Embed Size (px)
Citation preview

Original article
Diagnosis and treatment of autoimmune pancreatitis types1 and 2
S. Fritz1, F. Bergmann2, L. Grenacher3, M. Sgroi1, U. Hinz1, T. Hackert1, M. W. Büchler1 andJ. Werner4
Departments of 1General, Visceral and Transplantation Surgery, 2Pathology and 3Diagnostic and Interventional Radiology, University of Heidelberg,Heidelberg, and 4Department of General, Visceral and Transplantation Surgery, Ludwig-Maximilians University of Munich, Munich, GermanyCorrespondence to: Dr S. Fritz, Division of Pancreatic Surgery, Department of General, Visceral and Transplantation Surgery, University of Heidelberg, ImNeuenheimer Feld 110, 69120 Heidelberg, Germany (e-mail: [email protected])
Background: Autoimmune pancreatitis (AIP) is characterized by diffuse or focal swelling of the pancreas.AIP has been divided into types 1 and 2. The aim of the study was to evaluate and compare theclinicopathological characteristics, therapy and outcome of patients with AIP.Methods: The medical records of patients diagnosed with AIP between January 2003 and July 2011 werereviewed. Characteristics of patients with AIP types 1 and 2 were compared with those of patients withpancreatic ductal adenocarcinoma (PDAC).Results: AIP was classified as type 1 in 40 patients and type 2 in 32 according to the HISORt (Histology,Imaging, Serology, Other organ involvement, Response to therapy) criteria. Patients with histologicallyconfirmed AIP type 2 were younger than those with type 1 (P = 0⋅005). Some 30 of 32 patients withAIP type 2 were found to have a localized tumour-like pancreatic mass and underwent pancreatectomy,compared with only 16 of 40 with type 1 (P < 0⋅001). Three of 25 patients with AIP type 2 presented withraised serum levels of IgG4 compared with 21 of 38 with type 1 (P < 0⋅001). There was no difference insymptoms and involvement of other organs between AIP types 1 and 2. Presentation with weight losswas more common among patients with PDAC than those with AIP, but there was no difference in painor jaundice between the groups. Raised serum carbohydrate antigen 19-9 levels were more prevalent inpatients with PDAC.Conclusion: Patients with AIP type 2 frequently present with abdominal pain and a tumour-like mass.Differentiating AIP from PDAC is difficult, so making the clinical decision regarding operative versus
conservative management is challenging.
Paper accepted 24 April 2014Published online 22 July 2014 in Wiley Online Library (www.bjs.co.uk). DOI: 10.1002/bjs.9574
Introduction
During the past decade, recognition of autoimmune pan-creatitis (AIP) as a distinct clinical entity has increasedworldwide1,2. AIP accounts for approximately 5 per centof all patients with chronic pancreatitis3. The aetiologyand pathogenesis remain poorly understood4. Patientswith AIP frequently present with diffuse or focal swellingof the pancreas with or without jaundice owing to extra-hepatic cholestasis5. Even with use of modern thin-sliceabdominal imaging the differential diagnosis betweenAIP and a malignant pancreaticobiliary tumour remainschallenging6,7. Consequently, affected patients are fre-quently referred for surgery and undergo pancreaticresection to exclude definitely the risk of harbouring amalignant pancreatic tumour8.
During the international AIP consensus meeting in20099, the need to differentiate between two subtypesof AIP was outlined10–13. AIP types 1 and 2 differ withregard to treatment response and relapse rate. Type 1fits the classical criteria of AIP and is associated witha histological pattern of lymphoplasmacytic sclerosingpancreatitis1,14–16. Affected patients usually present withabdominal pain, weight loss, anorexia and jaundice. Thereis frequently diffuse swelling of the pancreas, often associ-ated with an irregular narrowing of the pancreatic duct17.Some 75 per cent of patients with AIP type 1 present withraised serum levels of IgG418. AIP type 1 is frequentlyassociated with other autoimmune-related diseases6,19,20.
AIP type 2 is characterized by a so-called idiopathicduct-centric pancreatitis and pathognomonic ‘granulocyte
© 2014 BJS Society Ltd BJS 2014; 101: 1257–1265Published by John Wiley & Sons Ltd

1258 S. Fritz, F. Bergmann, L. Grenacher, M. Sgroi, U. Hinz, T. Hackert et al.
epithelial lesion (GEL)-positive pancreatitis’21,22. Firstdescribed by Ectors and colleagues23, GELs are charac-terized by focal detachment, disruption and destruction ofthe epithelium of interlobular ducts24. Although the histo-morphology of AIP type 2 has been described in variousreports, little is known about the clinical characteristicsand outcome of these patients11. The diagnosis of AIP type1 can usually be made on clinical grounds, by imaging25
and laboratory tests1,19,26, whereas histological proof ismandatory for the definite diagnosis of AIP type 212,27,28.
The aim of the study was to evaluate the clinicopatho-logical characteristics, therapy and outcome of patientswith AIP types 1 and 2.
Methods
All patients seen at the Pancreas Centre of the Depart-ment of Surgery, University of Heidelberg, who fulfilledthe HISORt (Histology, Imaging, Serology, Other organinvolvement, Response to therapy) criteria29 for AIPbetween January 2003 and July 2011 were eligible forthe study. Following the HISORt classification system,AIP was diagnosed when patients met at least one ofthe following criteria: histologically confirmed diagnosisof AIP following surgical resection or biopsy (HISORtdiagnostic criteria group A); typical radiological features(such as diffusely enlarged sausage-shaped gland withirregular narrowing of the main pancreatic duct) andassociated serological changes (HISORt diagnostic criteriagroup B); and typical radiological features of AIP and animaging-confirmed response to steroid therapy (HISORtdiagnostic criteria group C). Patients with AIP type 2 werediagnosed exclusively based on histology. If histology wasnot available, but the patient met the HISORt criteria, thepatient was assigned to the AIP type 1 cohort19.
Patients with known risk factors for chronic pancreatitis,such as alcohol consumption exceeding 60 g/day, pancreasdivisum, history of necrotizing pancreatitis or abdominaltrauma, were excluded from the study.
A standard record form, including details of age and sex,symptoms, other organ involvement, abdominal imaging,blood tests, treatment and quality of life, was filled outby the physician at each visit. Any specific informationrelevant to the study (recurrent disease, surgical proce-dures, complications) were documented. Evaluation ofthe patients’ medical history focused on pancreaticobiliarydiseases, previous pancreatic surgery, autoimmune-relateddiseases including sclerosing cholangitis, sclerosingsialoadenitis, involvement of lacrimal glands or kidneys,retroperitoneal fibrosis, and allergic manifestations such asallergic rhinitis, atopic dermatitis or bronchial asthma30.
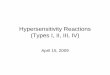
Fig. 1 Typical sausage-shaped pancreas of a 51-year-old man withautoimmune pancreatitis type 1. Multidetector computedtomography in the portal-venous phase shows diffuse swelling ofthe entire pancreas (arrows)
This study and the questionnaire used were approved bythe local ethics committee of the University of Heidelberg.
Imaging studies
All patients underwent either multidetector computedtomography (MDCT), magnetic resonance imaging(MRI) and/or magnetic resonance cholangiopancreato-graphy (MRCP). Endoscopic retrograde pancreatogra-phy and endoscopic ultrasonography were consideredfor evaluation of pancreatic morphology when avail-able. Radiological features characteristic of AIP includeddiffusely enlarged pancreas with loss of normal lob-ularity (sausage-like appearance) (Fig. 1), delayed andlow-density ‘rim’ enhancement, and a dilated main pan-creatic duct together with focal or diffuse narrowing25.‘Tumour-like lesion’ was used to describe a focalmass-forming lesion resembling a pancreatic malig-nancy (Fig. 2). Thin-slice imaging was also used toexclude potential metastatic disease and to assess whetherthere were abdominal extrapancreatic autoimmune-relatedlesions.
Blood tests
Serum concentrations of IgG and IgG4 were determinedat the time of diagnosis by automated immunonephelo-metry. In all patients who underwent primary surgery forsuspected pancreatic cancer, IgG levels were determinedas soon as the final histological diagnosis of AIP was
© 2014 BJS Society Ltd www.bjs.co.uk BJS 2014; 101: 1257–1265Published by John Wiley & Sons Ltd

Autoimmune pancreatitis types 1 and 2 1259
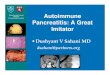
a Axial plane
b Coronal view
Fig. 2 Multidetector computed tomography with intravenouscontrast showing tumorous lesion in the pancreatic head of apatient with autoimmune pancreatitis type 2: a axial plane (noteendoprosthesis in distal part of bile duct) and b coronal view
available. Levels of IgG of at least 16⋅0 g/l, and IgG4 of140 g/l or more, were considered raised31. The followingautoantibodies were used as markers for autoimmunedisease; levels were considered to be raised when valueswere above the upper limit of normal (in parentheses):antinuclear antibody (ANA; more than 1 : 80), rheumatoidfactor (RF; over 25 units/ml), antineutrophil cytoplas-mic antibodies (ANCA; more than 1 : 10), male germcell-associated kinase antibody (MAK; over 60 units/ml),thyroid-stimulating hormone receptor antibodies (TRAK;over 1⋅00 units/ml), lactoferrin antibody (antibody ratioless than 10), carbonic anhydrase 1 antibodies (positive),carbonic anhydrase 2 antibodies (positive), extractablenuclear antigens (ENA; more than 6⋅3 units/l) and solubleinterleukin 2 receptor (sCD25; over 900 units/ml). ANA,ANCA, MAK, TRAK, ENA, RF and sCD25 levels weredetermined using enzyme-linked immunosorbent assays.
Histopathology
Haematoxylin and eosin staining, and immunohisto-chemistry for IgG4-positive plasma cells was carried outroutinely in all resected specimens and biopsies. Diagnos-tic criteria for AIP included periductal lymphoplasmocyticinfiltrate, periductal concentric fibrosis (Fig. 3a) anddetection of vasculitis (Fig. 3c)13. AIP type 2 was diag-nosed when an idiopathic duct-centric pancreatitis withtypical GELs was present (Fig. 3b) in combination withabsent or rare IgG4-positive plasma cells (10 or fewer perhigh-power field (HPF)). AIP type 1 was characterizedby lymphoplasmacytic sclerosing pancreatitis includingdense fibrosis with rich lymphoplasmacytic infiltration(‘storiform fibrosis’), and obliterative phlebitis (Fig. 3c).In addition, numerous IgG4-positive plasma cells (morethan 10/HPF) were identified in AIP type 1 (Fig. 3d)27.Histopathological diagnoses were made in accordancewith the 2011 international consensus diagnostic criteriafor autoimmune pancreatitis28.
Follow-up
All patients, whether managed conservatively or by surgery,were seen in the outpatient clinic after 3 months. There-after the interval for future visits was determined on anindividual basis depending on clinical symptoms or othercomplaints. The date of last follow-up was July 2011.Follow-up data were obtained in the outpatient clinic orfrom the patient’s last visit to the general physician. Eval-uation included the current status of the disease, as well asthe occurrence or relapse of pancreatic or extrapancreaticmanifestations.
Comparison of autoimmune pancreatitiswith pancreatic ductal adenocarcinoma
All patients with AIP type 1 or 2 who presented with a local-ized lesion suspicious for malignancy were matched withcontrols with pancreatic ductal adenocarcinoma (PDAC).The following parameters were used to match one patientwith AIP (case) with two patients with PDAC (controls):age (± 5 years), sex and site of disease. All controls wereidentified from the institutional database of pancreaticcancer.
Statistical analysis
The records of all patients diagnosed with AIP wereentered into a database. Continuous data are presentedas median (range), unless indicated otherwise. The dis-tribution of age was compared between groups using the
© 2014 BJS Society Ltd www.bjs.co.uk BJS 2014; 101: 1257–1265Published by John Wiley & Sons Ltd

1260 S. Fritz, F. Bergmann, L. Grenacher, M. Sgroi, U. Hinz, T. Hackert et al.
a Periductal fibrosis and infiltrates b Granulocytic intraepithelial lesions
c Venulitis d IgG4-positive plasma cells
Fig. 3 Histological features of autoimmune pancreatitis: a periductal concentric fibrosis (arrow) and periductal infiltrates of lymphocytesand plasma cells (dotted arrow) (haematoxylin and eosin stain, original magnification×18); b granulocytic intraepithelial lesions (arrow)in type 2 autoimmune pancreatitis (haematoxylin and eosin stain, original magnification×72); c venulitis (arrow) (haematoxylin andeosin stain, original magnification×72); d increased number of immunohistochemically IgG4-positive plasma cells (stained red) inautoimmune pancreatitis type 1 (methylene blue counterstain, original magnification×72)
Mann–Whitney U test. Fisher’s exact test was used foranalysis of categorical variables. All tests were two-sidedand statistical significance was assumed at the 5 per centlevel. Statistical evaluation was performed using the SAS®version 9.1 for Windows® (SAS Institute, Cary, NorthCarolina, USA).
Results
Some 72 patients (52 men, 20 women) with AIP wereincluded in the study. None of the patients underwent core
biopsy for preoperative diagnosis. A total of 47 patientshad a pancreatic resection. AIP type 1 was diagnosedin 40 patients, and in 25 the diagnosis was establishedby clinical presentation, imaging and serology (HISORtdiagnostic criteria group B and C) (Fig. 1). In 15 patients,histopathological examination of the resection specimenwas performed (HISORt diagnostic criteria group A).There were 32 patients with AIP type 2, all diagnosed afterpancreatectomy.
Characteristics of the patients with AIP types 1 and 2 aresummarized in Table 1. Patients presented with abdominal
© 2014 BJS Society Ltd www.bjs.co.uk BJS 2014; 101: 1257–1265Published by John Wiley & Sons Ltd

Autoimmune pancreatitis types 1 and 2 1261
Table 1 Characteristics of patients with autoimmune pancreatitistypes 1 and 2
AIP type 1 AIP type 2(n=40) (n=32) P‡
Age (years)* 52 (18–74) 44⋅5 (20–75) 0⋅267§Sex ratio (M : F) 29 : 11 23 : 9 >0⋅999
Clinical presentationAbdominal pain 32 25 >0⋅999Jaundice 13 12 0⋅804Diarrhoea/steatorrhoea 14 8 0⋅444Acute or recurrent acute
pancreatitis20 12 0⋅344
Weight loss 9 7 >0⋅999Site of disease
Head/body 12 27 <0⋅001Tail 1 4 0⋅164Entire gland 27 1 <0⋅001
ImagingDiffuse pancreatic swelling 26 1 <0⋅001Tumour-like pancreatic mass
(suspicious for malignancy)16 30 <0⋅001
SerologyRaised IgG (≥16 g/l) 8 of 38 2 of 24 0⋅048Raised IgG4 (≥140 g/l) 21 of 38 3 of 25 <0⋅001Raised ANA 12 of 38 8 of 25 0⋅792Other raised autoimmune
antibodies20 of 38 10 of 25 0⋅150
Autoimmune-related diseases 13 9 0⋅799Psoriasis 0 2 0⋅194Rheumatism 5 1 0⋅217Autoimmune gastritis 3 2 >0⋅999Hashimoto’s thyroiditis 1 2 0⋅581Hepatitis, SLE 2 2 >0⋅999Sjögren’s syndrome 3 1 0⋅624Inflammatory bowel disease 0 2 0⋅194
Initial therapy†Pancreatic resection 13 31 <0⋅001Corticosteroids 16 1 <0⋅001Best supportive care 11 0 <0⋅001
*Values are median (range). †First 2 weeks after diagnosis. AIP,autoimmune pancreatitis; ANA, antinuclear antibody; SLE, systemiclupus erythematosus. ‡Fisher’s exact test, except §Mann–Whitney U test.
pain and a medical history of acute or recurrent acutepancreatitis. One-third were jaundiced and nine of the 32patients with AIP type 2 had associated autoimmune dis-eases. Patients with AIP type 2 were younger than patientswith type 1 (P = 0⋅267), and more often showed a local-ized pancreatic mass on imaging (30 of 32 versus 16 of 40;P < 0⋅001). Patients with AIP type 2 had a lower preva-lence of raised serum levels of IgG (2 of 24 versus 8 of 38;P = 0⋅048) and IgG4 (3 of 25 versus 21 of 38; P < 0⋅001).
Comparing only histologically confirmed AIP type 1 (15patients) with type 2 (32 patients), a higher proportion ofpatients with AIP type 1 had raised levels of IgG4 (8 of 13versus 3 of 25; P = 0⋅002). Patients with AIP type 2 weresignificantly younger (P = 0⋅005), but all other clinical,
Table 2 Indications for surgery, procedures and outcomes
AIP type 1 AIP type 2(n=40) (n= 32)
Indication for surgical treatmentPancreatic resection to exclude malignancy
(tumour-like mass)9 24
Pain following conservative management ofpancreatitis
2 3
Unsuccessful steroid therapy 0 1Pancreatic duct stenosis* 0 2Cystic pancreatic lesion suspicious for IPMN 1 1Total pancreatectomy for suspected total
gland disease0 1
Cholestasis suspicious for malignantobstructive process
3 0
Operative procedurePancreaticoduodenectomy 11 23Duodenum-preserving pancreatic head
resection2 4
Total pancreatectomy 1 1Distal pancreatectomy 1 4
OutcomesDeath 0 0Mean hospital stay (days) 9⋅5 10Reoperation (postop. bleeding) 0 1Delayed gastric emptying 3 4Pancreatic fistula 0 1Lymphatic fistula 0 1Cholangitis 0 1Intra-abdominal abscess 1 0Surgical-site infection 1 0Pneumonia 0 1Urinary tract infection 1 0
*Pancreatic resection for pancreatic duct stenosis following previouspancreatic surgery (duodenum-preserving pancreatic head resection andleft pancreatic resection). AIP, autoimmune pancreatitis; IPMN,intraductal papillary mucinous neoplasm.
laboratory and imaging data were comparable betweentypes 1 and 2.
Treatment of autoimmune pancreatitis
Most patients with AIP type 1 were treated conservativelyin the first 3 weeks after diagnosis with corticosteroids orbest supportive care, whereas the majority with AIP type2 underwent surgical resection (Table 1). Fifteen of the 40patients with AIP type 1 eventually underwent pancrea-tectomy. The indications for surgical treatment, type ofoperation and outcome within 28 days are summarized inTable 2.
Clinical course after surgery for autoimmunepancreatitis
Follow-up was available for at least 6 months after surgeryfor all but one patient with AIP type 2. After operation, all
© 2014 BJS Society Ltd www.bjs.co.uk BJS 2014; 101: 1257–1265Published by John Wiley & Sons Ltd

1262 S. Fritz, F. Bergmann, L. Grenacher, M. Sgroi, U. Hinz, T. Hackert et al.
Table 3 Comparison between autoimmune pancreatitis and pancreatic ductal adenocarcinoma for each subtype of autoimmunepancreatitis
AIP type 1 PDAC AIP type 2 PDAC
(n=16) (n=32) P (n=30) (n=60) P†
Age (years)* 63 (24–71) 64 (39–71) 0⋅956 45 (16–79) 46 (33–79) 0⋅327‡Sex ratio (M : F) 16 : 0 32 : 0 – 21 : 9 42 : 18 1⋅000
Site of disease 1⋅000 1⋅000
Head/body 14 (88) 28 (88) 27 (90) 54 (90)
Tail 2 (12) 4 (12) 3 (10) 6 (10)
Pain 10 (63) 15 (47) 0⋅369 23 (77) 40 (67) 0⋅465
Jaundice 11 (69) 21 (66) 1⋅000 13 (43) 37 (62) 0⋅114
Weight loss 4 (25) 24 (75) 0⋅002 6 (20) 40 (67) < 0⋅001
Acute pancreatitis 5 (31) 2 (6) 0⋅033 11 (37) 8 (13) 0⋅015
Tumour markers
CA19-9 >37 units/ml 2 (13) 24 (75) <0⋅001 5 (17) 47 (78) < 0⋅001
CEA >2⋅5 μg/l 5 of 15 (33) 19 (59) 0⋅125 5 (17) 23 of 59 (39) 0⋅052
Values in parentheses are percentages unless indicated otherwise; *values are median (range). AIP, autoimmune pancreatitis; PDAC, pancreatic ductaladenocarcinoma; CA, carbohydrate antigen; CEA, carcinoembryonic antigen. †Fisher’s exact test, except ‡Mann–Whitney U test.
patients with AIP type 2 showed a decrease in abdominalpain. Typical disease relapse was characterized by recurrentepisodes of pain and pancreatitis. Six patients with AIP type2 received corticosteroid therapy. Five patients receivedcorticosteroids after operation, including four patients withrecurrent disease. Recurrence developed within a medianof 34 (3–50) months. One patient received corticosteroids4 weeks after surgery as prophylactic therapy and onebefore surgery as initial treatment.
Among the patients with AIP type 1 who underwentpancreatic resection, nine complained of abdominal painbefore the operation. Four of these patients had raisedserum levels of carbohydrate antigen (CA) 19-9 (at least38 units/ml) and/or carcinoembryonic antigen (5 μg/l ormore) in preoperative investigations. Seven of 15 patientshad a raised total serum bilirubin level (1⋅5 mg/dl or more).After surgical resection, seven of nine patients experi-enced relief of pain, two reported unchanged pain intensityafter surgery, and one experienced new-onset mild abdom-inal pain.
Comparison between autoimmune pancreatitisand pancreatic ductal adenocarcinoma
Table 3 shows a comparison of patients with AIP andmatched patients with PDAC. Seven of those withAIP aged between 15 and 32 years were matched withpatients with PDAC up to 20 years older. One 48-year-oldman presented with a mass-forming tumour in the tailof the pancreas that was suspected to be a neoplastictumour, but had features suggestive of AIP. Owing tohis relatively young age and preference, he receivedconservative therapy with corticosteroids for 2 weeks,
which was successful. Weight loss was more com-mon among patients with PDAC than those with AIP.Raised serum CA19-9 levels were more prevalent amongpatients with PDAC. There was no difference in pain orjaundice.
Discussion
Although there have been consensus conferences in Asiaand the USA to establish an exact definition for the diag-nosis of AIP, no clear characterization and classificationof the different subtypes is yet available. To determinethe correct classification for diagnosis of AIP, the Japanesecriteria32, HISORt criteria29, consensus Asian criteria26,Korean criteria33 and the M-ANNHEIM classification34
were reviewed. Although all classifications have overlap-ping criteria, there are important differences. According tothe Japanese diagnostic criteria, typical imaging is manda-tory for the diagnosis of AIP. In the present study of pre-dominantly surgical patients with a histological diagnosis,preoperative imaging was not specific for AIP in manypatients. These patients would not have been diagnosedwith AIP using the Japanese criteria. It has been shownthat the HISORt criteria have the highest sensitivity (92per cent) for the diagnosis of AIP35. These criteria are inaccordance with the 2011 international consensus diagnos-tic criteria for AIP28 and seemed most appropriate for thepresent study.
The most feared scenario is PDAC misdiagnosed as AIP.Recent advances in MDCT, MRI and/or MRCP imagingtechniques have led to high-quality image acquisitionthat has improved the ability confidently to recognizetypical features of AIP17. However, it remains a challenge
© 2014 BJS Society Ltd www.bjs.co.uk BJS 2014; 101: 1257–1265Published by John Wiley & Sons Ltd

Autoimmune pancreatitis types 1 and 2 1263
to differentiate between AIP and pancreatic cancer,particularly in patients with AIP type 2 who present with asuspected malignant lesion. In these patients, late enhance-ment seems to be a key feature and is best detected withMRI. With regard to symptoms, patients with PDAC morefrequently presented with weight loss than those with AIPin the present study. However, no weight loss occurs inone in three patients with pancreatic cancer, particularly inthe earlier stages. Thus, this clinical variable does not seemto be helpful in discriminating between PDAC and AIPin individual patients. Likewise, in patients with a lesionsuspicious for AIP and normal serum tumour marker levels(particularly CA19-9), PDAC cannot be excluded reliably,because a raised level of CA19-9 is found in only 75 percent of patients with PDAC36.
It has been reported that the serum IgG4 level is raisedin 94 per cent of patients with AIP37. In the present study,only 55 per cent of patients (21 of 38) with AIP type 1and 12 per cent (3 of 25) with type 2 had raised IgG4levels, in accordance with a recent report38. IgG4 levelsmay be raised in up to 10 per cent of subjects withoutAIP, which further complicates the differential diagnosis ofpancreatic cancer39. Therefore, IgG4 is not a good markerwith which to identify patients with AIP. Surgical resectionis warranted if there is any doubt about the diagnosis anda tumour-like pancreatic mass is present. Alternatively,corticosteroid therapy can be given for 2 weeks to patientswith typical AIP morphology on MRI, followed by furtherMRI to evaluate the response to steroids. However, thetreatment response always must be evaluated critically, andit has to be kept in mind that serum IgG4 levels may‘improve’ with steroid therapy even though the underlyingdisease is pancreatic cancer6.
The present study has confirmed that histology shouldbe the standard, not only for the diagnosis of AIP,but also to differentiate between the two subtypes. Incontrast to current literature, there were few clinicaldifferences between AIP types 1 and 2 in the presentcohort. High serum levels of IgG4 were found pri-marily in patients with AIP type 1, but three of 25patients with AIP type 2 also had raised serum levels ofIgG4. In contrast to Park and colleagues11, the presentauthors conclude that IgG4 serum levels are helpful nei-ther in diagnosing AIP nor in differentiating betweentypes 1 and 2.
The present study has confirmed that patients with AIPtype 2 are on average 8 years younger than those with AIPtype 1, as shown in an international multicentre study10. Inaccordance with the report of Sah and colleagues12 and theHonolulu consensus document27, there were no differencesin sex distribution between the two AIP subtypes. Nor
was there a difference in extrapancreatic manifestationsbetween AIP types 1 and 2. Therefore, this study cannotconfirm the widely held belief that AIP type 1 is a systemicIgG4-related disease, whereas type 2 is exclusively confinedto the pancreas20.
Beside IgG4 serum levels, there seems to be a differ-ence between AIP types 1 and 2 with regard to mor-phology and location of the inflammatory mass. In thepresent study, patients with AIP type 1 more frequentlyshowed diffuse swelling of the entire pancreas, whereas atumour-like mass mimicking pancreatic cancer was foundin the majority of patients with AIP type 2. Thus, incontrast to Maire and colleagues40, who reported thatsurgery was performed more often in AIP type 1, thepresent results indicate that AIP type 1 can more fre-quently be diagnosed without histology and surgical resec-tion, because this type is usually associated with typicalfeatures of AIP according to the Asian or HISORt crite-ria. In contrast, in patients with AIP type 2 the indicationfor operative versus conservative therapeutic managementremains challenging.
Disclosure
The authors declare no conflict of interest.
References
1 Finkelberg DL, Sahani D, Deshpande V, Brugge WR.Autoimmune pancreatitis. N Engl J Med 2006; 355:2670–2676.
2 Pearson RK, Longnecker DS, Chari ST, Smyrk TC,Okazaki K, Frulloni L et al. Controversies in clinicalpancreatology: autoimmune pancreatitis: does it exist?Pancreas 2003; 27: 1–13.
3 Kim KP, Kim MH, Song MH, Lee SS, Seo DW, Lee SK.Autoimmune chronic pancreatitis. Am J Gastroenterol 2004;99: 1605–1616.
4 Kwon S, Kim MH, Choi EK. The diagnostic criteria forautoimmune chronic pancreatitis: it is time to make aconsensus. Pancreas 2007; 34: 279–286.
5 Chari ST. Current concepts in the treatment ofautoimmune pancreatitis. JOP 2007; 8: 1–3.
6 Gardner TB, Levy MJ, Takahashi N, Smyrk TC, Chari ST.Misdiagnosis of autoimmune pancreatitis: a caution toclinicians. Am J Gastroenterol 2009; 104:1620–1623.
7 Agrawal S, Daruwala C, Khurana J. Distinguishingautoimmune pancreatitis from pancreaticobiliary cancers:current strategy. Ann Surg 2012; 255: 248–258.
8 Kamisawa T, Okazaki K, Kawa S. Diagnostic criteria forautoimmune pancreatitis in Japan. World J Gastroenterol2008; 14: 4992–4994.
© 2014 BJS Society Ltd www.bjs.co.uk BJS 2014; 101: 1257–1265Published by John Wiley & Sons Ltd

1264 S. Fritz, F. Bergmann, L. Grenacher, M. Sgroi, U. Hinz, T. Hackert et al.
9 Chari ST, Kloeppel G, Zhang L, Notohara K, Lerch MM,Shimosegawa T; Autoimmune Pancreatitis InternationalCooperative Study Group (APICS). Histopathologic andclinical subtypes of autoimmune pancreatitis: the Honoluluconsensus document. Pancreas 2010; 39: 549–554.
10 Kamisawa T, Chari ST, Giday SA, Kim MH, Chung JB,Lee KT et al. Clinical profile of autoimmune pancreatitisand its histological subtypes: an international multicentersurvey. Pancreas 2011; 40: 809–814.
11 Park DH, Kim MH, Chari ST. Recent advances inautoimmune pancreatitis. Gut 2009; 58: 1680–1689.
12 Sah RP, Chari ST, Pannala R, Sugumar A, Clain JE, LevyMJ et al. Differences in clinical profile and relapse rate oftype 1 versus type 2 autoimmune pancreatitis.Gastroenterology 2010; 139: 140–148.
13 Zhang L, Chari S, Smyrk TC, Deshpande V, Klöppel G,Kojima M et al. Autoimmune pancreatitis (AIP) type 1 andtype 2: an international consensus study on histopathologicdiagnostic criteria. Pancreas 2011; 40: 1172–1179.
14 Esposito I, Born D, Bergmann F, Longerich T, Welsch T,Giese NA et al. Autoimmune pancreatocholangitis,non-autoimmune pancreatitis and primary sclerosingcholangitis: a comparative morphological andimmunological analysis. PLoS One 2008; 3: e2539.
15 Zhang L, Notohara K, Levy MJ, Chari ST, Smyrk TC.IgG4-positive plasma cell infiltration in the diagnosis ofautoimmune pancreatitis. Mod Pathol 2007; 20: 23–28.
16 Klöppel G, Lüttges J, Sipos B, Capelli P, Zamboni G.Autoimmune pancreatitis: pathological findings. JOP 2005;6(Suppl): 97–101.
17 Sahani DV, Sainani NI, Deshpande V, Shaikh MS,Frinkelberg DL, Fernandez-del Castillo C. Autoimmunepancreatitis: disease evolution, staging, response assessment,and CT features that predict response to corticosteroidtherapy. Radiology 2009; 250: 118–129.
18 Morselli-Labate AM, Pezzilli R. Usefulness of serum IgG4in the diagnosis and follow up of autoimmune pancreatitis: asystematic literature review and meta-analysis.J Gastroenterol Hepatol 2009; 24: 15–36.
19 Chari ST, Smyrk TC, Levy MJ, Topazian MD, TakahashiN, Zhang L et al. Diagnosis of autoimmune pancreatitis: theMayo Clinic experience. Clin Gastroenterol Hepatol 2006; 4:1010–1016.
20 Deshpande V, Gupta R, Sainani N, Sahani DV, Virk R,Ferrone C et al. Subclassification of autoimmunepancreatitis: a histologic classification with clinicalsignificance. Am J Surg Pathol 2011; 35: 26–35.
21 Klöppel G. Chronic pancreatitis, pseudotumors and othertumor-like lesions. Mod Pathol 2007; 20(Suppl 1):S113–S131.
22 Notohara K, Burgart LJ, Yadav D, Chari S, Smyrk TC.Idiopathic chronic pancreatitis with periductallymphoplasmacytic infiltration: clinicopathologic features of35 cases. Am J Surg Pathol 2003; 27: 1119–1127.
23 Ectors N, Maillet B, Aerts R, Geboes K, Donner A,Borchard F et al. Non-alcoholic duct destructive chronicpancreatitis. Gut 1997; 41: 263–268.
24 Zamboni G, Lüttges J, Capelli P, Frulloni L, Cavallini G,Pederzoli P et al. Histopathological features of diagnosticand clinical relevance in autoimmune pancreatitis: a study on53 resection specimens and 9 biopsy specimens. VirchowsArch 2004; 445: 552–563.
25 Rehnitz C, Klauss M, Singer R, Ehehalt R, Werner J,Büchler MW et al. Morphologic patterns of autoimmunepancreatitis in CT and MRI. Pancreatology 2011; 11:240–251.
26 Otsuki M, Chung JB, Okazaki K, Kim MH, Kamisawa T,Kawa S et al. Asian diagnostic criteria for autoimmunepancreatitis: consensus of the Japan–Korea Symposium onAutoimmune Pancreatitis. J Gastroenterol 2008; 43:403–408.
27 Chari ST, Kloeppel G, Zhang L, Notohara K, Lerch MM,Shimosegawa T. Histopathologic and clinical subtypes ofautoimmune pancreatitis: the Honolulu consensusdocument. Pancreatology 2010; 10: 664–672.
28 Shimosegawa T, Chari ST, Frulloni L, Kamisawa T, KawaS, Mino-Kenudson M et al.; International Association ofPancreatology. International consensus diagnostic criteriafor autoimmune pancreatitis: guidelines of the InternationalAssociation of Pancreatology. Pancreas 2011; 40: 352–358.
29 Chari ST. Diagnosis of autoimmune pancreatitis using itsfive cardinal features: introducing the Mayo Clinic’sHISORt criteria. J Gastroenterol 2007; 42(Suppl 18): 39–41.
30 Kamisawa T, Imai M, Egawa N, Tsuruta K, Okamoto A.Serum IgG4 levels and extrapancreatic lesions inautoimmune pancreatitis. Eur J Gastroenterol Hepatol 2008;20: 1167–1170.
31 Forcione DG, Brugge WR. New kid on the block?Autoimmune pancreatitis. Best Pract Res Clin Gastroenterol2010; 24: 361–378.
32 Okazaki K, Kawa S, Kamisawa T, Naruse S, Tanaka S,Nishimori I et al.; Research Committee of IntractableDiseases of the Pancreas. Clinical diagnostic criteria ofautoimmune pancreatitis: revised proposal. J Gastroenterol2006; 41: 626–631.
33 Kim KP, Kim MH, Kim JC, Lee SS, Seo DW, Lee SK.Diagnostic criteria for autoimmune chronic pancreatitisrevisited. World J Gastroenterol 2006; 12: 2487–2496.
34 Schneider A, Löhr JM, Singer MV. The M-ANNHEIMclassification of chronic pancreatitis: introduction of aunifying classification system based on a review of previousclassifications of the disease. J Gastroenterol 2007; 42:101–119.
35 Naitoh I, Nakazawa T, Ohara H, Ando T, Hayashi K,Okumura F et al. Comparative evaluation of the Japanesediagnostic criteria for autoimmune pancreatitis. Pancreas2010; 39: 1173–1179.
36 Hartwig W, Strobel O, Hinz U, Fritz S, Hackert T, Roth Cet al. CA19-9 in potentially resectable pancreatic cancer:
© 2014 BJS Society Ltd www.bjs.co.uk BJS 2014; 101: 1257–1265Published by John Wiley & Sons Ltd

Autoimmune pancreatitis types 1 and 2 1265
perspective to adjust surgical and perioperative therapy. AnnSurg Oncol 2013; 20: 2188–2196.
37 Hirano K, Kawabe T, Yamamoto N, Nakai Y, Sasahira N,Tsujino T et al. Serum IgG4 concentrations in pancreaticand biliary diseases. Clin Chim Acta 2006; 367: 181–184.
38 Kamisawa T, Takuma K, Tabata T, Inaba Y, Egawa N,Tsuruta K et al. Serum IgG4-negative autoimmunepancreatitis. J Gastroenterol 2011; 46: 108–116.
39 Ghazale A, Chari ST, Smyrk TC, Levy MJ, Topazian MD,Takahashi N et al. Value of serum IgG4 in the diagnosis ofautoimmune pancreatitis and in distinguishing it frompancreatic cancer. Am J Gastroenterol 2007; 102: 1646–1653.
40 Maire F, Le Baleur Y, Rebours V, Vullierme MP, CouvelardA, Voitot H et al. Outcome of patients with type 1 or 2autoimmune pancreatitis. Am J Gastroenterol 2011; 106:151–156.
Snapshot quiz
Snapshot quiz 14/13
Question: What does this photograph of the perineum and abdominal CT show?
The answer to the above question is found on p. 1279 of this issue of BJS.
Al-Choule H, Ilum L, Sparre P, Olaison G: Department of Surgery, Holbaek Hospital, Smedelundsgade 60, Holbæk 4300, Denmark(e-mail: [email protected])
Snapshots in Surgery: to view submission guidelines, submit your snapshot and view the archive, please visitwww.bjs.co.uk
© 2014 BJS Society Ltd www.bjs.co.uk BJS 2014; 101: 1257–1265Published by John Wiley & Sons Ltd