Embed Size (px)
Citation preview

Diabetes Mellitus
Chun-Jen Lin, MDTaipei Veterans General Hospital
- BS control and stroke

DM is associated with a substantially increased risk for first ischemic stroke
AHA guideline for primary stroke prevention, 2011
The adjusted RR is in the range of 1.5 to 3.7Abott et al., JAMA 1987, Odonnell et al., Lancet 2010, Almdal
et al., Arch Int Med 2004, Emerging et al., Lancet 2010

Get With The Guidelines-Stroke in Taiwan, Circulation 2010
Taiwan Stroke Registry

Diagnosis of DM
• HbA1c > 6.5%
• Fasting blood sugar > 126 mg/dl
• Postpradial blood sugar > 200 mg/dl during OGTT (75g)
• Random > 200 mg
ADA guideline 2014

Selvin et al., NEJM 2010
N=11092~15-yrs f/u

DM diagnosed
CAD
Stroke

DM control with stroke prevention

Steno-2 Study
Gade et al., NEJM 2003
patients with type 2 diabetes and microalbuminuria

N=63 N=67
Gade et al., NEJM 2003

Gade et al., NEJM 2003
Mean f/u: 7.8 yrs

Gade et al., NEJM 2003

Further f/u: 13.3 yrsSteno-2 Study

Review of clinical trials
Jay et al., Circulation 2009

Meta-analysis
Diab Vasc Dis Res 2010
No benefits in the intensive treated patients

Interpretations
• Not only BS, but also all vascular risk factors are important!
• The risk of hypoglycemia in intensive glycemic controls may outweigh the benefits
• Only those with short-duration of DM, young,
minimal CVD may have benefit from intensive glycemic control.
Jay et al., Circulation 2009, AHA guideline of stroke treatment 2014

Treatment Targets
• HbA1c < 7%
• Fasting blood sugar 70-130 mg/dl
• Peak postprandial blood sugar < 180 mg/dl
ADA guideline 2014

BS control in acute stroke

Christopher et al., Lancet Neurol 2007
UK Glucose Insulin in Stroke Trial (GIST-UK)


Glycemic control in acute stroke
Quinn et al., Cardiovas ther 2010
ESO: < 180 mg/dl
AHA: < 200 mg/dl
• Treatment target

Options for Antidiabetic Treatment
Glucose dependent
GLP-1 Mimetics (Exenatide, Liraglutide)
-Glucosidase Inhibitors
(Acarbose, Miglitol, Voglibose)
DPP-4 Inhibitors (Sitagliptin, Vildagliptin, Saxagliptin, Linagliptin, Alogliptin)
Glucose independent
Exogenous Insulin
GlinidesSulfonylurea
MetforminPioglitazone
Insulin ResistanceInhibition of
Glucose ResorptionInsulin Secretion

ADA guideline 2014


工商服務
健保價: 29.7元

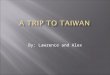
Significant lowering of urinary albumin/creatinine ratio by treatment with Pioglitazone in type 2 diabetic patients
-15
+2
-20
-10
0
10
Schernthaner et al JCEM 2004;
89:6086
Hanefeld et alDiab.Care 2004;
28:141
Matthews et al Diab.Metab Res.Rev.
2005; 21:167-174
-10
+6
p<0.027-19
-1
p<0.002p<0.017
SU +Metformin
(n=313)Pioglitazone
(n=597)Metformin
(n=597)
PIO +Metformin
(n=317)
Metformin +SU
(n=320)PIO +SU (n=319)
Chan
ge o
f urin
ary
albu
min
/cre
atini
ne ra
tio
after
52
wee
ks (%
)

Cardiovascular
Calcium Scoring
Carotid Intima Medial Thickness
CHICAGO TRIAL: A Study Evaluating Carotid Intimal- Medial Thickness in Atherosclerosis using Pioglitazone
Objective: Demonstrate the impact of Pioglitazone vs Glimepiride on atherosclerosis as measured by CIMT and EBCT in 400 patients with type 2 diabetes mellitus (18 month treatment period)
The Chicago Trial has been presented at the AHA 2006 in Chicago
Mazzone T et al. JAMA 2006; 296:2572–258 Davidson M et al. Circulation 2008 ;117:2123-2130

Study Diagram
CHICAGO TRIAL
Screening
Week –7 W0 W4 W8 W16 W24 W32 W40 W48 W60 W72
CIMT CIMT CIMT CIMT
Pioglitazone 15-45mg QD
Glimepiride 1-4mg QD

Week 24 Week 48 Week 72Baseline-0.010
LS M
ean
Cha
nge
from
Bas
elin
eP
oste
rior
Wal
l CIM
T (
mm
)
0.005
0.010
0.015
-0.005
0.000
Glimepiride Pioglitazone HCI
-0.013 (95% CI: -0.024, -0.002)Treatment group difference, Final Visit
LS mean (SE)Baseline CIMT (mm)
0.779 (0.008)GLM (N=186)
0.771 (0.008)PIO (N=175)
Mean Change in Average CIMT
CHICAGO TRIAL: A Study Evaluating Carotid Intima-Media Thickness in Atherosclerosis comparing Pioglitazone versus Glimepiride

Risk of MI, IHD or a composite of major Macrovascular Events from Meta-analyses of Trials with Rosiglitazone or Pioglitazone versus Comparators
Schernthaner G & Chilton R . Diab.Metab.Obes 2010
Rosiglitazone meta-analyses
Hazard or Odds or Risk Ratio3.50.0 0.5 1.0 1.5 2.0 2.5 3.0
GSK-ICT (MI) 7,8,20,21
Dahbreh & Econom opoulos (MI, lowest estimate) 19
Selvin et al. (CV morbidity) 22Friedrich et al. (MI)a 25
Friedrich et al. (IHD)a 25Schuster et al. (MI) 17FDA (Serious IHD) 9,21Nissen & Wolski (MI) 6Sing et al. (MI) 10
Bracken (MI, incl.RECORD) 18
Psaty & Furberg (MI) 16
Monami et al. (MI) 23
GSK-ICT (IHD) 7,8,20,21
Diamond et al. (MI, highest estimate) 15
Bracken (MI, excl.RECORD) 18
Dahbreh & Econom opoulos (MI, lowest estimate) 19
Diamond et al. (MI, lowest estimate) 15
FDA (IHD) 9,21
FDA (CV death/MI/Stroke) 7,8,20,21GSK-ICT (CV death/MI/Stroke) 7,8,20,21Manucci et al (Non-fatal coronary events) 24Manucci et al (Non-fatal MI) 24
Pioglitazone meta-analyses
Selvin et al (CV morbidity, incl.PROactive) 22
Manucci et al (Non-fatal coronary events) 33
Lincoff et al (Death/MI/stroke, excl.PROactive) 28
Selvin et al (CV morbidity, incl.PROactive) 22
Nagajothi et al (MI) 34Lincoff et al (Death/MI) 28
Lincoff et al (Death/MI/stroke, incl. PROacitve) 28Perez et al (Death/MI/stroke, incl.PROactive) 29
Lincoff et al (MI) 28
Perez et al (Death/MI/stroke, excl.PROactive) 29

Protection of multiple Organs by Actos (Pioglitazone)
47% of SecondaryStroke in Patients with previous Stroke (PROactive)
28% of Re-Infarction in Patients with previous MI (PROactive) 37% of Acute CoronarySyndrome after previous MI (PROactive)
21% of MI, Stroke & Death in Patients with CKD (PROactive)
Stop of Progression of Coronary Atherosclerosis (PERISCOPE)
Microalbuminuria (QUARTET) 51% Mortality in Patients on Hemodialysis (USA)
Reduction of CIMT (Carotid artery Intima- Media Thickness)(CHICAGO)
Reduction of Inflammation & Necrosis in NASH (Nonalcoholic Steatohepatitis)
50% Risk for Hepatocellular Ca
Scherthaner et al., Diab therap 2013

Who needs TZD ?


Take Home Massages
• HbA1c is a better marker than fasting sugar for
therapeutic monitoring.
• Intensive BS control alone does not provide additional
benefits in regard of stroke prevention.
• TZD is one of OADs that target at insulin resistance.
• Suitable for patients especially with increased waist
circumference, low HDL cholesterol level, and fatty
liver.
• Proved to be not associated with bladder cancer.













![arXiv:1504.02004v2 [hep-ex] 29 Sep 2015 - Hanyang...8Department of Physics, Fu Jen Catholic University, Taipei 24205 9Justus-Liebig-Universit at Gieˇen, 35392 Gieˇen 10Gifu University,](https://img.pdfslide.us/doc/110x75/601f79c446164878663e48a6/arxiv150402004v2-hep-ex-29-sep-2015-hanyang-8department-of-physics-fu.jpg)