Embed Size (px)
Citation preview

...........................................................................................................................
Diagnosing ectopic pregnancy andcurrent concepts in the managementof pregnancy of unknown locationE. Kirk1,2,*, C. Bottomley3, and T. Bourne2,4
1North Middlesex University Hospital, Sterling Way, London N18 1QX, UK 2Queen Charlotte’s & Chelsea Hospital, Imperial College, Du CaneRoad, London W12 0HS, UK 3Chelsea and Westminster Hospital, Fulham Road, London SW10 9NH, UK 4Department of Development andRegeneration, University Hospitals Leuven, Campus Gasthuisberg, KU Leuven, B-3000 Leuven, Belgium
*Correspondence address. E-mail: [email protected]
Submitted on April 10, 2013; resubmitted on July 31, 2013; accepted on August 15, 2013
table of contents
† Introduction† Methods† Tubal ectopic pregnancy
History and presentationUltrasound diagnosisSurgical diagnosis
† Non-tubal ectopic pregnancyHeterotopic pregnancy
† Pregnancy of unknown locationDiagnosisClinical outcomesClinical management
† Future work† Conclusion
background: A diagnosis of ectopic pregnancy (EP) is primarily achieved using transvaginal ultrasonography (TVS). Pregnancy of unknownlocation (PUL) is the term used to categorize a pregnancy in a woman with a positive pregnancy test when no pregnancy has been visualized usingTVS. This review appraises current tools for the diagnosis of EP, describes the diagnostic criteria for non-tubal EP and reviews the literature on theclinical management of PUL.
methods: We performed a targeted search using the PubMed database. All articles published in the English language from January 1984 toMarch 2013 were screened for eligibility.
results: Using TVS to diagnose EP is highly sensitive (87–99%) and specific (94–99.9%). Variations exist in the criteria used for ultrasounddiagnosis. Studies report that between 5 and 42% of women seen for ultrasound assessment with a positive pregnancy test have a PUL. For PUL,measurements of serum human chorionic gonadotrophin (hCG) and progesterone are used to predict pregnancy viability and therefore give anindication of the risk of an EP. Only 6–20% of PUL are subsequently diagnosed with EP. Non-tubal EPs are relatively uncommon, difficult to diag-nose and result in disproportionate morbidity and mortality.
conclusions: Access to expertise and equipment for high-quality TVS means the majority of women with EP in developed countries can bediagnosed rapidly and accurately. Identifying PUL, which are low risk and therefore requiring less follow-up, finding better serum markers for EPand safely identifying women who do not require intervention for EP are the current diagnostic challenges.
Key words: ectopic pregnancy / pregnancy of unknown location / transvaginal ultrasonography / prediction models / expectant management
& The Author 2013. Published by Oxford University Press on behalf of the European Society of Human Reproduction and Embryology. All rights reserved.For Permissions, please email: [email protected]
Human Reproduction Update, Vol.20, No.2 pp. 250–261, 2014
Advanced Access publication on October 6, 2013 doi:10.1093/humupd/dmt047
by guest on March 1, 2016
http://humupd.oxfordjournals.org/
Dow
nloaded from

IntroductionAny pregnancy implanted outside the endometrial cavity is defined as anectopic pregnancy (EP). Most are located within the Fallopian tube. Theincidence of EP varies from 11 to 20 per 1000 live births in developedcountries (Centres for Disease Control, 1995; Boufous et al., 2001;Bakken and Skjeldestad, 2003; Lewis 2007), though it is as high as 4%in assisted conception populations (Fernandez and Gervaise, 2004).The case fatality rate in developed countries has declined over recentyears, suggesting that earlier diagnosis and better treatment have madean impact (O’Herlihy, 2011).
Diagnosis based on clinical signs of tubal rupture (hypovolaemicshock) is now uncommon and transvaginal ultrasonography (TVS) isthe primary diagnostic tool for clinically stable women with a suspectedEP (Jurkovic and Wilkinson, 2011). Data from a specialist early pregnancyunit show that up to 73.9% of women with an EP may be diagnosed on aninitial TVS assessment (Kirk et al., 2008) and 94% are diagnosed prior tosurgical intervention (Condous et al., 2005a).
Non-tubal EPs although relatively uncommon are associated withhigher morbidity and mortality. Pregnancy of unknown location (PUL)is the term used to classify a pregnancy in women with a positiveurinary pregnancy test when an initial TVS detects neither an intrauterinenor extrauterine pregnancy. A small proportion of women classified witha PUL have an underlying EP.
The aim of this review is first to detail the diagnostic criteria for bothtubal and non-tubal EP. The secondary aim is to define the use of theterm ‘PUL’ and describe how to use biochemical markers to triagewomen to appropriate follow-up when they have a PUL.
MethodsWe performed a targeted search using the PubMed database employingcombinations of the following search terms: EP, tubal/cornual/interstitial/Caesarean scar/intramural/ cervical/ abdominal EP, PUL. All articlespublished in the English language from January 1984 to March 2013 wereselected. The restriction to articles after 1984 was due to this being whenTVS became commonly used in clinical practice.
All potential papers were screened for eligibility by review of the title andabstract, to assess relevance in terms of focus on either diagnosis of any typeof EP or an original or review paper on any aspect of PUL. The full text ver-sions of all papers selected in the screening process were read and assessedfor relevance. Reference listsof all primary and reviewarticles were examinedfor any relevant citations (from any year), which may have been missed in theoriginal key word search.
One main author performed the search for each specific section [tubal EPdiagnosis (CB), non-tubal EP diagnosis (EK), PUL (EK)] with all three authorssubsequently rechecking the included articles for relevance.
Tubal Ectopic PregnancyMost (93–98%) EPs are located within the Fallopian tube. Of these, 13%are isthmic, 75% ampullary and 12% fimbrial (Bouyeret al., 2002; Walker,2007; Varma and Gupta, 2009). The aetiology remains poorly definedbut is likely to be a combination of impaired embryo–tubal transportand alterations in the tubal environment allowing early implantation(Shaw et al., 2010a, b).
History and presentationRisk factors for tubal EP are well described, with highest risk associatedwith tubal damage following surgery or infection (especially Chlamydiatrachomatis), smoking and IVF (Ankum et al., 1996; Tay et al., 2000;Bouyer et al., 2003; Shaw et al., 2010a, b; Shaw et al., 2011). Howeveralthough the attributable risk of these factors is 0.76 (Bouyer et al.,2003), many women with EP have no identifiable risk factors and mostwomen with a risk factor do not have an EP.
The triad of pain, vaginal bleeding and amenorrhoea was historicallyused to suspect a diagnosis of EP (Weckstein et al., 1985). These symp-toms, with or without syncope, shoulder tip pain and shock, generally ledto surgical intervention. Now, history and physical examination alonerarely leads to the diagnosis or exclusion of an EP, with most diagnosedearlier in the course of the disease. One-third of women with an EP haveno clinical signs and up to 10% have no symptoms(Kaplan et al., 1996; Tayet al., 2000). The symptoms of EP are often non-specific and difficult todifferentiate fromthose of other gynaecological, gastrointestinal and uro-logical disorders, including appendicitis, salpingitis, corpus luteum cystrupture, miscarriage, adnexal torsion or urinary tract infection.
The amount of bleeding associated with EP varies, although classicallythe patient will complain of ‘spotting’. Heavy bleeding, in the absence offurther TVS and hCG assessment, may lead to a clinical misdiagnosis ofmiscarriage. Abdominal pain is often absent or a late finding, probablydue to earlier recognition of pregnancy from the use of highly sensitivecommercially available urinary pregnancy tests and to easy access toTVS. The majority of women with abdominal pain in early pregnancydo not have an EP (Bottomley et al., 2009).
Less common features of EP include nausea, vomiting and diarrhoea.In ruptured EP, there may be abdominal distension and tenderness, peri-tonism and haemorrhagic shock. A diagnosis of EP should be consideredin all women of reproductive age with a sudden onset of abdominal painor gastrointestinal symptoms (Lewis, 2007).
Ultrasound diagnosisThe use of ultrasonography to diagnose EP was first described over40 years ago (Kobayashi et al., 1969). However until the 1980s, the ultra-sound ‘diagnosis’ was based on an inability to visualize an intrauterinepregnancy (IUP) rather than definitive identification of an extrauterinepregnancy. This was considered an indication for laparoscopy, with an in-evitable high rate of ‘negative laparoscopy’ (Brown and Doubilet, 1994).
The use of TVS has changed the diagnostic approach to one based onvisualizing the ectopic mass (Condous et al., 2005a). TVS has beendemonstrated to be superior to transabdominal ultrasound (TAS),with sensitivities for the diagnosis of EP in early studies of 77–80% forTAS and 88–90% for TVS (Cacciatore et al., 1989; Valenzano et al.,1991). As expertise and equipment has improved, the sensitivity ofTVS for the diagnosis of EP has increased further (Condous et al.,2005a; Kirk et al., 2007a).
The accuracy of a diagnosis of tubal EP using ultrasonographyIt is important to appreciate that not all EP will be seen using TVS and cer-tainly not on one visit. A prospective study on over 5000 consecutivewomen including 120 tubal EPs found that 73.9% were visualized onTVS when the patient first attended the clinic (Kirk et al., 2007a). Theremaining cases were not seen and were initially classified as PUL.Most EPs were then visualized on subsequent follow-up scans (prior to
Current concepts in ectopic pregnancy and PUL 251
by guest on March 1, 2016
http://humupd.oxfordjournals.org/
Dow
nloaded from

surgery) making the overall sensitivity of TVS 98.3%. A number of otherstudies have also assessed the accuracy of TVS for diagnosing tubal EP.They too report high sensitivities of 87.0–99.0% and specificities of94.0–99.9% (Braffman et al., 1994; Shalev et al., 1998; Atri et al., 2003;Condous et al., 2005a; Kirk et al., 2008). A meta-analysis of 2216women with an EP concluded that visualizing an adnexal mass separatefrom the ovary using TVS had a sensitivity of 84.4% and specificity of98.9% (Brown and Doubilet, 1994).
A study comparing the features of women with an EP who had a diag-nosis made on the initial scan compared with those first classified as aPUL found that EPs in the PUL group were too small and probably tooearly in their natural history to be visualized, rather than being ‘missed’(Kirk et al., 2008). Suboptimal quality ultrasound equipment, operator in-experience, increased maternal body mass index, uterine fibroids orovarian pathology may also make visualization of an EP difficult.
Criteria for the ultrasound diagnosis of tubal EPEndometrium. There is no specific endometrial appearance or thicknessthat reliably supports a diagnosis of EP (Mehta et al., 1999). In up to 20%cases a collection of fluid may be seen within the endometrial cavity, clas-sically referred to as a ‘pseudosac’ (Marks et al., 1979; Frates and Laing,1995; Benson et al., 2013). However, an hypoechoic area in the endo-metrial cavity is far more likely to be an early IUP (Doubilet andBenson, 2010), and so a presumptive diagnosis of EP should not bemade solely on the basis of this finding.
Free pelvic fluid. A small amount of anechoic free fluid in the Pouch ofDouglas is commonly found with both intrauterine and ectopic gesta-tions (Nyberg et al., 1991). The presence of echogenic fluid has beenreported in 28–56% of women with an EP (Fleischer et al., 1990;Nyberg et al., 1991). This correlates well with the surgical findings of hae-moperitoneum (Sickler et al., 1998), but does not confirm tubal rupture,as blood commonly leaks from the fimbrial tube. The amount of echo-genic fluid visualized in the pelvis correlates closely with findings atsurgery. As a rule of thumb, if fluid reaches the fundus of the uterus oris present in the utero-vesical pouch, it is significant. A further markerof serious intra-abdominal bleeding is the presence of fluid in Morrison’spouch between the liver and the kidney. This simple examination formsthe basis of the focused assessment by sonography for trauma (FASTscan) used in emergency departments (Scalea et al., 1999).
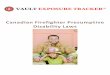
Tubal EP. Tubal EPs are usually positively diagnosed using ultrasound byvisualizing an adnexal mass that moves separate to the ovary. The mostcommon finding, in around 60% of cases, is an inhomogeneous or a non-cystic adnexal mass sometimes known as the ‘blob’ sign (Braffman et al.,1994; Shalev et al., 1998; Atri et al., 2003; Condous et al., 2005a; Kirket al., 2008) (Fig. 1). A meta-analysis of 10 studies found that this wasthe most effective criterion on which to base the diagnosis of a tubal EP(Brown and Doubilet, 1994), with a specificity, positive predictive value,sensitivity and negative predictive value of 98.9%, 96.3%, 84.4% and94.8%, respectively. The mass is generally spherical, but a more tubular ap-pearance may be seen if bleeding creates a haematosalpinx.
In around 20% of cases it may be possible to visualize an empty extra-uterine gestational sac or ‘bagel sign’ (Condous et al., 2005a; Kirk et al.,2008). In another 20%, this sac may contain a yolk sac and/or an embry-onic pole that may or may not have cardiac activity (see Fig. 1). The term‘viable ectopic’ is applied when embryonic cardiac activity is visualized.
Some authors consider that a definitive diagnosis of tubal EP can onlybe made when an extra-uterine gestation sac containing a yolk sac or em-bryonic pole is visualized (Barnhart et al., 2011). A recent consensus onnomenclature proposed that the term ‘definite EP’ be used if a yolk sacand/or embryo (with or without cardiac activity) is seen (Barnhartet al., 2011). The term ‘probable EP’ is suggested if an inhomogeneousmass or an extrauterine sac-like structure is visualized. Using this classi-fication, the specificity of ultrasound to detect EP is very high, but the sen-sitivity is lower as the inhomogeneous and empty sac masses are notcounted as definitive EPs.
The rationale for reserving the term ‘definite EP’ to those with embry-onic structures is that false-positive diagnoses of EP, though rare, arefound even when the criteria for diagnosis are very strict (Krag Moelleret al., 2009), likely due to other pathology such as the presence of ped-unculated or broad ligament fibroids, pelvic inflammation or highly exo-phytic ovarian cysts. This more conservative approach is linked to theneed for a very high level of diagnostic certainty in the event thatmedical treatment is being considered. If methotrexate is used, a false-positive diagnosis of EP may lead to the inadvertent termination of an un-detected IUP (Nurmohamed et al., 2011), or severe abnormality in anysurviving pregnancy. The American College of Obstetricians and Gyne-cologists (ACOG) recommend that methotrexate only be administered
Figure 1 Transvaginal scan images of tubal ectopic pregnancies:(a) an inhomogeneous mass and (b) a yolk sac and fetal pole in an extra-uterine sac.
252 Kirk et al.
by guest on March 1, 2016
http://humupd.oxfordjournals.org/
Dow
nloaded from

to women with a ‘probable ectopic pregnancy‘ (as opposed to ‘defini-tive’) in cases where the hCG has been serially monitored to confirmthe change is incompatible with an IUP. The difficult issue is how todefine ‘incompatible’. The ACOG defines this as a ,53% rise in hCGover 48 h (Agency for Healthcare Research and Quality, 2008).However, Condous et al. showed that a viable IUP may have an hCGrise of significantly ,50%, so giving methotrexate with an hCG rise of53% could possibly lead to termination of a wanted pregnancy.An hCG rise of ,35% is now considered a safer definition of non-viabilityin women with probable EP when methotrexate is being considered(Seeber et al., 2006).
The lower threshold of an initial ultrasound finding of an inhomogen-eous mass or empty sac structure is reasonable for the majority ofwomen, when surgical or expectant management is proposed, as themanagement options do not jeopardize any possible intrauterine gesta-tion. The criteria for ultrasound diagnosis of a tubal EP are summarized inTable I.
Against this background the recent guidelines in the UK published bythe National Institute for Clinical Excellence are a major concern. Thisguidance recommends the use of methotrexate as the first-line treat-ment for EP; however, no consideration is given to definitively excludingthe possibility of a viable IUP. The presumption therefore is that a false-positive diagnosis of EP is not possible, which is clearly wrong. If followed,
in the authors’ opinions, this guidance will inevitably lead to cases where aviable intauterine pregnancy is terminated in error (Newbatt et al., 2012;Bourne et al., 2013).
Pulsed Doppler ultrasound has been examined as a tool for diagnosingEP. However, the range of values for vascular indices associated with anEP means that there is significant overlap with those associated withangiogenesis within a corpus luteum (Bourne et al., 1991; Jurkovicet al., 1992; Pellerito et al., 1995). Currently Doppler is not consideredto significantly contribute to the diagnosis of EP.
Surgical diagnosisMost surgery for EP is nowcarried out as a therapeutic procedureafter anEP has been diagnosed with TVS (Jurkovic and Wilkinson, 2011). Diag-nostic surgery is generally reserved for women presenting with signs ofan acute abdomen and hypovolaemic shock. A surgical diagnosis mayalso be made in women with a PUL who become symptomatic. Althoughlaparoscopy is still considered by some to be the ‘gold standard’ for diag-nosing EP, this position is now untenable given the high predictive value ofultrasound (Condous et al., 2005a), the widespread use of conservativemanagement strategies and the clinical reality that false-positive and-negative diagnoses of EP occur even at surgery (Li et al., 1991; Atriet al., 1996). If an EP cannot be visualized with TVS performed by an
.............................................................................................................................................................................................
Table I Sonographic criteria for the diagnosis or ectopic pregnancies.
Type of EP Sonographic criteria
Tubal (1) Empty uterine cavity(2) An inhomogeneous adnexal mass or, an empty extra-uterine gestation sac or a yolk sac or fetal pole+ cardiac activity
in an extra-uterine sac
Interstitial (1) Empty uterine cavity(2) Products of conception/gestation sac located in the interstitial (intramyometrial) portion of the tube
surrounded by a continuous rim of myometrium(3) Interstitial line sign (thin echogenic line extending from a central uterine cavity echo to the periphery of the interstitial sac)
Cornual (1) A single interstitial portion of the Fallopian tube in the main uterine body(2) Products of conception/gestation sac mobile and separate from the uterus surrounded by the myometrium(3) Vascular pedicle joining the gestational sac to the unicornuate uterus
Cervical (1) Empty uterine cavity(2) Barrel shaped cervix(3) Products of conception/gestation sac below the level of the internal cervical os(4) Negative sliding organ sign
Caesarean section scar (1) Empty uterine cavity(2) Products of conception/gestation sac located anteriorlyat the level of the internal os covering the presumed site of the previous
lower segment Caesarean section scar(3) Negative sliding organ sign(4) Evidence of peritrophoblastic flow on color Doppler examination
Ovarian (1) Empty uterine cavity(2) Cystic structure with a wide echogenic ring on or within the ovary, generally seen surrounded by ovarian
cortex and separate from the corpus luteum
Intramural (1) Empty uterine cavity(2) Products of conception/gestation sac completely surrounded by myometrium and separate from the endometrial cavity
Abdominal (1) Empty uterine cavity(2) No evidence of a dilated Fallopian tube or complex adnexal mass(3) Gestation sac surrounded by loops of bowel and separated by peritoneum(4) Wide mobility similar to fluctuation of the sac
Ackerman et al. (1993); Timor-Tritsch et al. (1994); Jurkovic et al. (1996); Jurkovic et al. (2003); Gerli et al. (2004); Jermy et al. (2004); Comstock et al. (2005); Condous et al. (2005a);Laing(2007); Jurkovic and Marvelos (2007).
Current concepts in ectopic pregnancy and PUL 253
by guest on March 1, 2016
http://humupd.oxfordjournals.org/
Dow
nloaded from

experienced operator, there is a low chance of finding a visible EP atlaparoscopy. In one study 4.5% (2/44) of women were subsequentlydiagnosed with an EP following a negative laparoscopy (Li et al., 1991).Another study reported a 3–4% false-negative rate and 5% false-positiverate associated with laparoscopy (Atri et al., 1996).
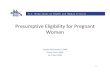
Non-tubal Ectopic PregnancyUp to 7% of EP are located outside the Fallopian tube (Bouyer et al.,2002). Although relatively rare, these pregnancies are responsible for sig-nificant morbidity and mortality (Lewis, 2007). The diagnostic criteria fornon-tubal EP are shown in Table I. Although these criteria exist, there area paucity of data relating to their diagnostic performance, and care mustbe taken to avoid misdiagnosis. A common example is of a normal IUPimplanted laterally in an arcuate uterus being misdiagnosed as an intersti-tial pregnancy. Furthermore, new developments in ultrasonography haverendered some of these criteria redundant. Using 3D ultrasound, acoronal view of the uterus can be obtained. This view means that invari-ably a connection can be seen between the endometrial cavity and inter-stitial portion of the Fallopian tube (Fig. 2). In the future it seems highly
likely that the use of 3D ultrasound in this context will be an integralpart of diagnostic guidance (Lawrence and Jurkovic, 1999).
The classification of a Caesarean section scar pregnancy may also bedifficult as it is not unusual for a gestation sac to implant over a scar,without extending into the scar (Naji et al., 2013). Given these uncertain-ties, there is an argument that all such pregnancies over or in a scar shouldbe referred to specialist centres both to confirm the diagnosis and fortreatment.
Heterotopic pregnancyA heterotopic pregnancy occurs when any form of EP is found simultan-eously with an IUP (Fig. 3). The incidence of heterotopic pregnancy innatural conceptions was originally estimated to be 1 in 30 000 pregnan-cies (DeVoe and Pratt, 1948). Clinically they are associated with assistedreproductive techniques, where the incidence is thought to be 1–3 in100 pregnancies (Molloy et al., 1990; Fernandez and Gervaise, 2004).The risk increases in proportion to the number of embryos transferredwith IVF. If more than 4 embryos are transferred the risk has beenquoted as 1 in 45 (Dor et al., 1991). In clinical practice, it is importantto remember that visualizing an IUP does not exclude the presence ofa further pregnancy elsewhere in the pelvis, especially if the pregnancyis the result of IVF.
Figure 2 Interstitial ectopic pregnancy: (a) 2D grey-scale image and(b) 3D image.
Figure 3 Heterotopic pregnancy: (a) 2D grey-scale image and (b) 3Dimage. The two images are not of the same case.
254 Kirk et al.
by guest on March 1, 2016
http://humupd.oxfordjournals.org/
Dow
nloaded from

Pregnancy of unknown location‘Pregnancy of unknown location’ (PUL) is a descriptive term used to clas-sify a pregnancy when a TVS has shown no signs of either an intrauterineor extrauterine pregnancy or retained products of conception. Studiesreport that 5–42% of women attending for an ultrasound assessmentin early pregnancy will be classified as having a PUL (Hahlin et al., 1995;Cacciatore et al., 1998; Banerjee et al., 1999, 2001; Condous et al.,2004a). Reports from specialized early pregnancy units describe lowerPUL rates of 8–10% (Kirk et al., 2007b; Cordina et al., 2011). A consen-sus statement produced by the International Society of Ultrasound inObstetrics and Gynecology stated that modern units should try to main-tain a PUL rate of ,15% (Condous et al., 2006a). The PUL rate may beinfluenced by a number of factors but in particular the quality of the ultra-sonography performed within a unit is important. Accordingly, it hasbeen proposed as a benchmark for judging the performance of any facilityoffering early pregnancy ultrasound.
DiagnosisPUL is not a diagnosis. It is a term used to classify a pregnancy until thefinal clinical outcome is known. Any woman classified as having a PULneeds follow-up to determine the final clinical outcome, which may bean ongoing viable IUP, a failed pregnancy, an EP or rarely a persistingPUL. The need for appropriate clinical supervision and follow-up whencaring for women with a PUL was highlighted in the 2006–2008Centre for Maternal and Child Enquiries report where a maternaldeath secondary to a ruptured EP occurred in a woman where a preg-nancy described as a PUL was subsequently inappropriately managed(O’Herlihy, 2011). Current thinking has moved away from establishingpregnancy location towards triaging PUL according to the risk of harmto the patient. Accordingly probable EPs are designated as high riskand probable IUP are classified as low risk alongside PUL that are des-tined to fail. In this way appropriate follow-up arrangements can bemade that reflect the chance of a complication occurring.
Before a pregnancy can be classified as a PUL, it follows that thereneedto be clear criteria for definitively diagnosing IUP and EP. Unfortunately,these criteria vary worldwide which partly explains why PUL rates andsubsequent outcomes differ both between units and in the literature.In a recent review, there was such clinical heterogeneity in the definitionof PUL outcome, that only data for the outcome EP could be analyzed(Van Mello et al., 2012). A consensus paper with authors from theUSA, UK, Belgium, the Netherlands and Australia also highlighted thisproblem (Barnhart et al., 2011). The issue relates to when it is consideredsafe to make a definitive diagnosis of a pregnancy in the uterus or tube.These areas of uncertainty are outlined below.
PUL or early IUP?When a small empty intrauterine gestational sac-like structure is visua-lized on TVS, the concern is that it may not be a true gestation sac buta collection of fluid in the endometrial cavity (‘pseudosac’). In theabsence of any visible embryonic structures, some operators will classifysuch a finding as a PUL. To overcome this, Barnhart et al in their consen-sus paper suggested the following new categorization system for initialultrasound findings:
(i) Definite EP: extrauterine gestational sac with yolk sac and/orembryo (with or without cardiac activity).
(ii) PUL-probable EP: inhomogeneous adnexal mass or extrauterinesac-like structure.
(iii) ‘True’ PUL: no signs of either an intrauterine or extrauterine preg-nancy on TVS.
(iv) PUL-probable IUP: intrauterine gestational sac-like structure.(v) Definite IUP: intrauterine gestational sac with yolk sac and/or
embryo (with or without cardiac activity).
Generally in the USA and some units in the UK where the broader def-inition of PUL is used encompassing points 2, 3, and 4 above, a small intra-uterine gestational sac without obvious embryonic structures would beclassified as a PUL. In other units, the same findings would be regarded asconfirmation of an intrauterine gestational sac.
PUL or miscarriage?When a woman presents with a PUL and a history of heavy bleeding it istempting to make a diagnosis of complete miscarriage. However, the evi-dence shows that such cases should be classified as PUL and evaluatedfurther unless a prior ultrasound has confirmed an IUP. In a study of152 women with such a history, 5.9% were subsequently found tohave an underlying EP (Condous et al., 2005b).
Difficulty also arises in women found to have a slightly thickened or ir-regular endometrium with a possible small amount of retained productsof conception. We know that measurements of endometrial thickness orvolume on TVS are not good tests for predicting the finding of chorionicvilli at curettage, and so are unreliable for diagnosing an incomplete mis-carriage (Sawyer et al., 2007), although the use of power Doppler hasbeen reported as being useful for confirming the presence of significantretained products in the cavity (Casikar et al., 2012). There is currentlyno consensus on the correct management of these cases. Where no de-finitive retained products of conception are seen, it would seem appro-priate to adopt the safer approach and manage these cases as PUL, thusalso avoiding the possibility of curettage in the presence of a potentiallyviable early IUP. It follows that some units with very high PUL rates maybe managing a larger proportion of incomplete miscarriages as PULbecause of this diagnostic uncertainty.
PUL or EP?In some protocols, the criteria to definitively diagnose an EP require anextra-uterine gestational sac with a yolk sac or embryo to be visualized(Barnhart et al., 2011). Therefore when an inhomogeneous adnexalmass is seen, an initial classification of PUL will be made. This will leadto more EP being classified as PUL. If a sonographer feels unable to cat-egorically make a diagnosis of EP, it is now recommended that a diagnosisof ‘probable EP’ be made (Barnhart et al., 2011).
These different approaches to the classification of PUL reflect the clin-ical environment of a given unit. If the quality of ultrasound is inconsistent,patient compliance low, and risk of litigation high, then criteria used tomake a definitive diagnosis of an IUP or EP will be more exacting. Theresult will be that more women will be classified as having a PUL andundergo some sort of supervised follow-up. When ultrasound findingscan be relied upon and patients can be expected to return to the clinicin the event of problems, the balance of risk changes and diagnostic cri-teria may be looser. The stricter criteria for making a definitive diagnosisof EP become particularly relevant when treatment with methotrexate isbeing considered.
Current concepts in ectopic pregnancy and PUL 255
by guest on March 1, 2016
http://humupd.oxfordjournals.org/
Dow
nloaded from

Clinical outcomesThere are four possible clinical outcomes once a pregnancy has beenclassified as a PUL: an IUP or failed PUL (low risk of complications) oran EP or persistent PUL (higher risk of complications). The concern forclinicians when a woman is classified with a PUL is that a diagnosis ofEP may have been missed. Hence, previously the clinical scenario wenow call a PUL would often be categorized as a ‘query ectopic’ or‘ectopic until proved otherwise’. This is entirely inappropriate as theterms are clearly not synonymous. Evidence shows that from 6% andat most 20% of women with a PUL have an EP (Hahlin et al., 1995;Banerjee et al., 1999, 2001; Condous et al., 2007a, b; Kirk et al.,2007b). Between 30 and 47% of PUL are ultimately diagnosed with anongoing IUP (Kirk et al., 2006, 2007b; Condous et al., 2007a; Bignardiet al., 2010) with the majority (50–70%) found to be failing pregnancieswhere the location is never confirmed (Banerjee et al., 1999, 2001;Condous et al., 2006a, 2007a; Kirk et al., 2007b). It is therefore clearthat most women with PUL are not at risk of significant complications.Recent management protocols have begun to reflect this, with the em-phasis on triage according to risk rather than establishing pregnancy loca-tion (Cordina et al., 2011; Van Calster et al., 2013).
A very small proportion of women with a PUL may be given the de-scriptive term of ‘persisting PUL’. In such cases the hCG level does notspontaneously decline and no intrauterine or EP is identified on follow-upTVS (Condous et al., 2004a). These are likely to be either a small EP thathas not been visualized or retained trophoblast in the endometrial cavity.The final classification of a persisting PUL is dependent on the interven-tion or treatment given and includes: treated persistent PUL, resolvedpersistent PUL and non-visualized EP. These are explained in moredetail in the 2011 consensus statement (Barnhart et al., 2011).A treated persistent PUL is defined as one managed medically withmethotrexate without confirmation of the location of the pregnancyby ultrasound, laparoscopy or uterine evacuation. These cases are im-portant as treatment should only be considered when a potentiallyviable IUP has been definitively excluded (Agency for Healthcare Re-search and Quality, 2008).
A resolved persistent PUL is defined as resolution of serum hCG to anon-pregnant value after expectant management or after uterine evacu-ation without evidence of chorionic villi on pathological examination. Ifthe hCG level rises after a uterine evacuation which fails to identify chori-onic villi, a diagnosis of a ‘non-visualized EP’ can be made. In the rareeventof relatively low and unresolving levels of serum hCG, clinicians shouldalso be alert to the possibility of an hCG-secreting tumour beingpresent (Condous et al., 2003; Einenkel et al., 2010; Cong et al., 2011).The optimal management of persisting PUL is not known and there isthe need for a randomized trial between expectant management,uterine curettage and methotrexate. There is no International Classifica-tion of Diseases (ICD-10) code for a final diagnosis of persistent orresolved PUL. A new code has been ascribed to such cases inDenmark and the authors recommend such a classification is adoptedinternationally.
Serum biochemistryHuman chorionic gonadotrophin. Single measurements of serum hCG arenot used to predict the outcome of PUL. A recent meta-analysis con-firmed that absolute single levels of hCG perform poorly as a predictorof PUL outcome (Van Mello et al., 2012). There is a common
misconception that a single level of serum hCG, for example,1000 IU/l, means an EP is unlikely. This is a false assumption as the ma-jority of EPs detected in modern practice have initial serum hCG valuesbelow this level (Condous et al., 2005c). Similarly, a high hCG (forexample .2000 IU/l) does not necessarily exclude the presence of aviable IUP, although it makes it less likely (because a miscarriage maybe classified as a PUL before the hCG level has declined significantly).
In contrast serial measurement of serum hCG offers good test per-formance for predicting viability and is certainly better at predicting loca-tion than measurements of serum progesterone. The use of the serialhCG level was first described by Kadar and Romero in 1981 who sug-gested that the minimal rate of increase in serum hCG with a viableIUP was 66% in 48 h. A subsequent study showed the minimum rise inhCG for a viable IUP to be 24% at 24 h and 53% at 48 h (Barnhartet al., 2004a). More recently, a rise of 35% over 48 h was proposed asthe minimal rise consistent with a viable IUP (Seeber et al., 2006). In clin-ical practice many units use a minimum value of between 50 and 66% toindicate an increase in serum hCG compatible with viability (Horne et al.,2011), but this is not sufficiently conservative and may lead to inadvertenttermination of a pregnancy should an intervention be carried out.It should also be remembered that some EP also demonstrate a‘normal’ rise in hCG.
The changes expected in serum hCG levels over 48 h for failing PULshave also been examined. The rate of decline in hCG is dependent on theinitial serum hCG level, with a more rapid decline associated with higherstarting concentrations (Barnhart et al., 2004b). In a study, the rate ofhCG decline ranged from 21 to 35% at 48 h to 60 to 84% at 7 days(Barnhart et al., 2004b). The change in serum hCG over 48 h may be re-ferred to as the hCG ratio (hCG at 48 h/hCG at 0 h). A decrease in hCGof .13% or an hCG ratio of ,0.87 has a sensitivity of 92.7% and speci-ficity of 96.7% for predicting a failing PUL (Condous et al., 2006b).
Unfortunately, there is no single method to characterize the pattern ofserum hCG change over 48 h in women classified with a PUL who aresubsequently diagnosed with an EP (Silva et al., 2006). Up to 15–20%will have serum hCG doubling times similar to that of an IUP whilstaround 10% EP will have hCG pattern behaving like a failing PUL(Goldstein, 2006; Silva et al., 2006). The majority though, will haveserial serum hCG levels that increase more slowly than would beexpected with an IUP (‘suboptimal rise’) or decrease more slowly thanwould be expected with a failing PUL. The sensitivity of the serumhCG ratio to predict EP ranges from 74 to 100% and the specificityranges from 28 to 97% (Van Mello et al., 2012).
Progesterone. The serum progesterone level is a good indicator of earlypregnancy viability, but a poor predictor of location. Levels of,20 nmol/l have a high positive predictive value for failing pregnancies(Banerjee et al., 2001), whilst levels .25 nmol/l are ‘likely to predict’and levels .60 nmol/l are ‘strongly associated with’ viable pregnancies(RCOG, 2006). A meta-analysis of 26 studies was performed to assessthe accuracy of a single progesterone level for the diagnosis of EP (Molet al., 1998). This study found that progesterone did not have sufficientdiscriminative capacity to diagnose EP with certainty.
The utility of progesterone is in fact in selecting women with failing PULas being at low risk and so needing reduced follow-up. Whether thesefailing PUL are failing EP or failing IUP is not of clinical importance.A recent systematic review and meta-analysis (5 studies with 1998 par-ticipants and cut-off values from 3.2 to 6 ng/ml) has shown that a single
256 Kirk et al.
by guest on March 1, 2016
http://humupd.oxfordjournals.org/
Dow
nloaded from

progesterone level predicts a non-viable pregnancy with a pooled sensi-tivity of 74.6% (95% confidence interval 50.6–89.4%), specificity of98.4% (90.9–99.7%), positive likelihood ratio of 45 (7.1–289) and nega-tive likelihood ratio of 0.26 (0.12–0.57) (Verhaegen et al., 2012).
Other serum markers. Creatine kinase, cancer antigen 125, activin A,inhibin A, inhibin pro-aC-related immunoreactivity and insulin-likegrowth factor-binding protein have all been evaluated (Condous et al.,2005c; Kirk et al., 2009; Chetty et al., 2011). Of these, inhibin A maybe useful for predicting spontaneous resolution of PUL, but is not asgood as progesterone (Kirk et al., 2009; Chetty et al., 2011).
Finding a novel marker to better discriminate EP from the rest of thePUL population nevertheless remains an important area of research.Recent attention has focused on metalloprotease 12 (ADAM 12)(Rausch et al., 2011) and fibronectin (Brown et al., 2013) as potentiallypromising candidate markers.
Mathematical prediction modelsA number of mathematical models have been developed for the predic-tion of PUL outcome. These include logistic regression models andBayesian networks, based on variables such as serum hCG and proges-terone levels, endometrial thickness and the amount of vaginal bleeding(Banerjee et al., 2001; Condous et al., 2004b, 2007a, b; Gevaert et al.,2006). These models have been shown to have high sensitivities forthe prediction of PUL outcome and can be used to rationalize follow-up(Kirk et al., 2007b). The most widely evaluated model developed is M4(Condous et al., 2007a), which takes into account the fact that theinitial hCG level adds information regarding the likely outcome as wellas the hCG ratio.
Rationalizing follow-upInitially mathematical models were optimized to identify EPs in the PULpopulation. The main aim for their use now is to identify PUL that are ‘lowrisk’ (failing PULs and IUPs) in order to safely reduce follow-up for thesepregnancies whilst focusing resources towards pregnancies at increasedrisk of being an EP. In a multi-centre diagnostic accuracy study of 1962patients using the model M4 to predict outcome, 62–75% of PULswere considered low risk of which 96–98% were confirmed to haveeither a failed PUL or IUP (Van Calster et al., 2013). In contrast,80–92% of EPs were considered high risk. In the majority of EP, allocatedto the low-risk group, the hCG ratio was declining and so it is likely thatthese EP would have resolved without the need for intervention.
It is interesting to contrast this approach with the PUL triage studyusing single measurements of progesterone evaluated by Cordina et al.(2011). In this study a serum progesterone of ,10 nmol/l was used todefine a failing pregnancy. Of 676 PUL, 252 were classified as failingPUL with this approach and only 4 of these needed intervention.These results, although not externally validated, are of interest, thoughwith 252 failing PUL in the study, and with 10% of these cases lost tofollow-up, it is hard to make a definitive comment on safety. Theseresults contrast with those of Condous et al. (2005e). He defined alow-risk PUL as one with a single hCG of ,25 IU/l or progesteroneof ,10 nmol/l. It was found that when this approach was applied retro-spectively, 84% of non-ectopic or failing pregnancies could have been dis-charged from the system, but at a cost of 67% of EP in the studypopulation potentially having no further follow-up. This study suggests
a single visit strategy should be approached with caution pending externalvalidation of the approach.
The problem with the use of serum progesterone is that it classifiesmany viable IUP as high risk, which clearly limits the ability to functionas an effective triage tool. The M4 model, on the other hand, classifiesboth failing pregnancies and viable IUPas low risk, which greatly enhancesits utility for triage. Looking forward, it seems likely that a system usingboth progesterone and hCG as a two-step procedure will be theoptimal approach which will enable some failing PUL to be triaged atthe initial visit, and the residual pregnancies should be triaged at 48 hafter application of the M4 model. The M4-based protocol can beaccessed from the following link: http://homes.esat.kuleuven.be/~biomed/M4PUL/M4triage.htm.
Surgical interventionThe combination of the absence of avisualized IUP using TVS and a serumhCG level above a set discriminatory zone historically was considered anindication for diagnostic laparoscopy. This is no longer the case. Laparos-copy is now rarely indicated unless a woman is symptomatic or haemo-dynamically unstable. This is because many failing PUL and some IUP mayhave initial hCG levels above, and some clinically significant EP will havehCG levels below, given any discriminatory zone. Condous et al.(2005d) evaluated the diagnostic accuracy of discriminatory zones forhCG levels of .1000, 1500 and 2000 IU/l for the detection of EP inwomen with a PUL. It was found that as the discriminatory zoneincreases, the sensitivity to detect EP decreases, and most EP in thepopulation of women with PUL studied had serum hCG levels belowthe often-quoted discriminatory zone of 1000 IU/l.
Uterine curettage is used by some clinicians to diagnose pregnancy lo-cation with the aim of differentiating between an EP and a non-viable IUP.Advocates of curettage report that a failure to definitively ascertain thelocation of a pregnancy may have implications for counseling aboutfuture risk of EP and lead to unnecessary exposure to methotrexate(Chung et al., 2011). However, there is the risk that a potentiallyongoing IUP may be terminated if the preoperative criteria are not strin-gent enough to exclude a viable IUP before the procedure. Recognizedindications for curettage include: (i) no visible IUP on TVS with aserum hCG . 2000 IU/ml; (ii) an abnormal rise in hCG level, definedas ,50% increase in 2 days and (iii) an abnormal fall in hCG level,defined as ,20% decline in 2 days (Chung et al., 2011). In a study of321 women who underwent uterine curettage with no visible IUP orthose with an abnormal hCG trend, 73.2% were ultimately diagnosedwith an EP whilst 26.8% were found to have a non-viable IUP (Chunget al., 2011). These and other biochemical criteria that define non-viability in the PUL population have been evaluated to establish if thecriteria used could result in inadvertent termination of a pregnancy ifcurettage was performed (Condous et al., 2006c). Up to 12.3% ofwomen undergoing curettage were deemed at risk of having a viableIUP interrupted (Condous et al., 2006c). Uterine curettage should there-fore not be used routinely in the management of PUL but may have a rolein diagnosing the location of failing PULs, once the possibility of a poten-tially viable IUP has been excluded.
Clinical managementThe majority of women categorized with a PUL have minimal or absentsymptoms and are haemodynamically stable. Expectant outpatient
Current concepts in ectopic pregnancy and PUL 257
by guest on March 1, 2016
http://humupd.oxfordjournals.org/
Dow
nloaded from

management of such cases is safe (Hahlin et al., 1995; Banerjee et al.,1999, 2001; Kirk et al., 2007b). All compliant women with a PULshould be counselled about the possible outcomes and be givenwritten information detailing the plan for further investigation andwhen and how to seek urgent medical care during any follow-up period.
The majority of women classified with a PUL will be subsequently diag-nosed with a failed pregnancy, resolving spontaneously without interven-tion (Banerjee et al., 1999). There is no consensus on what is anacceptable surgical intervention rate in women classified with a PUL(Condous et al., 2006a), although studies report rates of between 0.5and 11% (Banerjee et al., 2001; Condous et al. 2003; Kirk et al., 2007b;Cordina et al., 2011). It is evident that the management of PUL needsto concentrate resources and surveillance on women with the highestrisk of significant pathology, whilst minimizing intervention and follow-upin women at low risk of complications.
Most women with a PUL are followed up with serum hCG measure-ments and repeat TVS examination until a final diagnosis is confirmed.Women with PUL should be triaged into low- and high-risk groupsthat require different levels of intensity for follow-up. By using the M4model or hCG ratio, PUL may be classified as being ‘low-risk failing’ or‘low-risk intrauterine’. ‘Low-risk failing’ may be followed up with aurinary pregnancy test after 2 weeks and telephone advice. A womanwith a ‘low-risk intrauterine’ may return for an ultrasound scan to
assess viability in 2 weeks. In the event of being classified as high risk,further assessment is required either with a further ultrasound scanwithin 48 h or a further hCG measurement. Figure 4 summarizes sug-gested management algorithms for PUL.
Future workThe ideal diagnostic tool for an EP would be a single serum marker toreplace ultrasound and serial biochemistry (Shaw et al., 2010a). Whilethe major focus of work until now has been on diagnosing all EP, reliabletools are needed to identify those women with EP or PUL who do notrequire active intervention.
The common assumption is that earlier diagnosis of EP means moreeffective management, because more conservative managementoptions may be employed (Hajenius et al., 2007), although this is notborne out in studies thus far (Fernandez et al., 2013; Van Mello et al.,2013). Until robust evidence suggests that medical treatment leads tolower subsequent EP rates or higher subsequent IUP rates, then theoverall benefit from earlier diagnosis is unproved providing the diagnosisis made prior to tubal rupture. It is likely that women with suspected ordefinite EP that would otherwise spontaneously resolve are currentlybeing over-treated.
Figure 4 Possible PUL management algorithm. *Women must be given information and advice, be deemed compliant with follow-up and have no sig-nificant language orother communication barrier. Women should be advised to return for review before the scheduled follow-up visit if they have anyseverepain or concerns. **If hCG . 1000 IU/l at 0 h and history not suggestive of complete miscarriage, then repeat TVS as soon as possible. Adapted fromCondous et al. (2006b); Kirk et al. (2007b). TVS, transvaginal ultrasound.
258 Kirk et al.
by guest on March 1, 2016
http://humupd.oxfordjournals.org/
Dow
nloaded from

ConclusionThe primary assessment approach for a woman with a possible EP isultrasonography. This should be carried out transvaginally and allrecent data on diagnosing EP, defining PUL, performance of discrimin-atory zones and diagnosing miscarriage relate to this approach. Ultra-sound is operator dependent and requires appropriate training andsignificant experience for good results to be obtained. We have shownthat where there is easy access to expertise and equipment to providehigh-quality TVS, the vast majority of women with tubal EPs may be diag-nosed rapidly and accurately. The diagnosis of non-tubal EP can also beachieved through careful ultrasound assessment, although diagnosis ismore often delayed leading to increased morbidity.
The need for a single serum marker for EP and a method to differen-tiate between women with PUL and EP who do and do not require inter-vention are the current diagnostic challenges. The current trend in themanagement of PUL is thus directed to detecting the women with‘low-risk’ PUL who can undergo minimal follow-up whilst concentratingresources on the women with ‘high-risk’ PUL in whom the majority ofharmful EPs will be found. In the meantime, algorithms such to managewomen with PUL safely, consistently and with minimal unnecessary inter-vention should be adopted.
Authors’ rolesAll three authors (E.K., C.B and T.B.) made substantial contributions tothe plan of the article, review and interpretation of the literature anddrafting and revision of the manuscript. All authors approved the finalversion to be published.
FundingT.B. is supported by the National Institute for Health Research (NIHR)Biomedical Research Centre based at Imperial College HealthcareNHS Trust and Imperial College London. The views expressed arethose of the authors and not necessarily reflect those of the NHS, theNIHR or the Department of Health.
ReferencesAckerman TE, Levi CS, Dashefsky SM, Holt SC, Lindsay DJ. Interstitial line: sonographic
finding in interstitial (cornual) ectopic pregnancy. Radiology 1993;189:83–87.Agency for Healthcare Research and Quality. Medical management of ectopic
pregnancy, 2008. http://www.guidelines.gov/content.aspx?Id=12625#Section427 (6 August 2013).
Ankum WM, Mol BW, Van der Veen F, Bossuyt PM. Risk factors for ectopic pregnancy:a meta-analysis. Fertil Steril 1996;65:1093–1099.
Atri M, Leduc C, Gillett P, Bret PM, Reinhold C, Kintzen G, Aldis AE, Thibodeau M. Roleof endovaginal sonography in the diagnosis and management of ectopic pregnancy.Radiographics 1996;16:755–774.
Atri M, Valenti DA, Bret PM, Gillett P. Effect of transvaginal sonography on the use ofinvasive procedures for evaluating patients with a clinical diagnosis of ectopicpregnancy. J Clin Ultrasound 2003;31:1–8.
Bakken IJ, Skjeldestad FE. Reduced number of extrauterine pregnancies—increasedfertility of women during the 1990s? Tidsskr Nor Laegeforen 2003;123:3011–3014.
Banerjee S, Aslam N, Zosmer N, Woelfer B, Jurkovic D. The expectant managementof women with pregnancies of unknown location. Ultrasound Obstet Gynecol 1999;14:231–236.
BanerjeeS,Aslam N, WoelferB, LawrenceA,Elson J, Jurkovic D. Expectant managementof early pregnancies of unknown location: a prospective evaluation of methods topredict spontaneous resolution of pregnancy. BJOG 2001;108:158–163.
Barnhart KT, Sammel MD, Rinaudo PF, Ahou L, Hummel AC, Guo W. Symptomaticpatients with an early viable intrauterine pregnancy: HCG curves redefined. ObstetGynecol 2004a;104:50–55.
Barnhart K, Sammel MD, Chung K, Zhou L, Hummel AC, Guo W. Decline of serumhuman chorionic gonadotrophin and spontaneous complete abortion: defining thenormal curve. Obstet Gynecol 2004b;104:975–981.
Barnhart K, van Mello NM, Bourne T, Kirk E, Van Claster B, Bottomley C, Chung K,Condous G, Goldetein S, Hajenius PJ et al. Pregnancy of unknown location: aconsensus statement of nomenclature, definitions, and outcome. Fertil Steril 2011;95:857–866.
Benson CB, Doubilet PM, Peters HE, Frates MC. Intrauterine fluid with ectopicpregnancy: a reappraisal. J Ultrasound Med 2013;32:389–393.
Bignardi T, Condous G, Kirk E, Van Claster B, Van Huffel S, Timmerman D, Bourne T.Viability of intrauterine pregnancy in women with pregnancy of unknown location:prediction using human chorionic gonadotrophin ratio vs. progesterone. UltrasoundObstet Gynecol 2010;35:656–661.
Bottomley C, Van Belle V, Mukri F, Kirk E, Van Huffel S, Timmerman D, Bourne T. Theoptimal timing of an ultrasound scan to assess the location and viability of an earlypregnancy. Hum Reprod 2009;24:1811–1817.
Boufous S, Quartararo M, Mohsin M, Parker J. Trends in the incidence of ectopicpregnancy in New South Wales between 1990–1998. Aust N Z J Obstet Gynaecol2001;41:436–438.
Bourne TH, Jurkovic D, Waterstone J, Campbell S, Collins WP. Intrafollicular bloodflow during human ovulation. Ultrasound Obstet Gynecol 1991;1:53–59.
Bourne T, Barnhart K, Benson CB, Brosens J, Van Calster B, Condous G,Coomerasamy A, Doubilet PM, Goldstein SR, Gould D et al.. NICE guidance onectopic pregnancy and miscarriage restricts access and choice and may beclinically unsafe. BMJ 2013;346:f197. doi: 10.1136/bmj.f197.
Bouyer J, Coste J, Fernandez H, Pouly JL, Job-Spira N. Sites of ectopic pregnancy: a10 year population-based study of 1800 cases. Hum Reprod 2002;17:3224–3230.
Bouyer J, Coste J, Shojaei T, Pouly JL, Fernandez H, Gerbaud L, Job-Spira N. Risk factorsfor ectopic pregnancy: a comprehensive analysis based on a large case–control,population-based study in France. Am J Epidemiol 2003;157:185–194.
Braffman BH, Coleman BG, Ramchandani P, Arger PH, Nodine CF, Dinsmore BJ,Louie A, Betsch SE. Emergency department screening for ectopic pregnancy:a prospective US study. Radiology 1994;190:797–802.
Brown DL, Doubilet PM. Transvaginal sonography for diagnosing ectopic pregnancy:positivity criteria and performance characteristics. J Ultrasound Med 1994;13:259–266.
Brown JK, Lauer KB, Ironmonger EL, Inglis NF, Bourne TH, Critchley HO, Horne AW.Shotgun proteomics identifies serum fibronectin as a candidate diagnostic biomarkerfor inclusion in future multiplex tests for ectopic pregnancy. PLoS One 2013;8:e66974.
Cacciatore B, Ylostalo P, Stenman UH, Widholm O. Suspected ectopic pregnancy:ultrasound findings and hCG levels assessed by an immunofluorometric assay. Br JObstet Gynaecol 1988;95:497–502.
Cacciatore B, Stenman UH, Ylostalo P. Comparison of abdominal and vaginalsonography in suspected ectopic pregnancy. Obstet Gynecol 1989;73:770–774.
Casikar I, Lu C, Oates J, Bignardi T, Alhamdan D, Condous G. The use of powerDoppler colour scoring to predict successful expectant management in womenwith an incomplete miscarriage. Hum Reprod 2012;27:669–675.
Chetty M, Sawyer E, Tew T, Chapman AJ, Elson J. The use of novel biochemical markersin predicting spontaneously resolving ‘pregnancies of unknown location’. HumReprod 2011;26:1318–1323.
Chung K, Chandavarkar U, Opper N, Barnhart K. Reevaluating the role of dilatation andcurettage in the diagnosis of pregnancy of unknown location. Fertil Steril 2011;96:659–662.
Comstock C, Huston K, Lee W. The ultrasonographic appearance of ovarian ectopicpregnancies. Obstet Gynecol 2005;105:42–45.
Condous G, Thomas J, Okaro E, Bourne T. Placental site trophoblastic tumormasquerading as an ovarian ectopic pregnancy. Ultrasound Obstet Gynecol 2003;21:504–506.
Condous G, Lu C, Van Huffel S, Timmerman D, Bourne T. Human chorionicgonadotrophin and progesterone levels for the investigation of pregnancies ofunknown location. Int J Gynecol Obstet 2004a;86:351–357.
Current concepts in ectopic pregnancy and PUL 259
by guest on March 1, 2016
http://humupd.oxfordjournals.org/
Dow
nloaded from

Condous G, Okaro E, Khalid A, Timmerman D, Lu C, Zhou Y, Van Huffel S, Bourne T.The use of a new logistic regression models or predicting the outcome of pregnanciesof unknown location. Hum Reprod 2004b;19:1900–1910.
Condous G, Okaro E, Khalid A, Lu C, Van Huffel S, Timmerman D, Bourne T. Theaccuracy of transvaginal sonography for the diagnosis of ectopic pregnancy priorto surgery. Hum Reprod 2005a;20:1404–1409.
Condous G, Okaro E, Khalid A, Bourne T. Do we need to follow-up completemiscarriages with serum human chorionic gonadotrophin levels? BJOG 2005b;112:827–829.
Condous G, Kirk E, Syed A, Van Calster B, Van Huffel S, Timmerman D, Bourne T. Dolevels of serum cancer antigen 125 and creatine kinase predict the outcome inpregnancies of unknown location? Hum Reprod 2005c;20:3348–3354.
Condous G, Kirk E, Lu C, Van Huffel S, Gevaert O, De Moor B, De Smet F,Timmerman D, Bourne T. Diagnostic accuracy of varying discriminatory zone forthe prediction of ectopic pregnancy in women with pregnancy of unknownlocation. Ultrasound Obstet Gynecol 2005d;26:770–775.
Condous G, Okaro E, Khalid A, Lu C, Van Huffel S, Timmerman D, Bourne T.A prospective evaluation of a single-visit strategy to manage pregnancies ofunknown location. Hum Reprod 2005e;20:1398–1403.
Condous G, Timmerman D, Goldstein S, Valentin L, Jurkovic D, Bourne T. Pregnanciesof unknown location: consensus statement. Ultrasound Obstet Gynecol 2006a;28:121–122.
Condous G, Kirk E, Van Calster B, Van Huffel S, Timmerman D, Bourne T. Failingpregnancies of unknown location: a prospective evaluation of the humanchorionic gonadotrophin ratio. BJOG 2006b;113:521–527.
CondousG, Kirk E, Lu C, VanCalster B, VanHuffel S, Timmerman D, Bourne T. There isno role for uterine curettage in the contemporary diagnostic workup of women witha pregnancy of unknown location. Hum Reprod 2006c;21:2706–2710.
Condous G, Van Calster B, Kirk E, Haider Z, Timmerman D, Van Huffel S, Bourne T.Prediction of ectopic pregnancy in women with a pregnancy of unknown location.Ultrasound Obstet Gynecol 2007a;29:680–687.
Condous G, Van Calster B, Kirk E, Haider Z, Timmerman D, Van Huffel S, Bourne T.Clinical information does not improve the performance of mathematical models inpredicting the outcome of pregnancies of unknown location. Fertil Steril 2007b;88:572–580.
Cong Q, Li G, Jiang W, Li B, Wang Y, Yao L, Wang S, Xu C. Ectopic choriocarcinomamasquerading as a pregnancy of unknown location: case report and review of theliterature. J Clin Oncol 2011;29:845–848.
Cordina M, Schramm-Gajraj K, Ross JA, Lautman K, Jurkovic D. Introduction of a singlevisit protocol in the management of selected patients with pregnancy of unknownlocation: a prospective study. BJOG 2011;118:693–697.
DeVoe RW, Pratt JH. Simultaneous intra-uterine and extra-uterine pregnancy. Am JObstet Gynecol 1948;56:1119–1126.
Dor J, Seidman DS, Levran D, Ben-Rafael Z, Ben-Shiomo I, Mashiach S. The incidence ofcombined intrauterine and extrauterine pregnancy after in vitro fertilization andembryo transfer. Fertil Steril 1991;55:833–834.
Doubilet PM, Benson CB. First, do no harm . . . To early pregnancies. J Ultrasound Med2010;29:685–689.
Einenkel J, Handzel R, Horn LC. Persisting pregnancy of unknown location—keepyour eyes peeled for choriocarcinoma. Eur J Gynecol Reprod Biol 2010;153:229–231.
Fernandez H, Gervaise A. Ectopic pregnancies after infertility treatment:modern diagnosis and therapeutic strategy. Hum Reprod Update 2004;10:503–513.
Fernandez H, Capmas P, Lucot JP, Resch B, Panel P, Bouyer J, GROG. Fertility afterectopic pregnancy: the DEMETER randomized trial. Hum Reprod 2013;28:1247–1253.
Fleischer AC, Pennell RG, McKee MS, Worrell JA, Keefe B, Herbert CM, Hill GA,Cartwright PS, Kepple DM. Ectopic pregnancy: features at transvaginalsonography. Radiology 1990;174:375–378.
Frates MC, Laing FC. Sonographic evaluation of ectopic pregnancy: an update. AJR Am JRoentgenol 1995;165:251–259.
From the Centers for Disease Control and Prevention. Ectopic pregnancy—UnitedStates, 1990–1992. JAMA 1995;273:533.
Gerli S, Rossetti D, Baiocchi G, Clerici G, Unfer V, Carlo Di Renzo G. Earlyultrasonographic diagnosis and laparoscopic treatment of abdominal pregnancy.Eur J Obstet Gynecol Reprod Biol 2004;113:103–105.
Gevaert O, De Smet F, Kirk E, Van Calster B, Bourne T, Van Huffel S, Moreau Y,Timmerman D, De Moor B, Condous G. Predicting the outcome of pregnancies
of unknown location: Bayesian networks with expert prior information comparedto logistic regression. Hum Reprod 2006;21:1824–1831.
Goldstein S. The diagnosis of miscarriage. In: Bourne T, Condous G (eds). Handbook ofEarly Pregnancy Care. UK: Informa Health Care Ltd, 2006, 27–35.
Hahlin M, Thorburn J, Bryman I. The expectant management of early pregnancies ofuncertain site. Hum Reprod 1995;10:1223–1227.
Hajenius PJ, Mol F, Mol BW, Bossuyt PM, Ankum WM, van der Veen F. Interventions fortubal ectopic pregnancy. Cochrane DatabaseSyst Rev2007; Issue 1. Art No. CD000324.
Horne AW, McBride R, Denison FC. Normally rising hCG does not predict live birth inwomen presenting with pain and bleeding in early pregnancy. Eur J Obstet GynecolReprod Biol 2011;156:120–121.
Jermy K, Thomas J, Doo A, Bourne T. The conservative management of interstitialpregnancy. BJOG 2004;111:1283–1288.
Jurkovic D, Mavrelos D. Catch me if you scan: ultrasound diagnosis of ectopicpregnancy. Ultrasound Obstet Gynecol 2007;30:1–7.
Jurkovic D, Wilkinson H. Diagnosis and management of ectopic pregnancy. BMJ 2011;10:342.
Jurkovic D, Bourne TH, Jauniaux E, Campbell S, Collins WP. Transvaginal color Dopplerstudy of blood flow in ectopic pregnancies. Fertil Steril 1992;57:68–73.
Jurkovic D, Hackett E, Campbell S. Diagnosis and treatment of early cervical pregnancy:a review and a report of two cases treated conservatively. Ultrasound Obstet Gynecol1996;8:373–380.
Jurkovic D, Hillaby K, Woelfer B, Lawrence A, Salim R, Elson J. First-trimester diagnosisand management of pregnancies implanted into the lower uterine segment Cesareansection scar. Ultrasound Obstet Gynecol 2003;21:220–227.
Kadar N, Romero R. HCG assays and ectopic pregnancy. Lancet 1981;1:1205–1206.Kaplan BC, Dart RG, Moskos M, Kuligowska E, Chun B, Adel Hamid M, Northern K,
Schmidt J, Kharwadkar A. Ectopic pregnancy: prospective study with improveddiagnostic accuracy. Ann Emerg Med 1996;28:10–17.
Kirk E, Condous G, Haider Z, Lu C, Van Huffel S, Timmerman D, Bourne T. Thepractical application of a mathematical model to predict the outcome ofpregnancies of unknown location. Ultrasound Obstet Gynecol 2006;27:311–315.
Kirk E, Papageorghiou AT, Condous G, Tan L, Bora S, Bourne T. The diagnosticeffectiveness of an initial transvaginal scan in detecting ectopic pregnancy. HumReprod 2007a;22:2824–2828.
KirkE,CondousG,VanCalsterB,VanHuffelS,TimmermanD,BourneT.Rationalizing thefollow-up of pregnancies of unknown location. Hum Reprod 2007b;22:1744–1750.
Kirk E, Daemen A, Papageorghiou AT, Bottomley C, Condous G, De Moor B,Timmerman D, Bourne T. Why are some ectopic pregnancies characterized aspregnancies of unknown location at the initial transvaginal ultrasoundexamination? Acta Obstet Gynecol Scand 2008;87:1150–1154.
Kirk E, Papageorghiou A, Van Calster B, Condous G, Cowans N, Van Huffel,Timmerman D, Spencer K, Bourne T. The use of serum inhibin A and activin Alevels in predicting the outcome of pregnancies of unknown location. Hum Reprod2009;24:2451–2456.
Kobayashi M, Heliman L, Fillisti L. Ultrasound: an aid in the diagnosis of ectopicpregnancy. Am J Obstet Gynecol 1969;103:1131–1140.
Krag Moeller LB, Moeller C, Thomsen SG, Andersen LF, Lundvall L, Lidegaard Ø, Kjer JJ,Ingemanssen JL, Zobbe V, Floridon C et al. Success and spontaneous pregnancy ratesfollowing systemic methotrexate versus laparoscopic surgery for tubal pregnancies:a randomized trial. Acta Obstet Gynecol Scand 2009;88:1331–1337.
Laing FC. Ectopic Pregnancy. In: Timor-Tritsch IE, Goldstein SR (eds). Ultrasound inGynecology, 2nd edn. New York, USA: Churchill Livingstone, 2007, 161–173.
Lawrence A, Jurkovic D. Three-dimensional ultrasound diagnosis of interstitialpregnancy. Ultrasound Obstet Gynecol 1999;14:292–293.
Lewis G (ed.). The Confidential Enquiry into Maternal and Child Health (CEMACH).Saving Mothers’ Lives: reviewing maternal deaths to make motherhood safer—2003–2005. The Seventh Report on Confidential Enquiries into Maternal Deathsin the United Kingdom. London, UK: CEMACH, 2007.
Li TC, Tristam A, Hill AS, Cooke ID. A review of 254 ectopic pregnancies in a teachinghospital in the Trent Region, 1977–1990. Hum Reprod 1991;6:1002–1007.
Marks WM, Filly RA, Callen PW, Laing FC. The decidual cast of ectopic pregnancy:A confusing ultrasonographic appearance. Radiology 1979;133:451–454.
Mehta TS, Levine D, McArdle CR. Lack of sensitivity of endometrial thickness inpredicting presence of an ectopic pregnancy. J Ultrasound Med 1999;18:117–122.
Mol BW, Lijmer JG, Ankum W, van der Veen F, Bossuyt PM. The accuracy of singleserum progesterone measurement in the diagnosis of ectopic pregnancy:a meta-analysis. Hum Reprod 1998;13:3220–3227.
260 Kirk et al.
by guest on March 1, 2016
http://humupd.oxfordjournals.org/
Dow
nloaded from

Molloy D, Deambrosis W, Keeping D, Hynes J, Harrison K, Hennessey J. Multiple-sited(heterotopic) pregnancy after in vitro fertilization and gamete intrafallopian transfer.Fertil Steril 1990;53:1068–1071.
Naji O, Wynants L, Smith A, Abdallah Y, Saso S, Stalder C, Van Huffel S,Ghaem-Maghami S, Van Calster B, Timmerman D et al. Does the presence of acaesarean section scar affect implantation site and early pregnancy outcome inwomen attending an early pregnancy assessment unit? Hum Reprod 2013;28:1489–1496.
Newbatt E, Beckles Z, Ullman R, Lumsden MA, Guideline Development Group.Ectopic pregnancy and miscarriage: summary of NICE guidance. BMJ 2012;345:e8136.
Nurmohamed L, Moretti ME, Schechter T, Einarson A, Johnson D, Lavigne SV,Erebara A, Koren G, Finkelstein Y. Outcome following high-dose methotrexatein pregnancies misdiagnosed as ectopic. Am J Obstet Gynecol 2011;205:533.e1–533.e3.
Nyberg DA, Hughes MP, Mack LA, Wang KY. Extra-uterine findings of ectopicpregnancy at transvaginal US: importance of echogenic fluid. Radiology 1991;178:823–826.
O’Herlihy. Deaths in early pregnancy. In: Lewis G. (ed.). Centre for Maternal and ChildEnquiries (CMACE). Saving Mothers’ Lives: Reviewing Maternal Deaths to MakeMotherhood Safe 2006–2008. The Eighth Report on Confidential Enquiries intoMaternal Deaths in the United Kingdom. BJOG 2011;118(Suppl. 1):1–203.
Pellerito JS, Troiano RN, Quedens-Case C, Taylor KJ. Common pitfalls of endovaginalcolor Doppler flow imaging. Radiographics 1995;15:37–47.
Raskin M. Diagnosis of cervical pregnancy by ultrasound. A case report. Am J ObstetGynecol 1978;130:234–235.
Rausch ME, Sammel MD, Takacs P, Chung K, Shaunik A, Barnhart KT. Developmentof a multiple marker test for ectopic pregnancy. Obstet Gynecol 2011;117:573–582.
Royal College of Obstetricians and Gynaecologists. Green Top Guideline No. 25. TheManagement of Early Pregnancy Loss. London, UK: RCOG Press, 2006.
Sawyer E, Ofuasia E, Ofili-Yeboviu D, Helmy S, Gonzalez J, Jurkovic D. The value ofmeasuring endometrial thickness and volume on transvaginal ultrasound scan forthe diagnosis of incomplete miscarriage. Ultrasound Obstet Gynecol 2007;29:205–209.
Scalea T, Rodriguez A, Chiu W, Brenneman F, Fallon W, Kato K, McKenney M,Nerlich M, Ochsner M, Yoshii H. Focused Assessment with Sonography forTrauma (FAST): results from an international consensus conference. J Trauma1999;46:466–472.
Seeber BE, Sammel MD, Guo W, Zhou L, Hummel A, Barnhart KT. Application ofredefined human chorionic gonadotropin curves for the diagnosis of women atrisk for ectopic pregnancy. Fertil Steril 2006;86:454–459.
Shalev E, Yarom I, Bustan M, Weiner E, Ben-Shlomo I. Transvaginal sonography as theultimate diagnostic tool for the management of ectopic pregnancy: experience with840 cases. Fertil Steril 1998;69:62–65.
Shaw JL, Dey SK, Critchley HO, Horne AW. Current knowledge of the aetiology ofhuman tubal ectopic pregnancy. Hum Reprod Update 2010a;16:432–444.
Shaw JL, Oliver E, Lee KF, Entrican G, Jabbour HN, Critchley HO, Horne AW. Cotinineexposure increases Fallopian tube PROKR1 expression via nicotinic AChRalpha-7:a potential mechanism explaining the link between smoking and tubal ectopicpregnancy. Am J Pathol 2010b;177:2509–2515.
Shaw JL, Wills GS, Lee KF, Horner PJ, McClure MO, Abrahams VM, Wheelhouse N,Jabbour HN, Critchley HO, Entrican G et al. Chlamydia trachomatis infectionincreases fallopian tube PROKR2 via TLR2 and NFkB activation resulting in amicroenvironmentpredisposed toectopicpregnancy. AmJ Pathol2011;178:253–260.
Sickler GK, Chen PC, Dubinsky TJ, Maklad N. Free echogenic pelvic fluid: correlationwith hemoperitoneum. J Ultrasound Med 1998;17:431–435.
Silva C, Sammel MD, Zhou L, Gracia C, Hummel AC, Barnhart K. Human chorionicgonadotrophin profile for women with ectopic pregnancy. Obstet Gynecol 2006;107:605–610.
Tay JI, Moore J, Walker JJ. Ectopic pregnancy. BMJ 2000;320:916–919.Timor-Tritsch IE, Monteagudo A, Mandeville EO, Peisner DB, Anaya GP, Pirrione EC.
Successful management of viable cervical pregnancy by local injection ofmethotrexate guided by transvaginal ultrasonography. Am J Obstet Gynecol 1994;170:737–739.
Valenzano M, Anserini P, Remorgida V, Brasca A, Centonze A, Costantini S.Transabdominal and transvaginal ultrasonographic diagnosis of ectopic pregnancy:clinical implications. Gynecol Obstet Invest 1991;31:8–11.
Van Calster B, Abdallah Y, Guha S, Kirk E, Van Hoorde K, Condous G, Priesler J,Hoo W, Stalder C, Bottomley C et al. Rationalizing the management ofpregnancies of unknown location: temporal and external validation of a riskprediction model on 1962 pregnancies. Hum Reprod 2013;28:609–616.
Van Mello N, Mol F, Opmeer BC, Ankum WM, Barnhart K, Coomarasamy A, Mol BW,van der Veen F, Hajenius PJ. Diagnostic value of serum hCG on the outcome ofpregnancy of unknown location: a systematic review and meta-analysis. HumReprod Update 2012;18:603–617.
van Mello NM, Mol F, Verhoeve HR, van Wely M, Adriaanse AH, Boss EA, Dijkman AB,Bayram N, Emanuel MH, Friederich J et al. Methotrexate or expectant managementin women with an ectopic pregnancy or pregnancy of unknown location and lowserum hCG concentrations? A randomized comparison. Hum Reprod 2013;28:60–67.
Varma R, Gupta J. Tubal ectopic pregnancy. Clin Evid (Online) 2009;Pii:1406.Verhaegen J, Gallos ID, van Mello NM, Abdel-Aziz M, Takwoingi Y, Harb H, Deeks JJ,
Mol BW, Coomarasamy A. Accuracy of single progesterone test to predict earlypregnancy outcome in women with pain or bleeding: meta-analysis of cohortstudies. BMJ 2012;345:e6077.
Walker J. Ectopic pregnancy. Clin Obstet Gynecol 2007;50:89–99.Weckstein LN, Boucher AR, Tucker H, Gibson D, Rettenmaier MA. Accurate diagnosis
of early ectopic pregnancy. Obstet Gynecol 1985;65:393–397.
Current concepts in ectopic pregnancy and PUL 261
by guest on March 1, 2016
http://humupd.oxfordjournals.org/
Dow
nloaded from