Embed Size (px)
Citation preview

Diagnosing and Managing COPD
Douglas ArenbergUniversity of Michigan
Division of Pulmonary & Critical Care Medicine

• Session Objectives: By the end of this session, participants will be able to…
• Understand the characteristic subjective and objective findings in patients with COPD, when to perform, and how to interpret spirometry in COPD
• Understand the goals of managing patients with COPD and the treatments aimed at achieving these goals

COPD
• Diagnosis• You can’t diagnose if you don’t look, because most people with COPD won’t
come in talking about being out of breath.
• Treatment Goals: improve quality-of-life, prevent exacerbations, treat exacerbations, preserve lung function
• Drugs that improve symptoms, drugs that prevent exacerbations, and drugs that reduce decline in FEV1.
• Flu vaccine, pneumococcal vaccine. Stand your ground, be firm, be right, but vaccinate your patients with COPD.
• Supplemental oxygen Do’s and Don’t’s

Global Strategy for Diagnosis, Management and Prevention of COPD
Diagnosis and Assessment: Key Points
• COPD dx should be considered in any patient with dyspnea, chronic cough or sputum production, and a history of exposure to risk factors for the disease.
• Spirometry is required to make the diagnosis; the presence of a post-bronchodilator FEV1/FVC < 0.70 confirms the presence of persistent airflow limitation and thus of COPD
© 2015 Global Initiative for Chronic Obstructive Lung Disease

Global Strategy for Diagnosis, Management and Prevention of COPD
Risk Factors for COPD
Genes
Infections
Socio-economic status
Aging Populations© 2015 Global Initiative for Chronic Obstructive Lung Disease
!!Second Hand Smoke!!

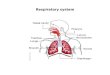
SYMPTOMS
chronic coughshortness of breath
EXPOSURE TO RISKFACTORS
tobaccooccupation
indoor/outdoor pollution
SPIROMETRY: Required to establish diagnosis
Global Strategy for Diagnosis, Management and Prevention of COPD
Diagnosis of COPD
sputum
© 2015 Global Initiative for Chronic Obstructive Lung Disease

USPSTF. JAMA 2016; 315: 1372-7
Symptoms are not always obvious!!

• Assess symptoms• Assess degree of airflow limitation using spirometry
• The goals of assessment are to determine the severity of the disease, including the severity of airflow limitation, the impact on the patient’s health status, and the risk of exacerbations
• Comorbidities (CAD, DM, CVD) occur frequently in COPD patients, and should be actively looked for and treated appropriately if present.
Global Strategy for Diagnosis, Management and Prevention of COPD
Assessment of COPD
© 2015 Global Initiative for Chronic Obstructive Lung Disease
Use spirometry for grading severity according to spirometry, using four grades split at 80%, 50% and 30% of predicted

http://www.catestonline.org/english/indexEN.htm CAT score Impact
>30 • Referral to specialistAlso consider:• Additional pharmacological treatments• Pulmonary rehabilitation• Focus on preventing exacerbations
20-29
10-19 • Reviewing maintenance rx – is it optimal?•Pulmonary rehabilitation• Prevent exacerbations • Aggravating factors; still smoking?
<10 Smoking cessation• Annual flu vaccination• Reduce exposure to exacerbation risk factors• Symptom management


• Assess symptoms• Assess degree of airflow limitation using spirometry
• The goals of assessment are to determine the severity of the disease, including the severity of airflow limitation, the impact on the patient’s health status, and the risk of exacerbations
• Comorbidities (CAD, DM, CVD) occur frequently in COPD patients, and should be actively looked for and treated appropriately if present.
Global Strategy for Diagnosis, Management and Prevention of COPD
Assessment of COPD
© 2015 Global Initiative for Chronic Obstructive Lung Disease
Use spirometry for grading severity according to spirometry, using four grades split at 80%, 50% and 30% of predicted

GOLD Grading System: FEV1 Airflow Limitation (80-50-30)
12Global Initiative for Chronic Obstructive Lung Disease (GOLD). GOLD COPD web site. http://www.goldcopd.org/uploads/users/files/GOLD_Report_2015_Apr2.pdf. Accessed June 18, 2015.
Postbronchodilator FEV1/FVC <.70 • Confirms presence of persistent airflow limitation
• Supports diagnosis of COPD
GOLD Grade 4
GOLD Grade 1
GOLD Grade 2
GOLD Grade 3
• Mild• FEV1 ≥80% predicted
• Moderate• 50% ≤FEV1 <80%
predicted
• Severe• 30% ≤FEV1 <50% predicted
• Very severe• FEV1 <30% predicted

Assess symptoms Assess degree of airflow limitation using
spirometry Assess risk of exacerbations
Assess comorbiditiesUse history of exacerbations and spirometry. Two exacerbations or more within the last year
or an FEV1 < 50 % of predicted value areindicators of high risk. Hospitalization for a COPD
exacerbation associated with increased risk of death.
Global Strategy for Diagnosis, Management and Prevention of COPD
Assessment of COPD
© 2015 Global Initiative for Chronic Obstructive Lung Disease

Global Strategy for Diagnosis, Management and Prevention of COPD
Assess Risk of Exacerbations
• Unlike stock market, past performance probably predicts future results:
• Past exacerbations often predict future risk• Two or more exacerbations within the last year or an FEV1 < 50 % of predicted indicate higher risk
• One or more hospitalizations for COPD exacerbation should be considered highrisk.
© 2015 Global Initiative for Chronic Obstructive Lung Disease

(C) (D)
(A) (B)
Combined Assessment of COPD requires 3 ‘axes’ to determine severity
© 2015 Global Initiative for Chronic Obstructive Lung Disease
Exac
erba
tions
per
yea
r
CAT < 10mMRC 0-1
CAT > 10 mMRC > 2
GOLD 3-4
GOLD 1-2
2 or more or
1 with hospitaladmission
0-1 (without hospital admission)
Spiro
met
ricSe
verit
y
High risk Less symptoms
Low risk Less symptoms
High risk More symptoms
Low risk Less symptoms

Most COPD Patients Do Not Receive Recommended Treatment
LACC, long-acting anticholinergic; SACC, short-acting anticholinergic Make B et al. Int J Chron Obstruct Pulmon Dis. 2012;7:1-9.
Patients not receivingrecommended
maintenance therapy
16

Exac
erba
tions
per
yea
r
CAT < 10mMRC 0-1
CAT > 10 mMRC > 2
GOLD 3-4
GOLD 1-2 SAMA prn
orSABA prn
LABA or
LAMA
ICS* + LABAor
LAMA
Global Strategy for Diagnosis, Management and Prevention of COPD
Manage Stable COPD: Pharmacologic TherapyRECOMMENDED FIRST CHOICE
A B
DC
ICS* + LABAand/orLAMA
© 2015 Global Initiative for Chronic Obstructive Lung Disease
2 or more or
1 with hospitaladmission
0-1 (without hospital admission)
Spiro
met
ricSe
verit
y

Exac
erba
tions
per
yea
r
0
CAT < 10mMRC 0-1
GOLD 4
CAT > 10 mMRC > 2
GOLD 3
GOLD 2
GOLD 1
Global Strategy for Diagnosis, Management and Prevention of COPD
Manage Stable COPD: Pharmacologic TherapyALTERNATIVE CHOICE
A B
DC
© 2014 Global Initiative for Chronic Obstructive Lung Disease
2 or more or
> 1 leadingto hospitaladmission
1 (not leadingto hospitaladmission)
LAMA and LABA or
LAMA and PDE4-inh or
LABA and PDE4-inh
ICS + LABA and LAMA or
ICS + LABA and PDE4-inhor
LAMA and LABA or
LAMA and PDE4-inh.
LAMA or
LABAor
SABA and SAMA
LAMA and LABA

Relieve symptoms Improve exercise tolerance Improve health status
Prevent disease progression Prevent and treat exacerbations Reduce mortality
Reducesymptoms
Reducerisk
Global Strategy for Diagnosis, Management and Prevention of COPD
Manage Stable COPD: Goals of Therapy
© 2015 Global Initiative for Chronic Obstructive Lung Disease

• Avoidance of risk factors• Smoking cessation!!!!!! (there are not enough exclamation points on my keyboard)
- Avoid/Reduce of indoor pollution- Reduce occupational exposure
• Influenza vaccination• Pneumococcal Vaccine
Global Strategy for Diagnosis, Management and Prevention of COPD
Manage Stable COPD: All COPD Patients
© 2015 Global Initiative for Chronic Obstructive Lung Disease

Pulmonary Rehabilitation: What does it do?
Lacasse Y et al. Lancet. 1996;348:1115-1119.
-2 -1 0 1 2 3 4Effect Size (SD units)
McGavin, 1977
Cockcroft, 1981Booker, 1984
Jones, 1985
Lake, 1990
Simpson, 1992
Weiner, 1992
Goldstein, 1994
Wijkstra, 1994
Guell, 1995
Strijbos, 1996
Overall effect
Study Favors control Favors treatment
• Dyspnea as a function of O2 consumption• The muscles lose their mitochondrial machinery from
inactivity• Rehab gradually recovers the function of this “cog”
O2 in
CO2 outO2 delivery
(Don’t forget
Hemoglobin and
vascular diseaseOxidative respiration
(This is costly to
maintain)

Pulmonary Rehabilitation: Outcomes
Outcome Control Rehab PDeaths (n) 12 6 NSHospitalized (n) 41 40 NSRespiratory admissions/pt 1.9 1.4 .04All-cause admissions/pt 2.2 1.7 .048Hospital days
(respiratory) 18.1 9.4 .021Hospital days
(all causes) 21.0 10.4 .022
Griffiths TL et al. Lancet. 2000;355:362-368.

• Emphysema by Hx/PE/HRCT
• FEV1 ≤ 45%; TLC > 100%; RV ≥ 150%
• pCO2 ≤ 60, pO2 ≥ 45• BMI ≤ 31.1 males, ≤ 32.3 females
• Exclusion• Previous thoracic
surgery• Significant CV disease
• Exclusionary pulmonary disease
• Unsuitable HRCT• Unplanned weight loss
• Life-threatening systemic disease
• No consentThe National Emphysema Treatment Trial Research Group. Chest. 1999;116:1750-1761.The National Emphysema Treatment Trial Research Group. NEJM 2001; 345: 1075-83
Lung Volume Reduction Surgery‘NETT; inclusion and exclusion criteria

Years after randomization0 1 2 3 4 5 6 7 8
Prob
abilit
y of d
eath
0.0
0.2
0.4
0.6
0.8
1.0
Medical
LVRS
608 526 496 454 352 227 122 29 LVRS 610 564 507 441 335 210 99 29 Medical
Overall P=0.02
P2 yr=0.48
P5 yr=0.02
Lung volume reduction surgery reduces mortality compared with medical management in selected patients with severe emphysema
RR = 0.85
Naunheim et al. Ann Thorac Surg 2006; 82: 431-43

Emphasys Endobronchial Valve TM
• Stent-like retainer
• Flexible seals
• One-way valve
• Removable
Key Features
Investigational device only. Not currently approved for sale.

Lung Transplantation
- Survival following transplant:
- 2 years, 60-65%; 40% at 5 years
- Average waiting time for Tx: 2 y
J Heart Lung Transplant 1998:17;703
Oxygen therapy
- Survival benefit for resting hypoxia
- NO benefit for exercised induced hypoxia
- Oxygen does NOT relieve dyspnea better than placebo

Oxygen in COPDIn the 1980s, two landmark trials, (NOTT) (1980) and the MRC (1981), showed that long-term oxygen therapy (LTOT, ≥ 18 hr/day) was the sole treatment that improved survival in patients with COPD.
Nocturnal Oxygen Therapy Trial Group. Ann Intern Med 1980;93:391–398.
Medical Research Council Working Party. Lancet 1981;1:681–686.
Indications for Long-term Oxygen Therapy (LTOT) in COPDPaO2 <55 mmHg or SaO2 < 88% (room air)PaO2 56–59 mmHg or SaO2 89%–90%, with (one or more):
Pulmonary hypertensionEvidence of cor pulmonale or edema due to heart failureElevated hematocrit (>56%)

NEJM 2016;375(17):1617-27
• After seven months and the randomization of only 34 patients, the trial was redesigned to also include patients with moderate exercise-induced desaturation (SpO2 ≥ 80% for ≥5 minutes and <90% for ≥10 second during 6-minute walk test)
• Ultimately 738 patients were randomized to receive long-term supplemental oxygen versus (24-hour oxygen for those with resting desaturation and during exercise and sleep for those with exercise desaturation) no long-term supplemental oxygen.

NEJM 2016;375(17):1617-27
• No difference between groups in time to death or first hospitalization (hazard ratio 0.94; 95% CI 0.79-1.12; p=0.52).
• No difference in rates of hospitalization, COPD exacerbations, quality of life, lung function or 6 MW distance

GOLD Grading System:FEV1 Airflow Limitation
30Global Initiative for Chronic Obstructive Lung Disease (GOLD). GOLD COPD web site. http://www.goldcopd.org/uploads/users/files/GOLD_Report_2015_Apr2.pdf. Accessed June 18, 2015.
Postbronchodilator FEV1/FVC <.70 • Confirms presence of persistent airflow limitation
• Supports diagnosis of COPD
GOLD Grade 4
GOLD Grade 1
GOLD Grade 2
GOLD Grade 3
• Mild• FEV1 ≥80% predicted
• Moderate• 50% ≤FEV1 <80%
predicted
• Severe• 30% ≤FEV1 <50% predicted
• Very severe• FEV1 <30% predicted

COPD: Summary• Diagnosis
• You can’t diagnose if you don’t look (40% rule)• Ask patients at risk about exercise tolerance (Are you able to do
everything you like to do without worrying about your breathing?”, cough, sputum production
• Treatment Goals: reduce symptoms, prevent exacerbations, manage risk factors (SMOKING!)
• Flu vaccine, pneumococcal vaccines. • Supplemental oxygen should be reserved for treating hypoxia, not
dyspnea

Questions/Discussion…