-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
1/35
Diagnostic and Management
Approach of BardycardiaBudi Yuli Setianto, MD, PhD
FIHA, FINASIM, FAsCC, FAPSIC
Department of Cardiology and Vasculer Medicine Faculty
ofMedicine Gadjah Mada University-Functional Medical StaffSardjito
Hospital Yogyakarta
1
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
2/35
Case Scenario
An 80-year-old woman reports
feeling weak and short of breath
for 2 hours while walking shortdistances. She feels
exhausted
moving from the car to the ED
stretcher. On physical exam she
is pale and sweaty; HR = 35 bpm;BP = 90/60 mm Hg; RR = 18
rpm.
Rhythm: see next slide.
2
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
3/35
80-Year-Old Woman:
Symptomatic Bradycardia
Identify A, B, and C
Which one is most likely
to be her rhythm?
3
A
B
C
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
4/35
Rhythms to Learn
Sinus bradycardia
Heart blocks
1stdegree
2nddegree type I
2nddegree type II
3rddegree
4
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
5/35
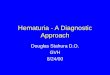
Cardiac Conduction System 1
5
Left bundle branch
Posterior division
Anterior division
Purkinje fibersRight bundle branch
Bundle of His
AV node
Internodal pathways
Sinus node
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
6/35
Cardiac Conduction System 2
6
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
7/35
Rates of Intrinsic
Cardiac Pacemakers
Primary pacemaker
Sinus node (60-100 bpm)
Escape (Subsidiary) pacemakers
AV junction (40-60 bpm)
Ventricular (
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
8/35
8
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
9/35
Determining the Rate
9
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
10/35
Determining the Rate
10
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
11/35
Analyzing Rhythm Strips
Key questions
Are QRS complexes present?
Are P waves present?
How is the P wave related to the
QRS complex?
11
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
12/35
Relationship of P Waves and QRS
Complexes
Every P wave is followed by a QRS complex
with a normal PR interval
Every P wave is followed by a QRS complex but
the PR interval is prolonged
Some P waves are notfollowed by a QRS
complex; more P waves than QRS complexes
12
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
13/35
What Is This Rhythm?
13
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
14/35
Sinus Bradycardia
14
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
15/35
What Is This Rhythm?
15
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
16/35
First Degree AV Block
16
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
17/35
Diagnosis?
17
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
18/35
Second Degree AV Block Type I
18
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
19/35
Diagnosis?
19
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
20/35
Second Degree AV Block Type II
20
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
21/35
What Is This Rhythm?
21
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
22/35
Third Degree AV Block Type III
22
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
23/35
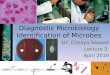
Differentiation of Second- and
Third-Degree AV Blocks
23
More Ps than QRSs
PR fixed?
no
QRSs thatlook alikeregular?
no
yes
yes
yes
2nd-degree AV blockFixed
Mobitz II
3rd-degree AV block
2nd-degree AV blockVariableMobitz I
Wenckebach
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
24/35
Bradycardia Algorithm (1 of 2)
24
Bradycardia
Heart Rate less than 60 bpm andinadequate for clinical
condition
Maintain patent airway; assist breathing as needed
Give oxygen
Monitor ECG (identify rhythm), blood pressure, oximetry
Establish IV access
Serious signs or symptoms of poor
perfusion caused by the bradycardia
(eg. acute altered mental status, ongoing chest pain,
hypotension or other signs of shock)
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
25/35
Bradycardia Algorithm (2 of 2)
25
Observe/Monitor
Prepare for transvenous pacing Treat contributing causes
Consider expert consultation
PoorPerfusion
AdequatePerfusion
Prepare for transcutaneous
pacing;use without delay for
high degree block (type II
second -degree block or third-
degree AV block)
Consider Atropine 0.5 mg/IV
while awaiting pacer. May
repeat to a total dose of 3 mg. If
ineffective, begin pacing.
Consider Epinephrine (2 to 10
g/min) or dopamine (2 to 10
g/kg/min infusion while
awaiting pacer or if pacing
ineffective.
Reminders
If pulseless arrest develops go to
Pulseless Arrest Algorithm Search for and treat possible
contributing
factors:
Hypovolemia
Hypoxia
Hydrogen ion (acidosis)
Hypo/Hyper-kalemia
Hypoglycemia Hypothermia
Toxins
Tamponade, cardiac
Tension pneumothorax
Thrombosis (coronary or
pulmonary)
Trauma (hypovolemia, inc ICP)
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
26/35
26
What Is This Rhythm?
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
27/35
Treatment?
27
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
28/35
Treatment?
28
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
29/35
Transcutaneous Pacing
29
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
30/35
Indications for
Transcutaneous Pacing
Hemodynamically unstable bradycardias
In the setting of AMI: sinus node dysfunction,
type II 2nd-degree block, 3rd-degree heart
block
Bradycardia with symptomatic ventricular
escape beats
30
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
31/35
Transcutaneous Pacing
31
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
32/35
Transcutaneous Pacing
The pacing rate is set at 80 beats per minute.
In conscious bradycardic patients, pacing isbegun in the demand
mode at rates slightly faster
than the native rhythm and at minimal currentoutput
The current is gradually increased by 5 to 10 mAat a time until
cardiac capture is documented,
which defines the pacing threshold. The finalcurrent output
should be set at the pacingthreshold or 5 to 10 mA above it.
32
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
33/35
Transcutaneous Pacing
In the setting of a bradysystolic arrest or with
unconscious patients, it is recommended to turn
the stimulating current to maximal output (200
mA) to ensure ventricular capture
Once capture is achieved, the current may be
gradually decreased until loss of capture, whichdefines the
pacing current threshold
33
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
34/35
Transcutaneous Pacing
34
-
7/25/2019 Diagnostic and Management Approach of
Bardycardia_dr.yuli
35/35
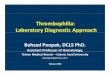
Transcutaneous Pacing:
Capture vs No Capture
35
Pacing below threshold:no capture
Pacing above threshold:with capture
Pacing Spike
Capture: Spike + broad QRS
QRS: opposite polarity
25 Feb 88 Lead I Size 1.0 HR=41
25 Feb 88 Lead I Size 1.0 HR=43 35 mA
25 Feb 88 Lead I Size 1.0 HR=71 60 mA
Bradycardia: No Pacing
Pacing Below Threshold (35 mA): No Capture
Pacing Above Threshold (60 mA): With Capture (Pacing-PulseMarker
)
Bradycardia: no pacing