Embed Size (px)
Citation preview

BACKGROUNDPeriodontitis in children is a rare occurrence, but pediatric dentists should be equipped with the knowledge of proper diagnosis and management. In 2017, the American Academy of Periodontology (AAP) updated the disease classification of periodontitis to group former diagnoses that share similar pathophysiology. Understanding of the patient’s medical history, clinical and radiographic presentation, and disease course are vital to the management of the child with periodontitis. This case report details the diagnosis and treatment planning of a young female with stage IV grade C periodontitis using evidence-based guidelines.
REFERRAL AND BIOPSYPeriodontal disease in children is divided into the following categories: Periodontal Health, Gingivitis- dental plaque induced, Gingival disease-non dental plaque induced, and Periodontitis. This patient has bone loss and clinical attachment loss eliminating periodontal health and gingivitis from the differential list. The patient has no systemic factors eliminating clinical manifestation of systemic conditions or gingival disease-non dental plaque induced as well. Periodontitis is further divided into periodontitis or Necrotizing Ulcerative Periodontitis (NUP). The patient’s symptoms were not consistent with NUP, so patient has clinical diagnosis of Periodontitis (formerly localized aggressive periodontitis). Using the AAP disease classification, the patient's complete diagnosis is:• Stage IV: due to CAL>= to 5mm and radiographic bone loss extending to mid-third of root
or beyond• Grade C: %bone loss/age > 1.0, destruction exceeds expectation given biofilm deposits
and early onset1
TREATMENT OPTIONSFor Stage IV Grade C periodontitis, the main treatment options are :1. Scaling and root planing with periodic maintenance and effective daily plaque control2. Extraction of affected primary teeth The following are not indicated for this case: Local antibiotic delivery • Does not provided superior results to
scaling and root planning• “defined, but limited, beneficial response”
usually reserved for a few localized persistent lesions 3
Surgical intervention• Indicated to provide better access for
removal of plaque, reduce probing depths, regenerate tissue2
Systemic antibiotics• Indicated as an adjunctive therapy when
“multiple sites are unresponsive to mechanical debridement, acute infections, medically compromised individual, tissue-invasive organisms, ongoing disease progression”2
• Unnecessary to routinely administer antibiotics, NSAIDS or sub antimicrobial doses of doxycline2
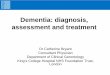
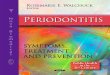
CLINICAL PRESENTATIONA five-year-old female with an unremarkable medical history presented in June of 2018 with poor oral hygiene and visible gingival recession associated with the labial of #N-Q, approximately 2-3mm. Patient had dental treatment in the OR in October of 2018 with similar clinical findings noted. In July 2019 patient presented with 3 to 4 mm of recession along the buccal marginal gingiva including teeth #M, N, O, P, Q, and R. Teeth #M, N, O, P, Q, and R exhibited class I mobility. Very little plaque and calculus present on clinical exam. Patient returned to clinic in October of 2020 with 5mm of clinical attachment loss on the facial of #N-Q and 1mm recession noted on #M and R. There was class II mobility on #O and P and class I mobility on #M,N,Q,R. The interdental papilla between #O and P gingiva had a fibrin coating appearance due to patient habit of picking at the area.
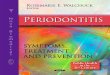
RADIOGRAPHIC INTERPRETATIONLower occlusal radiographs taken periodically and reveal horizontal and vertical bone loss extending to the apical 1/3 of the root in the mandibular anterior region. Posterior bitewings taken at same intervals reveal no bone loss in the posterior region.
REFERENCES1. Council O. Classification of Periodontal Diseases in Infants, Children, Adolescents, and Individuals with Special Health Care Needs. Journal of Periodontology (Table 1). 2018;6:28.2. Research, Science and Therapy Committee Guidelines of the American Academy of Periodontology. Treatment of Plaque-induced Gingivitis, Chronic Periodontitis, and Other Clinical Conditions. J Periodontol 2001;72:1790-1800.3.Position Paper: The Role of Controlled Drug Delivery for Periodontitis. J Periodontol. 2000 Jan;71(1):125-140. doi: 10.1902/jop.2000.71.1.125. PMID: 29537535.
Diagnosis and Treatment Planning of Periodontitis in the Child Patient
Lauren White, DDS• Juan F. Yepes, DDS, MD, DrPH, MS Indiana University School of Dentistry, Indianapolis, Indiana – Riley Hospital for Children
June 2018 October 2020
June 2018 October 2018 July 2019
October 2020