Embed Size (px)
Citation preview
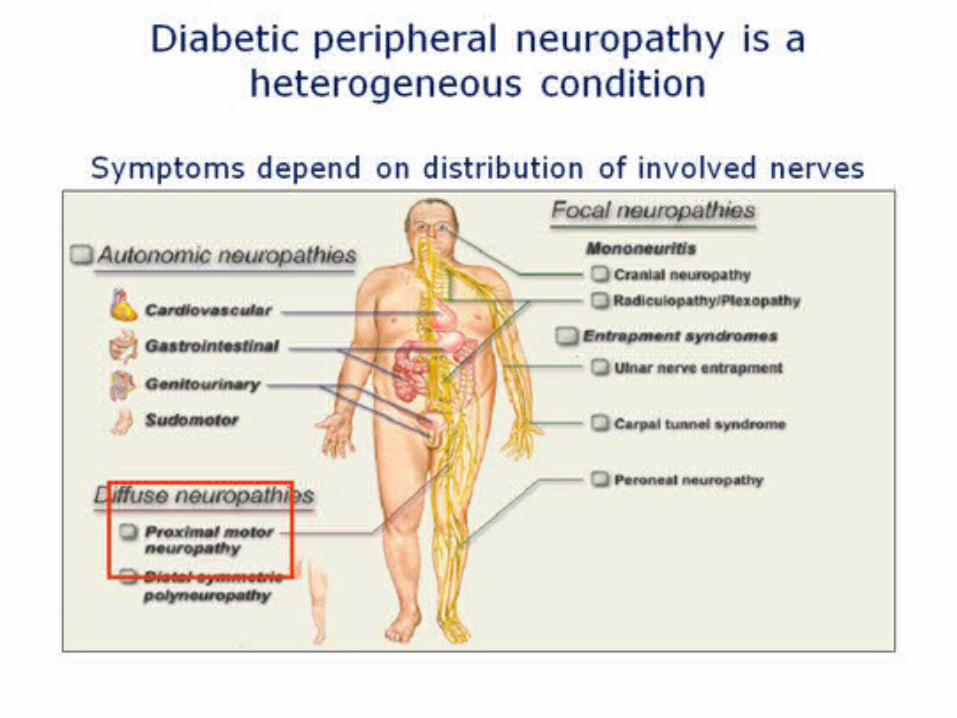
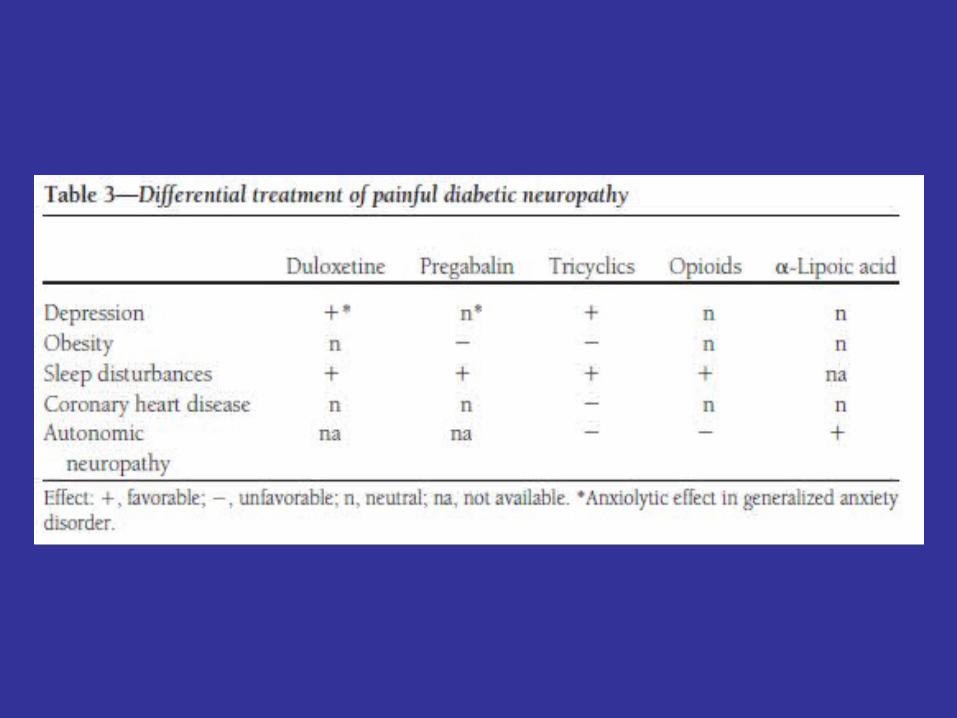
Diabetic neuropathy
Dr Jeff Kimber
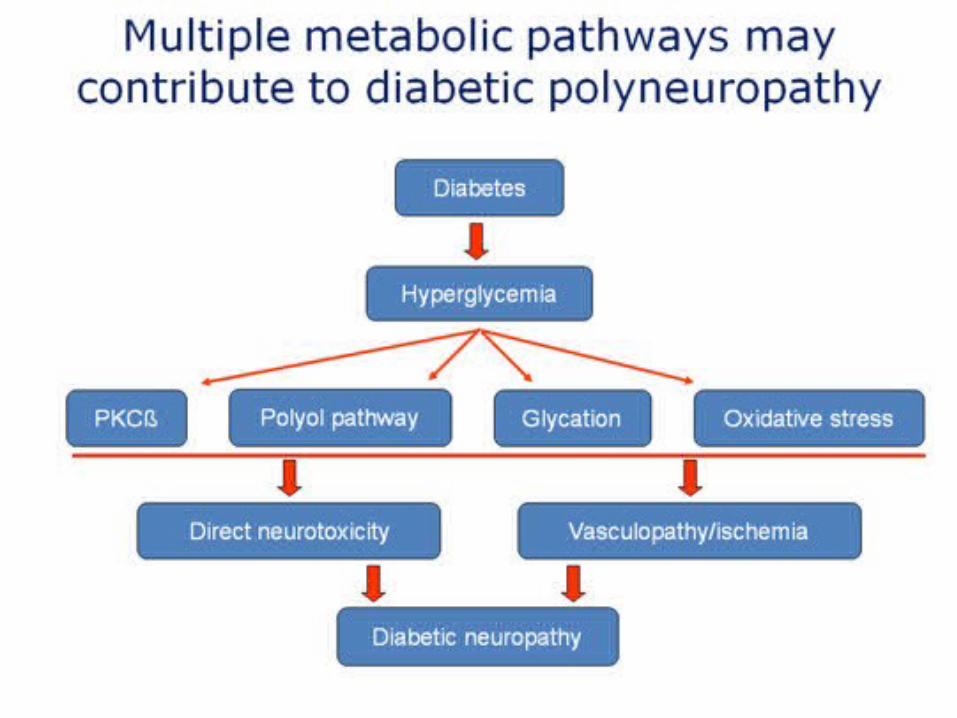
– Protein kinase C beta (PKCb) activation• altered expression of endothelial nitric oxide synthetase and vascular endothelial
growth factor . neurons and glial cells, are stimulated with growth, survival, and axonal outgrowth. It has potential for a dual impact on both the vasculature and neurons and could represent an important therapeutic intervention in diabetic neuropathy.
– Polyol pathway: an alternative metabolic fate for glucose. • Aldose reductase is a key enzyme in this pathway and generates sugar alcohols such
as sorbitol. In animal models of diabetes, there is an association between increased flux through the polyol pathway and a reduction in nerve conduction velocity (NCV), both of which can be ameliorated with aldose reductase inhibitors (ARIs). In humans this situation is not clear.
– Glycation: • Glycation involves the non-enzymatic reaction between glucose and amino groups of
proteins (forming a covalent attachment via the Amidori reaction). The rate of this reaction is proportional to the ambient concentration of glucose. Glycation of proteins may alter their function. There is also evidence for specific receptors for these glycated proteins. Interaction with these receptors may induce monocytes and endothelial cells to increase the production of cytokines and adhesion molecules. Intervention trials have used aminoguanidine to block the glycation reaction, or have utilised soluble receptors to block the downstream effects of receptor binding.
– Oxidative stress: • There is an increasing body of data to support the role of oxidative stress in the
pathogenesis of diabetic neuropathy in animal models. There is emerging evidence that single-nucleotide polymorphisms of the genes for mitochondrial and extracellular superoxide dismutases may confer an increased risk for the development of neuropathy.
Said G (2007) Diabetic neuropathy—a review
Nat Clin Pract Neurol 3: 331–340 doi:10.1038/ncpneuro0504
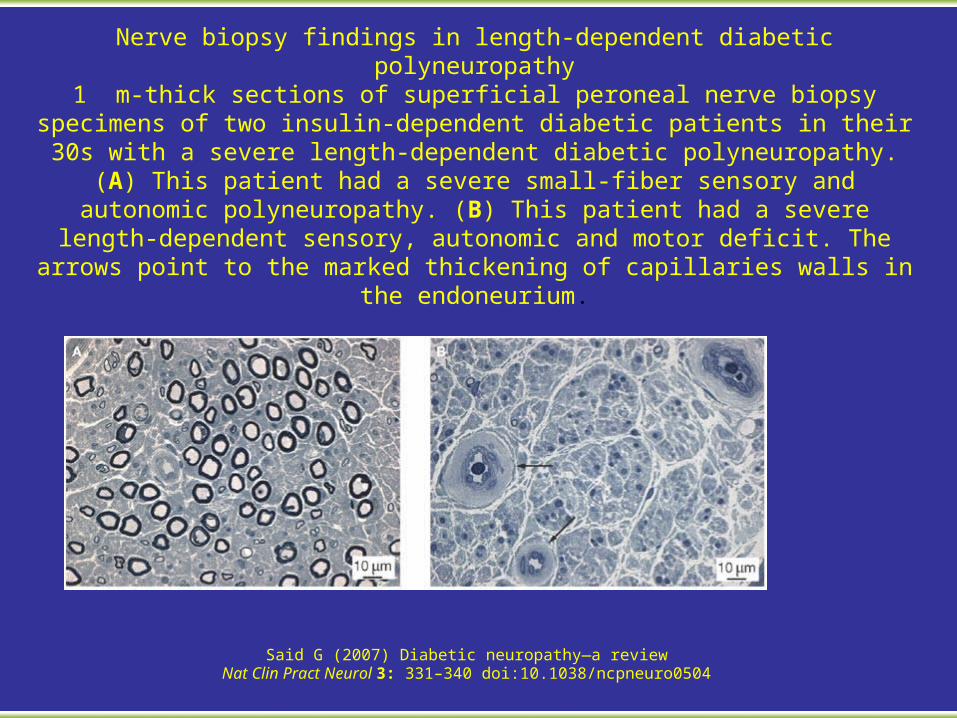
Nerve biopsy findings in length-dependent diabetic polyneuropathy1 m-thick sections of superficial peroneal nerve biopsy specimens of two insulin-dependent diabetic patients in their 30s with a severe length-dependent diabetic polyneuropathy. (A) This patient had a severe small-fiber sensory and autonomic
polyneuropathy. (B) This patient had a severe length-dependent sensory, autonomic and motor deficit. The arrows point to the marked thickening of
capillaries walls in the endoneurium.
Said G (2007) Diabetic neuropathy—a review
Nat Clin Pract Neurol 3: 331–340 doi:10.1038/ncpneuro0504
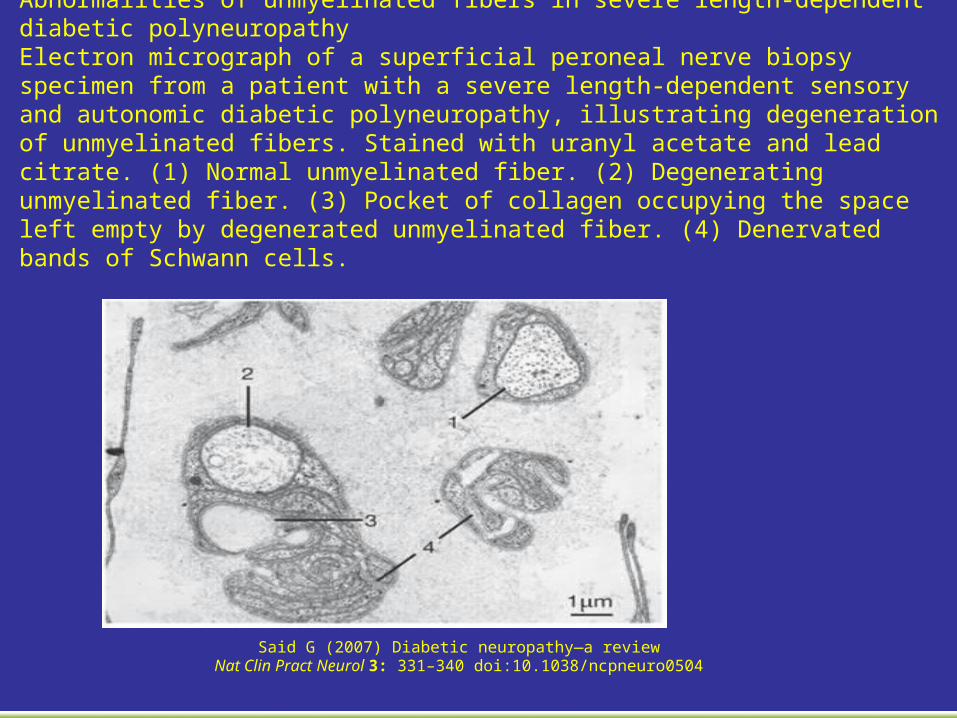
Abnormalities of unmyelinated fibers in severe length-dependent diabetic polyneuropathyElectron micrograph of a superficial peroneal nerve biopsy specimen from a patient with a severe length-dependent sensory and autonomic diabetic polyneuropathy, illustrating degeneration of unmyelinated fibers. Stained with uranyl acetate and lead citrate. (1) Normal unmyelinated fiber. (2) Degenerating unmyelinated fiber. (3) Pocket of collagen occupying the space left empty by degenerated unmyelinated fiber. (4) Denervated bands of Schwann cells.
Said G (2007) Diabetic neuropathy—a review
Nat Clin Pract Neurol 3: 331–340 doi:10.1038/ncpneuro0504
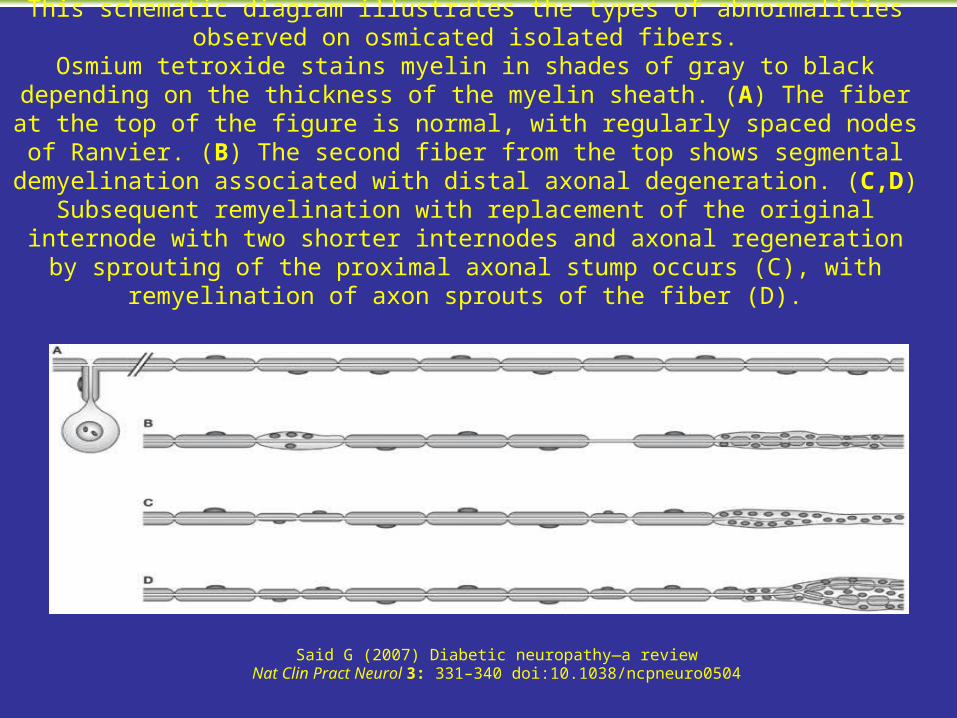
Abnormalities of isolated fibers in length-dependent diabetic polyneuropathyThis schematic diagram illustrates the types of abnormalities observed on osmicated
isolated fibers.Osmium tetroxide stains myelin in shades of gray to black depending on the thickness
of the myelin sheath. (A) The fiber at the top of the figure is normal, with regularly spaced nodes of Ranvier. (B) The second fiber from the top shows segmental demyelination associated with distal axonal degeneration. (C,D) Subsequent
remyelination with replacement of the original internode with two shorter internodes and axonal regeneration by sprouting of the proximal axonal stump occurs (C), with
remyelination of axon sprouts of the fiber (D).
– Pathology • Axonal loss
– Axon loss: Large & small axons in motor-sensory neuropathies – Younger patients with IDDM: Loss is uniform among fascicles – Older patients with NIDDM: May have multifocal axonal loss
• Axonal regeneration • Capillary walls: Thickened; Hyalinization (Reduplication of basement
membranes) • Axonal swellings in distal axons • Collagen: Increased around vessels
– Collagen I & III increase: A common change in many neuropathies
– Collagen IV, V, VI increase » Around endoneurial vessels » Collagen, Type VI increase relatively specific for diabetes
• Basal lamina: Tubes often persist after axonal degeneration
Said G (2007) Diabetic neuropathy—a reviewNat Clin Pract Neurol 3: 331–340 doi:10.1038/ncpneuro0504
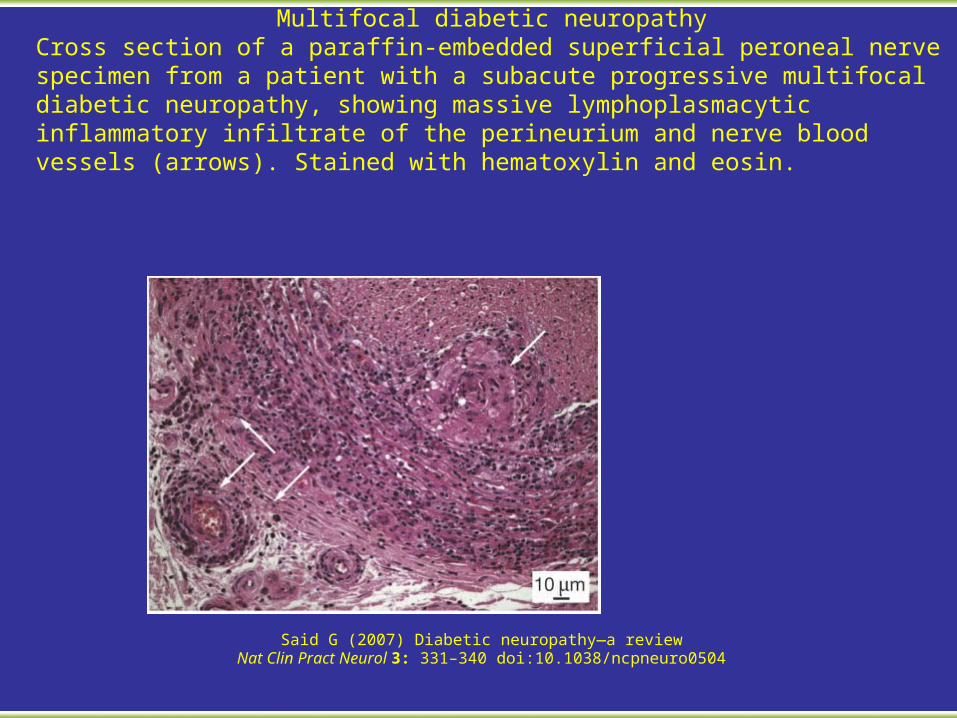
Multifocal diabetic neuropathyCross section of a paraffin-embedded superficial peroneal nerve specimen from a patient with a subacute progressive multifocal diabetic neuropathy, showing massive lymphoplasmacytic inflammatory infiltrate of the perineurium and nerve blood vessels (arrows). Stained with hematoxylin and eosin.
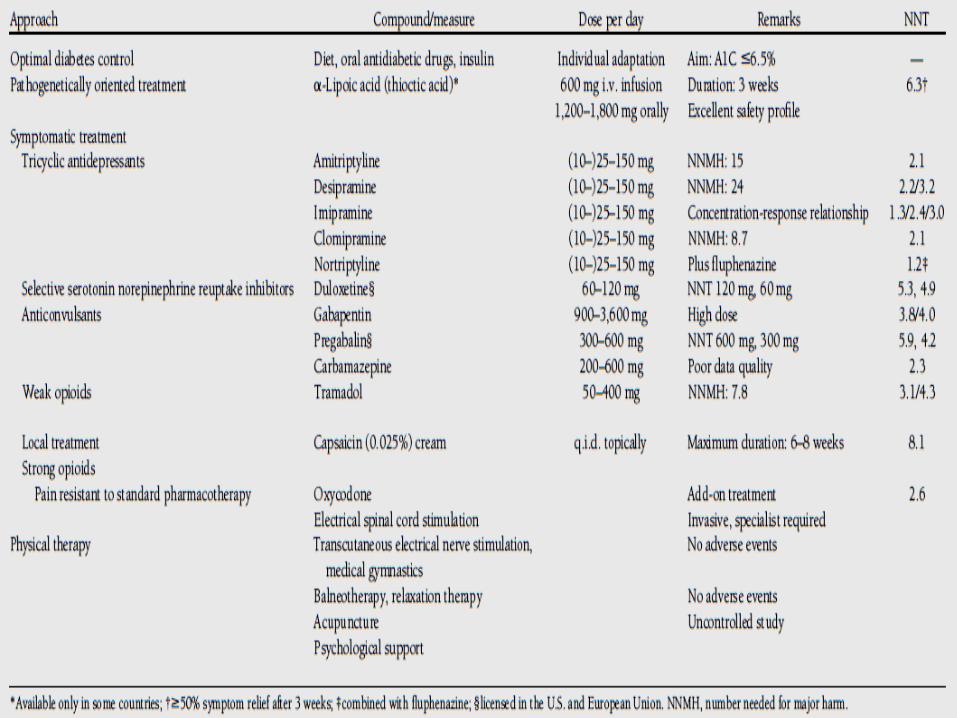
• Acute Diabetic Neuropathies • Acute painful
– Pain • Burning & hypersensitivity: Feet • May be severe • Often worse at night
– Signs: Often only mild changes • Mild sensory loss: Distal; Symmetric • Tendon reflexes: Normal or Reduced
– Associations • Poorly controlled diabetes • Recent onset insulin therapy • Rapid weight loss
– Improvement: After control of diabetes & weight gain
GI • Gastroparesis
– Gastric motor disorders are relatively common: Occur in up to 50% of brittle diabetics
– Symptoms • Discomfort: Nausea, Vomiting, Early satiety, Postprandial bloating, Diffuse epigastric
pain • Early satiety • Weight loss: Variable; May be profound • Some patients asymptomatic • Laboratory: Food residue retained in stomach
– Other associations • Poor correlation between symptoms and laboratory-demonstrated gastroparesis • Reversible component: Asociated with hyperglycemia
• Constipation – Most common lower-GI symptom: Up to 60% – Can alternate with episodes of diarrhea
• Nocturnal diarrhea – Profuse watery diarrhea
• May persist for hours to several days • Can be accompanied by fecal incontinence
– Associated with somatic & autonomic neuropathy – More common in type 1 diabetes – Rule out drug toxicity: Metformin
• Fecal incontinence – Due to: Incompetence of anal sphincter or Reduced rectal sensation – Exacerbated by diarrhea
• Hypohidrosis – Loss of thermoregulatory sweating – Initially distal: Glove-stocking distribution – May become diffuse: With more severe autonomic
neuropathies • Hyperhidrosis: Feet associated with coldness • Gustatory sweating
– Excessive facial sweating in response to food, especially spicy
– Associated with cervical sympathetic denervation • Skin: May be among earliest manifestations of
autonomic neuropathy • Mechanisms: Changes in microvascular skin
blood flow & sudomotor function • Clinical features: Dry skin; Hypohidrosis;
Development of ulcers, fissures & cracks
• Voiding dysfunction: Dysfuncton of bladder emptying – Frequency: Symptomatic in up to 50% of patients with diabetes,
and there is – Physiological evidence of bladder dysfunction: 43–87% of
insulin-dependent diabetes – Earliest manifestation of autonomic bladder dysfunction
• Impaired sensation • Increases the threshold for initiating micturition reflex
– Intermediate features: Reduced detrusor activity causes • Incomplete bladder emptying • Increased postvoid residual • Reduced peak urinary flow rate • Bladder overdistension
– Late features • Urinary retention • Overflow incontinence
• Erectile dysfunction – Frequency
• Most common symptom of diabetic autonomic neuropathy • 30–75% of diabetic men
– Clinical syndromes • Ejaculatory failure: Sympathetic nervous system dysfunction • Erectile dysfunction with preserved ejaculation & orgasm
– Impaired nitric-oxide mediated relaxation of smooth muscle in corpus cavernosum
– Locations: Autonomic nerves; Endothelium – Course
• Initially partial • Progression to complete over 1 to 2 years • Usually irreversible
– Increased frequency with • Age • Duration of diabetes • Vascular disease
– Pathogenic factors • Autonomic neuropathy • Atherosclerotic involvement of the internal pudendal artery • Impaired endothelium-dependent relaxation of penile smooth muscle • Metabolic control impaired • Somatic sensory impairment
• Retrograde ejaculation: Uncommon; Occurs in diabetics with selective sympathetic failure • Females: Reduced vaginal lubrication
• Resting TachycardiaWhereas abnormalities in HRV are early findings of CAN, resting tachycardia and a fixed heart rate are characteristic late findings in diabetic patients with vagal impairment. Resting heart rates of 90 to 130 bpm occur. The highest resting heart rates have been found in patients with parasympathetic damage, occurring earlier in the course of CAN than sympathetic nerve function; in those with evidence for combined vagal and sympathetic involvement, the rate returns toward normal but remains elevated. A fixed heart rate that is unresponsive to moderate exercise, stress, or sleep indicates almost complete cardiac denervation. Thus, heart rate may not provide a reliable diagnostic criterion of CAN in the absence of other causes unless it is increased by more than 100 bpm.
• Exercise IntoleranceAutonomic dysfunction impairs exercise tolerance, reduces response in heart rate and blood pressure (BP), and blunts increases in cardiac output in response to exercise. Diabetic patients who are likely to have CAN should be tested for cardiac stress before undertaking an exercise program. Patients with CAN need to rely on their perceived exertion, not heart rate, to avoid hazardous levels of intensity of exercise. Presently, there is inadequate evidence to recommend routine screening of asymptomatic diabetic patients with an exercise ECG test.
• Intraoperative and Perioperative Cardiovascular InstabilityPerioperative cardiovascular morbidity and mortality are increased 2- to 3-fold in patients with diabetes. Compared with nondiabetic subjects, diabetic patients undergoing general anesthesia may experience a greater degree of decline in heart rate and BP during induction of anesthesia and less of an increase after tracheal intubation and extubation.
Vasopressor support is needed more often in diabetic individuals with CAN than in those without CAN. The normal autonomic response of vasoconstriction and tachycardia does not completely compensate for the vasodilating effects of anesthesia. There is an association between CAN and more severe intraoperative hypothermia that results in decreased drug metabolism and impaired wound healing. Reduced hypoxic-induced ventilatory drive requires preoperative CAN screening for loss of HRV. The anesthesiologist and surgeon should be alerted to this risk.
• Distal: Sensory ±autonomic Most common type of diabetic neuropathy – Clinical features
• Sensory loss: Usually pansensory – Occasionally with selective involvement of fiber types
» Small fiber: Pain: Often involved early » Large fiber: Paresthesias; Absent ankle reflexes
– Associated with foot ulcers in chronic DM » 7x increase » Middle-aged & elderly diabetic patients » Location: Soles of the feet » Frequent neuropathic osteoarthropathy
• Discomfort – Pain, Burning, Fatigue – Distribution
» Distal: Usual, Orofacial: Occasional; Burning mouth; Fatigue • Weakness
– Severity: Mild, – Distribution: Legs; Distal
• Charcots joints– Onset
» Age: 50 to 65 years » Course: Usually gradual, Ocasionally acute » Location: Navicular bone
– Locations: Foot 60%; Ankle 10% – Associations
» Poorly controlled insulin-dependent diabetes » Osteopenia (100%) » Calcification: Vascular smooth muscle cells (78% to 90%) » ? Regional increased blood flow (Hyperemia) » ? Related to disorders of OPG/RANK-L pathway
– X-rays: Bone & Joint destruction; Calcific deposits around joint
– Temporal risk of neuropathy after onset of DM • Symptomatic evidence
– 5 years: 4% to 10% – 25 years: 13% to 15% – Mean time after DM onset: 8 years – Increased Frequency: Women; Increased Age
• Objective evidence (Clinical or electrophysiologic): 65% to 80% of all diabetics
– Risk factors & associations • Clinical features
– General: Increased, Age, Body weight, Height. Disease duration – Diabetes
» Duration, Hemoglobin A1C, Triglycerides high: More progressive axon loss» Type 2 diabetes, Arterial stiffening & thickness,» Metformin treatment: Associated with low B12 & More severe neuropathy
– Systemic disorders » Hypertension (Diastolic), Retinopathy, metabolic syndrome, Smoking
– Albuminuria – Intensive insulin therapy reduces risk of developing neuropathy by 60%
• Aldose reductase 2 gene polymorphism – Dinucleotide repeat 2.1 kb upstream (5' end) of transcription start site
» Near osmoregulatory element for aldose reductase gene transcription – Z+2 allele: 14% risk of DM neuropathy after 20 years – Other alleles: 38% risk
• T-cell Receptor β chain – Associated with susceptibility to microvascular complications in IDDM
• Other possible pathogenic factors – Metabolic compromise – Ischemia – Oxidative stress – Neurotrophic support: Reduced
– Progression • Neuropathy may be asymptomatic for long periods • Longer latency: After onset of Type I, than Type II, diabetes • Slow over 5 to 20 years • Effects of glycemic control11
– Progression of neuropathy occurs despite good efforts at control
– Least progression: Aggressive blood sugar control – Control benefits other associated features: Triglyceride
and high-density lipoprotein cholesterol levels – Electrodiagnostic testing
• SNAP amplitudes: Reduced • Conduction velocities: Normal or Mildly reduced • Refractory periods: Shorter in diabetic nerves, ? related to
reduced nodal Na+ currents
• DIABETIC NEUROPATHIES: ASYMMETRIC
• General feature: Often have acute or stepwise onset
• Lumbosacral plexopathy – Nosology: Similar syndromes
• Proximal diabetic neuropathy • Diabetic amyotrophy • Multifocal diabetic neuropathy
– Epidemiology • Overall prevalence: 0.08% of diabetics • More frequent with type II (1.1%) than type I (0.3%) diabetes
– Clinical features • Weakness
– Asymmetric – Proximal weakness: Quadriceps; Thigh adductors; Psoas – Distal weakness: Ankles & Toes – Localized to lumbosacral plexus or lumbar roots
• Pain – Localized to: Hip, buttock, or thigh – May be severe – Usuallly lasts months after disease onset
• Sensory loss: Distal – Associated factors
• Poor diabetic control • Weight loss • Non-insulin dependent diabetes
– Differential diagnosis • Lumbosacral plexopathy • Cauda equina lesion
– Electrodiagnostic • EMG: Multifocal denervation in paraspinous & leg muscles • NCV: Axonal loss; Small CMAPS & SNAPs
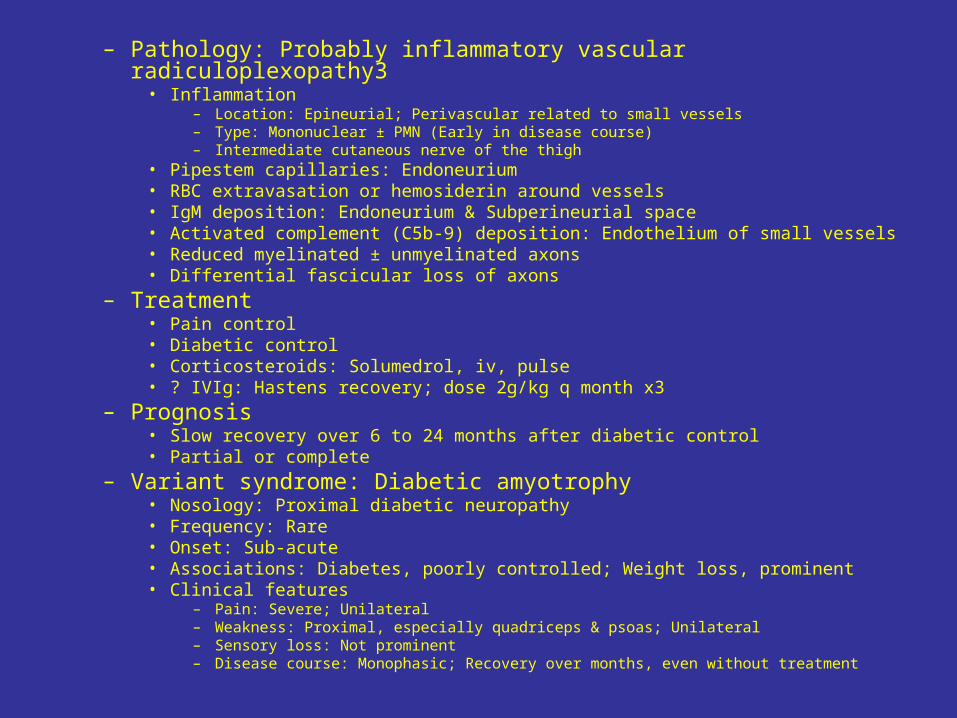
– Pathology: Probably inflammatory vascular radiculoplexopathy3 • Inflammation
– Location: Epineurial; Perivascular related to small vessels – Type: Mononuclear ± PMN (Early in disease course) – Intermediate cutaneous nerve of the thigh
• Pipestem capillaries: Endoneurium • RBC extravasation or hemosiderin around vessels • IgM deposition: Endoneurium & Subperineurial space • Activated complement (C5b-9) deposition: Endothelium of small vessels • Reduced myelinated ± unmyelinated axons • Differential fascicular loss of axons
– Treatment • Pain control • Diabetic control • Corticosteroids: Solumedrol, iv, pulse • ? IVIg: Hastens recovery; dose 2g/kg q month x3
– Prognosis • Slow recovery over 6 to 24 months after diabetic control • Partial or complete
– Variant syndrome: Diabetic amyotrophy • Nosology: Proximal diabetic neuropathy • Frequency: Rare • Onset: Sub-acute • Associations: Diabetes, poorly controlled; Weight loss, prominent • Clinical features
– Pain: Severe; Unilateral – Weakness: Proximal, especially quadriceps & psoas; Unilateral – Sensory loss: Not prominent – Disease course: Monophasic; Recovery over months, even without treatment
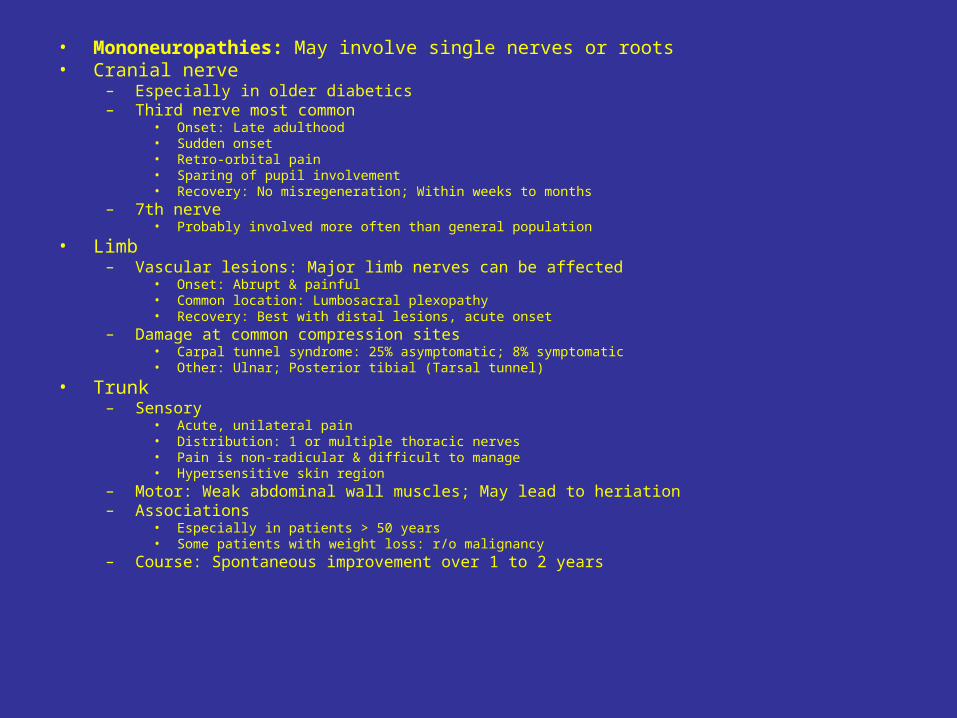
• Mononeuropathies: May involve single nerves or roots • Cranial nerve
– Especially in older diabetics – Third nerve most common
• Onset: Late adulthood • Sudden onset • Retro-orbital pain • Sparing of pupil involvement • Recovery: No misregeneration; Within weeks to months
– 7th nerve • Probably involved more often than general population
• Limb – Vascular lesions: Major limb nerves can be affected
• Onset: Abrupt & painful • Common location: Lumbosacral plexopathy • Recovery: Best with distal lesions, acute onset
– Damage at common compression sites • Carpal tunnel syndrome: 25% asymptomatic; 8% symptomatic • Other: Ulnar; Posterior tibial (Tarsal tunnel)
• Trunk – Sensory
• Acute, unilateral pain • Distribution: 1 or multiple thoracic nerves • Pain is non-radicular & difficult to manage • Hypersensitive skin region
– Motor: Weak abdominal wall muscles; May lead to heriation – Associations
• Especially in patients > 50 years • Some patients with weight loss: r/o malignancy
– Course: Spontaneous improvement over 1 to 2 years
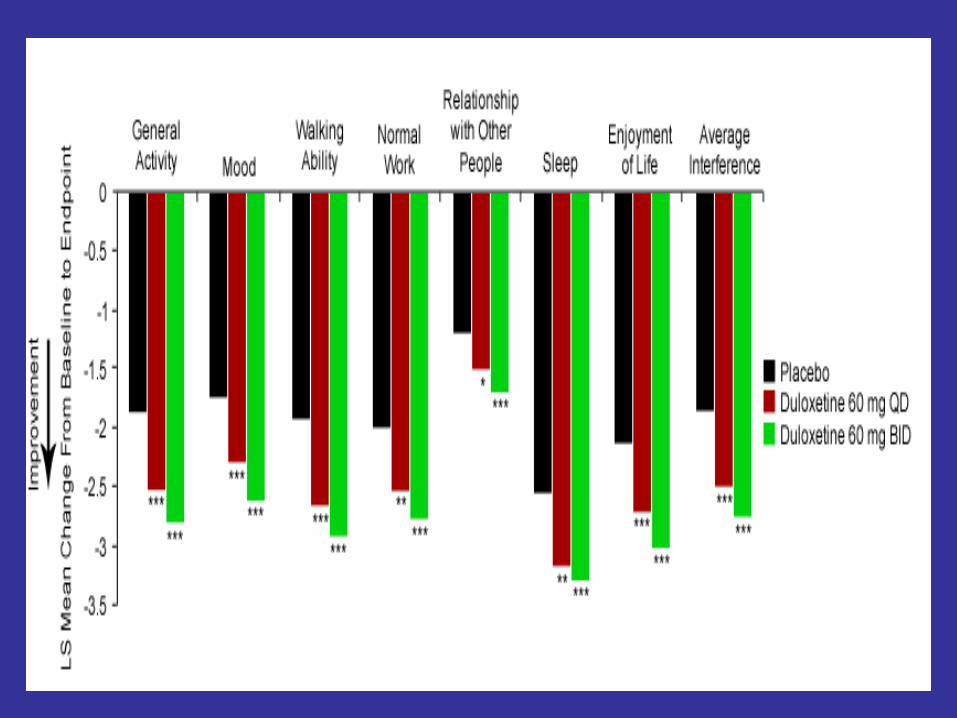
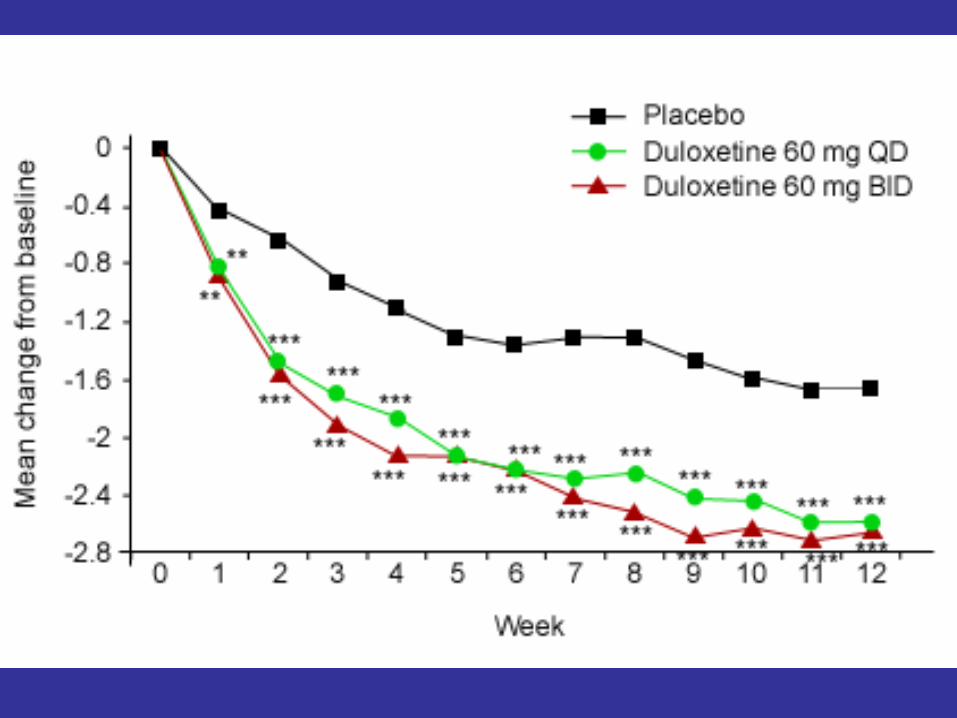
• Duloxetine for the management of diabetic peripheral neuropathic pain: Evaluation of functional outcomes.
• Adapted from Armstrong DG et al. Pain Med 2007;8:410-418
• ObjectiveTo assess the effectiveness of duloxetine, compared with placebo, on patient-reported health outcomes over a 12-week period, in the management of diabetic peripheral neuropathic pain (DPNP).
• Trial designPooled analysis of patient reported functional outcomes results from three randomised, double-blind, 12-week multicentre studies In study 1 (n = 457), patients with DPNP were randomly assigned to treatment with duloxetine 20 mg once daily (QD), 60 mg QD, 60 mg twice daily (BID), or placebo In study 2 (n = 334) and study 3 (n = 348), patients with DPNP were randomly assigned to treatment with duloxetine 60 mg QD, 60 mg BID, or placebo
• Key findings
Duloxetine was significantly superior to placebo: – in all the domains in the SF-36 health survey and the BPI interference – on all items in the analysis of the EQ-5D (60 mg QD; P = 0.004 and 60 mg
BID; P < 0.001)
Copyright ©2007 American Heart Association
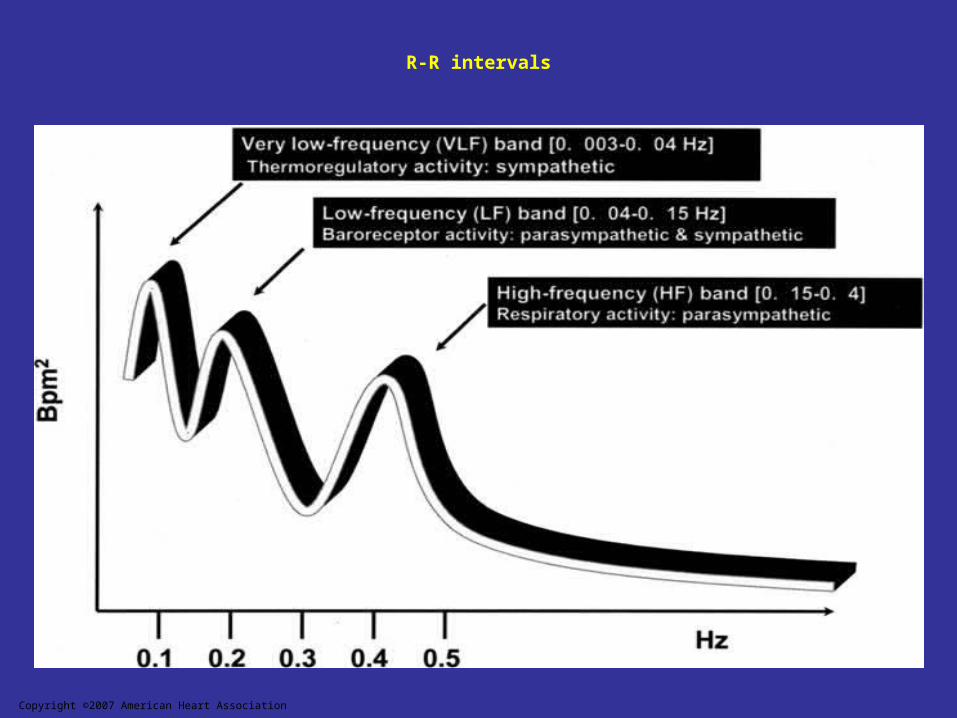
R-R intervals
Copyright ©2007 American Heart Association
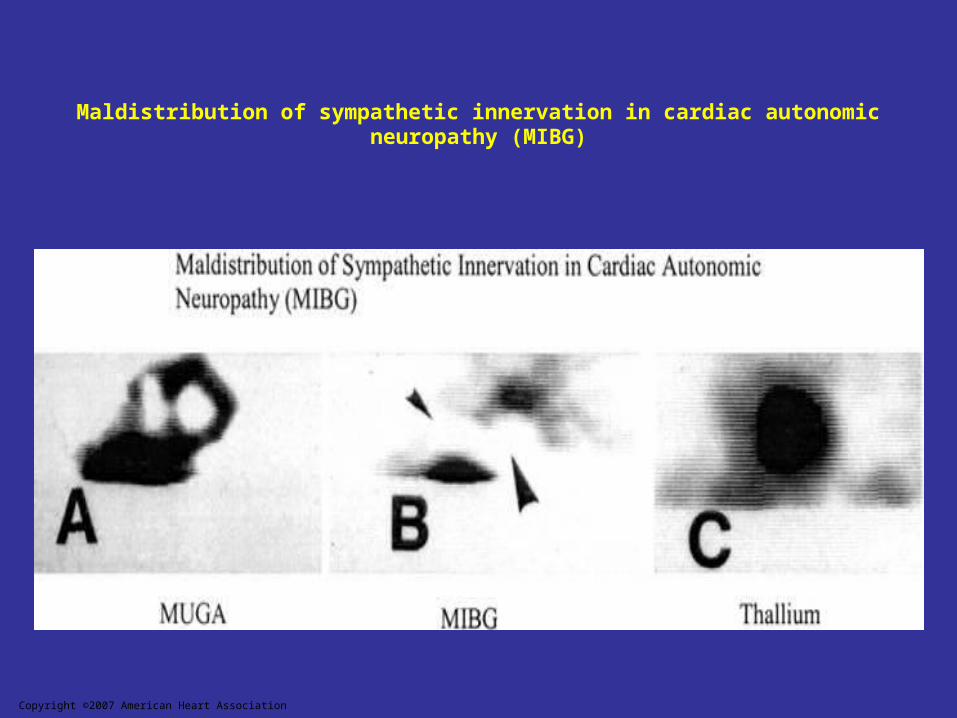
Maldistribution of sympathetic innervation in cardiac autonomic neuropathy (MIBG)
• Orthostatic Hypotension
Orthostatic hypotension is defined as a fall in BP (ie, >30 mm Hg systolic or >10 mm Hg diastolic BP) in response to a postural change from supine to standing.Symptoms include weakness, faintness, dizziness, visual impairment, and even syncope after a change from a lying to a standing posture. Orthostatic hypotension may become disabling, but the BP fall may also be asymptomatic.Orthostatic symptoms can be misjudged as hypoglycemia and can be aggravated by a number of drugs, including vasodilators, diuretics, phenothiazines, and particularly tricyclic antidepressants and insulin. A change from lying to standing normally results in activation of a baroreceptor-initiated, centrally mediated sympathetic reflex, resulting in an increase in peripheral vascular resistance and cardiac acceleration. In patients with diabetes, orthostatic hypotension is usually attributable to damage to the efferent sympathetic vasomotor fibers, particularly in the splanchnic vasculature. In addition, a decrease in total vascular resistance contributes to pathogenesis of this disorder. In individuals with orthostatic hypotension, there may be a reduced norepinephrine response relative to the fall in BP. Reduced cardiac acceleration and cardiac output may also be important, as well as low blood volume or reduced red cell mass. Other factors such as postprandial blood pooling, the hypotensive role of insulin, and treatment of kidney or heart failure with diuretics, leading to volume depletion, could aggravate orthostatic symptoms.
• Orthostatic Tachycardia and Bradycardia SyndromesSymptoms compatible with orthostasis, such as feeling faint or dizzy, circumoral paresthesia, and headache, may occur on changes from a supine to an erect position and may be caused by postural tachycardia syndrome (POTS), inappropriate sinus tachycardia, neurocardiogenic syncope, or abnormalities in baroreceptor function.
• The hallmark of these abnormalities is the absence of a fall in BP with standing, but a tachycardia or bradycardia with the change in posture.
• The pathogenesis of POTS is obscure. Some patients have defective peripheral vasoconstriction and an increase in calf blood flow, whereas others have increased peripheral arterial resistance and decreased blood flow.
• POTS is associated with a selective defect in intraepidermal nerve fiber in the skin. Norepinephrine concentrations have been significantly related to the estimate of the severity of autonomic neuropathy, and loss of peripheral sympathetic C fiber tone seems to translate to inadequate cardiac venous return with thoracic hypovolemia.
• POTS patients have paradoxically unchanged plasma renin activity and low aldosterone, given their marked reduction in plasma volume. These patients also have a significant reduction in plasma erythropoietin, suggesting that the kidney may play a role in the pathogenesis of this condition.
• POTS patients have exaggerated muscle sympathetic nerve activity with baroreceptor-reflex challenges. A cadre of POTS patients have shown normal peripheral resistance and blood volume in the supine position but thoracic hypovolemia and splanchnic pooling in the upright position. Selective and maintained orthostatic pooling in the splanchnic bed occurs in low-flow POTS despite marked peripheral vasoconstriction in these patients. Local splanchnic vasoregulatory factors may counteract the vasoconstriction in these patients.
• In addition to these syndromes, there are selected patients with orthostatic symptoms who have a paradoxical bradycardia on standing; the symptoms closely mimic those of hypotension. It is important to recognize these differences because each is amenable to simple intervention.
• Silent Myocardial Ischemia/Cardiac Denervation Syndrome
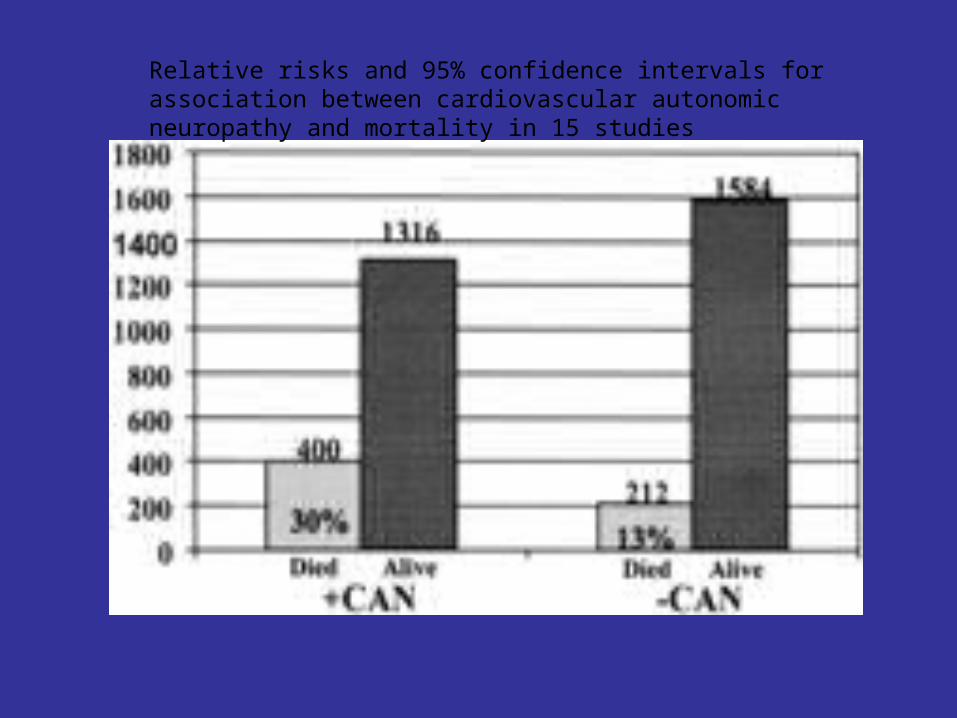
Relative risks and 95% confidence intervals for association between cardiovascular autonomic neuropathy and mortality in 15 studies
• Neuropathy Among the Diabetes Control and Complications Trial Cohort 8 Years After Trial Completion
OBJECTIVE—To evaluate the impact of prior intensive diabetes therapy on neuropathy among former Diabetes Control and Complications Trial (DCCT) participants.
• RESEARCH DESIGN AND METHODS—At the conclusion of the DCCT, subjects in the intensive group were encouraged to maintain intensive therapy, and subjects in the conventional group were encouraged to begin intensive therapy. Thereafter, we annually assessed neuropathy as part of the Epidemiology of Diabetes Intervention and Complications (EDIC) study. Neuropathy was defined using the Michigan Neuropathy Screening Instrument (MNSI). We recorded potential adverse consequences of neuropathy.
• RESULTS—At the first EDIC examination, 1,257 subjects participated in the neuropathy assessment. Consistent with DCCT results, the former intensive group showed a lower prevalence of neuropathy than the conventional group based on positive questionnaire (1.8 vs. 4.7%; P = 0.003) or examination (17.8 vs. 28.0%; P < 0.0001) results. Despite similar levels of glycemic control, symptoms and signs of neuropathy remained less prevalent among the former intensive group compared with the conventional group. At the beginning of the EDIC study, prior intensive therapy reduced the odds of having symptoms and signs of neuropathy using MNSI criteria by 64% (P = 0.0044) and 45% (P < 0.0001), respectively, with similar odds reductions observed for both neuropathic symptoms (51%, P < 0.0001) and neuropathic signs (43%, P < 0.0001) across 8 years of EDIC follow-up.
• CONCLUSIONS—The benefits of 6.5 years of intensive therapy on neuropathy status extended for at least 8 years beyond the end of the DCCT, similar to the findings described for diabetic retinopathy and nephropathy.
• Time to onset of neuropathic pain reduction: a retrospective analysis of data from nine controlled trials of pregabalin for painful diabetic peripheral neuropathy and postherpetic neuralgia. Sharma U
• Abstract• These retrospective analyses of daily mean pain scores from nine placebo-
controlled trials of pregabalin at 150, 300, or 600 mg/day (pregabalin, n = 1205; placebo, n = 772) examined time to significant reduction of pain during the first 2 weeks of treatment of painful diabetic peripheral neuropathy and postherpetic neuralgia. Time to onset of reduction in pain-defined as the first day for which patients treated with pregabalin had significant reductions (P < 0.05) in mean pain score compared with the placebo group for that day and the subsequent day-was calculated for all treatment groups demonstrating statistically significant reduction in pain at trial end point. The time to a 1-point or greater improvement in mean pain score was measured for each patient who was a responder at end point (30% or greater improvement in mean pain score).
• In seven of the nine trials (representing 11 of 14 pregabalin arms), significant reduction in pain was achieved at end point. The time to onset for reduction in pain was treatment Day 1 or 2 in nine of these successful treatment arms. Individual responder analysis confirmed that responders in the pregabalin groups reported a 1-point or greater pain reduction earlier than responders in placebo groups (P < 0.0001). However, this analysis is not a direct estimate of the likelihood that an individual patient would experience noticeable pain relief by the end of the second day.
• Overall, for patients who will respond to pregabalin, statistically significant and sustained reduction of pain associated with diabetic peripheral neuropathy and posttherapeutic neuralgia occurs early, usually by the end of 2 days of pregabalin treatment.
• Lamotrigine for treatment of pain associated with diabetic neuropathy: results of two randomized, double-blind, placebo-controlled studies.
• Vinik A et al• Diabetes Institute, Eastern Virginia Medical School, 855 West Bramdleton, Norfolk, VA
23510, USA.
• Abstract• To assess the efficacy and tolerability of lamotrigine in pain associated with diabetic
neuropathy, two replicate randomized, double-blind, placebo-controlled studies were conducted.
• Patients (n=360 per study) with painful diabetic neuropathy were randomized to receive lamotrigine 200, 300, or 400 mg daily or placebo during the 19-week treatment phase, including a 7-week dose-escalation phase and a 12-week, fixed-dose maintenance phase.
• The mean reduction in pain-intensity score from baseline to week 19 (primary endpoint) was greater (p < or = 0.05) in patients receiving lamotrigine 400 mg than placebo in Study 2 (observed scores, -2.7 versus -1.6 on a 0- to 10-point scale). This finding was not replicated in Study 1. Lamotrigine 200 and 300 mg did not significantly differ from placebo at week 19 in either study. Lamotrigine 300 and 400 mg were only occasionally more effective than placebo for secondary efficacy endpoints. The 200-mg dose did not separate from placebo. In a post hoc analysis of pooled data including only patients who reached their target dose, lamotrigine 400 mg conferred greater (p0.05) mean reduction in pain-intensity score from baseline to week 19 than placebo (-2.5 for 300 mg and -2.7 for 400mg versus -2.0 for placebo).
• Adverse events were reported in 71-82% of lamotrigine-treated patients compared with 63-70% of placebo-treated patients. The most common adverse events with lamotrigine were headache and rash.
• Compared with placebo, lamotrigine (300 and 400 mg daily) was inconsistently effective for pain associated with diabetic neuropathy but was generally safe and well tolerated.
• A double-blind, randomised multicentre trial comparing duloxetine with placebo in the management of diabetic peripheral neuropathic pain.
• Adapted from Raskin J et al. Pain Med 2005;6:346-356
• ObjectiveTo assess efficacy and safety of duloxetine, a selective serotonin and norepinephrine reuptake inhibitor, on the reduction of pain severity, in patients with diabetic peripheral neuropathic pain (DPNP)
• Trial design
Multicentre, parallel, double-blind, randomised, placebo-controlled trial that enrolled 348 patients with pain due to peripheral neuropathy caused by type 1 or type 2 diabetes mellitus Patients (n=116 per group) were randomly assigned to receive duloxetine 60 mg once daily (QD), duloxetine 60 mg twice daily (BID), or placebo, for 12 weeks Primary outcome measure was the weekly mean score of 24-hour average pain severity evaluated on an 11-point Likert scale Secondary outcome measures and safety were also evaluated
• Key findings
Duloxetine-treated groups improved significantly more (P<0.001) on the 24-hour average pain score than patients on placebo Duloxetine demonstrated superiority to placebo in all secondary analyses of the primary efficacy measure A significant treatment effect for duloxetine was observed in most secondary measures for pain Discontinuations due to adverse events were more frequent in the duloxetine 60 mg BID- (12.1%) versus the placebo- (2.6%) treated group Duloxetine showed no adverse effects on diabetic control, and both doses were well tolerated
• Extension study• An open-label 52-week clinical extension comparing duloxetine with routine care in patients with diabetic peripheral
neuropathic pain Adapted from Wernicke JF et al. Pain Med 2007;8:503-513
• ObjectivesTo assess the safety of duloxetine at a fixed-dose of 60 mg twice daily (BID) for up to 52 weeks, and to compare duloxetine with routine care in the management of patients with diabetic peripheral neuropathic pain (DPNP)
• Trial design
Patients who completed the 13 week acute therapy period were randomly reassigned in a 2:1 ratio to therapy with duloxetine 60 mg BID (n=197) or routine care (n=96) for an additional 52 weeks Safety of duloxetine was assessed by the occurrence of serious adverse events (SAEs), discontinuation, treatment-emergent adverse events (TEAEs), laboratory assessments, vital signs, electrocardiograms (ECGs), and electrophysiological assessments of peripheral nerves The impact of treatment on patient-reported health outcomes was measured by the 36-item Short Form Health Survey (SF-36) and the European Quality of Life Instrument-5D version (EQ-5D) self-report questionnaire
• Key findings
14 patients discontinued due to adverse events or death (11 [5.6%] duloxetine- and three [3.1%] routine care-treated patients) No significant therapy-group differences were observed for patients with ≥1 serious adverse event. In total, 110 (55.8%) duloxetine- and 47 (49%) routine care-treated patients had ≥1 treatment-emergent adverse event (TEAE) TEAE: 110 (55.8%) patients treated with duloxetine and 47 (49%) treated according to routine-care procedures had one or more TEAE. Asthenia was the only TEAE to show a significant therapy-group difference (11 [5.6%] duloxetine- versus 0 patients in routine care-treated group) Duloxetine did not appear to adversely affect lipid profiles, or nerve or eye function No significant therapy-group differences were observed in mean change in systolic blood pressure, weight, or electrocardiogram parameters Significant therapy-group differences were observed in favour of duloxetine in the SF-36 physical component summary score, and subscale scores of physical functioning, bodily pain, mental health, and vitality
• Conclusion
Results of this study support the use of duloxetine in the long-term management of DPNP