Embed Size (px)
Citation preview

Diagnostic and emergency Diagnostic and emergency care for life-threatening care for life-threatening
injuries of the injuries of the cardiovascular systemcardiovascular system
Prepared by:Prepared by:C.m.s., assistant professor of C.m.s., assistant professor of
emergency medical care emergency medical care KSMUKSMU
A.R. AlpyssovaA.R. Alpyssova

The purpose of the lectureThe purpose of the lecture
After completing the lecture, students should After completing the lecture, students should focus on issues of diagnosis and emergency focus on issues of diagnosis and emergency treatment for life-threatening injuries of the treatment for life-threatening injuries of the cardiovascular system in the amount of the first cardiovascular system in the amount of the first medical care (doctor's line crews), and depending medical care (doctor's line crews), and depending on the patient - in the amount of specialized care on the patient - in the amount of specialized care (intensive care team, intensive team therapy).(intensive care team, intensive team therapy).

Lecture planLecture plan
Coronary artery disease: definition, classificationCoronary artery disease: definition, classification Sudden cardiac death.Sudden cardiac death. Unstable angina.Unstable angina. Myocardial infarction.Myocardial infarction. Acute disorders of cardiac rhythm and conductionAcute disorders of cardiac rhythm and conduction Pulmonary edema, acute left ventricular failurePulmonary edema, acute left ventricular failure
hypertensive crisishypertensive crisis

CHDCHDCHD (coronary heart disease) - an acute or chronic CHD (coronary heart disease) - an acute or chronic heart disease caused by a decrease or cessation of heart disease caused by a decrease or cessation of delivery of blood to the myocardium.delivery of blood to the myocardium.
Classification of CHD Classification of CHD 1- STENOKARDIYA 1- STENOKARDIYA1.Unstable angina1.Unstable angina 1.1. For the first time emerged 1.1. For the first time emerged 1.2. progressing 1.2. progressing 1.3. Spontaneous (angiospastic, variant, 1.3. Spontaneous (angiospastic, variant, Printsmetalla)Printsmetalla)Early post-infarction angina (up to two weeks)Early post-infarction angina (up to two weeks)2. angina2. angina(With functional class 1-4)(With functional class 1-4)

2- Myocardial Infarction:2- Myocardial Infarction: 1. Depths of defeat 1. Depths of defeat 1.1Transmural (includes macrofocal, Q-attack) 1.1Transmural (includes macrofocal, Q-attack) 1.2.Subendocardial (including subendocardial, 1.2.Subendocardial (including subendocardial, mural)mural)2. With the flow and the localization2. With the flow and the localization2.1 Acute myocardial2.1 Acute myocardial 1) anterior wall myocardial 1) anterior wall myocardial 2) lower wall of the myocardium 2) lower wall of the myocardium 3) refined the localization of other 3) refined the localization of other 4) unspecified location 4) unspecified location 2.2. Repeated myocardial infarction (with 72 2.2. Repeated myocardial infarction (with 72 hours. Up to 28 days from the start of AMI)hours. Up to 28 days from the start of AMI) 1) anterior wall myocardial 1) anterior wall myocardial 2) lower wall of the myocardium 2) lower wall of the myocardium 3) refined the localization of other 3) refined the localization of other 4) unspecified location 4) unspecified location

3. Acute coronary heart disease unspecified3. Acute coronary heart disease unspecified (Sudden cardiac death up to 6 hours) (Sudden cardiac death up to 6 hours)4. Chronic ischemic heart disease4. Chronic ischemic heart disease 1.1 atherosclerotic cardio 1.1 atherosclerotic cardio 1.2. of past myocardial infarction (PMI) 1.2. of past myocardial infarction (PMI) 1.3.anevrizma of heart 1.3.anevrizma of heart 1.4.undecease myocardial ischemia 1.4.undecease myocardial ischemia 1.5. Intermediate coronary syndrome 1.5. Intermediate coronary syndrome

Sudden cardiac deathSudden cardiac death
Sudden cardiac death (the primary respiratory arrest) - Sudden cardiac death (the primary respiratory arrest) - a death in the presence of witnesses, which came a death in the presence of witnesses, which came immediately or within 6 (even one) hours, most often immediately or within 6 (even one) hours, most often caused by ventricular fibrillation and no signs that caused by ventricular fibrillation and no signs that allow to put other than coronary heart disease allow to put other than coronary heart disease diagnosis.diagnosis. The most common cause of sudden death is The most common cause of sudden death is myocardial infarction.myocardial infarction. The main mechanisms for sudden cardiac death The main mechanisms for sudden cardiac death are:are:-ventricular fibrillation (VF)-ventricular fibrillation (VF)-ventricular flutter-ventricular flutter-asystole cardiac-asystole cardiac-electromechanical dissociation cardiac-electromechanical dissociation cardiac

The main diagnostic criteria for sudden death:The main diagnostic criteria for sudden death: lack of consciousnesslack of consciousness absence of respiration or the appearance of absence of respiration or the appearance of
breathing agonal typebreathing agonal type lack of pulse in the carotid arterieslack of pulse in the carotid arteries
dilated pupils (if not done neyroleptanalgeziya dilated pupils (if not done neyroleptanalgeziya not take drugs, no anesthesia was given, no not take drugs, no anesthesia was given, no hypoglycemia)hypoglycemia)
the appearance of a pale gray color of skin.the appearance of a pale gray color of skin.

ECG changes during clinical death:ECG changes during clinical death:ventricular fibrillation recorded chaotic, irregular, ventricular fibrillation recorded chaotic, irregular, sharply deformed ventricular waves, varying in sharply deformed ventricular waves, varying in height, shape, widthheight, shape, widthwith ventricular flutter ventricular waves are with ventricular flutter ventricular waves are more or less correct form, highlight the complex more or less correct form, highlight the complex QRS, the segment ST, T wave is not possible, the QRS, the segment ST, T wave is not possible, the isoelectric line is missingisoelectric line is missingasystole in the heart on ECG is determined by the asystole in the heart on ECG is determined by the contour line, any wave or missing teethcontour line, any wave or missing teethwith electromechanical dissociation rate can with electromechanical dissociation rate can register a rare sinus, nodal rhythm, which goes register a rare sinus, nodal rhythm, which goes into idioventricular, then alternatedinto idioventricular, then alternatedby asystoleby asystole

Emergency care for sudden cardiac death:Emergency care for sudden cardiac death: Cardiopulmonary resuscitation is performed in Cardiopulmonary resuscitation is performed in
two stages:two stages: 1 - stage - reconstruction of the airway, artificial 1 - stage - reconstruction of the airway, artificial
ventilation, chest compressions (usually ABC)ventilation, chest compressions (usually ABC) 2 - stage - an electrical defibrillation, drug 2 - stage - an electrical defibrillation, drug
therapytherapy When sudden cardiac death, acute management When sudden cardiac death, acute management
should begin with immediate defibrillation (if should begin with immediate defibrillation (if conditions permit). If not using an conditions permit). If not using an electrocardiogram to establish the form of cardiac electrocardiogram to establish the form of cardiac arrest, you must still perform defibrillation, ie, it is arrest, you must still perform defibrillation, ie, it is produced "blindly", without wasting time on produced "blindly", without wasting time on diagnostic activities and registration of the ECG. diagnostic activities and registration of the ECG. In the absence of a defibrillator performed In the absence of a defibrillator performed resuscitation measures in a such sequence.resuscitation measures in a such sequence.

Immediately put the patient face up on the hard Immediately put the patient face up on the hard bed with raised legs, with thrown back head.bed with raised legs, with thrown back head.
Sharp punch to the bottom of the sternum once Sharp punch to the bottom of the sternum once or twice.or twice.
-Ensure access of air into the airways-Ensure access of air into the airways -Perform artificial respiration means "mouth-to -Perform artificial respiration means "mouth-to
mouth"mouth" -Along with mechanical ventilation to produce -Along with mechanical ventilation to produce
chest compressions to circulate blood and provide chest compressions to circulate blood and provide access to a veinaccess to a vein
-Produce electrical defibrillation.-Produce electrical defibrillation. -Carry medication and use 100% oxygen-Carry medication and use 100% oxygen

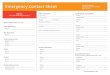
Algorithm of action at ventricular fibrillationAlgorithm of action at ventricular fibrillation(scheme of the American Heart Association)(scheme of the American Heart Association)
Ventricular fibrillation or sustained ventricular tachycardia without a pulse.Ventricular fibrillation or sustained ventricular tachycardia without a pulse.
Check the pulse of the carotid artery. If the pulse is notCheck the pulse of the carotid artery. If the pulse is not
Precardiac blowPrecardiac blow
Check the pulse of the carotid artery. If the pacient hasn’t the pulse.Check the pulse of the carotid artery. If the pacient hasn’t the pulse.
Chest compressions and ventilation, while preparing difibrillatorChest compressions and ventilation, while preparing difibrillator
Determine the type of arrhythmia (ventricular fibrillation or ventricular tachycardia) on the monitorDetermine the type of arrhythmia (ventricular fibrillation or ventricular tachycardia) on the monitor
Defibrillation discharge 200 JDefibrillation discharge 200 J
Defibrillation discharge 200-300 JDefibrillation discharge 200-300 J

Defibrillation discharge up to 360 joulesDefibrillation discharge up to 360 joules
If no pulse - chest compressions and mechanical ventilationIf no pulse - chest compressions and mechanical ventilation
Establish intravenous infusionEstablish intravenous infusion
Epinephrine 0.5-1 mg intravenouslyEpinephrine 0.5-1 mg intravenously
Intubation of traheyaIntubation of traheya
Defibrillation discharge up to 360 jouleDefibrillation discharge up to 360 joule
Lidocaine 1 mg / kg intravenouslyLidocaine 1 mg / kg intravenously
Defibrillation discharge up to 360 joulesDefibrillation discharge up to 360 joules

Bretily 5 mg / kg intravenously Bretily 5 mg / kg intravenously
Perhaps the use of sodium bicarbonate Perhaps the use of sodium bicarbonate
Defibrillation charge to 360 joules Defibrillation charge to 360 joules
Bretily 10 mg / kg intravenouslyBretily 10 mg / kg intravenously
Defibrillation discharge up to 360 joules Defibrillation discharge up to 360 joules
Again lidocaine or bretily Again lidocaine or bretily
Defibrillation discharge up to 360 joules Defibrillation discharge up to 360 joules

Note:Note:A- Ventricular tachycardia without pulse is treated as A- Ventricular tachycardia without pulse is treated as ventricular fibrillation;ventricular fibrillation;
B - After every discharge pulse check and rhythm. If B - After every discharge pulse check and rhythm. If ventricular fibrillation recurs, use category, which previously ventricular fibrillation recurs, use category, which previously gave effect;gave effect;
C - the injection of adrenaline to repeat every 5 minutesC - the injection of adrenaline to repeat every 5 minutes D- endotracheal intubation is desirable and should be carried D- endotracheal intubation is desirable and should be carried
out simultaneously with other resuscitation at the earliest out simultaneously with other resuscitation at the earliest possible time. However, if mechanical ventilation can be possible time. However, if mechanical ventilation can be performed without intubation, the initial stages of resuscitation performed without intubation, the initial stages of resuscitation and defibrillation is more important than the injection of and defibrillation is more important than the injection of adrenalin;adrenalin;
E - some doctors prefer to re-injection of lidocaine (0.5 mg E - some doctors prefer to re-injection of lidocaine (0.5 mg bolus every 8 minutes until a total dose of 8 mg / kg);bolus every 8 minutes until a total dose of 8 mg / kg);

F - the injection of sodium bicarbonate is usually not F - the injection of sodium bicarbonate is usually not recommended, since its effectiveness is questionable. At recommended, since its effectiveness is questionable. At this stage it is possible to introduce it in a dose of 1 mEq / this stage it is possible to introduce it in a dose of 1 mEq / kg, ie 2 ml of 4% solution / kg. If you decide to resort to the kg, ie 2 ml of 4% solution / kg. If you decide to resort to the bicarbonate, it can be injected every 10 minutes at a dose bicarbonate, it can be injected every 10 minutes at a dose of 1 ml of 4% solution / kg.of 1 ml of 4% solution / kg.

AsystoleAsystole If the nature of the arrhythmia is unknown and possible ventricular fibrillation, defibrillation If the nature of the arrhythmia is unknown and possible ventricular fibrillation, defibrillation conduct, as in ventricular fibrillationconduct, as in ventricular fibrillation
If asystole is installedIf asystole is installed
Continue chest compressions and mechanical ventilationContinue chest compressions and mechanical ventilation
Establish intravenous infusionEstablish intravenous infusion Epinephrine 0.5-1 mg intravenously Epinephrine 0.5-1 mg intravenously
intubate the tracheaintubate the trachea
Atropine 1 mg intravenously (repeated after 5 minutes)Atropine 1 mg intravenously (repeated after 5 minutes)
Perhaps the use of sodium bicarbonatePerhaps the use of sodium bicarbonate Perhaps the use of pacing Perhaps the use of pacing

electromechanical dissociationelectromechanical dissociation Continue to external cardiac massage and artificial Continue to external cardiac massage and artificial ventilationventilation
Establish intravenous infusion Establish intravenous infusion Epinephrine 0.5-1 mg intravenously Epinephrine 0.5-1 mg intravenously intubation intubation Perhaps the use of pacing Perhaps the use of pacing A refuse of the CPR is possible:A refuse of the CPR is possible:
in the terminal stage of an incurable diseasein the terminal stage of an incurable disease if from the moment of cardiac arrest lasted more than if from the moment of cardiac arrest lasted more than
5 minutes5 minutes

Termination of CPR is possible if:Termination of CPR is possible if:During the measure appears, that CPR does not shown to the During the measure appears, that CPR does not shown to the patient patient In using all available methods, doesn’t noticed the signs of In using all available methods, doesn’t noticed the signs of effectiveness of CPR during 30 min. effectiveness of CPR during 30 min. Observed frequentative stops of heart, that is unyield to any Observed frequentative stops of heart, that is unyield to any medical influences.medical influences.

AnginaAngina Angina pectoris - clinical form of IHD (attack of Angina pectoris - clinical form of IHD (attack of retrosternal pain that occurs when non-compliance in retrosternal pain that occurs when non-compliance in myocardial oxygen demand and its delivery)myocardial oxygen demand and its delivery)Unstable angina Unstable angina coronary flow determines the stage at coronary flow determines the stage at which the risk of myocardial infarction and sudden death which the risk of myocardial infarction and sudden death increases significantly.increases significantly. Diagnostic criteria for unstable anginaDiagnostic criteria for unstable angina1. For the first time emerged angina (up to 1 month from 1. For the first time emerged angina (up to 1 month from the appearance of the first attack)the appearance of the first attack)2.Progressive angina (angina increased pain intensity, 2.Progressive angina (angina increased pain intensity, duration and frequency of attacks)duration and frequency of attacks)3.Spontanious (angiospastic, variant, Printsmetalla)3.Spontanious (angiospastic, variant, Printsmetalla)4.Early postinfarction angina (14 days from myocardial 4.Early postinfarction angina (14 days from myocardial infarction)infarction)

Treatment program in unstable angina: Treatment program in unstable angina: 1. Pain; 1. Pain; 2. elimination of myocardial ischemia by 2. elimination of myocardial ischemia by
antianginal drugs (nitrates, beta-blockers, antianginal drugs (nitrates, beta-blockers, calcium channel blockers); calcium channel blockers);
3. reduce the risk of acute myocardial infarction 3. reduce the risk of acute myocardial infarction and mortality with help of anticoagulant and and mortality with help of anticoagulant and antiplatelet agents; antiplatelet agents;
4. balloon coronary angioplasty and coronary 4. balloon coronary angioplasty and coronary artery bypass grafting artery bypass grafting

Acute myocardial infractionAcute myocardial infractionMyocardial infarction (MI) - is ischemic necrosis of Myocardial infarction (MI) - is ischemic necrosis of cardiac muscle, which develops as a result of cardiac muscle, which develops as a result of acute failure of coronary circulation.acute failure of coronary circulation. Classification:Classification:*magnitude and depth of lesions of the heart *magnitude and depth of lesions of the heart muscle; muscle; *the nature of the disease;*the nature of the disease;*Localization of MI; *Localization of MI; on the stage of disease; on the stage of disease; *by the presence of complications of myocardial *by the presence of complications of myocardial infarction. infarction. *The magnitude and depth of destruction of *The magnitude and depth of destruction of heart muscle:heart muscle:
transmuraltransmural Not transmural MI.Not transmural MI.

When transmural MI (myocardial infarction with a tooth Q) When transmural MI (myocardial infarction with a tooth Q) captures the focus of necrosis, or the entire thickness of captures the focus of necrosis, or the entire thickness of cardiac muscle of subendocardial myocardial layers to cardiac muscle of subendocardial myocardial layers to subepikardial or most of it, which is reflected on the surface subepikardial or most of it, which is reflected on the surface ECG as the formation of a pathological Q wave or QS ECG as the formation of a pathological Q wave or QS complex in several ECG leads . Hence the synonym of complex in several ECG leads . Hence the synonym of transmural myocardial infarction - "myocardial infarction transmural myocardial infarction - "myocardial infarction with a tooth Q". Typically, such damage to the heart muscle with a tooth Q". Typically, such damage to the heart muscle is extensive enough and focus of necrosis extended to two is extensive enough and focus of necrosis extended to two or more segments of the left ventricle (macrofocal MI).or more segments of the left ventricle (macrofocal MI).
In untransmular MI (myocardial infarction without tooth Q) In untransmular MI (myocardial infarction without tooth Q) captures only the focus of necrosis subendocardial or captures only the focus of necrosis subendocardial or intramural divisions of the left ventricle (LV) and is not intramural divisions of the left ventricle (LV) and is not accompanied by pathological changes of the complex QRS accompanied by pathological changes of the complex QRS ("wave myocardial infarction without Q").("wave myocardial infarction without Q").

By the nature By the nature of course of the disease are of course of the disease are distinguished primary, recurrent and recurrent MI.distinguished primary, recurrent and recurrent MI.PrimaryPrimary MI diagnosed in the absence of MI diagnosed in the absence of anamnestic and instrumental signs of myocardial anamnestic and instrumental signs of myocardial infarction in the past.infarction in the past.Re-infarctionRe-infarction is diagnosed when a patient, in is diagnosed when a patient, in whom there is documented information of past whom there is documented information of past myocardial infarction, there are credible signs of myocardial infarction, there are credible signs of new foci of necrosis.new foci of necrosis.For recurrent For recurrent myocardial infarction clinical myocardial infarction clinical laboratory and instrumental signs of the formation laboratory and instrumental signs of the formation of new foci of necrosis appear in a period of 72 of new foci of necrosis appear in a period of 72 hours (3 days) until 28 days after myocardial hours (3 days) until 28 days after myocardial infarction, ie, before the end of its basic processes infarction, ie, before the end of its basic processes of scarring.of scarring.

Acc.to localization MI distinguished:Acc.to localization MI distinguished:behindseptal (peredneperegorodochny);behindseptal (peredneperegorodochny);behindverhushechny; behindverhushechny; anterolateral; anterolateral; behindbazal (high front);behindbazal (high front); common anterior (septal, apical and lateral);common anterior (septal, apical and lateral);backdiafragmalny (lower);backdiafragmalny (lower);posterolateral; posterolateral; backbazalny; backbazalny; common rear;common rear;IM the right ventricle.IM the right ventricle.

By stage of the disease are distinguished:By stage of the disease are distinguished: acute period - up to 2 hours from the start of it;acute period - up to 2 hours from the start of it; acute period - up to 10 days from the onset of MI;acute period - up to 10 days from the onset of MI; subacute period - from 10 days before the end of 4-8 weeks;subacute period - from 10 days before the end of 4-8 weeks; postinfarction period - usually after 4-8 weeks.postinfarction period - usually after 4-8 weeks.
Sometimes singled out the prodromal period, which corresponds Sometimes singled out the prodromal period, which corresponds to a certain extent, the notion of unstable angina, myocardial to a certain extent, the notion of unstable angina, myocardial infarction complicated by development.infarction complicated by development.
The most common complications of MI include:The most common complications of MI include: acute left ventricular failure (pulmonary edema);acute left ventricular failure (pulmonary edema);
cardiogenic shock;cardiogenic shock; ventricular and supraventricular arrhythmias;ventricular and supraventricular arrhythmias; violations conductivity (CA-blockade, AV block, bundle-branch violations conductivity (CA-blockade, AV block, bundle-branch
block, block);block, block); acute left ventricular aneurysm;acute left ventricular aneurysm; external and internal discontinuities infarction, cardiac external and internal discontinuities infarction, cardiac
tamponade;tamponade; aseptic pericarditis (epistenokarditichesky);aseptic pericarditis (epistenokarditichesky); thromboembolism. thromboembolism.

Diagnostic criteria:Diagnostic criteria:1. complaints and medical history.1. complaints and medical history.The main clinical sign of myocardial infarction is the anginal The main clinical sign of myocardial infarction is the anginal pain.pain.The nature of anginal pain in myocardial infarction is similar The nature of anginal pain in myocardial infarction is similar to that of angina, but it is expressed more strongly in high-to that of angina, but it is expressed more strongly in high-intensity pain is perceived as a "dagger", tearing, tearing, intensity pain is perceived as a "dagger", tearing, tearing, burning, scorching, "a stake through the chest.”burning, scorching, "a stake through the chest.”Pain develops in waves, regularly decreasing, but not Pain develops in waves, regularly decreasing, but not stopping completely.stopping completely. Localization of anginal pain - usually in the chest deep in the Localization of anginal pain - usually in the chest deep in the chest, at least - on the left side of chest or epigastric region.chest, at least - on the left side of chest or epigastric region. Anginal pain radiates to left shoulder, arm, forearm and Anginal pain radiates to left shoulder, arm, forearm and wrist. Top of anginal pain in myocardial infarction - a sudden, wrist. Top of anginal pain in myocardial infarction - a sudden, often in the morning hours, the duration - a few hours.often in the morning hours, the duration - a few hours.Sublingual nitroglycerin re not relieves anginal pain in Sublingual nitroglycerin re not relieves anginal pain in myocardial infarction.myocardial infarction.

Other known variants of the beginning of the Other known variants of the beginning of the IM-asthmatic, IM-asthmatic, abdominal, arrhythmic, and cerebrovascular abdominal, arrhythmic, and cerebrovascular asymptomatic.asymptomatic.
Asthmatic variant Asthmatic variant usually observed in pacients with extensive usually observed in pacients with extensive re-infarction of MI at which by the total destruction of the heart re-infarction of MI at which by the total destruction of the heart muscle is rapidly developing acute left ventricular failure clinic.muscle is rapidly developing acute left ventricular failure clinic.
Abdominal variant Abdominal variant characterized localized pain in the characterized localized pain in the epigastrium and dyspeptic disorders. Most often it develops in epigastrium and dyspeptic disorders. Most often it develops in the lower myocardial infarction.the lower myocardial infarction.
Arrhythmic option Arrhythmic option observing in those cases where the observing in those cases where the clinical. picture is dominated by pronounced disturbances of clinical. picture is dominated by pronounced disturbances of rhythm and conduction - paroxysmal supraventricular or rhythm and conduction - paroxysmal supraventricular or ventricular tachycardia, full A-B blockade.ventricular tachycardia, full A-B blockade.
Cerebrovascular version Cerebrovascular version meets in elderly patients with meets in elderly patients with infringement of brain circulation. May appear faint, dizziness, infringement of brain circulation. May appear faint, dizziness, nausea, vomiting, and sometimes - SMC transient symptoms. nausea, vomiting, and sometimes - SMC transient symptoms. Part of pacients MI proceeds with the minimum or complaints Part of pacients MI proceeds with the minimum or complaints they are absence.they are absence.

Typical symptoms of acute myocardial infarction:Typical symptoms of acute myocardial infarction: anginal painanginal pain inspiratory dyspneainspiratory dyspnea discoloration of the skin (pallor, marbling, cyanosis);discoloration of the skin (pallor, marbling, cyanosis); cold clammy sweats;cold clammy sweats; excitation or inhibition of the patient;excitation or inhibition of the patient; Restlessness;Restlessness; fear of death;fear of death; Polyuria;Polyuria; Physical examination:Physical examination: pale skin;pale skin; cold sweat;cold sweat; heart sounds muffled;heart sounds muffled; Blood pressure decreased slightly, mainly systolic blood Blood pressure decreased slightly, mainly systolic blood
pressure can sometimes slightly raised or infarction may occur pressure can sometimes slightly raised or infarction may occur against the background of a hypertensive crisis;against the background of a hypertensive crisis;
respiratory failure (shortness of breath, feeling short of breath);respiratory failure (shortness of breath, feeling short of breath);

3. Laboratory investigations3. Laboratory investigations Determination of troponin T using the rapid test.Determination of troponin T using the rapid test. 4. Instrumental investigations:4. Instrumental investigations: ECG ECG reveals foci of necrosis in the heart muscle, its depth and reveals foci of necrosis in the heart muscle, its depth and
location, state behindinfarct zone, the dynamics of the process.location, state behindinfarct zone, the dynamics of the process. ECG signs:ECG signs:
The presence of pathologic wave Q.The presence of pathologic wave Q. R-wave amplitude decrease on approaching the zone of R-wave amplitude decrease on approaching the zone of
necrosis.necrosis. Discordant QRS complex and T waveDiscordant QRS complex and T wave
appearance of left bundle branch block.appearance of left bundle branch block. When Subendocardial MI on ECG is absence the dent Q, was When Subendocardial MI on ECG is absence the dent Q, was
observed the lowering ST-segment on 2 mm and more below observed the lowering ST-segment on 2 mm and more below izoelectric line acc-ing to poisons, the inversion of the dent T.izoelectric line acc-ing to poisons, the inversion of the dent T.
5. Differential Diagnosis:5. Differential Diagnosis: Most often should differentiated MI the infarction from Most often should differentiated MI the infarction from
prolonged attacks of angina, pulmonary embolism, acute prolonged attacks of angina, pulmonary embolism, acute abdominal diseases, dissecting aortic aneurysm.abdominal diseases, dissecting aortic aneurysm.

List of main and additional diagnostic measures:List of main and additional diagnostic measures: 1. Monitoring of cardiac rhythm 1. Monitoring of cardiac rhythm 2. Pulse oximetry. 2. Pulse oximetry. Tactics of giving a medical care: Tactics of giving a medical care:1. treatment goals: 1. treatment goals: stabilization of vital body functions stabilization of vital body functions (maintenance of stable hemodynamics, heart rate (maintenance of stable hemodynamics, heart rate correction).correction).2. non-drug treatment:2. non-drug treatment: 1. Physical and emotional rest. 1. Physical and emotional rest.3. drug treatment3. drug treatment1. Nitroglycerine, pills or spray at 0.4-0.5 mg sublingually, 1. Nitroglycerine, pills or spray at 0.4-0.5 mg sublingually, with lack of effectiveness - to repeat, izoket-aerosol dose of with lack of effectiveness - to repeat, izoket-aerosol dose of 1-2, with lack of effectiveness - to repeat.1-2, with lack of effectiveness - to repeat.2. Acetylsalicylic acid 325 mg chew2. Acetylsalicylic acid 325 mg chew3. Oxygen therapy.3. Oxygen therapy.

4. For pain relief (depending on the severity of pain, 4. For pain relief (depending on the severity of pain, general condition, age) -general condition, age) - -morphine until 10 mg intravenously tively for 2-4 mg to -morphine until 10 mg intravenously tively for 2-4 mg to relieve pain or symptoms of overdose (decrease in relieve pain or symptoms of overdose (decrease in respiratory rate to 10-12 in 1 minute, pupillary constriction, respiratory rate to 10-12 in 1 minute, pupillary constriction, reduced blood pressure).reduced blood pressure). - Fentanyl, administered in doses of 50 mg intravenously - Fentanyl, administered in doses of 50 mg intravenously slowly in two stages.slowly in two stages.
To conduct the neyroleptanalgeziya narcotic analgesics are To conduct the neyroleptanalgeziya narcotic analgesics are used in conjunction with a neuroleptic (usually by used in conjunction with a neuroleptic (usually by droperidolom).droperidolom).
In view of the effect on blood pressure dose of droperidol is In view of the effect on blood pressure dose of droperidol is chosen according to its original value: the systolic pressure chosen according to its original value: the systolic pressure of 100-110 mm Hg. - 2.5 mg, 120-160 mm Hg. - 5 mg, more of 100-110 mm Hg. - 2.5 mg, 120-160 mm Hg. - 5 mg, more than 160-180 mm Hg. - Up to 10 mg.than 160-180 mm Hg. - Up to 10 mg.
If you can not use narcotic analgesics or in their absence If you can not use narcotic analgesics or in their absence should be inject the tramadol.should be inject the tramadol.

5. In order to improve coronary blood flow infusion of 5. In order to improve coronary blood flow infusion of izosorbit dinitrate 10 mg intravenously, drip, slowly, under izosorbit dinitrate 10 mg intravenously, drip, slowly, under the control of blood pressurethe control of blood pressure6. In the absence of contraindications - Atenolol 50-100 mg 6. In the absence of contraindications - Atenolol 50-100 mg orally.orally.7. In order to restore coronary blood flow:7. In order to restore coronary blood flow:- Streptokinase 1.5 million units in / tively drip for 30 minutes - Streptokinase 1.5 million units in / tively drip for 30 minutes after the jet injection of 30 mg of prednisolone;after the jet injection of 30 mg of prednisolone;aktilize, alteplase, tissue plasminogen activator: introduced aktilize, alteplase, tissue plasminogen activator: introduced for 90 minutes in three stages, 15 mg / bolus, 50 mg / drip for 90 minutes in three stages, 15 mg / bolus, 50 mg / drip for 30 minutes and 35 mg / drip for 60 minutes, at the same for 30 minutes and 35 mg / drip for 60 minutes, at the same time should be the appointment of heparin at a dose of 5000 time should be the appointment of heparin at a dose of 5000 ED / bolus and aspirin 160 - 300 mgED / bolus and aspirin 160 - 300 mg
5. Indications for hospitalization 5. Indications for hospitalization of patients with AMI of patients with AMI admitted to intensive care or cardiology department.admitted to intensive care or cardiology department.6. Preventive measures 6. Preventive measures include blood pressure include blood pressure monitoring, heart rate, heart rhythm disturbances and monitoring, heart rate, heart rhythm disturbances and correction occurred.correction occurred.

Acute disorders of cardiac rhythm and conduction.Acute disorders of cardiac rhythm and conduction. Heart arrhythmias Heart arrhythmias - disturbances of frequency, - disturbances of frequency, rhythm and / or sequence of heartbeats: acceleration rhythm and / or sequence of heartbeats: acceleration (tachycardia) or slowing (bradycardia) rhythm, premature (tachycardia) or slowing (bradycardia) rhythm, premature contractions (extrasystoles), disorganization of the contractions (extrasystoles), disorganization of the rhythmic activity (atrial fibrillation), etc.rhythmic activity (atrial fibrillation), etc.
Tachycardia - three or more consecutive cardiac cycles with Tachycardia - three or more consecutive cardiac cycles with a frequency of 100 or more per minute.a frequency of 100 or more per minute.
Unstable tachycardia - tachycardia lasting less than 30 Unstable tachycardia - tachycardia lasting less than 30 seconds.seconds.
Sustained tachycardia - tachycardia lasting more than 30 Sustained tachycardia - tachycardia lasting more than 30 seconds.seconds.
Paroxysm - a form of paroxysmal tachycardia with a clearly Paroxysm - a form of paroxysmal tachycardia with a clearly defined beginning and end of the attack.defined beginning and end of the attack.
Bradycardia - three or more consecutive cardiac Nicla with Bradycardia - three or more consecutive cardiac Nicla with frequency of less than 60 minutes.frequency of less than 60 minutes.

ETIOLOGY AND PATHOGENESIS ETIOLOGY AND PATHOGENESIS Arrhythmias are caused by violation:Arrhythmias are caused by violation:- Education excitation (automaticity)- Education excitation (automaticity)- Conduction excitement (conduction)- Conduction excitement (conduction)- A combination of these components- A combination of these components
Acute disorders of rhythm and conduction disturbances Acute disorders of rhythm and conduction disturbances occurs:occurs:as a complication of diseases of the cardiovascular system:as a complication of diseases of the cardiovascular system:
Coronary heart disease (including myocardial infarction, Coronary heart disease (including myocardial infarction, postinfarction cardio);postinfarction cardio);rheumatic heart diseases,rheumatic heart diseases,primary and secondary cardiomyopathies,primary and secondary cardiomyopathies,myocarditis.myocarditis.Background:Background:- Hypertension- Hypertension-congestive heart failure-congestive heart failure-electrolyte disorders (eg, hypokalemia, hypocalcemia, -electrolyte disorders (eg, hypokalemia, hypocalcemia, hypomagnesemia).hypomagnesemia).

In consequence of congenital anomalies:In consequence of congenital anomalies:- Conducting system (Wolff-Parkinson-White syndrome - Conducting system (Wolff-Parkinson-White syndrome - WPW, Lawn Genonga-Levine-LGL)- WPW, Lawn Genonga-Levine-LGL)-repolarization process (Romano-Ward syndrome, -repolarization process (Romano-Ward syndrome, Dzhervela-Lange-Nielsen, Brugada).Dzhervela-Lange-Nielsen, Brugada).
When you receive drugs -When you receive drugs --cardiac glycosides,-cardiac glycosides,-theophylline;-theophylline;-drugs prolong the interval QT (eg, antiarrhythmic -drugs prolong the interval QT (eg, antiarrhythmic drugs: amiodarone, sotalol, quinidine);drugs: amiodarone, sotalol, quinidine);-psychoactive drugs, etc. -psychoactive drugs, etc.
When taking alcohol or excessive consumption of When taking alcohol or excessive consumption of caffeine-containing beverages.caffeine-containing beverages.
When extracardiac pathology (lung, thyroid, infectious When extracardiac pathology (lung, thyroid, infectious diseases).diseases).

CLASSIFICATIONCLASSIFICATIONOn UMC all arrhythmias and conduction (supraventricular On UMC all arrhythmias and conduction (supraventricular and ventricular arrhythmias, conduction abnormalities) to and ventricular arrhythmias, conduction abnormalities) to differentiate between requiring and not requiring differentiate between requiring and not requiring emergency treatment.emergency treatment.
Supraventricular arrhythmias requiring urgent Supraventricular arrhythmias requiring urgent treatmenttreatmentParoxysmal supraventricular tachycardiaParoxysmal supraventricular tachycardiaParoxysmal atrial fibrillation lasting less than 48 hours, Paroxysmal atrial fibrillation lasting less than 48 hours, regardless of the presence of impaired hemodynamicsregardless of the presence of impaired hemodynamicsParoxysmal atrial fibrillation lasting longer than 48 hours, Paroxysmal atrial fibrillation lasting longer than 48 hours, accompanied by tachysystole ventricular hemodynamics accompanied by tachysystole ventricular hemodynamics and the violationand the violationStable (persistent) atrial fibrillation, the ventricles and Stable (persistent) atrial fibrillation, the ventricles and accompanied tachysystole violation of hemodynamicsaccompanied tachysystole violation of hemodynamics

Permanent form of atrial fibrillation, the ventricles Permanent form of atrial fibrillation, the ventricles and accompanied tachysystole violation of and accompanied tachysystole violation of hemodynamics.hemodynamics.
Paroxysmal form of atrial flutter lasting less than Paroxysmal form of atrial flutter lasting less than 48 hours48 hours
Paroxysmal form of atrial flutter lasting more than Paroxysmal form of atrial flutter lasting more than 48 hours, accompanied by ventricular 48 hours, accompanied by ventricular tachysystole (1:1 or 2:1) and hemodynamic tachysystole (1:1 or 2:1) and hemodynamic instabilityinstability

Not requiring emergency treatmentNot requiring emergency treatmentSinus tachycardiaSinus tachycardiaSupraventricular (including atrial) beatsSupraventricular (including atrial) beatsParoxysmal atrial fibrillation lasting longer than 48 hours, not Paroxysmal atrial fibrillation lasting longer than 48 hours, not accompanied by tachysystole ventricular hemodynamics and the accompanied by tachysystole ventricular hemodynamics and the violationviolationStable (persistent) atrial fibrillation, not accompanied by tachysystole Stable (persistent) atrial fibrillation, not accompanied by tachysystole ventricular hemodynamics and the violationventricular hemodynamics and the violationPermanent form of atrial fibrillation, is not accompanied by Permanent form of atrial fibrillation, is not accompanied by tachysystole and ventricular hemodynamics violation mtachysystole and ventricular hemodynamics violation mParoxysmal form of atrial flutter lasting more than 48 hours, not Paroxysmal form of atrial flutter lasting more than 48 hours, not accompanied by tachysystole ventricular hemodynamics and the accompanied by tachysystole ventricular hemodynamics and the violationviolationClinical manifestations of hemodynamic disorders: acute left Clinical manifestations of hemodynamic disorders: acute left ventricular failure (arterial hypotension, pulmonary edema), coronary ventricular failure (arterial hypotension, pulmonary edema), coronary insufficiency (anginal attack, signs of myocardial ischemia on ECG), a insufficiency (anginal attack, signs of myocardial ischemia on ECG), a disorder of consciousness.disorder of consciousness.

Ventricular arrhythmias requiring urgent Ventricular arrhythmias requiring urgent treatmenttreatmentventricular fibrillationventricular fibrillationSustained monomorphic ventricular tachycardiaSustained monomorphic ventricular tachycardiaSustained polymorphic ventricular tachycardia Sustained polymorphic ventricular tachycardia (including (including torsades depointes, torsades depointes, type (pirouette)type (pirouette)Unstable ventricular tachycardia in patients with Unstable ventricular tachycardia in patients with myocardial infarctionmyocardial infarctionFrequent, steam room, politopnaya, ventricular Frequent, steam room, politopnaya, ventricular premature beats in patients with myocardial premature beats in patients with myocardial infarctioninfarction

Not requiring emergency treatmentNot requiring emergency treatmentventricular extrasystolesventricular extrasystolesReplacement rhythm (accelerated idioventricular Replacement rhythm (accelerated idioventricular rhythm, the rhythm of the AB-connection) with a heart rhythm, the rhythm of the AB-connection) with a heart rate> 50 per minute and with no serious rate> 50 per minute and with no serious
violations of the hemodynamicviolations of the hemodynamicReperfusion arrhythmias after successful thrombolytic Reperfusion arrhythmias after successful thrombolytic therapy in patients with myocardial infarction (slow therapy in patients with myocardial infarction (slow ventricular tachycardia, accelerated idioventricular ventricular tachycardia, accelerated idioventricular rhythm), unaccompanied serious violations of rhythm), unaccompanied serious violations of hemodynamicshemodynamics

Conduction abnormalities requiring emergency treatmentConduction abnormalities requiring emergency treatmentSinus node dysfunction (sick sinus syndrome) with syncope, Sinus node dysfunction (sick sinus syndrome) with syncope, seizures of Morgagni-Adams-Stokes equations with a heart rate seizures of Morgagni-Adams-Stokes equations with a heart rate <40 beats per minute<40 beats per minute
AB block and the degree with syncope, seizures of Morgagni-AB block and the degree with syncope, seizures of Morgagni-Adams-Stokes equations with a heart rate <40 beats per Adams-Stokes equations with a heart rate <40 beats per minuteminute
Complete AB block with syncope, seizures of Morgagni-Adams-Complete AB block with syncope, seizures of Morgagni-Adams-Stokes equations with a heart rate <40 per minuteStokes equations with a heart rate <40 per minute
Sinus node dysfunction without syncope and seizures of Sinus node dysfunction without syncope and seizures of Morgagni-Adams-StokesMorgagni-Adams-Stokes
AB block I degreeAB block I degree AB block II degree without syncope and seizures of Morgagni-AB block II degree without syncope and seizures of Morgagni-
Adams-StokesAdams-Stokes Complete AB block with a heart rate> 40 per minute without Complete AB block with a heart rate> 40 per minute without
syncope and seizures of Morgagni-Adams-Stokessyncope and seizures of Morgagni-Adams-Stokes Mono-, bi-and trifastsikulyarnye block bundle-branch blockMono-, bi-and trifastsikulyarnye block bundle-branch block

CLINICAL PICTURECLINICAL PICTURECardiac rhythm and conduction can occur as Cardiac rhythm and conduction can occur as asymptomatic and manifest striking symptoms asymptomatic and manifest striking symptoms ranging from palpitations, disruptions of the heart ranging from palpitations, disruptions of the heart "flip" and "tumbling" of the heart and ending the "flip" and "tumbling" of the heart and ending the development of severe arterial hypotension, angina, development of severe arterial hypotension, angina, syncope and manifestations of acute heart failure. syncope and manifestations of acute heart failure. Clarification of the nature of arrhythmias and Clarification of the nature of arrhythmias and conduction of the heart is set on the basis of ECGconduction of the heart is set on the basis of ECG

ECG criteria for the diagnosis of cardiac arrhythmias ECG criteria for the diagnosis of cardiac arrhythmias that requires emergency treatment at the stage of the that requires emergency treatment at the stage of the
UMC:UMC:Paroxysmal supraventricular tachycardia.Paroxysmal supraventricular tachycardia.- Rhythm is correct, heart rate 120-250 per minute, QRS - Rhythm is correct, heart rate 120-250 per minute, QRS complexes are narrow (less than 0.12). Depending on the complexes are narrow (less than 0.12). Depending on the nature of the electrophysiological supraventricular tachycardia nature of the electrophysiological supraventricular tachycardia paroxizmal P wave in standard ECG or can not be identified, paroxizmal P wave in standard ECG or can not be identified, merging with the ventricular complex and situated within, or merging with the ventricular complex and situated within, or to register, lying behind the complex to register, lying behind the complex QRScQRSc R-PR-P interval more interval more than 0.1 seconds.than 0.1 seconds.ParoxysmalParoxysmal form of atrial fibrillation (atrial fibrillation), form of atrial fibrillation (atrial fibrillation), 5.0 mm/nB 25.0 im / c5.0 mm/nB 25.0 im / c- Rhythm is wrong, - Rhythm is wrong, QRSQRS complexes are narrow (less than complexes are narrow (less than 0.12). There are no 0.12). There are no PP wave, identifies the "wave of atrial wave, identifies the "wave of atrial fibrillation" - large-scale or smallwave fluctuations of contour, fibrillation" - large-scale or smallwave fluctuations of contour, the frequency of atrial waves - 350 - 600 per minute, the frequency of atrial waves - 350 - 600 per minute, RRRR intervals are vary.intervals are vary.

Auricular flutterAuricular flutter- Rhythm can be regular (at AB-holding from 1:1 - Rhythm can be regular (at AB-holding from 1:1 to 4:1 and more) as well as incorrect if an AB is to 4:1 and more) as well as incorrect if an AB is constantly changing. The frequency of ventricular constantly changing. The frequency of ventricular contractions depends on the degree of AB contractions depends on the degree of AB conduction (often 2:1) and is usually 90-150 per conduction (often 2:1) and is usually 90-150 per minute. minute. QRSQRS complexes are narrow (less than complexes are narrow (less than 0.12). There are no 0.12). There are no PP wave, instead of them to wave, instead of them to reveal the contours sawtooth "flutter waves" reveal the contours sawtooth "flutter waves" (dents (dents FF), most distinct in leads II, III, aVF and V, ), most distinct in leads II, III, aVF and V, with a frequency of 250-450 per minute.with a frequency of 250-450 per minute.

Sustained paroxysmal monomorphic ventricular Sustained paroxysmal monomorphic ventricular tachycardiatachycardia- Arrhythmias lasting longer than 30 seconds, which arises - Arrhythmias lasting longer than 30 seconds, which arises in the ventricles of the heart. The rhythm can be as correct in the ventricles of the heart. The rhythm can be as correct and incorrect with a heart rate of 120 to 250 per minute. and incorrect with a heart rate of 120 to 250 per minute. On standard ECG On standard ECG QRSQRS complexes wide (over 0.12), having complexes wide (over 0.12), having the same morphology. Are a common feature "grippers", ie the same morphology. Are a common feature "grippers", ie swaps "normal sinus' swaps "normal sinus' QRSQRS complexes and" drain systems complexes and" drain systems »»QRS, QRS, formed as a result of the spread of excitation at the formed as a result of the spread of excitation at the same time as from the sinus node, and from the excitation same time as from the sinus node, and from the excitation source, which is located in the ventricles.source, which is located in the ventricles.
Unstable ventricular tachycardia in the acute phase Unstable ventricular tachycardia in the acute phase of myocardial infarctionof myocardial infarction- Arrhythmias arising in the ventricles of the heart, in which - Arrhythmias arising in the ventricles of the heart, in which the standard ECG identify three or more consecutive wide the standard ECG identify three or more consecutive wide (more than 0.12 seconds) (more than 0.12 seconds) QRS QRS complex frequency of 100-complex frequency of 100-250 per minute, lasting no more than 30 s.250 per minute, lasting no more than 30 s.

Polymorphic ventricular tachycardia (bidirectional, Polymorphic ventricular tachycardia (bidirectional, spindle-shaped, "piruetnaya", or spindle-shaped, "piruetnaya", or torsades de pointestorsades de pointes). ). Rhythm wrong with HR of 150-250 per min., wide polymorphic Rhythm wrong with HR of 150-250 per min., wide polymorphic deformed complexes deformed complexes QRSQRS. On a standard ECG . On a standard ECG QRSQRS complexes complexes wide (more than 0.12), constantly changing their morphology. wide (more than 0.12), constantly changing their morphology. Occurs most frequently with the syndrome prolongation QT. Occurs most frequently with the syndrome prolongation QT. Can be both stable and unstable so-headed character. Can be both stable and unstable so-headed character. Characterized by a sinusoidal pattern - a group of 2 or more Characterized by a sinusoidal pattern - a group of 2 or more gastric-x complexes with one direction of ventricular complexes gastric-x complexes with one direction of ventricular complexes are replaced by groups with contrary area.are replaced by groups with contrary area.ventricular extrasystolesventricular extrasystoles- An extraordinary wide (over 0.12), the deformed complex - An extraordinary wide (over 0.12), the deformed complex QRSQRS, discordant mixture of ST and T wave compensatory pause , discordant mixture of ST and T wave compensatory pause (as full or partial) may be present or absent.(as full or partial) may be present or absent.Complete atrioventricular blockComplete atrioventricular block- Characterized by complete dissociation of atrial and gastric-- Characterized by complete dissociation of atrial and gastric-wave rhythms, at which no one atrial stimulation does not reach wave rhythms, at which no one atrial stimulation does not reach the gastrics of heart. Accompanied by expressive bradicardia.the gastrics of heart. Accompanied by expressive bradicardia.

Paroxysmal supraventricular tachycardiaParoxysmal supraventricular tachycardia
Paroxysmal supraventricular tachycardia - Paroxysmal supraventricular tachycardia - paroxysmal heart rhythm disorders, characterized paroxysmal heart rhythm disorders, characterized by a high heart rate (150-250 min) and in most by a high heart rate (150-250 min) and in most cases, the correct timing. On the pathogenesis of cases, the correct timing. On the pathogenesis of release: mechanism of release: mechanism of re-entryre-entry or circular motion or circular motion of the pulse, trigger, abnormal automaticity, and of the pulse, trigger, abnormal automaticity, and additional ways to conduct.additional ways to conduct.On UMC do not spend on the differentiation of On UMC do not spend on the differentiation of supraventricular tachycardia on atrial and supraventricular tachycardia on atrial and atrioventricular.atrioventricular.

TREATMENTTREATMENTNon-pharmacological therapyNon-pharmacological therapyAgainst the background of stable haemodynamics and clear Against the background of stable haemodynamics and clear awareness of the patient relief of paroxysm begins with awareness of the patient relief of paroxysm begins with techniques aimed at stimulation of the vagus nerve and techniques aimed at stimulation of the vagus nerve and slowing down of a atrio-ventricular site. Conducting tests of slowing down of a atrio-ventricular site. Conducting tests of vagal contraindicated in the presence of acute coronary vagal contraindicated in the presence of acute coronary syndrome, pulmonary embolism is suspected, in pregnant syndrome, pulmonary embolism is suspected, in pregnant women. Vagal tests: breath, forced a cough, rapid straining women. Vagal tests: breath, forced a cough, rapid straining after a deep inspiration (Valsalva maneuver), to induce after a deep inspiration (Valsalva maneuver), to induce vomiting or by pressure on the tongue, swallowing a crust of vomiting or by pressure on the tongue, swallowing a crust of bread, dip the face in ice water (diving reflex dog). A sample bread, dip the face in ice water (diving reflex dog). A sample of Aschoff (pressure on the eyeballs) is not recommended due of Aschoff (pressure on the eyeballs) is not recommended due to risk of damage to the retina. Carotid sinus massage is only to risk of damage to the retina. Carotid sinus massage is only valid when there is no lack of confidence in cerebral blood valid when there is no lack of confidence in cerebral blood flow (usually younger patients).flow (usually younger patients).

Drug therapyDrug therapyRelief supraventr th tachycardia can start with a 3-prep-Relief supraventr th tachycardia can start with a 3-prep-Comrade: adenosine, verapamil (only with narrow QRS), Comrade: adenosine, verapamil (only with narrow QRS), procainamide. When unperturbed STI other therapies, WPW-procainamide. When unperturbed STI other therapies, WPW-syndrome, against coronary. or heart failure STI acceptable syndrome, against coronary. or heart failure STI acceptable approx-s amiodarone (delayed-ing nastupl-s ef-ta).approx-s amiodarone (delayed-ing nastupl-s ef-ta).Adenosine at a dose of 6 mg / bolus is administered for 1-3 Adenosine at a dose of 6 mg / bolus is administered for 1-3 seconds, then a solution of NaCl 0,9% -20 ml and raise the limb. seconds, then a solution of NaCl 0,9% -20 ml and raise the limb. If no effect after 2 minutes to re-introduce 12 mg (3 ml), If no effect after 2 minutes to re-introduce 12 mg (3 ml), adenosine, and if after 2 minutes the rhythm was not restored - adenosine, and if after 2 minutes the rhythm was not restored - again 12 mg (3 ml) of adenosine.again 12 mg (3 ml) of adenosine.

Verapamil (only with narrow complexes QRS) is introduced Verapamil (only with narrow complexes QRS) is introduced into / in the bolus dose of 2.5-5 mg for 2-4 minutes (to into / in the bolus dose of 2.5-5 mg for 2-4 minutes (to avoid the development of collapse or expressive avoid the development of collapse or expressive bradycardia) with a possible re-introduction of 5.10 mg bradycardia) with a possible re-introduction of 5.10 mg intravenously 15 - 30 min while maintaining the tachycardia intravenously 15 - 30 min while maintaining the tachycardia and lack of hypotension. Necessary counter-vat heart rate, and lack of hypotension. Necessary counter-vat heart rate, blood pressure, ECGblood pressure, ECGProcainamide (novokainamid) 10% -10 ml (1000 mg), Procainamide (novokainamid) 10% -10 ml (1000 mg), diluted 0.9% NaCl rum 20 ml (concentration of 50 mg / ml) diluted 0.9% NaCl rum 20 ml (concentration of 50 mg / ml) and enter intravenously slowly with urgent 50 mg / min in and enter intravenously slowly with urgent 50 mg / min in during 20 min under constant control of rhythm, heart rate, during 20 min under constant control of rhythm, heart rate, blood pressure and ECG. At the time of recovery of sinus blood pressure and ECG. At the time of recovery of sinus rhythm, introduction of drug stoped.rhythm, introduction of drug stoped.

Indications for hospitalizationIndications for hospitalization The appearance of complications, require The appearance of complications, require
cardioversion.cardioversion. First registered rhythm disturbances.First registered rhythm disturbances. Lack of effect of drug therapy (pre-hospital use Lack of effect of drug therapy (pre-hospital use
only one arrhythmic agent).only one arrhythmic agent). Frequently recurrent arrhythmias.Frequently recurrent arrhythmias.

Atrial fibrillation or fibrillation of cardiomyocytes Atrial fibrillation or fibrillation of cardiomyocytes - - rhythm disturbance, characterized by chaotic excitation rhythm disturbance, characterized by chaotic excitation and reduction of irregular groups of cardiomyocytes with and reduction of irregular groups of cardiomyocytes with atrial rate of 350-600 per minute, resulting in a lack of atrial rate of 350-600 per minute, resulting in a lack of coordinated atrial systole. Depending on the duration of coordinated atrial systole. Depending on the duration of existence and the ability to stop (spontaneous or under the existence and the ability to stop (spontaneous or under the influence of antiarrhythmic drugs or cardioversion) influence of antiarrhythmic drugs or cardioversion) distinguish the following forms of atrial fibrillation.distinguish the following forms of atrial fibrillation.- - Paroxysmal form of atrial fibrillation. Paroxysmal form of atrial fibrillation. The most The most important feature of this form - the ability to self-important feature of this form - the ability to self-termination. At the same time in most patients the duration termination. At the same time in most patients the duration of arrhythmia is less than 7 days (usually less than 24 of arrhythmia is less than 7 days (usually less than 24 hours). From a practical point of view on the EMC isolated hours). From a practical point of view on the EMC isolated paroxysmal atrial fibrillation to 48 hours and more than 48 paroxysmal atrial fibrillation to 48 hours and more than 48 hours.hours.

- Stable (persistent) form of atrial fibrillation.- Stable (persistent) form of atrial fibrillation.The most important feature of this form - the inability to self-The most important feature of this form - the inability to self-termination, but it can be eliminated by medical or electrical termination, but it can be eliminated by medical or electrical cardioversion. In addition, the stable form of atrial fibrillation cardioversion. In addition, the stable form of atrial fibrillation have a significantly greater than the paroxysmal form, duration have a significantly greater than the paroxysmal form, duration of existence. Temporary measure stable form of atrial of existence. Temporary measure stable form of atrial fibrillation is the duration of more than 7 days (up to a year or fibrillation is the duration of more than 7 days (up to a year or more).more).
- Continuous form of atrial fibrillation. - Continuous form of atrial fibrillation. For a permanent For a permanent form include those cases of atrial fibrillation, which can not be form include those cases of atrial fibrillation, which can not be adjusted with the help of medication or electrical cardioversion, adjusted with the help of medication or electrical cardioversion, regardless of the duration of the arrhythmia. In terms of regardless of the duration of the arrhythmia. In terms of frequency allocated ventricular fibrillation following forms:frequency allocated ventricular fibrillation following forms:tachysystol(over 90 min);tachysystol(over 90 min);normoyistol (60-90 per minute);normoyistol (60-90 per minute);bradisistol (less than 60 min.)bradisistol (less than 60 min.)

TREATMENTTREATMENTThe issue of needness of restore sinus rhythm on hospital stage The issue of needness of restore sinus rhythm on hospital stage at first depends on a combination of 2 factors trench: the forms of at first depends on a combination of 2 factors trench: the forms of atrial fibrillation and the presence and severity of the disorder-in atrial fibrillation and the presence and severity of the disorder-in hemodynamics: acute left ventricular insufficientcy (hypotension, hemodynamics: acute left ventricular insufficientcy (hypotension, pulmonary edema), coronary insufficientcy (anginal attack, signs of pulmonary edema), coronary insufficientcy (anginal attack, signs of myocardial ischemia on ECG), disorders of consciousness.myocardial ischemia on ECG), disorders of consciousness.Digoxin (preferably linen manifested in the presence of the first Digoxin (preferably linen manifested in the presence of the first heart failure (CH). Antishown in WPW-syndrome, acute MI.heart failure (CH). Antishown in WPW-syndrome, acute MI.Verapamil (if no signs of CH in patient ) - intravenously bolusly in Verapamil (if no signs of CH in patient ) - intravenously bolusly in dose of 5 mg for 2-4 minutes (in escaping. Do I collapse, or dose of 5 mg for 2-4 minutes (in escaping. Do I collapse, or expressed bradycardia) with a possible re-introduction of m by expressed bradycardia) with a possible re-introduction of m by 5.10 mg 15-30 minutes at saving tachycardia and the absence of 5.10 mg 15-30 minutes at saving tachycardia and the absence of hypotension. Antishown with WPW-syndrome, artery. hypotension hypotension. Antishown with WPW-syndrome, artery. hypotension (SBP less than 90 mm Hg), cardiogen. shock, chronic and acute (SBP less than 90 mm Hg), cardiogen. shock, chronic and acute heart failure, also in pacients, who take heart failure, also in pacients, who take ββ--adrenobol-ia due to the adrenobol-ia due to the high risk of developing full AB-blockades or assistoliya.high risk of developing full AB-blockades or assistoliya.

Propranolol (nonselective β-blocker) - intravenously, Propranolol (nonselective β-blocker) - intravenously, stream, slowly introduced into the initial dose of 1 mg (1 stream, slowly introduced into the initial dose of 1 mg (1 ml of 0.1%) in the absence of effect repeat the same dose ml of 0.1%) in the absence of effect repeat the same dose every 2-3 minutes until the achievement the maximum every 2-3 minutes until the achievement the maximum dose of 10 mg. Antishown with arterial hypotension, dose of 10 mg. Antishown with arterial hypotension, acute heart failure, obliterating diseases of arteries, acute heart failure, obliterating diseases of arteries, asthma, pregnancy.asthma, pregnancy. INDICATION FOR HOSPITALIZATIONINDICATION FOR HOSPITALIZATION
Newly diagnosed atrial fibrillation.Newly diagnosed atrial fibrillation. Paroxysmal atrial fibrillation of before heart that can not Paroxysmal atrial fibrillation of before heart that can not
be medical cardioversion.be medical cardioversion. Atrial fibrillation (paroxysmal or persistent), accompanied Atrial fibrillation (paroxysmal or persistent), accompanied
by disorders of hemodynamics or myocardial ischemia, by disorders of hemodynamics or myocardial ischemia, which was cut short with medications or with electrical which was cut short with medications or with electrical cardioversion.cardioversion.
With the development of complications of antiarrhythmic With the development of complications of antiarrhythmic therapy.therapy.

Atrial flutter Atrial flutter - a significant acceleration of atrial rate (up to 250-- a significant acceleration of atrial rate (up to 250-450 per minute, typically in the range 280-320), while retaining the 450 per minute, typically in the range 280-320), while retaining the right atrial rhythm. The frequency of ventricular abridgement right atrial rhythm. The frequency of ventricular abridgement depends on carrying out in AB-node and in majority situations to the depends on carrying out in AB-node and in majority situations to the ventricles is held only every second (2:1) or third ectopic pulse (3-ventricles is held only every second (2:1) or third ectopic pulse (3-1). 1). TREATMENTTREATMENT
Sequence of actions on prehospital first stage in atrial flutter is not Sequence of actions on prehospital first stage in atrial flutter is not distinguished from that fibrillation of beforeheart of the first and distinguished from that fibrillation of beforeheart of the first and depends on the form of atrial flutter, the nature of decease of the depends on the form of atrial flutter, the nature of decease of the heart, on the background of which appears the infringment of the heart, on the background of which appears the infringment of the rhythm, as well as the availability and degree of expressiveness of rhythm, as well as the availability and degree of expressiveness of violation of hemodynamics and coronary circulation. When violation of hemodynamics and coronary circulation. When hemodynamic instability, the development of complications against hemodynamic instability, the development of complications against the background of atrial flutter with a high gastric reduction 's (AB-the background of atrial flutter with a high gastric reduction 's (AB-holding 1-1) shows the urgent cardioversion, synchronized with holding 1-1) shows the urgent cardioversion, synchronized with RR dent (the initial level of 100 J). With ineffectiveness of discharge dent (the initial level of 100 J). With ineffectiveness of discharge capacity of 100 J spend up discharge energy to 200 J.capacity of 100 J spend up discharge energy to 200 J. INDICATION FOR HOSPITALIZATIONINDICATION FOR HOSPITALIZATION
Same as for atrial fibrillation.Same as for atrial fibrillation.

Ventricular tachycardiaVentricular tachycardia Paroxysmal tachycardia with wide complex Paroxysmal tachycardia with wide complex QRSQRS may represent may represent
a true ventricular arrhythmias (ie, occur distal to the division of a true ventricular arrhythmias (ie, occur distal to the division of bundle branch block on his legs), and supraventricular bundle branch block on his legs), and supraventricular paroxysmal tachycardia in violation of the legs by Puig-branch paroxysmal tachycardia in violation of the legs by Puig-branch block.block. TreatmentTreatment
Ventricular tachycardia is an indication for immediate active Ventricular tachycardia is an indication for immediate active therapy aimed at restoring rhythm. In unstable hemodynamics therapy aimed at restoring rhythm. In unstable hemodynamics ventricular tachycardia require immediate cardioversion. The ventricular tachycardia require immediate cardioversion. The initial energy of 100 J (in the case of tachycardia type initial energy of 100 J (in the case of tachycardia type «torsade «torsade de pointes»de pointes» - 200 J) with an increase in the inefficiency of the - 200 J) with an increase in the inefficiency of the first-class up to 360 J. After the restoration of sinus rhythm first-class up to 360 J. After the restoration of sinus rhythm conduct emergency hospitalization and supportive therapy conduct emergency hospitalization and supportive therapy infusion of lidocaine or amiodarone. Ventricular fibrillation of infusion of lidocaine or amiodarone. Ventricular fibrillation of the heart requires cardio-pulmonary resuscitation.the heart requires cardio-pulmonary resuscitation.

In conventional of stable hemodynamics is shown drug therapy.In conventional of stable hemodynamics is shown drug therapy. Lidocaine - drug for relief of ventricular tachycardia – Lidocaine - drug for relief of ventricular tachycardia –
intravenously bolus dose of 1-1.5 mg / kg (2% 4-5 ml) injected in intravenously bolus dose of 1-1.5 mg / kg (2% 4-5 ml) injected in during 3-5 min. If required, repeating injection of the dose in during 3-5 min. If required, repeating injection of the dose in after 5-10 minutes (until common dose 3 mg / kg).after 5-10 minutes (until common dose 3 mg / kg).
Procainamide (novokainamid) - shown insufficiency of lidocaine Procainamide (novokainamid) - shown insufficiency of lidocaine and maintaining stable hemodynamics or when in impossible and maintaining stable hemodynamics or when in impossible carrying out electro impulse therapy – intravenously slowly, 100 carrying out electro impulse therapy – intravenously slowly, 100 mg (10% 10 ml separate by solution NaCl 0,9% to 10 ml and mg (10% 10 ml separate by solution NaCl 0,9% to 10 ml and injected to 1 ml in during 1 min), then repeat injection of 100 injected to 1 ml in during 1 min), then repeat injection of 100 mg after every 5 min to the summary dose are 1000 mg (17 mg after every 5 min to the summary dose are 1000 mg (17 mg / kg of body weight)mg / kg of body weight)

Amiodarone – in presence antishown to procainamide - Amiodarone – in presence antishown to procainamide - intravenouslyintravenously infusion of 150 mg (3 ml) in 40 ml 5% dextrose infusion of 150 mg (3 ml) in 40 ml 5% dextrose solution in during 10-20 min. Amiodarone is not compatible solution in during 10-20 min. Amiodarone is not compatible in solution with other drugs. Secondary effects occurs in in solution with other drugs. Secondary effects occurs in quickly intravenously injection: hypotension and quickly intravenously injection: hypotension and bradycardia.bradycardia.Magnesium sulfate- use intravenously in the 1000-2000 mg Magnesium sulfate- use intravenously in the 1000-2000 mg (10% of 10-20 ml, 20% 5 - 10 ml or 25% of 4-8 ml) is (10% of 10-20 ml, 20% 5 - 10 ml or 25% of 4-8 ml) is injected slowly (first 3 ml in during 3 min) in during 10-injected slowly (first 3 ml in during 3 min) in during 10-15min. In the absence of effect is carrying out repeated 15min. In the absence of effect is carrying out repeated injection after 30 min. After reach of effect the supporting injection after 30 min. After reach of effect the supporting therapy concluded in drop injection of MgSO4 with speed 3-therapy concluded in drop injection of MgSO4 with speed 3-20 mg / min in during 2-5 hours.20 mg / min in during 2-5 hours.

Indications for hospitalization.Indications for hospitalization.In paroxysmal ventricular tachycardia after the In paroxysmal ventricular tachycardia after the provision of necessary medical interventions, all patients provision of necessary medical interventions, all patients must be hospitalized.must be hospitalized.Ventricular beats on prehospital stage requires drug Ventricular beats on prehospital stage requires drug therapy only in one situation - there are frequent therapy only in one situation - there are frequent (several extrasystoles per minute), or steam politop or (several extrasystoles per minute), or steam politop or extrasystoles in acute myocardial infarction. At the same extrasystoles in acute myocardial infarction. At the same drugs of choice - lidocaine or amiodarone. In the absence drugs of choice - lidocaine or amiodarone. In the absence of ventricular arrhythmias prophylactic administration of of ventricular arrhythmias prophylactic administration of lidocaine in patients with myocardial infarction is lidocaine in patients with myocardial infarction is contraindicated, since it increases the risk of fatal contraindicated, since it increases the risk of fatal ventricular arrhythmias.ventricular arrhythmias.Monotop rare beats appointment does not require any Monotop rare beats appointment does not require any antiarrhythmic drugs.antiarrhythmic drugs.

bradyarrhythmiasbradyarrhythmias Acutely arising bradyarrhythmias (heart rate Acutely arising bradyarrhythmias (heart rate <60 per minute) associated with:<60 per minute) associated with:vagotonic reaction (sinus bradycardia);vagotonic reaction (sinus bradycardia);disorder automatism function or blockade of the disorder automatism function or blockade of the sinus node: sick sinus syndrome;sinus node: sick sinus syndrome;violation of excitation in the atrioventricular node:violation of excitation in the atrioventricular node:with AV block I or II degreewith AV block I or II degreetermination - with AV block III degree;termination - with AV block III degree;bradisistolicheskaya form of atrial fibrillation;bradisistolicheskaya form of atrial fibrillation;caused by drug therapy: p-blockers, calcium caused by drug therapy: p-blockers, calcium antagonists nedigidropiridinovye, amiodarone, antagonists nedigidropiridinovye, amiodarone, clonidine, digitalis glycosides, etc.;clonidine, digitalis glycosides, etc.;cessation of the pacemaker.cessation of the pacemaker.

Bradyarrhythmias requires the therapy on pre-Bradyarrhythmias requires the therapy on pre-hospital stage, if:hospital stage, if:accompanied by unstable hemodynamics accompanied by unstable hemodynamics (decrease in blood pressure <80 mm Hg, the (decrease in blood pressure <80 mm Hg, the development of syncope, heart attack, asthma or development of syncope, heart attack, asthma or pulmonary edema, severe anginal attack);pulmonary edema, severe anginal attack);arose as a complication of organic heart disease arose as a complication of organic heart disease (myocardial infarction);(myocardial infarction);developed during resuscitation;developed during resuscitation;there were frequent attacks of Morgagni-Adams-there were frequent attacks of Morgagni-Adams-Stokes (sudden dizziness, blackout, loss of Stokes (sudden dizziness, blackout, loss of consciousness), asystole in more than 20 developed consciousness), asystole in more than 20 developed marked cyanosis, convulsions, involuntary urine marked cyanosis, convulsions, involuntary urine loweringlowering and defecation.and defecation.

TREATMENTTREATMENTEnsure airway, venous access.Ensure airway, venous access.Oxygen therapy.Oxygen therapy.Constant monitoring of respiratory function, cardiovascular Constant monitoring of respiratory function, cardiovascular system (heart rate and blood pressure).system (heart rate and blood pressure).Readiness for ventilation and resuscitation.Readiness for ventilation and resuscitation.
Drug therapyDrug therapyAtropine is administered intravenously jet 0.5-1 mg (0.1% 0.5-Atropine is administered intravenously jet 0.5-1 mg (0.1% 0.5-1.0 ml), if required, after 5 minutes introduction is repeated until 1.0 ml), if required, after 5 minutes introduction is repeated until common maximum dose 3 mg. common maximum dose 3 mg. Attention: Attention: A dose of atropine A dose of atropine sulfate is less than 0.5 mg may paradoxically lead to a slowing of sulfate is less than 0.5 mg may paradoxically lead to a slowing of heart rate! heart rate! Side effects: Side effects: dry mouth, dry skin, mydriasis, thirst, dry mouth, dry skin, mydriasis, thirst, cycloplegia, constipation, loss of memory in the elderly. On vital cycloplegia, constipation, loss of memory in the elderly. On vital indications is not anti indications. With caution apply for angle-indications is not anti indications. With caution apply for angle-closure glaucoma, severe heart failure, ischemic heart disease, closure glaucoma, severe heart failure, ischemic heart disease, mitral stenosis, intestinal, prostate hyperplasia, chronic renal mitral stenosis, intestinal, prostate hyperplasia, chronic renal failure, hypertension, hyperthyroidism, myasthenia gravis, failure, hypertension, hyperthyroidism, myasthenia gravis, pregnancy.pregnancy.

Ineffectiveness of atropine therapy is an indication for Ineffectiveness of atropine therapy is an indication for temporary pacing. Depending on the equipment and temporary pacing. Depending on the equipment and crew training can be used indoor or throughcrew training can be used indoor or through oesophagus pacing. When in impossibility of carrying oesophagus pacing. When in impossibility of carrying out of cardioversion for health reasons is permissible out of cardioversion for health reasons is permissible application intravenously drip of epinephrineapplication intravenously drip of epinephrine
Indications for hospitalizationIndications for hospitalization Hospitalization is indicated for occurred acute Hospitalization is indicated for occurred acute
bradyarrhythmias with heart rate less than 40 beats bradyarrhythmias with heart rate less than 40 beats per minute, the available episodes of Morgagni-per minute, the available episodes of Morgagni-Adams-Stokes or syncope condition. In unstable Adams-Stokes or syncope condition. In unstable hemodynamics hold urgent hospitalization in the hemodynamics hold urgent hospitalization in the intensive care unit.intensive care unit.

Pulmonary edema, acute left ventricular failurePulmonary edema, acute left ventricular failure Acute left ventricular failure (ALVF) Acute left ventricular failure (ALVF) and its basic and its basic manifestation - cardiac asthma and pulmonary edema - manifestation - cardiac asthma and pulmonary edema - represent a pathological condition due to ample propotevanie-represent a pathological condition due to ample propotevanie-ing liquid part of blood in the interstitial tissue of the lungs and ing liquid part of blood in the interstitial tissue of the lungs and then into the alveoli, which clinically severe asthma, cyanosis then into the alveoli, which clinically severe asthma, cyanosis and choking the breath . and choking the breath .
Classification:Classification: 1. Congestive type: SNS left ventricular (cardiac asthma, 1. Congestive type: SNS left ventricular (cardiac asthma,
pulmonary edema), right ventricular OCH (venous stasis in the pulmonary edema), right ventricular OCH (venous stasis in the systemic circulation).systemic circulation).
2.Gipokinetichesky type: cardiogenic shock.2.Gipokinetichesky type: cardiogenic shock. Risk factors:Risk factors:
age over 60 years;age over 60 years; re-infarction and asthma version of its development;re-infarction and asthma version of its development; a history of circulatory disorders, obesity, chronic disease x, a history of circulatory disorders, obesity, chronic disease x,
frequent angina appeared to MI-Ia.frequent angina appeared to MI-Ia.

In acute left ventricular heart failure:In acute left ventricular heart failure:sudden onset with a feeling of shortness of breath;sudden onset with a feeling of shortness of breath;increasing shortness of varying severity, often increasing shortness of varying severity, often turning into asthma;turning into asthma;sometimes breathing Cheyne-Stoyksa (alternating sometimes breathing Cheyne-Stoyksa (alternating short periods of hyperventilation with respiratory short periods of hyperventilation with respiratory failure);failure);Cough (initially dry, and then sputum), and later - Cough (initially dry, and then sputum), and later - frothy sputum, often painted in pink);frothy sputum, often painted in pink);forced position of the patient sitting or semi-sitting forced position of the patient sitting or semi-sitting (orthopnea);(orthopnea);patient agitated, restless;patient agitated, restless;pallor and humidity of the skin ("cold" sweat), pallor and humidity of the skin ("cold" sweat), cyanotic mucous membranes;cyanotic mucous membranes;

tachycardia (120-150 per minute), protodiastolic gallop rhythm;tachycardia (120-150 per minute), protodiastolic gallop rhythm; swelling of the neck veins;swelling of the neck veins; normal or reduced blood pressure;normal or reduced blood pressure; rales at first may not listen to or determined by the scant rales at first may not listen to or determined by the scant
amount of finely wheezing over the lower portions of the lungs, amount of finely wheezing over the lower portions of the lungs, swelling of the mucous membrane of the small bronchi may swelling of the mucous membrane of the small bronchi may show a moderate pattern of bronchial obstruction with a show a moderate pattern of bronchial obstruction with a lengthening of expiration, wheezing and dry symptoms of lengthening of expiration, wheezing and dry symptoms of emphysema;emphysema;
with alveolar pulmonary edema syndrome (pulmonary with alveolar pulmonary edema syndrome (pulmonary edema) edema) - voiced mixed wet rales over all the light that can - voiced mixed wet rales over all the light that can listen to at a distance (bubbling breath);listen to at a distance (bubbling breath);
percussion - a moderate shift to the left border of the relative percussion - a moderate shift to the left border of the relative cardiac dullness (dilatation of the left ventricle).cardiac dullness (dilatation of the left ventricle).

Differential diagnosis:Differential diagnosis:Differential diagnostic sign of acute left ventricular failure Differential diagnostic sign of acute left ventricular failure with asthma may be dissociation between the severity of the with asthma may be dissociation between the severity of the condition, and (in the absence of express expiratory dyspnea, condition, and (in the absence of express expiratory dyspnea, and character of "silent zones"), the paucity of auscultatory and character of "silent zones"), the paucity of auscultatory pattern.pattern.When alveolar pulmonary edema detected voiced mixed wet When alveolar pulmonary edema detected voiced mixed wet rales over all the light that can listen to at a distance (bubbling rales over all the light that can listen to at a distance (bubbling breath).breath).In the differential diagnosis of shortness of breath hold with:In the differential diagnosis of shortness of breath hold with:spontaneous pneumothorax (dyspnea combined with a pain spontaneous pneumothorax (dyspnea combined with a pain syndrome);syndrome);central apnea (intracranial process);central apnea (intracranial process);psychogenic dyspnea (tachypnea);psychogenic dyspnea (tachypnea);attack of angina.attack of angina.

List of basic diagnostic measures:List of basic diagnostic measures:1. Determination of the onset of dyspnea and the nature of 1. Determination of the onset of dyspnea and the nature of her behavior (or the sudden appearance of a gradual her behavior (or the sudden appearance of a gradual increase), as well as conditions for the occurrence of increase), as well as conditions for the occurrence of shortness of breath (at rest or exercise).shortness of breath (at rest or exercise).2. Establishment of the symptoms that preceded the 2. Establishment of the symptoms that preceded the present state (chest pain, an episode of hypertensive present state (chest pain, an episode of hypertensive crisis).crisis).3. Establishment of drugs taken by patients and their 3. Establishment of drugs taken by patients and their effectiveness.effectiveness.4. Clarification of history (recent myocardial infarction, an 4. Clarification of history (recent myocardial infarction, an episode of congestive heart failure).episode of congestive heart failure).5. Assessment of general condition and vital signs: 5. Assessment of general condition and vital signs: consciousness, breathing and circulation.consciousness, breathing and circulation.6. Position the patient: orthopnea.6. Position the patient: orthopnea.7. Visual assessment: skin (pale, high humidity), the 7. Visual assessment: skin (pale, high humidity), the presence of acrocyanosis, swelling of the neck veins and presence of acrocyanosis, swelling of the neck veins and veins of the upper body, peripheral edema (lower veins of the upper body, peripheral edema (lower extremities, ascites).extremities, ascites).

8. Estimate the frequency of respiratory 8. Estimate the frequency of respiratory (tachypnea), pulse (tachycardia or bradycardia (tachypnea), pulse (tachycardia or bradycardia rarely).rarely).9. Measurement of blood pressure lowering SBP 9. Measurement of blood pressure lowering SBP below 90 mm Hg. - A sign of shock, hypotension below 90 mm Hg. - A sign of shock, hypotension (in severe damage to the myocardium) or (in severe damage to the myocardium) or hypertension (with the stress response of the hypertension (with the stress response of the organism).organism).10. Percussion: the presence of increasing border 10. Percussion: the presence of increasing border of the relative dullness of the heart to the left or of the relative dullness of the heart to the left or right (cardiomegaly).right (cardiomegaly).11. Palpation: displacement of apex beat and 11. Palpation: displacement of apex beat and offset the increased availability of unhealthy liver.offset the increased availability of unhealthy liver.12. Auscultation of the heart: protodiastolic or 12. Auscultation of the heart: protodiastolic or presystolic gallop rhythm, systolic murmur at the presystolic gallop rhythm, systolic murmur at the apex of the heart.apex of the heart.13. Auscultation of the lungs: presence of rales.13. Auscultation of the lungs: presence of rales.

The list of additional diagnostic measures:The list of additional diagnostic measures:ECG signs of left ventricular congestive heart ECG signs of left ventricular congestive heart failure:failure:split and increase in amplitude of the P wave in split and increase in amplitude of the P wave in leads I, II, aVL, V5-6;leads I, II, aVL, V5-6;increase in amplitude and duration of the second increase in amplitude and duration of the second negative phase of the P wave or the formation of a negative phase of the P wave or the formation of a negative P wave in lead V1;negative P wave in lead V1;negative or biphasic tooth RIII;negative or biphasic tooth RIII;increase the width of the P wave - more than 0.1sincrease the width of the P wave - more than 0.1s

The tactic of providing emergency assistance:The tactic of providing emergency assistance:The algorithm first aid at OLZHN:The algorithm first aid at OLZHN:
1. Inhalation of vapors 1. Inhalation of vapors through a nasal catheter through a nasal catheter alcohol (anti-foaming).alcohol (anti-foaming).
The initial infusion rate of oxygen (at 96 ° C ethanol) The initial infusion rate of oxygen (at 96 ° C ethanol) 2-3 L / min, for several (10) minutes. When the 2-3 L / min, for several (10) minutes. When the mucous membranes become accustomed to the mucous membranes become accustomed to the irritating action of gas, the rate was adjusted to 9-10 irritating action of gas, the rate was adjusted to 9-10 l / min. Inhalation continued for 30-40 minutes with l / min. Inhalation continued for 30-40 minutes with 10-15 minutes intervals.10-15 minutes intervals.
2. Relief of "respiratory panic" 2. Relief of "respiratory panic" narcotic analgesics: narcotic analgesics: morphine, 1.0 ml of 1% solution diluted in 20 ml 0.9% morphine, 1.0 ml of 1% solution diluted in 20 ml 0.9% sodium chloride solution and administered sodium chloride solution and administered intravenously breathlessness.intravenously breathlessness.
3. 3. Heparin Heparin 5000 units intravenously.5000 units intravenously. ITEMS 1-3 ARE MANDATORY!ITEMS 1-3 ARE MANDATORY!

sit down the patient's with lower extremities;sit down the patient's with lower extremities; nitroglycerin sublingual in tablets (0.5-1 mg) or in nitroglycerin sublingual in tablets (0.5-1 mg) or in
aerosol, or in spray (0.4-0.8 mg or 1-2 doses) or aerosol, or in spray (0.4-0.8 mg or 1-2 doses) or intravenously injection of 0.1% alcohol solution to intravenously injection of 0.1% alcohol solution to 10 mg per 100 ml isotonic sodium chloride 10 mg per 100 ml isotonic sodium chloride infusion, to increase the rate of injection of 25 mg infusion, to increase the rate of injection of 25 mg / min to effect under the control of blood pressure / min to effect under the control of blood pressure to achieve the effect;to achieve the effect;
furosemide 40-80 mg intravenously;furosemide 40-80 mg intravenously; diazepam intravenously fractionally until an effect diazepam intravenously fractionally until an effect
or achieve a total dose of 10 mg.or achieve a total dose of 10 mg.

5. In 5. In arterial hypertension:arterial hypertension: sit down the patient's with lower extremities;sit down the patient's with lower extremities; nitroglycerin tablets (preferably spray) 0.4-0.5 mg nitroglycerin tablets (preferably spray) 0.4-0.5 mg
sublingually, on one occasion;sublingually, on one occasion; furosemide 40-80 mg intravenously;furosemide 40-80 mg intravenously; intravenously nitroglycerin 0.1% alcohol solution to 10 intravenously nitroglycerin 0.1% alcohol solution to 10
mg per 100 ml of isotonic sodium chloride infusion, mg per 100 ml of isotonic sodium chloride infusion, increasing the rate of injection of 25 mkg / min to increasing the rate of injection of 25 mkg / min to effect under the control of blood pressure to achieve effect under the control of blood pressure to achieve the effect, or sodium nitroprusside 30 mg in 300 ml the effect, or sodium nitroprusside 30 mg in 300 ml 5% dextrose intravenously, gradually increasing the 5% dextrose intravenously, gradually increasing the speed of infusion of the drug from 0.3 mg / (mkg/ min) speed of infusion of the drug from 0.3 mg / (mkg/ min) to effect, controlling blood pressure;to effect, controlling blood pressure;
diazepam intravenously to effect a fractional or diazepam intravenously to effect a fractional or achieve a total dose of 10 mg.achieve a total dose of 10 mg.

6. In 6. In moderate hypotension moderate hypotension (systolic blood (systolic blood pressure 75 - 90 mm Hg):pressure 75 - 90 mm Hg):
put the patient, raising his head;put the patient, raising his head;
dopamine 250 mg in 250 ml isotonic sodium dopamine 250 mg in 250 ml isotonic sodium chloride solution, increasing the infusion rate of 5 chloride solution, increasing the infusion rate of 5 mg / (kgh /min) to stabilize blood pressure at the mg / (kgh /min) to stabilize blood pressure at the lowest possible level;lowest possible level;
furosemide 40-80 mg intravenously.furosemide 40-80 mg intravenously.

7. In 7. In severe arterial hypotension:severe arterial hypotension: put the patient, raising his head;put the patient, raising his head; Dopamine 200 mg in 400 ml 5% dextrose intravenously, Dopamine 200 mg in 400 ml 5% dextrose intravenously,
increasing the infusion rate of 5 mg / (kghmin) to stabilize increasing the infusion rate of 5 mg / (kghmin) to stabilize blood pressure at the lowest possible level;blood pressure at the lowest possible level;
with an increase in blood pressure, accompanied by with an increase in blood pressure, accompanied by progressive pulmonary edema, in addition nitroglycerin progressive pulmonary edema, in addition nitroglycerin intravenous drip of 1% alcohol solution to 10 mg per 100 ml intravenous drip of 1% alcohol solution to 10 mg per 100 ml of isotonic sodium chloride solution, to increase the rate of of isotonic sodium chloride solution, to increase the rate of injection of 25 mkg / min to effect under the control of injection of 25 mkg / min to effect under the control of blood pressure to achieve the effect;blood pressure to achieve the effect;
furosemide 40-80 mg intravenously only after stabilization furosemide 40-80 mg intravenously only after stabilization of blood pressure.of blood pressure.
8. Monitoring of vital body functions (Pulse, pulse oximeter).8. Monitoring of vital body functions (Pulse, pulse oximeter).

Indications for emergency hospitalization:Indications for emergency hospitalization: In marked pulmonary edema after its In marked pulmonary edema after its
hospitalization can relieve or specialized teams of hospitalization can relieve or specialized teams of medical emergencies. The patient was medical emergencies. The patient was transported in a sitting position.transported in a sitting position.
Performance indicators of medical care:Performance indicators of medical care: 1. Reduce moisture of the skin.1. Reduce moisture of the skin. 2. Reduction or disappearance of wet rales in the 2. Reduction or disappearance of wet rales in the
lungs and respiratory bubbling.lungs and respiratory bubbling. 3. Improvement of subjective sensations - 3. Improvement of subjective sensations -
reducing breathlessness and choking.reducing breathlessness and choking. 4. The relative normalization of blood pressure.4. The relative normalization of blood pressure.

Hypertensive crisisHypertensive crisis Hypertensive crisis Hypertensive crisis - a clinical syndrome characterized by a - a clinical syndrome characterized by a
sudden increase in blood pressure to high values of individual, sudden increase in blood pressure to high values of individual, subjective and objective manifestations of cerebral, cardiovascular subjective and objective manifestations of cerebral, cardiovascular and common vegetative violations.and common vegetative violations.
ClassificationClassification (JNC-6) (JNC-6) in the course of HC in the course of HC is divided into:is divided into: 1.1. Complicated Complicated (critical, emergency) accompanied by a (critical, emergency) accompanied by a
symptoms of worsening of cerebral, coronary, renal circulation and symptoms of worsening of cerebral, coronary, renal circulation and requires a reduction of blood pressure during the first minutes and requires a reduction of blood pressure during the first minutes and hours with parenteral preparations.hours with parenteral preparations.
2. 2. UncomplicatedUncomplicated (non-critical, urgency), hypertensive crises (non-critical, urgency), hypertensive crises characterized by the absence of target organ damage and relative characterized by the absence of target organ damage and relative to the condition to the pits, requiring relatively urgent blood to the condition to the pits, requiring relatively urgent blood pressure reduction during several hours.pressure reduction during several hours.
Forms of uncomplicated hypertensive crises:Forms of uncomplicated hypertensive crises: 1. Neuro.1. Neuro. 2. Water and salt.2. Water and salt. 3. Cramping.3. Cramping.

Complications of hypertensive crises:Complications of hypertensive crises: 1.Tserebrovaskular:1.Tserebrovaskular: a) an acute cerebrovascular accident (stroke, a) an acute cerebrovascular accident (stroke,
subarachnoidsubarachnoid hemorrhage);hemorrhage); b) acute hypertensive encephalopathy with cerebral b) acute hypertensive encephalopathy with cerebral
edema.edema. 2.Cardial:2.Cardial: a) acute heart failure;a) acute heart failure; b) myocardial infarction, acute coronary syndrome.b) myocardial infarction, acute coronary syndrome. 3. Acute aortic dissection, rupture of an aortic 3. Acute aortic dissection, rupture of an aortic
aneurysm.aneurysm. 4. Acute renal failure.4. Acute renal failure. 5. Acute retinopathy with hemorrhage into 5. Acute retinopathy with hemorrhage into
the retina.the retina.

Risk factors: Risk factors: hypertensive crisis develops in the hypertensive crisis develops in the background:background:
1.Hypertensive disease (including as its first 1.Hypertensive disease (including as its first manifestation);manifestation);
2.Simptomatic arterial hypertension;2.Simptomatic arterial hypertension; 3.Renovaskuiar arterial hypertension;3.Renovaskuiar arterial hypertension; 4.Diabetic nephropathy;4.Diabetic nephropathy; 5.Feohromotsitoma;5.Feohromotsitoma; 6. Acute glomerulonephritis;6. Acute glomerulonephritis; 7. Eclampsia of pregnant;7. Eclampsia of pregnant; 8.Diffuz diseases of connective tissue with involving 8.Diffuz diseases of connective tissue with involving
of the kidneys;of the kidneys; 9. Using of sympathomimetic means (eg, cocaine);9. Using of sympathomimetic means (eg, cocaine); 10.Skull trauma;10.Skull trauma; 11.Heavy burns, etc.11.Heavy burns, etc.

The most common factors contributing to The most common factors contributing to the development of hypertensive crises:the development of hypertensive crises:
1. Discontinuation of antihypertensive 1. Discontinuation of antihypertensive medications;medications;
2. Psycho-emotional stress;2. Psycho-emotional stress; 3. Excessive consumption of salt and fluid;3. Excessive consumption of salt and fluid; 4. Exercise;4. Exercise; 5. Alcohol abuse;5. Alcohol abuse; 6. Meteorological variations.6. Meteorological variations.

Criteria for the diagnosis of uncomplicated HC:Criteria for the diagnosis of uncomplicated HC: For For hypertensive form of autonomic crisis hypertensive form of autonomic crisis is is
nature :nature : sudden onset;sudden onset; predominant increase in systolic blood pressure with predominant increase in systolic blood pressure with
increasing pulse;increasing pulse; shivering; excitement; anxiety, irritability;shivering; excitement; anxiety, irritability; hyperemia and humidity of the skin;hyperemia and humidity of the skin; thirst;thirst; headache;headache; nausea;nausea; visual disturbances in the form of "floaters" or veil visual disturbances in the form of "floaters" or veil
before the eyes;before the eyes; tachycardia;tachycardia; at the end of a crisis - fast, with the release of copious at the end of a crisis - fast, with the release of copious
pale urine.pale urine.

When the water-salt hypertensive crisis When the water-salt hypertensive crisis marked the form:marked the form:
less acute onset;less acute onset; predominant increase in diastolic pressure with predominant increase in diastolic pressure with
decreasing pulse;decreasing pulse; drowsiness, weakness;drowsiness, weakness; pallor;pallor; swelling;swelling; headache;headache; nausea, vomiting;nausea, vomiting; paresthesia;paresthesia; short-term weakness in the limbs, hemiparesis, short-term weakness in the limbs, hemiparesis,
aphasia, diplopia.aphasia, diplopia.

In the convulsive form of hypertensive crisis In the convulsive form of hypertensive crisis observed:observed:
sharp increase in systolic and diastolic blood sharp increase in systolic and diastolic blood pressure;pressure;
psychomotor agitation;psychomotor agitation; intense headache, dizziness;intense headache, dizziness; nausea, repeated vomiting;nausea, repeated vomiting; severe sight disorders - transient blindness, severe sight disorders - transient blindness,
double vision, etc.double vision, etc. loss of consciousness;loss of consciousness;
clonic-tonic convulsions.clonic-tonic convulsions.

Criteria for the diagnosis of complicated HC:Criteria for the diagnosis of complicated HC: relatively sudden onset;relatively sudden onset; individually high blood pressure (diastolic blood pressure exceeds 120-individually high blood pressure (diastolic blood pressure exceeds 120-
130 mm Hg);130 mm Hg); Signs of CNS dysfunction, encephalopathy with cerebral (intensiv. Signs of CNS dysfunction, encephalopathy with cerebral (intensiv.
Headache of diffuse nature, feel the noise in the head, nausea, Headache of diffuse nature, feel the noise in the head, nausea, vomiting, blurred vision. Possible seizures, drowsiness, and expressive vomiting, blurred vision. Possible seizures, drowsiness, and expressive violations of consciousness), and focal symptoms (paresthesia the tips violations of consciousness), and focal symptoms (paresthesia the tips of the fingers, lips, cheeks, feeling of weakness in the arms, legs, of the fingers, lips, cheeks, feeling of weakness in the arms, legs, double vision, transient speech disturbances, and transient double vision, transient speech disturbances, and transient hemiparesis);hemiparesis);
neurovegetative disorders (thirst, dry mouth, feeling internal neurovegetative disorders (thirst, dry mouth, feeling internal trembling, palpitations, like shivering tremor, rash);trembling, palpitations, like shivering tremor, rash);
Cardiac dysfunction with varying degrees of severity of subjective and Cardiac dysfunction with varying degrees of severity of subjective and objective manifestations;objective manifestations;
Expressed by an ophthalmologic symptoms (subjective symptoms and Expressed by an ophthalmologic symptoms (subjective symptoms and changes in the fundus - pronounced spazm arterioles, venules changes in the fundus - pronounced spazm arterioles, venules expansion, swelling, nipple leak of optic nerve, hemorrhage, retinal expansion, swelling, nipple leak of optic nerve, hemorrhage, retinal detachment);detachment);
First incurred or aggravated infringement- violations of kidneys.First incurred or aggravated infringement- violations of kidneys.

Complications of HC:Complications of HC:1. From the heart:1. From the heart:Acute myocardial infarction or angina destabilization;Acute myocardial infarction or angina destabilization;Acute left ventricular failure.Acute left ventricular failure.2. Acute aortic dissection.2. Acute aortic dissection.3. On the part of the brain:3. On the part of the brain:Acute hypertensive encephalopathy;Acute hypertensive encephalopathy;stroke;stroke;Transient ischemic attack.Transient ischemic attack.4. From the side of kidneys:4. From the side of kidneys:Acute renal failure.Acute renal failure.5. On the part of the retina:5. On the part of the retina:Acute retinopathy with hemorrhages to the retina.Acute retinopathy with hemorrhages to the retina.

Differential diagnosis:Differential diagnosis: Hypertensive crisis should be distinguished from Hypertensive crisis should be distinguished from
decompensation or deterioration of arterial hypertensiondecompensation or deterioration of arterial hypertension
diagnosticsign
HC Decompensation or worsening of hypertension
beginning The relatively sudden Increased blood pressure developing on the background of the saved self preserved region blood flow, usually due to inadequate treatment.
blood pressure degree Individual high degree of blood pressure (DBP exceeds 120-130 mm Hg);
Degree of BP corresponds to the degree of hypertension. Marks satisfactory endure of high BP figures.
Target organ damage symptoms of autonomicdisorders, damage ofaffecting organs
There are no signs of acute damage target organs, the nature complaints is headache.

List of basic diagnostic measures:List of basic diagnostic measures: 1.Assestment general condition and vital signs: consciousness 1.Assestment general condition and vital signs: consciousness
(arousal, stupor, unconscious), breathing (tachypnea (arousal, stupor, unconscious), breathing (tachypnea availability);availability);
2. Visual assessment:2. Visual assessment: a) The provisions of the patient (lying, sitting, orthopnea);a) The provisions of the patient (lying, sitting, orthopnea); b) skin color (pale, congestion, cyanosis) and humidityb) skin color (pale, congestion, cyanosis) and humidity c) vessels of the neck (swelling of the veins, visible pulsation);c) vessels of the neck (swelling of the veins, visible pulsation); d) presence of peripheral edema.d) presence of peripheral edema. 3. The study of the pulse (right, wrong), the measurement of 3. The study of the pulse (right, wrong), the measurement of
heart rate (tachycardia, bradycardia).heart rate (tachycardia, bradycardia). 4. Measuring blood pressure in both arms every 15-30 minutes.4. Measuring blood pressure in both arms every 15-30 minutes. 5. Percussion: the presence of increased limits of relative 5. Percussion: the presence of increased limits of relative
cardiac dullness to the left.cardiac dullness to the left. 6. Palpation: apex beat estimate, its localization.6. Palpation: apex beat estimate, its localization.

7. Auscultation of the heart: evaluation of tone, the 7. Auscultation of the heart: evaluation of tone, the presence of noise, accent and splitting of the II tonepresence of noise, accent and splitting of the II tone over aorta.over aorta.
8. Auscultation of the aorta (suspection to the aortic 8. Auscultation of the aorta (suspection to the aortic dissection or aneurysm rupture) and renal artery dissection or aneurysm rupture) and renal artery (stenosis of suspicion).(stenosis of suspicion).
9. Auscultation of the lungs: the presence of different-9. Auscultation of the lungs: the presence of different-sized moist rales on both sides.sized moist rales on both sides.
10. Clarification of the presence deterioration of 10. Clarification of the presence deterioration of vision, vomiting, seizures, angina, dyspnea; vision, vomiting, seizures, angina, dyspnea; assessment of diuresis.assessment of diuresis.
11. The study of neurological status: reduced level of 11. The study of neurological status: reduced level of consciousness, visual field defects, dysphagia, consciousness, visual field defects, dysphagia, impaired motor function in limbs, impaired static and impaired motor function in limbs, impaired static and gait, urinary incontinence.gait, urinary incontinence.

Instrumental study.Instrumental study. 1.Registration of ECG in 12-lead : evaluation of 1.Registration of ECG in 12-lead : evaluation of
rhythm, heart rate, conduction, signs of left rhythm, heart rate, conduction, signs of left ventricular hypertrophy, ischemia and myocardial ventricular hypertrophy, ischemia and myocardial infarction.infarction.
Additional diagnostic measures:Additional diagnostic measures: 1. Express analysis of blood glucose;1. Express analysis of blood glucose; 2. Daily monitoring of blood pressure (acc. to 2. Daily monitoring of blood pressure (acc. to
indications).indications).

Tactics of giving medical care.Tactics of giving medical care.Objective: Objective: stabilization of vital functions of organismstabilization of vital functions of organismUncomplicated hypertensive crisis:Uncomplicated hypertensive crisis:1. The patient's position - lying with a raised head end.1. The patient's position - lying with a raised head end.2. Control heart rate, blood pressure every 15 minutes.2. Control heart rate, blood pressure every 15 minutes.3. Gradual reduction of blood pressure on 15-25% from 3. Gradual reduction of blood pressure on 15-25% from baseline or ≤ 160 \ 110 mm Hg during 12-24 hours.baseline or ≤ 160 \ 110 mm Hg during 12-24 hours.4. Used oral antihypertensive medications (starting with 4. Used oral antihypertensive medications (starting with one drug): nifedipine, captopril, propranolol, bisoprolol, one drug): nifedipine, captopril, propranolol, bisoprolol, metoprolol).metoprolol).5. Reduction and stabilization of the peripheral 5. Reduction and stabilization of the peripheral resistance vasculature of the brain - 30 mg vincamineresistance vasculature of the brain - 30 mg vincamine

When combined elevated systolic blood When combined elevated systolic blood pressure and tachycardia:pressure and tachycardia:
Propranolol (nonselective Propranolol (nonselective β-β-blocker) inside 10-40 blocker) inside 10-40 mg;mg;
Clonidine (centrally acting agents) - under the Clonidine (centrally acting agents) - under the tongue of 0,075-0,150 mg.tongue of 0,075-0,150 mg.
In the preferential increase in diastolic In the preferential increase in diastolic blood pressure or in uniform increase of blood pressure or in uniform increase of systolic blood pressure and diastolic arterial systolic blood pressure and diastolic arterial blood pressure:blood pressure:
CaptoprilCaptopril (ACE (ACE ((АПФАПФ)) inhibitor) - 25 mg inhibitor) - 25 mg sublingually;sublingually;
Nifedipine Nifedipine (calcium channel blockers of II type, (calcium channel blockers of II type, dihydropyridines) - 10-20 mg sublingually.dihydropyridines) - 10-20 mg sublingually.

Complicated hypertensive crisis:Complicated hypertensive crisis: 1.Sanatsiya of respiratory tract.1.Sanatsiya of respiratory tract. 2. Oxygen therapy.2. Oxygen therapy. 3.Vein access.3.Vein access. 4. Treatment developed complications and 4. Treatment developed complications and
differentiated approach to the choice of differentiated approach to the choice of antihypertensive drugs.antihypertensive drugs.
5.Antihypertensive therapy is carried out with 5.Antihypertensive therapy is carried out with parenteral therapy.parenteral therapy.
6. Lowering of BP is rapidly (on 15-20% from 6. Lowering of BP is rapidly (on 15-20% from initial during one hour, then for 2-6 hours up to initial during one hour, then for 2-6 hours up to 160 mm and 100 mm Hg ( possible a transition to 160 mm and 100 mm Hg ( possible a transition to oral medications).oral medications).

Hypertensive crisis, compounded by an acute Hypertensive crisis, compounded by an acute myocardial infarction or acute coronary syndrome:myocardial infarction or acute coronary syndrome:
Goal: Goal: reduction of pain attacks, improved nutrition infarction, reduction of pain attacks, improved nutrition infarction, lowering blood pressure:lowering blood pressure:
Nitroglycerin Nitroglycerin 0.5 mg sublingually, in aerozol or spray (0.4 0.5 mg sublingually, in aerozol or spray (0.4 mg, or 1 dose), if necessary, repeat every 5-10 minutes, or mg, or 1 dose), if necessary, repeat every 5-10 minutes, or intravenously 10 ml of 0.1% solution in 100 ml 0.9% sodium intravenously 10 ml of 0.1% solution in 100 ml 0.9% sodium chloride infusion by drop (2-4 drops per minute) under the chloride infusion by drop (2-4 drops per minute) under the control of blood pressure and heart rate;control of blood pressure and heart rate;
Propranolol Propranolol (nonselective β-adrenoblocker) - slowly (nonselective β-adrenoblocker) - slowly intravenously injected 1 ml of 0.1% solution (1 mg) dose may intravenously injected 1 ml of 0.1% solution (1 mg) dose may be repeated above dose after 3-5 minutes until the heart rate be repeated above dose after 3-5 minutes until the heart rate of 60 per minute under the control of blood pressure and ECG, of 60 per minute under the control of blood pressure and ECG, with a maximum total dose of 10 mg;with a maximum total dose of 10 mg;
With continued high numbers of blood pressure: With continued high numbers of blood pressure: enalaprilat enalaprilat (ACE(ACE ((АПФАПФ)) inhibitor) 0,625-1,250 mg intravenously slowly inhibitor) 0,625-1,250 mg intravenously slowly during 5 minutes, pre-diluted in 20 ml 0.9% sodium chloride;during 5 minutes, pre-diluted in 20 ml 0.9% sodium chloride;

Morphine Morphine (narcotic analgesic), 1 ml of 1% solution diluted (narcotic analgesic), 1 ml of 1% solution diluted 20 ml 0.9% sodium chloride solution and to inject 20 ml 0.9% sodium chloride solution and to inject intravenously by a fractional 4-10 ml (or 2-5mg) every 5-15 intravenously by a fractional 4-10 ml (or 2-5mg) every 5-15 minutes until elimination the pain and shortness of breath, minutes until elimination the pain and shortness of breath, or until appearing the side effects (hypotension, respiratory or until appearing the side effects (hypotension, respiratory depression, vomiting);depression, vomiting);
Warfarin 2.5 mg, or acetylsalicylic acid Warfarin 2.5 mg, or acetylsalicylic acid - to chewed - to chewed 160-325 mg in order to improve prognosis.160-325 mg in order to improve prognosis.
Hypertensive crisis, complicated by acute left Hypertensive crisis, complicated by acute left ventricular failure:ventricular failure:
Goal: Goal: relief of pulmonary edema, decreased blood pressure:relief of pulmonary edema, decreased blood pressure: EnalaprilatEnalaprilat (ACE (ACE ((АПФАПФ)) inhibitor) 0,625-1,250 mg / slowly inhibitor) 0,625-1,250 mg / slowly
intravenously during 5 minutes, pre-diluted in 20 ml of 0.9% intravenously during 5 minutes, pre-diluted in 20 ml of 0.9% solution of NaCl;solution of NaCl;
FurosemideFurosemide 20-100 mg intravenously. 20-100 mg intravenously.

Hypertensive crisis, complicated by acute aortic Hypertensive crisis, complicated by acute aortic dissection or rupture of an aortic aneurysm:dissection or rupture of an aortic aneurysm:
Objective: Objective: a rapid decrease in blood pressure of 100-120 a rapid decrease in blood pressure of 100-120 mmHg and 80 (or 25% of the initial 5-10 min, and further to mmHg and 80 (or 25% of the initial 5-10 min, and further to these figures), decreased myocardial contractility:these figures), decreased myocardial contractility:
Propranolol – Propranolol – slowly intravenously. Injected in initial dose of 1 slowly intravenously. Injected in initial dose of 1 ml of 0.1% solution (1 mg), possible to repeat same dose after ml of 0.1% solution (1 mg), possible to repeat same dose after 3-5 minutes until the heart rate of 60 min. under the control BP 3-5 minutes until the heart rate of 60 min. under the control BP and ECG; the maximum total dose is 10 mg;and ECG; the maximum total dose is 10 mg;
Nitroglycerin Nitroglycerin intravenously 10 ml of 0.1% to solution 100 ml intravenously 10 ml of 0.1% to solution 100 ml 0.9% solution of NaCl by drop (2-4 drops per minute) and inject 0.9% solution of NaCl by drop (2-4 drops per minute) and inject with initial urgent 1 ml / min (1-2 drops per minute.). The rate of with initial urgent 1 ml / min (1-2 drops per minute.). The rate of injection can be increased every 5 min for 2-3 drops, depending injection can be increased every 5 min for 2-3 drops, depending on patient reaction;on patient reaction;

If β-adernoblokators antiindicated, in this case verapamil If β-adernoblokators antiindicated, in this case verapamil intravenously, bolus for 2-4 min 2.5 - 5 mg (0.25% - 1-2 ml) intravenously, bolus for 2-4 min 2.5 - 5 mg (0.25% - 1-2 ml) with a possible re-injection of 5-10 mg in 15-30 minutes .with a possible re-injection of 5-10 mg in 15-30 minutes .
For cropping of pain syndrome - For cropping of pain syndrome - morphine morphine 1 ml of 1% 1 ml of 1% solution dilute 20 ml 0.9% NaCl solution and injected solution dilute 20 ml 0.9% NaCl solution and injected intravenously, by a fractional 4.10 ml (or 2-5mg) every 5-15 intravenously, by a fractional 4.10 ml (or 2-5mg) every 5-15 minutes to eliminate pain and shortness of breath, or until minutes to eliminate pain and shortness of breath, or until the appearance of secondary effects (hypotension, the appearance of secondary effects (hypotension, respiratory depression, vomiting);respiratory depression, vomiting);

HC complicated by hypertensive encephalopathy:HC complicated by hypertensive encephalopathy: Lowering blood pressure quickly and carefully.Lowering blood pressure quickly and carefully. Enalaprilat Enalaprilat (ACE(ACE ((АПФАПФ)) inhibitor) 0,625-1,250 mg intravenously slowly inhibitor) 0,625-1,250 mg intravenously slowly
in during 5 min. Pre-diluted in 20 ml of 0.9% solution of NaCl;in during 5 min. Pre-diluted in 20 ml of 0.9% solution of NaCl; When seizures - When seizures - diazepam diazepam intravenously an initial dose of 10-20 mg, in intravenously an initial dose of 10-20 mg, in
the subsequent, if required, 20 mg intramuscularly or intravenously by the subsequent, if required, 20 mg intramuscularly or intravenously by drop.drop.
HC, complicated AIBC (Acute Insufficiency of Brain Circulation HC, complicated AIBC (Acute Insufficiency of Brain Circulation ((ОНМКОНМК)) or subarachnoid hemorrhage:)) or subarachnoid hemorrhage:
Blood pressure reduction is carried out slowly.Blood pressure reduction is carried out slowly. Enalaprilat Enalaprilat (ACE(ACE ((АПФАПФ)) inhibitor) 0,625-1,250 mg intravenously, inhibitor) 0,625-1,250 mg intravenously,
slowly, in during 5 min., pre-diluted in 20 ml of 0.9% solution NaCl;slowly, in during 5 min., pre-diluted in 20 ml of 0.9% solution NaCl;
HC, complicated by pre-eclampsia or eclampsia:HC, complicated by pre-eclampsia or eclampsia: Magnesium sulphate Magnesium sulphate intravenously bolus 400-1000 mg, with it the intravenously bolus 400-1000 mg, with it the
first 3 ml for 3 minutes or drip in 200 ml of 0.9% solution of NaCl;first 3 ml for 3 minutes or drip in 200 ml of 0.9% solution of NaCl; NifedipineNifedipine (blockers of calcium channel of II type, dihydropyridines) - (blockers of calcium channel of II type, dihydropyridines) -
10-20 mg sublingually.10-20 mg sublingually.

HC, complications of acute glomerulonephritis:HC, complications of acute glomerulonephritis: Nifedipine 10-40 mg PO;Nifedipine 10-40 mg PO; Furosemide 80-100 mg.Furosemide 80-100 mg.
Indications for emergency hospitalization:Indications for emergency hospitalization: Uncomplicated hypertensive crisisUncomplicated hypertensive crisis, not cropped , not cropped
during emergency care - hospitalization therapeutic or during emergency care - hospitalization therapeutic or cardiology department.cardiology department.
Complicated hypertensive crisis Complicated hypertensive crisis - emergency - emergency hospital with taking into account developing hospital with taking into account developing complications, transport the patient in lying position.complications, transport the patient in lying position.
Indicators of effectiveness performance medical Indicators of effectiveness performance medical care:care:stabilization of vital functions of organismstabilization of vital functions of organism

THANK YOU!THANK YOU!