Embed Size (px)
Citation preview
115
Abstract
The Marston Symptoms Checklist for detectingdepression was used to determine whether or notthe notion of ‘depressive equivalents’ can provide afew of the core characteristics necessary for thediagnosis of depressive disorders in people withsevere/profound intellectual disability (ID). Diag-noses of major depression were made by a psychia-trist using the DSM-III-R criteria, combined withinformation from records, staff, team, parents,behaviour profiles, direct observations, mental statusand follow-up visits. Twenty-two people with ID fulfilled the selection criteria from a larger sample of patients who had been evaluated in contactvisits. Scores on the checklist for major depressionfor subjects with severe/profound ID were similarto the core characteristics for diagnosis of majordepression by DSM-III-R criteria. Evidence wasfound for the presence of depressive equivalents inthe subjects, but these appeared to be secondary.The participants with severe/profound ID wereobserved mostly during the depressive phase ofbipolar I and bipolar II disorder, and major depres-sion, recurrent type. Melancholic features wereprominent in their presentation. Further studies of
people with ID are needed to determine whetherdepressive equivalents are more prominent in casesof major depression with atypical features than incases of major depression with melancholic features.
Keywords core characteristics, depression, depres-sive equivalents
Introduction
The prevalence of psychiatric disorders in peoplewith intellectual disability (ID) is higher than in thegeneral population (Campbell & Malone ;Borshwick-Duffy ). The diagnosis of depressivedisorders in people with ID has undergone thesame process of recognition as occurred for depres-sion in children. It has become clear that peoplewith ID do indeed suffer from affective disorders(Berman ; Reid ; Sovner & Hurley ;Szymanski & Biederman ; Reiss & Trenn ;Proust & Schaefer ; Sovner & Lowry ).The symptoms of depression in people withmild/moderate ID are similar to those in peoplewho do not have ID and can be diagnosed withDSM-III (APA ) criteria (Pawlarcyzk & Beck-with ). However, how should the diagnosis ofdepression be made in non-verbal people withsevere/profound ID, especially if affective symptomshave not been identified and reported by infor-mants (Sovner & Hurley )?
Journal of Intellectual Disability Research
pp –
© Blackwell Science Ltd
Diagnosis of depression in people with severe/profoundintellectual disability
J.A.Tsiouris
George A. Jervis Clinic, NY State Institute for Basic Research in Developmental Disabilities, Staten Island, New York, USA
Correspondence: Dr John A. Tsiouris, George A. Jervis Clinic, NY
State Institute for Basic Research in Developmental Disabilities,
Forest Hill Road, Staten Island, NY , USA (e-mail:

The DSM-III-R (APA ; Charlot et al. ;Meins ) and DSM-IV (APA ) criteria(Tsiouris & Patti ; Myers ) have beenapplied to diagnose or to confirm the diagnosis ofdepression in people with mild/moderate andsevere/profound ID. Meins () reported higherincidences of aggression, tantrums, self-injuriousbehaviour, screaming, crying and stereotypiesamong people with severe/profound ID and depres-sion than among those with mild/moderate ID. Theabove author introduced the term ‘behaviouraldepressive equivalents’ for these behaviours. Usinga checklist of signs and symptoms derived fromthe ICD- (WHO ) criteria for depressionand the Disability Assessment Schedule (Holmeset al. ), Marston et al. () reported that‘behavioural depressive equivalents’ were statisti-cally more prominent in the eight people withsevere ID than in the individuals with mild/mod-erate ID whom they studied, all of whom werediagnosed with depression. Suggestions have beenmade for the incorporation of behavioural depres-sive equivalents into the criteria for the diagnosis ofdepression in people with ID (Marston et al. )and for the characterization of behaviours as poten-tial indicators of underlying psychopathology(Holland & Koot ).
The present retrospective study was undertakenin an attempt to further clarify these suggestions.
Materials and methods
The psychiatric reports, rating scales and notes gen-erated by contacts (i.e. initial evaluation andfollow-up visits) with people with ID who wereevaluated and treated by the present author in adevelopmental centre from to werereviewed.
The information was collected by: () a review ofeach person’s chart; () an interview in person orby telephone with the parents, when available; ()– h of information-gathering from each person’streatment team; () a behaviour problem profilethat was completed during a meeting with teammembers; () follow-up visits and discussion withteam members; () a mental status examinationduring visits; and () behavioural observationsduring visits.
The following criteria were used to select caseswith a depressive disorder: () a diagnosis ofdepression according to DSM-III-R criteria wasmade in the initial evaluation or was clarified in thefollow-up visit; () the person responded to treat-ment in that the signs and symptoms of depressionwere reversed when antidepressants were prescribedalone or in combination with other psychotropics;() the person’s age was between and years;() signs/symptoms of dementia were not reportedor observed; and () the person was seen at leastonce for follow-up visits. Most people were seenmore than once. On the basis of these criteria,
cases were chosen for inclusion in the presentstudy.
Most of the subjects were evaluated duringdepressive episodes of unipolar, bipolar I or bipolarII disorder, and only six out of the subjects wereseen during their first depressive episode (at leastthe first documented one).
Each subject was observed in her or his resi-dence, workshop, or programme more than once.Verbal and non-verbal interaction took placebetween the person and the present author beforethe diagnosis was clarified. The person was viewedfrom a ‘longitudinal perspective’ (Sovner & Hurley).
The Marston Symptoms Checklist (Marstonet al. ) was completed for each case on the basis of the psychiatrist’s notes at the time the people were suffering from untreated depression.
Results
Out of the cases selected, nine were males and were females. Their ages ranged from to years, with a mean age of . years. Three subjects had mild ID, four had moderate ID, ninehad severe ID and six had profound ID. The aetiol-ogy of the ID of subjects was unknown. Thedocumented aetiologies of the ID of the remainingseven subjects were encephalitis (n = ), cerebralpalsy (n = ), Down’s syndrome (n = ), meningitis(n = ), microcephaly (n = ) and prematurity(n = ). The confirmed diagnoses according toDSM–III-R criteria for the subjects are shown inTable .
Journal of Intellectual Disability Research
J. A. Tsiouris • Diagnosis of depression116
© Blackwell Science Ltd, Journal of Intellectual Disability Research , –
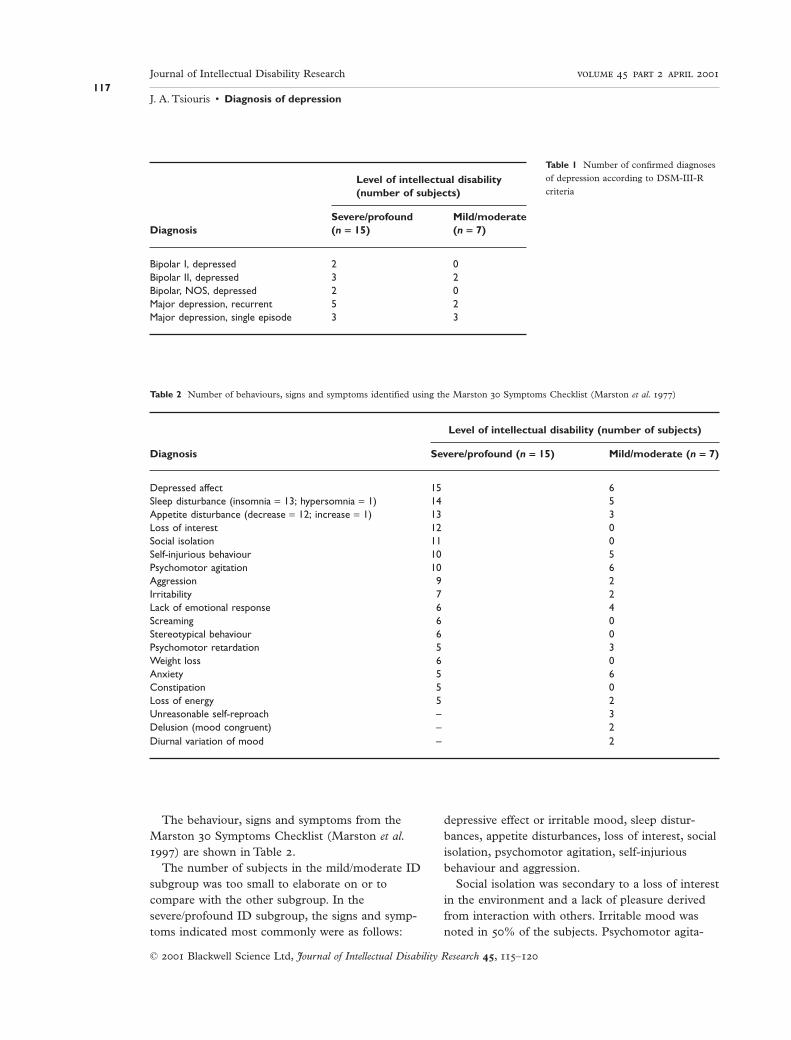
The behaviour, signs and symptoms from theMarston Symptoms Checklist (Marston et al.) are shown in Table .
The number of subjects in the mild/moderate IDsubgroup was too small to elaborate on or tocompare with the other subgroup. In thesevere/profound ID subgroup, the signs and symp-toms indicated most commonly were as follows:
depressive effect or irritable mood, sleep distur-bances, appetite disturbances, loss of interest, socialisolation, psychomotor agitation, self-injuriousbehaviour and aggression.
Social isolation was secondary to a loss of interestin the environment and a lack of pleasure derivedfrom interaction with others. Irritable mood wasnoted in % of the subjects. Psychomotor agita-
Journal of Intellectual Disability Research
J. A. Tsiouris • Diagnosis of depression117
© Blackwell Science Ltd, Journal of Intellectual Disability Research , –
Level of intellectual disability(number of subjects)
Severe/profound Mild/moderateDiagnosis (n = 15) (n = 7)
Bipolar I, depressed 2 0Bipolar II, depressed 3 2Bipolar, NOS, depressed 2 0Major depression, recurrent 5 2Major depression, single episode 3 3
Table 1 Number of confirmed diagnoses
of depression according to DSM-III-R
criteria
Table 2 Number of behaviours, signs and symptoms identified using the Marston Symptoms Checklist (Marston et al. )
Level of intellectual disability (number of subjects)
Diagnosis Severe/profound (n = 15) Mild/moderate (n = 7)
Depressed affect 15 6Sleep disturbance (insomnia = 13; hypersomnia = 1) 14 5Appetite disturbance (decrease = 12; increase = 1) 13 3Loss of interest 12 0Social isolation 11 0Self-injurious behaviour 10 5Psychomotor agitation 10 6Aggression 9 2Irritability 7 2Lack of emotional response 6 4Screaming 6 0Stereotypical behaviour 6 0Psychomotor retardation 5 3Weight loss 6 0Anxiety 5 6Constipation 5 0Loss of energy 5 2Unreasonable self-reproach – 3Delusion (mood congruent) – 2Diurnal variation of mood – 2

tion was twice as common as the psychomotorretardation noted in five cases in which loss ofenergy was noted. Psychomotor agitation was per-ceived by staff as the person having a lot of energy.Self-injurious behaviour indicated in cases as theexacerbation and increased severity of an existingbehaviour or the re-emergence of an old pattern.In a few cases diagnosed with bipolar I disorder,self-injurious behaviour was indicated during thedepressed phase and aggressive behaviour duringthe hypomanic/manic phase, as reported by Lowry& Sovner ().
Aggression was indicated in nine cases and wasmainly mild and defensive in nature. Usually, it wasdirected towards noisy consumers who invaded theisolation of others. It was also directed at staff whourged individuals to do different chores, to getready for their programme in the morning or toparticipate in activities which they had previouslyenjoyed.
Screaming and stereotypies were mostly part ofthe long-standing behavioural repertoire, especiallyin those diagnosed with autistic disorder. Weightloss was indicated in only six cases, althoughdecreased appetite was found in cases. This isexplained by the extra time caretakers spent feedingpeople lacking appetite, or by the extra food andfood supplements ordered by a dietitian when lossof weight was noted. In one case, in which anincrease in appetite and weight as well as hyper-somnia was noted, thyroid function tests revealedhypothyroidism as the cause of depressive sympto-matology. All of the symptoms were reversed upontreatment of the hypothyroidism.
Discussion
For more than weeks, all of the subjects in thesubgroup with severe/profound ID had at least fiveof the following six observable DSM-IV (APA) criteria for a diagnosis of major depression:() depressive affect/irritable mood; () sleep distur-bance; () appetite disturbance/weight loss or gain;() social isolation/loss of interest; () psychomotorretardation/agitation; and () loss of energy/fatigue.
‘Behavioural depressive equivalent’ (i.e. self-injurious behaviour and aggression) was present intwo-thirds of the people with severe/profound ID.
Self-injurious behaviour is a common behaviour inadults with Down’s syndrome and depressive dis-order (Burt et al. ). In the subgroup of sevensubjects with mild/moderate levels of ID, behav-ioural depressive equivalents appeared as commonsymptoms, but three of these subjects were diag-nosed with depression, single episode, mild to mod-erate with atypical features.
The above findings are in agreement with thefindings of a retrospective study by Myers ,who evaluated most of the cases reported, and withthe findings of Pawlarcyzk & Beckwith () andCharlot et al. (). In the latter two studies, theDSM-III and DSM-III-R criteria, respectively, wereapplied to the information found in the reportedcases or obtained from information on cases diag-nosed by others over the previous year. Although‘behavioural depression equivalent’ was prominentin the present study, as in the studies by Meins() and Marston et al. (), it was indicatedalong with the six basic observable criteria ofDSM-IV and did not replace them.
Sleep and appetite disturbances, and changes inthe level of activity have been found to be markersfor depression in people with severe/profound ID(Charlot et al. ). A study by Brody et al. ()of people without ID reported that three out of thefour main characteristics of the nine DSM-IV cri-teria (checked as positive in a questionnaire givento patients in family practice settings) identified% of people with depressive disorders, whichwere diagnosed later on with the use of researchdiagnostic criteria. The four characteristics includedsleep and appetite disturbances, anhedonia (i.e. lackof pleasure and loss of interest) and low self-esteem(i.e. low energy and feeling insecure), suggestingthat these four criteria are the core diagnostic cri-teria for depressive disorders. Agitation, rather thanlow energy and psychomotor retardation, was notedmore often in people with depression andsevere/profound ID than in people without ID.
The present study has shown that the first sixobservable criteria of DSM-III-R, including irri-table mood, which has been added to the DSM-IVfor diagnosing major depression in children and isused for adults with ID when the ‘developmentalperspective’ is used (Charlot et al. ), were suffi-cient for diagnosing major depression in peoplewith severe/profound ID.
Journal of Intellectual Disability Research
J. A. Tsiouris • Diagnosis of depression118
© Blackwell Science Ltd, Journal of Intellectual Disability Research , –

The depressive equivalents can be used as criticalbehaviours or potential indicators to alert cliniciansof the possibility of underlying depressive disorders,but not as core characteristics of depression. It isalso possible that depressive equivalents are moreprominent in people with severe to profound ID in whom the degree of depression is not severe.Another possibility is that, in cases of depressivedisorder with atypical features or depressive disor-der, not otherwise specified (NOS), the clinical presentation is different from that in clear cases ofmajor depression with melancholic features of mod-erate to severe degree. Behavioural equivalents canalso be used for monitoring treatment progress,but only after the diagnosis has been made usingDSM-IV criteria.
A limitation of the present study is that it wasretrospective. The methods used for original diag-noses, data collection and current study selectionminimize the possibility of bias. The cases wereselected for inclusion in the present study only afterthe diagnosis of depression was certain. Cases withcharacteristics of comorbid anxiety disorders whichrespond to treatment with antidepressants wereexcluded. Future prospective studies will betterdefine the presentation of depression in people withsevere/profound ID, although the problem of cir-cuitous reasoning cannot be avoided in such studieswithout an independent biological marker ofdepression.
Acknowledgements
This study was supported by the New York StateOffice of Mental Retardation and DevelopmentalDisabilities.
Grateful appreciation is extended to ValerieMazza for her contribution in typing this article forpublication and to Maureen Marlow for assistancein editing.
References
American Psychiatric Association (APA) () Diagnosticand Statistical Manual of Mental Disorders, rd edn.American Psychiatric Association, Washington, DC.
American Psychiatric Association (APA) () Diagnosticand Statistical Manual of Mental Disorders, rd edn –
Revised. American Psychiatric Association, Washington,DC.
American Psychiatric Association (APA) () Diagnosticand Statistical Manual of Mental Disorders, th edn.American Psychiatric Association, Washington, DC.
Berman M. I. () Mental retardation and depression.Mental Retardation , –.
Borshwick-Duffy S. A. () Epidemiology and preva-lence of psychopathology in people with mental retarda-tion. Journal of Consulting and Clinical Psychology ,–.
Brody D. S., Hahn S. R., Spitzer R. L., Kroenke K.,Linzer M., deGruy F. V. & Williams J. B. () Identifying patients with depression in the primary care setting. Archives of Internal Medicine , –.
Burt D. B., Loveland K. A. & Lewis K. R. () Depres-sion and the onset of dementia in adults with mentalretardation. American Journal on Mental Retardation ,–.
Campbell M. & Malone R. P. () Mental retardationand psychiatric disorders. Hospital and Community Psychiatry , –.
Charlot L. R., Doucette A. C. & Mezzacappa E. ()Affective symptoms of institutionalized adults withmental retardation. American Journal on Mental Retardation , –.
Holland A. J. & Koot H. M. () Mental health andintellectual disability: an international perspective.Journal of Intellectual Disability Research , –.
Holmes N., Shan A. & Wing L. () The DisabilityAssessment Schedule: a brief screening device for usewith the mentally retarded. Psychological Medicine ,–.
Lowry M. A. & Sovner R. () Severe problems associ-ated with rapid cycling bipolar disorder in two adultswith profound mental retardation. Journal of IntellectualDisability Research , –.
Marston G. W., Perry D. W. & Roy A. () Manifesta-tions of depression in people with intellectual disability.Journal of Intellectual Disability Research , –.
Meins W. () Symptoms of major depression in mentally retarded adults. Journal of Intellectual DisabilityResearch , –.
Myers B. A. () Major depression in persons withmoderate to profound mental retardation: clinical pre-sentation and case illustrations. Mental Health Aspects ofDevelopmental Disabilities , –.
Pawlarcyzk D. & Beckwith B. E. () Depressive symptoms displayed by persons with mental retardation:a review. Mental Retardation , –.
Prout H. T. & Schaefer B. M. () Self reports ofdepression by community-based mentally retarded
Journal of Intellectual Disability Research
J. A. Tsiouris • Diagnosis of depression119
© Blackwell Science Ltd, Journal of Intellectual Disability Research , –

adults. American Journal of Mental Deficiency ,–.
Reid A. H. () Psychoses in adult mental defectives: aclinical and psychological study. British Journal of Psychiatry , –.
Reiss S. & Trenn E. () Consumer demand for out-patient mental health services for mentally retardedpeople. Mental Retardation , –.
Sovner R. & Hurley A. () Do the mentally retardedsuffer from affective illness? Archives of General Psychia-try , –.
Sovner R. & Lowry M. () A behavioral methodologyfor diagnosing affective disorders in individuals withmental retardation. Habilitative Mental HealthcareNewsletter , –.
Szymanski L. S. & Biederman J. () Depression andanorexia nervosa of persons with Down syndrome.American Journal of Mental Deficiency , –.
Tsiouris J. A. & Patti P. J. () Drug treatment ofdepression associated with dementia or presented aspseudodementia in older adults with Down syndrome.Journal of Applied Research in Intellectual Disabilities ,–.
World Health Organization (WHO) () The Interna-tional Classification of Mental and Behaviour Disorders –Clinical Descriptions and Diagnostic Guidelines, th Revi-sion (ICD-). World Health Organization, Geneva.
Received January ; revised November
Journal of Intellectual Disability Research
J. A. Tsiouris • Diagnosis of depression120
© Blackwell Science Ltd, Journal of Intellectual Disability Research , –