Embed Size (px)
Citation preview
Introduction
Humanimmunodeficiencyvirus(HIV)associatedtuberculosis(TB)remainsamajorglobalpublichealthchallenge. By the end of 2009, an estimated 33.3millionpeoplewerelivingwithHIV,thevastmajorityin sub-Saharan Africa and Asia. An estimated 2.6million individuals had become newly infected withHIV and 1.8 million had died ofAIDS in that yearalone1.TBisthemostcommonopportunisticinfection(OI)amongHIV-infectedindividuals,andco-infectedindividuals areathigh riskofdeath2,3.TheestimatesoftheglobalburdenofdiseasecausedbyTBin2009
Review Article
Diagnosis&treatmentoftuberculosisinHIVco-infectedpatients
C.Padmapriyadarsini,G.Narendran&SoumyaSwaminathan
National Institute for Research in Tuberculosis (Indian Council of Medical Research), Chennai, India
ReceivedOctober31,2011
Human immunodeficiency virus (HIV) associated tuberculosis (TB) remains a major global public health challenge, with an estimated 1.4 million patients worldwide. Co-infection with HIV leads to challenges in both the diagnosis and treatment of tuberculosis. Further, there has been an increase in rates of drug resistant tuberculosis, including multi-drug (MDR-TB) and extensively drug resistant TB (XDRTB), which are difficult to treat and contribute to increased mortality. Because of the poor performance of sputum smear microscopy in HIV-infected patients, newer diagnostic tests are urgently required that are not only sensitive and specific but easy to use in remote and resource-constrained settings. The treatment of co-infected patients requires antituberculosis and antiretroviral drugs to be administered concomitantly; challenges include pill burden and patient compliance, drug interactions, overlapping toxic effects, and immune reconstitution inflammatory syndrome. Also important questions about the duration and schedule of anti-TB drug regimens and timing of antiretroviral therapy remain unanswered. From a programmatic point of view, screening of all HIV-infected persons for TB and vice-versa requires good co-ordination and communication between the TB and AIDS control programmes. Linkage of co-infected patients to antiretroviral treatment centres is critical if early mortality is to be prevented. We present here an overview of existing diagnostic strategies, new tests in the pipeline and recommendations for treatment of patients with HIV-TB dual infection.
Key words Co-infection-diagnosis-drugresistance-HIV-IRIS-treatment-tuberculosis
wereasfollows:9.4millionincidentcases(range8.9-9.9million), 1.3million deaths amongHIV-negativeTB patients (range 1.2-1.5million) and 0.38milliondeaths amongHIV-positiveTB patients (range 0.32-0.45million).MostTBcaseswere in theSouth-EastAsia, African and Western Pacific regions (35, 30and20%, respectively).An estimated11-13per centof incident caseswereHIV-positive4.TBmay occuratanystageofHIVdiseaseandisfrequentlythefirstrecognizedpresentationofunderlyingHIVinfection5,6.AscomparedtopeoplewithoutHIV,peoplelivingwithHIV(PLWH)havea20-foldhigherriskofdeveloping
850
IndianJMedRes134,December2011,pp850-865

TB7 and the risk continues to increase as CD4 cellcountsprogressivelydecline5.
AsaresultofWHO’s3by5campaign,>6millionHIV-infected individuals in resource limited settingshavehadaccesstoantiretroviraltherapy(ART)since20048,thoughthisisstillfarshortoftheactualneed.AlthoughART can reduce the incidence ofTB bothat the individual and population level, PLWH onARTstillhavehigherTBincidenceratesandahigherriskofdying fromTB9.Thismaybedue todelayedinitiation of ART or the fact that patients presentwith advanced TB or both10. Routine TB screeningamongPLWHofferstheopportunitytoidentifythosewithoutTB,preventTBbychemoprophylaxisaswellas to diagnose and promptly treatTB.However, co-administration of ART along with anti-TB therapypresents several management challenges, includingdrug-druginteractions,overlappingdrugtoxicitiesandimmunereconstitutionsyndrome.
Inthisreview,wesummarizeandupdateinformationonthescreening,diagnosisandmanagementofTBinHIVinfectedadults.
Diagnosis of TB in HIV-infected individuals
Clinical screening algorithms:TheWHOrecommendsTBscreeningatthetimethatHIVinfectionisdiagnosed,before the initiation of antiretroviral therapy and atregular intervals during follow up11. Currently thereis no internationally accepted evidence-based tool toscreen forTB inPLWH.Multiple studies have beenconducted todevelopasimplemethodfor rulingoutTBinpeoplewithHIVinfection,butmethodologicalissuesprecludetheuseofanyoftheseasthebasisforglobalhealthpolicy12-14.In2007,aWHOInternationalExpertCommittee issued newguidelines to improvethediagnosisofTBinHIVinfectedindividuals15.Thefeasibility, accuracy and operational performance ofthese guidelines were tested in various settings andwere found to be acceptable16. It was recommendedthatscreeningforTBshouldincludeaskingquestionsabout a combination of symptoms rather than onlyaboutchroniccough.Arecentmeta-analysisevaluatedthe performance of individual and combinations ofsymptoms as screening rules for TB among 8,148participants from 12 studies17. The best performingrule was the presence of any one of current cough,fever, night sweats or weight loss. The overallsensitivityof this rulewas79percent, increasing to90percentinclinicalsettingsbutthespecificitywasonly50percent.Thenegativepredictivevalueofthe
rulewashighacrossarangeofTBdiseaseprevalenceestimatesaswellasacrosshighandlowCD4counts.Themajor change to existing practice would be thereplacementofchroniccoughwithcurrentcoughasascreeningquestionandtheadditionofothersymptomstostandardscreening17.Whileascreening toolneedstohavehighsensitivityandnegativepredictivevalue,a diagnostic strategy should ideally have both highsensitivity and specificity. The screening tool couldbeusedinARTclinicstoidentifypatientseligibleforchemoprophylaxis as well as to identify those whoneedfurtherinvestigationsforTB.
Radiographic features:Thespectrumof radiographicmanifestation of pulmonary TB is dependent on therelative level of HIV-related immunodeficiency18.During the early phase ofHIVwhen individuals arenot immunosuppressed, the radiographic pattern issimilar to HIV uninfected individuals with moretypicallesions-upperlobeinfiltrateswithorwithoutcavities. With advancing immunosuppression, extrapulmonary involvement, intra-thoracic/mediastinallymphadenopathy,lowerlobeinfiltrateandmiliaryTBbecomemorecommon19.
Adding chest X-ray to symptom screeningincreasesthenumberofTBcasesdetectedbutisnon-specificandaddstothecostofscreening.ChestX-raycan still miss a substantial proportion of individualswithsub-clinicaldisease,oftenseeninadvancedHIVimmunosuppression20. Moreover, chest radiographsmay appear normal in 7-14% of patients with HIV/TB18,19.Thissub-populationofco-infectedindividualsisparticularlylikelytobenefitfromsputumcultureornucleicacidamplificationtestsforTBdiagnosis.
Sputum smear microscopy:ThemostfrequentmethodofTBdetectioninvolvesmicroscopicexaminationofsputumforacid-fastbacilli(AFB)21.Microscopyhastheadvantageofbeing inexpensive, relatively rapidto perform, and specific inmost settings.However,to be considered smear positive a specimen needsto contain approximately 105 mycobacteria permilliliter. The sensitivity of sputum microscopy inHIV infection ranges from 43 to 51 per cent22, andinmanyresource-limitedsettingswithhigh ratesofco-infection, the sensitivity may be much lower23.Methods that improve speed or sensitivity includefluorescence microscopy24 and alternative specimenprocessing methods, such as concentration, bleachsedimentation and same-day sputum collection (so-calledfrontloading)strategies25-27.Anyprocedurefor
PADMAPRIYADARSINIet al:HIV-TBCOINFECTION 851

digestionorliquefactionfollowedbycentrifugation,prolongedgravitysedimentation,orfiltrationincreasessensitivityby13to33percentoverdirectmicroscopy,whencultureisusedasthereferencestandard26.
Equipmentcostslimitthewideruseoffluorescencemicroscopes in resource-limited settings.Alternativetechnologies using light-emitting diode bulbs allowfluorescence microscopes at a much lower cost;field-level evaluation showed promising results andthis technology is now being widely scaled up28,29.Nevertheless, because sputum smear is the primarymode ofTB detection inmany resource constrainedsettings, a sizable number of smear-negativeindividuals often remain undiagnosed or receivedelayedanti-TBtherapy30.Itisalsoimportanttonotethatdrugsusceptibilitycannotbeascertainedbysmearmicroscopy, so treatment for drug resistant TB isinvariablyempirical.
Growth based detection: Culture of Mycobacterium tuberculosis is much more sensitive than smearmicroscopy and has been recommended to assist inthe diagnosis of TB in HIV-infected individuals31.Culturealsoallowssubsequentstraincharacterizationanddrugsusceptibilitytests.ThetraditionalmethodofinoculatingsolidmediumsuchastheLowenstein-Jenson(L-J) medium or Middlebrook medium is sensitivebutslow,asgrowthmaynotbevisibleuntilafter6-8wkofincubation.Thisresultsindelayininitiationoftherapy,withdetrimentaleffectsonoutcomeofHIV-TB co-infected patients. Automated liquid culturesystems detect growth of mycobacteria within 1-2wkbybacterialcarbondioxideproductionoroxygenconsumptionwithradiometricsensors(BACTEC460TB;BectonDickinsonDiagnosticInstrumentsSystems,USA), fluorescent sensors [BACTEC MycobacteriaGrowthIndicatorTube(MGIT)960;BectonDickinsonDiagnosticInstrumentsSystems],colorimetricsensors(MB/BacTsystem;OrganonTeknika),pressuresensors(ESPculturesystemII;DifcoLaboratories,USA),orredoxreagents,suchasAlamarblue32-35.
Microscopic observation drug susceptibility(MODS)assayisalowcostnon-commercialmethodthatcanbeusedfordetectionofmicrocolonies,cordformation and for early detection of drug resistance.It appears to have higher sensitivity, shorter time toculturepositivityandismorecosteffectivethanregularL-Jmedium36.
BacteriophagebasedassayshavebeenusedforTBdiagnostics (FASTPlaqueTB; Biotech Laboratories,
UK). The FAST Plaque TB assay can detectmycobacteria in 50-65 per cent of smear negativespecimens with a specificity of 98 per cent. Theseassayshaverelativelyhighaccuracywhenperformedon culture isolates. However, their sensitivity inHIV-TB co-infection is low with a higher risk ofcontamination37.
There are currently multiple rapid diagnostictechnologies under evaluation, such as recombinantmycobacteriophages (Luciferase reporter phage-based test “Bronx-box”)38, and colorimetric culturesystem using TK medium culture system (Salubris,Inc,MA,USA)39.Theintroductionoftheserapidandautomated systems has increased the sensitivity ofisolation of mycobacteria from clinical samples andhasbroughtdownthetimerequiredforpositiveculturesubstantially(9-10days).FastercultureresultsinHIV-infectedpatientscanresultinfasterimplementationofevidence-basedtherapy.
Molecular techniques: Nucleic acid amplificationtesting(NAAT)providesareliablewayofincreasingthe specificity of diagnosis (ruling in disease), butsensitivity is variable, especially in paucibacillarydisease. Commercial kits have the advantage ofbeing well standardized and reproducible. However,concerns about their accuracy, reliability, their highcost, requirement forproper laboratory infrastructureand strict quality control procedures limit theirapplicability in resource-limited settings. A fewmodifiedorsimplifiedversionsofNAATkitsincludeloop-mediated isothermal amplification (LAMP),fluorescence in-situ hybridization (FISH) and lineprobeassays(LPA)40.Arecentmeta-analysisshowedhigh sensitivity (>95%) and specificity (100%) forLPAwhencultureisolateswereused41.TheWHOhasendorsedtheuseoflineprobeassays,whichcandetectboth M. tuberculosis complex as well as isoniazidand rifampicin resistance on smear-positive sputumor on early positive growth on culture42. Line probeassays are being used in conjunctionwith culture intheIntermediateReferenceLaboratoriessetupbytheRevisedNationalTBControlProgramme(RNTCP)inIndia43.
GeneXpert-Rif:Recently, theWHOendorsed theuseof GeneXpert-Rif for the rapid diagnosis of TB aswell as rifampicin resistance among HIV-infectedindividualswithclinicalsuspicionofTB44.GeneXpertis a TB-specific automated, cartridge-based nucleicacid amplification assay, having fully integrated and
852 INDIANJMEDRES,DECEMBER2011

automated sample preparation, amplification anddetectionusingreal-timePCR,providingresultswithin100 minutes. Clinical validation trials done in fourdistinctlydiversesettingsshowedthat92.2percentofculture-positivepatientsweredetectedbyasingledirectXpertMTB/RIFtest(incomparisontothesensitivityof a singledirect smearof 59.5%)45.Sensitivityof asingleXpertMTB/RIFtestinsmear-negative/culture-positivepatientswas72.5percentwhichincreasedto90.2per centwhen three sampleswere tested.XpertMTB/RIFspecificitywas99percent.HIVco-infectionsubstantiallydecreasedthesensitivityofmicroscopy(to47%),butdidnotsignificantlyaffectXpertMTB/RIFperformance46. Xpert MTB/RIF detected rifampicinresistance with 99.1% sensitivity and excludedresistancewith100percentspecificity47,48.Meantimetodetection was<1dayforXpertMTB/RIF,1dayformicroscopy, 17days for liquid culture and>30daysfor solidculture45,46.Thus this test seems tohave thepotentialtocomplementthecurrentreferencestandardofTBdiagnostics and increase its overall sensitivityandspeed.Furtherimplementationresearchisrequiredtodeterminetheoptimallevelofthehealthcaresystemwherethissystemcanbecost-effectivelyutilized.
Serological diagnosis of TB
(i) Detection of antibodies: Performance of variousimmunebasedteststodetectantibodiestoM. tuberculosis antigens has been reviewed extensively40,49-51. Noneof the existing commercial serological tests showadequatesensitivityandspecificitytoberecommendedfor diagnostic use. Interestingly, the WHO recentlymade a negative recommendation against the use ofserologicaltestsforTB,basedondatasuggestingthatthese tests could neither replace sputummicroscopynor be used as an add-on test to rule outTB52.Thishasbeenendorsedby theRNTCPand isparticularlyrelevantinIndia,whereitisestimatedthatmillionsofthesetestsareperformedintheprivatesectorleadingtoahugewasteofresources53.
(ii) Detection of antigen:AttemptshavebeenmadetodetectM. tuberculosis MPB-64(TAUNS)antigensinperipheral blood, early secreted antigenic target 6 inthecerebrospinalfluid, lipoarabinomannan(LAM)intheurine,etc. byELISA–basedcommercial assays54-56.UrineLAMassays tend toperformbetter inHIV-infectedcomparedtoHIVuninfectedTBpatients.Thecombination of urine lipoarabinomannan testing andsputumsmearmicroscopyneedsfurtherevaluationforuseinsettingswithahighHIVburden57.
Tuberculin skin test: Tuberculin skin test if positiveprovidesevidenceofTBinfection.ManyHIVinfectedpatients will have a negative skin test despite TBinfectionordisease,duetoanergy.“Twostageorboostertest” is not a substitute to anergy testing; however,itmay have some utility in detectingM.tuberculosis infection in anergic HIV-TB co-infected patients51.Tuberculinskintestunderestimatestheprevalenceoflatent tuberculosis in endemic countries; it requirestrainedhealthcarestafftocorrectlyperformthetestsand accurately read the results, and also requires asecondpatientvisit58.ThetestisneitherusefultoruleindiseasenorinhighTBprevalencesettingstoidentifyeligibleindividualsforprophylaxis.
Other diagnostic techniques
(i). Interferon-γ release assay (IGRA):ThistestcanbeusedtodiagnoselatentTBinfectionandisparticularlyusefulinprofoundlyillpatientsandthosewithseveremalnutrition.Therearetwoin vitroteststodetectlatenttuberculosis:QuantiFERON-TBGold(Cellestis,USA)and theTSPOT-TB test (Oxford Immunotec,USA).Both use an enzyme- linked immunospot assay toquantifythenumberofperipheralbloodmononuclearcells producing IFN- γ in response to tuberculosis-specific antigen stimulation (ESAT-6 and CFP10).Both assays give objective results, with sensitivity(as measured in patients with active tuberculosis)comparabletothatofthetuberculinskintest,butaresignificantly more expensive59. IFN-γ assays do notdifferentiate between latent and active tuberculosisor between immune reconstitution inflammatorysyndrome (IRIS) and failure. Studies suggest thatIGRAsareidealforserialtestingbecausethesecanberepeatedwithoutboosting60-62.ThesearealsounaffectedbypreviousBCGvaccinationandrequirefewerpatientvisits.However,WHOrecommendedagainsttheuseofIGRAsfordiagnosisofactiveorlatentTB,inresource-limitedsettings63.
(ii) Sensing volatile organic compounds (VOCs):from tuberculosis bacteria in exhaled air or urineor headspace gas over sputum or bacterial culture,measuredusingsensorsorgaschromatography–massspectroscopy is a promising new technique64,65. Astudy from India compared theVOCs present in theurineofTBpatientswithVOCsintheurineofhealthysubjects, and found that infectionwithTB producesadistinct patternof certainVOCs inmuch the sameway that distinct fingerprint patterns can identifyindividuals65. Identification of these patterns sets the
PADMAPRIYADARSINIet al:HIV-TBCOINFECTION 853

stagefordevelopingaportable“electronicnose”thatcanquicklysniffurinesamplestodetectTB.
(iii) Electronic nose devices: Electronic nose (EN)devices are an array of chemical sensors combinedwith some sort of pattern recognition system,whicharebeinginvestigatedtodifferentiatebetweensputumsamplesfromTBpatientsandnon-TBpatients66.ThefunctionofanENistomimicthemammalianolfactorysystem and produce a unique classification based onthevolatileorganiccompoundsinsputum.
Screening for HIV among individuals with active TB
With regard to detectingHIV among individualswith active TB, provider initiated HIV testing isrecommendedforallTBpatients,asstandardofcare67.TherapidexpansionofHIVtestingforTBpatientshasbeenparticularlyencouraginginAfrica,whereonly4percentofTBpatientswere testedforHIVin2004,butby2008thatnumberhadincreasedto45percent4.InapilotstudyofimplementationofproviderinitiatedHIVtestingandcounsellinginIndia,HIVstatuswassuccessfullyascertainedfor70percentofTBpatientsandthiswasfoundtobefeasibleandacceptable68.Thepolicy has been rapidly scaled up with over 60 percentofTBpatientsbeingawareoftheirHIVstatusin2011.
Preventing TB among HIV-infected Individuals
The WHO currently recommends that all HIV-infectedpersonsbescreenedforTB,andHIV-infectedpersons without active TB disease be evaluated fortreatmentoflatentTBinfection69.Twometa-analyseshave shown that isoniazid (INH) taken daily for sixmonths (6H) reduces the incidence of TB by overtwo-thirds among HIV-infected individuals70,71. ThemostwidelyrecommendedregimenforTBpreventivetherapyisisoniazid300mgdailyfor6months.WHOguidelines (2010) strongly recommend the use of6Hregimen,with36H(3yearsof isoniazid)beingaconditional recommendation for countries to adoptdepending on local needs and resources72. However,very few high-burden TB countries have routinelyimplemented isoniazid preventive therapy (IPT) forPLWH, because of concerns about how to excludeTBdisease,fearsaboutselectionforINH-resistantM. tuberculosis (MTB)strains,andtheabsenceofpublichealth models for how to deliver this treatment73.Symptom screening can detect culture-confirmedTBdiseasewithgreaterthan90percentsensitivityand97
percentnegativepredictivevalue.NoneofthestudiesofIPThavedocumentedhigherratesofdrug-resistancesolelyattributabletoIPT.StudiesfromIndiaandSouthAfrica found the 6-month isoniazid regimen to beeffective,well toleratedwith low ratesof emergenceofdrugresistance74,75.TheSouthAfricancohortstudy,whichusedthreenewprophylacticregimens,didnotfind any superiority over the control regimen of 6monthsofisoniazid75.Incontrast,arandomizeddouble-blind,placebo-controlledtrialinBotswanafoundthat36months isoniazid prophylaxis wasmore effectivefor preventionofTB thanwas 6-month prophylaxis,chiefly benefitting those who were tuberculin skintestpositiveandthose initiatingART76.TheNationalAIDS Control Organization (NACO) intends to testthe effectiveness and feasibility of the WHO IPTguidelinesinARTclinicsasaprecursorforadoptingthisrecommendation77.
Treatment of TB and HIV in co-infected individuals
The basic principles of treatment for HIV-associated TB are the same as for HIV uninfectedindividuals. Certain areas of uncertainty remain,includingtheregimenduration,dosageandfrequencyofadministrationofanti-TBdrugs,optimaltimingofinitiationofARTandoptimalanti-TBdrugcombinationforpatientsonsecondlinetreatment.
(i) Anti-TB therapy: Currently, standard therapyconsists of four drugs in the intensive phase for2 months namely isoniazid (H), rifampicin (R),pyrazinamide (Z) and ethambutol (E) followedbyHand R in the continuation phase of four months. InIndia,underRNTCP,afullyintermittentthrice-weeklyregimenCategoryI(2EHRZ3/4HR3)isrecommendedfor newly diagnosedTB.This regimen is reinforcedwithstreptomycin(Sm)intheintensivephaseandthetotaldurationincreasedtoeightmonthsforretreatmentcases - Category II (2EHRZS3/1EHRZ3/5EHR3)78.Rifampicinplaysakeyrole in the treatmentofHIV-associated TB because of its ability to destroy bothintracellular and intermittently and slowly growingTB bacilli. Non-rifampicin containing regimens areassociated with inferior cure rates and prolong theperiodoftreatment79.Ameta-analysisonthedurationofrifampicinshowedthatrecurrenceswere2-3timeshigherifrifampicinusewasrestrictedto2months80.
Foralongtime,itwasbelievedthatlongerregimenscould potentially improve TB outcomes in HIVinfectedindividuals.Todeterminetheoptimalduration
854 INDIANJMEDRES,DECEMBER2011

of treatment, we conducted a randomized controlledclinical trial in the pre-HAART era, comparing thestandardRNTCP 6months regimen (2EHRZ3/4HR3)witha9monthextendedcontinuationphaseregimen(2EHRZ3/7HR3).Itwasfoundthatextensionto9monthsdidnot improve theoutcomeat theendof treatmentbut bacteriological recurrences were significantlyreduced during follow up. Irrespective of the lengthof the regimen, acquired rifampicin resistance washighamongfailuresintheabsenceofART81.Variousstudieshave shown that there is an increased riskoffailure with high probability of acquired rifampicinresistance, especially in ART naïve individualsreceivingintermittentregimens80,82,83.ThisinadditiontohighrecurrenceamongHIV-infectedTBpatientsledWHOtorecommendthatdailyTBregimens(atleastin the initial intensive phase) should be preferred tointermittentregimensamongHIV-infectedTBpatients84.Reviewoftheprimaryevidenceindicatesverylimited,low-qualityinformationonintermittency,mostlyfromobservational studies in the pre-antiretroviral era.DNAfingerprintingstudiesinIndiaindicatethatmostof the recurrences andmany of the failures resultedfromexogenousre-infection,indicatingpoorinfectioncontrol andhigh transmission, andnot poor regimenefficacy85. ConcurrentART duringTB treatment canturn the tide with high treatment success rates andlowfatality,failureandrecurrencerates.Asubsequenttrial conducted at the Tuberculosis Research Centre,Chennai,India(nowNationalInstituteforResearchinTuberculosis) compared the efficacyof twodifferentonce-dailyART regimens co-administered withATTandfoundthatthefavourableoutcometoTBtreatmenthad increased to 93 from83 per cent supporting thefact thatART is important for a favourable responseto ATT86. Treatment outcomes among HIV-infectedTBpatientstreatedintheprogrammeshowlowfailurerates, but high case-fatality associated with lack ofaccesstoART.
A recentmeta-analysis on the treatment ofHIV-associated TB, addressing the three key issues ofdosing schedule, duration of therapy and influenceofART concluded that relapsesweremore commonwithregimensusingrifampicinforlessthan2months,thrice-weekly regimens were associated with morefailures and greater relapses and that ART reducedfailuresandrelapsesconsiderably.Themainlimitationof thismeta- analysiswas the paucity of adequatelypoweredrandomized trials inHIV-TBaddressing theissueofdosingschedule87.Giventhepoorevidencefor
changeandoperationaladvantagesofan intermittentregimen, this recommendation has not yet beenimplementedbylargeAsiancountriesincludingIndiaand China until more evidence is generated throughrandomized controlled trials (RCT) to answer basicquestions of schedule and duration of TB treatmentamong PLWH88. TheNational Institute for ResearchinTuberculosis,Chennai, iscurrentlyaddressing thisissuethroughaRCTcomparingdailyvs.intermittentATTinHIV-associatedTB.
(ii) Anti-retroviral therapy:TheWHOguidelinesformanagementofHIV-infectedTBpatientsinresource-limited settings recommend a combination of twonucleoside reverse transcriptase inhibitors (NRTIs)alongwithonenon-nucleoside reverse transcriptaseinhibitor(NNRTI)forfirstlinetherapy89.InIndia,theNACOrecommendsaregimencontainingzidovudineor stavudine alongwith lamivudine and efavirenz90.RifamycinsinducethecytochromeCYP-450enzymesystem in the liver and intestinal wall, therebyincreasingthemetabolismofproteaseinhibitors(PIs)and NNRTIs91. The effect is weaker with rifabutinthanwithrifampin.Rifampinismetabolizedthroughdeacetylation and is not itself affectedby theCYP-3Asystem.Whenrifampicinandsomeantiretroviraldrugsaregiven together,decreased trough levelsofthe lattermay result, leading to therapeutic failure.Nevirapine levels are reduced by about 40–55 percent,efavirenzby18-25percent,delavaridineby96percentandmostPIsby80-90percent92.Ithasbeensuggested that thedoseofefavirenzbe increased to800mgwhenadministeredalongwithrifampicin,butthismaynotbenecessary insubjectsweighing<50kg93.Manystudieshaveshownexcellentvirologicaland clinical outcomes with the use of efavirenz600 mg along withATT. In India, efavirenz is thepreferred NNRTI for use in HIV-TB co-infectedindividuals at the standard dose of 600 mg once-daily90.However, inpatientswhocannot tolerateorhave contraindications to efavirenz (e.g. psychiatricdisturbances, pregnancy), a triple NRTI regimen ora combinationof twoNRTIs andnevirapine canbeused.Whileonce-dailynevirapinewas shown tobeinferior to efavirenz,with higher virological failureandmortalityrates,thiswasprobablyduetothesub-therapeuticlevelsachievedduringthelead-inperiod,in a situation of induced liver enzymes leading tofastermetabolismof nevirapine86.Manosuthiet al94 demonstrated comparable efficacy with ATT andconcomitantly administered twice-daily NVP and
PADMAPRIYADARSINIet al:HIV-TBCOINFECTION 855

efavirenz. In theirstudycomparingplasma levelsofNVPandtreatmentoutcomesbetweenpatientstreatedwith rifampicin based and non-rifampicin basedregimens, the level of NVPwas low in the formercomparedtonon-rifampicincontainingregimensbutthe virological and immunological outcomes weresimilar95.Analternatestrategyistomodifytheanti-TBregimenwithrifabutinreplacingrifampicin-thedoseofrifabutinrecommendedis300mgODtwice/thrice-weeklywithnevirapinebasedART91.
Many countries are now rolling out PI-basedsecondlineregimensforpatientswithfirstlinetherapyfailure89. Rifampicin markedly reduces the level ofunboosted PIs and hence is not recommended withnelfinavir, indinavir and atazanavir without boostingwithritonavir.Highdosesofritonavircanbeusedwithrifampicinbutattheexpenseofincreasedhepatotoxicity.RecommendeddosesofPIstobeusedwithrifampicinincludelopinavir/ritonavirat400/400mgorsaquinavir/ritonavirat1000/100mgBID.Alternatively,rifabutinwhichhas less interactionwithPIscanbeusedwithdosemodification.Rifabutinisusuallygivenatadoseof300mgdailyandthisremainsthesamewithNRTIsandsaquinavir.Thedoseneedstobeincreasedto450-600mgdailywithEFVwhileitshouldbedecreasedto150mg thrice-weeklywithamprenavir, ritonavirandlopinavir/ritonavir. 87 Rifabutin is contraindicated inleucopeniaandthrombocytopeniawhilehighdosesareknowntocauseuveitis.ThePIcurrentlyrecommendedwith rifabutinbasedATT is lopinavir/ritonavir at thestandarddoseof400/100mgBIDwhilethedosageofatazanavir/ritonaviriscurrentlyunknown.
(iii) Timing of ART & concomitant administration with ATT: It is currently recommended that HIV-infectedindividualswithTBreceiveprompttreatmentforbothdiseases, irrespective of CD4+T cell count, but theoptimal /ideal timing ofART is still under debate89.The advantages of early ART include reduction inearlymortality, improvement in cure rates, reductionin relapses, reduction in malabsorption secondarilypreventing drug resistance toATT and reduction inincidenceofHIV-associated opportunistic infectionsotherthanTB.Thedisadvantagesincludecumulativetoxicity, drug interactions of ART with rifampicin,limiting the choice of combinations and immunereconstitution inflammatory syndrome (IRIS). ThesecanhaveanadverseeffectonthelongtermadherencerequiredforthelifelongtherapyofART.ThesignificanttoxicitiesofthetwoclassesofdrugsarementionedinTableI.
Evidencefromrandomizedcontrolledtrialsshowsthat early initiation of ART during TB treatment isassociatedwith reducedmortality rates, especially inpatientswithprofound immunosuppression (CD4<50cells/μl).TheCAMELIAtrialconductedinCambodia(medianCD4count25cells/μl)showedthatmortalitywasreducedby34percentwhenARTwasinitiatedtwoweeksvs.eightweeksafteronsetofTBtreatment96.The STRIDE and SAPIT trials similarly observedlowerdeathsandAIDS-relatedeventswithcombinedandearlierARTandTB treatment,especiallyamongpeople with CD4 count <50 cells/μl97,98. Based onthese three trials, it is believed thatART should bestartedasamatterofemergency inTBpatientswithCD4 less than50cells/μlandasearlyaspossible intheremainingcases.CautionisneededinpeoplelivingwithHIVwithTBmeningitisasimmediateARTwassignificantly associated with more severe adverseeventswhencomparedtoinitiationofARTtwomonthsafterthestartofTBtreatmentwithoutsurvivalbenefit99.Our approach is to initiateARTwithin the first fewweeks as soon as TB treatment is tolerated and thepatientisstable,aftertreatmentofactiveopportunisticinfections.Table II gives the results of the availablestudiesontimingofART.
Tuberculosis immune reconstitution inflammatory syndrome (TB-IRIS)
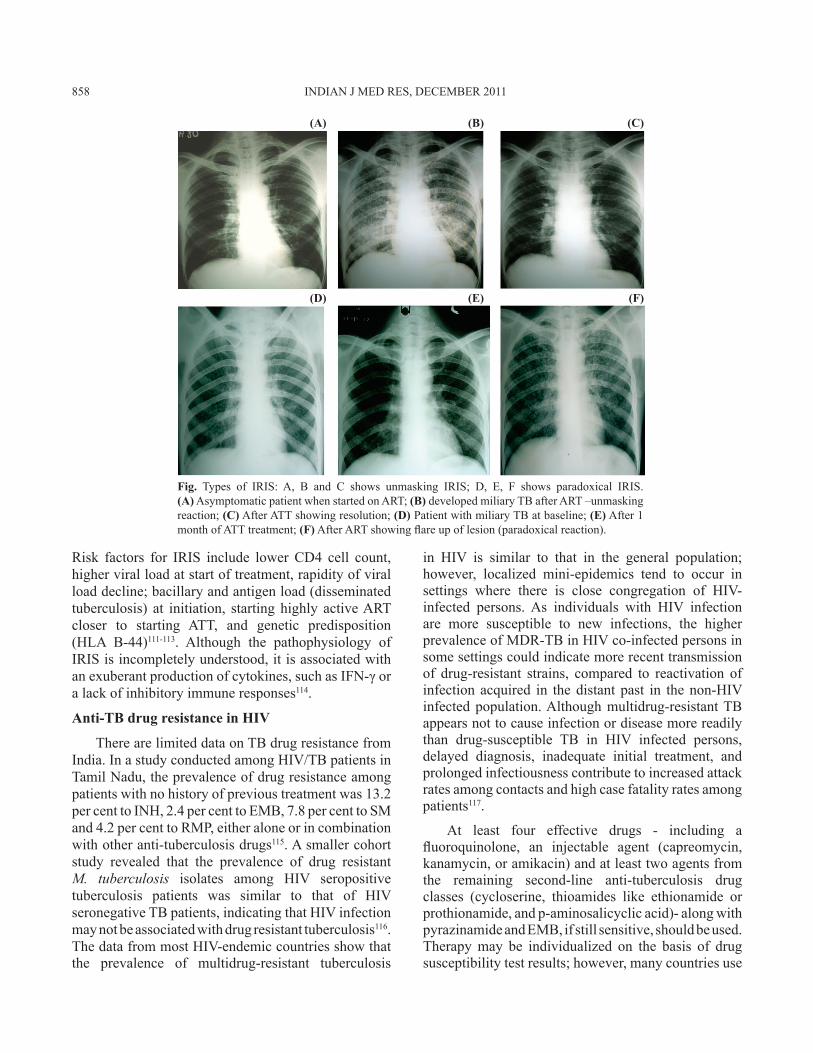
Transient worsening of symptoms and signs oftuberculosis or radiological deterioration after theinitiation of ART, despite a reduction in HIV load(>1 log10 copies/μl) and immunological recovery, isknown as IRIS. Consensus case definitions for TB-IRIShaverecentlybeenpublishedbytheInternationalNetwork for the Study of HIV-associated IRIS(INSHI)102. Drug resistance and other opportunisticinfectionsneed tobe ruledoutbefore adiagnosisofIRIS is made. Hypercalcaemia is a unique featureof tuberculosis IRIS103. There are two types of IRISpresentation: unmasking of undiagnosed tuberculosisandaparadoxicaldeteriorationofexistingtuberculosislesions or appearance of new lesions after initialimprovement(Fig.A-F).ManifestationsofIRISincludefever,lymphnodeenlargement,worseningrespiratorysymptomsandsigns,coldabscess,psoasabscesses,andworseningcentralnervoussystemlesions(tuberculomaand meningitis)103,104. The incidence of tuberculosisIRISrangesfrom8to43percentanditcanusuallybemanagedbyanti-inflammatorydrugsandsteroids,withdeathbeingarareoutcomeandassociatedmostlywithCNSIRIS105,110.Rarely,terminationofARTisrequired.
856 INDIANJMEDRES,DECEMBER2011
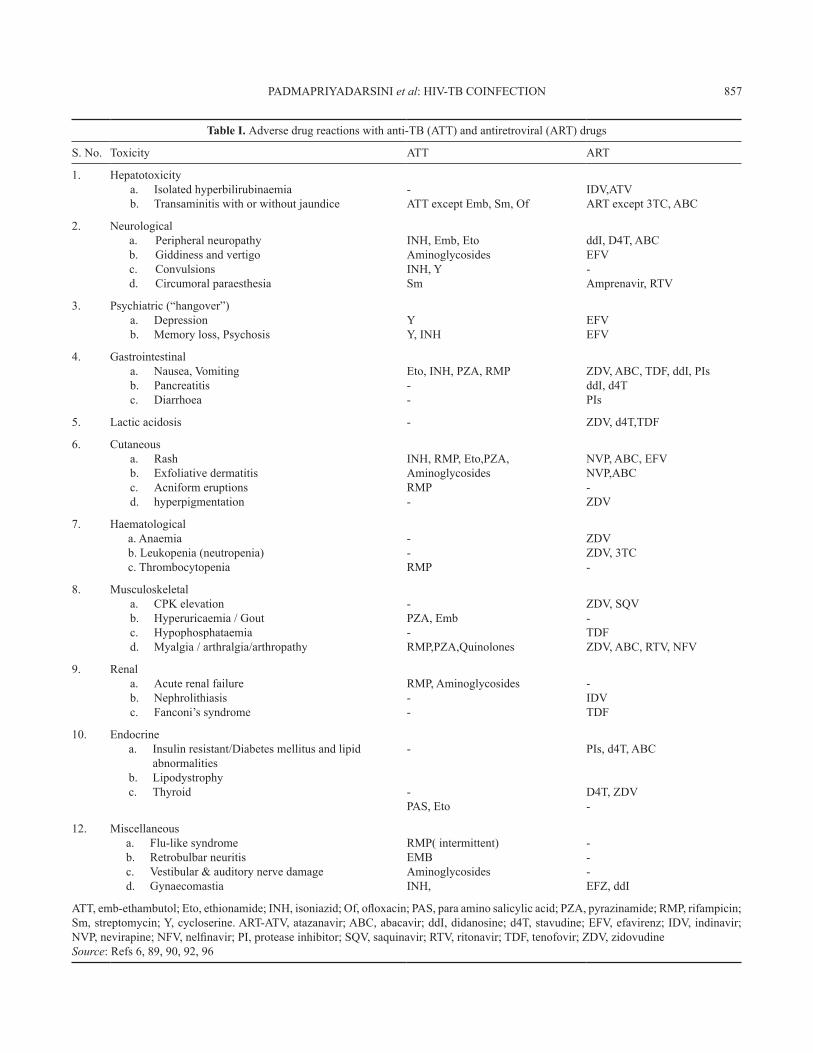
Table I. Adversedrugreactionswithanti-TB(ATT)andantiretroviral(ART)drugs
S.No. Toxicity ATT ART
1. HepatotoxicityIsolatedhyperbilirubinaemiaa.Transaminitiswithorwithoutjaundiceb.
-ATTexceptEmb,Sm,Of
IDV,ATVARTexcept3TC,ABC
2. NeurologicalPeripheralneuropathya.Giddinessandvertigob.Convulsionsc.Circumoralparaesthesiad.
INH,Emb,EtoAminoglycosidesINH,YSm
ddI,D4T,ABCEFV-Amprenavir,RTV
3. Psychiatric(“hangover”)Depressiona.Memoryloss,Psychosisb.
YY,INH
EFVEFV
4. GastrointestinalNausea,Vomitinga.Pancreatitisb.Diarrhoeac.
Eto,INH,PZA,RMP--
ZDV,ABC,TDF,ddI,PIsddI,d4TPIs
5. Lacticacidosis - ZDV,d4T,TDF
6. CutaneousRasha.Exfoliativedermatitisb.Acniformeruptionsc.hyperpigmentationd.
INH,RMP,Eto,PZA,AminoglycosidesRMP-
NVP,ABC,EFVNVP,ABC-ZDV
7. Haematologicala.Anaemiab.Leukopenia(neutropenia)c.Thrombocytopenia
--RMP
ZDVZDV,3TC-
8. MusculoskeletalCPKelevationa.Hyperuricaemia/Goutb.Hypophosphataemiac.Myalgia/arthralgia/arthropathyd.
-PZA,Emb-RMP,PZA,Quinolones
ZDV,SQV-TDFZDV,ABC,RTV,NFV
9. RenalAcuterenalfailurea.Nephrolithiasisb.Fanconi’ssyndromec.
RMP,Aminoglycosides--
-IDVTDF
10. EndocrineInsulinresistant/Diabetesmellitusandlipida.abnormalitiesLipodystrophyb.Thyroidc.
-
-PAS,Eto
PIs,d4T,ABC
D4T,ZDV-
12. MiscellaneousFlu-likesyndromea.Retrobulbarneuritisb.Vestibular&auditorynervedamagec.Gynaecomastiad.
RMP(intermittent)EMBAminoglycosidesINH,
---EFZ,ddI
ATT,emb-ethambutol;Eto,ethionamide;INH,isoniazid;Of,ofloxacin;PAS,paraaminosalicylicacid;PZA,pyrazinamide;RMP,rifampicin;Sm,streptomycin;Y,cycloserine.ART-ATV,atazanavir;ABC,abacavir;ddI,didanosine;d4T,stavudine;EFV,efavirenz;IDV,indinavir;NVP,nevirapine;NFV,nelfinavir;PI,proteaseinhibitor;SQV,saquinavir;RTV,ritonavir;TDF,tenofovir;ZDV,zidovudineSource:Refs6,89,90,92,96
PADMAPRIYADARSINIet al:HIV-TBCOINFECTION 857
Risk factors for IRIS include lowerCD4 cell count,higherviralloadatstartoftreatment,rapidityofviralloaddecline;bacillaryandantigenload(disseminatedtuberculosis) at initiation, startinghighly activeARTcloser to starting ATT, and genetic predisposition(HLA B-44)111-113. Although the pathophysiology ofIRISisincompletelyunderstood,itisassociatedwithanexuberantproductionofcytokines,suchasIFN-γoralackofinhibitoryimmuneresponses114.
Anti-TB drug resistance in HIV
TherearelimiteddataonTBdrugresistancefromIndia.InastudyconductedamongHIV/TBpatientsinTamilNadu,theprevalenceofdrugresistanceamongpatientswithnohistoryofprevioustreatmentwas13.2percenttoINH,2.4percenttoEMB,7.8percenttoSMand4.2percenttoRMP,eitheraloneorincombinationwithotheranti-tuberculosisdrugs115.Asmallercohortstudy revealed that the prevalence of drug resistantM. tuberculosis isolates among HIV seropositivetuberculosis patients was similar to that of HIVseronegativeTBpatients,indicatingthatHIVinfectionmaynotbeassociatedwithdrugresistanttuberculosis116.ThedatafrommostHIV-endemiccountriesshowthatthe prevalence of multidrug-resistant tuberculosis
in HIV is similar to that in the general population;however, localized mini-epidemics tend to occur insettings where there is close congregation of HIV-infected persons.As individuals with HIV infectionare more susceptible to new infections, the higherprevalenceofMDR-TBinHIVco-infectedpersonsinsomesettingscouldindicatemorerecenttransmissionof drug-resistant strains, compared to reactivation ofinfectionacquired in thedistantpast in thenon-HIVinfectedpopulation.Althoughmultidrug-resistantTBappearsnottocauseinfectionordiseasemorereadilythan drug-susceptible TB in HIV infected persons,delayed diagnosis, inadequate initial treatment, andprolongedinfectiousnesscontributetoincreasedattackratesamongcontactsandhighcasefatalityratesamongpatients117.
At least four effective drugs - including afluoroquinolone, an injectable agent (capreomycin,kanamycin,oramikacin)andatleasttwoagentsfromthe remaining second-line anti-tuberculosis drugclasses (cycloserine, thioamides like ethionamide orprothionamide,andp-aminosalicyclicacid)-alongwithpyrazinamideandEMB,ifstillsensitive,shouldbeused.Therapymay be individualized on the basis of drugsusceptibilitytestresults;however,manycountriesuse
Fig. Types of IRIS: A, B and C shows unmasking IRIS; D, E, F shows paradoxical IRIS. (A)AsymptomaticpatientwhenstartedonART;(B)developedmiliaryTBafterART–unmaskingreaction;(C)AfterATTshowingresolution;(D)PatientwithmiliaryTBatbaseline;(E)After1monthofATTtreatment;(F)AfterARTshowingflareupoflesion(paradoxicalreaction).
858 INDIANJMEDRES,DECEMBER2011
(A)
(D)
(B)
(E)
(C)
(F)
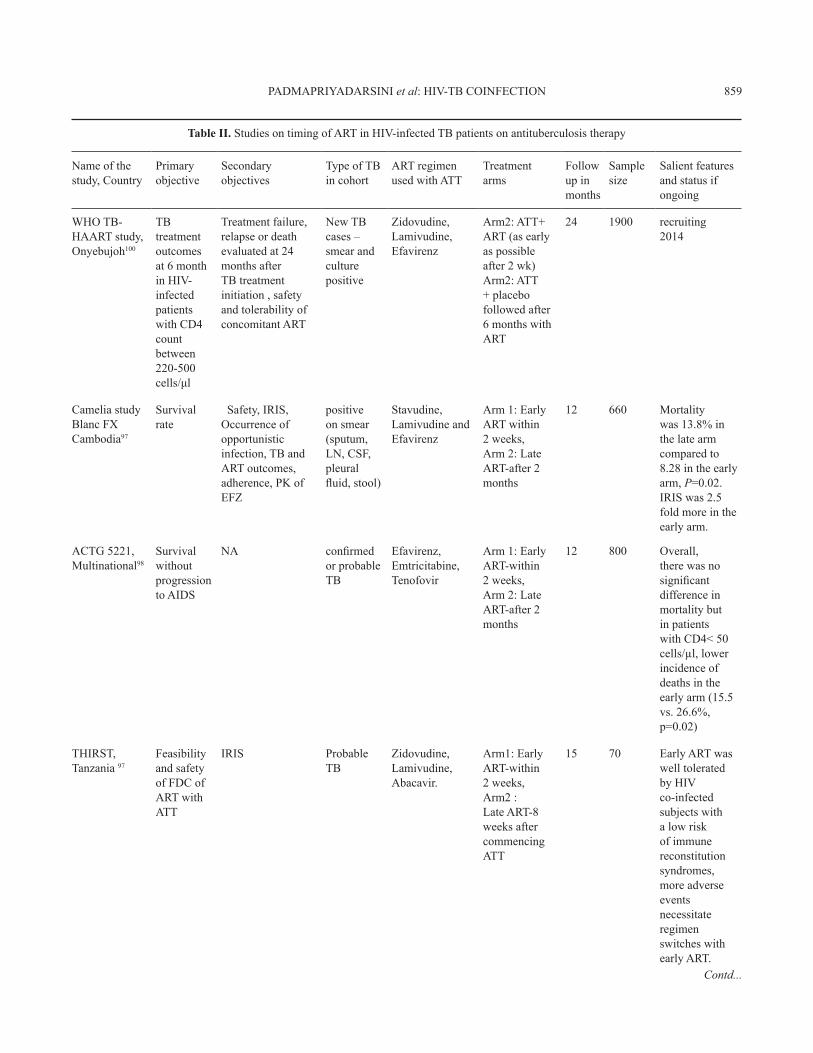
Table II. StudiesontimingofARTinHIV-infectedTBpatientsonantituberculosistherapy
Nameofthestudy,Country
Primaryobjective
Secondaryobjectives
TypeofTBincohort
ARTregimenusedwithATT
Treatmentarms
Followupinmonths
Samplesize
Salientfeaturesandstatusifongoing
WHOTB-HAARTstudy, Onyebujoh100
TBtreatmentoutcomesat6monthinHIV-infectedpatientswithCD4countbetween220-500cells/μl
Treatmentfailure,relapseordeathevaluatedat24monthsafterTBtreatmentinitiation,safetyandtolerabilityofconcomitantART
NewTBcases–smearandculturepositive
Zidovudine,Lamivudine,Efavirenz
Arm2:ATT+ART(asearlyaspossibleafter2wk)Arm2:ATT+placebofollowedafter6monthswithART
24 1900 recruiting2014
CameliastudyBlancFXCambodia97
Survivalrate
Safety,IRIS,Occurrenceofopportunisticinfection,TBandARToutcomes,adherence,PKofEFZ
positiveonsmear(sputum,LN,CSF,pleuralfluid,stool)
Stavudine,LamivudineandEfavirenz
Arm1:EarlyARTwithin2weeks,Arm2:LateART-after2months
12 660 Mortalitywas13.8%inthelatearmcomparedto8.28intheearlyarm,P=0.02.IRISwas2.5foldmoreintheearlyarm.
ACTG5221,Multinational98
SurvivalwithoutprogressiontoAIDS
NA confirmedorprobableTB
Efavirenz,Emtricitabine,Tenofovir
Arm1:EarlyART-within2weeks,Arm2:LateART-after2months
12 800 Overall,therewasnosignificantdifferenceinmortalitybutinpatientswithCD4<50cells/µl,lowerincidenceofdeathsintheearlyarm(15.5vs.26.6%,p=0.02)
THIRST,Tanzania97
FeasibilityandsafetyofFDCofARTwithATT
IRIS ProbableTB
Zidovudine,Lamivudine,Abacavir.
Arm1:EarlyART-within2weeks,Arm2:LateART-8weeksaftercommencingATT
15 70 EarlyARTwaswelltoleratedbyHIVco-infectedsubjectswithalowriskofimmunereconstitutionsyndromes,moreadverseeventsnecessitateregimenswitcheswithearlyART.
Contd...
PADMAPRIYADARSINIet al:HIV-TBCOINFECTION 859

Nameofthestudy,Country
Primaryobjective
Secondaryobjectives
TypeofTBincohort
ARTregimenusedwithATT
Treatmentarms
Followupinmonths
Samplesize
Salientfeaturesandstatusifongoing
SAPITtrial94 KarimSASouthAfrica
IncidenceofprogressiontoAIDSdefiningillnessandmortality
CD4,VL,opportunisticinfections
SmearpositivePTB
Didanosine,Lamivudine,Efavirenz
IntegratedArmArm1:EarlyART-within2weeksofATTArm2:atendofintensivephaseArm3: 6-8monthsafterATTcompleted(stoppedprematurelyduetoincreasedmortality)
18 700 InitiationofARTduringTBtherapyreducedmortalitysignificantlyby56%.IRISincidencewas12.4%intheintegratedarmvs3.4%inthesequentialarmbuttherewerenodeathsduetoIRIS
LN,lymphnode;CSF,cerebrospinalfluid;NA,notapplicable;FDC,fixeddrugcombination;VL,viralload;PTB,pulmonarytuberculosis
Table II (contd.). StudiesontimingofARTinHIV-infectedTBpatientsonantituberculosistherapy
standardized regimens that are basedon surveillanceofantituberculosisdrugresistanceinthecommunity117.DOTS plus regimen is currently followed in Indiacomprisingofkanamycin, levofloxacin, ethionamide,cycloserine, ethambutol, and pyrazinamide givenfor a period of 6-9 months daily in the intensivephase followed by all drugs except kanamycin andpyrazinamide during the continuation phase of 18months,withdosagesprescribedfor3weightbands115.Shorterregimensandnewerdrugsarebeingtestedbutconclusiveevidenceisstilltoemerge.Extensivelydrug-resistanttuberculosis(XDRTB)isdefinedasmultidrug-resistantTBplusresistancetoanyfluoroquinoloneandoneofthesecond-lineantituberculosisinjectableagents(kanamycin, amikacin, or capreomycin). Treatmentoptions are extremely limited and challenging, withhighfrequenciesofadverseeventsanddeath118.
TB-HIV co-ordination activities
In2007,approximately5percentofalldiagnosedTB cases in India came from Integrated CounsellingandTestingCentres(ICTCs),demonstratingthattheseareexcellentsitesforactiveTBcasefinding1.Further,the yield of cases was similar (approximately 20%)fromHIV infected and uninfected clients.One of theprogrammatic limitations encountered is the lack ofinvestigations for extrapulmonary TB at peripheralhealth facilities; another is the distance betweenDesignatedMicroscopyCentres(DMCs)andICTCsinsomedistricts.Thesystemworksmuchbetterwhenboth
are located at the same site. In a pilot study on 4000TB patients in two districts of Tamil Nadu, India, itwasdemonstratedthatover two-thirdswerewillingtoundergoanHIVtestandthemajorbarriertoacceptancewaspatientsnotperceivingthemselvestobeatrisk119.IfpatientsarecounselledandexplainedtheimportanceofhavinganHIVtest,whentheyarediagnosedwithTB,mostwillacceptthetest.Provider-initiatedHIVtestingandcounselling(PITC)isinternationallyrecommendedforTBpatients;thefeasibility,effectiveness,andimpactofthispolicyontheTBprogrammewereevaluatedina study across two districts in south India consideredto have generalized HIV epidemics, Tiruchirappalli(population2.5million)71 andMysore (population2.8million).WithimplementationofPITC,HIVstatuswassuccessfullyascertainedfor70percentofTBpatients.PreviouslyundiagnosedHIV-infectionwasdetectedin6.4percentofthoseTBpatientsnewlytested,enablingreferral for lifesaving anti-retroviral treatment. ARTuptake, however, was poor, suggesting that PITCimplementationshould includemeasures tostrengthenand supportART referral, evaluation, and initiation68.WithincreasingavailabilityofARTacrossthecountry,diagnosisofHIVisbeneficialtotheindividualashe/shecanbereferredtothenearestARTcentreforevaluationandinitiationofantiretroviraltreatment,ifindicated.TBclinics,therefore,formanimportantentrypointforHIVdiagnosis,careandsupport.Co-ordinationandcross-talkbetweenthesetwogovernmenthealthprogrammesarecrucialnotonlytoimprovetheoutcomeofHIV-infected
860 INDIANJMEDRES,DECEMBER2011
TBpatientsbutalsotocontroltheburdenoftuberculosisinIndia.
It isconcludedthat theHIVpandemicpresentsamassivechallengetoglobalTBcontrol.ThepreventionofHIVandTB,theextensionofWHODOTSprograms,andafocusedefforttocontrolHIV-relatedTBinareasofhighHIVprevalencearemattersofgreaturgency.
ReferencesGlobalReport.UNAIDSrepotontheglobalAIDSepidemic1.2010. Available from: http://www.unaids.org/globalreport/documents/20101123_GlobalReport_full_en.pdf,accessedonSeptember20,2011.Corbett E, Watt CJ, Walker N, Maher D, Williams BG,2.RaviglioneMC, et al.The growing burden of tuberculosis:global trends and interactionswith theHIV epidemic.Arch Intern Med 2003;163:1009-21.Lawn S, Churchyard G. Epidemiology of HIV associated3.tuberculosis.Curr Opin HIV AIDS2009;4:325-33.WHOreport2010.Globaltuberculosiscontrol.Availablefrom:4.http://whqlibdoc.who.int/publications/2010/9789241564069_eng.pdf,accessedonSeptember20,2011.Sonnenberg P, Glynn JR, Fielding K, Murray J, Godfrey-5.Faussett P, Shearer S. How soon after infection with HIVdoestheriskoftuberculosisstarttoincrease?AretrospectivecohortstudyinSouthAfricangoldminers.J Infect Dis2007;191:150-8.HavlirDV,GetahunH,Sanne I,NunnP.Opportunities and6.challengesforHIVcareinoverlappingHIVandTBepidemics.JAMA2008;300:423-30.GetahunH,GunnebergC,GranichR,NunnP.HIVinfection-7.associated tuberculosis: the epidemiology and the response.Clin Infect Dis2010;50:S201-7.Towards universal access by 2010: HowWHO is working8.withcountriestoscale-upHIVprevention,treatment,careandsupport. Geneva:WHO;2007.Available from:https://www.who.int/hiv/mediacentre/universal_access_progress_report_en.pdf,accessedon20September28,2011.LawnSD,MyerL,BekkerLG,WoodR.Burdenoftuberculosis9.in an antiretroviral treatment programme in sub-SaharanAfrica: impact on treatment outcomes and implications fortuberculosiscontrol.AIDS2006;20:1605-12.NunnP,WilliamsB,FloydK,DyeC,ElzingaG,Raviglione10.M.TuberculosiscontrolintheeraofHIV.Nat Rev Immunol 2005;5:819-26.Interim policy on collaborative TB/HIV activities. Geneva:11.World Health Organization; 2004 (Report no:WHO/HTM/TB/2004.330).DayJH,CharalambousS,FieldingKL,HayesRJ,Churchyard12.GJ,GrantAD.Screening for tuberculosis prior to isoniazidpreventivetherapyamongHIV-infectedgoldminersinSouthAfrica. Int J Tuberc Lung Dis2006;10:523-9.MohammedA,EhrlichR,WoodR,Cilliers F,MaartensG.13.Screening for tuberculosis in adults with advanced HIVinfectionprior topreventive therapy. Int J Tuberc Lung Dis 2004;8:792-5.
Shah S, Demissie M, Lambert L, Ahmed J, Leulseged S,14.KebedeT,et al. IntensifiedtuberculosiscasefindingamongHIV-infectedpersonsfromavoluntarycounselingandtestingcenterinAddisAbaba,Ethiopia.J Acquir Immune Defic Syndr 2009;50:537-45.WHO(2007)Improvingthediagnosisandtreatmentofsmear-15.negativepulmonaryandextrapulmonarytuberculosisamongadultsandadolescents:RecommendationsforHIV-prevalentand resource-constrained settings. Available from: http://whqlibdoc.who.int/hq/2007/WHO_HTM_TB_2007.379_eng.pdf,accessedonSeptember20,2011.KooleO,Thai S,KhunKE, PeR, vanGriensven J,Apers16.L,et al.Evaluationof the2007WHOguideline to improvethe diagnosis of tuberculosis in ambulatory HIV-positiveadults.PLoS ONE2011;6(4):e18502.doi:10.1371/journal.pone.0018502.GetahunH,KittikraisakW,HeilingCM,CorbettEL,Ayles17.H,CainKP,et al.Developmentofastandardizedscreeningrule for tuberculosis in people livingwithHIV in resourceconstrainedsettings:Individualparticipantdatameta-analysisofobservationalstudies.PLoS Med2011;8(1):e1000391.PostFA,WoodR,PillayGP.PulmonarytuberculosisinHIV18.infection: radiographic appearance is related to CD4+T-lymphocytescount.Tuberc Lung Dis1995;76:518-21.SwaminathanS,NarendranG,MenonPA,Padmapriyadarsini19.C,ArunkumarN,SudharshanamNM,et al. Impact ofHIVinfectiononradiographicfeaturesinpatientswithpulmonarytuberculosis.Indian J Chest Dis Allied Sci2007;49:133-6.ChurchyardG,FieldingKL,Lewis JJ,ChihotaVN,Hanifa20.Y,GrantAD.Symptomandchestradiographicscreeningforinfectious tuberculosis prior to starting isoniazid preventivetherapy:yieldandproportionmissedatscreening.AIDS2010;24:S19-2749.Hopewell P, PaiM,MaherD,UplekarM,RaviglioneMC.21.Internationalstandardsfortuberculosiscare.Lancet Infect Dis 2006;6 :710-25.Cattamanchi A, Dowdy DW, Davis JL, Worodria W, Yoo22.S, JolobaM,et al.Sensitivityofdirectversus concentratedsputumsmearmicroscopyinHIV-infectedpatientssuspectedofhavingpulmonarytuberculosis.BMC Infect Dis2009;9:53.ElliotAM,NamaamboK,AllenBW,LuoN,HayesRJ,Pobee23.JO, et al. Negative sputum smear results in HIV positivepatients with pulmonary tuberculosis in Lusaka, Zambia.Tubercle Lung Dis1993;74:191-4.Steingart KR, Henry M, Ng V, Hopewell PC, Ramsay A,24.Cunningham J, et al. Fluorescence versus conventionalsputum smear microscopy for tuberculosis: a systematicreview.Lancet Infect Dis2006;6:570-81.Cattamanchi A, Davis JL, Pai M, Huang L, Hopewell25.PC, Steingart KR, et al. Does bleach processing increasethe accuracy of sputum smear microscopy for diagnosingpulmonarytuberculosis?J Clin Microbiol2010;48:2433-9.Steingart KR, Ng V, Henry M, Hopewell PC, Ramsay A,26.CunninghamJ,et al.Sputumprocessingmethodstoimprovethe sensitivity of smear microscopy for tuberculosis: asystematicreview.Lancet Infect Dis2006;6:664-74.
PADMAPRIYADARSINIet al:HIV-TBCOINFECTION 861
Yassin MA, Cuevas LE. How many sputum smears are27.necessary for case finding in pulmonary tuberculosis?Trop Med Int Health2003;8:927-32.Dorman S. New diagnostic tests for tuberculosis: bench,28.bedside, and beyond. Clin Infect Dis 2010; 50 (Suppl 3):173-7.FINDstudytrialsataglance:PrimoStariLEDmicroscope.29.Availablefrom:http:// www.finddiagnostics.org,accessedonSeptember10,2011.MteiL,MateeM,HerfortO,BakariM,HorsburghCR,Waddell30.R, et al. High rates of clinical and subclinical tuberculosisamong HIV-infected ambulatory subjects in Tanzania.Clin Infect Dis2005;40:1500-7.World Health Organization. Improving the diagnosis and31.treatmentof smear-negativepulmonary and extrapulmonarytuberculosisamongadultsandadolescents:recommendationsforHIV-prevalentandresource-constrainedsettings.Geneva:WorldHealthOrganization;2007.Williams-BouyerN,YorkeR,LeeHI,WoodsGL.Comparison32.of the BACTECMGIT 960 and ESP culture system II forgrowthanddetectionofmycobacteria.J Clin Microbiol2000;38:4167-70.Gil-Setas A, Torroba L, Fernandez JL, Martinez-Artola V,33.Olite J. Evaluation of theMB/BacT system comparedwithMiddlebrook7H11andLowenstein-Jensenmediafordetectionandrecoveryofmycobacteria fromclinicalspecimens.Clin Microbiol Infect2004;10:224-8.LeeJJ,SuoJ,LinCB,WangJD,LinTY,TsaiYC.Comparative34.evaluation of the BACTEC MGIT 960 system with solidmediumforisolationofmycobacteria.Int J Tuberc Lung Dis 2003;7:569-74.FarniaP,MohammadiF,MirsaediM,ZarifeAZ,TabatabeeJ,35.BahadoriK,et al.Applicationofoxidationreductionassayformonitoringtreatmentofpatientswithpulmonarytuberculosis.J Clin Microbiol2004;42:3324-5.Moore DA, Mendoza D, Gilman RH, Evans CA, Hollm36.DelgadoMG,GuerraJ,et al.Microscopicobservationdrugsusceptibility assay, a rapid, reliable diagnostic test formultidrug resistant tuberculosis suitable for use in resourcepoorsettings.J Clin Microbiol2004;42:4432-7.Kalantri S, Pai M, Pascopella L, Riley L, Reingold A.37.BacteriophagebasedtestsforthedetectionofMycobacterium tuberculosis in clinical specimens: a systematic review andmeta-analysis.BMC Infect Dis2005;5:59.PaiM,MinionJ,SteingartK,RamsayA.Newandimproved38.tuberculosis diagnostics: evidence, policy, practice, andimpact.Curr Opin Pulm Med 2010;16:271-84.Baylan O, Kisa O, Albay A, Doganci L. Evaluation of a39.new automated, rapid, colorimetric culture system usingsolid medium for laboratory diagnosis of tuberculosis anddetermination of anti-tuberculosis drug susceptibility. Int J Tuberc Lung Dis2004;8:772-7.Chaudahary M, Gupta S, Khare S, Lal S. Diagnosis of40.tuberculosisinaneraofHIVpandemic:Areviewofcurrentstatus and futureprospects. Indian J Med Micro 2010;28 :281-9.MorganM,KalantriS,FloresL,PaiM.Acommercial line41.probe assay for the rapid detection of rifampicin resistance
inmycobacteriumtuberculosis:Asystematicreviewandmetaanalysis. BMC Infect Dis2005;5:62.World Health Organization. Molecular line probe assays42.for rapid screeningofpatients at riskofmultidrug resistanttuberculosis. Available from: http://www.who.int/tb/laboratory/lpa_policy.pdf,accessedonSeptember15,2011.ChauhanL.S.StatusReportonRNTCP.43. Indian J Tuberc2009;56:151-3.World Health Organization and STOP TB department.44.RoadmapforrollingoutXpertMTB/RIFforrapiddiagnosisofTBandMDR-TB.Availablefrom:http://www.who.int/tb/laboratory/roadmap_xpert_mtb-rif.pdf, accessed onOctober5,2011.RachowA,ZumlaA,HeinrichN,Rojas-PonceG,MtafyaB,45.ReitherKet al.RapidandaccuratedetectionofMycobacteriumtuberculosis in sputum samples by Cepheid Xpert MTB/RIFassay–aclinicalvalidationstudy.PLoS One2011;6 :e20458.Van Rie A, Page-Shipp L, Scott L, Sanne I, Stevens W.46.Xpert(®)MTB/RIFforpoint-of-carediagnosisofTBinhigh-HIVburden,resource-limitedcountries:hypeorhope?Expert Rev Mol Diagn2010;10:937-46.Zeka AN, Tasbakan S, Cavusoglu C. Evaluation of the47.GeneXpert MTB/RIF Assay for the Rapid Diagnosis ofTuberculosis and detection of RIF-resistance in PulmonaryandExtrapulmonarySpecimens.J Clin Microbiol2011;49 :4138-41.Boehme CC, Nabeta P, HillemannD, NicolMP, Shenai S,48.KrappF,et al.Rapidmoleculardetectionoftuberculosisandrifampinresistance.N Eng J Med2010;363:1005-15.Gennaro ML. Immunologic diagnosis of tuberculosis.49. Clin Infect Dis2000;30:S243-6.ChanED,HeifetsL,IsemanMD.Immunologicdiagnosisof50.tuberculosis:Areview.Tuberc Lung Dis2000;80:131-40.WanchuA.Advances in serology for diagnosingTB in the51.HIVinfected.Indian J Chet Dis Allied Sci2005;47:31-7.MorrisK.WHOrecommendsagainstinaccuratetuberculosis52.tests.Lancet2011;377:113-4.DowdyDW,SteingartKR,PaiM.Serologicaltestingversus53.otherstrategiesfordiagnosisofactivetuberculosisinIndia:acost-effectivenessanalysis.PLoS Med2011;8:e1001074.Khosla R, Dwivedi A, Sarin BC, Sehajpal PK. Peripheral54.blood based C-PCR assay for diagnosing extra-pulmonarytuberculosis.Indian J Exp Biol2009;47:447-53.KashyapRS,RamtekeSS,MoreySH,PurohitHJ,TaoriGM,55.DaginawalaHF.Diagnosticvalueofearlysecretedantigenictarget-6forthediagnosisoftuberculousmeningitispatients.Infection 2009;37:508-13.Mutetwa R, Boehme C, DimairoM, Bandason T,Munyati56.SS,MangwanyaD,et al.Diagnosticaccuracyofcommercialurinary lipoarabinomannandetection inAfrican tuberculosissuspects and patients. Int J Tuberc Lung Dis 2009; 13 :1253-9.ShahM,VariavaE,HolmesCB,CoppinA,GolubJE,McCallum57.J, et al. Diagnostic accuracy of a urine lipoarabinomannantest for tuberculosis in hospitalized patients in a high HIVprevalencesetting. J Acquir Immune Defic Syndr2009;52 :145-51.
862 INDIANJMEDRES,DECEMBER2011

SwaminathanS,SubbaramanR,VenkatesanP,Subramanyam58.S,KumarSR,MayerKH,et al.Tuberculinskin test resultsin HIV-infected patients in India: Implications for latenttuberculosistreatment.Int J Tuberc Lung Dis2008;12:168-73.PaiM, Riley LW, Colford JM Jr. Interferon-gamma assays59.intheimmunodiagnosisoftuberculosis:asystematicreview.Lancet Infect Dis2004;4:761-76`.Liebeschuets S, Bamber S, Ewer K, Deeks J, PathanAA,60.LalvaniA.DiagnosisoftuberculosisinSouthAfricanchildrenwithT-cell based assay:Aprospective cohort study.Lancet 2004;364:2196-203.Rangaka MX, Wilkinson KA, Seldone R, Van Cutsem G,61.MeintjesGA,MorroniC,et al.TheeffectofHIV-1infectiononT-cellbasedandskintestdetectionoftuberculosisinfection.Am J Respir Crit Care Med2007;175 :514-20.Pai M. Alternatives to the tuberculin skin test: interferon62.γ assays in the diagnosis of Mycobacterium tuberculosisinfection.Indian J Med Micro2005;23:151-8.WorldHealthOrganization.StrategicandTechnicalAdvisory63.Group (STAG-TB). 2010. Report of the 10th Meeting.Availablefrom:http:// www.who.int/tb/advisory_bodies/stag_tb_report_2010.pdf,accessedonSeptember30,2011.Philips M, Basa-Dalay V, Bothamley G, Cataneo RN,64.Lam PK, Natividad MPR, et al. Breath biomarkersof active pulmonary tuberculosis. Tuberculosis 2010; 90 :145-51.Banday KM, Pasikanti KK, Chan EC, Singla R, Rao KV,65.ChauhanVS,et al.Useofurinevolatileorganiccompoundstodiscriminatetuberculosispatientsfromhealthysubjects.Anal Chem 2011;83:5526-34.Arend Kolk,Michael Hoelscher, LeonardMaboko, Jung J,66.KuijperS,CauchiM,et al.Electronic-nosetechnologyusingsputum samples in diagnosis of patients with tuberculosis. J Clin Microbiol 2010;48 :4235-8.WorldHealthOrganizationUNJPoHA.Guidanceonprovider67.initiated HIV testing and counseling in health facilities.Geneva:WorldHealthOrganization,2007.VijayS,SwaminathanS,VaidyanathanP,ThomasA,Chauhan68.LS, Kumar P, et al. Feasibility of Provider-Initiated HIVTestingandCounselingoftuberculosispatientsundertheTBControlProgrammeintwodistrictsofSouthIndia.PLoS One 4(11):e7899.World Health Organization.69. Essential Prevention and Care Interventions for adults and adolescents living with HIV in resource limited settings.Geneva:WorldHealthOrganization;2008.Wilkinson D, Squire SB, Garner P. Effect of preventive70.treatment for tuberculosis in adults infected with HIV:systematic review of randomized placebo controlled trials.BMJ 1998;317:625-9.BucherH,GriffithLE,GuyattGH,SudreP,NaefM,SendiP,71.et al.IsoniazidprophylaxisfortuberculosisinHIVinfection:ameta-analysisofrandomizedcontrolled trials.AIDS1999;13:501-7.Guidelines for intensified tuberculosis case finding and72.isoniazid preventive therapy for people living with HIV inresource constrained settings. Stop TB department. World
Health Organization, Geneva 2011. Available from: http://whqlibdoc.who.int/publications/2011/9789241500708_eng.pdf,accessedonAugust2,2011.ChurchyardGJ,ScanoF,GeantAD,ChaissonRE.Tuberculosis73.preventivetherapyintheeraofHIVinfection:overviewandresearchpriorities.J Infect Dis2007;196:S52-62.Swaminathan S, Menon PA, Narendran G, Venkatesan P,74.Ramesh Kumar S, Ranjani Ramachandran, et al. Efficacyofasix-monthversusa36-monthregimenforpreventionoftuberculosisinHIV-infectedpersonsinIndia:ARandomizedclinicaltrial.UnpublishedData.MartinsonNA,BarnesGL,MoultonLH,MsandiwaR,Hausler75.H, RamM, et al. New regimens to prevent tuberculosis inadultswithHIVinfection.N Engl J Med2011;365 :11-20.SamandariT,AgizewTB,Nyirenda S,TedlaZ, SibandaT,76.ShangN,et al.6-monthversus36-monthisoniazidpreventivetreatment for tuberculosis in adults with HIV infection inBotswana: a randomized, double-blind, placebo-controlledtrial.Lancet2011:377:1588-98.NACOAnnualReport2010-2011.Availablefrom:77. http://www.nacoonline.org/upload/REPORTS/NACO%20Annual%20Report%202010-11.pdf,accessedonSeptember30,2011.CentralTBDivision,DirectorateGeneralofHealthServices,78.Ministry of Health and Family Welfare. TB India 2008 -RNTCP status report. Available from; http://www.tbcindia.org/pdfs/TB-India-2008.pdf,accessedonOctober2,2011.JindaniA,NunnAJ,EnarsonDA.Two8-monthregimensof79.chemotherapy for treatment of newly diagnosed pulmonarytuberculosis: international multicentre randomized trial.Lancet2004;364:1244-51.KorenrompEL,ScanoF,WilliamsBG,DyeC,NunnP.Effect80.of human immunodeficiency virus infection on recurrencesof tuberculosis after rifampin-based treatment: an analyticalreview.Clin Infect Dis2003;37:101-12.Swaminathan S, Narendran G, Venkatesan P, Iliayas S,81.SanthanakrishnanR,MenonPA,et al.Efficacyofa6-monthversus9-monthintermittenttreatmentregimeninHIV-infectedpatientswith tuberculosis: a randomizedclinical trial. Am J Respir Crit Care Med2010;181:743-51.BurmanW,BenatorD,VernonA,KhanA,JonesB,SilvaC,82.et al. Tuberculosis Trials Consortium. Acquired rifamycinresistance with twice-weekly treatment of HIV-relatedtuberculosis.Am J Respir Crit Care Med2006;173:350-6.Nahid P, Gonzalez LC, Rudoy I, de Jong BC, Unger A,83.Kawamura LM, et al.Treatment outcomes of patientswithHIVandtuberculosis.Am J Respir Crit Care Med2007;175 :1199-206. 84. WHO Library Cataloguing-in-Publication Data: Treatment of tuberculosis: guidelines, 4th ed., accessed onSeptember 28,2011fromWHO/HTM/TB/2009.420.Narayanan S, Swaminathan S, Supply P, Shanmugam S,85.NarendranG,HariL,et al. ImpactofHIV infectionon therecurrenceofTuberculosisinSouthIndia.J Infect Dis2010;201 :691-703.Swaminathan S, Padmapriyadarsini C, Venkatesan P,86.NarendranG,RameshKumarS, IliayasS,et al.Efficacyand safety of once-daily nevirapine- or efavirenz-basedantiretroviral therapy in HIV associated tuberculosis: A
PADMAPRIYADARSINIet al:HIV-TBCOINFECTION 863
randomized clinical trial.Clin Infect Dis 2011;53 : 716-24.Khan FA, Minion J, Pai M, Royce S, BurmanW, Harries87.AD,et al.TreatmentofactivetuberculosisinHIV-coinfectedpatients:Asystematic reviewandmeta-analysis.Clin Infect Dis2010;50:1288-99.SwaminathanS,PadmapriyadarsiniC,PonnurajaC,RanjaniR,88.SriramS,KumarRS,et al.Tuberculosistreatmentoutcomesamongpatients treatedwithashort-course intermittentanti-TB regimen and either once-daily Nevirapine or Efavirenzbased antiretroviral therapy: a randomized clinical trial.Abstractpresentedin41stUnionWorldConferenceonLungHealth, Berlin, November 2011. 2010; Clinical trials.govnumberNCT00332306.Antiretroviral therapy for HIV infection in adults and89.adolescents-WorldHealthorganization2010.Availablefrom:http://whqlibdoc.who.int/publications/2010/9789241599764_eng.pdf,accessedonSeptember12,2011.Antiretroviral Therapy Guidelines for HIV-Infected Adults90.and Adolescents Including Post-exposure Prophylaxis–NationalAidsControl organization2007.Available from:http://upaidscontrol.up.nic.in/ART%20Guidelines%20for%20HIV-Infected%20Adults%20and%20Adolescents%20Including%20Post-exposure.pdf, accessed onSeptember 12,2011.de JongBC, IsraelskiDM,CorbettEL,SmallPM.Clinical91.managementoftuberculosisinthecontextofHIVinfection.Annu Rev Med2004;55:283-301.McIlleron H, Meintjes G, Burman WJ, Maartens G.92.Complications of antiretroviral therapy in patients withtuberculosis: drug interactions, toxicity, and immunereconstitutioninflammatorysyndrome.J Infect Dis2007;196 :S63-S75.ManosuthiW,SungkanuparphS,ThakkinstianA,Vibhagool93.A,KiertiburanakulS,RattanasiriS,et al.Efavirenzlevelsand24-week efficacy inHIV-infected patientswith tuberculosisreceivinghighlyactiveantiretroviraltherapyandrifampicin.AIDS2005;19:1481486.Manosuthi W, Mankatitham W, Lueangniyomkul A,94.Chimsuntorn S, Sungkanuparph S. Standard-dose efavirenzvs.standard-dosenevirapineinantiretroviralregimensamongHIV-1 and tuberculosis co-infected patients who receivedRifampicin.HIV Med2008;9:294-9.ManosuthiW,SungkanuparphS,ThakkinstianA,Rattanasiri95.S,ChaovavanichA,PrasithsirikulW,et al.Plasmanevirapinelevelsand24-weekefficacyinHIV-infectedpatientsreceivingnevirapine-basedhighlyactiveantiretroviral therapywithorwithoutRifampicin.Clin Infect Dis2006;43:253-5.Blanc F, Sok T, Laureillard D, Borand L, Rekacewicz C,96.NerrienetE, et al. Earlier versus later start of antiretroviraltherapy in HIV-infected adults with tuberculosis.N Engl J Med2011;365:1471-81.Havlir D, Ive P, Kendall M, LuetkemeyerA, Swindells S,97.Kumwenda J,et al.A5521Team InternationalRandomizedTrial of Immediate vsEarlyART inHIV+PatientsTreatedfor TB:ACTG 5221 STRIDE Study.Abstract presented atthe XVIII Conference on Retroviruses and OpportunisticInfections;2011Feb27-Mar2;Boston(MA).
AbdoolKarimS,NaidooK,GroblerA,PadayatchiN,Baxter98.C,GrayA,et al.Timingof initiationofantiretroviraldrugsduringtuberculosistherapy.N Engl J Med 2010;25 :697-70.TorokME,YenNT,ChauTT,MaiNT,PhuNH,MaiPP,99. et al. Timing of initiation of antiretroviral therapy in humanimmunodeficiency virus (HIV)-associated tuberculousmeningitis.Clin Infect Dis2011;52:1374-83.WorldHealthOrganization.An evaluation of the impact of100.early initiation of Highly Active Anti-Retroviral Therapy(HAART)onTuberculosis (TB) treatmentoutcomes forTBpatients co-infected with Human Immunodeficiency Virus(HIV)[ISRCTN77861053].CurrentControlledTrials[online].Availablefrom:http://www.controlledtrials.com,accessedonOctober9,2011.Shao HJ, Crump JA, Ramadhani HO, Uiso LO, Ole-101.NguyaineS,MoonAM,et al.Earlyversusdelayedfixeddosecombinationabacavir/lamivudine/zidovudineinpatientswithHIVandtuberculosisinTanzania.AIDS Res Hum Retroviruses 2009;25:1277-85.MeintjesG,LawnSD, Scano F,MaartensG, FrenchMA,102.Worodria W, et al. International network for the study ofHIV-associated IRIS. Tuberculosis associated immunereconstitution inflammatory syndrome: case definitions foruse in resource-limited settings.Lancet Infect Dis2008;8 :516-23.Lawn SD, Bekker LG, Miller RF. Immune reconstitution103.disease associated with mycobacterial infections in HIV-infected individuals receiving antiretrovirals. Lancet Infect Dis2005;5:361-73.RobertsonJC,FichtenbaumCJ.CaseontheWeb:diagnosis104.andmanagementof the immune reconstitution syndrome inHIV-infectedpatients.InternationalAIDSSociety-USAWebsite.Availablefrom:http://www.iasusa.org/cow. Presentation 37,accessedonSeptember30,2011.Kumar RS, Narendran G, Patrawalla P, Menon PA,Mayer105.K, Swaminathan S. Immune reconstitution inflammatorysyndrome in HIV infected patients with and without priortuberculosis.Unpublisheddata.Lawn SD, Myer L, Beckker LG, Wood R. Tuberculosis106.associated immune reconstitution disease: incidence, riskfactors and impact in an antiretroviral treatment service inSouthAfrica.AIDS2007;21:335-73.RatnamI,ChiuC,KandalNB,EasterbrookPJ.Incidenceand107.riskfactorsforimmunereconstitutioninflammatorysyndromeinanethnicallydiverseHIVtype1-infectedcohort.Clin Infect Dis2006;42:418-27.NaritaM,AshkinD,HollenderES,PitchenikAE.Paradoxical108.worseningoftuberculosisfollowingantiretroviraltherapyinpatientswithAIDS.Am J Respir Crit Care Med1998;158 :157-61.BretonG,DuvalX,EstellatC,PoalettiX,BonnetD,Mvondo109.Mvondo D, et al. Determinants of immune reconstitutioninflammatorysyndromeinHIVtype1-infectedpatientswithtuberculosis after initiation of antiretroviral therapy. Clin Infect Dis2004;39:1709-12.Breen RA, Smith CJ, Bettinson H, Dart S, Bannister B,110.JohnsonMA,et alParadoxicalreactionsduringtuberculosistreatment in patients with and without HIV co-infection.Thorax2004;59 :704-7.
864 INDIANJMEDRES,DECEMBER2011

RobertsonJ,MeierM,WallJ,YingJ,FitctenbaumCJ.Immune111.reconstitutionsyndrome inHIV:validatingacasedefinitionand identifying clinical predictors in persons initiatingantiretroviraltherapy.Clin Infect Dis2006;42:1639-46.ManabeYC, Campbell JD, Sydnor E,MooreRD. Immune112.reconstitution inflammatory syndrome: risk factors andtreatment implications. J Acquir Immune Defic Syndr 2007;46:456-62.Price P, Morahan G, Huang D, Stone E, Cheong KY,113.Castley A, et al. Polymorphisms in cytokine genes definesubpopulations ofHIV-1 patientswho experienced immunerestorationdiseases.AIDS2002;16:2043-7.BourgaritA,CarcelainG,MartinezV,LascouxC,DelceyV,114.GicquelB,et al.ExplosionoftuberculinspecificTh1-responsesinducesimmunerestorationsyndromeintuberculosisandHIVco-infectedpatients.AIDS2006;20:F1-F7.Swaminathan S, Paramasivan CN, Ponnuraja C, Iliayas115.S, Rajasekaran S, Narayanan PR. Anti-tuberculosis drug
resistancetuberculosisinSouthIndia.Int J Tuberc Lung Dis 2005;9:896-900.PereiraM, Tripathy S, InamdarV, Ramesh K, BhavsarM,116.Date A, et al. Drug resistance pattern of MycobacteriumtuberculosisinseropositiveandseronegativeHIV-TBpatientsinPune,India.Indian Med J Res2005;121:235-9.Wells CD, Cegielski P, Nelson LJ, Laserson KF, Holtz117.TH, FinlayA, et al. HIV infection and multidrug resistanttuberculosis:theperfectstorm.J Infect Dis2007;196:S86-S107.Revised National Tuberculosis Control Programme-DOTS118.plus guidelines 2010. Available from: http://www.tbcindia.org/pdfs/DOTS_Plus_Guidelines_Jan2010.pdf, accessed onOctober13,2011.Thomas BE, Ramachandran R, Anitha S, Swaminathan S.119.FeasibilityofroutineHIVtestingamongTBpatientsthrougha Voluntary, Counseling and Testing Centre (VCTC). Int J Tuberc Lung Dis2007;11:1296-301.
Reprint requests:DrSoumyaSwaminathan,Scientist‘G’&HOD,DepartmentofClinicalResearch,NationalInstituteforResearchinTuberculosis,No.1,SathiyamoorthyRoad,Chetpet,Chennai600031,India
e-mail:[email protected]
PADMAPRIYADARSINIet al:HIV-TBCOINFECTION 865




![PerformanceofClinicalAlgorithmsfor Smear ... · 2 Tuberculosis Research and Treatment AFB smear-negative PTB for HIV-infected patients are still limited and inconsistent [6, 8]. This](https://img.pdfslide.us/doc/110x75/608cc3f7e89540310a24c5c9/performanceofclinicalalgorithmsfor-smear-2-tuberculosis-research-and-treatment.jpg)























