Embed Size (px)
Citation preview

Diagnosis Dementia:Diagnosis, Assessment, and
Referral
Soo Borson MDUniversity of Washington
Department of Psychiatry and Behavioral Sciences, School of Medicine
Department of Psychosocial and Community Health, School of Nursing

Hebert et al. Neurology 2004
New Cases of Alzheimer’s Disease

National Priorities for Dementia Care
• Detect cognitive impairment • Diagnose dementia when it’s present
– Dementia is… • A medical problem caused by specific disease processes,
and a target for medical treatment• A risk factor for other problems, and a modifier of other
conditions and treatments• A (usually) progressive condition with changing, stage-
specific problems and needs
• Provide dementia-specific, relevant, proactive , and comprehensive patient care

The Broad Impact of Dementia
• Health care– Delirium (OR 3.96, 95% CI 1.1-14.2) 1 – Low health literacy/adherence to pre-op instructions (OR
4.0, 95% CI 1.6-9.8) 2
– Med management deficits3
– More hospitalizations for ambulatory care sensitive conditions (OR 1.8, p < 0.0001)4
• Public safety– Driving risk 5
• At home, in the community– Need for everyday support and assistance 6
1. Alagiakrishnan et al. JAGS 2007. 2. Chew et al. Am J Surg 2004. 3. Lakey et al. Ann Pharmacother 2009. 4. Phelan et al (in prep). 5. AMA Driver Guide, http://www.ama-assn.org/ama/pub 6. Scanlan et al. Am J Geriatr Psychiatry 2007
© 3-11 Soo Borson MD

New Opportunities for Detecting Dementia in Primary Care
• The Medicare Annual Wellness Visit– New benefit - January 2011– Voluntary for patients and providers– No patient co-pay; Level 4 E/M for provider– Two assessment components
• Cognitive checkup – objective assessment• Health risk assessment
• One key goal: personal prevention plan• Missed opportunity
– Only 3-4% of seniors used the benefit in 1st half of 2012

Cognitive Assessment in the Annual Wellness Visit
• Many approaches– Ask the patient about problems with memory
or needing help to do things that used to be easy (e.g. paying bills)
– Ask someone else who knows the patient well– Give a screening test
• Some health care systems have adopted routine, systematic screening– Simple, uniform, quality control possible

1) GET THE PATIENT’S ATTENTION, THEN SAY: “I am going to say three words that I want you to remember. The words are:
Banana Sunrise Chair
Please say them for me now.” (Give the patient 3 tries to repeat the words. If unable after 3 tries, go to next item.)(Fold this page back at the TWO dotted lines BELOW to make a blank space and cover the memory words. Hand the patient a pencil/pen).
2)SAY ALL THE FOLLOWING PHRASES IN THE ORDER INDICATED: “Please draw a clock (provide paper, pencil). Start by drawing a large circle.” (When this is done, say) “Put all the numbers in the circle.” (When done, say) “Now set the hands to show 11:10 (10 past 11).”
SAY: “What were the three words I asked you to remember?”
___________________ ___________________ ____________________ (Score 1 point for each) 3-Item Recall Score
Score the clock (see other side for instructions): Normal clock 2 points Clock Score Abnormal clock 0 points
TOTAL SCORE = 3-ITEM RECALL PLUS CLOCK SCORE
Total score of 0, 1, or 2 possible impairment; 3, 4, or 5 suggests no impairment.
Case Study: Mini –Cog™
Mini-Cog™. Copyright Soo Borson MD All rights reserved.
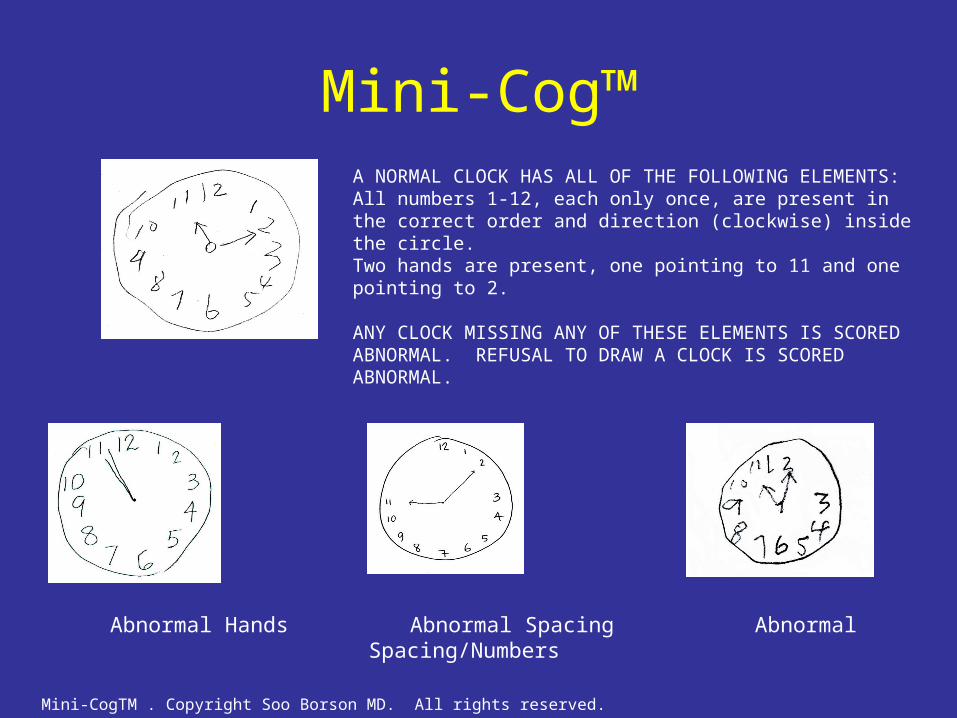
Mini-Cog™
A NORMAL CLOCK HAS ALL OF THE FOLLOWING ELEMENTS:All numbers 1-12, each only once, are present in the correct order and direction (clockwise) inside the circle.Two hands are present, one pointing to 11 and one pointing to 2. ANY CLOCK MISSING ANY OF THESE ELEMENTS IS SCORED ABNORMAL. REFUSAL TO DRAW A CLOCK IS SCORED ABNORMAL.
Abnormal Hands Abnormal Spacing Abnormal Spacing/Numbers
Mini-CogTM . Copyright Soo Borson MD. All rights reserved.

Detecting Dementia with the Mini-Cog™
94(41%)194 (84%)231Total
4 (6) **39 (55)71 (32)Mild Cognitive Impairment
5 (45) *9 (82)11 (6) Other dementia types
6 (40) **15 (100)15 (6) Vascular dementia
15 (56) *20 (91)22 (10) AD + vascular
69 (62) **111 (99)112 (47)Dementias
Probable AD
byPhysicians
byMini-Cog
Total N(%‡)
Diagnosis
Recognition Rate, N (%)
Borson et al. Int J Geriatric Psychiatry 2006* p < 0.05; ** p < 0.01

Moving from Screening to Diagnosis
• Screening for cognitive impairment – Identifies the majority of patients with
dementia– Cannot diagnose dementia or its cause
• Diagnostic assessment appropriate after– Positive screen– Negative screen but high clinical suspicion
Components of the Diagnostic Workup
• Thorough medical and family history• Mental status testing• Physical and neurological examination• Laboratory examination
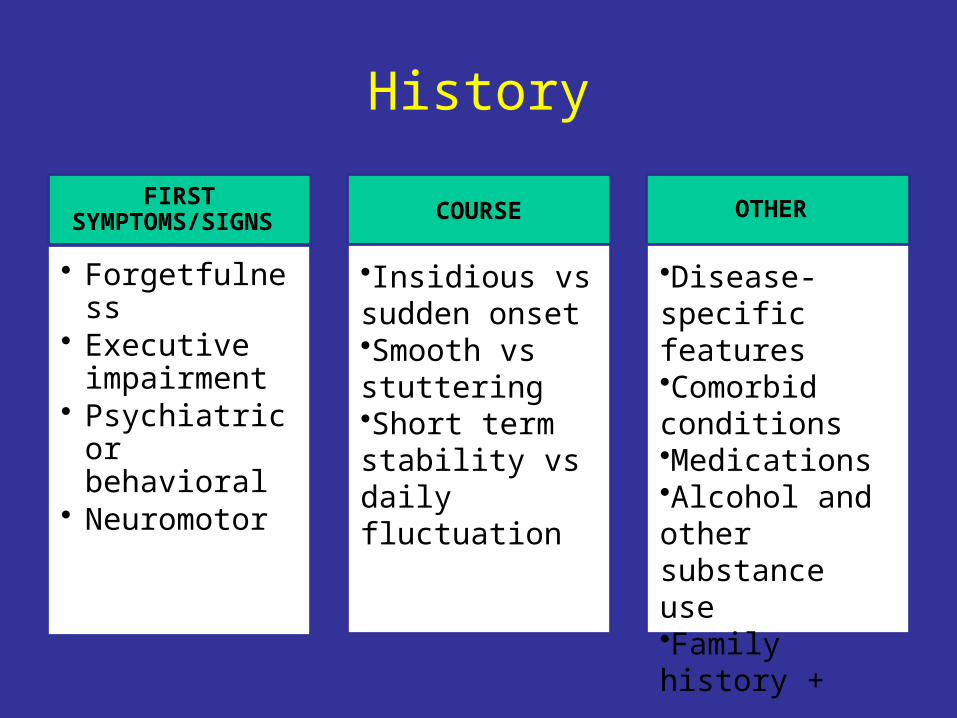
History
FIRST SYMPTOMS/SIGNS
• Forgetfulness• Executive
impairment• Psychiatric or
behavioral• Neuromotor
COURSE
•Insidious vs sudden onset•Smooth vs stuttering•Short term stability vs daily fluctuation
OTHER
•Disease-specific features•Comorbid conditions•Medications•Alcohol and other substance use•Family history +

Mental Status Testing• To establish presence of cognitive disorder
– Comparison with• Patient’s prior cognitive level • Normative expectations for the person
– Two or more core cognitive abilities affected• Memory and learning• Executive abilities• Language, cognitive control of motor acts, recognition of
objects, people• Visuospatial functions, navigation
– Everyday life affected by deficits
• To look for non-dementia causes, e.g. depression

Clinical Differential Diagnosis
Dementia present
Neuro exam normal
AD FTD
Neuro exam abnormal
VaD
PDD, ‘Park+’
DLB

Diagnostic Testing
• Routine “rule out” labs• Psychometric testing• Structural and functional neuroimaging
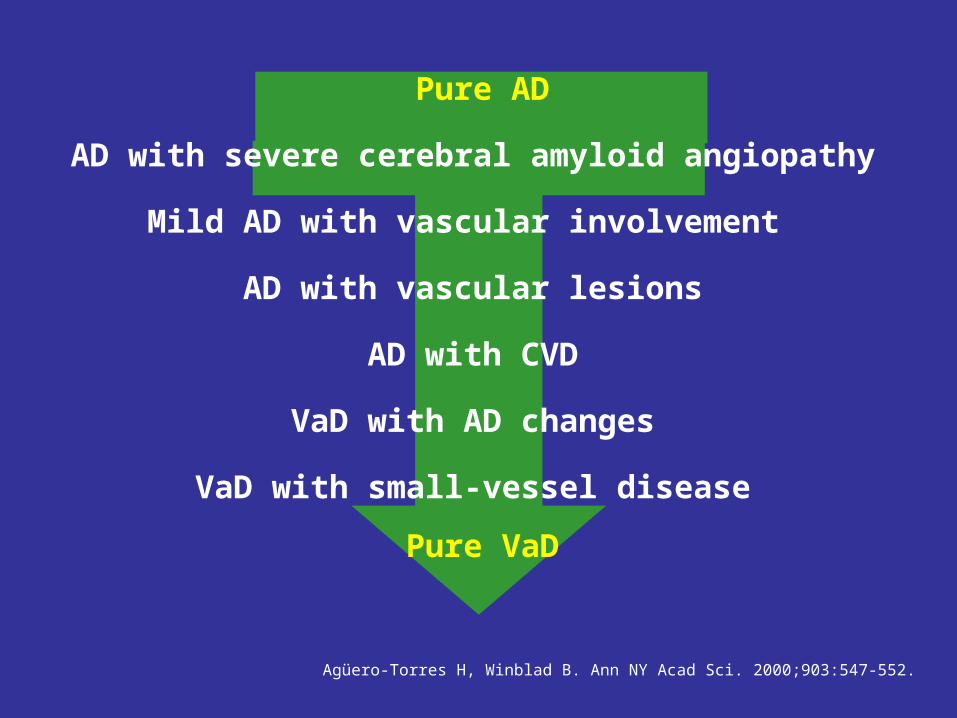
Pure AD
AD with severe cerebral amyloid angiopathy
Mild AD with vascular involvement
AD with vascular lesions
AD with CVD
VaD with AD changes
VaD with small-vessel disease
Pure VaD
Agüero-Torres H, Winblad B. Ann NY Acad Sci. 2000;903:547-552.

Common Patterns of Ischemic Vascular Dementia
Courtesy of T. Erkinjuntti.
Cortico-subcorticaloccipito-temporal infarct
Thalamic infarct
Cortical Strategic
Lacunar infarcts predominateWhite matter lesions predominate
Subcortical White Matter Subcortical Lacunar

DIAGNOSIS MRI SPECT/PET
Alzheimer Disease Med temporal, parietal atrophy; later, diffuse atrophy and ventricular enlargement
Parietotemporal assoc cortex, posterior cingulate; sensorimotor preservation
Frontotemporal Dementia
Frontal and/or lateral temporal atrophy
Prefrontal and temporal
Dementia with Lewy Bodies
Hippocampus, medial temporal preserved; putamen
atrophy
Parietotemporal plus occipital
Vascular Dementia Bilateral micro and/or macrovascular disease, no
set pattern
Asymmetric cortical, subcortical, cerebellar;
watershed; crossed cerebellar diaschisis;
lateralized hemispheric deficit

Pure AD
CONVENTIONAL SPECT IMAGES
3D – SSP PROCESSED IMAGES

Pure AD
FUSED MRI/SPECT IMAGES

AD + Vascular Disease


Lewy Body Dementia

Contribution of Combined MRI/SPECT to Diagnosis
• Findings significant for diagnosis in 78.5%• Pre-imaging diagnosis of neurodegenerative disease
rejected by imaging in 2.5%• Vascular component identified in 41 patients (51% of
sample)– 30% exclusively vascular – 53% AD + vascular– 7% FTD + vascular
• Imaging most helpful:– When diagnosis is difficult due to atypical features– To test clinical impression– To clarify complex etiologies
Research and Clinical Trials
• CSF biomarkers as indicators of AD risk– Amyloid beta , Tau
• Novel PET imaging compounds– FDA approval of amyloid imaging agents
• Not currently approved for clinical diagnostic use
• Genetic testing• Preclinical diagnosis of AD

Clinical Trials
• Primary pathway to therapeutic progress• Depend on referrals from practicing
physicians and other providers• You can help!
– Check out Alzheimer’s Association Trial Match
http://www.alz.org/research/clinical_trials/find_clinical_trials_trialmatch.asp

Specialist Referrals• Neuropsychologist (psychometric testing)
– Very mild impairment in highly intelligent persons– Atypical cognitive impairment mixed with psychiatric symptoms– Medicolegal indications (e.g. medical disability determinations)
• Neurologist– Difficult differential diagnosis– Rare disease suspected, e.g. CJD, NPH
• Geriatric psychiatrist– Difficult neurobehavioral problems– Ongoing management of patient + family
• Geriatrician– Frailty, falls
• Social worker– Care planning, caregiver support and community resources
• Psychologist– Psychotherapy for family members

An Integrative Framework for Dementia Care
Patient and Family
Care Partner
Differential Diagnosis
and
Staging
Neuropsychiatric Symptom Assessment & Management
Medical Comorbidity, Safety and Risk Management
Caregiver Assessment, Counseling,
Services, and Planning © 2008 Soo Borson MD

Evaluating the Quality of Dementia Care:New Measures
• AMA PCPI with AAN, AGS, AMDA, APA/AAGP, Alz Assoc, others• 10 quality measures, grouped into key domains
– Dementia assessment: cognition, stage, everyday functional deficits
– Screening for depressive symptoms– Neuropsychiatric symptom assessment and
management– Counseling about safety (falls, medications) and
driving– Comprehensive advance care planning and end of life
counseling– Caregiver education and support