Embed Size (px)
Citation preview

Diagnosi di HPV: I dati mondiali ed europei
Convegno Nazionale GISCi , Orvieto 2008
Silvia Franceschi
International Agency for Research on Cancer150 cours Albert Thomas
69372 LyonFrance

La mia presentazione di oggi:
• Frequenza dell’HPV (soprattutto IARC HPV Surveys).
• La diffusione del vaccino HPV nel mondo.
• Nuovi sviluppi nello screening (VIA e Fast HPV test).

All cases (n=14,097)
0
20
40
60
16 18 33 45 31 58 52 35HPV type
%Africa (n=1,373)
0
20
40
60
16 18 33 45 35 31 58 52HPV type
%
Asia (n=5,652)
0
20
40
60
16 18 58 33 52 45 31 35HPV type
%Europe (n=4,334)
0
20
40
60
16 18 33 31 45 35 58 56HPV type
%
North America(n=1,311)
0
20
40
60
16 18 31 33 45 52 35 58HPV type
%South and CentralAmerica (n=1,427)
0
20
40
60
16 18 31 45 33 58 52 35HPV type
%
8 most common HPV types in 14,097 cases of invasive cervical cancer by region
70%
72%
67% 74%
76%65%

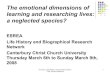
IARC Multi-centric HPV Prevalence Survey• Population-based samples of approx. 1000 women
• 100 women per 5-year age group
• Testing for at least 36 HPV types using GP5+/6+ PCR
and antibodies against 6 HPV types.
China
Lampang
Argentina
IARC Multi-centre HPV Prevalence Surveys
HanoiHo Chi Minh
Korea
ColombiaNigeria
Spain
Songkla
Chile
Italy
ShenzhenMexico
The Netherlands
India
completed ongoing
Mongolia
Algeria
Guinea Uganda
Poland
ShenyangShanxiNepal
Pakistan
IranGeorgia

Prevalence of cervical HPV DNA in sexually active women IARC Multi-centre HPV Prevalence Survey, 1995-2002
MongoliaNigeriaChina, ShenzhenArgentina IndiaChina, ShenyangPolandColombiaChina, ShanxiChileMexicoKoreaVietnam, Ho Chi Minh Italy, TurinThailand, LampangNetherlandsThailand, SongklaSpain Vietnam, Hanoi
999933534908
1940685834
1981671971
1340870918
101310243299716908
1007
0 5 10 15 20 25 30 35
hpv 16 or 18other high-risk typelow-risk type only

Age-specific high risk HPV prevalence in Manchester, 1988-93 and 2001-03
(Kitchener and Peto, 2006)
0
5
10
15
20
25
30
35
40
45
20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59Age group (years)
HPV
pre
vele
nce
(%)
Manchester, 1988-93 (MY0911 PCR)
ARTISTIC, 2001-03 (Hybrid Capture II)
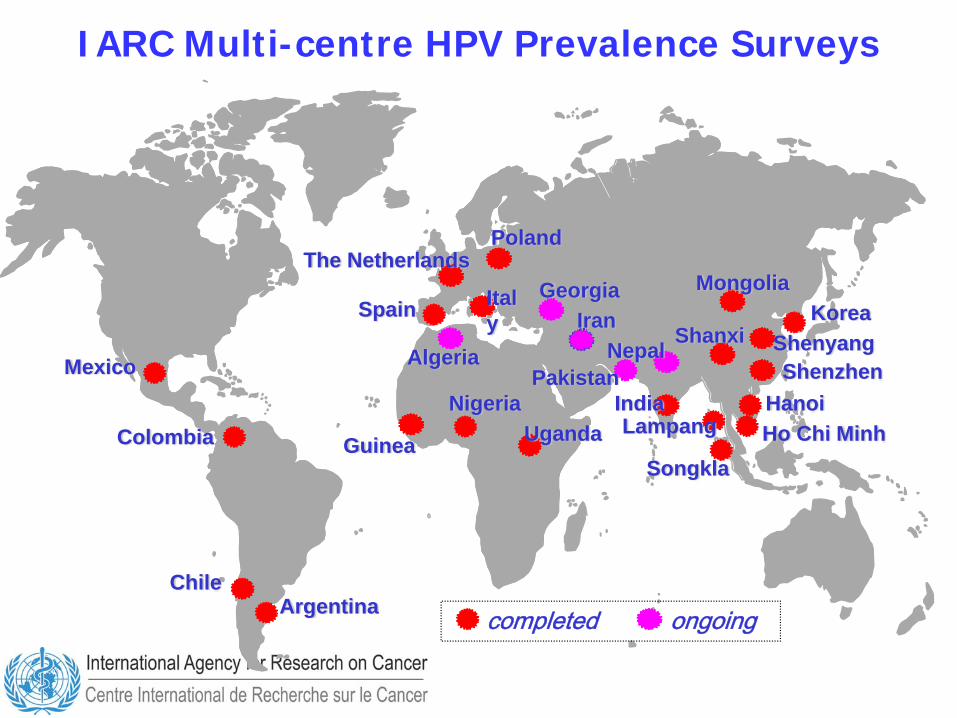
HPV 16 0r 18 Other high-risk types
Prevalence of cervical HPV DNA by age and HPV typeIARC Multi-centre HPV Prevalence Survey
Low-risk types only

Prevalence of cervical HPV DNA by age and HPV typeHPV 16 0r 18 Other high-risk types Low-risk types only
05
10152025303540
<25 25-34 35-44 45-54 55+Age group (years)
Prev
alen
ce (%
)
Poland, Warsaw
05
10152025303540
<25 25-34 35-44 45-54 55+Age group (years)
Prev
alen
ce (%
)
Italy, Torino

Prevalence of cervical HPV DNA by age and HPV typeHPV 16 0r 18 Other high-risk types Low-risk types only
Married
05
10152025303540
<25 25-34 35-44 45-54 55+Age group (years)
Prev
alen
ce (%
)
Poland, Warsaw
05
10152025303540
<25 25-34 35-44 45-54 55+Age group (years)
Prev
alen
ce (%
)
Italy, Torino

Prevalence of cervical HPV DNA by age and HPV typeHPV 16 0r 18 Other high-risk types Low-risk types only
Single/separated/widowedMarried
05
10152025303540
<25 25-34 35-44 45-54 55+Age group (years)
Prev
alen
ce (%
)
Poland, Warsaw
05
10152025303540
<25 25-34 35-44 45-54 55+Age group (years)
Prev
alen
ce (%
)
Italy, Torino

HPV infection in HIV-positive women
• Chronic infection with HPV 16, 18 and a dozen of other HPV types is considered the necessary cause of cervical cancer.
• Certain factors (e.g., high parity, long-term OC use, smoking, and immunodeficiency) can modify the probability of progression of HPV infection into precancerous lesions and cancer.
• HPV infections in HIV+ women are more likely to occur and persist than in HIV- women.
• Increased RRs of cervical cancer and precancerous lesions are seen among HIV+ women and their magnitude depends from screening practices, background HPV risk and competing causes of death in different areas of the world.

3
North America:
USA CanadaMexico
7
South America:
Brazil ArgentinaPeruColombiaChileEcuadorUruguay
18
Middle East & Africa:
Israel MoroccoUAEEgypt---------14 others
11 Asia Pacific:
AustraliaIndonesiaKoreaTaiwanHong KongSingapore--------------5 others
39
Europe:
Germany FranceUKSpainItaly---------34 others
Caribbean & Central America:
Costa RicaPuerto RicoGuatemalaBermuda--------------11 others
15
Gardasil/Silgard Approved in 93 Markets: Most Under Accelerated TimelinesIntelligence about approvals for GSK are not as timelyGlobal status of Merck Gardasil licensure, December 2007

Global status of GSK Cervarix® licensure, December 2007
Source: GSKbio, Belgium

Vaccine affordability and financing
• High-income (industrialized) countries—can afford to introduce HPV vaccine in the public sector, and several countries launched vaccine introduction in 2007.
• Poorest (GAVI-eligible) countries—will most likely have access to heavily subsidized vaccine from GAVI Alliance.
• Greatest difficulty now facing middle-income countries, that cannot afford current high prices and are not eligible for subsidized vaccine. Options under discussion:• Local private philanthropic financing schemes.• Tiered pricing for available vaccines, in accordance with capacity
to pay, promised by current manufacturers.• Eventual price decline as developing-country manufacturers enter
the market (starting 2015).

HPV vaccine theoretical/optimal global timeline for GAVI-eligible countries
Late 2008: WHO pre-qualifies HPV vaccine for UN procurement.WHO Strategic Advisory Group of Experts (SAGE) recommends global HPV vaccine use.GAVI/UNICEF/PAHO negotiate with manufacturers for HPV vaccine supply.
Early 2009: WHO issues position paper on HPV vaccine.GAVI incorporates HPV vaccine in portfolio of subsidized vaccines.GAVI invites eligible countries to apply for vaccine.
Mid 2010 : Vaccine delivered to first countries.

Regional Group Purchasing

PATH demonstration projects on HPV vaccine, 2007–2011
Build on results of formative research to
design, implement, and evaluate cervical cancer
vaccine delivery to young girls.

source: WHO/EIP Burden of Disease Projections –http://www.who.int/healthinfo/statistics/bodprojections2030/en/index.html
Peru
Uganda
India Vietnam
Four project countries
Age-adjusted cervical cancer incidence rates

Ideal age group for vaccination
Girls aged 10–13 years• Before sexual debut and exposure to the virus
that causes cervical cancer—for highest impact.• Age when girls are easier to reach efficiently.• First priority given to single cohort in low-
resource settings. • Vaccinating older adolescents and young women
(“catch-up”) less cost-effective and logistically more difficult; gives earlier result but with much lower “net” benefit.

Service delivery options
• School-based programs (all four countries).
• Comparing performance during and outside Child Health Days (Uganda).
• Comparing performance with and without community outreach for out-of-school girls (Peru, India).
• Comparing performance in school-based and health facility-based settings (Vietnam).

22
Characterictics of screening testsfor secondary prevention
Characteristics
Comments
Number of visits required for screening and treatment
Conventional cytology
HPV DNA tests
Visual inspection tests
Sensitivity
Specificity(for high-grade lesions and invasive cancer)
47-62% 66-100% 78-98%
60-95% 62-96% 49-86%
VIA VILI
67-79%
73-91%
Assessed over the last 50 years in a
wide range of settings in developed
and developing countries
2 or more visits
Assessed over the last decade in many settings in developed and relatively few in
developing countries
2 or more visits
Assessed over the last decade in many settings in
developing countries
Assessed by IARC over the last four
years in India and 3 countries in Africa.
Need further evaluation for reproducibility
Can be used in single-visit or 'see and treat' approach
where outpatient treatment is available
Source: Sankaranarayan et al. Int J Obstet Gynaecol, 2005.

Cluster Randomised Controlled Trial of VIA Screening,
Dindigul District, India
R. Sankaranarayanan et al. Effect of visual screening on cervical cancer incidenceand mortality in Tamil Nadu, India: a cluster-randomised trial Lancet, August 4, 2007
• 113 Village clusters• 80 252 eligible women aged 30-59 years
• Intervention: Single screening• Follow-up: 7 years

Hazard ratio (95% CI)*
Control group 1.0
Intervention group (VIA)Overall
Cervical cancer incidence 0.75 (0.59-0.95)Cervical cancer death 0.65 (0.47-0.89)
30-39 yearsCervical cancer incidence 0.62 (0.40-0.96)Cervical cancer death 0.34 (0.18-0.66)
40-49 yearsCervical cancer incidence 0.82 (0.55-1.24)Cervical cancer death 0.55 (0.31-1.00)
50-59 yearsCervical cancer incidence 0.76 (0.50-1.16)Cervical cancer death 0.99 (0.58-1.66)
* C.I.: Confidence interval
Overall and age-specific hazard ratio for incidence for all cervical cancers and for cervical cancer deaths

Comparison of VIA, cytology and HPV testing, CIN2+, 2005-2008
StudyPlace Sensitivity (%) Specificity (%)
N. VIA Cyto HPV VIA Cyto HPV
Sarian et al, 2005
Brazil10,138 50 58 83 90 99 86
De Vuyst et al,2005
Kenya653 73 83 94 78 90 69
Sangwa-Lugomaet al, 2006
Congo1,571 56 72 - 65 95 -
Pretorius et al, 2007
China8,497 46 88 97 92 81 80
Almonte et al, 2007
Peru5,435 55 70 77 77 84 89
Li et al,submitted
China2,562 35 87 90 89 85 86

VIA sensitivity overestimated
• Only a fraction of VIA-negative findings underwent colposcopy in some studies (verification bias).
• In others, all VIA-negative findings underwent colposcopy, but colposcopy was shown to be an alloyed gold standard due to the correlation between visual inspection methods.
• When “random biopsies” (Pretorius et al, 2007) were used, the sensitivity of VIA, but not cytology or HPV test, diminished substantially.
Fast, affordable, accurate, and acceptable HPV tests are on horizon
PATH project - START (Screening Technologies to Advance Rapid Testing)
- New developments: rapid HPV DNA, E 6 onco-protein tests,
- R&D and commercialization of two different rapid tests for primary screening in low-resource settings.
-Development catalyzed through public-private partnerships- Tests will be provided to the public health sector in middle and low-income countries at a preferential price for at least ten years