Embed Size (px)
Citation preview
Diabetes Footcare Primary care pathway
Dr Mike Merriman
06/03/15
Introduction
• Background • Why do we need and new pathway? • What do we want to achieve? • How are we doing?: Amputations • Evidence to reduce amputations primary care • How are we doing ?: Screening • Pathway overview • Quality assurance
The scale of the challenge?
Background
• People with diabetes are more likely to have foot problems due to
neuropathy and peripheral vascular disease. • 10% of people with diabetes will have an ulcer at some point in their
lives. • Diabetes is the most common cause of none traumatic limb
amputation. • 80% of amputations are preceded by ulceration.
Background
• After a first amputation people with diabetes are twice as likely to
have a further amputation. (1) • 70 % of people with amputation due to ulceration die within five
years. (1) • Nationally estimated that £639-£662 million was spend on diabetes
related foot care and amputations for 2010-2011 (2) • Approximately £293-£338 million spent on inpatient ulceration,
amputation and post-amputation care (2)
Why do we need a pathway?
• There are variations across our network of amputation rates. (nationally fourfold) (1)
• There are variations in screening rates. • Foot care in diabetes is high on the health agenda e.g. part of CQC
assessments for practices and new NICE guidance imminent. • There is avoidable mortality and morbidity related to diabetic foot
disease.
What do we want to achieve?
• All patients with diabetes have access to regular high quality foot screening which includes risk stratification.
• Foot screening is delivered by an appropriately trained workforce with quality assurance built into the process.
• Foot problems are identified early resulting in rapid assessment and treatment when required.
• Patients are provided with high quality supporting education. • Active foot disease is rapidly identified and referred for urgent
medical/surgical input.
What do we want to achieve?
• Patients requiring access to specialist support from a podiatry foot protection team have rapid access to these services.
• Patients requiring access to a specialist multi-disciplinary foot care team have rapid access to these services.
• All members of the primary and secondary care foot service, commissioners and patients are clear on the expected minimum timescales and pathway for referral and treatment.
• A focus is placed on management of diabetes to reduce the risk of foot and other diabetes related complications.

• Amputations How are we doing?


• From April 10 to March 13 in Cheshire and Merseyside (3):
• Total nights in hospital due to diabetic foot disease 66,309
• Episodes of care where an amputation is performed on those with
diabetes 993 • For non traumatic major amputation (04/05) the1-year mortality rate was
32.7% and for minor amputation 18.3% (4)
• For a first major amputation the five-year cumulative mortality estimated at 68% - 78.7% (4)

Can we prevent amputations? Service Structure
• Ulceration and outcomes for patients are improved if there is: (1) – Screening for high risk patients – Foot protection service – Multidisciplinary foot care service – Implementation of pathway and guideline

Can we prevent amputations? Evidence
• Reduced ulceration • Reduced rates of hospital admission • Reduced length hospital Stay • Reduced hospital costs • Reduced levels and extent of amputation
Can we prevent amputations? Screening in practice
Remove shoes socks bandages and dressing Neuropathy :- check sensation 10g monofilament Limb Ischaemia:- Pulses as per PAD guidelines Ulceration Callus Infection Deformity Gangrene Charcot Arthropathy
Can we prevent amputations? Risk stratification
• Low risk: no risk factors present, for example, no signs of neuropathy,
no signs of peripheral arterial disease, and no other risk factors. • Moderate risk: 1 risk factor present, for example, signs of neuropathy
or signs of peripheral arterial disease, but without callus or deformity. Disabled adults who cannot see their feet are also at moderate risk.
• High risk: previous ulceration or amputation, or on renal replacement therapy, or more than 1 risk factor present, for example, signs of neuropathy or signs of peripheral arterial 1 disease, with callus or deformity

Can we prevent amputations? Risk stratification
• Active diabetic foot problem: ulceration, spreading infection, critical
ischaemia, gangrene, suspicion of an acute Charcot arthropathy, or an unexplained hot, red, swollen foot with or without pain.
Can we prevent amputations? General Diabetes Care
• Foot assessments at diagnosis along with education consistent for the
patient.
• Ulceration is related to poor diabetes control to help prevent progression we also need to focus on medical management.
Can we prevent amputations?
• Screening How are we doing?

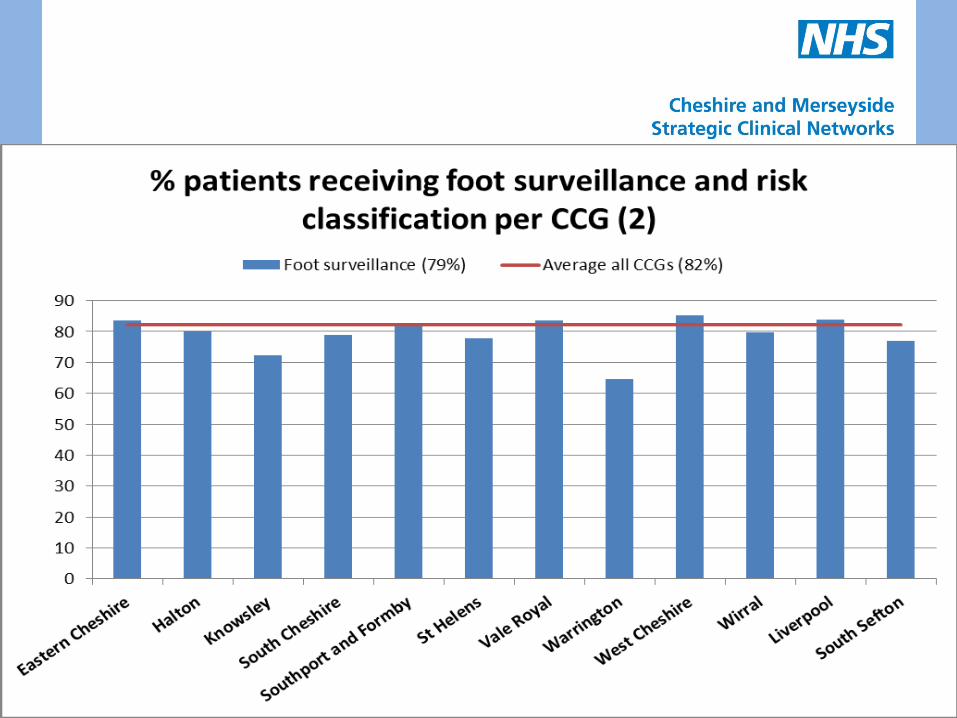
How are we doing? Screening
• The percentage of patients with diabetes, on the register, with a
record of a foot examination and risk classification in Cheshire and Merseyside 79.5

Diabetes Foot Screening in some areas is a risk!
How do we meet the challenge?

NICE consultation document states:
• A diabetic foot protection service (for preventing diabetic foot
problems, and for treating and managing diabetic foot problems in the community).
• A multidisciplinary foot care service (for managing diabetic foot problems in hospital and in the community that cannot be managed by the foot protection service).
NICE consultation document states:
• Robust protocols and clear local pathways for the continued and
integrated care of people across all healthcare settings, including emergency care and general practice. The protocols should set out the relationship between the foot protection service and the multidisciplinary foot care service.
• Regular reviews of treatment and patient outcomes, in line with the National Diabetes Audit
We need a pathway?

Primary Care Quality Assurance
• GP practices require on going update of competencies. • Podiatry to offer rolling quality assurance of screener competence
every three years via practice visit. • Revalidated with certificate. • Training should be part of staff induction.
Summary
• Foot problems in diabetes are a major challenge. • There are variations across the network of amputation and screening
rates. • There is evidence to support structured care and screening in
improving outcomes for patients. • The new pathway forms a basis for commissioning to help address the
existing inequalities in patient care and experience.

References 1. Diabetic Foot Problems: Prevention and management of foot
problems in people with diabetes NICE Guideline Draft Consultation Jan 2015
2. Kerr, M. Foot care for people with diabetes: the economic case for change. London: NHS Diabetes, 2012.
3. YHPHO. Quality and Outcomes Framework 2013- 14. YHPHO, 2014. Available online: http://www.hscic.gov.uk/catalogue/PUB15751
4. YHPHO. Diabetes Footcare Activity Profiles. YHPHO, 2014. Available online: http://www.yhpho.org.uk/diabetesprofilesfoot/default.aspx
5. Kerr, M. Foot care for people with diabetes: the economic case for change. London: NHS Diabetes, 2012.