Embed Size (px)
Citation preview
Review Article
Diagnostic Accuracy of Cone-beam Computed Tomographyand Conventional Radiography on Apical Periodontitis:A Systematic Review and Meta-analysisKamile Leonardi Dutra, DDS, MSc,* Let�ıcia Haas, DDS, MSc,* Andr�e Lu�ıs Porporatti, DDS, MSc,†
Carlos Flores-Mir, DDS, MSc, PhD,‡ Juliana Nascimento Santos, DDS, MSc, PhD,§
Luis Andr�e Mezzomo, DDS, MSc, PhD,¶k M�arcio Correa, DDS, MSc, PhD,¶
and Graziela De Luca Canto, DDS, MSc, PhD‡¶k
Abstract
Introduction: Endodontic diagnosis depends on accu-rate radiographic examination. Assessment of the loca-tion and extent of apical periodontitis (AP) caninfluence treatment planning and subsequent treat-ment outcomes. Therefore, this systematic review andmeta-analysis assessed the diagnostic accuracy of con-ventional radiography and cone-beam computed tomo-graphic (CBCT) imaging on the discrimination of APfrom no lesion. Methods: Eight electronic databaseswith no language or time limitations were searched. Ar-ticles in which the primary objective was to evaluate theaccuracy (sensitivity and specificity) of any type ofradiographic technique to assess AP in humans wereselected. The gold standard was the histologic exami-nation for actual AP (in vivo) or in situ visualizationof bone defects for induced artificial AP (in vitro). Ac-curacy measurements described in the studies weretransformed to construct receiver operating character-istic curves and forest plots with the aid of ReviewMan-ager v.5.2 (The Nordic Cochrane Centre, Copenhagen,Denmark) and MetaDisc v.1.4. software (Unit of ClinicalBiostatistics Team of the Ram�on y Cajal Hospital, Ma-drid, Spain). The methodology of the selected studieswas evaluated using the Quality Assessment Tool forDiagnostic Accuracy Studies-2. Results: Only 9 studiesmet the inclusion criteria and were subjected to a qual-itative analysis. A meta-analysis was conducted on 6 ofthese articles. All of these articles studied artificial APwith induced bone defects. The accuracy values (areaunder the curve) were 0.96 for CBCT imaging, 0.73for conventional periapical radiography, and 0.72 fordigital periapical radiography. No evidence was foundfor panoramic radiography. Conclusions: Periapicalradiographs (digital and conventional) reported goodFrom the*Postgraduate Program in Dentistry, Health Sciences Cegram in Applied Oral Sciences, Bauru School of Dentistry, UniversityAlberta, Edmonton, Alberta, Canada; §Facult�e de Medicine Dentaire,Florianopolis, Santa Catarina, Brazil; and kBrazilian Centre for Evide
Address requests for reprints to Dr Kamile Leonardi Dutra, PostgrUniversit�ario, Trindade CEP: 88040-370, Florianopolis, SC, Brazil. E-0099-2399/$ - see front matter
Copyright ª 2016 American Association of Endodontists.http://dx.doi.org/10.1016/j.joen.2015.12.015
356 Leonardi Dutra et al.
diagnostic accuracy on the discrimination of artificial AP from no lesions, whereasCBCT imaging showed excellent accuracy values. (J Endod 2016;42:356–364)
Key Wordsdental radiography, diagnosis, meta-analysis, periapical periodontitis, review, sensi-tivity, specificity, X-ray computed tomographic imaging
Apical periodontitis (AP) is an inflammatory/immune response in the apical perio-dontium that often results from intracanal microorganisms (1). The resulting api-
cal bone resorption is a defense mechanism that prevents the spread of infection andappears radiolucent on radiographs (2, 3).
Because AP is usually asymptomatic, it is frequently only detected during routineradiographic examination (4). In this sense, radiography is essential for the successfuland timely diagnosis of AP and historically has been limited to periapical and panoramicradiographs (5). However, periapical radiographs and panoramic imaging have inherentlimitations such as superimposition and distortion of important structures that commonlymask lesions (6, 7). In addition, lesions in cancellous bone cannot be consistentlydetected with these radiographic techniques (8). Therefore, in some cases, extensivebone resorption may be present even when there is no radiographic evidence of it (8,9).
Currently, the use of cone-beam computed tomographic (CBCT) imaging hasmade it possible to visualize the related anatomic structures in 3 dimensions with higherresolution. This has improved the overall diagnostic efficacy and made early diagnosispossible for some specific clinical situations (10, 11). In endodontic practice, CBCTimaging with limited field of view (FOV) has been suggested for diagnosis in patientswith contradictory or nonspecific clinical signs and symptoms (12).
Clinicians must be aware of how accurate each radiographic method is and whichimage can provide the most reliable information regarding bone resorption around theAP. To the best of the authors’ knowledge, there are no studies correlating the diagnosticaccuracy (sensitivity and specificity) of conventional radiography and CBCT imaging bymeans of a meta-analysis.
A previous systematic review of radiologic diagnosis of AP in endodontics foundthat the diagnosis made through conventional periapical radiography (CPR) presentedsimilar accuracy outcomes compared with digital periapical radiography (DPR) andCBCT imaging (13). Another systematic review that evaluated the diagnostic efficacy
nter, Federal University of Santa Catarina, Florianopolis, Santa Catarina, Brazil; †Postgraduate Pro-of Sao Paulo, Sao Paulo, Brazil; ‡School of Dentistry, Faculty of Medicine and Dentistry University ofUniversit�e Laval, Qu�ebec, Canada; ¶Department of Dentistry, Federal University of Santa Catarina,nce-based Research, Federal University of Santa Catarina, Florianopolis, Santa Catarina, Brazil.aduate Program in Dentistry, Health Sciences Center, Federal University of Santa Catarina, Campusmail address: [email protected]
JOE — Volume 42, Number 3, March 2016

Review Article
of CBCT imaging for AP focused on a 6-tiered hierarchical model andconcluded that the standard use of CBCT imaging for diagnosing APwas not justified (14). However, these systematic reviews did not pro-vide a specific quantitative synthesis (meta-analysis) of the available ev-idence regarding the diagnostic capability of the radiographic methods.Therefore, the present systematic review and meta-analysis wereperformed to answer the following focused question: ‘‘What is the diag-nostic accuracy of conventional radiography and CBCT imaging on thediscrimination of AP versus no lesion?’’
MethodsThis systematic review followed the Preferred Reporting Items for
Systematic Reviews and Meta-Analyses checklist (15) and the appro-priate Cochrane guidelines (16).
Protocol and RegistrationThe systematic review protocol was registered at the international
prospective register of systematic reviews (PROSPERO) (17) undernumber CRD42015024704.
Study DesignA systematic review of human studies was undertaken to evaluate
the diagnostic accuracy of conventional radiography and CBCT imaging,including conventional and digital panoramic and periapical radio-graphs, to assess AP. The accuracy of the images was used to discrim-inate the diagnosis of AP from no lesion.
Eligibility CriteriaInclusion Criteria. Studies in which the primary objective was toevaluate the diagnostic accuracy of conventional radiography andCBCT imaging, including conventional and digital panoramic and peri-apical radiographs, to assess AP in humans were included. The goldstandard was histologic examination of periapical biopsy specimensfor in vivo and postmortem studies or in situ visualization of bone de-fects for induced artificial AP for in vitro studies. Studies performing adiagnosis of actual or artificial AP compared with a control group withno lesions were selected. No language or time restrictions were applied.
Exclusion Criteria. Exclusion criteria included studies that did notassess actual or artificial AP; reviews, case reports, letters, personalopinions, book chapters, and conference abstracts; studies conductedusing animal models; studies that evaluated other diagnostic methodssuch as micro–computed tomographic imaging, ultrasonography,and radiographic subtraction; studies that did not use the preconizedgold standard; noncontrolled studies in which the presence or absenceof lesions could not be assessed; and studies that did not report sensi-tivity or specificity or in which the data reported could not be used toextrapolate diagnostic accuracy.
Information SourcesDetailed individual search strategies for each of the following elec-
tronic databases were performed: Embase, Google Scholar, LILACS, MED-LINE using the Ovid search engine, PubMed, Science Direct, Scopus, andWeb of Science. ProQuest was searched for additional partial gray literaturefor any references that may have beenmissed. All searches were conductedon May 18, 2015. In addition to the electronic search, a hand search wasmade, and reference lists of the selected articles were screened.
Search StrategyAppropriate key words and Medical Subject Heading terms were
selected and combined with the use of Boolean operators (AND,
JOE — Volume 42, Number 3, March 2016
OR). The search strategy was adapted for each database search withthe support of a health sciences librarian (Supplemental Table S1 isavailable online at www.jendodon.com).
The following search string summarizes the initial search done inPubMed: ([‘‘Periapical lesions’’ OR ‘‘periapical periodontitis’’ OR‘‘periapical radiolucency’’ OR ‘‘dental pulp diseases’’ OR ‘‘periapicaldiseases’’ OR ‘‘apical pathology’’ OR ‘‘endodontic pathology’’ OR ‘‘peri-apical healing’’ OR ‘‘periapical repair’’] AND [‘‘sensitivity’’ OR ‘‘speci-ficity’’ OR ‘‘accuracy’’ OR ‘‘receiver operating characteristics curve’’]AND [‘‘dental radiography’’ OR ‘‘panoramic radiography’’ OR ‘‘periap-ical radiography’’ OR ‘‘cone beam computed tomography’’]).
EndNote basic software (Thompson Reuters, New York, NY) wasused to remove any duplicate articles.
Study SelectionA 2-phase selection of articles was conducted. In phase 1, 2 re-
viewers with expertise in endodontics and oral radiology independentlyreviewed the titles and abstracts of all the references. Any articles thatdid not appear to meet the inclusion criteria were excluded. In phase2, the selected full articles were independently reviewed and screenedby the same reviewers. Any disagreement was resolved by means of dis-cussion. When mutual agreement between the 2 reviewers was notreached, a third reviewer with expertise in oral radiology was involvedto make a final decision. The final selection was always based on the fulltext of the publication.
Data Items and Collection ProcessFor all the included studies, the following descriptive characteristics
were recorded: study characteristics (authors, year, and country ofpublication), sample characteristics (type and size), intervention charac-teristics (lesions, control group, index test, and reference standard),observer characteristics (number, type, and kappa value), and findings.One reviewer collected the required information from the selected articles.The second reviewer cross-checked the collected information andconfirmed its accuracy. Again, any disagreement in either phase wasresolved by means of discussion, and the third reviewer made a final de-cision if consensus was not reached by the first 2 reviewers. If the requireddata were not complete or the data presented could not be extrapolated,attempts were made to contact the authors to retrieve the missing informa-tion. No further information was obtained through these contact attempts.
Risk of Bias in Individual StudiesThe methodologic quality of the selected studies was evaluated us-
ing the Quality Assessment Tool for Diagnostic Accuracy Studies-2(QUADAS-2) (18). It consisted of 4 key domains that discussed patientselection, index test, reference standard, flow of patients through thestudy, and timing of the index tests and reference standard. Two authorsindependently assessed each domain in terms of the potential risk ofbias. Risk of bias was judged as ‘‘low,’’ ‘‘high,’’ or ‘‘unclear,’’ and a thirdreviewer resolved any disagreement when needed.
Summary MeasuresThe diagnostic sensitivity and specificity of radiographic methods
in the detection of AP against controls (no lesions) were considered asthe main outcome.
Synthesis of ResultsTo decrease the heterogeneity, the studies were analyzed in 3
groups (only ones for which data were available): CPR, DPR, andCBCT imaging. The accuracy of the different imaging methods to
Accuracy of CBCT and CPR on Apical Periodontitis 357
Review Article
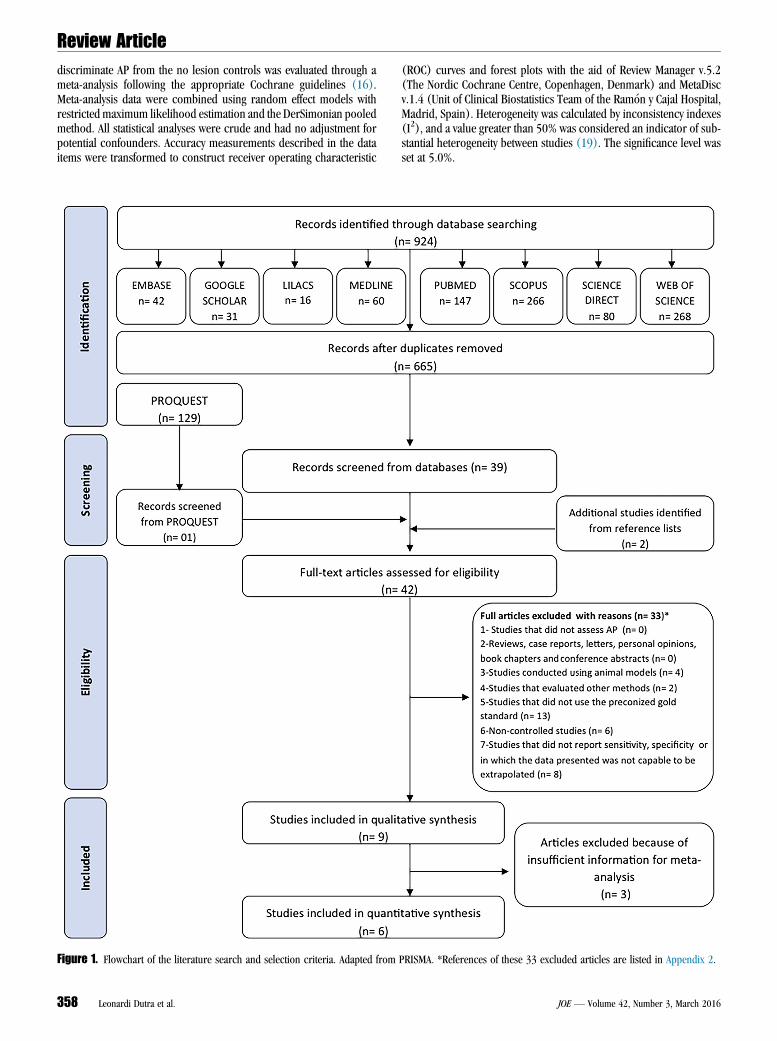
discriminate AP from the no lesion controls was evaluated through ameta-analysis following the appropriate Cochrane guidelines (16).Meta-analysis data were combined using random effect models withrestricted maximum likelihood estimation and the DerSimonian pooledmethod. All statistical analyses were crude and had no adjustment forpotential confounders. Accuracy measurements described in the dataitems were transformed to construct receiver operating characteristicFigure 1. Flowchart of the literature search and selection criteria. Adapted from
358 Leonardi Dutra et al.
(ROC) curves and forest plots with the aid of Review Manager v.5.2(The Nordic Cochrane Centre, Copenhagen, Denmark) and MetaDiscv.1.4 (Unit of Clinical Biostatistics Team of the Ram�on y Cajal Hospital,Madrid, Spain). Heterogeneity was calculated by inconsistency indexes(I2), and a value greater than 50% was considered an indicator of sub-stantial heterogeneity between studies (19). The significance level wasset at 5.0%.
PRISMA. *References of these 33 excluded articles are listed in Appendix 2.
JOE — Volume 42, Number 3, March 2016
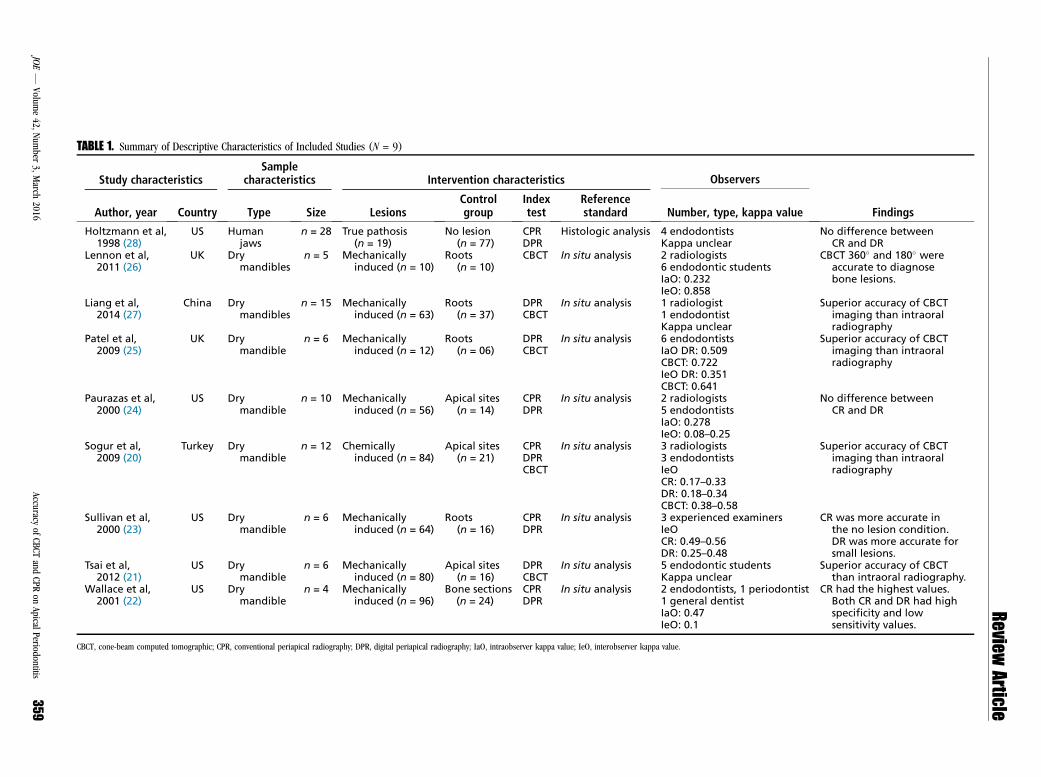
TABLE 1. Summary of Descriptive Characteristics of Included Studies (N = 9)
Study characteristicsSample
characteristics Intervention characteristics Observers
FindingsAuthor, year Country Type Size LesionsControlgroup
Indextest
Referencestandard Number, type, kappa value
Holtzmann et al,1998 (28)
US Humanjaws
n = 28 True pathosis(n = 19)
No lesion(n = 77)
CPRDPR
Histologic analysis 4 endodontistsKappa unclear
No difference betweenCR and DR
Lennon et al,2011 (26)
UK Drymandibles
n = 5 Mechanicallyinduced (n = 10)
Roots(n = 10)
CBCT In situ analysis 2 radiologists6 endodontic studentsIaO: 0.232IeO: 0.858
CBCT 360� and 180� wereaccurate to diagnosebone lesions.
Liang et al,2014 (27)
China Drymandibles
n = 15 Mechanicallyinduced (n = 63)
Roots(n = 37)
DPRCBCT
In situ analysis 1 radiologist1 endodontistKappa unclear
Superior accuracy of CBCTimaging than intraoralradiography
Patel et al,2009 (25)
UK Drymandible
n = 6 Mechanicallyinduced (n = 12)
Roots(n = 06)
DPRCBCT
In situ analysis 6 endodontistsIaO DR: 0.509CBCT: 0.722IeO DR: 0.351CBCT: 0.641
Superior accuracy of CBCTimaging than intraoralradiography
Paurazas et al,2000 (24)
US Drymandible
n = 10 Mechanicallyinduced (n = 56)
Apical sites(n = 14)
CPRDPR
In situ analysis 2 radiologists5 endodontistsIaO: 0.278IeO: 0.08–0.25
No difference betweenCR and DR
Sogur et al,2009 (20)
Turkey Drymandible
n = 12 Chemicallyinduced (n = 84)
Apical sites(n = 21)
CPRDPRCBCT
In situ analysis 3 radiologists3 endodontistsIeOCR: 0.17–0.33DR: 0.18–0.34CBCT: 0.38–0.58
Superior accuracy of CBCTimaging than intraoralradiography
Sullivan et al,2000 (23)
US Drymandible
n = 6 Mechanicallyinduced (n = 64)
Roots(n = 16)
CPRDPR
In situ analysis 3 experienced examinersIeOCR: 0.49–0.56DR: 0.25–0.48
CR was more accurate inthe no lesion condition.DR was more accurate forsmall lesions.
Tsai et al,2012 (21)
US Drymandible
n = 6 Mechanicallyinduced (n = 80)
Apical sites(n = 16)
DPRCBCT
In situ analysis 5 endodontic studentsKappa unclear
Superior accuracy of CBCTthan intraoral radiography.
Wallace et al,2001 (22)
US Drymandible
n = 4 Mechanicallyinduced (n = 96)
Bone sections(n = 24)
CPRDPR
In situ analysis 2 endodontists, 1 periodontist1 general dentistIaO: 0.47IeO: 0.1
CR had the highest values.Both CR and DR had highspecificity and lowsensitivity values.
CBCT, cone-beam computed tomographic; CPR, conventional periapical radiography; DPR, digital periapical radiography; IaO, intraobserver kappa value; IeO, interobserver kappa value.
ReviewArticle
JOE—
Volume42,
Num
ber3,March
2016Accuracy
ofCBCT
andCPR
onApical
Periodontitis359
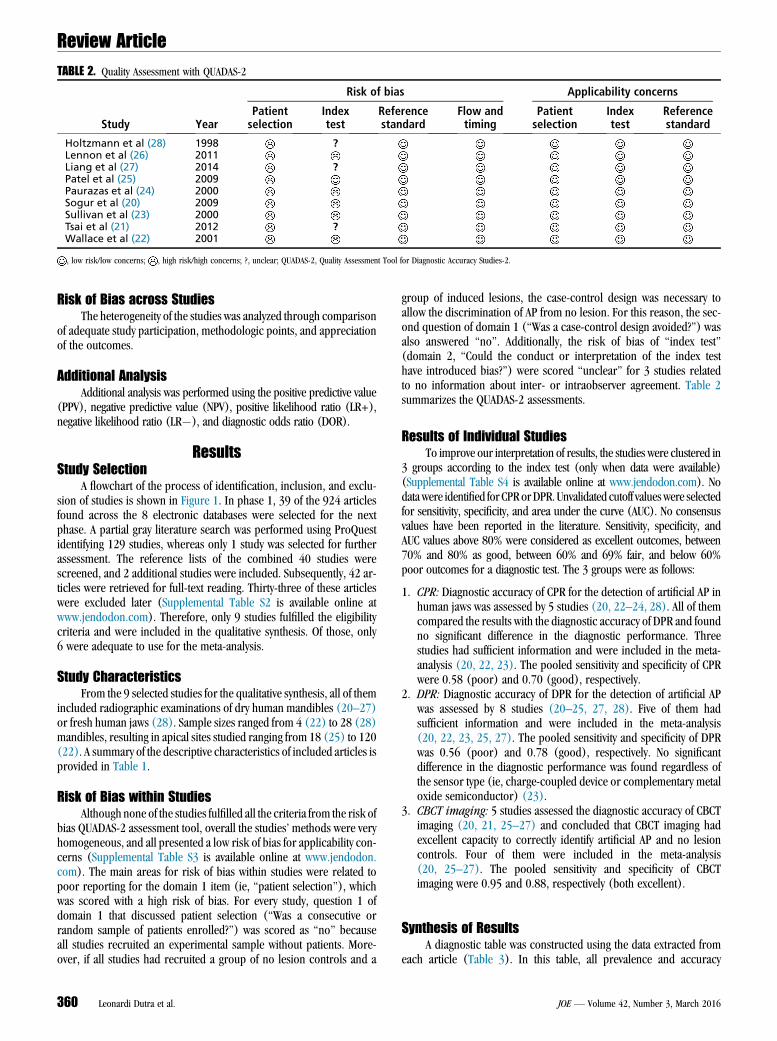
TABLE 2. Quality Assessment with QUADAS-2
Study Year
Risk of bias Applicability concerns
Patientselection
Indextest
Referencestandard
Flow andtiming
Patientselection
Indextest
Referencestandard
Holtzmann et al (28) 1998 ?Lennon et al (26) 2011Liang et al (27) 2014 ?Patel et al (25) 2009Paurazas et al (24) 2000Sogur et al (20) 2009Sullivan et al (23) 2000Tsai et al (21) 2012 ?Wallace et al (22) 2001
, low risk/low concerns; , high risk/high concerns; ?, unclear; QUADAS-2, Quality Assessment Tool for Diagnostic Accuracy Studies-2.
Review Article
Risk of Bias across StudiesThe heterogeneity of the studies was analyzed through comparison
of adequate study participation, methodologic points, and appreciationof the outcomes.
Additional AnalysisAdditional analysis was performed using the positive predictive value
(PPV), negative predictive value (NPV), positive likelihood ratio (LR+),negative likelihood ratio (LR�), and diagnostic odds ratio (DOR).
ResultsStudy Selection
A flowchart of the process of identification, inclusion, and exclu-sion of studies is shown in Figure 1. In phase 1, 39 of the 924 articlesfound across the 8 electronic databases were selected for the nextphase. A partial gray literature search was performed using ProQuestidentifying 129 studies, whereas only 1 study was selected for furtherassessment. The reference lists of the combined 40 studies werescreened, and 2 additional studies were included. Subsequently, 42 ar-ticles were retrieved for full-text reading. Thirty-three of these articleswere excluded later (Supplemental Table S2 is available online atwww.jendodon.com). Therefore, only 9 studies fulfilled the eligibilitycriteria and were included in the qualitative synthesis. Of those, only6 were adequate to use for the meta-analysis.
Study CharacteristicsFrom the 9 selected studies for the qualitative synthesis, all of them
included radiographic examinations of dry human mandibles (20–27)or fresh human jaws (28). Sample sizes ranged from 4 (22) to 28 (28)mandibles, resulting in apical sites studied ranging from 18 (25) to 120(22). A summary of the descriptive characteristics of included articles isprovided in Table 1.
Risk of Bias within StudiesAlthough none of the studies fulfilled all the criteria from the risk of
bias QUADAS-2 assessment tool, overall the studies’ methods were veryhomogeneous, and all presented a low risk of bias for applicability con-cerns (Supplemental Table S3 is available online at www.jendodon.com). The main areas for risk of bias within studies were related topoor reporting for the domain 1 item (ie, ‘‘patient selection’’), whichwas scored with a high risk of bias. For every study, question 1 ofdomain 1 that discussed patient selection (‘‘Was a consecutive orrandom sample of patients enrolled?’’) was scored as ‘‘no’’ becauseall studies recruited an experimental sample without patients. More-over, if all studies had recruited a group of no lesion controls and a
360 Leonardi Dutra et al.
group of induced lesions, the case-control design was necessary toallow the discrimination of AP from no lesion. For this reason, the sec-ond question of domain 1 (‘‘Was a case-control design avoided?’’) wasalso answered ‘‘no’’. Additionally, the risk of bias of ‘‘index test’’(domain 2, ‘‘Could the conduct or interpretation of the index testhave introduced bias?’’) were scored ‘‘unclear’’ for 3 studies relatedto no information about inter- or intraobserver agreement. Table 2summarizes the QUADAS-2 assessments.
Results of Individual StudiesTo improve our interpretation of results, the studies were clustered in
3 groups according to the index test (only when data were available)(Supplemental Table S4 is available online at www.jendodon.com). Nodatawere identified for CPRorDPR. Unvalidated cutoff valueswere selectedfor sensitivity, specificity, and area under the curve (AUC). No consensusvalues have been reported in the literature. Sensitivity, specificity, andAUC values above 80% were considered as excellent outcomes, between70% and 80% as good, between 60% and 69% fair, and below 60%poor outcomes for a diagnostic test. The 3 groups were as follows:
1. CPR: Diagnostic accuracy of CPR for the detection of artificial AP inhuman jaws was assessed by 5 studies (20, 22–24, 28). All of themcompared the results with the diagnostic accuracy of DPR and foundno significant difference in the diagnostic performance. Threestudies had sufficient information and were included in the meta-analysis (20, 22, 23). The pooled sensitivity and specificity of CPRwere 0.58 (poor) and 0.70 (good), respectively.
2. DPR: Diagnostic accuracy of DPR for the detection of artificial APwas assessed by 8 studies (20–25, 27, 28). Five of them hadsufficient information and were included in the meta-analysis(20, 22, 23, 25, 27). The pooled sensitivity and specificity of DPRwas 0.56 (poor) and 0.78 (good), respectively. No significantdifference in the diagnostic performance was found regardless ofthe sensor type (ie, charge-coupled device or complementary metaloxide semiconductor) (23).
3. CBCT imaging: 5 studies assessed the diagnostic accuracy of CBCTimaging (20, 21, 25–27) and concluded that CBCT imaging hadexcellent capacity to correctly identify artificial AP and no lesioncontrols. Four of them were included in the meta-analysis(20, 25–27). The pooled sensitivity and specificity of CBCTimaging were 0.95 and 0.88, respectively (both excellent).
Synthesis of ResultsA diagnostic table was constructed using the data extracted from
each article (Table 3). In this table, all prevalence and accuracy
JOE — Volume 42, Number 3, March 2016
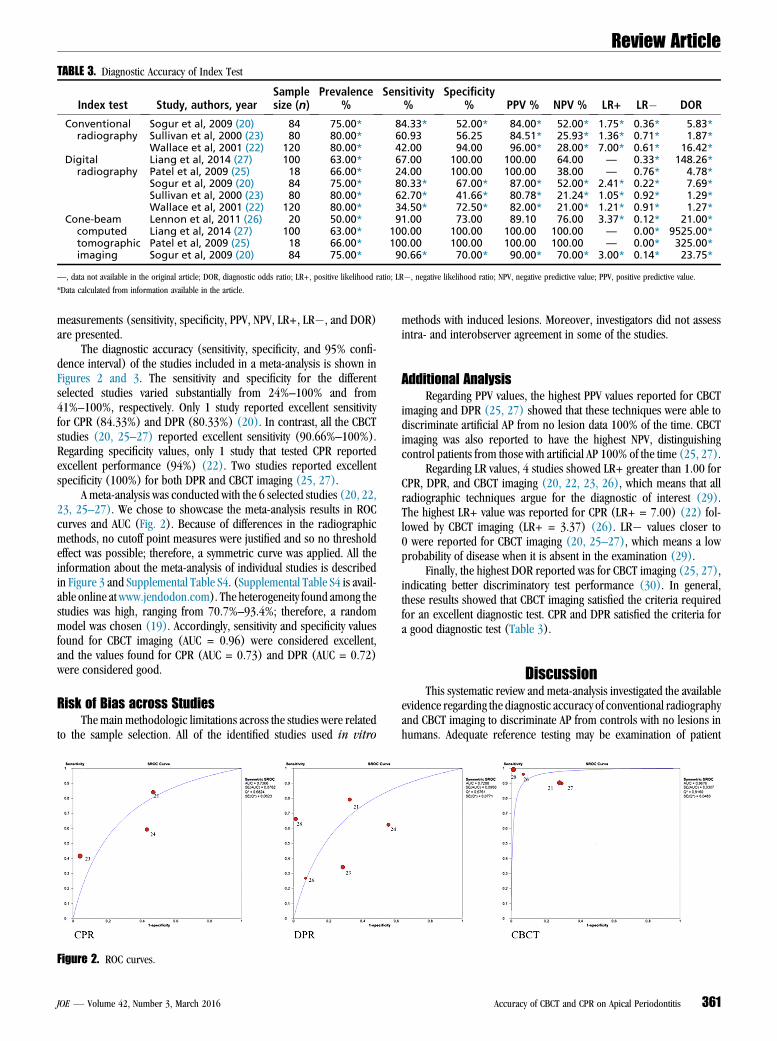
TABLE 3. Diagnostic Accuracy of Index Test
Index test Study, authors, yearSamplesize (n)
Prevalence%
Sensitivity%
Specificity% PPV % NPV % LR+ LR� DOR
Conventionalradiography
Sogur et al, 2009 (20) 84 75.00* 84.33* 52.00* 84.00* 52.00* 1.75* 0.36* 5.83*Sullivan et al, 2000 (23) 80 80.00* 60.93 56.25 84.51* 25.93* 1.36* 0.71* 1.87*Wallace et al, 2001 (22) 120 80.00* 42.00 94.00 96.00* 28.00* 7.00* 0.61* 16.42*
Digitalradiography
Liang et al, 2014 (27) 100 63.00* 67.00 100.00 100.00 64.00 — 0.33* 148.26*Patel et al, 2009 (25) 18 66.00* 24.00 100.00 100.00 38.00 — 0.76* 4.78*Sogur et al, 2009 (20) 84 75.00* 80.33* 67.00* 87.00* 52.00* 2.41* 0.22* 7.69*Sullivan et al, 2000 (23) 80 80.00* 62.70* 41.66* 80.78* 21.24* 1.05* 0.92* 1.29*Wallace et al, 2001 (22) 120 80.00* 34.50* 72.50* 82.00* 21.00* 1.21* 0.91* 1.27*
Cone-beamcomputedtomographicimaging
Lennon et al, 2011 (26) 20 50.00* 91.00 73.00 89.10 76.00 3.37* 0.12* 21.00*Liang et al, 2014 (27) 100 63.00* 100.00 100.00 100.00 100.00 — 0.00* 9525.00*Patel et al, 2009 (25) 18 66.00* 100.00 100.00 100.00 100.00 — 0.00* 325.00*Sogur et al, 2009 (20) 84 75.00* 90.66* 70.00* 90.00* 70.00* 3.00* 0.14* 23.75*
—, data not available in the original article; DOR, diagnostic odds ratio; LR+, positive likelihood ratio; LR�, negative likelihood ratio; NPV, negative predictive value; PPV, positive predictive value.
*Data calculated from information available in the article.
Review Article
measurements (sensitivity, specificity, PPV, NPV, LR+, LR�, and DOR)are presented.
The diagnostic accuracy (sensitivity, specificity, and 95% confi-dence interval) of the studies included in a meta-analysis is shown inFigures 2 and 3. The sensitivity and specificity for the differentselected studies varied substantially from 24%–100% and from41%–100%, respectively. Only 1 study reported excellent sensitivityfor CPR (84.33%) and DPR (80.33%) (20). In contrast, all the CBCTstudies (20, 25–27) reported excellent sensitivity (90.66%–100%).Regarding specificity values, only 1 study that tested CPR reportedexcellent performance (94%) (22). Two studies reported excellentspecificity (100%) for both DPR and CBCT imaging (25, 27).
A meta-analysis was conducted with the 6 selected studies (20, 22,23, 25–27). We chose to showcase the meta-analysis results in ROCcurves and AUC (Fig. 2). Because of differences in the radiographicmethods, no cutoff point measures were justified and so no thresholdeffect was possible; therefore, a symmetric curve was applied. All theinformation about the meta-analysis of individual studies is describedin Figure 3 and Supplemental Table S4. (Supplemental Table S4 is avail-able online at www.jendodon.com). The heterogeneity found among thestudies was high, ranging from 70.7%–93.4%; therefore, a randommodel was chosen (19). Accordingly, sensitivity and specificity valuesfound for CBCT imaging (AUC = 0.96) were considered excellent,and the values found for CPR (AUC = 0.73) and DPR (AUC = 0.72)were considered good.
Risk of Bias across StudiesThe main methodologic limitations across the studies were related
to the sample selection. All of the identified studies used in vitro
Figure 2. ROC curves.
JOE — Volume 42, Number 3, March 2016
methods with induced lesions. Moreover, investigators did not assessintra- and interobserver agreement in some of the studies.
Additional AnalysisRegarding PPV values, the highest PPV values reported for CBCT
imaging and DPR (25, 27) showed that these techniques were able todiscriminate artificial AP from no lesion data 100% of the time. CBCTimaging was also reported to have the highest NPV, distinguishingcontrol patients from those with artificial AP 100% of the time (25, 27).
Regarding LR values, 4 studies showed LR+ greater than 1.00 forCPR, DPR, and CBCT imaging (20, 22, 23, 26), which means that allradiographic techniques argue for the diagnostic of interest (29).The highest LR+ value was reported for CPR (LR+ = 7.00) (22) fol-lowed by CBCT imaging (LR+ = 3.37) (26). LR� values closer to0 were reported for CBCT imaging (20, 25–27), which means a lowprobability of disease when it is absent in the examination (29).
Finally, the highest DOR reported was for CBCT imaging (25, 27),indicating better discriminatory test performance (30). In general,these results showed that CBCT imaging satisfied the criteria requiredfor an excellent diagnostic test. CPR and DPR satisfied the criteria fora good diagnostic test (Table 3).
DiscussionThis systematic review and meta-analysis investigated the available
evidence regarding the diagnostic accuracy of conventional radiographyand CBCT imaging to discriminate AP from controls with no lesions inhumans. Adequate reference testing may be examination of patient
Accuracy of CBCT and CPR on Apical Periodontitis 361
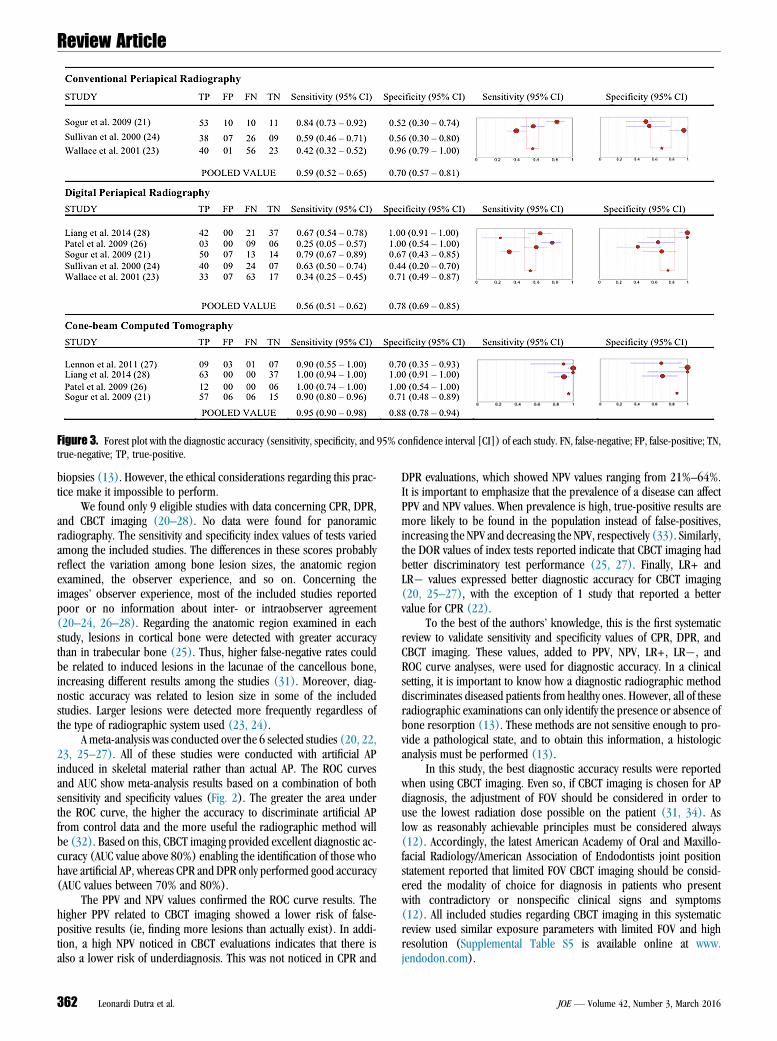
Figure 3. Forest plot with the diagnostic accuracy (sensitivity, specificity, and 95% confidence interval [CI]) of each study. FN, false-negative; FP, false-positive; TN,true-negative; TP, true-positive.
Review Article
biopsies (13). However, the ethical considerations regarding this prac-tice make it impossible to perform.
We found only 9 eligible studies with data concerning CPR, DPR,and CBCT imaging (20–28). No data were found for panoramicradiography. The sensitivity and specificity index values of tests variedamong the included studies. The differences in these scores probablyreflect the variation among bone lesion sizes, the anatomic regionexamined, the observer experience, and so on. Concerning theimages’ observer experience, most of the included studies reportedpoor or no information about inter- or intraobserver agreement(20–24, 26–28). Regarding the anatomic region examined in eachstudy, lesions in cortical bone were detected with greater accuracythan in trabecular bone (25). Thus, higher false-negative rates couldbe related to induced lesions in the lacunae of the cancellous bone,increasing different results among the studies (31). Moreover, diag-nostic accuracy was related to lesion size in some of the includedstudies. Larger lesions were detected more frequently regardless ofthe type of radiographic system used (23, 24).
A meta-analysis was conducted over the 6 selected studies (20, 22,23, 25–27). All of these studies were conducted with artificial APinduced in skeletal material rather than actual AP. The ROC curvesand AUC show meta-analysis results based on a combination of bothsensitivity and specificity values (Fig. 2). The greater the area underthe ROC curve, the higher the accuracy to discriminate artificial APfrom control data and the more useful the radiographic method willbe (32). Based on this, CBCT imaging provided excellent diagnostic ac-curacy (AUC value above 80%) enabling the identification of those whohave artificial AP, whereas CPR and DPR only performed good accuracy(AUC values between 70% and 80%).
The PPV and NPV values confirmed the ROC curve results. Thehigher PPV related to CBCT imaging showed a lower risk of false-positive results (ie, finding more lesions than actually exist). In addi-tion, a high NPV noticed in CBCT evaluations indicates that there isalso a lower risk of underdiagnosis. This was not noticed in CPR and
362 Leonardi Dutra et al.
DPR evaluations, which showed NPV values ranging from 21%–64%.It is important to emphasize that the prevalence of a disease can affectPPV and NPV values. When prevalence is high, true-positive results aremore likely to be found in the population instead of false-positives,increasing the NPV and decreasing the NPV, respectively (33). Similarly,the DOR values of index tests reported indicate that CBCT imaging hadbetter discriminatory test performance (25, 27). Finally, LR+ andLR� values expressed better diagnostic accuracy for CBCT imaging(20, 25–27), with the exception of 1 study that reported a bettervalue for CPR (22).
To the best of the authors’ knowledge, this is the first systematicreview to validate sensitivity and specificity values of CPR, DPR, andCBCT imaging. These values, added to PPV, NPV, LR+, LR�, andROC curve analyses, were used for diagnostic accuracy. In a clinicalsetting, it is important to know how a diagnostic radiographic methoddiscriminates diseased patients from healthy ones. However, all of theseradiographic examinations can only identify the presence or absence ofbone resorption (13). These methods are not sensitive enough to pro-vide a pathological state, and to obtain this information, a histologicanalysis must be performed (13).
In this study, the best diagnostic accuracy results were reportedwhen using CBCT imaging. Even so, if CBCT imaging is chosen for APdiagnosis, the adjustment of FOV should be considered in order touse the lowest radiation dose possible on the patient (31, 34). Aslow as reasonably achievable principles must be considered always(12). Accordingly, the latest American Academy of Oral and Maxillo-facial Radiology/American Association of Endodontists joint positionstatement reported that limited FOV CBCT imaging should be consid-ered the modality of choice for diagnosis in patients who presentwith contradictory or nonspecific clinical signs and symptoms(12). All included studies regarding CBCT imaging in this systematicreview used similar exposure parameters with limited FOV and highresolution (Supplemental Table S5 is available online at www.jendodon.com).
JOE — Volume 42, Number 3, March 2016
Review Article
Studies that did not compare an index test with the gold standardwere not included (35–47) because only an acceptable gold standardcan prove the clinical relevance and reduce the risks of both false-positive and false-negative findings (31). Adequate reference testingmay be the examination of biopsies from patients and autopsies fromdeceased individuals (13, 28, 31). However, ethical considerationsregarding this practice make it impossible to perform. In this study,we considered the in situ visualization of artificial lesions (in vitrostudies) (20–27) or the histologic analysis of the surgical specimen(in vivo and postmortem studies) (28) as the gold standard. Studiesusing an animal model were excluded (31, 48–50) because of thedifferent apical anatomy that may be correlated to poor accuracyresults, leading to no clinical extrapolation (31).
The main methodologic limitation of our systematic review is thatall included studies used in vitro methods in which artificial AP wereinduced in the skeletal material by drilled holes (21–27) or acidapplied at the periapical bone tissue (20). Even though mechanicallyinduced lesions can be accurately measured, it does not produce thediffuse borders of natural AP, and chemically induced lesions have amore natural appearance but are difficult to measure (13).
In conclusion, CPR and DPR showed good diagnostic accuracy onthe discrimination of artificial AP from no lesion, whereas CBCT imagingreported excellent accuracy values.
AcknowledgmentsThe authors thank Mrs Maria Gorete Monteguti Savi for her
invaluable contribution at the stage of the search strategy con-struction.
The authors deny any conflicts of interest related to this study.
Supplementary MaterialSupplementary material associated with this article can be
found in the online version at www.jendodon.com (http://dx.doi.org/10.1016/j.joen.2015.12.015).
References1. American Association of Endodontists. Glossary of Endodontic Terms, 8th ed. Chi-
cago: American Association of Endodontists; 2012. Available at: http://www.aae.org/uAPoadedfiles/publications_and_research/member_publications/03glossaryofendoterms_web(1).pdf. Acessed September 10, 2015.
2. Nair PN. New perspectives on radicular cysts: do they heal? Int Endod J 1998;31:155–60.
3. Kakehashi S, Stanley HR, Fitzgerald RJ. The effects of surgical exposures of dentalpulps in germ-free and conventional laboratory rats. Oral Surg Oral Med Oral Pathol1965;20:340–9.
4. Bender IB. Factors influencing the radiographic appearance of bony lesions.J Endod 1982;8:161–70.
5. American Association of Endodontists, American Academy of Oral and MaxillofacialRadiology. Use of cone-beam computed tomography in endodontics. Joint PositionStatement of the American Association of Endodontists and the American Academyof Oral and Maxillofacial Radiology. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2011;111:234–7.
6. LeQuire AK, Cunningham CJ, Pelleu GB Jr. Radiographic interpretation of experi-mentally produced osseous lesions of the human mandible. J Endod 1977;3:274–6.
7. Katebzadeh N, Hupp J, Trope M. Histological periapical repair after obturation ofinfected root canals in dogs. J Endod 1999;25:364–8.
8. Bender IB, Seltzer S. Roentgenographic and direct obervation of experimental le-sions in bone. J Am Dent Assoc 1961;62:708.
9. Bender IB, Seltzer S. Roentgenographic and direct observation of experimental le-sions in bone: I. 1961. J Endod 2003;29:702–6.
10. Patel S, Durack C, Abella F, et al. Cone beam computed tomography in endodontics:a review. Int Endod J 2015;48:3–15.
11. Nair MK, Nair UP. Digital and advanced imaging in endodontics: a review. J Endod2007;33:1–6.
JOE — Volume 42, Number 3, March 2016
12. American Association of Endodontists; American Academy of Oral and MaxillofacialRadiology. Use of cone beam-computed tomography in endodontics: 2015 update.Available at: http://www.aae.org/uAPoadedfiles/clinical_resources/guidelines_and_position_statements/cbctstatement_2015update.pdf. Accessed September10, 2015.
13. Petersson A, Axelsson S, Davidson T, et al. Radiological diagnosis of periapicalbone tissue lesions in endodontics: a systematic review. Int Endod J 2012;45:783–801.
14. Kruse C, Spin-Neto R, Wenzel A, Kirkevang LL. Cone beam computed tomographyand periapical lesions: a systematic review analysing studies on diagnostic efficacyby a hierarchical model. Int Endod J 2015;48:815–28.
15. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematicreviews and meta-analyses: the PRISMA statement. Int J Surg 2010;8:336–41.
16. Deeks J, Gatsonis C, The Cochrane Collaboration. Cochrane handbook for system-atic reviews of diagnostic test accuracy version 1.0. Available at: http://srdta.cochrane.org/. Accessed April 16, 2015.
17. Prospero. International prospective register of systematic reviews.CDR42015024704. Available at: http://www.cdr.york.ac.uk/prospero/disAPay_record.asp?ID=CRD42015024704. Accessed May 4, 2015.
18. Whiting PF, Rutjes AW, Westwood ME, et al. QUADAS-2: a revised tool for the qualityassessment of diagnostic accuracy studies. Ann Intern Med 2011;155:529–36.
19. Deeks J, Higgins J, Altman D. Analysing data and undertaking meta-analysis. In:Higgins J, Green S, eds. Cochrane Handbook for Systematic Reviews of InterventionsVersion 5.1.0 [update March 2011]. The Cochrane Collaboration; 2011. Availableat: http://srdta.cochrane.org/. Accessed April 16, 2015.
20. Sogur E, Baksi BG, Grondahl HG, et al. Detectability of chemically induced apicalperiodontitis by limited cone beam computed tomography, intra-oral digital andconventional film radiography. Dentomaxillofac Radiol 2009;38:458–64.
21. Tsai P, Torabinejad M, Rice D, Azevedo B. Accuracy of cone-beam computed tomog-raphy and periapical radiography in detecting small apical periodontitis. J Endod2012;38:965–70.
22. Wallace JA, Nair MK, Abomr D, et al. A comparative evaluation of the diagnostic ef-ficacy of film and digital sensors for detection of simulated apical periodontitis. OralSurg Oral Med Oral Pathol Oral Radiol Endod 2001;92:93–7.
23. Sullivan JE, di Fiore PM, Koerber A. Radiovisiography in the detection of apical peri-odontitis. J Endod 2000;26:32–5.
24. Paurazas SB, Geist JR, Pink FE, et al. Comparison of diagnostic accuracy of digitalimaging by using CCD and CMOS-APS sensors with E-speed film in the detection ofperiapical bony lesions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000;89:356–62.
25. Patel S, Dawood A, Mannocci F, et al. Detection of periapical bone defects in humanjaws using cone beam computed tomography and intraoral radiography. Int Endod J2009;42:507–15.
26. Lennon S, Patel S, Foschi F, et al. Diagnostic accuracy of limited-volume cone-beamcomputed tomography in the detection of periapical bone loss: 360 degrees scansversus 180 degrees scans. Int Endod J 2011;44:1118–27.
27. Liang YH, Jiang L, Gao XJ, et al. Detection and measurement of artificial apical peri-odontitis by cone-beam computed tomography. Int Endod J 2014;47:332–8.
28. Holtzmann DJ, Johnson WT, Southard TE, et al. Storage-phosphor computed radi-ography versus film radiography in the detection of pathologic periradicular boneloss in cadavers. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;86:90–7.
29. McGee S. Simplifying likelihood ratios. J Gen Intern Med 2002;17:647–50.30. Glas AS, Lijmer JG, Prins MH, et al. The diagnostic odds ratio: a single indicator of
test performance. J Clin Epidemiol 2003;56:1129–35.31. Hedesiu M, Baciut M, Baciut G, et al. Comparison of cone beam CT device and field
of view for the detection of simulated periapical bone lesions. Dentomaxillofac Ra-diol 2012;41:548–52.
32. Zou K, O’Malley A, Mauri L. Receiver-operating characteristic analysis for evaluatingdiagnostic tests and predictive models. Circulation 2007;115:654–7.
33. Last JM. A Dictionary of Epidemiology, 2nd ed. New York: Oxford University Press;1988.
34. Venskutonis T, Plotino G, Juodzbalys G, Mickeviciene L. The importance of cone-beam computed tomography in the management of endodontic problems: a reviewof the literature. J Endod 2014;40:1895–901.
35. Ahlowalia MS, Patel S, Anwar HMS, et al. Accuracy of CBCT for volumetric measure-ment of simulated apical periodontitis. Int Endod J 2013;46:538–46.
36. Bohay RN. The sensitivity, specificity, and reliability of radiographic periapical diag-nosis of posterior teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000;89:639–42.
37. Eraso FE, Analoui M, Watson AB, Rebeschini R. Impact of lossy compression ondiagnostic accuracy of radiographs for apical periodontitis. Oral Surg Oral MedOral Pathol Oral Radiol Endod 2002;93:621–5.
38. Estrela C, Bueno MR, Leles CR, et al. Accuracy of cone beam computed tomographyand panoramic and periapical radiography for detection of apical periodontitis.J Endod 2008;34:273–9.
Accuracy of CBCT and CPR on Apical Periodontitis 363

Review Article
39. Nagata Y. A comparison of diagnostic accuracy of a newly developed photofluoro-graphic panoramic system with conventional panoramic radiography. Dentomaxil-lofac Radiol 2001;30:137–40.
40. Patel N, Rushton VE, Macfarlane TV, Horner K. The influence of viewing con-ditions on radiological diagnosis of periapical inflammation. Br Dent J 2000;189:40–2.
41. Ridao-Sacie C, Segura-Egea JJ, Fernandez-Palacin A, et al. Radiologicalassessment of periapical status using the periapical index: comparison ofperiapical radiography and digital panoramic radiography. Int Endod J2007;40:433–40.
42. Rios-Santos JV, Ridao-Sacie C, Bullon P, et al. Assessment of periapical status: acomparative study using film-based periapical radiographs and digital panoramicimages. Med Oral Patol Oral Cir Bucal 2010;15:952–6.
43. Rohlin M, Kullendorff B, Ahlqwist M, et al. Comparison between panoramic andperiapical radiography in the diagnosis of periapical bone lesions. DentomaxillofacRadiol 1989;18:151–5.
44. Saidi A, Naaman A, Zogheib C. Accuracy of cone-beam computed tomography andperiapical radiography in endodontically treated teeth evaluation: a five-year retro-spective study. J Int Oral Health 2015;7:15–9.
364 Leonardi Dutra et al.
45. Tammisalo T, Luostarinen T, Vahatalo K, Tammisalo EH. Comparison of periapicaland detailed narrow-beam radiography for diagnosis of periapical bone lesions.Dentomaxillofac Radiol 1993;22:183–7.
46. Tammisalo T, Luostarinen T, Vahatalo K, et al. Radiographic detectability of peri-odontal diseases: a comparison of periapical radiography with detailed zonography.Dentomaxillofac Radiol 1995;24:185–90.
47. Venskutonis T, Plotino G, Tocci L, et al. Periapical and endodontic status scale basedon periapical bone lesions and endodontic treatment quality evaluation using cone-beam computed tomography. J Endod 2015;41:190–6.
48. Stavropoulos A, Wenzel A. Accuracy of cone beam dental CT, intraoral digital andconventional film radiography for the detection of apical periodontitis: an ex vivostudy in pig jaws. Clin Oral Investig 2007;11:101–6.
49. de Paula-Silva FW, Wu MK, Leonardo MR, et al. Accuracy of periapical radi-ography and cone-beam computed tomography scans in diagnosing apical peri-odontitis using histopathological findings as a gold standard. J Endod 2009;35:1009–12.
50. Townsend NB, Hawkes CS, Rex R, et al. Investigation of the sensitivity and specificityof radiological signs for diagnosis of periapical infection of equine cheek teeth.Equine Vet J 2011;43:170–8.
JOE — Volume 42, Number 3, March 2016