Ophthalmology, Atlanta, Georgia, November 1-6, 1981.
Supported by NIH grant # EY 070271 and EY 02106 and the Smith-Kettlewell Eye Research Foundation.
Reprint requests to Elbert Magoon, MD, Smith-Kettlewell Institute of Visual Sciences, 2232 Webster Street, San Francisco, CA 94115.
traocular muscle under electromyographic control to selectively eliminate the action of possibly abnormal muscles.
This paper describes four cases where these injections were found to be helpful: case 1 is Duane's syndrome with vertical upshoot; case 2 is IV nerve palsy; case 3 is a patient with orbital anomalies; and in case 4 Xylocaine is used to predict the effect of long-term paralysis with botulinum toxin.
TECHNIQUE
Topical anesthetic drops (proparacaine) are used for anesthesia. One drop of 1% epinephrine reduces the vascularity of tissues and probably makes subconjunctival hemorrhage less likely. A syringe of 2% Xylocaine is attached to a special electromyography (EMG) needle electrode identical to those used for therapeutic injections of Oculinum.3 This is a 26-gauge needle with an insulated wire running down the bore of the needle to provide an EMG signal. The needle is used with a small portable amplifier/speaker box that has been designed for this purpose and gives the surgeon auditory feedback from the EMG potentials. The needle is inserted into the extraocular muscle insertion region and advanced about 15 mm along the orbital side of the muscle with the eye looking in the primary position. Then the patient is instructed to look into the
0161-6420/82/0500/0489/$00.65 © American Academy of Ophthalmology 489
OPHTHALMOLOGY • MAY 1982 • VOLUME 89 • NUMBER 5
field of action of the muscle to increase muscle activity, and the needle is angled into the muscle. At this point a strong EMG signal will be heard, and the needle Can be advanced 5 to 10 mm more while continuing to monitor the EMG signal. When the needle is well into the muscle, the Xylocaine can be injected. The EMG signal will gradually disappear indicating that the muscle is becoming paralyzed. With minimal effect on surrounding eye muscles, 0.2 to 0.5 cc of 2% Xylocaine usually gives effective paralysis of that muscle. Routinely a drop of chloramphenicol is given after the procedure. The whole procedure takes about five minutes. Within a few minutes the change in eye movements caused by paralysis of the injected muscle can be assessed.
CASE REPORTS
Case I-Duane's syndrome. A 16-year-old girl was referred for evaluation of Duane's syndrome , involving the left eye with upshoot on adduction. At age 3 she had a left medial rectus recession of 4.5 mm for left hypertropia and esotropia. For persistent left hypertropia she had a 3.5 mm recession of the left superior rectus and resection of the left inferior rectus 4.5 mm. After operation her hypertropia persisted.
Upon examination the visual acuity was 20125 right eye, 20/100 left eye. There was a 40 prism diopter left hypertropia in the primary position at distance fixation. The left eye showed very little abduction or adduction, and also demonstrated a moderate deficiency of depression. On attempted adduction of the left eye, there was significant enophthalmos and elevation. There was also a slight "A" pattern and a slight hypertropia of the left eye in all positions of gaze.
Electromyography recording from the left superior rectus showed a normal pattern of activity . Recording from the left inferior oblique showed a possible increase of some units on adduction. However, after 0.4 ml of Xylocaine reduced the EMG of this left inferior oblique to an unrecordable level, there was still no substantial alteration in the pattern of overshoot, which proved the inferior oblique was not responsible for the overshoot. [The elevation on adduction of the left eye.] Following 0.5 cc Xylocaine into the left lateral rectus, there was a marked reduction in enophthalmos and of the vertical overshoot on adduction of the left eye, which proved co-contraction of the horizontal muscles was the cause of the overshoot.
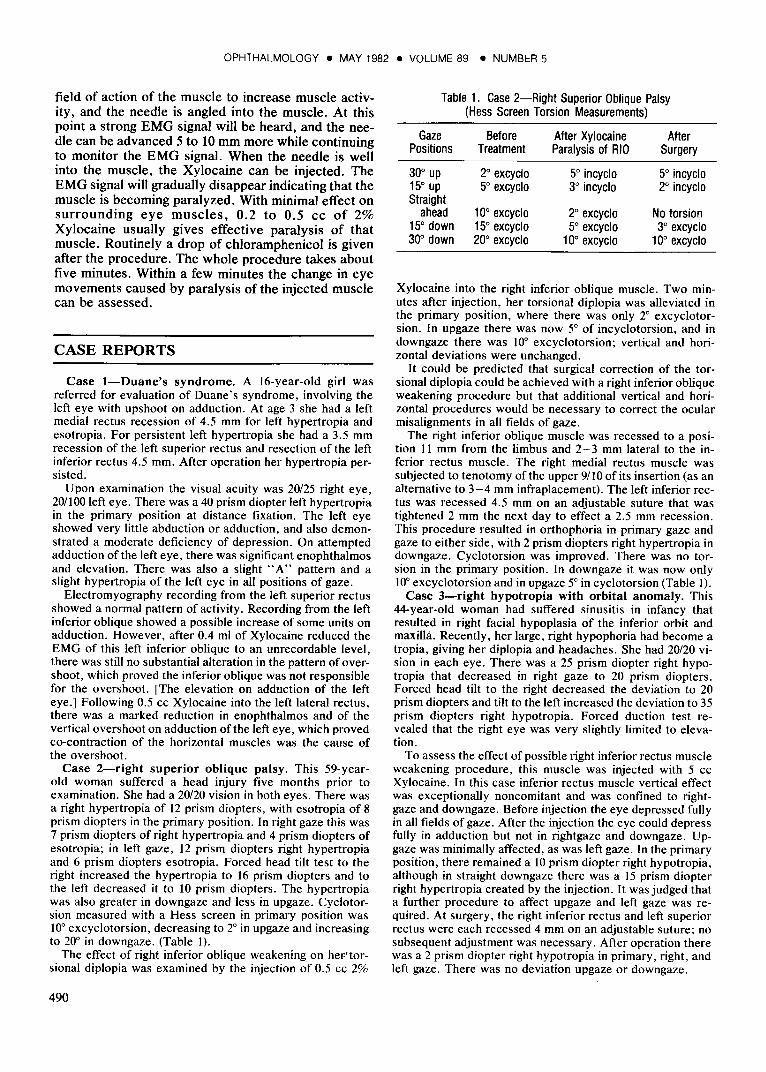
Case 2-right superior oblique palsy. This 59-yearold woman suffered a head injury five months prior to examination. She had a 20/20 vision in both eyes. There was a right hypertropia of 12 prism diopters, with esotropia of 8 prism diopters in the primary position. In right gaze this was 7 prism diopters of right hypertropia and 4 prism diopters of esotropia; in left gaze, 12 prism diopters right hypertropia and 6 prism diopters esotropia. Forced head tilt test to the right increased the hypertropia to 16 prism diopters and to the left decreased it to 10 prism diopters . The hypertropia was also greater in downgaze and less in upgaze. Cyclotorsion measured with a Hess screen in primary position was 10" excyclotorsion, decreasing to 2° in upgaze and increasing to 20" in downgaze. (Table I).
The effect of right inferior oblique weakening on heF'torsional diplopia was examined by the injection of 0.5 cc 2%
490
Table 1. Case 2-Right Superior Oblique Palsy (Hess Screen Torsion Measurements)
Gaze Before After Xylocaine After Positions Treatment Paralysis of RIO Surgery
30° up 2° excyclo 5° incyclo 5° incyclo 15° up 5° excyclo 3° incyclo 2° incyclo Straight
ahead 10° excyclo 2° excyclo No torsion 15° down 15° excyclo 5° excyclo 3° excyclo 300 down 20° excyclo 10° excyclo 10° excyclo
Xylocaine into the right inferior oblique muscle. Two minutes after injection, her torsional diplopia was alleviated in the primary position, where there was only 2° excyclotorsion. In upgaze there was now 5° of incyclotorsion, and in downgaze there was 10° excyclotorsion; vertical and horizontal deviations were unchanged.
It could be predicted that surgical correction of the torsional diplopia could be achieved with a right inferior oblique weakening procedure but that additional vertical and horizontal procedures would be necessary to correct the ocular misalignments in all fields of gaze.
The right inferior oblique muscle was recessed to a position II mm from the limbus and 2 - 3 mm lateral to the inferior rectus muscle. The right medial rectus muscle was subjected to tenotomy of the upper 9/10 of its insertion (as an alternative to 3-4 mm infraplacement). The left inferior rectus was recessed 4.5 mm on an adjustable suture that was tightened 2 mm the next day to effect a 2.5 mm recession. This procedure resulted in orthophoria in primary gaze and gaze to either side, with 2 prism diopters right hypertropia in downgaze. Cyclotorsion was improved. There was no torsion in the primary position. In downgaze it was now only 10" excyclotorsion and in upgaze 5° in cyclotorsion (Table O.
Case 3-right hypotropia with orbital anomaly. This 44-year-old woman had suffered sinusitis in infancy that resulted in right facial hypoplasia of the inferior orbit and maxilla. Recently, her large, right hypophoria had become a tropia, giving her diplopia and headaches. She had 20/20 vision in each eye. There was a 25 prism diopter right hypotropia that decreased in right gaze to 20 prism diopters . Forced head tilt to the right decreased the deviation to 20 prism diopters and tilt to the left increased the deviation to 35 prism diopters right hypotropia . Forced duction test revealed that the right eye was very slightly limited to elevation .
To assess the effect of possible right inferior rectus muscle weakening procedure, this muscle was injected with 5 cc Xylocaine. In this case inferior rectus muscle vertical effect was exceptionally noncomitant and was confined to rightgaze and downgaze. Before injection the eye depressed fully in all fields of gaze. After the injection the eye could depress fully in adduction but not in rightgaze and downgaze. Upgaze was minimally affected, as was left gaze. In the primary position, there remained a 10 prism diopter right hypotropia, although in straight downgaze there was a 15 prism diopter right hypertropia created by the injection. It was judged that a further procedure to affect upgaze and left gaze was required. At surgery, the right inferior rectus and left superior rectus were each recessed 4 mm on an adjustable suture; no subsequent adjustment was necessary. After operation there was a 2 prism diopter right hypotropia in primary, right, and left gaze. There was no deviation upgaze or downgaze.

MAGOON, et al • XYLOCAINE INJECTION
Case 4-sixth nerve innervational anomaly. A 20-year-old woman had undergone successful surgery for a brain tumor. There was, however, left sixth nerve damage resulting in almost total paralysis. Over one year after her neurosurgery, the left medial rectus muscle was recessed 8 or 9 mm and the left lateral rectus resected 7 or 8 mm. This resulted in good mobility of the left eye and satisfactory alignment much of the time.
However, after gazing to the left, the left eye would not be able to return to primary position. This caused diplopia and exotropia that was quite distressing to the patient. This anomaly was studied extensively with EMG and found to be an innervational anomaly (neuromyotonia) of the lateral rectus muscle. That is, some left lateral rectus muscle motor units were unable to be appropriately inhibited. Carbamazepine (Tegretol) treatment was not tolerated. An injection of Xylocaine weakened the lateral rectus muscle sufficiently to prevent the patient's distressing symptoms. Semi-annual injection of Botulinum toxin (Oculinum) has been a successful treatment for over three years.
DISCUSSION
Analysis using normal muscle physiology is usually sufficient to guide surgery. However, in cases of abnormal innervations, muscle insertions and mechanics, it may be helpful to be certain exactly what are the effects of certain muscles. In these situations diagnostic injection of Xylocaine may be helpful.
Case 1 is a typical Duane's co-contraction upshoot.4,5 With Xylocaine injection, one can be certain the inferior oblique plays no role in the upshoot on adduction, and that it is caused solely by cocontraction of medial and lateral rectus muscles. EMG alone can determine horizontal rectus muscle cocontraction and can demonstrate the patterns of muscle recruitment; but temporary paralysis is the only preoperative way to determine quantitatively which muscles are causing the upshoot. Surgery can be guided by this knowledge.
A positive forced duction test in Duane's syndrome always presents a problem. One does not know how much force is contributed by active anomalous innervation to the lateral rectus, and how much is contributed by passive stretch of a fibrotic muscle. Xylocaine injection can eliminate the active innervational component and enable one to perform a truly passive forced duction test.
Case 2 is an example of torsional diplopia where Xylocaine injection helps the surgeon predict whether simple weakening of the inferior oblique muscle (as by a Z-lengthening procedure) will cure the torsional problem. Also, it helps predict the need for additional vertical muscle surgery to correct the vertical deviation.
The inferior rectus muscle has been injected to predict the effect of inferior rectus recession on the various fields of gaze as in case 3. Since the division of labor between vertical muscles in various fields of gaze varies from patient to patient, injection helps predict effects of surgery.
Case 4 illustrates the use of Xylocaine injection to predict whether long-term abolition of innervation will be effective therapeutically. In addition to Duane's syndrome, IV nerve palsy, and orbital anomalies, the technique has been found to be helpful in cases of III nerve anomalous regeneration, partial VI nerve palsy, and possible anomalous muscle insertions. The technique may not be of value for routine horizontal strabismus, but it has been found helpful for situations where division of labor between individual muscles is uncertain.
By causing temporary paralysis, Xylocaine injections help assess the active force of innervated muscle, but not passive stretch forces. This helps predict the effect of a surgical weakening procedure in the field of action of the muscle. But a few minutes of paralysis will not remove passive stretch forces and will not predict the effects of recession of a tight muscle in gaze positions out of the field of its action.
No complications except for small subconjunctival hemorrhage have been encountered. By force measurements at least 90% of muscle strength can be temporarily eliminated with Xylocaine. The precise localization of the drug is critical to this purpose. The technique requires a thorough knowledge of eye muscle mechanics and innervational patterns seen by electromyography. Since the techniques and EMG apparatus for diagnostic Xylocaine injection are the same as those recently developed for the therapeutic injection of botulinum toxin (Oculinum), they are readily available to interested ophthalmologists.
REFERENCES
1. Scott AB, Collins CC, O'Meara DM, Zipf RF. Contribution of individual extraocular muscles to eye movement. ARVO Abstracts. Invest Ophthalmol 1973; 63.
2. Tamler E, Jampolsky A, Marg E. Electromyography in strabismus. Califomia Med 1959; 90:437-9
3. Scott AB. B'otulinum toxin injection into extraocular muscles as an alternative to strabismus surgery. Ophthalmology 1980; 87:1044-9.
4. Scott AB. Upshoots and downshoots. In: Souza-Dias C ed. V Congress of the CLADE (Conselho Latino-Americano de Estrabismo), October 16-17, 1976, Guaruja-Brasil. Sao Paulo: Oficinas das Edicoes Loyola, 1978.
5. Scott AB, Wong GY. Duane's syndrome: an electromyographic study. Arch Ophthalmol 1972; 87:140-7.
491