Embed Size (px)
Citation preview
1
DIAGNOSIS & TREATMENT Visceral leishmaniasis or Kala-azar is a intracellular protozoal infection caused by Leishmania donovani and transmitted by phlebotomine sandflies. Kala-azar is a major public health problem in the areas of its prevalence, principally India and its neighbors Bangladesh and Nepal, and Brazil and Sudan. In India the disease is found in Bihar, Jharkhand, West Bengal and pockets of eastern Uttar Pradesh. A national health programme to eliminate the disease by 2010 is in operation in India. The programme relies on case management, vector control, community involvement in control activities and capacity building as the principal components of the elimination strategy. The Kala-azar elimination programme is a centrally sponsored programme, under which the cost of all materials, i.e. insecticides, diagnostic kits, drugs and cost of operations is borne by the Central Government.
Diagnosis and treatment of Kala-azar are problematic because of a variety of reasons. While treatment is lengthy and relatively costly, definitive diagnosis of Kala-azar requires tissue specimens, which are conventionally obtained by organ needle aspiration for microscopic demonstration of amastigote forms in stained smears. Bone marrow and the spleen and, in some regions, lymphnode are the tissues most often sampled in patients with suspected infection. The diagnostic sensitivity of splenic aspiration is high (95% - 98%), but the procedure carries a risk of bleeding; the sensitivity of examination of bone marrow specimens is considered to be lower (53% - 95%). Organ aspiration and accurate examination of smears also require technical skills that are not uniformly available in rural areas. Culture or PCR testing of aspirate material improves parasitologic yield, but these methods are seldom undertaken outside of research laboratories (1).
In the Kala-azar endemic areas of India, Napier�s aldehyde test has been
used for a long time. The test relies on the jellification caused by the binding of the serum globulins to the formaldehyde. The serum globulins increase in a variety of infections and thus this test is rather non-specific. A positive reaction may also be seen in diseases like, tuberculosis, cirrhosis of liver, malaria, etc. Further, in kala-azar, the test becomes positive only when infection is atleast three months old and may remain positive even after six months of cure.
Therefore a rapid, accurate, field suitable and non-invasive method of diagnosis of kala-azar has long been sought to circumvent the need for obtaining tissue specimens and preceding limitations. A range of assays have been developed to detect antileishmanial antibody. In these guidelines that diagnostic tests commonly used for kala-azar diagnosis, including development of newer techniques are set out. 1. Hematological examination : Progressive leucopenia and severe anemia are striking features of L donovani infection. There is a progressive decline in total leucocyte count. Differential leucocyte count gives a higher monocyte and lymphocyte count. The total erythrocyte and platelet counts also decline but the decline in erythrocyte count is not comparable to the extent of leuocopenia. There is severe anemia and as such the haemoglobin contents must be estimated.
id24612168 pdfMachine by Broadgun Software - a great PDF writer! - a great PDF creator! - http://www.pdfmachine.com http://www.broadgun.com
2
2. Detection of Leishmania donovani : For detection of the presence of L. donovani in the body of the patient, a variety of tests are being used.
(a) Serological tests (b) Napier�s Aldehyde test
The concentration of gamaglobulins in blood increases considerably following infection with L.donovani.. Formaldehyde has a tendency to blind these serum immunoglobulins. The aldehyde test procedure is simple. Five cubic millimeter�s venous blood is drawn from the patient and left for clotting. Serum is separated by removing supernatant after centrifugation. To one ml of serum, 2-3 drops of commercial formalin (40% formaldehyde) are added. Opaque jellification like white of a boiled egg indicates a positive reaction. Jellification time indicates intensify of infection as indicated in the table below:
Jellification time Intensity of reaction 2 minutes ++++ 20 minutes +++ 120 minutes ++ 24 hours +
The serum globulins increase in a variety of infections and thus this test is considered to be rather non-specific. A positive reaction may also be seen in diseases like tubeculosis, cirrhosis of liver, malaria, etc. Further, in kala-azar, the test becomes positive only when infection is at least three months old and may remain so even after six months of cure. Napier and Das Gupta (1931) recorded that 98 percent of cases showing a definitely positive aldehyde reaction were kala-azar and treatment was commenced immediately. Persons not showing positive aldehyde, inspite of long duration fever and splenomegaly, were diagnosed as splenomegaly and not kala-azar and all patients showing negative or doubtful aldehyde test, who had fever and no splenic enlargement, were looked upon as potential kala-azar or malaria cases. Such cases were put on quinine therapy and kept under observation. In this way no cases of kala-azar who once attended their clinic escaped diagnosis eventually. In view of these facts, the results of this test must be interpreted by corroborating them with positive clinical findings. (ii) Complement Fixation test : The compliment fixation test is used to detect specific antibodies present in the serum. The test is essentially an antigen-antibody reaction in which the antibodies present in the serum are bound to an antigen. The antigen used in the test is prepared from either human tubercle bacilli (Witebsky, Kligenstein & Kuhn: WKK antigen) or from Kedrowsky�s acid test bacillus. The test is more sensitive as compared to
aldehyde test as later becomes positive only after three months. However, cross reactions are observed in cases of pulmonary tuberculosis, leprosy and Mycobacterium infections. (iii) Immuno-flourescent antibody test (IFAT) : Fluorescent antibodies appear in the serum during the active phase of the disease and earlier than
3
complement fixing antibodies during the prepatent period and persist for a long time after cure. The parasite antigen labelled with fluorescent dye is conjugated with serum antibodies and seen under fluorescent microscope. (iv) Indirect hemagglutination test (IHA) : This is also based on the principle of antigen-antibody relation. The serum antibodies are conjugated with parasite antigens to observe agglutination. (v) Enzyme Linked Immunosorbant Assay (ELISA) : Soluble antigen or sonicated extract of promastogotes are used to capture antibodies specific to Leishmania. Though sensitive and specific it may give cross reactions with infections like malaria, tuberculosis, leprosy, etc. at very low titers. (vi) Direct Agglutinition Test : The test is based on antigen-antibody reaction. Trypsin treated, strained and formalin preserved promastigotes are used as antigen which show agglutination with specific antibodies present in patients serum. The test is performed at room temperature though the antigens are stored under controlled temperature in freezer. 50 microlitre (ul) antigen suspension is added to 50 ul diluted serum with through mixing for minimum 30 seconds in microlitre plate and incubated for 18 hours at room temperature (optimally 18-22�C). The results are read visually against white background and compared with positive (standard) and negative (blank) controls run parallel. Most serological tests are non-specific, permitting detection of antigens shared by related organisms. They do not distinguish antigens confined to a single species as group reactions mask specific ones. The extreme morphological similarity among related flagellates is paralleled by many antigenic similarities of leishmania spp. (Heyneman, 1971) (b) Detection of Leishmania donovani : Detection of L. donovani is the most specific test for diagnosis of kala-azar. Following methods are used for this purpose. (i) Examination of spleen or borne marrow aspirates : Spleen and bone marrow are the preferred sites of L donovani and thus parasites are available in high densities in these organs. Since these tests are specific and practicable, the techniques for spleen and bone marrow aspiration and straining of the smears are discussed in some detail: (a) Splenic aspiration : Splenic aspiration is one of the most sensitive and widely used procedure and sensitivity may be as high as 95-97%. As a prerequisite for deciding splenic aspiration it is essential to determine prothrombin time and platelet count. If the prothrombin time is more than 5 seconds longer than the control sample and the total platelet count is less than 40000/cu.mm the splenic aspiration is contraindicated. The procedure of splenic aspiration is given in standard text books including the WHO Expert Committee Report No. TRS: 793, 1990. The procedure requires considerable skill and experience and should be performed only by qualified and experienced persons.
4
(b) Bone marrow aspiration : Bone marrow is another tissue of reticulo-endothelial system which is preferred site of L. donovani. The preferred site for bone marrow aspiration include sternum preferably manubrium of the sternum, iliac crest and sometimes tibia. Materials Required
1. Sternal puncture needle 2. Sterile or Disposable syringe 2 ml. with 21 or 23 gauge needle & 5 or 10 ml. syringe 3. Sterile tubes with culture media 4. Glass microslides 5. Xylocaine 2% 6. Savlon or surgical spirit
The sternal puncture needle or bone marrow aspiration needle is a special
type of needle made of very strong steel. The needle is stout and short provided with a well-fitting stylet. The needle is provided with an adjustable guard as a protection against excessive penetration across the bone.
The usual site for bone puncture is manubrium or the first or second
pieces of the body of the sternum. The patient should be on his back. The site of puncture should be cleared or shaved, if hairy. The site should then be thoroughly cleared with savlon and surgical spirit. Local anesthetics like xylocaine 2% should be applied with the help of a 2 ml. syringe. Xylocaine must be dropped at 4-5 places and the skin should be pierced carefully to ensure that it penetrates the skin, subcutaneous tissue and periosteum overlying the site selected for aspiration.
Preparation of Bone Marrow film : The preparation of bone marrow film is a careful procedure. In the successful splenic aspiration, the aspirate is largely free of blood but bone marrow aspirates invariably contains substantial quantities of blood. This excessive blood interferes in the clarity of the slide for examination of LD bodies. Immediately after drawing aspirate in the syringe attached to the sternal puncture needle, a drop is put on clean glass microslides about one cm. from the edge. The excess blood should then be removed from each drop by sucking off with the help of fine Pasteur pipette / filter paper. A thin film of marrow fragments should then be made with the help of the edge of another microslide using it as spreader. The marrow fragments should be dragged behind the spreader edge to make a trail of marrow cells and to avoid causing a distortion of the cells as explained under splenic aspiration procedure. Staining and examination of films of splenic/ bone marrow aspirates : Every glass microslide on which a film has been prepared should be labelled properly. The most common practice is to write the patient�s name and
date on a reference number on the slide itself with a market pencil. A paper label may be affixed later. The marking with pencil is not specified during staining procedure. A prerequisite to successful staining is that the film should be properly fixed with fixatives and should not be left dry for more than a few hours, if not stained immediately. For best results, films should be stained as far as possible, immediately after it is air dried. The most properly used fixative is methanol (methyl alcohol). The air dried slide should be dipped in a staining jar containing methanol for about 20 minutes.

5
Preparation of Stains : Although most of the stains used commonly are available commercially in ready to use formulation or as standards only to be diluted as per instructions, the stains can also be prepared in laboratory. Procedure for preparation of two most commonly used stains i.e. Geimsa and Leishman, both based on Romanowsky dyes, are given below: Giemsa stain : Giemsa stain is available in powdered form. Weigh 1.5 gm of stain powder (Azure B type) and put it in a conical flask. Measure 10 ml of glycerol in a measuring cylider and add to the stain powder in the conical flask. Mix them thoroughly by using beads for about 90 to 120 minutes. Measure 100 ml. of methanol in a measuring cylinder and add to the conical flask containing mixture of Giesma powder and glycerol with constant stirring to ensure thorough mixing. Keep it for 7 days through a good quality filter paper preferably Whatman No. 1 Diluted stain should be prepared the same day when it is used. Leishman stain : Leishman stain is also available in the powdered form. Weigh 0.4 gm of stain powder and put in a conical flask. Measure 100 ml of methanol (acetone free) in a measuring cylinder and add into the flask containing the stain powder. Mix thoroughly and heat at 500C for about 15 minutes. Stir or shake the mixture while heating for through mixing and uniform heating. Filter the solution and keep it at room temperature. The stain can be used immediately after its preparation but if allowed to stand, its quality is improved. Buffer water used for washing of stained slides may be prepared either by using ready to use buffer salts available commercially. Staining of Smears : The air dried and properly fixed slides are transferred to a jar containing giemsa stain diluted with 15-20 vol. of buffered water. The slides then should be dried at room temperature by keeping then upright for excess stain to drain out. If Leishman stain is used, the slide is first flooded with the stain solution by keeping the slide horizontal on a slide rack or on a tray with the help of two glass rods using them as support. After about 30 seconds to 1 minute, double the volume of water should be added and the slide should be left for staining for another 5-7 minutes. The slide should be washed in a stream of buffered water until it acquires a pinkish tinge. The slide should then be left upright for drying at room temperature. The grading of parasitimea is done by the criteria suggested by the WHO (10x eyepiece and 100x oil immersion lens):
Grade Average parasite density 6+ >100 parasites/fields 5+ 10-100 parasites fields 4+ 1-10 parasites fields 3+ 1-10 parasites/ 10 fields 2+ 1-10 parasites/ 100 fields 1+ 1-10 parasites 1000 fields 0 0 parasites 1000 fields (Source : WHO TRS 793)
6
It may be noted carefully that as the parasitimea decreases, it is mandatory To examine slide for longer duration and for larger smear area (No. of fields)
Diagnosis of post Kala-azar Dermal Leishmaniasis : The parasite demonstration in the dermal lesions is the diagnostic criteria for PKDL. The skin biopsy material can be collected with the help of serilized needle from the nodular and erythematous areas. A homogenous smear is prepared on a clean slide and well-stained preparations are examined under the microscope for the presence of amastigotes or leishmania stages (LD bodies). Smears from depigmented macules usually do not show any amastigotes. Sero-diagnosis and culture preparations help in confirmatory diagnosis of macular lesions of PKDL. In India, the diagnostic criteria followed under the Kala-azar control scheme are based on the recommendations of an Expert Committee (Dec 1995) that suggested criteria to be followed at various levels of health delivery system as follows and the same are summaraized. I. Rural/ PHC
Clinical suspects : Persons with fever of more than 3 weeks duration, not responding to a full course of anti-malarials and antibiotics is to be suspected for visceral leishmaniasis. These suspected cases are to be referred to Medical Officer attached to the PHCs/BPHCs. Use of Diagnostic Tests
Napier�s Aldhyde test : Napier�s Aldhyde Test is to be continued in its present form until it can be replaced by other suitable tools. The Medical Officers must be made fully conversant with proper reading and interpretation of the result. Wherever possible attempts are to make available facilities for bone marrow aspirations, skin scraping and collection and dispatch of blood for serological tests in difficult cases. II. Secondary level (Sub-divisional and district level)
1. As far as possible multiple diagnostic tools must be made available. 2. Emphasis must be given more on parasitological diagnosis which can be supplemented by serological tools like DAT, ELISA or any other tests (now rK 39). 3. Appropriate training and motivation of the health workers, including Medical Officers at the secondary level must be undertaken to make the use of the diagnostic tools more meaningful. 4. Considering the bleeding diathesis in Indian Kala-azar, splenic aspiration should be reserved for Divisional/ institutional/ Medical Colleges level. It should be done wherever needed by a person fully acquainted with the technique and only after excluding coagulation abnormalities (bleeding time/prothrombin time) and if present, in such cases only after injection of vitamin K once a day for 3 consecutive days.
7
III. Tertiary level (Medical Colleges and Research Institutions/ State level hospitals) 1. This should act as the highest level of health care delivery vis-à-vis Kala- azar diagnosis and treatment. Therefore, other available diagnostic tools must be made available. 2. As far as possible parasitological diagnosis should serve as the basis for putting a patient on anti-leishmanial therapy. However, other tools like serology may also be considered to supplement the clinically positive but parasitologically negative cases. 3. Facilities for parasite isolation are to be made available particularly in view of assessment of cure following the chemotherapy. Culture should also be done in cases of hypopigmented patch of PKDL which are usually smear negative. 4. Whenever needed in any such case, lymph node biopsy and culture should be encouraged.
rK39 � Rapid Diagnostic Test:
Now a rapid dipstick test based on the recombinant K39 protein is available for rapid diagnosis of kala-azar. K39 is an epitope apparently conserved on amastigotes of Leishmania species that cause visceral infection; by use of laboratory ELISA testing, circulating anti-K39, IgG is detectable in 95%-100% of patients who have kala-azar, irrespective of geographic region. Using K39 antigen-impregnated nitrocellulose strips developed for field conditions, fingerstick-obtained blood and serum samples tested from Indian subjects demonstrated a positive anti-K39 immunochromatographic reaction in 362 patients with aspirate-proven kala-azar; with an estimated sensitivity of 100% and a specificity of 97%. The strip testing proved simple to perform and yielded results within five minutes (1). The rapid diagnostic test when evaluated in comparison to the diagnostic performances of DAT, based both on freeze-dried and liquid antigens, on parasitologically confirmed Kala-azar and Post-Kala-azar Dermal Leishmaniasis (PKDL), the sensitivity of the tests was almost 100%, rK39 was found, to be more sensitive. It was concluded that these tests are comparable to parasitology in terms of their sensitivity and can replace parasitology as the basis for a decision to treat visceral leishmaniasis at peripheral health centers in endemic areas. 2. The antigen: The recombinant antigen is a 39-amino acid (rK39) cloned in Escherichia Coli, from the C terminus of the kinesin protein of Leishmania major in India. The rK39 rapid diagnostic test has undergone extensive evaluation and has been found to be highly sensitive and specific in the diagnosis of both VL and PKDL. 3. Kala-azar Case Definition for enrolling a subject for dipstick testing is as follows,
8
�a case presenting to a clinician with a fever of more than two weeks duration, with splenomegaly and not responding to the full course of anti-malarials, should be subjected to rK39 dipstick test.�
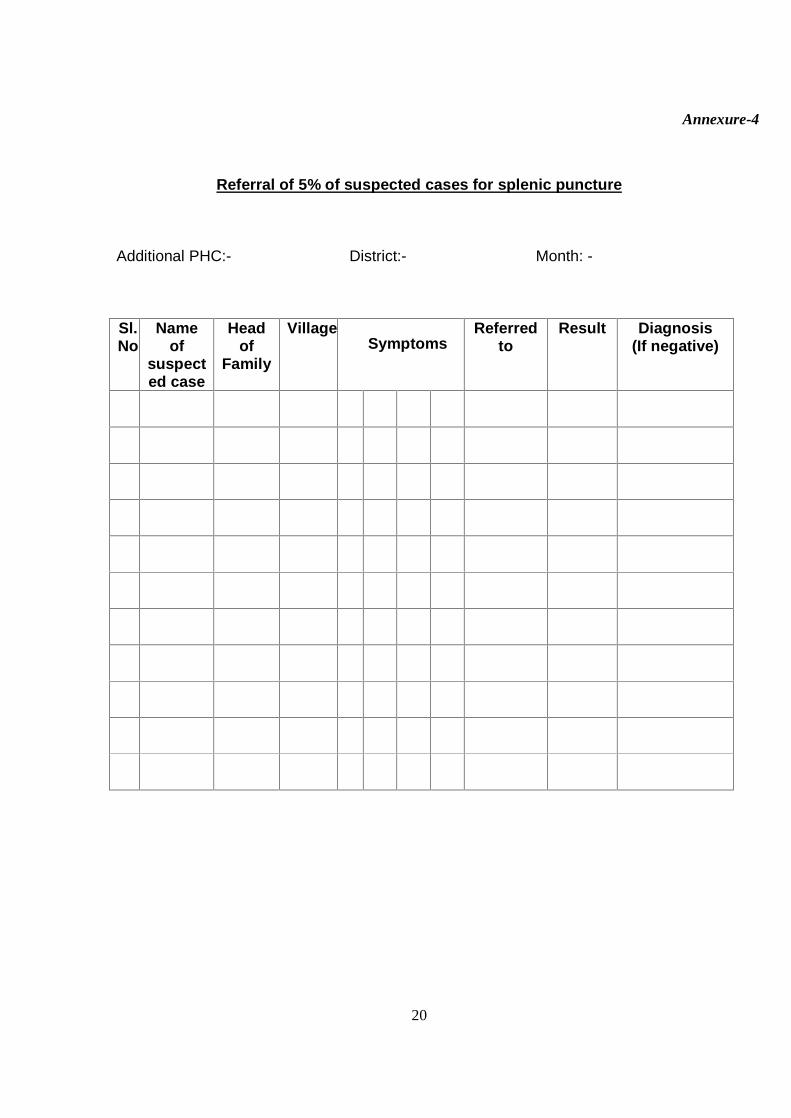
The expert group on the introduction of rapid diagnosis and miltefosine
into the programme had recommended at least five percent of the suspected kala-azar cases, conforming to the case definition of kala-azar and reporting to the PHC for rapid diagnosis should be subjected to splenic aspirate examination. The cases, to be referred for splenic aspiration, will be only those reporting to the Additional PHC�s within very short distances of the higher centers of diagnosis and treatment. The Chief Medical Officer, of the district will designate such centers, and referrals will only be made to such centers, after ensuring that splenic aspiration is to be conducted by experienced and skilled personnel, in properly equipped laboratories.
In case a suspected patient of kala-azar referred for splenic aspiration is found to be negative for parasites, he/she may be referred to a higher center, according to the discretion of the medical officer. The data will be recorded in the accompanying format. 4. Exclusion Criteria: The rK39 is not to be used in the following cases:
Kala-azar relapses In cases of kala-azar re-infection kala-azar and HIV co-infection
5. Kit Contents : Kala-azar dipstick test strip�s is a membrane, pre-coated with a recombinant VL antigen on the test line region and chicken anti-protein A on the control line region. The Kit contains the following:
1. Twenty-five (25) individually pouched Test Strips or twenty-five (25) test strips in a vial with desiccant in the cap.
2. One vial of Chase Buffer solution. 6. Principle: The kala-azar dipstick rapid test is a immunochromatographic assay for qualitative detection of antibodies to L. donovani in human serum. The assay is for aid in the presumptive diagnosis of VL.
During testing the serum sample reacts with the dye conjugate (Protein A-Colloidal Conjugate, which has been pre-coated in the test device). The mixture then migrates upwards on the membrane chromatographically by capillary action to react with rK39 antigen on the membrane and generate a red line. Presence of this red line indicates a positive result while its absence indicates a negative result.
Regardless of the presence of antibody to VL antigen, as the mixture continues to migrate across the membrane to the immobilized chicken anti-protein A region, a red line at the control line will always appear. The presence of this red line serves as a verification for sufficient sample volume and proper flow and is a control for the reagents.
9
7. Test Procedure:
1. 1 or 2 drops of finger prick blood may be assayed for anti K39 IgG.
2. Remove the Kala-azar dipstick strip from the pouch or vial
3. Place one drop of blood on the absorbent pad on the strip bottom.
4. Place the test strip into a test tube so that the end of the strip is facing downward.
5. Allow the mixture to migrate upto the strip by capillary action.
6. Add 2-3 drops of the Buffer solution provided with the test kit to the pad.
7. Read the results in 10 minutes. It is significant that the background is clear before reading the test, especially when samples have low titer of anti-Leishmanial antibody, and only a weak band appears in the test region (T). Results interpreted after 10 minutes can be misleading.
8. Interpretation:
A positive result: The test is positive when a control line and test line appear in the test area. A positive result indicates that the Kala-azar dipstick detected antibodies to L.donovani. A faint line is a positive result. The red color in the test region will vary depending on the concentration of anti-Leishmanial antibodies present. The test line for �weakly positive� sera samples may show results
between a weak positive red line to a faintly red, almost white background. (�Weakly positive� samples are those with low affinity or low titer antibodies
against the recombinant test antigen). A Negative Result: The test is negative when only the control line appears. A negative result indicates that the Kala-azar dipstick did not detect antibodies to L. donovani. An Invalid Result: If no lines appear at either the control or test line areas the test is invalid. The test is also invalid if no control line appears, even though a test line is seen. It is recommended to retest using a fresh dipstick and fresh blood sample should be used in such a case.
9. Storage: The sealed pouch or vial containing the test strip along with the buffer vial is designed to be stored at room temperature (200C - 280C) for the duration of its shelf life. Exposure to temperatures over 300C can impact the performance of the test and should be minimized. The strips should not be frozen. The test should be used within one hour after removal from the pouch or vial to prevent exposure to humidity.
The shelf life of dip-stick is quiet long so the dip-stick can be easily stored
in Primary Health Centre (PHC), in the endemic states. 10. Training: Expert Group recommended that training is a crucial input for success of these new diagnostic and treatment strategies. The trainings on
10
rapid diagnosis will be part of the overall capacity building exercise to be undertaken by NVBDCP with the assistance of IMS, Benaras and RMRIMS, Patna and other identified institutes by states. The training of technicians may be undertaken by the Institute of Medical Sciences, Benaras & RMRIMS, Patna, to be carried out in batches of 30 to 40 technicians and may be completed in about 10 batches. Funds for carrying out these trainings can be provided by the NVBDCP. The separate course for the Medical Officers of the Additional PHC�s of endemic states can be organized by RMRIMS, Patna. 11. IEC: There is always a tendency to resist a novel strategy. The IEC campaigns to promote compliance of diagnostics and treatment need to be emphasized that the dip-sticks are an easy to perform, simple procedure, and they do not entail any cost to the individual. It may also need to be emphasized that dip-stick diagnosis will be followed by free treatment of the kala-azar disease with miltefosine. 12. Supervision: Supervision is a critical input in the effective implementation of any activity. It is a positive contribution from the supervisor and not just fault finding. At the district officers level following should be ensured.
That serological diagnosis of the kala-azar suspected cases with rK39 is carried out after obtaining precise clinical information, and is not applied to random fever cases. The rK39 confirmed cases are to be enrolled for miltefosine treatment, and these strips are not wasted on randomly selected fever cases.
That test are performed and interpreted strictly according to the national
guidelines. To ensure that there is no pilferage of the test dipsticks to private
channels. That the storage of the dipsticks is in the desiccants, kept in cool, safe
places, away from excessive humidity and temperature. That the reports and records match with the actual beneficiaries of
treatment. That the community leaders are informed about the new diagnostic
procedure, and suspected cases are encouraged to avail of the facility.
11
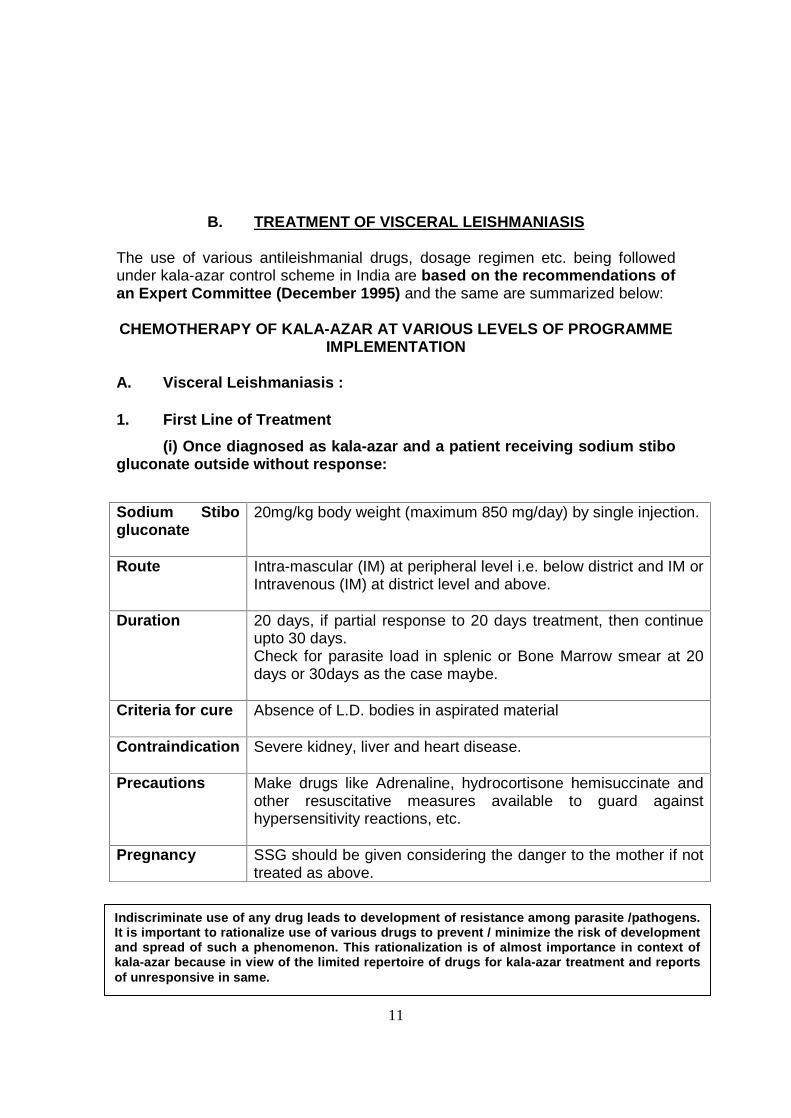
B. TREATMENT OF VISCERAL LEISHMANIASIS The use of various antileishmanial drugs, dosage regimen etc. being followed under kala-azar control scheme in India are based on the recommendations of an Expert Committee (December 1995) and the same are summarized below: CHEMOTHERAPY OF KALA-AZAR AT VARIOUS LEVELS OF PROGRAMME
IMPLEMENTATION
A. Visceral Leishmaniasis :
1. First Line of Treatment
(i) Once diagnosed as kala-azar and a patient receiving sodium stibo gluconate outside without response:
Sodium Stibo gluconate
20mg/kg body weight (maximum 850 mg/day) by single injection.
Route Intra-mascular (IM) at peripheral level i.e. below district and IM or Intravenous (IM) at district level and above.
Duration 20 days, if partial response to 20 days treatment, then continue upto 30 days. Check for parasite load in splenic or Bone Marrow smear at 20 days or 30days as the case maybe.
Criteria for cure Absence of L.D. bodies in aspirated material
Contraindication Severe kidney, liver and heart disease.
Precautions Make drugs like Adrenaline, hydrocortisone hemisuccinate and other resuscitative measures available to guard against hypersensitivity reactions, etc.
Pregnancy SSG should be given considering the danger to the mother if not treated as above.
Indiscriminate use of any drug leads to development of resistance among parasite /pathogens. It is important to rationalize use of various drugs to prevent / minimize the risk of development and spread of such a phenomenon. This rationalization is of almost importance in context of kala-azar because in view of the limited repertoire of drugs for kala-azar treatment and reports of unresponsive in same.
12
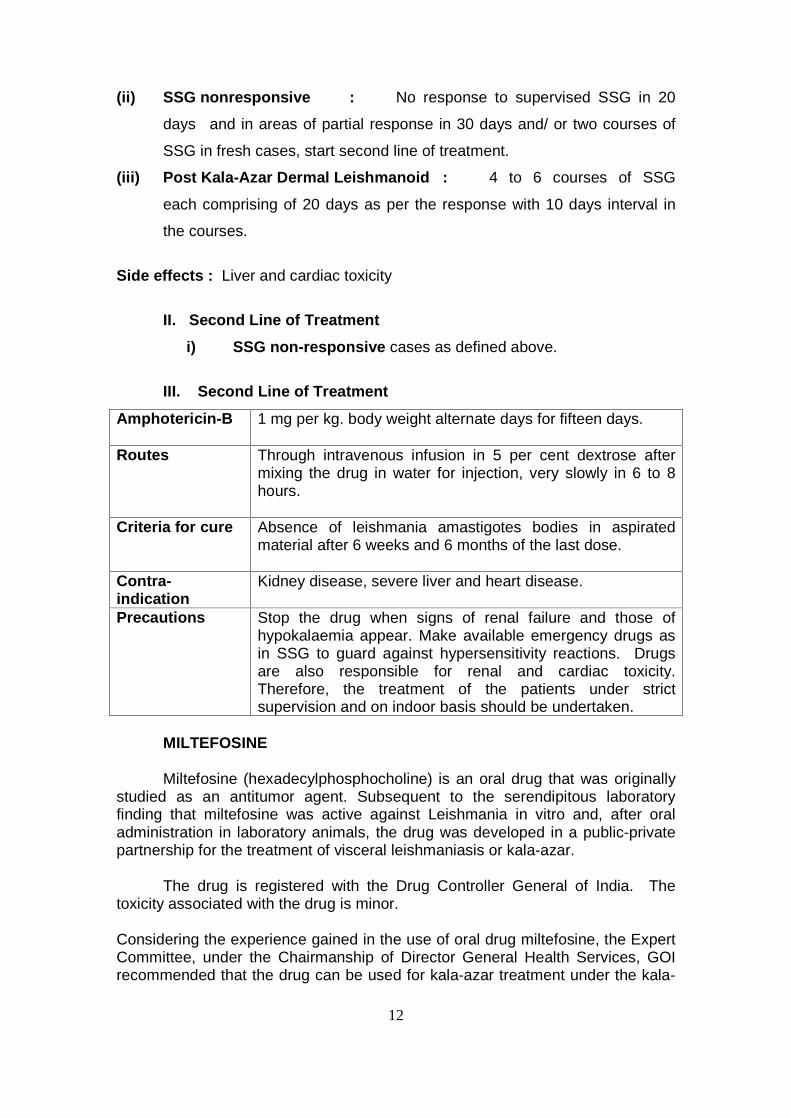
(ii) SSG nonresponsive : No response to supervised SSG in 20
days and in areas of partial response in 30 days and/ or two courses of
SSG in fresh cases, start second line of treatment.
(iii) Post Kala-Azar Dermal Leishmanoid : 4 to 6 courses of SSG
each comprising of 20 days as per the response with 10 days interval in
the courses.
Side effects : Liver and cardiac toxicity
II. Second Line of Treatment
i) SSG non-responsive cases as defined above.
III. Second Line of Treatment
Amphotericin-B 1 mg per kg. body weight alternate days for fifteen days.
Routes Through intravenous infusion in 5 per cent dextrose after mixing the drug in water for injection, very slowly in 6 to 8 hours.
Criteria for cure Absence of leishmania amastigotes bodies in aspirated material after 6 weeks and 6 months of the last dose.
Contra-indication
Kidney disease, severe liver and heart disease.
Precautions Stop the drug when signs of renal failure and those of hypokalaemia appear. Make available emergency drugs as in SSG to guard against hypersensitivity reactions. Drugs are also responsible for renal and cardiac toxicity. Therefore, the treatment of the patients under strict supervision and on indoor basis should be undertaken.
MILTEFOSINE Miltefosine (hexadecylphosphocholine) is an oral drug that was originally
studied as an antitumor agent. Subsequent to the serendipitous laboratory finding that miltefosine was active against Leishmania in vitro and, after oral administration in laboratory animals, the drug was developed in a public-private partnership for the treatment of visceral leishmaniasis or kala-azar.
The drug is registered with the Drug Controller General of India. The
toxicity associated with the drug is minor.
Considering the experience gained in the use of oral drug miltefosine, the Expert Committee, under the Chairmanship of Director General Health Services, GOI recommended that the drug can be used for kala-azar treatment under the kala-
13
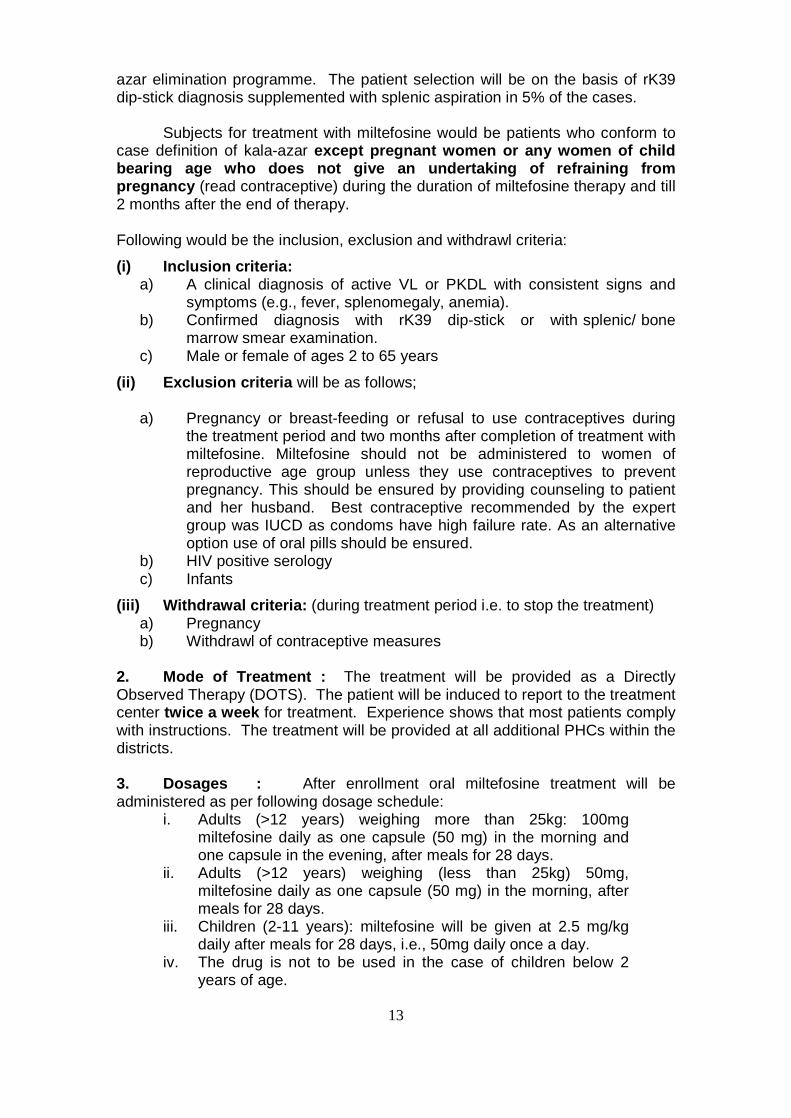
azar elimination programme. The patient selection will be on the basis of rK39 dip-stick diagnosis supplemented with splenic aspiration in 5% of the cases. Subjects for treatment with miltefosine would be patients who conform to case definition of kala-azar except pregnant women or any women of child bearing age who does not give an undertaking of refraining from pregnancy (read contraceptive) during the duration of miltefosine therapy and till 2 months after the end of therapy. Following would be the inclusion, exclusion and withdrawl criteria:
(i) Inclusion criteria: a) A clinical diagnosis of active VL or PKDL with consistent signs and
symptoms (e.g., fever, splenomegaly, anemia). b) Confirmed diagnosis with rK39 dip-stick or with splenic/ bone
marrow smear examination. c) Male or female of ages 2 to 65 years
(ii) Exclusion criteria will be as follows;
a) Pregnancy or breast-feeding or refusal to use contraceptives during the treatment period and two months after completion of treatment with miltefosine. Miltefosine should not be administered to women of reproductive age group unless they use contraceptives to prevent pregnancy. This should be ensured by providing counseling to patient and her husband. Best contraceptive recommended by the expert group was IUCD as condoms have high failure rate. As an alternative option use of oral pills should be ensured.
b) HIV positive serology c) Infants
(iii) Withdrawal criteria: (during treatment period i.e. to stop the treatment) a) Pregnancy b) Withdrawl of contraceptive measures
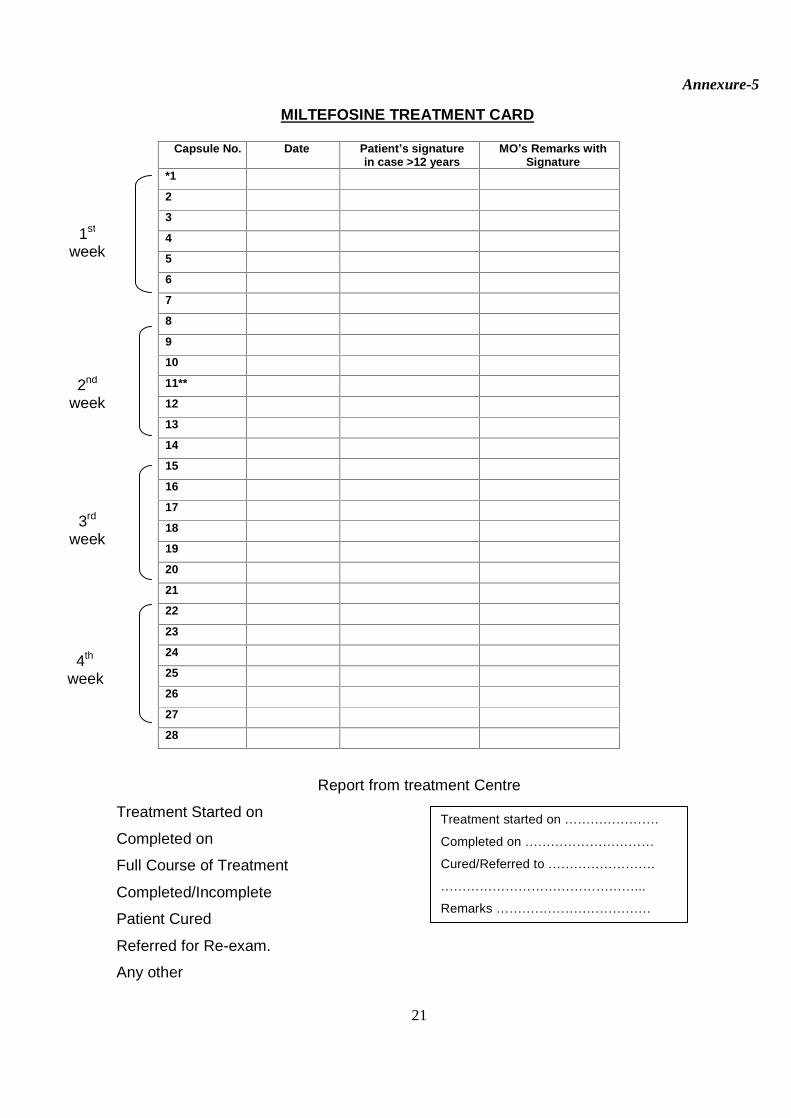
2. Mode of Treatment : The treatment will be provided as a Directly Observed Therapy (DOTS). The patient will be induced to report to the treatment center twice a week for treatment. Experience shows that most patients comply with instructions. The treatment will be provided at all additional PHCs within the districts. 3. Dosages : After enrollment oral miltefosine treatment will be administered as per following dosage schedule:
i. Adults (>12 years) weighing more than 25kg: 100mg miltefosine daily as one capsule (50 mg) in the morning and one capsule in the evening, after meals for 28 days.
ii. Adults (>12 years) weighing (less than 25kg) 50mg, miltefosine daily as one capsule (50 mg) in the morning, after meals for 28 days.
iii. Children (2-11 years): miltefosine will be given at 2.5 mg/kg daily after meals for 28 days, i.e., 50mg daily once a day.
iv. The drug is not to be used in the case of children below 2 years of age.
14
4. Clinical Response : The response will be judged on clinical grounds, i.e., absence of fever, splenomegaly and anemia. 5. Quality Assurance : The specification for procurement of miltefosine conform strictly to the chemical content of the drug, and its shelf life, etc. This is all the more necessary since miltefosine is the sole proprietary drug.
6. Drug Storage : The concerned Medical Officer of the treatment center shall be responsible for ensuring that the drug miltefosine is stored in a cool, secure, limited-access area, protected from extremes of light, temperature and humidity. Patients will be educated about these conditions for storage of the drug supplied to them. 7. Adverse Reaction : Adverse reactions to miltefosine are mostly mild. The treating physician should monitor and watch for any adverse reactions. However, 98% of the patients are not likely to present with any adverse drug reaction. Even of those who report gastrointestinal reactions, 90% will have vomiting only once a month. Should any skin rashes or gastro-intestinal symptoms develop the doctor may consider stoppage of the drug and refer the patient to higher treatment centre. A monitoring of renal and hepatic functions is recommended wherever feasible as about 1% patients may develop nephrotoxicity or hepatotoxicity. 8. Information, Education & Communication (IEC) : In view of the risks of development of the resistance to miltefosine the judicious use of the drug is imperative. The unresponsiveness rate to miltefosine has already risen from 3% to 6%. An injudicious use will certainly render a highly effective and safe drug, ineffective in future. IEC campaign to create awareness about the new tools available under the programme should soberly design the messages, to attract the patient to the treatment centre without creating undue hype which may lead to over-consumption. Measures against pilferage of the drug and its leakage to private sector should be ensured. 9. Role of Family : Kala-azar treatment, even with an easy to administer oral drug, miltefosine, is a protracted affair stretching over twenty eight days, and involving twice daily administration of the (in case of adults more than 12 years ago) drug. The family has a direct stake in the successful completion of the treatment, as it is the family that bears the economic burden and possible economic deprivation resulting from the patients illness. Thus the family must know the course of kala-azar treatment, its durations, precautions, and actions in the case of adverse reactions, if any. It must also know the implications of the complete course of treatment and also the difference between symptomatic cure and complete parasitological cure. This is all the more important, as there is a strong tendency on part of the patient to discontinue treatment the moment there is symptomatic relief and he/she begins to feel better. This tendency to skip treatment is a dangerous tendency both for the individual and the community. IEC messages, which can be communicated to the patient and his attendant in the form of a short brochure, should reinforce the need for a complete course of treatment with the following messages:
15
Kala-azar is a life-threatening disease, which is caused by parasite
introduced into the body of the patient from another person, through the bite of an insect.
It is this kala-azar causing parasite that is responsible for all the suffering of the individual patient and many others in the community.
Unless the body of the patient is freed of these parasites, the patient will not recover complete health.
This is possible only after the patient consumes the effective drug, miltefosine, over a minimum period of 28 days.
Discontinuation of treatment midway is dangerous for the patient, as well as the community, as the parasites of kala-azar if not removed from the body of the patient will again cause the disease in him/her, and what is even worse, some of them be transferred, through the bite of the insect to other healthy individuals.
Having gained this much information, the family members must also be
alert about the development of similar symptoms in the contacts of the patients. Thus the simple case definition of kala-azar, should also be incorporated in the brochure, so that the contacts and other family members are advised diagnosis at the treatment centre.
The simple knowledge can also be utilized in cautioning the neighbour�s to
seek proper diagnosis and treatment in case of onset of kala-azar symptoms. The IEC should also emphasize the use of personal protective measures to protect the individual from re-infection. 10. Monitoring : At district level monitoring of the use of miltefosine would be carried out by Chief Medical Officers & District Programme Officers as per operational details under DOTs treatment schedule. Medical Officer Incharges in respective PHCs will bear overall responsibility for ensuring compliance among the patients. Independent monitoring will be carried out by RMRIMS, Patna on a selected sample basis as per protocol to be developed by them.
11. Evaluation : The extension of the miltefosine therapy will be taken up after evaluation of the results of the pilot use in the two districts. The Dte. NVBDCP can extend the area of miltefosine treatment after observing carefully the results of the pilot use. The present expert group can undertake the evaluation of miltefosine after 1 year of the initiation of use in the selected districts. 12. Post Kala-azar Dermal Leishmaniasis (PKDL) : Since there is a widespread concern that cases of PKDL act as the reservoir of a disease in the community, the Expert Group recommended that the dose and duration of miltefosine treatment in the case of PKDL should be studied and studies completed expeditiously. Till then standard treatment of PKDL should be continued.
16
Reference: 1. S. Sundar, M. Sahu, H. Mehta, A. Gupta, U. Kohli, M. Rai. J.D. Bezman and
H.W. Murray (2002). Noninvasive Management of Indian Viseceral Leishmaniasis: Clinical application of Diagnosis by K39 antigen strip testing at a kala-azar referral unit. Clin. Inf. Dis. 35.1. 581 � 586
2. Bern, C., Jha S N., Joshi A B, Thakur GD, Bista MB (2000) Use of recombinant K39 dipstick test and direct agglutination test in a setting endemic for visceral leishmaniasis in Nepal. Am. J. Trop. Med. Hyg. 63: 153 � 7.
3. Berman JD (1997) Human Leishmaniasis : Clinical, diagnostic, and chemotherapeutic developments in the past ten years. Clin. Inf. Dis. 24 : 684 � 703.
4. Shyam Sundar, T.K. Jha, C.P. Thakur, Juergen Engel, Herbert Sinderman, Christina Fischer, Klans Jurge, Anthony Bryceson, and Jonathan Berman. (2002). Oral miltefosine for Indian Visceral Leishmaniasis N.Eng. Jour. Med. 347.22. 1739 � 45.
5. WHO. (1990). Control of Leishmaniasis. Report of a WHO Expert Committee. WHO Technical Report Series No. 793. WHO, Geneva. 1 � 158.
6. Sarman Singh, Veena Kumari, and niti Singh. (2002). Predicting Kala-azar Disease manifestation in Asymptomatics with latent leishmania donovani infection by defection of antibody against recombinant K39 antigen. Clin. Diagn. Lab. Immunol. 9(3). 568-572.
17
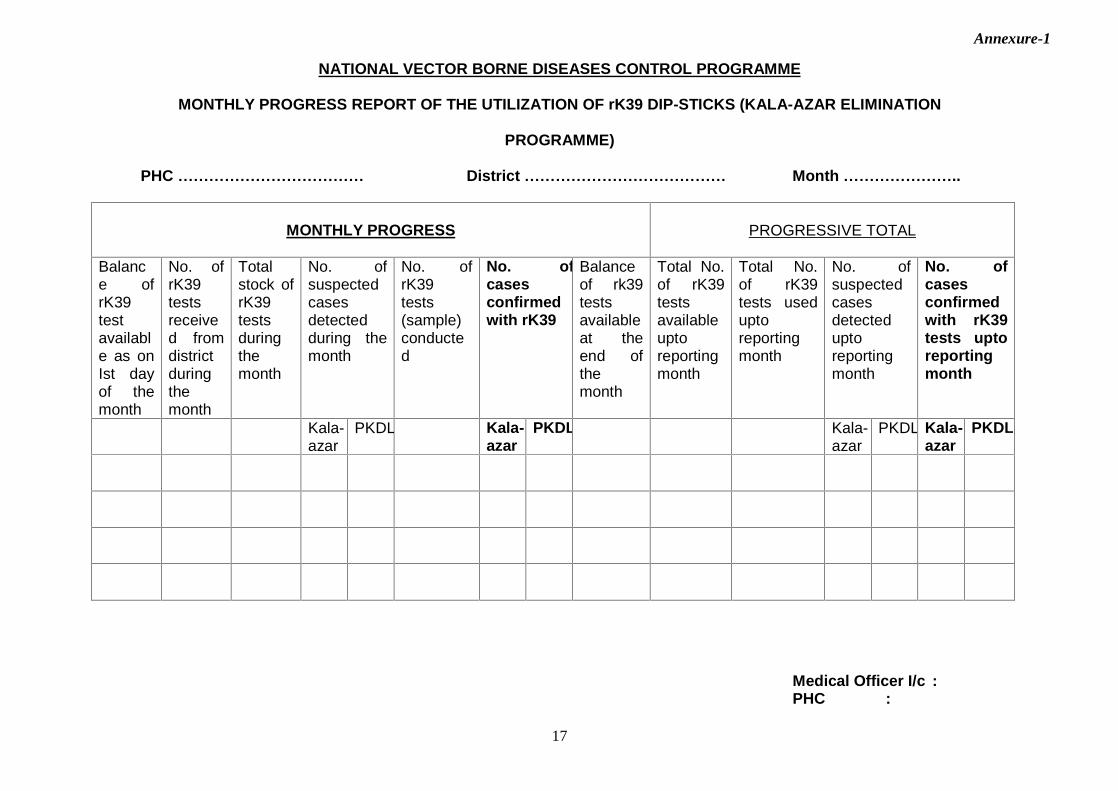
NATIONAL VECTOR BORNE DISEASES CONTROL PROGRAMME
MONTHLY PROGRESS REPORT OF THE UTILIZATION OF rK39 DIP-STICKS (KALA-AZAR ELIMINATION
PROGRAMME)
PHC ������������ District ������������� Month �������..
MONTHLY PROGRESS
PROGRESSIVE TOTAL
Balance of rK39 test available as on Ist day of the month
No. of rK39 tests received from district during the month
Total stock of rK39 tests during the month
No. of suspected cases detected during the month
No. of rK39 tests (sample) conducted
No. of cases confirmed with rK39
Balance of rk39 tests available at the end of the month
Total No. of rK39 tests available upto reporting month
Total No. of rK39 tests used upto reporting month
No. of suspected cases detected upto reporting month
No. of cases confirmed with rK39 tests upto reporting month
Kala-azar
PKDL Kala-azar
PKDL Kala-azar
PKDL Kala-azar
PKDL
Medical Officer I/c :
PHC :
Annexure-1
18
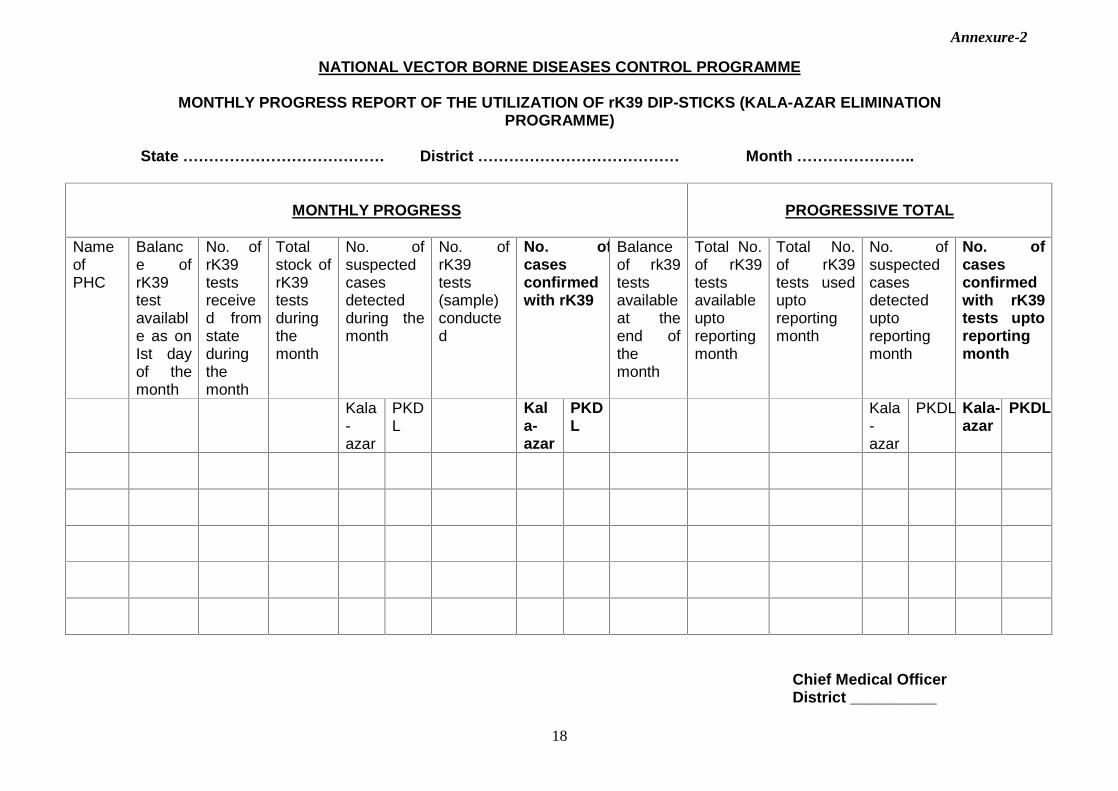
NATIONAL VECTOR BORNE DISEASES CONTROL PROGRAMME
MONTHLY PROGRESS REPORT OF THE UTILIZATION OF rK39 DIP-STICKS (KALA-AZAR ELIMINATION PROGRAMME)
State ������������� District ������������� Month �������..
MONTHLY PROGRESS
PROGRESSIVE TOTAL
Name of PHC
Balance of rK39 test available as on Ist day of the month
No. of rK39 tests received from state during the month
Total stock of rK39 tests during the month
No. of suspected cases detected during the month
No. of rK39 tests (sample) conducted
No. of cases confirmed with rK39
Balance of rk39 tests available at the end of the month
Total No. of rK39 tests available upto reporting month
Total No. of rK39 tests used upto reporting month
No. of suspected cases detected upto reporting month
No. of cases confirmed with rK39 tests upto reporting month
Kala-azar
PKDL
Kala-azar
PKDL
Kala-azar
PKDL Kala-azar
PKDL
Chief Medical Officer District __________
Annexure-2
19
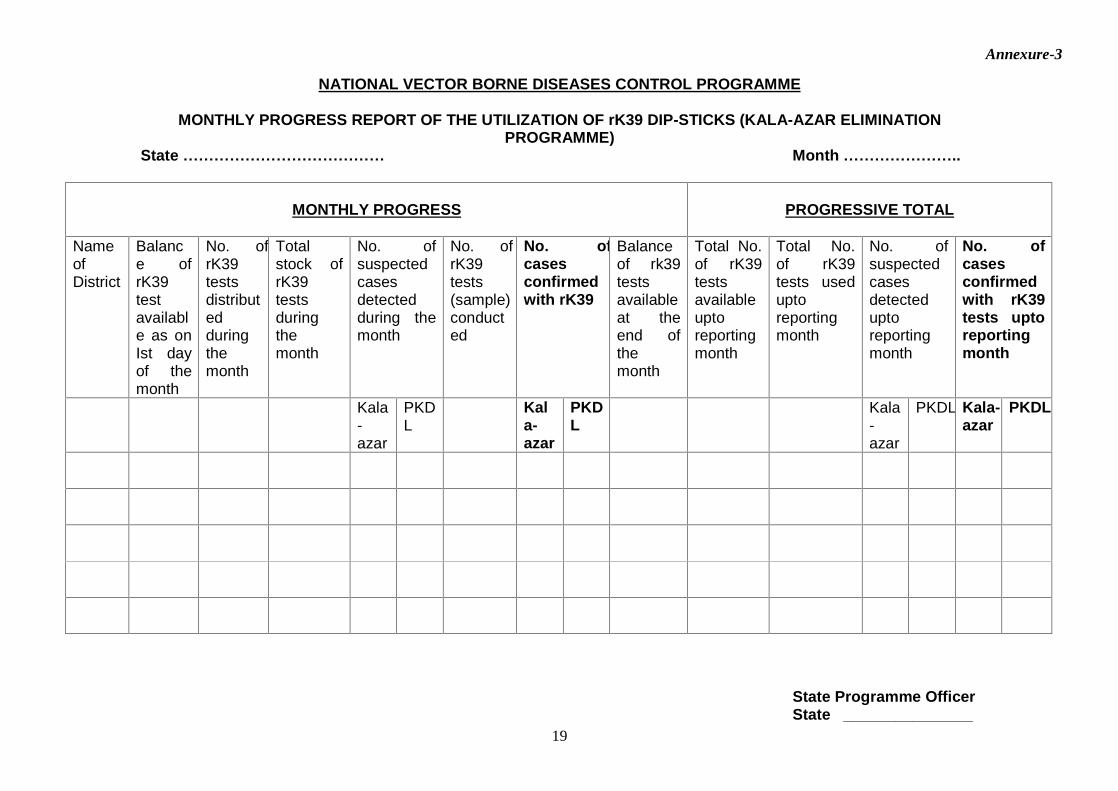
NATIONAL VECTOR BORNE DISEASES CONTROL PROGRAMME
MONTHLY PROGRESS REPORT OF THE UTILIZATION OF rK39 DIP-STICKS (KALA-AZAR ELIMINATION PROGRAMME)
State ������������� Month �������..
MONTHLY PROGRESS
PROGRESSIVE TOTAL
Name of District
Balance of rK39 test available as on Ist day of the month
No. of rK39 tests distributed during the month
Total stock of rK39 tests during the month
No. of suspected cases detected during the month
No. of rK39 tests (sample) conducted
No. of cases confirmed with rK39
Balance of rk39 tests available at the end of the month
Total No. of rK39 tests available upto reporting month
Total No. of rK39 tests used upto reporting month
No. of suspected cases detected upto reporting month
No. of cases confirmed with rK39 tests upto reporting month
Kala-azar
PKDL
Kala-azar
PKDL
Kala-azar
PKDL Kala-azar
PKDL
State Programme Officer State _______________
Annexure-3
20
Referral of 5% of suspected cases for splenic puncture
Additional PHC:- District:- Month: -
Sl. No
Name of
suspected case
Head of
Family
Village Symptoms
Referred to
Result Diagnosis (If negative)
Annexure-4
21
MILTEFOSINE TREATMENT CARD
Capsule No. Date Patient�s signature in case >12 years
MO�s Remarks with Signature
*1
2
3
4
5
6
7
8
9
10
11**
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
Report from treatment Centre
Treatment Started on
Completed on
Full Course of Treatment
Completed/Incomplete
Patient Cured
Referred for Re-exam.
Any other
Treatment started on �������.
Completed on ����������
Cured/Referred to ��������.
���������������...
Remarks ������������
1st week
2nd week
3rd week
4th week
Annexure-5





























