Embed Size (px)
Citation preview

Diagnostic Evaluation of Lower Urinary Tract Symptoms in Women
Jeffrey P. Weiss, MD, FACS
Professor and Chair
Department of Urology
SUNY Downstate College of Medicine
VA NY Harbor Healthcare System
Brooklyn, NY
Lower Urinary Tract Symptoms (LUTS)
• Storage symptoms(irritative symptoms)
• Emptying symptoms (obstructive symptoms)
Storage Symptoms
• Urinary Frequency
• Urgency
• Nocturia
• Incontinence
• Pain
Voiding Symptoms
• Hesitancy / Weak Stream / Straining
• Incomplete emptying
• Urinary Retention
• Pain

Pain
• Dysuria
• Perineal “Aching”
• Inner Aspect Of Thighs
• Suprapubic Fullness

Conditions causing symptoms
• Urethral obstruction
• Impaired detrusor contractility
• Detrusor overactivity
• Low bladder compliance
• Sensory urgency
• Learned voiding dysfunction
• Polyuria
Differential Diagnosis
• OAB• Pelvic prolapse• Urethral stricture• Neurogenic voiding dysfunction• Urethral diverticulum• Acquired voiding dysfunction• Diabetes insipidus

Remediable Conditions
• Storage– Sphincteric incontinence– Fistula– Overactive bladder
• Voiding– Prolapse– acquired voiding dysfunction– urethral diverticulum– urethral stricture– primary bladder neck obstruction

Evaluation
• History & physical exam
• Questionnaire
• Urinalysis & culture
• Voiding diary

Physical Examination
• General
• Urologic
• Neurologic
• Neuro-urologic

Physical Examination
• General– Cognitive function – Signs of CHF– Peripheral edema
• Urologic– Exam with full bladder for SUI– Pelvic prolapse: location– Palpable urethral mass– Vaginal mucosal health

Physical Examination
• Neurologic– Cognitive function – Gait– Muscular strength– Deep tendon reflexes
• Neurourologic– Perianal sensation– Anal sphincter tone & control– Bulbocavernosus reflex
Bladder Diary
• Essential component of the w/u
• Time & amount of each urination
• Description of symptoms
• +/- oral intake
• The diary is a snapshot to be
compared to day to day sx
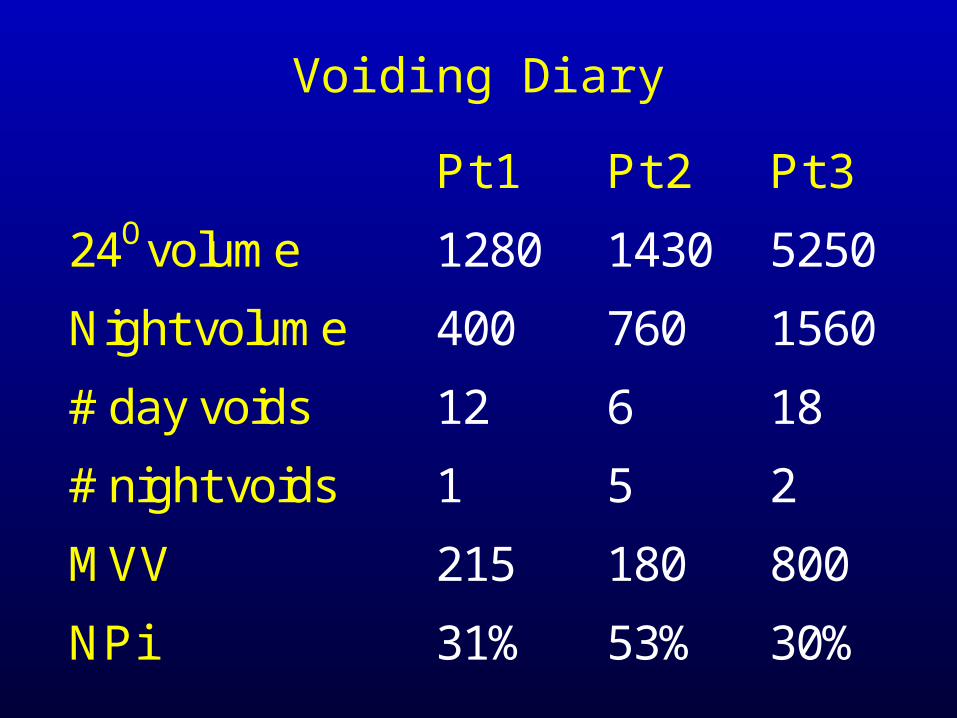
Pt 1 Pt 2 Pt 3
24Ovolume 1280 1430 5250
Night volume 400 760 1560
# day voids 12 6 18
# night voids 1 5 2
MVV 215 180 800
NPi
31% 53% 30%
Voiding Diary

Pad Test
• Useful for quantifying the amount of urine loss – two kinds:
• Stress pad test (20 min – 1 hour)(to provoke incontinence)
• 24 hour – 3 day – 7 day pad test( to mimic typical day)

Evaluation
• Q & PVR
• Urodynamics
• Cystoscopy
• Upper tract
imaging
Renal ultrasound
CTU

Uroflow
• Functional evaluation of interactionbetween the bladder & urethra
• Low flow:bladder outlet obstructionimpaired detrusor contractility
• Normal flow:does not exclude obstruction

ml/S
20
10
Uroflow
Normal
Seconds
ObstructedImpaired contractilityAcquired voiding dysfunction

Post Void Residual Urine
• Ultrasound
• Catheterization
• Contrast imaging study
Post Void Residual Urine• An elevated PVR means that the
bladder did not contract strongly enough for that urethra during that particular micturition
• It does not necessarily mean thereis bladder outlet obstruction
• A low PVR does not exclude urethralobstruction
• Highly variable and should be repeated

Upper Tract Imaging(indications)
• Significant urethral obstruction
• Detrusor sphincter dyssynergia
• Low bladder compliance
• Adult onset enuresis
• Women with LUTS & low Q whodon’t want RX

Indications for Cystoscopy*• hematuria• sterile pyuria• pelvic/bladder/urethral pain• vesicovaginal fistula• extra-urethral incontinence• I do cystoscopy preoperatively
on all patients including prolapse• To be sure there are 2 ureteral orifices• No surprises
4th ICI, 2008

Urodynamics: Purpose
• Reproduce symptoms
• Diagnose pathophysiology of underlying symptoms
• Identify risk factors
• Direct treatment
• Prognosticate

Urodynamics
• An interactive test between patient & physician
• The findings must be interpreted at the time of the study
• It is not possible to interpret the study by looking at the tracings afterwardsunless there has been a detailed annotation

Prior to Urodynamics
• What are the symptoms?
• Was SUI or prolapse found on exam?
• Neurologic lesion?
• Bladder capacity (MVV)
• Q & PVR• Formulate questions to be answered by the study

Indications for Urodynamics
• Low uroflow
• High PVR
• Uncertain diagnosis
• Finding that requires further evaluation
• Persistent symptoms despite apparently appropriate treatment

Storage Phase Urodynamics
• Cystometrogram (CMG)
• Leak Point Pressure
• Urethral Pressure Measurements
• EMG
• Cystogram

Emptying Phase Urodynamics
• Detrusor pressure – uroflow study
• Micturitional urethral pressure profile
• Sphincter electromyography (EMG)
• Post void residual
• Voiding cystourethrogram

Cystometry (CMG)
• Measurement of bladder pressure and volume during bladder filling:
• Bladder sensations
• Bladder pressure
• Involuntary bladder contractions
• Bladder compliance
• Bladder capacity
• Control over micturition

Cystometry
• Once aware, can she contractthe sphincter ?
• Does sphincter contraction abort the stream?
• Does sphincter contraction abortthe detrusor contraction?

Idealized CMG
pdet
Volume
Storage Voiding
Videourodynamics
• Combines urodynamics with fluoroscopic imaging of the LUT during
–bladder filling
–provocative maneuvers
–voiding
• Most accurate means of assessment


(Voiding) Detrusor PressureUroflow Study
• Urethral obstruction = high detrusor pressure & low uroflow
• Impaired detrusor contractility = low or poorly sustained detrusor pressure& low flow
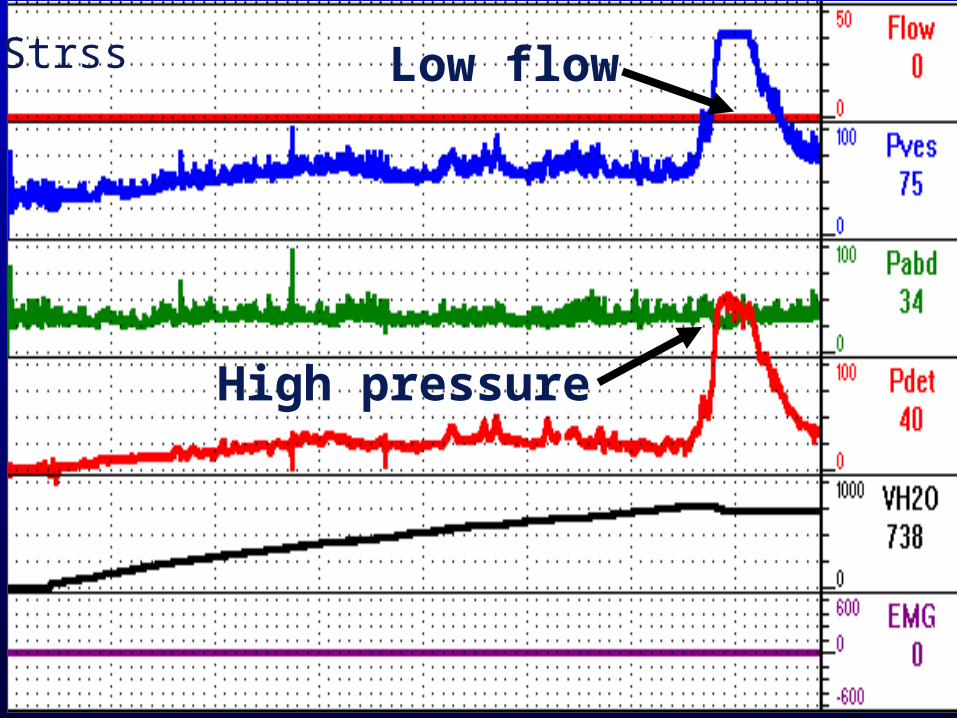
2Strss
High pressure
Low flow

JK
Low pressure
Low flow

Evaluation of Incontinence
• HX, PE (observation of SUI, prolapse)
• UA
• Q-tip test
• Bladder diary (incontinence episodes)
• Pad test
• Q & PVR (straining pattern)

Conditions Causing Incontinence
• Bladder problems– Detrusor overactivity– Low bladder compliance– Fistula
• Sphincter problems– Urethral hypermobility– Intrinsic sphincter deficiency

Q-tip Test
> 30O = hypermobility
Cough or strain
Vesical Leak Point Pressure(VLPP)
• The bladder is filled with 150 ml • The patient coughs or strains• VLPP = Pves at leakage• Low VLPP = intrinsic sphincter
deficiency
A means of quantitating intrinsic
sphincter strength
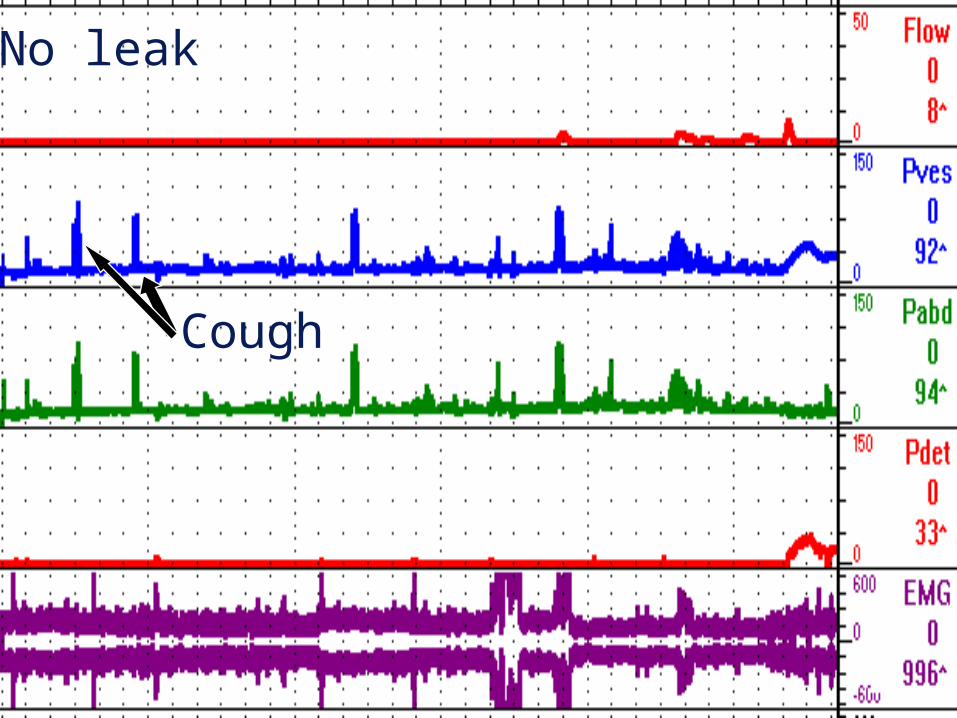
RwnNo leak
Cough

Rwn
VLPP
leak
Cough
VLPP = 45 cm H20Qtip = 0 > 10O

Mixed Stress & Urge Incontinence
• Difficult diagnostic problem
•“If I wait too long, I leak…”
• Relative severity of each
• Differential diagnosis:
• Stress hyperreflexia
• SUI & DO
• SUI & sensory urgency

Voi
Rbn
Involuntary detrusor contraction Incontinent
VLPP = 60

Formulating a Treatment Plan
• Diary • Pad test• Patient activity level & lifestyle• VLPP• Q-tip angle• Bother index• Patient preferences
Urodynamic Diagnoses
• Urethral obstruction
• Impaired detrusor contractility
• Detrusor overactivity
• Low bladder compliance
• Sensory urgency
• Learned voiding dysfunction
Female Urethral Obstruction
• High detrusor pressure:Pdet@Qmax > 20 cm H20
• Low uroflow:Qmax < 15 ml/S
• Site of obstruction = narrowest point of urethra during voiding

Urethral Obstruction: 5 Main Causes in Women
• Pelvic prolapse• Urethral diverticulum• Urethral stricture• Bladder neck obstruction• Pelvic floor dysfunction• DESD

0
20
40
60
80
100
120
140
160
0 10 20 30 40 50
pd
et.
ma
x (
cm
/H
2 O
)
Moderate Obstruction (Type II)
Severe Obstruction (Type III)
Mild Obstruction (Type I)
Unobstructed (Type 0)
Free Flow Qmax (ml/S)

Urodynamic Diagnoses
• Urethral obstruction
• Impaired detrusor contractility
• Detrusor overactivity
• Low bladder compliance
• Sensory urgency
• Learned voiding dysfunction

• Idiopathic
• Neurogenic
• Overdistension
• Decompensation
• Pharmacologic
• Psychologic
Etiology Of Impaired Detrusor Contractility
Urodynamic Diagnoses
• Urethral obstruction
• Impaired detrusor contractility
• Detrusor overactivity
• Low bladder compliance
• Sensory urgency
• Learned voiding dysfunction
Detrusor Overactivity• Hyperreflexia = neurologic
stroke Parkinson's disease multiple sclerosis transverse myelopathy
• Instability = non–neurologic urinary tract infection urethral obstruction bladder cancer bladder stones idiopathic

Urodynamic Diagnoses
• Urethral obstruction
• Impaired detrusor contractility
• Detrusor overactivity
• Low bladder compliance
• Sensory urgency
• Learned voiding dysfunction
BLADDER COMPLIANCE• The ratio of a small change in bladder
volume to a small change in detrusor pressure
• bladder vol. = bladder compliance pdet
• A measure of bladder wall "stiffness”
• High filling pressures are more clinically relevant

Causes of Low Bladder Compliance
• Myelodysplasia
• Thoracolumbar SCI
• Indwelling catheter
• Bladder surgery
• Urethral obstruction

DS
Stop filling
Involuntary detrusor contraction
Vesico-ureteral reflux

Urodynamic Diagnoses
• Urethral obstruction
• Impaired detrusor contractility
• Detrusor overactivity
• Low bladder compliance
• Sensory urgency
• Learned voiding dysfunction

SENSORY URGENCY
• An uncomfortable urge to void unassociated with detrusor overactivity
• Synonymous with hypersensitive bladder and painful bladder syndromes

Urodynamic Diagnoses
• Urethral obstruction
• Impaired detrusor contractility
• Detrusor overactivity
• Low bladder compliance
• Sensory urgency
• Learned voiding dysfunction
Learned Voiding Dysfunction
• Voluntary or involuntary, conscious
or unconscious contractions of the
striated urethral musculature
• Inability to relax the striated urethral
muscles
• Inability to relax the smooth urethral
muscles

ml/S
20
10
Uroflow
Seconds
Acquired voiding dysfunction

Conclusions
• LUTS are fairly non-specific
• Very poor correlation between sx &underlying pathophysiology
• So, the more complete the workup, the greater the likelihood of attaining the correct diagnosis

Conclusions
• Essential ingredients of a good w/up:– Focused history & exam– Clear understanding of patient complaints– Bladder diary– Q & PVR– Videourodynamics is the gold standard– Cystoscopy & upper tract imaging when indicated