-
Diabetic Foot
-
Two main Complications of Hyperglycemia
-
Predisposing peripheral vascular diseaseAtherosclerosis
(medium-sized vessels below the knee)Compromised blood
supplyCoagulative necrosisDry gangreneInfectionWet
gangreneIschemiaUlcer
-
NeuropathyNeuropathyMotorSensoryAutonomic nociception
Proprioception,Unawarenessof foot positionReduced sweatingDry
skinFissures andcracksMuscle wastingFoot weaknessPostural
deviationDeformities, stressand shear pressuresTraumaStress on
bones & jointsPlantar pressure
Callus formation
InfectionUlcer
-
Activation of Protein Kinase CIntracellular
hyperglycaemiaStimulates de novo synthesis for diacylglycerol
(DAG)Activates PKC Downstream effects:Production of vascular
endothelial growth factor Increased vasoconstrictionincreased
deposition of extracellular matrix and basement membrane
materialProduction of plasminogen activator inhibitor Production of
proinflammatory cytokines
-
Disturbance in polyol pathwayHyperglycemiaincrease IC
glucose(eg: nerves, lens, kidney, blood vessels)metabolize by
aldose reductasesorbitol (polyol)Fructose
Accumulated sorbitol & fructoseIncrease IC osmolarityInflux
of waterOsmotic cell injury NADPH used up during polyol
pathwayDecreased GSH (Reduced glutathione)Cells susceptible to
oxidative stressOxidative cell injuryNerve Damage
-
Diffentiation of Ischaemic and Neuropathy Ulcer
-
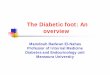
Claw toeSevere atrophy of the intrinsic foot muscles (lumbrical
& interossei)d/t motor neuropathy resulted in imbalance of foot
muscles & cocked-up toes.
-
Neuropathic foot ulcerCallus formation on its surrounding ulcer
lesion.
-
InfectionIndividuals with DM have a greater frequency and
severity of infection. Reasons: abnormalities in cell-mediated
immunity and phagocyte function diminished
vascularizationHyperglycaemia aids the colonization and growth of a
variety of organisms (Candida and other fungal species). Common
pathogens:
Combined with local ischemia, insensitivity to skin injury and
localized pressure d/t deformity, more susceptible to infection
-
Clinical presentation of diabetic foot
-
Ischemic foot ulcer
-
Foot ulcers
-
Charcot JointDiabetic neuropathy is the most common cause.
An acute Charcots foot will have swelling, erythema, raised skin
temperature, joint effusion and bone resorption in an insensate
foot
-
Charcot JointRocker bottom charcot foot
-
Gangrene Dry gangreneno infectionlittle tissue liquefactionIn
early stages, dull, aching pain, extremely painful to palpate,
cold, dry and wrinkled.In later stages, skin gradually changes in
color todark brown, thendark purplish-blue, thencompletely
black
Wet gangreneBacterial infectioncopious tissue
liquefactionoffensive odorswollen, red and warm.usually develops
rapidly due to blockage of venous and/or arterial blood
flowGangrene is a condition that involves the death and decay of
tissue, usually in the extremities due to loss of blood
supply.Treatment is surgical debridement and amputation.
-
****Firm evidence was set forth that proinflammatory cytokines,
especially the receptor activator of the nuclear factor-B (RANK)
ligand (RANKL) system is responsible for abnormally intense
osteoclastogenesis (4). Increased osteoclastic activity is
indicated for the excessive and unsupported bone turnover
Furthermore, the neurovascular theory relates to the increase in
peripheral blood flow that is responsible for the weakening and the
osteopenia found in the Charcot foot, causes bone resorption and
demineralization. This increased perfusion is due to the loss of
vascular sympathetic tone associated with the autonomic
neuropathy.
It is the result of a combination of motor, autonomic, and
sensory neuropathies in which there is muscle and joint laxity that
lead to changes in the arches of the foot. Further, the autonomic
denervation leads to bone demineralization via the impairment of
vascular smooth muscle, which leads to an increase in blood flow to
the bone with a consequential osteolysis. An illustration of some
commonly described abnormalities*A prospective study conducted in
Singapore with 202 diabetic patients revealed that 42.1% of the
patients had sensory neuropathy and 2% of them had Charcot
arthropathy (29). The incidences of Charcot foot in type 1 and type
2 diabetes do not differ, although osteopenia, as a predisposing
factor, appears to be more prevalent in type 1
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3733015/**