Embed Size (px)
Citation preview
Diabetes mellitus and echocardiographic left ventricular function in free-living elderly men and women: The Cardiovascular Health Study
Marshall Lee, MD, a Julius M. Gardin, MD, b James C. Lynch, MS, c Vivienne-Elizabeth Smith, MD, d
Russell P. Tracy, PhD, e Peter J. Savage, MD, f Moyses Szklo, MD, g and Beverly J. Ward, MS c Davis and Irvine, Calif., Seattle, Wash., Albany, N.Y., Burlington, Vt:, and Bethesda and Baltimore, Md.
This report describes the relation among diabetes, blood pressure, and prevalent cardiovascular disease, and echocardiographically measured left ventricular mass and filling (transmitral valve flow) velocities in the Cardiovascu- lar Health Study, a cohort of 5201 men and women >-65 years of age. Ventricular septal and left posterior wall thicknesses were greater in diabetic than in nondiabetic subjects, show- ing a significant linear trend (p = 0.025 for ventricular septal thickness in both sexes combined, p = 0.002 for posterior wall thickness) with increased duration of diabetes. In- creased wall thickness of the ventricular septum or the left posterior wall was not associated with prevalent coronary heart disease (CHD) in the cohort. Increased left ventricular mass was associated with diabetic persons not reporting CHD and with all subjects with CHD regardless of glucose tolerance status. After adjusting for body weight, blood pressure, heart rate, and prevalent coronary or cerebrovas- cular disease, diabetes (as measured by glucose level, insulin use, oral hypoglycemic use, and a positive history of diabetes before baseline examination) remained an inde- pendent predictor of increased left ventricular mass among men and women (174.2 gm in diabetic men vs 169.8 gm in normal men, 138.2 gm in diabetic women vs 134.0 gm in normal women, p = 0.043 for both sexes combined). Both early and late diastolic transmitral peak flow velocities were higher with increased duration of diabetes, but the calcu- lated ratio of the early peak flow velocity to the late velocity (E/A ratio) did not differ significantly between subjects with historical diabetes and those with normal fasting glucose (both genders combined, p = 0.190). Glucose level, insulin use, oral hypoglycemic use, and a positive history of diabe-
From a the Department of General Medicine, University of California, Davis; bthe Division of Cardiology, Department of Medicine, University of California, Irvine; Cthe Department of Biostatistics, University of Wash- ington, Seattle; dthe Division of Cardiology, Albany Medical College; ethe Department of Pathology and Department of Biochemistry, School of Med- icine, University of Vermont, Burlington; fthe Division of Epidemiology and Clinical Applications, National Heart, Lung, and Blood Institute, Bethesda; and gtho School of Hygiene and Public Health, Johns Hopkins University, Baltimore.
Supported by contracts N01-HC85079 to HC-85086 from the National Heart, Lung, and Blood Institute.
Received for publication Feb. 12, 1996; accepted May 31, 1996.
Reprint requests: Marshall Lee, MD, General Medicine Investigative Clinic, 2000 Stockton Blvd., Ste. 100, Sacra~ento, CA 95817.
4/1/75867
tes before baseline examination were significant indepen- dent predictors of the late transmitral peak flow velocity and its integrated flow-velocity curve but not for the integral of the early peak flow velocity or the E/A ratio. Diabetes is as- sociated with abnormal left ventricular structure and func- tion in elderly persons. This association persists after adjustment for body weight, blood pressure, heart rate, and reported coronary or cerebrovascular disease. (Am Heart J 1997; 133:36-43.)
Heart disease is a major cause of illness and death among persons with diabetes. Accelerated coronary artery and peripheral atherosclerotic disease, are recognized as important outcomes related to dura- tion of diabetes and adequacy of blood sugar con- trol.1, 2 In addition to atherosclerosis, several studies suggest that diabetes modifies left ventricular (LV) myocardial structure and function at an early stage and that these subclinical abnormalities are unre- lated to atherosclerosis. 3, 4 Concomitant factors such as hypertension and obesity contribute significantly to both the atherosclerotic and the myocardial ab- normalities found with diabetes, but such abnormal- ities have also been detected in patients with normal blood pressure without symptomatic heart disease.
Echocardiography has been used previously to de- tect abnormalities of cardiac structure and function in persons with diabetes without clinical evidence of cardiovascular disease. The prevalence of LV hyper- trophy in the absence of hypertension was found to be increased among women who either had glucose intolerance or frank diabetes in the Framingham Study. 5 Impaired LV diastolic filling and reduced end-diastolic volume may accompany diabetes inde- pendent of ischemic cardiac disease, heart rate, or blood pressure. 6 Doppler echocardiography of flow velocity through the mitral valve during diastole has demonstrated reduced early and increased late LV filling in young diabetic persons without microangi-
36

Volume 133, Number 1
American Heart Journal Lee et al. 37
opathy o r coronary hea r t disease. 7 Such findings suggest ear ly reduct ion of LV filling in diabetes, which m a y be independen t of age or dura t ion of di- abetes, s Most of these invest igat ions were per formed in younger pa t ien ts wi th type I diabetes melli tus, however, and the contr ibut ion of diabetes to echocar- diographical ly evident cardiac dysfunct ion in older persons, and the predic t ive s t rength for clinical dis- ease of positive echocardiographic findings thought to be associated wi th the diabetic s ta te has not b e e n determined.
This repor t describes LV s t ruc ture and funct ion and associations with diabetes and impai red glucose tolerance in the Cardiovascular Hea l th S tudy (CHS) cohort, compris ing 5201 free-living e lde r ly subjects who u n d e r w e n t an extensive basel ine Clinical exam- ination, including echocardiography. The CHS is a mul t iyea r prospective invest igat ion of the correlates of cardiovascular and cerebrovascular morbidi ty and mor ta l i ty in m e n and women >-65 years of age living in the community .
METHODS
Ambulatory subjects were recruited in four United States communities: Forsyth County, N.C.; Sacramento County, Calif.; Allegheny County, Pa.; and Washington County, Md. The overall objectives and design of the CHS 9 and the rationale and design of the echocardiographic ex- amination protocol 1° have been presented in detail previ- ously. In brief, subjects were interviewed to obtain a thor- ough medical history, an inventory of physical activities, personal habits, dietary intake, and measures of cognitive function. In addition, anthropometric measurements, re- cumbent, sitting, and standing blood pressure, 12-lead electrocardiography, and carotid ultrasonography were performed. Reports of preexisting cardiovascular and cere- brovascular disease that were obtained by questionnaire at the baseline examination were confirmed by physician contact or by reviewing relevant hospital discharge sum- maries at the local centers.
All blood samples were drawn after an overnight fast. An oral glucose tolerance test (OGTT) was performed by veni- puncture for glucose and insulin levels two hours following the ingestion of a 75 gm glucose load. Aliquots of serum were prepared and frozen at -70 ° C, and were shipped to the Laboratory for Clinical Biochemistry Research at the University of Vermont, where all blood and serum studies were performed. Serum glucose was measured on a Kodak Ektachem 700 Analyzer (Ektachem Test Methodologies, Eastman Kodak, Rochester, N.Y.).
Fasting blood glucose samples were not drawn on 94 subjects who did not fast within a 9-hour period before venipuncture, and their data are not included in subse- quent analyses. Another 399 subjects did not undergo OGTT because of current oral hypoglycemic or insulin therapy for diabetes. Data on fasting giucose and 2-hour
glucose were missing in 34 and 194 eligible subjects, respectively.
Diabetes was diagnosed at the baseline examination if either of the following findings was present: fasting blood glucose (FBS) of ->140 mg/dl or 2-hour blood glucose of ->200 mg/dl (World Health Organization criteria). 11 In ad- dition, subjects taking insulin or oral hypoglycemic agents at the baseline examination or reporting having received a diagnosis of diabetes from a physician were classified as diabetic by history. Impaired glucose tolerance was defined by a FBS of <140 mg/dl and an OGTT with blood sugar measurements of 140 to 199 mg/dl. All subjects were clas- sifted in the following four' groups: diabetic by history (physician diagnosis or oral hypoglycemic or insulin ther- apy), diabetic (fasting blood or OGTT criteria), impaired glucose tolerance (OGTT criteria), and normal. Because no direct information was collected about the duration of di- abetes in the subjects, we ordered these subgroups in as- cending order of presumed severity of diabetes, as follows: normal FBS or negative history; impaired glucose toler- ance; diabetic FBS or OGTrp; and diabetic by history. We analyzed trends within the echocardiographic variables among these diabetic subgroups.
A detailed protocol of the echocardiographic examina- tion has been presented elsewhere. ~° In brief, 30 minutes was allotted during an extensive clinical visit to obtain M- mode, two-dimensional, spectral, and color Doppler stud- ies in each CHS subject with a Toshiba SSH-160A cardiac ultrasound machine (Toshiba America Medical Systems, Tustin, Calif.) and according to a standardized protocol. The studies were recorded on S-VHS videotapes, which were sent to the Echocardiography Reading Center at the University of California, Irvine. Images were digitized and measurements were made from these images using an off- line image analysis system equipped with customized computer algorithms. M-mode and two-dimensional echocardiographic images ef the LV were obtained for evaluation of ventricular septal and LV posterior wall thickness in diastole and systole, LV internal dimension in diastole and systole, left atrial, and aortic root dimension, LV volume in diastole and systole, and qualitative scores for LV ejection fraction and Segmental wall motion. LV mass, end-systolic stress, and percentage fractional short- ening were calculated according to formulas presented in Table I. Ventricular septal and left posterior wall thick- nesses and calculated left ventricular mass were adjusted for body weight in the data analysis. Pulsed Doppler mea- surements of early (E) and late (A) transmitral peak flow velocities (and flow velocity integrals) were made using the peak velocity convention (i.e, by tracing the outer edge of the spectral envelope). The ratio of the early diastolic to late diastolic velocity (E/A ratio) was calculated as an in- dex of the relative atrial contribution to LV filling. Three hundred forty-eight subjects with atrial fibrillation or with implanted cardiac pacemakers were excluded from the analysis of Doppler data.
Stage II hypertension was present at the baseline examination if the random-zero seated blood pressure (av- erag e of three readings) exceeded 159 mm Hg systolic or

January 1997 3 8 Lee et al. American Heart Journal
Table I. Formulas for echocardiographic variables calcu- lated from primary measurements made in M-mode and two-dimensional studies
Echocardiographic variable Formula
LV mass (gin) = 0.8(1.04[(VSTd + LVIDd + PWTd) 3 - (LVIDd)3]) + 0.6
LV end-systolic s t ress 0.334P × (LVID s)
PWT s x [1 + (PWTs/LVID~)]
LV fractional = LVID d - LVID~ shortening (%) x 100
LVIDa
LVIDd, LV internal dimension at end diastole; LVIDs, LV internal dimen- sion at end systole; P, systolic blood pressure (arm cuff); PWTd, LV peste- rior wall thickness at end diastole;PWTs, LV posterior wall thickness at end systole; VSTd, ventricular septal thickness at end diastole.
exceeded 94 mm Hg diastolic. Hypertension was also present if the subject reported a physician's diagnosis of hypertension and was taking antihypertensive medication (diuretic agents, p-blocking drugs, calcium-channel antag- onists, vasodilators, or angiotensin converting enzyme in- hibitors, alone or in combination). Stage 1 hypertension was present if the average of the three blood pressure readings was 140 to 159 mm Hg systolic or 90 to 94 mm Hg diastolic. 12
Statistics. Adjusted means of the diabetes subgroups were computed for each of the echocardiographic LV vari- ables. These means were adjusted for the following cova- riates: age (72 years), systolic blood pressure (135 mm Hg), diastolic blood pressure (70 mm Hg), weight (150 lb for women and 175 lb for men), heart rate (68 beats/min), ab- sence of definite coronary heart disease, and absence of definite or possible cerebrovascular disease, including transient ischemic attack and stroke. Using multivariate analysis of variance, tests for linear trends across diabetes subgroups, ordered from normal to impaired glucose toler- ance (from least diabetic severity or duration) to diabetic FBS to positive history of diabetes (highest diabetic sever- ity or duration), were performed to assess the role of dia- betes status as a predictor after adjustment for other covariates. Tests for interaction between gender and dia- betes status and for curvature beyond the linear fit were also performed, where curvature was investigated by us- ing the method of Cox and Wermuth. 13
As an alternative to treating diabetes as an ordered four-category variable, we considered four variables taken together as indicators of diabetes status: glucose level, in- sulin use, oral hypoglycemic medication use, and diabetes by history. These four variables were added simulta- neously to the multiple regression equations after first ad- justing for gender and the covariates described above. Partial F statistics were calculated to assess the indepen- dent contribution of the categorical diabetic state to the echocardiographic variables. The corresponding p values
were computed by comparing these partial F statistics to an F statistic with (4, n-k-l) degrees of freedom, where n is the sample size and k is the total number of variables in the new regression equation. All analyses were performed with the SAS and SPSS/PC+ statistical packages. 14,15
RESULTS
Fas t ing hyperglycemia (glucose >139 mg/dl) was found in 11.6% of m en and 7.9% of women. Combin- ing those wi th known diabetes and those whose glu- cose abnormal i t ies were newly discovered by CHS, 52.2% of all m en and 51.6% of all women had diabe- tes or impai red glucose tolerance. Only 546 (11.1%) subjects repor ted a previous diagnosis of diabetes on en t ry into the study. Near ly 50% of the diabetes and 80% of the abnormal glucose tolerance discovered dur ing the en t ry blood tes t in this group was previ- ously undiagnosed.
M-mode m easu rem en t s of left vent r icu la r mass could not be made in 34% of subjects with CHS. As previously reported, 16 the proport ion of subjects with missing da ta for LV mass increased wi th increasing age and was h igher among diabetic subjects (40% missing LV mass data) t h a n among nondiabet ic subjects (34% missing LV mass data). In the ent i re CHS cohort, calculated LV mass was strongly re la ted to age and was significantly h igher in men (mean 177.0 gm) t h a n in women ( m e a n 135.1 gin) (p < 0.0001). 16 Among the Doppler variables, in- creasing age and female sex were associated wi th grea te r late t r ansmi t r a l peak flow velocity (p < 0.0001 for a tes t of l inear t rend) and a corre- sponding decrease in the E/A ratio. There appeared to be no significant differences be tween white and nonwhi te persons in LV mass, or among the Doppler variables. However, the n u m b er of nonwhite people in the CHS initial examina t ion cohort was small (n = 249).
Table II presents m e a n M-mode echocardiographic values expressed as l inear t rends be tween diabetic subgroups a r ranged in order of increasing dura t ion or sever i ty of diabetes. The echocardiographic values have been adjusted for age, systolic and diastolic blood pressure , body weight, hea r t rate , and repor t of coronary h ea r t disease (CHD) or cerebrovascular disease at en t ry into the study. In our ordered anal- ysis, worsening glucose tolerance was weakly asso- ciated with increased LV mass (p = 0.043). Among the wall measu remen t s , there was an association be tween increasing sever i ty of glucose intolerance and vent r icu la r septal thickness (p = 0.025), and LV poster ior wall thickness in diastole (p = 0.002). No l inear t r end could be establ ished be tween severi ty of diabetes and LV in te rna l d imension in e i ther systole
Volume 133, Number 1
American Heart Journal Lee et al. 39
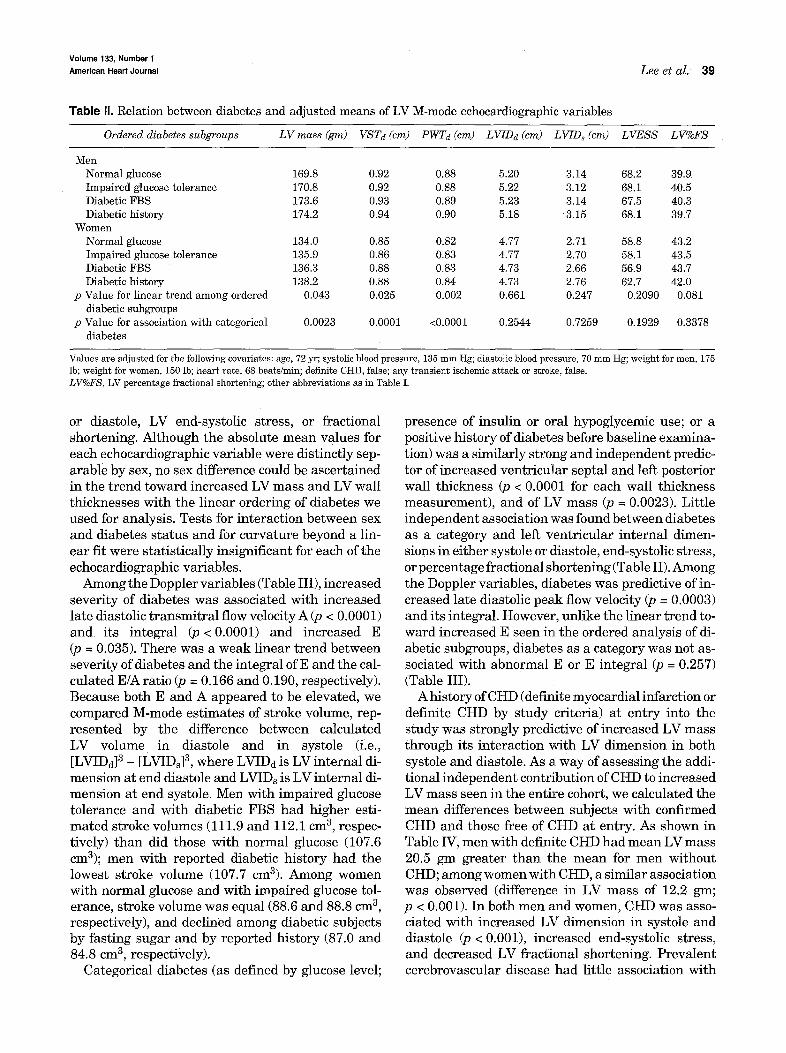
Table g. Relation between diabetes and adjusted means of LV M-mode echocardiographic variables
Ordered diabetes subgroups LV mass (gm) VST d (cm) PWTd (cm) LVIDd (cm) LVID s (cm) LVESS LV%FS
Men Normal glucose 169.8 0.92 0.88 5.20 3.14 68.2 39.9 Impaired glucose tolerance 170.8 0.92 0.88 5.22 3.12 68.1 40.5 Diabetic FBS 173.6 0.93 0.89 5.23 3.14 67.5 40.3 Diabetic history 174.2 0.94 0.90 5.18 3.15 68.1 39.7
Women Normal glucose 134.0 0.85 0.82 4.77 2.71 58.8 43.2 Impaired glucose tolerance 135.9 0.86 0.83 4.77 2.70 58.1 43.5 Diabetic FBS 136.3 0.88 0.83 4.73 2.66 56.9 43.7 Diabetic history 138.2 0.88 0.84 4.73 2.76 62.7 42.0
p Value for linear trend among ordered 0.043 0.025 0.002 0.661 0.247 0.2090 0.081 diabetic subgroups
p Value for association with categorical 0.0023 0.0001 <0.0001 0.2544 0.7259 0.1929 0.3378 diabetes
Values are adjusted for the following covariates: age, 72 yr; systolic blood pressure, 135 mm Hg; diastolic blood pressure, 70 mm Hg; weight for men, 175 lb; weight for women, 150 lb; heart rate, 68 beats/rain; definite CHD, false; any transient ischemic attack or stroke, false. LV%FS, LV percentage fractional shortening'; other abbreviations as in Table I.
or diastole, LV end-systolic stress, or fractional shortening. Although the absolute mean values for each echocardiographic variable were distinctly sep- arable by sex, no sex difference could be ascertained in the trend toward increased LV mass and LV wall thicknesses with the linear ordering of diabetes we used for analysis. Tests for interaction between sex and diabetes status and for curvature beyond a lin- ear fit were statistically insignificant for each of the echocardiographic variables.
Among the Doppler variables (Table III), increased severity of diabetes was associated with increased late diastolic transmitral flow velocity A (p < 0.0001) and its integral (p < 0.0001) and increased E (p = 0.035). There was a weak linear trend between severity of diabetes and the integral of E and the cal- culated E/A ratio (p = 0.166 and 0.190, respectively). Because both E and A appeared to be elevated, we compared M-mode estimates of stroke volume, rep- resented by the difference between calculated LV volume in diastole and in systole (Le., [LVIDd] 3 - [LVIDs] 3, where LVIDd is LV internal di- mension at end diastole and LVIDs is LV internal di- mension at end systole. Men with impaired glucose tolerance and with diabetic FBS had higher esti- mated stroke volumes (111.9 and 112.1 cm 3, respec- tively) than did those with nozznal glucose (107.6 cm3); men with reported diabetic history had the lowest stroke volume (107.7 cm3). Among women with normal glucose and with impaired glucose tol- erance, stroke volume was equal (88.6 and 88.8 cm 3, respectively), and declined among diabetic subjects by fasting sugar and by reported history (87.0 and 84.8 cm 3, respectively).
Categorical diabetes (as defined by glucose level;
presence of insulin or oral hypoglycemic use; or a positive history of diabetes before baseline examina- tion) was a similarly strong and independent predic- tor of increased ventricular septal and left posterior wall thickness (p < 0.0001 for each wall thickness measurement), and of LV mass (p = 0.0023). Little independent association was found between diabetes as a category and left ventricular internal dimen- sions in either systole or diastole, end-systolic stress, or percentage fractional shortening (Table II). Among the Doppler variables, diabetes was predictive of in- creased late diastolic peak flow velocity (p = 0.0003) and its integral. However, unlike the linear trend to- ward increased E seen in the ordered analysis of di- abetic subgroups, diabetes as a category was not as- sociated with abnormal E or E integral (p = 0.257) (Table III).
A history of CHD (definite myocardial infarction or definite CHD by study criteria) at entry into the study was strongly predictive of increased LV mass through its interaction with LV dimension in both systole and diastole. As a way of assessing the addi- tional independent contribution of CHD to increased LV mass seen in the entire cohort, we calculated the mean differences between subjects with confirmed CHD and those free of CHD at entry. As shown in Table IV, men with definite CHD had mean LV mass 20.5 gm greater than the mean for men without CHD; among women with CHD, a similar association was observed (difference in LV mass of 12.2 gm; p < 0.001). In both men and women, CHD was asso- ciated with increased LV dimension in systole and diastole (p < 0.001), increased end-systolic stress, and decreased LV fractional shortening. Prevalent cerebrovascular disease had little association with

January 1997
40 Lee et al. American Heart Journal
Table III. Relation between diabetes and adjusted means of Doppler LV filling echocardiographic variables
Ordered diabetic subgroups E A E/A ratio E integral A integral
Men Normal glucose 0.67 0.73 0.95 0.119 0.080 Impaired glucose tolerance 0.69 0.75 0.96 0.121 0.081 Diabetic FBS 0.68 0.79 0.90 0.116 0.086 Diabetic history 0.68 0.78 0.94 0.120 0.085
Women Normal glucose 0.73 0.81 0.95 0.123 0.087 Impaired glucose tolerance 0.74 0.84 0.93 0.125 0.090 Diabetic FBS 0.75 0.85 0.94 0.129 0.092 Diabetic history 0.76 0.88 0.91 0.129 0.095
p Value for linear trend in 0.035 0.0001 0.190 0.166 <0.0001 diabetic subgroups
p Value for association with 0.257 0.0003 0.7119 0.4i94 0.0055 categorical diabetes
Values are adjusted for the following covariates: age, 72 yr; systolic blood pressure, 135 mm Hg; diastolic blood pressure, 70 mm Hg; weight for men, 175 lb; weight for women, 150 lb; heart rate, 68 beats/rain; definite CHD, false; any transient ischemic attack or stroke, false.
Table IV. Effects of definite CHD or any cerebrovascu]ar disease on adjusted echocardiographic variables
LVmass VSTd PWTd LVIDd LVIDs LVESS LV%FS E E integral A A integral E/Aratio
Men Definite CHD 20.5* 0.01 0.01 0.30* 0.44* 18.2" -4.4* 0.04* 0.007* 0.00 0.002 0.08* Positive TIA or stroke 3.7 0.02 0.01 -0.03 0.06 5.0 -1.4 0.00 0.000 0.00 0.001 0.07
Women Definite CHD 12.2" 0.01 0.01 0.20* 0.24* 6.8* -2.1" 0.02 0.007 0.00 0.000 0.03 Positive TIA or stroke 1.8 0.03 0.03 -0.08 -0.08 -4.3 0.5 0.07* 0.011 0.06* 0.005 0.05
T/A, Transient ischemic attack; other abbreviations as in Tables I and III. *Incremental differences from the adjusted mean echocardiographic variable conferred by adding CHD or adding TIA or stroke to the analyzed variable (p < 0.001).
any of the echocardiographic variables, reaching significance only for E and A among women, with no effect on the E/A ratio. By contrast, in the diabetic subjects, A and septal and posterior wall thicknesses were all greater than in the nondiabetic subjects, after adjusting for CHD in both groups. Diabetes was not associated with LV internal dimensions at end-systole or at end-diastole, whereas subjects with CHD showed a strong association with both end-systolic and end-di- astolic LV internal dimensions. LV mass was strongly associated with CHD and with diabetes.
DISCUSSION
Abnormalities of cardiac structure and function have been reported in persons with type I and with type II diabetes. The CHS studied an elderly popu- lation in whom diabetes can be considered almost exclusively Type II, and in which the prevalence of diabetes is high and similar to that reported by the National Center for Health statistics among persons aged 65 to 74 years. 17 The associations between age and left ventricular mass and ventricular filling ob-
served by others is, 19 are generally confirmed by our study. We found a strong independent association of increased LV mass with categorical diabetes among both men and women in our study, in contrast with the Framingham Heart Study, 5 which found a significant association only among women. Other investigators have suggested the prominent association of duration of the diabetic state in the development of structural and functional cardiac abnormalities. 2° In our study, we could only estimate the duration of the diabetic state. We made the as- sumptions that impaired glucose tolerance was the condition least likely to be diagnosed as diabetes (other than normal blood glucose) and that subjects who had FBS in the diabetic range without a previ- ous diagnosis had recent rather than longstanding diabetes. After adjusting for age, systolic and dias- tolic blood pressure, body weight, heart rate, and CHD or cerebrovascular disease at entry, an inde- pendent trend for increased LV mass (although not achieving statistical significance) can be seen with the increasing gradient of the diabetic state as

Volume 133, Number 1
American Heart Journal Lee et al. 41
established by the classification scheme in our study. We recognize the uncertainty inherent in the as- sumptions we used in defining the severity or the duration of diabetes; an objective measure of dura- tion of the diabetic s tate such as tissue accumulation of advanced glycosylated end products 21 may be able to overcome this type of limitation.
A stronger association with increased LV mass is seen when all indicators of diabetes are taken as a group in multivariate analysis after adjustment for the other confounders listed. With the latter analy- sis, it appears that diabetes is associated with increased ventricular septal and left posterior wall thicknesses. Increased LV mass, which includes wall thickness and internal dimensions in its calculation, is also associated with diabetes. The inability to cal- culate LV mass from M-mode echocardiographic data was increased among older subjects and in men; in heavier and taller subjects; and in those with hy- pertension, CHD, and diabetes. 16 LV mass is known to be higher among men with CHD and hypertension. Our data similarly suggests higher LV mass among persons with diabetes, and it is possible that this report underestimates the true mean LV mass among dia-
bet ic persons as well as the entire CHS cohort. Although analysis of prevalent CHD in the CHS
cohort is not the main theme of this paper, it should be noted that definite myocardial infarction and other CHD by study criteria appear to be linked to increased LV internal dimension in both systole and diastole without being associated with wall thick- ness measurements in any significant way. In con- trast, wall thickness was increased among the diabetic subjects (classified categorically or by the spectrum of worsening glucose tolerance) who did not report CHD on entry into the study. In addition, decreased fractional shortening and increased LV end-systolic stress among subjects with CHD at en- try, taken in concert with the LV internal dimension data, suggest an echocardiographic profile consistent with impaired LV function among patients with CHD, 16 one that differs importantly from that seen among the diabetic subjects in our study. Among the diabetic subjects in our study, there was no associa- tion between diabetes and either LV fractional short- ening or LV end-systolic stress. Wall thickness ab- normalities among the diabetic elderly persons in our study are consistent with those found in investi- gations of insulin-requiring diabetic persons in whom increased septal and LV posterior wall echodensity w a s f o u n d . 22 Such findings may be an early indica- tor of intramyocardial collagen deposition resulting in increased wall thickness with increasing duration of the diabetic state.
We observed a linear trend of increasing E with increased severity of the diabetic state in ordered analysis. In contrast, other investigators found re- duced E (and reduced early diastolic LV filling inte- gral) in patients with type 1 and with type 2 diabe- tes with no clinical coronary manifestations 6, 20, 23 among subjects who were not elderly and were thus not comparable to our population. Plausible mecha- nisms that may account for increased early LV fill- ing velocity with worsening diabetes in elderly per- sons include higher cardiac output or higher resting left atrial pressure. In this study, we did not measure mitral deceleration time, a measurement that would have permitted a detailed investigation of early diastolic filling reflecting loading, wall compliance, and ventricular relaxation patterns that may have distinguished diabetic heart function from the nor- mal elderly heart. 24
The Doppler pattern of increased A noted with di- abetes appears similar to previous observations 6, 25 among diabetics. A combination of intrinsically im- paired LV relaxation, and increased peripheral vas- cular resistance, which increases afterload, may contribute to a prominent peak in A among elderly diabetic persons, as it may with persons with high blood pressure. In our analysis, the increased A we observed in diabetic subjects was independent of blood pressure, age, heart rate, and clinical CHD and suggests chronically elevated afterload within this population associated with diabetes.
As with the aging Framingham c o h o r t , 26 m e a n ra- tio of the early diastolic peak velocity to the late peak velocity (E/A) among our entire cohort of elderly subjects was less than 1 lm/sec. The E/A was not as- sociated with diabetes in our study; however, there was a trend toward reduced E/A in ordered analysis of the diabetic subgroups. Our findings contrast with significantly reduced E/A among young diabetic per- s o n s , 6 but are consistent with no important alter- ation in E/A in another study, which excluded sub- jects with hypertension or clinical coronary heart disease. 22 Among healthy elderly subjects, previous studies have found decreased E, increased A, and re- duction in the E/A ratio independent of LV mass or ventricular loadingS, 2s We found a significant in- crease in A among elderly diabetic subjects; the sim- ilarity of E/A when compared with nondiabetic sub- jects is accounted for by a higher mean value for E among diabetic subjects in the ordered analysis. E appears to increase with worsening diabetes; among men (but not women) in our study, total stroke vol- ume also appeared to increase. A filling velocity pat- tern analogous to this one was observed in another study, which reported an unusual reduction in E and

January 1997 42 Lee et al. American Heart Journal
increased A among insulin-requiring diabetic per- sons administered nitroglycerine. 29 The investiga- tors observed little difference in resting Doppler measures between unchallenged diabetic and non- diabetic subjects, and they hypothesized that the ni- trate conferred a large venous preload reducing effect only among diabetic subjects, reducing total stroke volume and increasing the E/A ratio. This se- lective reactivity among diabetic persons suggests abnormal diastolic LV function affecting early filling velocities in the same direction as those we obtained at rest in the elderly diabetic persons.
Another possible explanation for the lack of differ- ence between diabetic and nondiabetic persons with respect to E/A is that some proportion of our popula- tion may have subclinical CHD not reported to us or recognized in our classification process for CHD, 16 and thus we may not have been able to entirely ac- count for disease effects on LV structure and function in the current analysis. Clinically evident myocar- dial disease has been reported to be associated with decreases and increases in E ("pseudonormaliza- tion"), depending on hemodynamic variables such as left atrial and LV pressure in early diastole, preload, and rate of LV relaxation. 3°, 31 An important limita- tion of our study is that these effects were not assessed directly (e.g., by measurement of mitral de- celeration time), and opposing hemodynamic factors among the different groups within our cohort may have reduced the strength of the association with the Doppler velocity measurements.
Conclusions. The CHS is a prospective study mon- itoring disease occurrence and its outcomes in a large cohort of elderly persons. This article reports the first systematic survey of LV structure and function among free-living elderly diabetic persons. We found that among the free-living elderly persons, diabetes appears to be independently associated with abnor- mal LV wall thickness and diastolic filling abnor- malities. There is a strong suggestion that the asso- ciation appears to be duration or severity dependent. This ongoing study may be able to determine whether its aging diabetic cohort is more prone to congestive heart failure and other cardiovascular events inde- pendent of other nondiabetic cardiovascular risk factors and may identify important LV parameters acting as precursors to clinical cardiovascular dis- ease.
REFERENCES
1. Wilson PW, Cupples LA, Kannel WB. Is hyperglycemia associated with cardiovascular disease? The Framingham Study. Am Heart J 1991; 121(2 Pt 1):586-90.
2. Krolewski AS, Warram JH, Valsania P, Martin BC, Laffel LM, Chris-
tlieb AR. Evolving natural history of coronary artery disease in diabe- tes mellitus. Am J Med 1991;90:56S-61S.
3. Ahmed SS, Jal~ri GA, Narang RM, Regan TJ. Preclinical abnormality of left ventricular function in diabetes mellitus. Am Heart J 1975; 89:153-8.
4. Grossman E, Shemesh J, Shamiss A, Thaler M, Carroll J, Rosenthal T. Le~ ventricular mass in diabetes-hypertension. Arch Intern Med 1992;152:1001-4.
5. Galderisi M, Anderson KM, Wilson PWF, Levy D. Echocardiographic evidence for the existence of a distinct diabetic cardiomyopathy (The Framinghamm Study). Am J Cardiol 1991;68:85-9.
6. Paillole C, Dahan M, Paycha F, Cohen-Solal A, Passa P, Gourgon R. Prevalence and significance of left ventricular filling abnormalities de- termined by Doppler echocardiography in young Type I (insulin- dependent) diabetic patients. Am J Cardiol 1990;64:1010-6.
7. Bouchard A, Sanz N, Botvinick EH, Phillips N, Heilbron D, Byrd BF; et al. Noninvasive assessment of cardiomyopathy in normotensive di- abetic patients between 20 and 50 years old. Am J Med 1989;87:160-6.
8. Attali JR, Sachs RN, Valensi P, Palsky D, Tellier P, Vulpillat M, et al. Asymptematic diabetic cardiomyopathy: a noninvasive study. Diabetes Res Clin Pract 1988;4:183-90.
9. Fried L, Borhani N, Enright P for the CHS Collaborative Research Group. The Cardiovascular Health Study: design and rationale. Ann Epidemiol 1991;1:263-76.
10. Gardin JM, Wong ND, Bommer W, Klopfenstein HS, Smith V-E; Tabatznik B, et al. Echocardiographic design of a multicenter investi- gation of free-living elderly subjects: the Cardiovascular Health Study. J Am Sac Echocardiogr 1992;5:63-72.
11. WHO Expert Committee on Diabetes Mellitus. Second report of the WHO Expert Committee on Diabetes Mellitus. World Health Organi- zation Technical Report Series 1980;646:1-80.
12. Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure. Fifth report of the Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure (JNC V). Arch Intern Med 1993; 153:154-83.
13. Cox DR, Wermuth N. Tests oflinearity, multivariate normality and the adequacy of linear scores. Applied Statistics 1994;43:347-55.
14. SAS version 6.04. Cary (NC): SAS Institute, 1989. 15. SPSS/PC+ version 2.0. Chicago: SPSS, 1988. 16. Gardin JM, Siscovick D, Anton-Cutver H, Lynch JC, Smith VE,
Klopfenstein HS, et al. Sex, age and disease affect echocardiographic left ventricular mass and systolic function in the free-living elderly: The Cardiovascular Health Study. Circulation 1995;91(6):1739-48.
17. Harris ML, Hadden WC, Knowler WC, Bennett PH. Prevalence of di- abetes and impaired glucose tolerance and plasma glucose levels in U.S. population aged 20-74 years. Diabetes 1987;36:523-34.
18. Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. N Eng] J Med 1990;322:1561-6.
19. Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Left ven- tricular mass and incidence of coronary heart disease in an elderly co- hort: the Framingham Heart Study. Ann Intern Med 1989;110:101-7.
20. Robillon JF, Sadoul JL, Jullien D, Morand P, Freychet P. Abnormal- ities suggestive of cardiomyopathy in patients with type 2 diabetes of relatively short duration. Diabete et Metabolisme 1994;20:473-80.
21. Wautier JL, Wautier MP, Schmidt AM, Anderson GM, Hori O, Zouk- ourian C~ et al. Advanced glycation end products (AGEs) on the surface of diabetic erythrocytes bind to the vessel wall via a specific receptor inducing oxidant stress in the vasculature: a link between surface-as- sociated AGEs and diabetic complications. Proc Natl Acad Sci USA 1994;91:7742-6.
22. Di Bello V, Talarico L, Picano E, Di Muro C, Landini L, Paterni M, et al. Increased echodensity of myocardial wall in the diabetic heart: an ultrasound tissue characterization study. J Am Coll Cardiol 1995; 25:1408-15.
23; Vanninen E, Mustonen J, Vaiulo P, Lansimies E, Uusitupa M. Left ventricular function and dimensions in newly diagnosed non-insulin- dependent diabetes mellitus. Am J Cardiol 1992;70:371-8.
24. Cacciapuoti F, D'Avino M, Lama D, Bianchi U, Perrone N, Varricchio M. Progressive impairment of left ventricular diastolic filling with ad- vancing age: a Doppler echocardiographic study. J Am Geriatr Soc 1992;40:245-50.

Volume 133, Number 1
American Heart Journal Lee et al. 43
25. Appleton CP, Hatle LK, Popp RL. Relation oftransmitral flow velocity flow patterns to left ventricular diastolic function: new insights from a combination hemodynamic and Doppler echocardiographic study. J Am 29. Coll CardioI 1988;12:426-40.
26. Sagie A, Benjamin EJ, Galderisi M, Larson MG, Evans JC, Fuller DL, et al. Reference values for Doppler indexes of left ventricular diastolic filling in the elderly. J Am Soc Echocardiogr 1993;6:570-6. 30.
27. Gardin JM, Rohan MK, Davidson D, Dabestani A, Sklansky MI, Gar- cia R, et al. Doppler transmitraI flow velocity parameters: relationship between age, body surface area, blood pressure and gender in normal subjects. Am J Noninvasive Cardiol 1987;1:3-10. 31.
28. Kitzman DW, Sheikh KH, Beere PA, Phillips JL, Higginbotham MB. Age-related alterations of Doppler left ventricular filling indexes in normal subjects are independent of left ventricular mass, heart rate,
contractility and loading conditions. J Am Coll Cardiol 1991;18:1243- 50. Gotzsche O, Sihm I, Lund S, Schmitz O. Abnormal changes in trans- mitral flow after acute exposure to nitroglycerin and nifedipine in un- complicated insulin-dependent diabetes mellitus: a Doppler echocar- diographic study. Am Heart J 1993;126:1417-26. Nishimura RA, Abel MD, HaLle LK, Tajik AJ. Assessment of diastolic function of the heart: background and current applications of Doppler echocardiography--part I. physiologic and pathophysiologic features. Mayo Clin Proc 1989;64:71-81. Nishimura RA, Abel MD, Ha¢le LK, Tajik AJ. Assessment of diastolic function of the heart: backgreund and current applications of Doppler echocardiography--Part II. clinical studies. Mayo Clin Proc 1989; 64:181-204.
BOUND VOLUMES AVAILABLE TO SUBSCRIBERS
Bound volumes of the AMERICAN HEART JOURNAL are available only to subscribers for the 1997 issues from the Publisher at a cost of $92.50 for domestic, $120.38 for Canadian, and $112.50 for international subscribers for Vol. 133 (Janua1~r-June) and Vol. 134 (July-December). Shipping charges are included. Each bound volume contains a subject and author index, and all advertising is removed. Copies are shipped within 60 days after publication of the last issue in the volume. The binding is durable buckram with the journal name, volume number, and year stamped in gold on the spine. Payment must accompany all orders. Contact Mosby-Year Book, Inc., Subscription Ser- vices, 11830 Westline Industrial Dr., St. Louis, MO 63146, USA; phone (800)453-4351 or (314)453- 4351.
Subscr ipt ions must be in force to qualify. B o u n d vo lumes are not avai lable in place of a regular Journa l subscript ion.









![Hypertension Associated with Atherosclerosis Risk Factors ... · diabetes mellitus, left ventricular hypertrophy, psychosocial factorsbesides sy, s- tolic arterial hypertension [7]](https://img.pdfslide.us/doc/110x75/5d4edcdd88c99342288b9569/hypertension-associated-with-atherosclerosis-risk-factors-diabetes-mellitus.jpg)

















