-
8/8/2019 Diagnosis and Treatment of Metabolic Syndrome in
Menopausal Women
1/12
MM
16 MENOPAUSEMANAGEMENT
The Controversy
A diagnosis of metabolic syndromehas been the subject of
controversy.
This controversy has several facets.4-7
There are multiple definitions ofmetabolic syndrome, which has
ledto some confusion as to whether ornot the syndrome describes an
actualbiological entity or whether it issimply a construct. Small
changes in
the cut points used in the definitionof metabolic syndrome will
likelyimpact its specificity and sensitivityin the prediction of
cardiovascularrisk. Some have questioned whetheror not the risk of
atheroscleroticcardiovascular disease (ASCVD) as-sociated with
metabolic syndrome isgreater than that of the sum of itsrisk
factors. However, the risk of
ASCVD rises geometrically rather
than linearly with the addition ofmetabolic syndrome risk
factors,and the increased incidence of type2 diabetes mellitus
(T2DM) addi-tionally increases long-term risk.3
There is also controversy concerningthe clinical utility of the
metabolicsyndrome, as no prospective trials
yet exist demonstrating that the di-agnosis of the metabolic
syndromeand implementation of specific ther-
apeutic regimens would affect the
Metabolic syndrome is a disorder of combined lipid and
glucose metabolism in a genetically susceptible individual
with sufficient visceral adiposity to provoke adipose tissue
dysfunction. This adipose tissue dysfunction also results in
hypertension, glucose intolerance, and a proinflammatory,
prothrombotic state. Physiologic features of menopause
such as decreased insulin sensitivity, estrogen deficiency,
shiftto an android body habitus and weight gain, as well as lack
of
physical activitycontribute to the development and risk of
metabolic syndrome in menopause. Age itself remains a
predominant risk factor for metabolic syndrome.
Endocrinologist Gerald Reaven, who helped to draw attention
to the metabolic syndrome concept, is quoted as having said,
All obese people are not created equalinsulin resistance is
the major determinant of cardiovascular disease in
overweight/obese individuals.1 Previously thought of as a
pre-diabetes
syndrome, metabolic syndrome is now more properly viewed as
a pre-coronary syndrome because of the associated increased
risk of cardiovascular events. Cardiovascular disease
remains
the leading cause of morbidity and mortality among
menopausal
women, and despite preventive efforts we have been less
successful in reducing this risk in women than in men.2,3
Early and accurate risk prediction and aggressive prevention
would seem to be what is needed.
Diagnosis and Treatmentof Metabolic Syndromein Menopausal
WomenGregory S. Pokrywka, MD, FACP
(continued on page 17)
-
8/8/2019 Diagnosis and Treatment of Metabolic Syndrome in
Menopausal Women
2/12
MM
NOVEMBER/DECEMBER2007 17
morbidity or mortality from ASCVDor from T2DM. (Post hocanalysis
doesreveal that patients with metabolicsyndrome derive incremental
benefitfrom intensified statin therapy8).
Regardless of whether metabolicsyndrome is ultimately
determined
to be a distinct biological entity, adiagnosis serves to
identify patientsat a two- to three-fold increased riskfor ASCVD,
who might benefitfrom more intensive lifestyle and,possibly,
pharmacologic therapy.9
The predictive value of metabolicsyndrome has generally not
beenshown it to be superior to the Fram-ingham Risk Score (FRS) in
delin-eating short-term (10-year) ASCVD
risk.
10
However, the diagnosis ofmetabolic syndrome remains astrong
predictor oflong-term coro-nary heart disease (CHD) risk
andidentifies potentially high-risk pa-tients, especially in women
over 55
years of age. A diagnosis of meta-bolic syndrome identifies
those atrisk for T2DM and stroke; the FRSdoes not. The FRS may, in
fact, se-riously underestimate lifetime car-
diovascular risk in women.
11
Thus, clinicians face a dilemmawith regard to accurate risk
predic-tion and treatment, and may need toresort to additional
tools, such asimaging studies, biomarkers and ad-
vanced lipoprotein analysis to aug-ment the FRS. However,
validationof cardiac imaging and biomarkersas tools to screen for
long-term riskin insulin-resistant states awaits
prospective trial data.12
The diag-nosis of metabolic syndrome ex-
tends the concept of CVD risk andshould not be viewed as a
competi-tor to the FRS tool, but rather asan enhancement.4
Metabolic Syndrome in Women:
What Studies Show
Although no studies have specifi-cally looked at menopausal
women,multiple studies (the San AntonioHeart Study, the
Atherosclerosis
Risk in Communities study, theHoorn study, and the Health,
Agingand Body Composition study) havesuggested that the metabolic
syn-drome may be more predictive ofCHD events in women than
inmen.13-15A recent, 10-year, prospec-tive multicenter trial in
China of ap-proximately 30,000 subjects showedthat metabolic
syndrome signifi-cantly increased CVD risk com-
pared with patients who do nothave metabolic syndrome but whodo
have hyperglycemia. The riskof CVD in this population was
largely attributable to the accom-panying metabolic
abnormalitiesof metabolic syndrome rather thanthe hyperglycemia
alone.16
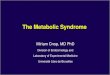
Metabolic syndrome had an ad-verse impact on CVD health
andmortality in the Botnia Study,17 aprospective 7-year trial with
morethan 3,000 patients (average age of
women, >50 years). There was a 2-to 3-fold relative risk
increase in
total mortality, CHD mortality,CHD incidence, myocardial
infarc-tion and stroke (Figure 1).17
The recently completed Monitor-ing of Trends and Determinants
inCardiovascular Disease trial18 is aprospective Danish
population-based study of 2,493 men and
women, ages 41 to 72 years, withoutmajor CVD at baseline. Over a
me-dian follow-up of 9.4 years, the rel-
ative risk (RR) of cardiovascular endpoints (CV death, nonfatal
ischemicheart disease and nonfatal stroke,adjusted for age, gender,
smoking
Figure 1. Metabolic syndrome has a negative impact on CV
healthand mortality.17
Diagnosis and Treatment of Metabolic
Syndrome in Menopausal Women
(continued from page 16)
-
8/8/2019 Diagnosis and Treatment of Metabolic Syndrome in
Menopausal Women
3/12
MM
18 MENOPAUSEMANAGEMENT
and low-density lipoprotein choles-terol [LDL-C]) was increased
by1.56 (95% confidence interval [CI],1.12 to 2.17).18 The authors
con-cluded that both insulin resistanceand metabolic syndrome, as
definedby the National Cholesterol Educa-tion Program Adult
Treatment Panel(NCEP-ATP III), independentlypredict cardiovascular
disease.
A new meta-analysis of 40 studies
varying in length from 2 to 16 yearsin 172,573 individuals,
using end-points of new heart disease events ordeath, showed
metabolic syndromehad an RR of 1.78 (95% CI, 1.58-2.00). The
association was strongerin women than in men (RR, 2.63 vs.1.98, P=
0.09.) Multivariate analy-sis adjusting for the individual
com-ponents of metabolic syndromedemonstrated cardiovascular
risk
beyond that associated with its in-dividual risk factors (RR,
1.54; 95%CI, 1.32-1.79).19
The Enlarged Waist/ElevatedTriglycerides (EWET) trial was
thefirst long-term prospective study ofmetabolic syndrome risk
factors ina community-based, menopausal-specific population.20
Rather thaninvestigating all the factors ofmetabolic syndrome as
defined by
the American Heart Association/National Heart, Lung, and
BloodInstitute (AHA/NHLBI), EWETused only the two parameters of
en-larged waist size (over 35 inches)and elevated triglycerides
(128mg/dL) in estimating cardiovascularmortality in 557 menopausal
womenages 48 to 76, who were followedprospectively for 8.5 years.
Mortality
was increased almost 5-fold by the
presence of EWET, and metabolicsyndrome risk factors other
than
elevated triglycerides and elevatedwaist added little to risk
prediction inthis model. The authors concludedthat the presence of
EWET may bethe best indicator of cardiovascularrisk in menopausal
women. Newstudies confirm that both fastingand nonfasting
triglycerides are im-portant independent risk factors
forcardiovascular events.21,22
The Role of Risk Factors
The incidence of new-onset T2DM,a CHD relative risk equivalent
inthe NCEP guidelines, correlates
with the number of characteristics,or risk factors, of metabolic
syn-drome. Patients with four or five riskfactors for metabolic
syndrome havea 24-fold greater risk for T2DMcompared with patients
who haveno risk factors.23 There is also evi-
dence that CHD risk increases withthe number of components of
meta-bolic syndrome,24 as does ischemicstroke risk (two to three
times in-creased relative risk).25 Analysis ofthe Framingham
Offspring Study(1,774 women, average age >50 years)revealed
significant increases in totalCVD and hard CVD outcomes
(my-ocardial infarction or CHD death)
with the diagnosis of metabolic
syndrome.
24
The increases in theseevents were steeper in women than inmen,
which correlated with the num-ber of metabolic syndrome risk
fac-tors present (Table 1). Increases inrelative risk of T2DM were
greaterthan increases in CVD events.
Diagnostic Criteria
The AHA/NHLBI diagnostic crite-ria for metabolic syndrome (Table
2)
are well known and are discussed indetail elsewhere.9These
criteria can
be adapted for multiethnic popula-tions; for example, by
reducing thecriterion for elevated waist circum-ference in South
Asian women. Theincidence of the metabolic syndromeincreases with
age; the prevalence ofmetabolic syndrome increased
fromapproximately 7% among partici-pants between ages 20 and 29 to
ap-proximately 43% for patients over60 years of age.26The
prevalence of
metabolic syndrome differs withrace, with the age-adjusted
preva-lence being highest among Mexican-
American individuals and lowestamong African-Americans and
peo-ple of other racial categories. Themost recent data suggest
that ap-proximately 50 million Americanshave metabolic
syndrome.
Pathophysiology
The pathophysiology of metabolicsyndrome involves
dysfunctionaladipocytes (adiposopathy). Adipo-sopathy is defined as
pathologicadipose tissue dysfunction that maybe initiated and/or
exacerbated byfat accumulation in genetically sus-ceptible
patients.27 Increased vis-ceral adipose tissue dysfunctionoften
correlates with the amount of
visceral adipose tissue and also with
an increased number of metabolicsyndrome components (score).The
Womens Ischemia SyndromeEvaluation (WISE) study demon-strated the
importance of where amenopausal womans body fat ismainly
located.28The odds ratio ofsignificant coronary artery diseaseby
angiography was related to thepresence or absence of
metabolicsyndrome at any weight, even in the
absence of obesity. The relative risk ofmortality and CVD events
was more
-
8/8/2019 Diagnosis and Treatment of Metabolic Syndrome in
Menopausal Women
4/12
MM
NOVEMBER/DECEMBER2007 19
closely related to metabolic syndromethan to body mass index
(BMI).
Many patients have a geneticallyimpaired inability to make new
adi-pose cells (adipogenesis) under con-ditions of positive caloric
balance,resulting in adipose cell hypertro-phy and resultant
hypoxic-inducedstress. These stressed adipocytesrelease pathologic
adipocytokines,lipotoxic nonesterified free fatty
acids (NEFAs) and other pro-inflammatory factors that
promoteendothelial dysfunction, increaseinsulin resistance and
increase CVDrisk. Adiposopathy reduces the ben-eficial cytokine
adiponectin, whichhas a number of anti-atheroscleroticeffects on
the vasculature, promotesinsulin sensitivity, and has beenstrongly
linked to reduction of car-diovascular risk.27
Clinical diagnosis of metabolicsyndrome is an excellent way
toidentify the increased CVD risk ofadiposopathy and the
associatedatherogenic triada cluster of non-traditional risk
factors that confersa dramatic increase in CVD risk:
hyperinsulinemia, small, dense LDL particles, and an elevated
number of athero-
genic ApoB lipoprotein particles.
The risk of ischemic heart dis-ease is differentially increased
ac-cording to the cumulative numberof traditional and
nontraditionalrisk factors. The presence of theatherogenic triad
confers an almost21-fold increased relative risk overpatients in a
similar quartile of tra-ditional risk factors.29
The NCEP-ATP III 2004 ad-
dendum guidelines recommendclassification of risk according
to
the presence of major risk factors(family history of premature
CVD,low high-density lipoprotein cho-lesterol [HDL-C], age,
smokinghistory and hypertension) and theFRS. Intensity of treatment
of plasmalipid concentrations is directly pro-portional to the risk
predicted by
this algorithm.30
However, there aredistinct advantages in shifting the
emphasis from a lipid-concentra-tion risk management strategy
toa lipoprotein-concentration riskmanagement
strategy.31,32Although
we have traditionally used plasmalipid (cholesterol and
triglyceride)concentrations as determined bythe standard lipid
panel (total-
cholesterol, LDL-C, HDL-C, verylow-density lipoprotein
cholesterol
Table 2. National Cholesterol Education Program9
Adult Treatment Panel III (NCEP-ATP III)
Metabolic Syndrome diagnosis suggested by the presence of 3 or
more of the
following features:
1. Waist >35 inches in women ( >31 inches in South
Asians)
2. Triglycerides >150 mg/dL (or on drug treatment with a
fibrate or niacin for elevated TG)
3. HDL-C 100 mg/dL (or on drug treatment for elevated
glucose)
TG = triglycerides; DBP = diastolic blood pressure; HDL-C =
high-density lipoprotein cholesterol;
SBP = systolic blood pressure
EventNo. of Metabolic
Syndrome Risk Factors
Age-Adjusted Relative Risk (95% CI)
Men Women
CVD 0 Referent Referent
12 1.48 (0.693.16) 3.39 (1.318.81)
3 3.99 (1.898.41) 5.95 (2.2016.11)
Hard CVD 0 Referent Referent
12 0.98 (0.362.67) 3.77 (0.4531.28)
3 2.55 (0.966.79) 7.21 (0.8164.37)
Total CHD 0 Referent Referent
12 1.24 (0.542.83) 3.29 (0.9511.34)
3 3.01 (1.336.83) 3.96 (1.0215.38)
T2DM 0 Referent Referent
12 4.16 (0.9817.64) 6.10 (1.8520.10)
3 23.83 (5.8098.01) 29.69 (9.1096.85)
Table 1. Metabolic Syndrome Components and CV RiskA Greater
Number of Metabolic Syndrome Components Leads to Greater Risk
for CV Events: Framingham Offspring Study 8-Year Follow-Up
CVD = cardiovascular disease; CHD = coronary heart disease; T2DM
= type 2 diabetes mellitus
Wilson PWF, et al. Circulation 2005;112:3066-3072. Reprinted
with permission of Lippincott Williams & Wilkins.
-
8/8/2019 Diagnosis and Treatment of Metabolic Syndrome in
Menopausal Women
5/12
MM
20 MENOPAUSEMANAGEMENT
[VLDL-C] and triglycerides), it isnow well established from
epidemi-ologic and clinical trials that, infact, CVD risk tracks
more closely
with plasma lipoprotein concentra-tions.31,32 This is especially
true ininsulin-resistant populations.
Plasma lipoprotein concentra-tions are better than any of
theplasma cholesterol indices at assess-ing residual risk patients
experience
after theyve begun treatment.Apolipoprotein B is a surface
pro-tein component of atherogeniclipoproteins (LDL, VLDL,
inter-mediate density lipoproteins andremnant particles). Each of
theselipoproteins contains a single mole-cule of ApoB.
Cardiovascular risk isincreased by an increased ApoB par-ticle
concentration. ApoB determi-nation is simple, standardized and
directly measured (unlike LDL-C,which is a calculated value). An
eas-ily calculated non-HDL-C value(total-cholesterol concentration
mi-nus the HDL-cholesterol concen-tration) serves as an
alternative
validated tool for assessment of riskfrom all circulating ApoB
parti-cles.33 LDL particle concentration(LDL-P) determined by
nuclearmagnetic resonance imaging is an
alternative method for determiningplasma lipoprotein
concentration-associated risk.34
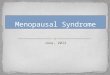
The lipoprotein abnormalities ofmetabolic syndrome are an
exces-sive number of atherogenic ApoBlipoprotein particles,
accompaniedby reduced numbers, as well as dys-function, of HDL
particles (Figure2). Under conditions of adiposopa-thy, visceral
fat cells are unable to
properly control and store NEFAs.35
When the liver is confronted with an
excessive concentration of NEFAs(and/or when augmented by an
ex-cessive simple carbohydrate diet),triglyceride synthesis is
initiated.
The liver is not adapted to handlean excessive load of
triglycerides.Hypertriglyceridemic situations likemetabolic
syndrome lead to an over-production of large triglyceride-rich
ApoB-containing VLDLs, whichare associated with fasting and
postprandial hypertriglyceridemia.Triglyceride-rich VLDLs,
them-selves highly atherogenic, are subjectto altered lipolysis,
which createssmaller VLDL particles (remnants)and small, dense LDL
and HDLparticles. This process results in lowHDL-C and HDL particle
counts(HDL-P). Patients with small LDLparticles typically have high
LDL-P(ApoB) concentrations.31 Since many
metabolic syndrome patients withsmall LDL particles have
lowHDL-C, they will often have ab-normalities of non-HDL-C,
total
cholesterol (TC)/HDL-C and tri-glycerides (TG)/HDL-C ( >4:1
isabnormal) ratios.36The scenario ofnormal LDL-C associated with
el-evated non-HDL-C, or abnormal
TC/HDL-C or TG/HDL-C ratioscan be used to identify elevated
ApoB and likely contributes to theresidual CV risk so common
inthese patients.34,37
Low HDL-C is the most com-
mon abnormality associated withCVD events in the Framinghamstudy
and is often associated withinsulin-resistant syndromes
likemetabolic syndrome. Low HDL-Cis often associated with
increasednumbers of atherogenic VLDLremnants and small LDL
particles.
Also contributing to the risk is thealtered functionality of HDL
parti-cles common in proinflammatory
states like metabolic syndrome andT2DM. Inflammatory proteins
ren-der HDL particles less efficaciousat performing macrophage
reverse
Figure 2. Lipoprotein abnormalities of insulin
resistance/adiposopathy.
-
8/8/2019 Diagnosis and Treatment of Metabolic Syndrome in
Menopausal Women
6/12
MM
22 MENOPAUSEMANAGEMENT
cholesterol transport, and deliveringanti-inflammatory,
anticoagulantand profibrinolytic proteins to areasof arterial
plaque. It is becoming ev-ident that the new term HDLfunctionality
is likely very impor-tant in atherogenesis. Therapeuti-cally
improving HDL functionalitymay be more important than in-creasing
HDL-C.38,39
Treatment
The 2007 AHA guidelines for theprevention of cardiovascular
diseaserisk in women emphasize the as-sessment of lifetime risk in
womeninstead of the previous emphasisupon assessment ofshort-term
risk.10
The Framingham risk paradigm isexcellent at assessing 10-year
risk in
women, but we now have substantialdata showing that even the
presence
of one major cardiovascular risk fac-tor in a woman over 50
years of age will increase her lifetime risk forcardiovascular
disease dramatically.
There is also evidence that there isa broad heterogeneity of
risk pres-ent in women with a given FRS. Ahigh-risk FRS (>20%)
identifies
women at high risk, but a lower scoreis not sufficient to ensure
that an indi-vidual woman is at low risk. The com-
bined use of metabolic syndromediagnosis with a lipoprotein
particle-based treatment approach provides arational approach to
management ofrisk in menopausal women.
Therapeutic lifestyle change. Thegoals of treatment in metabolic
syn-drome are to simultaneously de-crease the instance of CHD
eventsand to prevent or delay the devel-opment of T2DM. The
cornerstone
of treatment is therapeutic lifestylechange directed at
improving adi-
pose tissue dysfunction, not neces-sarily reduction in adipose
tissuemass. The establishment of a meta-bolic syndrome clinic in
the health-care providers office to specificallytarget and treat
metabolic syndromethrough therapeutic lifestyle changeis a
promising approach, as intensivelifestyle modification has
beenshown to improve components ofmetabolic syndrome.40-42
Thera-
peutic lifestyle change in metabolicsyndrome consists of
promotion ofdaily moderate-intensity exercise,modest weight
reduction, a healthylow glycemic index or Mediter-ranean-style diet
and increased con-sumption of omega-3 fatty acids(Table 3). Modest
weight reduction(5-10%) and walking 150-180min/week improves many
of thephysiologic abnormalities of meta-
bolic syndrome and slows the pro-gression to T2DM.
Self-monitoringof parameters such as food intake,body weight and
exercise level iscritical for success. Exercise man-agement should
consist of at least 30minutes of moderate-to-vigorous
physical activity on most days ofthe week. If this activity is
weight-bearing, the dual benefit of potentialprevention of
menopausal osteo-porosis can also be accomplished.
The use of inexpensive pedometersto set and track goals for the
simplestform of modest-intensity exercise
walkingis practical and effective;more than 10,000 steps/day is
con-sidered an active lifestyle. An ex-
ercise prescription of adding >1,000kcal/week of exercise
(~20,000-25,000 steps/week) consisting ofmoderate-intensity walking
is rec-ommended.43 Patients should be re-minded that regardless of
any weightloss achieved, physical activity is in-sulin sensitizing
and is of cardiores-piratory and psychological value.44
Goals for an individualized dietinclude a reasonable reduction
in
weight of 7% to 10% over 1 year,with the eventual goal of
obtainingideal body weight. This is achievedby the initiation of
reduced caloricintake and reduced consumption ofsimple
carbohydrates, under the su-pervision of a clinical nutritionist
if
Table 3. Implementing Therapeutic Lifestyle Changes
Specific contract with patient for goals and
self-monitoring.
Exercise at least 30 minutes of moderate to vigorous physical
activity on mostdays of the week. Using pedometer, walking
>10,000 steps/day is desirable.
Diet reduction of weight by 7-10% over 1 year with reduced
caloric intake and
reduced consumption of simple carbohydrates (low glycemic index
diet). Womenshould consume a diet rich in fruits and vegetables;
whole-grain, high-fiber foods;limited intake of saturated fat to
10% of energy (if possible to 7%); cholesterol to300 mg/d; no more
than 1 alcoholic drink per day; consumption of trans-fatty
acids(FA) should be as low as possible.
Increased omega-3 FA consumption (~850-1000 mg EPA + DHA /
day)
Women should not smoke and should avoid environmental tobacco
smoke.
EPA=eicosapentaenoic acid; DHA=docosahexaenoic acid
-
8/8/2019 Diagnosis and Treatment of Metabolic Syndrome in
Menopausal Women
7/12
MM
NOVEMBER/DECEMBER2007 23
possible. Attainment of ideal bodyweight is obviously difficult
in thispopulation, but even modest weightloss has been associated
with labo-ratory improvement and clinical riskreduction.40
Increased soluble fiberintake and reduction of saturatedand trans
fatty acid intake are to berecommended as well. Plant stanolesters
significantly lower LDL-Cand are available in various func-
tional foods.
45
Increased omega-3fatty acid consumption (approxi-mately 1,000 mg
of eicosapentaenoicacid [EPA] and docosahexaenoicacid [DHA] per
day) reduces risk in
women with CVD, and it is reason-able to extend this treatment
tohigh-risk patients such as those withmetabolic syndrome.
Pharmacologic treatment. Pharma-cologic treatment of
cardiovascular
risk in metabolic syndrome is basedon the assessment and
treatment ofrisk using an atherogenic particle-based approach.46
Aggressive treat-ment is safe, effective and well
within the scope of practice of allprimary care providers,47 and
neednot be left to internists and cardiol-ogists once risk is
identified.
An aggressive goal is to reducethe atherogenic ApoB particle
count
to physiologic levels associated withlow CVD risk (Table 4).
Statindrugs inhibit cholesterol synthesis inalmost all cells,
although the liver isthe organ that clears ApoB parti-cles. The
largest body of evidencefor pharmacologic risk reduction
ininsulin-resistant patients exists forstatins. First-line
pharmacologicstrategy to reduce ApoB-containingparticles would be
appropriately
dosed statin therapy. A complemen-tary strategy would be to
reduce the
number of circulating triglyceride-rich VLDL particles driving
thelipoprotein abnormalities of meta-bolic syndrome, by either
reducingtheir production in the liver or in-creasing their
catabolism, with fi-brates, niacin or high-dose omega-3fatty acids.
The fibrates regulate
multiple genes involved with glucoseand fatty acid metabolism,
lipopro-tein synthesis and catabolism, and
vascular inflammation. They de-crease the hepatic production
oftriglycerides, increase the catabolismof triglyceride-rich
lipoproteins andincrease the synthesis and function-
Table 4. Metabolic Syndrome Pharmacologic Treatment
9,11,31,32
Assessment and treatment of risk using an atherogenic
particle-basedapproach (instead of a traditional lipid-based
approach)
Primary goal: reduce atherogenic ApoB particles to physiologic
levels
Lifestyle approaches should be encouraged to reach the following
optimal lipid levels:
LDL-C < 100 mg/dL
HDL-C > 50 mg/dL
TG < 150 mg/dL
Non HDL-C < 130 mg/dL
Framingham Risk Scoring should be done to stratify absolute
10-year risk of ASCVD.
Goals of treatment for those atmoderately high risk
(
2 risk major risk factors, with10-20% risk) and high-risk
patients (known CVD or T2DM or CHD equivalent*):
Non-HDL-C < 130 mg/dL OR ApoB < 80 mg/dL OR NMR LDL-P <
1000 nMol/L
Very high-risk women (established CVD plus any of the following:
MetSyn, multiplemajor risk factors, severe and poorly controlled
risk factors, T2DM) have lower goals:
Non-HDL-C < 100 mg/dL OR ApoB < 60 mg/dL OR NMR LDL-P <
1000 nMol/L
Statin is first-line Rx to reduce ApoB particles.
If not at non-HDL-C, ApoB or LDL-P goal, add fenofibrate.
Ezetimibe or bile acidsequestrant or Rx extended-release niacin can
be added if goal not attained.
Aggressive hypertension control. Optimal BP < 120/80. Treat
to < 130/80, withACE inhibitors/ARBs preferred, with thiazide
diuretics next if needed.
Management of hyperglycemia (FBS > 100 mg/dL ) with
metformin, especiallywith an abnormal glucose tolerance test.
81- to 162-mg enteric-coated aspirin, unless
contraindicated.
Weight-loss medications or bariatric surgery may be helpful in
some patients.
*CHD equivalent = known peripheral arterial disease, abdominal
aortic aneurysm, carotidartery disease, chronic renal disease
(creatinine > 1.2 mg/dL)
LDL-C = low-density lipoprotein cholesterol; HDL-C= high-density
lipoprotein cholesterol;TG = triglycerides; ASCVD = atherosclerotic
cardiovascular disease; T2DM = type 2 diabetes mellitus;CHD =
coronary heart disease; Apo-B = apolipoprotein B; NMR = nuclear
magnetic resonance;MetSyn = metabolic syndrome; LDL-P = LDL
particle concentration; FBS = fasting blood sugar
-
8/8/2019 Diagnosis and Treatment of Metabolic Syndrome in
Menopausal Women
8/12
MM
24 MENOPAUSEMANAGEMENT
ality of HDL particles.48 Trial datareveal that fibrates are
significantlymore efficacious in insulin-resistantpatients. In the
Fenofibrate Inter-
vention and Event Lowering inDiabetes (FIELD) trial,
fenofibratedemonstrated a trend toward CVDrisk reduction
(nonsignificant ab-solute risk reduction) in women
with T2DM, as well as reduction ofmicrovascular endpoints, such
as the
need for laser-photocoagulationretinal therapy,
microalbuminuriaand peripheral amputations.49 Con-sistent with
other fibrate trials,FIELD patients with dyslipidemia(triglycerides
>150 mg/dL and HDL
-
8/8/2019 Diagnosis and Treatment of Metabolic Syndrome in
Menopausal Women
9/12
MM
NOVEMBER/DECEMBER2007 25
concerns.57Aggressive hypertensioncontrol (treat to 10%
10-yearrisk of CVD on the FRS shouldreceive low-dose aspirin
therapy(81-162 mg enteric-coated aspirin),unless contraindicated.
The man-agement of insulin-resistant hyper-glycemia (especially
impaired glucosetolerance) itself can be augmented
with the addition of pharmacologictherapy with metformin.
Metforminadditionally may provoke weight loss
or stabilization, and has been shownto reduce mortality in
T2DM59 andthe progression to T2DM. The useof thiazolinediones as
insulin-sensitizing agents for risk reductionand T2DM prevention
has been ad-
vocated.60 A recent meta-analysissuggested increased CVD risk
withthe thiazolinedione rosiglitazone,61
although this is controversial.62Therole of other hypoglycemic
and
insulin-resistance-reducing drugs,such as acarbose, exenatide
andsitagliptin, is unclear.
Summary and Conclusions
The diagnosis of metabolic syn-drome helps to identify
menopausalpatients at increased long-term riskfor ASCVD, T2DM and
ischemicstroke. Despite the fact that thesepatients may have only
modest
elevations of individual risk factors,such as high blood
pressure and
elevated lipids, the presence ofmetabolic syndrome helps
identifypatients with the adverse physiologicstate of adiposopathy,
and its accom-panying pathologic combination ofabnormal
lipoproteins, cytokines andpro-inflammatory factors. These
pa-tients might benefit from more in-tensive therapeutic lifestyle
changesand pharmacologic therapy, targetedspecifically at improving
their un-
derlying adiposopathy and increasedatherogenic ApoB
lipoproteins, andat prevention of T2DM. The patienthand-out on
pages 27 and 28 willserve as a valuable tool for makingpatients
active participants in achiev-ing these goals.
Gregory S. Pokrywka, MD, FACP, is Assis-
tant Professor of Medicine at Johns Hop-
kins University School of Medicine,
Baltimore, MD; and Director of the Balti-more Lipid Center,
Towson, MD.
Dr. Pokrywka participates in the Speakers
Bureaus for AstraZeneca PharmaceuticalsLP, Abbott Laboratories,
Sanofi-Aventis,
Oscient, LipoScience, Diadexus and Reliant
Pharmaceuticals, LLC.
This article includes discussion of off-
label use of medications.
Submitted: May 29, 2007. Accepted: July
23, 2007.
References
1. Reaven GM. Role of insulin resistance in human dis-ease.
Diabetes 1998;37:1595-1607.
2. American Heart Association. Women and cardiovas-
cular disease facts. Available at
www.americanheart.org/presenter.jhtml?identifier=3039318. Accessed
5/27/07.
3. Polotsky AJ, Santoro N. Menopause and cardiovascu-lar
disease: endogenous reproductive hormone exposureaffects risk
factors. Menopause Management2007;16:21-25.
4. Grundy SM. Metabolic syndrome: connecting andreconciling
cardiovascular and diabetes worlds. J Am
CollCardiol2006;47:10931100.
5. Kahn R, Buse J, Ferrannini E, et al. The metabolicsyndrome:
time for a critical appraisal: joint statementfrom the American
Diabetes Association and the Euro-pean Association for the Study of
Diabetes. DiabetesCare 2005;28:22892304.
6. Blaha M, Elasy TA. Clinical use of the metabolicsyndrome. Why
the confusion? Clin Diabetes 2006;24:125-131.
7. Schneider JG, Tompkins C, Blumenthal RS. Themetabolic
syndrome in women. Cardiology Rev2006;14:1-6.
8. Deedwania P, Barter P, Carmena R, et al; Treating toNew
Targets Investigators. Reduction of low-densitylipoprotein
cholesterol in patients with coronary heart dis-ease and metabolic
syndrome: analysis of the Treating toNew Targets study.
Lancet2006;368:919-28.
9. Grundy SM, Cleeman JI, Daniels SR, et al. AmericanHeart
Association; National Heart, Lung, and Blood Insti-tute: Diagnosis
and management of the metabolic syn-drome. Circulation
2005;112:273552.
10. Rutter M, Meigs J, Wilson P. Cardiovascular risk andthe
metabolic syndrome. Metabolic Syndrome and Re-lated Disorders
2006;4:252-60.
11. Mosca L, Banka CL, Benjamin EJ, et al, for the
ExpertPanel/Writing Group. Evidence-based guidelines for
car-diovascular disease prevention in women: 2007
update.Circulation 2007;115:1481-1501.
12. Bax JJ, Inzucchi SE, Bonow RO, et al. Cardiac imag-ing for
risk stratification in diabetes. Diabetes
Care2007;30:1295-1304.
13. Lorenzo C, Williams K, Hunt K, Haffner SM. The Na-tional
Cholesterol Education ProgramAdult TreatmentPanel III,
International Diabetes Federation, and WorldHealth Organization
definitions of the metabolic syndromeas predictors of incident
cardiovascular disease and dia-betes. Diabetes Care
2007;30:8-13.
14. Schneider JG, Tompkins C, Blumenthal RS. Themetabolic
syndrome in women. Cardiology Rev2006;
14:1-6.
PPharmacologic
(orlistat and
sirbutramine) and
bariatric surgery
approaches to weight
reduction seem
promising, although
clinical correlation
with event reduction
awaits further
research.
-
8/8/2019 Diagnosis and Treatment of Metabolic Syndrome in
Menopausal Women
10/12
MM
26 MENOPAUSEMANAGEMENT
15. Dekker JM, Girman C, Rhodes T, et al. Metabolicsyndrome and
10 year cardiovascular disease risk in the
Hoorn study. Circulation 2005;112:666-73.
16. Liu J, Grundy SM, Wang W, et al. Ten year risk of
car-diovascular incidence related to diabetes, prediabetes andthe
metabolic syndrome. Am Heart J2007;153:552-58.
17. Isomaa B, Almgren P, Tuomi T, et al. Cardiovascularmorbidity
and mortality associated with the metabolic syn-drome. Diabetes
Care 2001;24:683-89.
18. Jeppesen J, Hansen TW, Rasmussen S, et al.
Insulinresistance, the metabolic syndrome, and risk of incident
car-diovascular disease. J Am Coll Cardiol2007;49:2112-19.
19. Gami A, Witt BJ, Howard DE, et al. Metabolic syn-drome and
risk of incident cardiovascular events anddeath: a systematic
review and meta-analysis of longitudi-nal studies. J Am Coll
Cardiol2007;49:403-14.
20. Tanko LB, Bagger YZ, Qin G, et al. Enlarged waist
combined with elevated triglycerides is a strong predictorof
accelerated atherogenesis and related cardiovascularmortality in
postmenopausal women. Circulation 2005;111:1883-90.
21. Sarwar N, Danesh J, Eriksdottir J, et al. Triglyceridesand
the risk of coronary heart disease. 10,158 incidentcases among
262,525 participants in 29 westernprospective studies. Circulation
2007;115:450-58.
22. Bansal S, Buring J, Rifai N, et al. Fasting comparedwith
nonfasting triglycerides and risk of cardiovascularevents in women.
JAMA. 2007;298:309-16.
23. Sattar N, Gaw A, Scherbakova O, et al. Metabolicsyndrome
with and without C-reactive protein as a predic-tor of coronary
heart disease and diabetes in the West ofScotland Coronary
Prevention study. Circulation 2003;108:414-19.
24. Wilson PW, DAgostino RB, Parise H, et al. Metabolicsyndrome
as a precursor of cardiovascular disease andtype 2 diabetes
mellitus. Circulation 2005; 112:306 6-72.
25. Kurl, S, Laukkanen JA, Niskanen L, et al. Metabolicsyndrome
and the risk of stroke in middle-aged men.Stroke 2006 37:80611.
26. Ford ES, Giles WH, Dietz, WH. Prevalence of themetabolic
syndrome among US adults. Findings from theThird National Health
and Nutrition Examination Survey.JAMA 2002;287:356-59.
27. Bays H, Dujovne C. Adiposopathy is a more nationaltreatment
target for metabolic disease than obesity alone.Curr Atheroscler
Rep 2006;8:144-56.
28. Kip KE, Marroquin OC, Kelley DE, et al. Clinical im-portance
of obesity versus the metabolic syndrome in car-diovascular risk in
women. Circulation 2004;109:706-13.
29. Lamarche B, Tchernof A, Dagenais GR, et al. Small,dense LDL
particles and the risk of ischemic heart dis-ease. Prospective
results from the Quebec Cardiovascu-lar Study. Circulation
1997;95:6975.
30. Grundy SM, Cleeman JI, Bairey N, et al, for the
Coor-dinating Committee of the National Cholesterol
EducationProgram. Implications of Recent Clinical Trials for the
Na-tional Cholesterol Education Program Adult TreatmentPanel III
Guidelines. Circulation. 2004;110:227-39.
31. Barter PJ, Ballantyne CM, Carmena R, et al. Apo Bversus
cholesterol in estimating cardiovascular risk and inguiding
therapy: report of the thirty-person/ten countrypanel. J Intern
Med2006;259:24758.
32. Mudd J, Borlaug B, Johnston P, et al. Beyond low-density
lipoprotein cholesterol: defining the role of low-
density lipoprotein heterogeneity in coronary arterydisease.
JACC 2007:50:1735-41.
33. Liu J, Sempos C, Donahue R, et al.
Non-high-densitylipoprotein and very-low-density lipoprotein
cholesterol
and their risk predictive values in coronary heart disease.Am J
Cardiol2006;98:1363-68.
34. Cromwell W, Otvos J. Low-density lipoprotein particlenumber
and risk for cardiovascular disease. Curr AtheroscleRep 2004,
6:38187.
35. Bays H, Abate N, Chandalia M. Adiposopathy: sickfat causes
high blood sugar, high blood pressure and dys-lipidemia. Future
Cardiol2005;1:3959.
36. Dayspring T. Cardiovascular disease: a comprehen-sive primer
for clinicians. Menopause Management2002;11:1-9.
37. Cromwell W, Otvos J. Heterogeneity of low-densitylipoprotein
particle number in patients with type 2 dia-betes mellitus and
low-density lipoprotein cholesterol
-
8/8/2019 Diagnosis and Treatment of Metabolic Syndrome in
Menopausal Women
11/12
What is metabolic syndrome? Why is it a concern?
Metabolic syndrome is a disorder that affects the waythe body
metabolizes fat and sugar. It can occur inthose who have too much
waistline fat and who in-herit this tendency. With more Americans
being over-
weight and obese, metabolic syndrome is becomingincreasingly
common. The metabolic syndrome hasbeen thought of as a prediabetic
syndrome, butdoctors increasingly regard it as a
precoronarysyndrome (a condition that increases the risk ofheart
disease). Metabolic syndrome greatly increases
your long-term risk of cardiovascular events, such asheart
attacks, strokes and sudden death, and alsodramatically increases
your risk of type 2 diabetes.
Who is at risk for metabolic syndrome?
Metabolic syndrome affects women more severelythan men, and it
is more likely to occur at menopause
and beyond. Where a woman accumulates fat in herbody is an
important factor in determining whethershes at higher risk for
metabolic syndrome. Theapple shape is a higher-risk situation than
the pearshape. Excessive waistline fat causes sick fat cells,
which produce a toxic stew of substances, increas-ing a womans
risk of developing cardiovasculardisease and diabetes.
How is metabolic syndrome diagnosed?
Metabolic syndrome is diagnosed if you have 3 of the
following 5 conditions: Waist (at the top of the hip) measures
more than35 inches (more than 31 inches in South Asians)
Blood pressure is over 130/85 mmHg (or youre al-ready taking
blood-pressure-lowering medications)
High-density lipoprotein (good) cholesterol(HDL-C) is less than
50 mg/dL (or youre alreadytaking medication for low HDL-C)
Triglyceride (TG) level is over 150 mg/dL (oryoure taking
medication for elevated TG)
Fasting blood sugar is greater than 100 mg/dL (or
youre taking medication to lower blood sugar)
As the number of these risk factors increases, sodoes your risk
for cardiovascular disease.
Fortunately, metabolic syndrome is treatable andmost of the
events associated with it are preventable.The key to reversing this
process is a commitment tomodest weight loss and regular exercise.
You need tomake a specific contract for goals with your health-care
provider, and you need to implement self-
monitoring to follow your progress.
NOVEMBER/DECEMBER2007 27
Resources
http://www.goredforwomen.org
http://www.womenheart.org/index.asp
http://www.hearthealthywomen.org
http://www.menopause.org
http://www.thewalkingsite.com
More detailed lipid and lipoprotein information canbe found
at:
http://www.lipoprofile.com/index.cfm
http://cks.library.nhs.uk/lipids_management/in_depth/background_information
Metabolic Syndromeand Menopause
Physiciansareencouragedtocopyanddistributethispatientinformationhandout.
Patient Information
-
8/8/2019 Diagnosis and Treatment of Metabolic Syndrome in
Menopausal Women
12/12
M M
Your Treatment Goals:
Weight reduction of 10% over 1 year (with the eventualgoal of
attaining your ideal body weight).
YOUR WEIGHT-LOSS GOAL:is to weigh less than ________________
lbs.
(90% of your current body weight.)
DietFollow a reduced-calorie diet with carbohydrates that arelow
on the glycemic index (GI) (visit www.glycemicindex.com). The
glycemic index ranks carbohydrates accordingto their effect on
blood sugar. Foods low in GI carbohy-drates create smaller changes
in your levels of blood sugarand insulin, and are key to losing
weight, maintainingweight loss, and lowering your risk of heart
disease anddiabetes. (Visit
http://www.americanheart.org/presenter.
jhtml?identifier=4644.]
Women should:
consume a diet rich in fruits and vegetables choose whole-grain,
high-fiber foods limit alcohol intake to no more than 1 drink/day
limit cholesterol to 300 mg/day limit intake of saturated
(animal-derived) fats to 10% of
total calories (7% is even better) and keep consumptionof
trans-fatty acids as low as possible
YOUR Diet Plan:
ExerciseExercise at least 30 min/day, with moderate to
vigorousphysical activity on most days of the week. If walking
andusing a pedometer, more than 10,000 steps/day is desir-able
(adding over 1,000 kcal/week of exercise, ~20,000-25,000
steps/week) [1 mile walked = approximately 2000steps]. A physician
should be consulted before begin-ning any rigorous exercise
regimen.
YOUR Exercise Plan:
Lower your blood pressure if its high!A blood pressure reading
of less than 120/80 mmHg is op-timal. Medications are recommended
if your blood pressureis consistently higher than 130/80 mmHg.
YOUR blood pressure:_______________________________________
YOUR blood pressure medication:
______________________________________________
Keep your fasting blood sugar below 100 mg/dL (the optimal
level).
YOUR fasting blood sugar:
___________________________________________________________________
YOUR blood-sugar reducing medication: ______________________
Goals for Cholesterol and Triglycerides: LDL (low-density
lipoprotein, bad) cholesterol: LESS
THAN 100 mg/dL HDL (high-density lipoprotein, good)
cholesterol:
GREATER THAN 50 mg/dL Triglycerides: LESS THAN 150 mg/dL Non
HDL-cholesterol (total cholesterol minus HDL
cholesterol): LESS THAN 130 mg/dL
Traditional cholesterol and triglyceride measurements meas-ure
fat (lipids) in the blood. In metabolic syndrome thesemeasurements
less accurately predict the number of lipopro-tein particles
implicated in causing cardiovascular diseases.Your doctor will use
different goals, and perhaps advancedtests such as ApoB and NMR
LDL-P to more accuratelycount the atherosclerosis-causing
lipoprotein particles.
YOUR LIPID Value(s):
Future Risk of Heart DiseaseYour risk of having a heart attack
within 10 years is esti-mated in a calculation called the
Framingham Risk Score(FRS). The FRS is designed for adults age 20
years andolder who do not have heart disease or diabetes. To
cal-culate your FRS, visit
http://hp2010.nhlbihin.net/atpiii/calculator.asp.
YOUR Framingham Risk Score:
Women at moderately high risk (with a 10-20% 10-yearrisk) and
high-risk patients ( >20% 10-year risk OR knowncoronary disease,
diabetes or their equivalents) should havea non-HDL cholesterol
goal of LESS THAN 130 mg/dL.Very high-risk women should have an
even lower non-HDLcholesterol goal (LESS THAN 100 mg/dL).
Your doctor will discuss the need for
cholesterol/lipoprotein-lowering medicines to help you reach these
goals.
YOUR medications are:
Additional Advice:Stop smoking and avoid environmental smoke
exposure.The following are recommended for most menopausalwomen
with metabolic syndrome unless contraindi-cated by certain medical
conditions. Talk to your doc-tor about whether you should NOT take:
daily aspirin therapy to prevent heart attack Omega-3 fatty acid
supplements that contain 850-1,000
mg/day of the active ingredients DHA and EPA.
Patient Information