Embed Size (px)
Citation preview
10/22/21
1
Neuropsychiatric SymptomsDiagnosing & Clinical Decision Support
1
Nicole ConiglioCo-Founder, President, & CMO Psych360
2

10/22/21
2
BioNicole Coniglio is the President, Chief Medical Officer, and Founding Member of Psych360. Since 2015, her strategic and clinical leadership has grown Psych360 from a startup to the largest long-term care mental health platform in Ohio serving over 250 long-term care communities through more than 50,000 annual patient encounters. As a visionary leader in providing psychiatric and psychological solutions in the long-term care industry, Nicole has a passion for evidence-based mental health care, patient experience, and improved quality of life for underserved populations.
Nicole’s leadership and board experience extends to the PALTC Behavioral and Mental Health Advisory Council, the Geriatric Practice Management Corp, and the Ohio Association of Advanced Practice Nurses. She has been asked to speak at engagements for the American Society of Consultant Pharmacists, the Ohio Health Care Association, Leading Age, the Geriatric Association of Advanced Practice Nurses, and the Ohio Society of Healthcare Risk Managers.
Nicole graduated from Kent State University with her Master of Science in Nursing degree and received her Psychiatric Mental Health Nurse Practitioner Post-Master’s Certificate from the University of Cincinnati.
3
OBJECTIVES
NEUROPSYCHIATRIC & BEHAVIORAL SYMPTOMS
ASSOCIATED WITH DEMENTIA
TYPES OF DEMENTIA, DIAGNOSIS, &
DIFFERENTIALS
SCREENING TESTS FOR DIAGNOSIS
4
NON-PHARMACOLOGIC INTERVENTIONS
5
4
10/22/21
3
Neuropsychiatric Symptoms in Dementia
98% Incidence
5
Behavioral Disturbances Associated with Dementia● Behavioral disturbances can be
difficult to manage, causing stress to the patient and their caregivers.
● Behaviors can fall into 3 different symptom groups::
➔ Activity Disturbances ➔ Mood Disturbances ➔ Thought and Perceptual
Disturbances 14
6
10/22/21
4
4 Categories of Behavioral Disturbances
7
Physically AggressiveHitting, kicking, bitng, scratching, spitting, pinching
Verbally AggressiveCursing, screaming, or
threatening
Physically Non-AggressivePacing, wandering, inappropriately handling objects, exit-seeking
Verbally Non-AggressiveConstant repetition of sentences or requests
7
UNMET NEEDSAddress Underlying NeedsWhat is causing the inappropriate behavior?
True cause of SymptomsPossible sensory deprivation, boredom, and/or loneliness. Others may need lower lighting, good toileting procedures, better communication, or appropriate pain treatment
18
8
10/22/21
5
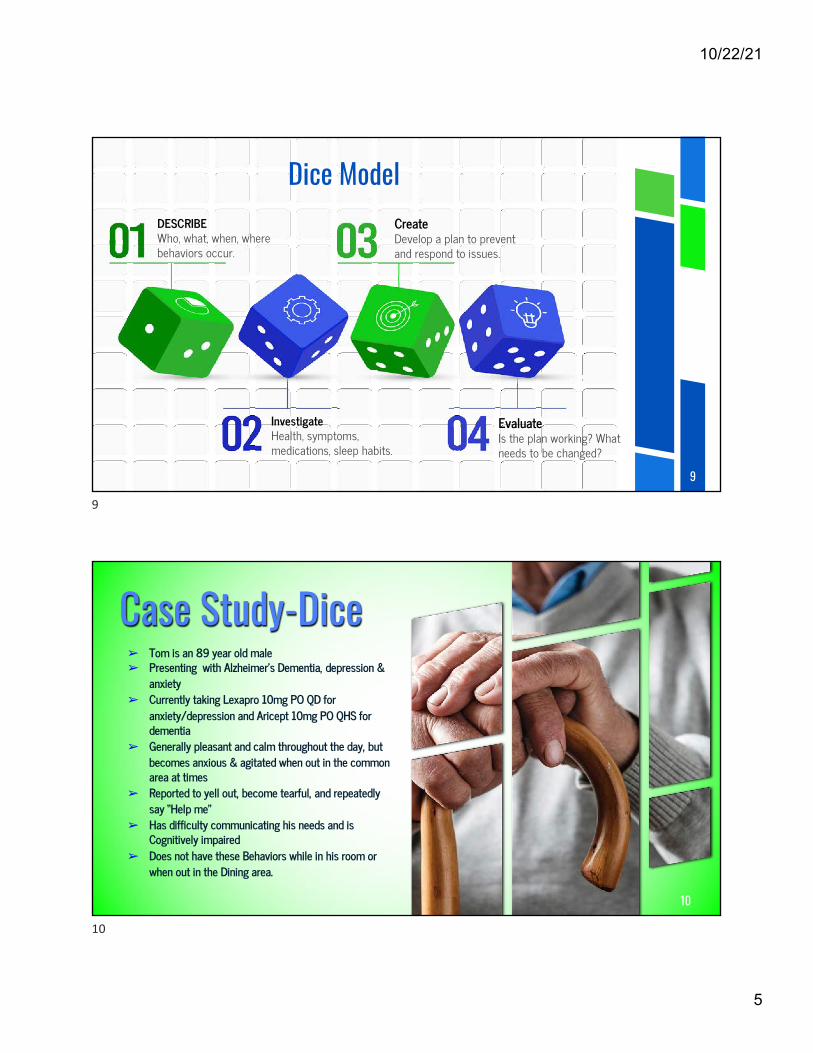
Dice Model
9
DESCRIBEWho, what, when, where behaviors occur.
InvestigateHealth, symptoms, medications, sleep habits.
CreateDevelop a plan to prevent and respond to issues.
EvaluateIs the plan working? What needs to be changed?
9
Case Study-Dice➢ Tom is an 89 year old male➢ Presenting with Alzheimer’s Dementia, depression &
anxiety➢ Currently taking Lexapro 10mg PO QD for
anxiety/depression and Aricept 10mg PO QHS for dementia
➢ Generally pleasant and calm throughout the day, but becomes anxious & agitated when out in the common area at times
➢ Reported to yell out, become tearful, and repeatedly say “Help me”
➢ Has difficulty communicating his needs and is Cognitively impaired
➢ Does not have these Behaviors while in his room or when out in the Dining area.
10
10
10/22/21
6
Activity Disturbance▸ Agitation▸ Wandering▸ Verbal or Physical
Aggression▸ Resisting care▸ Apathy▸ Impulsiveness
▸ Eating Disturbances▸ Sleep Problems▸ Diurnal/Sleep-wake
cycle disturbances▸ Socially Inappropriate
Behaviors▸ Repetitive Behaviors
50-80% cognitively impaired LTC residents have Agitation or Aggression
11
Mood Disturbances
Elation Anxiety
Mood / LabilityFluctuations
Irritability
24
12
10/22/21
7
Thought & Perceptual DisturbancePsychosis▸ 40% AD▸ 16-75% PD❖ Delusions
➢Fixed false beliefs
➢Paranoia
❖ Hallucinations
➢ Hearing or seeing non-present entities
13
Diagnosis(1) a comprehensive history;
(2) a complete physical and neurologic examination
- cognitive, behavioral, and activities of daily living assessment;
(3) laboratory and neuroimaging studies
14
10/22/21
8
HistoryO- onsetL- LocationD- DurationC- CharacteristicsA- AggravatingR- RelievingT- Treatment
15
Emotional Metabolic Traumatic /TumorsEndocrine Infectious StrokeAuto-
ImmuneDegenerative
Alzheimer’s DiseaseParkinson’s DiseasePick’s Disease
DepressionPsychosis
Liver failurekidney failureToxins
Hypothyroidism Brain injuryCancer
BacterialFungalViralPrion
Multiple sclerosislupus
Brain InfarctionHemorrhage
DifferentialsMedical conditions that can cause Dementia
Encephalopathy or Delirium Mental Retardation Language Disorders Psychiatric Disorders
Drugs Cerebral Palsy Strokes Depression
Differential Diagnosis for Dementia
16
10/22/21
9
Disease 1st Symptom Mental Status Neuropsychiatry Neurology Imaging
Alzheimer's Disease
Memory Loss Episodic Memory Loss
Initially Normal Initially Normal Entorhinal Cortex and Hippocampal Atrophy
Fronto-temporal Dementia
Apathy; poor judgment/insight, speech/language;
hyperorality
Frontal/executive, language; spares
drawing
Apathy, disinhibition, hyperorality,
euphoria, depression
May have vertical gaze palsy, axial
rigidity, dystonia, alien hand, or
MND
Frontal, insular, and/or temporal atrophy; spares posterior
parietal lobe
Dementia with Lewy
Bodies
Visual hallucinations, REM
sleep disorder, delirium, Capgras'
syndrome, parkinsonism
Drawing and frontal/executive; spares memory; delirium prone
Visual hallucinations, depression, sleep
disorder, delusions
Parkinsonism Posterior parietal atrophy; hippocampi
larger than in AD
Vascular Dementia
Often but not always sudden;
variable; apathy, falls, focal weakness
Frontal/executive, cognitive slowing; can spare memory
Apathy, delusions, anxiety
Usually motor slowing, spasticity;
can be normal
Cortical and/or subcortical infarctions, confluent white matter
disease
17
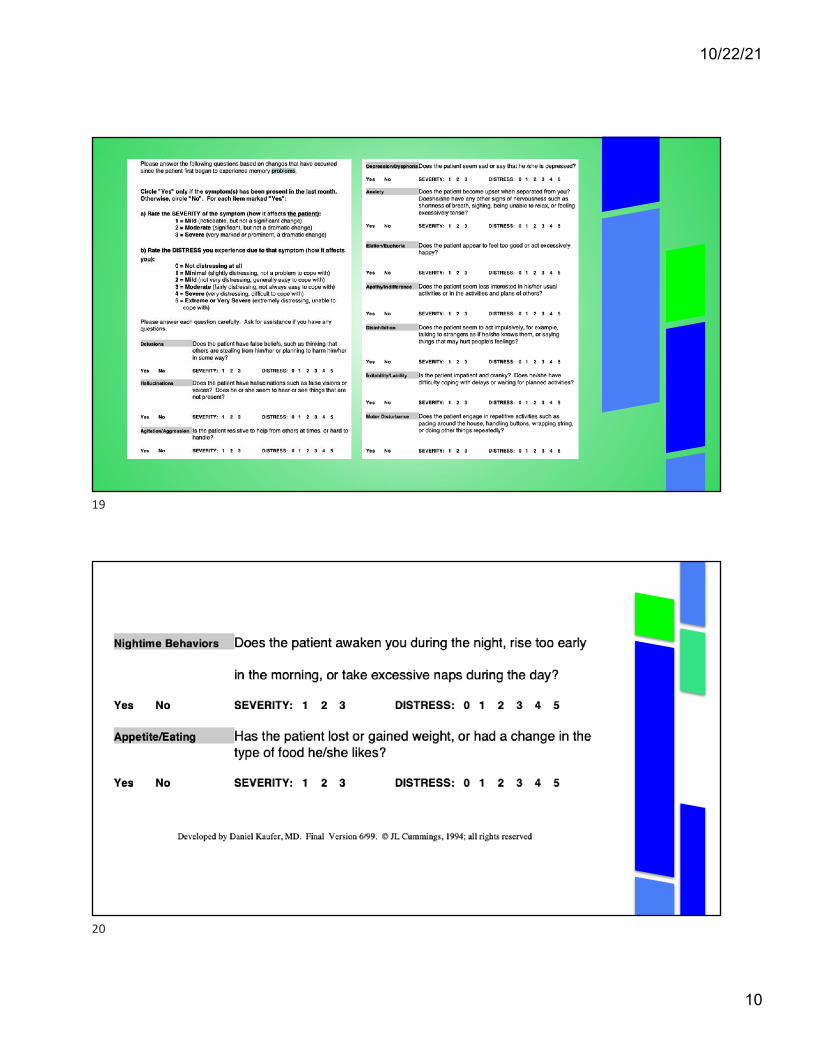
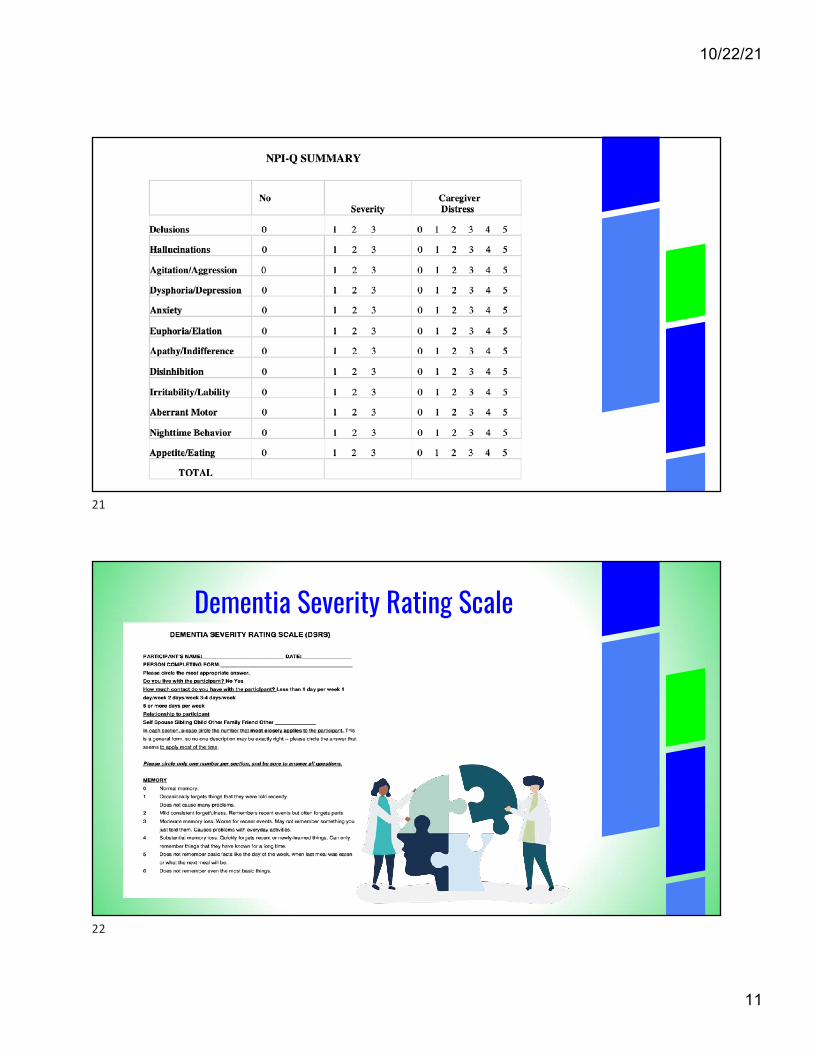
NPI-Q► Self-administered questionnaire
► Review of the previous month
► 12 NPI-Q Domains► Rate the Severity of
Symptoms (3 pt scale)
► Rate the caregiver distress (5 pt scale)
Initial response “Yes” or “No”Yes responses
►
18
10/22/21
10
19
20
10/22/21
11
21
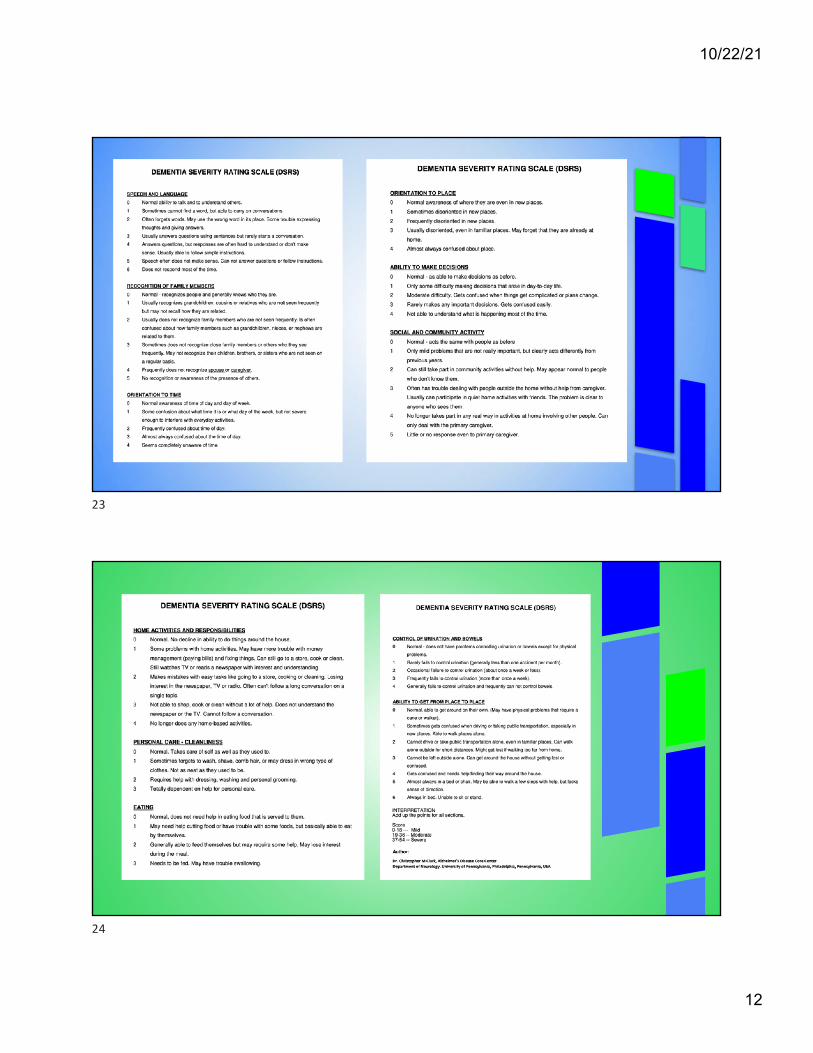
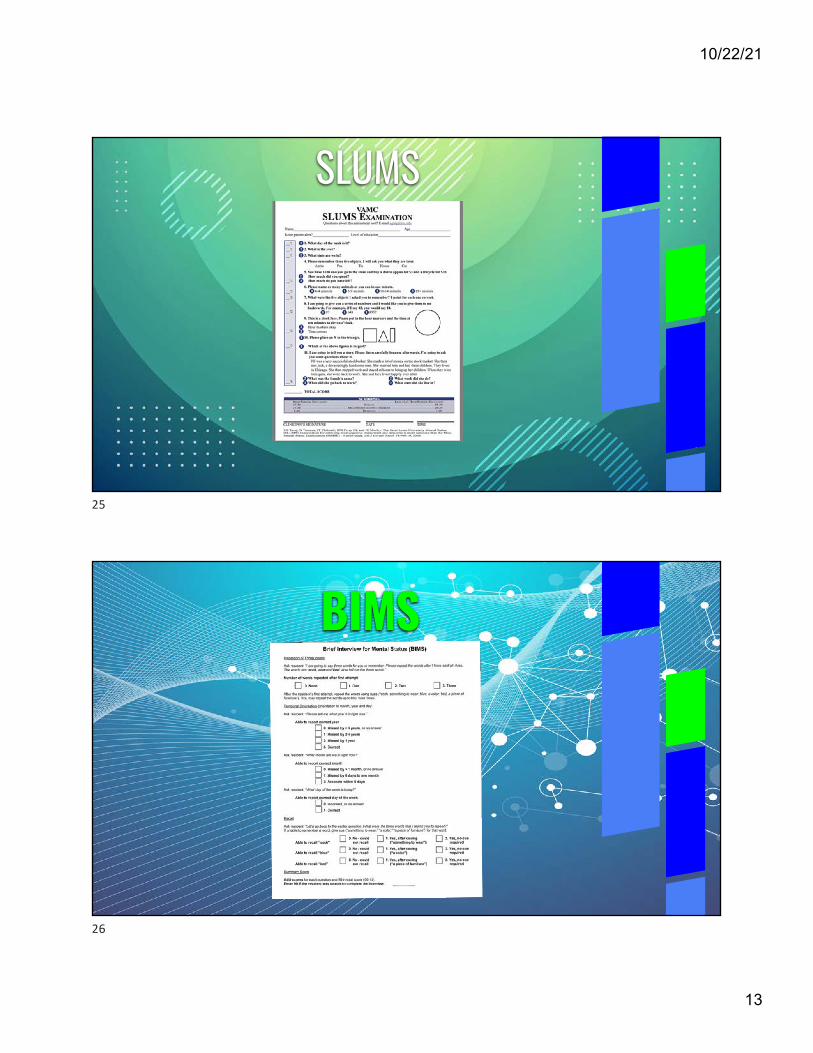
Dementia Severity Rating Scale
22
10/22/21
12
23
24
10/22/21
13
SLUMS
25
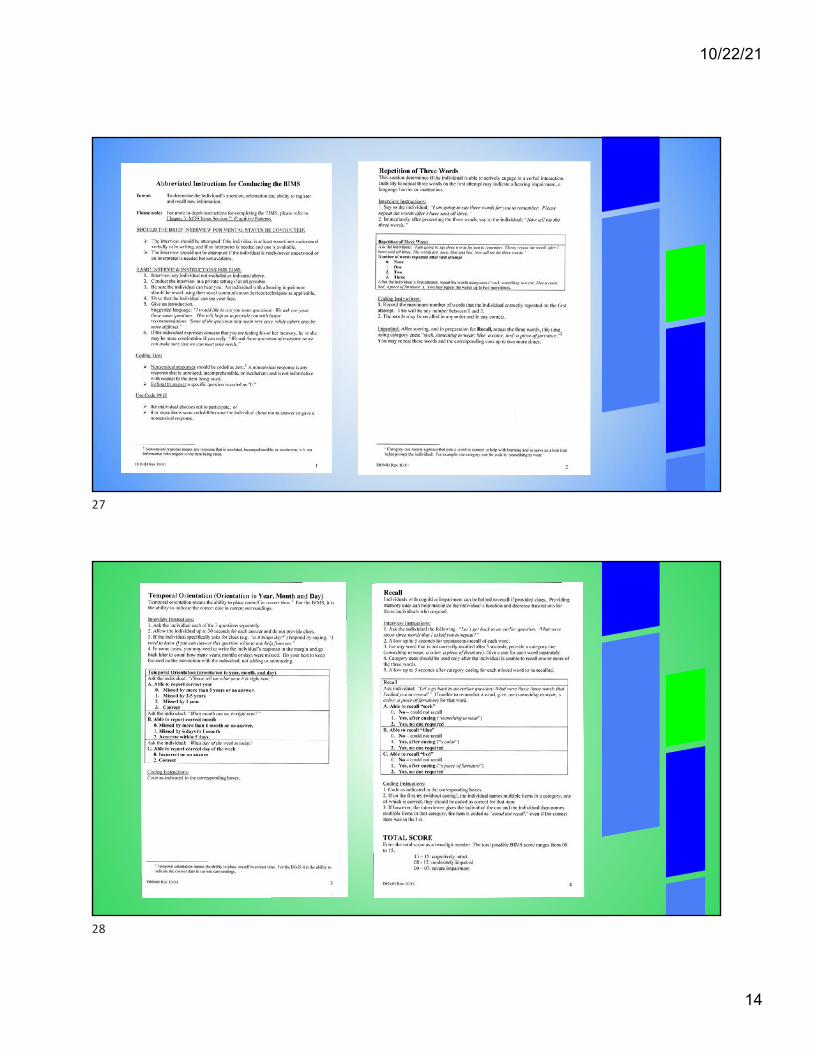
BIMS
26
10/22/21
14
27
28
10/22/21
15
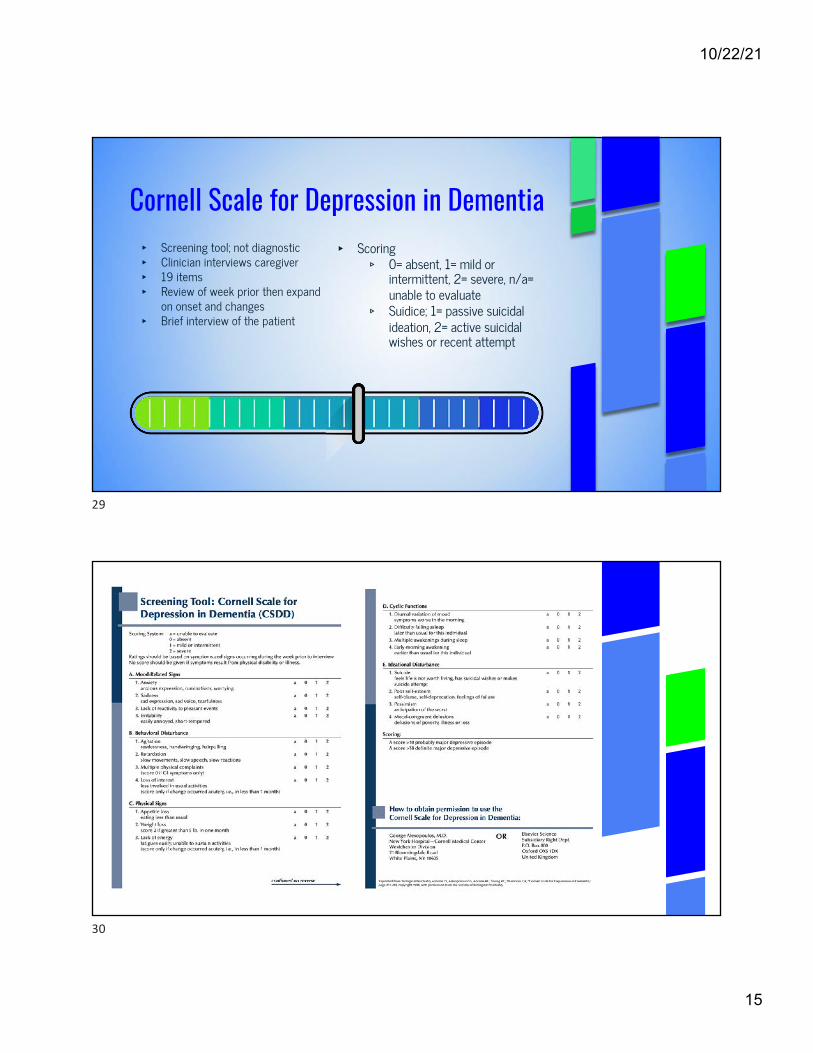
Cornell Scale for Depression in Dementia▸ Screening tool; not diagnostic▸ Clinician interviews caregiver▸ 19 items▸ Review of week prior then expand
on onset and changes▸ Brief interview of the patient
▸ Scoring▹ 0= absent, 1= mild or
intermittent, 2= severe, n/a= unable to evaluate
▹ Suidice; 1= passive suicidal ideation, 2= active suicidal wishes or recent attempt
29
30
10/22/21
16
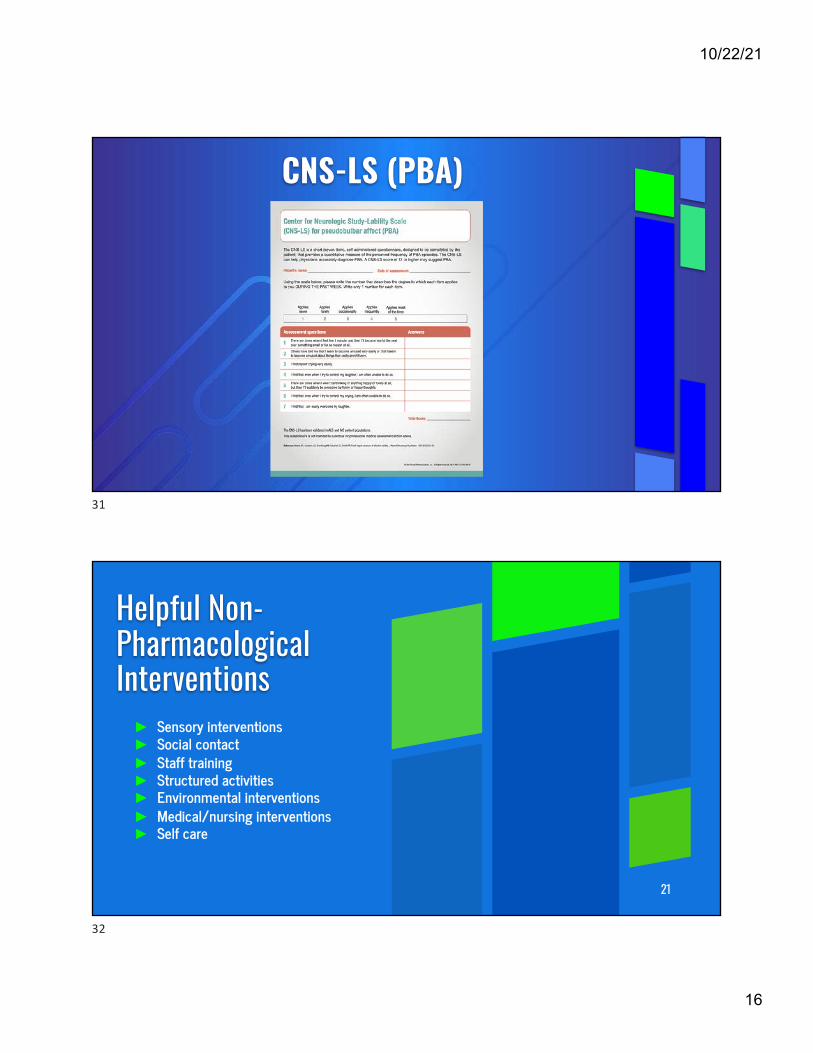
CNS-LS (PBA)
31
Helpful Non-Pharmacological Interventions► Sensory interventions ► Social contact► Staff training► Structured activities ► Environmental interventions ► Medical/nursing interventions► Self care
21
32
10/22/21
17
IMPORTANCE OF NON-PHARMACOLOGICAL INTERVENTIONS
ADVERSE REACTIONSAND RISKS Control Behaviors REDUCE PATIENT AND
CAREGIVER DISTRESS
33
33
Sensory Interventions
34
Sounds❑Music❑White noise❑Decreasing noise
Touch❑Hand Massages
Smell❑ Essential Oils
34
10/22/21
18
Social Contact
35
● Pet Therapy● One to One Interaction● Patient Activities and Socialization Groups● Personal Relationships with Family and Friends
35
Staff Training
36
● Training on adapting ADL’s to patient levels
● Communication skills● Empathy training● Crisis Prevention Intervention
training/Trauma Informed Care
● Teepa Snow training
In-Service Training on Various Topics
36
10/22/21
19
Structured Activities
37
● Games● Social Activities● Singing ● Physical Activities● Reminiscence Therapy
37
Environmental Interventions
38
● Wandering Areas● Nature Enhanced Environments● Reduced Stimulation ● Reassuring Safety
38
10/22/21
20
MEDICAL/NURSING CARE▸ Sleep▸ Hygiene Interventions▸ Pain Management▸ Meeting Patient Needs▸ Communication▸ Empathy▸ Redirection/Reorientation▸ Continuity of Care▸ Maintaining Schedule and Familiarity▸ Having Patience
39
39
Conclusion▸ 98% incidence Neuropsychiatric Symptoms of Dementia▸ Non-Pharmacologic measures most effective▸ Pharmacologic measures
▹ 84% of nursing home and 29% of community-dwelling elders residing in the USA
▸ Presence of neuropsychiatric symptoms leads to greater functional impairment in patients with dementia & cognitive impairment
▸ Behaviors accelerate or lead to Nursing home placement
40





























