Embed Size (px)
Citation preview

Diabetes
Julia von Oettingen, MD

HistoryInsulin Regimen: □ Twice a day 70/30 Insulin (Mixtard)
□ AM breakfast dose_________IU □ PM dinner dose________IU□ Total Daily Dose per kg = ______(total Units per day) ÷ ______ (weight in kg) = ______U/kg/day
Review of blood sugars:•blood sugar check in clinic today : ________________mg/dL•If patient keeps log at home, average blood sugar wasAM □ not checked Lunch □ not checked PM □ not checked
□ <100 □ <100 □ <100□ 100-150 □ 100-150 □ 100-150□ 151-200 □ 151-200 □ 151-200□ 200-300 □ 201-300 □ 201-300□ >300 □ >300 □ >300
•Any recorded overnight (2AM) blood sugars:________________mg/dL•Highest sugar recorded:___mg/dLLowest sugar recorded:_____ mg/dL• Number of times EXTRA dose was given: ______________
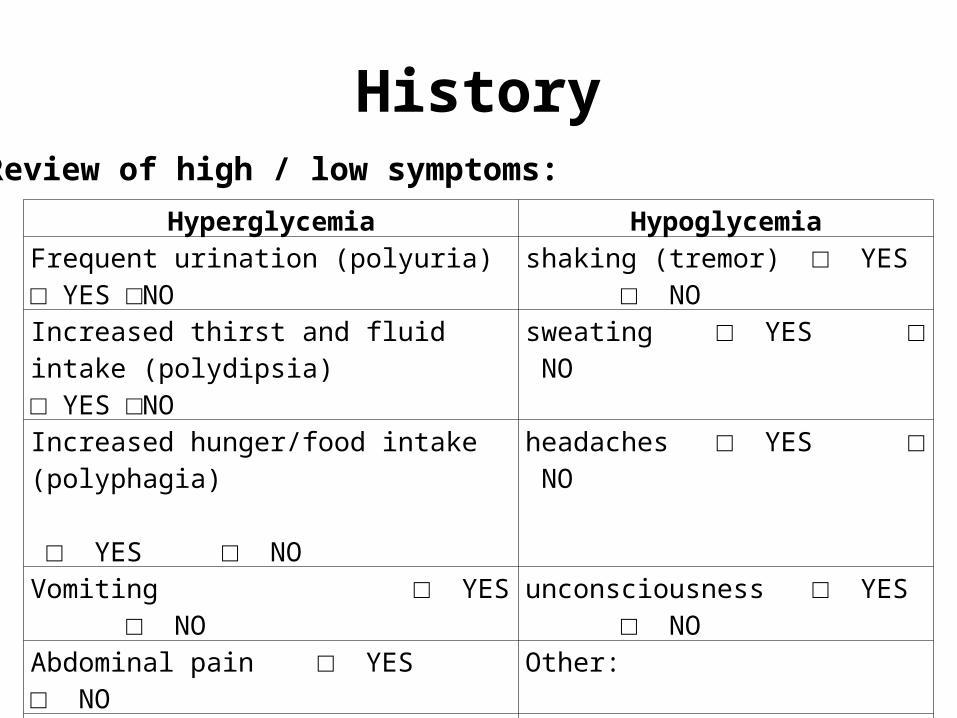
HistoryReview of high / low symptoms:
Hyperglycemia HypoglycemiaFrequent urination (polyuria) □ YES □NO shaking (tremor) □ YES □ NO
Increased thirst and fluid intake (polydipsia)□ YES □NO
sweating □ YES □ NO
Increased hunger/food intake (polyphagia) □ YES □ NO
headaches □ YES □ NO
Vomiting □ YES □ NO unconsciousness □ YES □ NO
Abdominal pain □ YES □ NO Other:
Other:Frequency: □ daily □ weekly □ monthly
Frequency: □ daily □ weeky □ monthly

History
Other History:• Retinopathy: □ vision changes □ trouble seeing• Hypothyroidism: □ low energy □ wt gain □ constipation □ dry skin • Psychosocial: □ coping strategies □ feelings of depression• 10y after diagnosis: □ pain or hyperaesthesia in hand/feet □ regular foot check (every night) □ bloating / abdominal pain / vomiting (gastroparesis)
Patient’s problems:Ask about problems with costs, access to medication or diabetes supplies, access to clinic, inability to contact medical provider by phone, lack of caregiver to administer insulin.Describe:_____________________________________________________
Review of Diet:Number of meals per day: □ 1 □ 2 □ 3 □ >3 □ food insecurity (irregular)Types of foods eaten: □ rice □ fish □ meat □ vegetables □ fruit □ other____Intake of high sugar drinks / foods: □ never □ daily □ weekly □ monthly

Physical Exam check box or circle if 2 choices givenHR_____ BP___/___ RR_____ Temp______ Wt________kg
Gen: □ well appearing □ weak or dehydrated □ altered mental statusHEENT: □ moist MM □ acetone odor □ thyroid exam_____________Heart: □ S1 and S2 □ RRR □ no murmur □ other___________Lungs: □ clear □ tachypnea □ Kussmaul resp □ other___________Abd: □ soft □ ND □ NT □ BS positive □ other___________________GU: □ normal external MALE / FEMALE genitalia □ pubertal / not pubertalNeuro: □ awake and alert □ altered mental status □ GCS_____ □ DTRs____Skin: □ cap refill ____sec □ dry □ pallor □ rashExtr: □ sensation to light touch tested: intact / not intact, describe________________
□ vibration sense tested: intact / not intact, describe_______________________□ foot inspected for ulcers: present / absent, describe______________________
Other:□ Injection sites: infection – present / absent; lipohypertrophy - present / absent, location__________________________________□ Joint exam: limited mobility – present / absent□ hypothyroidism: goiter – present / absent; brittle hair – present / absent; dry skin – present / absent

Education:□ insulin regimen reviewed □ blood sugar testing reviewed□ proper insulin administration reviewed (drawing up insulin, subQ route, changing sites)□ symptoms of hypo- and hyperglycemia reviewed□ plan for hypoglycemia reviewed: 1. give sugar ASAP (sugar water, juice, syrup, hard candy) 2. check BS after 20min 3. eat light meal after 30min 4. CALL YOUR DOCTOR□ plan for hyperglycemia reviewed: 1. check your sugar 2. if >300, drink a lot of water (1L/h for big children, 0.5L/h for small children) to avoid
DKA, and check BS before every meal 3. if >400 or read “hi” on glucometer, continue to drink a lot of water and give 10% of
total daily insulin =_________ and advise to CALL DOCTOR 4. if you are feeling unwell CALL YOUR DOCTOR or COME TO THE EMERGENCY ROOM□ short- and long term complications of type 1 diabetes reviewed 1.both hypo- and hyperglycemia can lead to coma and death 2. poor BS control leads to problems with the eyes (risk of blindness), kidney (risk of kidney failure and death), nerves (painfull hands and feet, foot ulcers) and heart (early death)□ diet and avoidance of high sugar foods/drinks□ patient questions answered

Assessment:□ good control (BS levels 100-170, patient compliant)□ acceptable control (BS levels 150-250, patient compliant)□ fair control (BS levels 250-300, partial compliance)□ poor control (BS levels >300, poor compliance consider admission)□ DKA (BS levels >>300, non-compliant needs admission)
Plan:•Insulin dose: □ no change □ following changes:______________________
□ new TDD = ____U/day ÷ ___ wt in kg = ____U/kg/day □ new EXTRA dose = _____Units
•Yearly checks: □ eyes□ clinical suspicion of thyroid disease low / unsure /high □ check TSH□ urine for microalbuminuria or protein (as a marker of kidney disease)
•Medication refill:□ cooler/refrigerator or other method of storing (specify: _________)□ Insulin vial□ Insulin syringes□ Lancets □ Needles□ glucometer □ glucometer strips□ book for logging BS
•Referrals: □ ophthalmology □ dietician □ social work □ other: _______________

Insulin start doses
• Estimate Total daily dose (TDD) of insulin:– <3y: 0.3U/kg/day– 3-12 y: 0.5-0.8 U/kg/day (always err on the lower side first, go
up later as needed)– 12-16y: 0.8-1 U/kg/d– >16y: 0.8 U/kg/d
• Using 70/30 insulin (70% NPH and 30% Regular) give:– AM dose: 2/3 TDD before breakfast– PM dose: 1/3 TDD before supper

Insulin start doses
Example:• 10 year old boy with first manifestation of
type 1 diabetes who weighs 30kg• TDD= 0.5 U/kg/day=0.5x30= 15U per day• AM dose= 2/3 x 15U= 10U• PM dose= 1/3 x 15U= 5U

Goal blood sugars
• Generally: the younger the child, the higher• If child has food security and can measure
RBS:– 150-200 in young children– 100-200 in older children
• If child has no food security, no RBS:– 150-250 in all children

General Principles before making adjustments:
• Check for external factors of different demand:– Has the insulin consistently been properly stored? – Has a new vial recently been opened? – Is the patient repeatedly using the same injection sites?
Look for signs of lipohypertrophy! – Is the patient using the right type of insulin and the right
dosages?– Has there been a change in the caregiver who provides the
insulin (and may not know the right doses)?
In all these cases DO NOT change dose but readjust external factor and follow up with patient whether glycemia improves

General Principles before making adjustments:
• Check for causes of different demand:– Is the patient entering his/her “honeymoon”phase– Has the patient been ill?– Has the patient made a change to their diet?
(quantity, types of foods, frequency of meals)– Have they made changes in their level of exercise?
• More exercise less insulin required lower sugars• Less exercise more insulin required higher sugars

Adjusting the dose:• Find a pattern of high/low sugar levels
– Sugars high or low in the MORNING adjust PM dose– Sugars are high or low in the EVENING adjust the AM dose
• Adjust one dose (AM or PM) at one time, unless ALL sugars are >300 or persistent symptoms of hyperglycemia
• Do not adjust the insulin dose by more than 10%• Wait 2-3 days before making a new change to a change
that was just made– UNLESS the patient is having hypoglycemia after a dose increase
change back to lower dose• Upon changing a dose:
– Have patient measure sugars for a minimum of 2 days (in AM and PM)
– call or return to clinic to see if a readjustment is needed

Adjusting the dose
• Example: • 10year old 30kg boy in the above example
who takes 10U in AM and 5U in PM. • All his sugars are HIGH (>250) in the morning…
you would increase the PM dose by 10% of 5U = 0.5U and thus increase his PM dose to 5.5U

No blood sugars?In patients who are not checking blood sugars:• Base your adjustment on clinical symptoms and a
blood sugar check, urine glucose and urine ketones in the clinic increase AM and/or PM dose by 10% if all of these are indicative of hyperglycemia
• If the patient has persistent polyuria, polydipsia, polyphagia, you should increase the AM and/or PM dose by 10%
• Have the patient check in with you frequently (if necessary every 2 days) after any change to see if they are improving
• Provide teaching about hypo/hyperglycemia symptoms
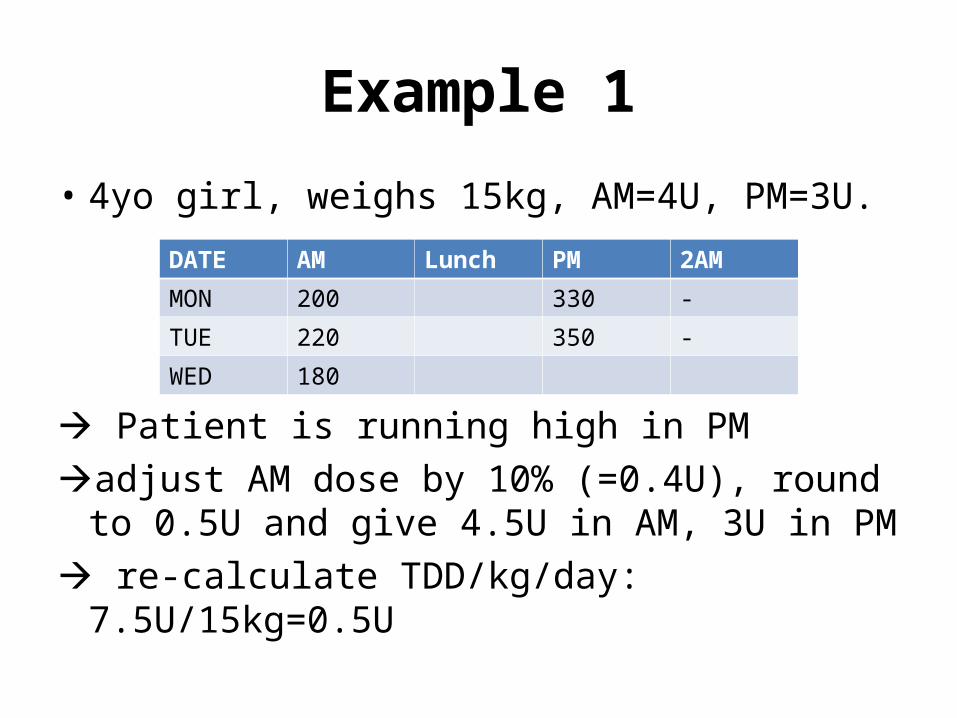
Example 1
• 4yo girl, weighs 15kg, AM=4U, PM=3U.
Patient is running high in PMadjust AM dose by 10% (=0.4U), round to
0.5U and give 4.5U in AM, 3U in PM re-calculate TDD/kg/day: 7.5U/15kg=0.5U
DATE AM Lunch PM 2AM
MON 200 330 -
TUE 220 350 -
WED 180

Example 2• 13yo boy, wt 40kg, AM dose=14U, PM dose=10U
Overall running high, but few values! adjust AM dose by 10% (=1.4U) can round to 2U
and give 16U in AM TDD = 26U/40kg = 0.65U/kg/dayFollow up in 2days , give your phone number for
earlier problems
DATE AM Lunch PM 2AM
MON -- 350 --
TUE 380 400 --
WED --

Example 3• 6yo girl, wt 20kg, AM dose=8U, PM dose=4U
Ask about symptoms!!Check RBS, urine glucose and urine ketones!!Educate about need to check sugars 2d before
coming to clinicAdjust only if patient persistently hyperglycemic
and above tests are suggestive of hyperglycemiaTDD = 12U/20kg = 0.6U/kg/day
DATE AM Lunch PM 2AM
MON -- -- --
TUE -- -- --
WED --