Embed Size (px)
Citation preview

Diabetes and cardiovascular disease
Kausik Ray, MD
Imperial College London,
London, United Kingdom

DM and CVD Risk
Professor Kausik Ray
BSc, MBChB. MD, Mphil, FRCP (Lon), FRCP (Ed), FACC, FESC, FAHA
Professor of Public Health
School of Public Health, Imperial College London, UK

IDF diabetes atlas, 4th edition, 2009
2010 2030
Total number of people with diabetes (age 20-79)
285 million 438 million
Prevalence of diabetes (age 20-79)
6.6 % 7.8 %
Prevalence of diabetes in 2030

Coronary heart disease
Coronary death
Non-fatal myocardial infarction
Cerebrovascular disease
Ischaemic stroke
Haemorrhagic stroke
Unclassified stroke
Other vascular deaths
2.00 (1.83 - 2.19)
2.31 (2.05 - 2.60)
1.82 (1.64 - 2.03)
1.82 (1.65 - 2.01)
2.27 (1.95 - 2.65)
1.56 (1.19 - 2.05)
1.84 (1.59 - 2.13)
1.73 (1.51 - 1.98)
HR (95% CI)
26 505
11 556
14 741
11 176
3799
1183
4973
3826
Number
of cases
64 (54-71)
41 (24-54)
37 (19-51)
42 (25-55)
1 (0-20)
0 (0-26)
33 (12-48)
0 (0-26)
I2 (95% CI)
11 2 4
Hazard ratio (diabetes vs. no diabetes)
Outcome
Lancet. 2010 Jun 26;375(9733):2215-22
Diabetes doubles the risk of vascular diseaseData from 528,877 participants (adjusted for age sex, cohort, SBP, smoking, BMI)

Diabetes risk is not explained by conventional risk factors
Ischaemic stroke
Age and sex
Plus smoking status
Plus BMI
Plus SBP
Plus non-HDL-C
Plus HDL cholesterol
Plus log-triglycerides
2.06 (1.82-2.34)
2.10 (1.85-2.39)
2.00 (1.78-2.25)
1.91 (1.70-2.14)
1.93 (1.71-2.16)
1.87 (1.67-2.09)
1.87 (1.67-2.09)
HR (95% CI)
11 2 4
2.56 (2.15-3.05)
2.59 (2.16-3.09)
2.45 (2.08-2.88)
2.27 (1.94-2.65)
2.26 (1.94-2.64)
2.24 (1.94-2.60)
2.24 (1.94-2.59)
11 2 4
HR (95% CI)Adjusted for Coronary heart disease
11 2 4 11 2 4
Hazard ratio (diabetes vs. no diabetes)
Lancet. 2010 Jun 26;375(9733):2215-22

DM duration matters to CVD
Men with diabetes without MI Men with MI
None
N=3197
Late onset
N=307
Mean duration
1.7 years
Early onset
N=107
Mean duration
16 years
Without
diabetes
N=368
CVD events (n=534)
Age 1.00 1.59 (1.19,2.12) 2.61 (1.73,3.96) 2.35 (1.88,2.95)
Adj 1.00 1.53 (1.15,2.06) 2.52 (1.65,3.84) 2.23 (1.76,2.83)
Wannamethee, Shaper, Whincup, Lennon, Sattar (Archives Int Med in press)

Type 2 diabetes increases CHD/CVD risk over time
• CVD/CHD risk at or prior to diagnosis is determined by conventional CHD risk factors
• Hyperglycaemia in the diabetic range increases CHD risk over time
• After a diabetes duration of >8 years CHD risk equivalence is reached
Sattar N. Diabetologia 2013;56:686-695.
CH
D r
isk
Age
Diagnosis
~8–10years’
duration
CHD equivalence threshold

Prevention of Diabetes becomes increasingly essential
Why ?
• CV risk is incompletely explained by conventional risk factors
• Prognosis is worse with duration
How ?
• Tackling Obesity/ sedentary lifestyle/ caloric intake
• Legislation

Question: 1 what modality is best to lower CVD risk in DM ?Question: 2 how intensive should therapy be?
• Lipid-lowering?
• Blood pressure?
• Glucose-lowering?
• Aspirin?
• Lifestyle ?

Statins- reduce CV events consistently(per 39mg/dl lower LDL-C)
CTT Lancet 2008 ,371, 117-25

Time to First Major Cardiovascular Event in Patients With Diabetes
*CHD death, nonfatal non–procedure-related MI, resuscitated cardiac arrest, fatal or nonfatal stroke
HR = 0.75 (95% CI
0.58, 0.97)
P=0.026Atorvastatin 10 mg
Atorvastatin 80 mg
0 1 2 3 4 5 6
Time (years)
0.20
0.10
0.15
0.05
0
Cum
ula
tive
incid
ence
of
majo
r card
iovascula
r e
vents
*
Relative risk reduction = 25%

Fibrates ?

Fibrates and CVD risk reduction among those with atherogenic dyslipidemia
TG>200mg/dl and HDL <39mg/dl
Sacks et al NEJM 2010

Summary on lipids in T2DM
• Statin therapy remains the best lipid modifying agent
• Lower cholesterol targets (intensive statins) based on absolute risk. 50% LDL-C reduction or LDL-C <70mg/dl or 30%/ 100mg/dl in lower risk
• Fibrates, used as monotherapy or in combination therapy may have CVD benefit among those with atherogenic dyslipidemia and DM

Outline
• What treatments reduce CVD risk in Diabetes?
• Lipid-lowering?
• Blood pressure?
• Glucose-lowering?
• Aspirin?

Diabetics derive similar proportional reductions in risk as non-diabetics with BP lowering
BP treatment Trialists. Archives 2005, 165, 1410-1419

UKPDS lowering SBP reduces principally Strokes
BMJ 1998;317:703-713

ACCORD
Average after 1st year: 133.5 Standard 119.3 Intensive, Delta = 14.2
NEJM 2010, 362, 1575-1585

Primary & Secondary Outcomes
Intensive Events (%/yr)
StandardEvents (%/yr) HR (95% CI) P
Primary 208 (1.87) 237 (2.09) 0.88 (0.73-1.06) 0.20
Total Mortality 150 (1.28) 144 (1.19) 1.07 (0.85-1.35) 0.55
CardiovascularDeaths
60 (0.52) 58 (0.49) 1.06 (0.74-1.52) 0.74
Nonfatal MI 126 (1.13) 146 (1.28) 0.87 (0.68-1.10) 0.25
Nonfatal Stroke 34 (0.30) 55 (0.47) 0.63 (0.41-0.96) 0.03
Total Stroke 36 (0.32) 62 (0.53) 0.59 (0.39-0.89) 0.01
NEJM 2010, 362, 1575-1585

BP summary
• Actual BP achieved critical rather than agent used
– Meta-analysis
• Target BP <140/90 SBP for all
• More intensive target < 120 SBP results in stroke benefits

Outline
• What treatments reduce the CVD risk in Diabetes?
• Lipid-lowering?
• Blood pressure?
• Glucose-lowering?
• Aspirin?

Long-term beneficial effects on CVD risk following intensive treatment: DCCT/EDIC
0.12
0.10
0.08
0.06
0.04
0.02
0.00
Years since entry
Conventional therapy
Intensive therapy
1 2 3 4 5 6 7 8 9 10 11 12 210
Cu
mu
lati
ve in
cid
ence
of
any
pre
def
ined
card
iova
scu
lar
ou
tco
me
705714
683688
629618
11392
Intensive therapyConventional therapy
No. at risk
*Nonfatal MI or stroke; CV death; subclinical MI; angina; or the need for revascularization with angioplasty or coronary-artery bypass
13 14 15 16 17 18 19 20
42% risk reductionP=0.02
EDIC mean HbA1c over 11 years follow-up: 8.2%
EDIC mean HbA1c over 11 years follow-up: 8.0%
Nathan DM et al. N Engl J Med. 2005;353:2643-2653

Endpoints UKPDS PROactive ADVANCE VADT ACCORD Overall
Av FU 10.1 2.9 5.0 5.6 3.5 4.95
Person years of FU
46 237 15 059 55 700 10 030 35 879 162 905
Difference HbA1c (%)
0.9 0.6 0.5 1.5 1.1 0.9
NF- MI 362 263 309 142 421 1495
CHD 685 366 647 167 453 2318
Strokes 238 193 484 64 148 1127
Death from any cause
842 363 1031 197 460 2892
Ray KK, et al. Lancet. 2009;373:1765-1772

Effects of more vs less intensive control of glucose on non-fatal MI, CHD, stroke and mortality
I2=0% (95% CI 0-69.3%), p=0.61
Overall
ADVANCE
ACCORD
PROactive
VADT
UKPDS
21.86
28.86
9.44
21.81
0.83 (0.75, 0.93)
0.98 (0.78, 1.23)
0.78 (0.64, 0.95)
0.83 (0.64, 1.06)
0.81 (0.58, 1.15)
0.78 (0.62, 0.98)
100.00
28.86
18.03
1.4 .6 .8 1.2 1.4 1.6 1.8 2
Odds Ratio
Study
Intensive therapy better Standard therapy better
Weight
(%)
Odds Ratio
(95% CI)
Non-fatal MI
I2=0% (95% CI 0-53%), p=0.78
Overall
UKPDS
PROactive*
Study
ACCORD
ADVANCE
VADT
0.85 (0.77, 0.93)
Odds Ratio
(95% CI)
100.00
20.22
25.68
36.48
9.03
0.75 (0.54, 1.04)
0.81 (0.65, 1.00)
0.82 (0.68, 0.99)
0.92 (0.78, 1.07)
0.85 (0.62, 1.17)
8.59
Weight
(%)
1.4 .6 .8 1.2 1.4 1.6 1.8 2
Odds RatioIntensive therapy better Standard therapy better
CHD
I2=0% (95% CI 0-62%), p = 0.70
Overall
ACCORD
ADVANCE
PROactive†
UKPDS
VADT†
0.93 (0.81, 1.06)
1.05 (0.76, 1.46)
0.91 (0.51, 1.61)
0.78 (0.47, 1.28)
16.21
5.18
0.97 (0.81, 1.16)
0.81 (0.60, 1.08)
100.00
51.38
20.47
6.76
1.4 .6 .8 1.2 1.4 1.6 1.8 2
Odds RatioIntensive therapy better Standard therapy better
StudyOdds Ratio
(95% CI)
Weight
(%)
Stroke
Ray KK, et al. Lancet. 2009; 373:1765–72
I2=58% (95% CI 0-84%), p=0.049
Overall
ADVANCE
ACCORD
UKPDS
VADT
PROactive
1.02 (0.87, 1.19)
0.93 (0.82, 1.05)
1.28 (1.06, 1.54)
1.09 (0.81, 1.47)
0.96 (0.77, 1.19)
29.38
23.64
10.05
15.46
21.47
0.79 (0.53, 1.20)
100.00
1.4 .6 .8 1.2 1.4 1.6 1.8 2
Odds RatioIntensive therapy better Standard therapy better
Study
Odds Ratio
(95% CI)Weight
(%)
All-cause mortality
*Included non-fatal myocardial infarction and death from all-cardiac mortality. †Included only non-fatal strokes.

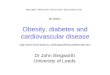
CV risk reduction requires multiple interventions including blood pressure and lipid management
-12,5
-8,2
-2,9
-14
-12
-10
-8
-6
-4
-2
0
Nu
mb
er
of
CV
eve
nts
* p
reve
nte
d
Per 4mmHg lower SBP
Per 1mmol/L lower LDL-C
Per 0.9% lower HbA1c
Benefit of different interventions per 200 diabetic patients treated for 5 years
*Comprised non-fatal myocardial infarction, coronary heart disease, stroke and all-cause mortality
Ray KK, et al. Lancet. 2009;373:1765–72

The vertical dashed line indicates the overall hazard ratio. The size of each square is proportional to the number of patients
ACCORD Study Group. N Engl J Med 2008;358:2545–2559
0.6 1.0 1.4
p value
Favours intensive Favours standard
0.04
0.03
Hazard ratio(95% CI)
Primary outcome
Subgroup
Total
Previous CV event
No
Yes
Glycated haemoglobin at baseline
≤8.0%
>8.0%
ACCORD: intensive glucose control beneficial in patients with no previous CVD or HbA1c <8%


What is the mechanism ?

Summary
• An HbA1c of 6.6 vs 7.5 % over 5y results in
• about a 15% lower risk of CHD
• without an excess mortality risk
• But
• Absolute benefit is modest

Outline
• What treatments reduce the CVD risk in Diabetes?
• Lipid-lowering?
• Blood pressure?
• Glucose-lowering?
• Aspirin?

Effect of aspirin primary prevention of major CVD events in diabetes
De Berardis G et al. BMJ 2009;339:bmj.b4531

Significant increase in risk of bleeding with aspirin

Aspirin: summary for DM patients
• Men- benefit on NFMI
• Women none overall for any endpoint
• Absolute benefits are modest and approximately equal to the risk of bleeding
• For every 10, 000 people Tx in PP about 5 fewer NFMI, but 1 extra haemorrhagic stroke and 3 major bleeds

Conclusions
• When you have it multimodality intervention to reduce macro-vascular and microvascular disease complications
• Prevention is better than cure

Prevention is better than cure!
Tuomilheto NEJM, 2001, 344, 1343-1350