Embed Size (px)
Citation preview
DIAGNOSIS AND
MANAGEMENT OF DHF
AND DSS
11/20/2012 1
INTRODUCTION
DHF relatively new diseases in Indonesia
1968 in Surabaya and Jakarta
1973 in Manado
Management divided in DHF and DSS
Mortality rate in : 1968 41.3 %
1992 2.9 %
1995 2.5 %
11/20/2012 2
DIAGNOSIS WHO 1975 / 1986
Base on 4 clinical and 2 laboratoric criteria
Clinical : High fever 2 – 7 days
Hemorrhagic manifestation
Hepatomegaly
Shock
Laboratoric Thrombocytopenia
Hemoconcentration
Dx : Minimally 2 clinical + Lab criteria
The accuracy : 75 – 90 % 11/20/2012 3
The severity of disease divided in 4
grade
I : Fever + non spesific + RL (+)
II : I + Other hemorrh manifest
III : II + mild shock
IV : III + severe shock
Grade I + II : DHF
III + IV : DSS
11/20/2012 4
DHF : - permeability
- Fever crisis
DHF I, II :
Crisis days III >
IVFD 12 – 24 hours
PCV , Tr < 50 000
Health center / >
11/20/2012 5
Fever phase
Oral fluid : 50 ml/kgBW for 4 – 6 hours
IVFD manitenance : 80 – 100 ml/kg/days
Antipyretic : paracetamol 10 mg/kgBW/time
Convulsion : Phenobarbital 5 mg/kgBW/days
Critical Ill : Days 3 - 5
11/20/2012 6
SUBSTITUTION FLUID IN DHF
Maintenance + 5 – 8 %
Vomiting every time
Cannot drink
fever
PCV periodically
Acidosis : NaBic
PCV > 20 % IVFD : GED mild - mod
11/20/2012 7
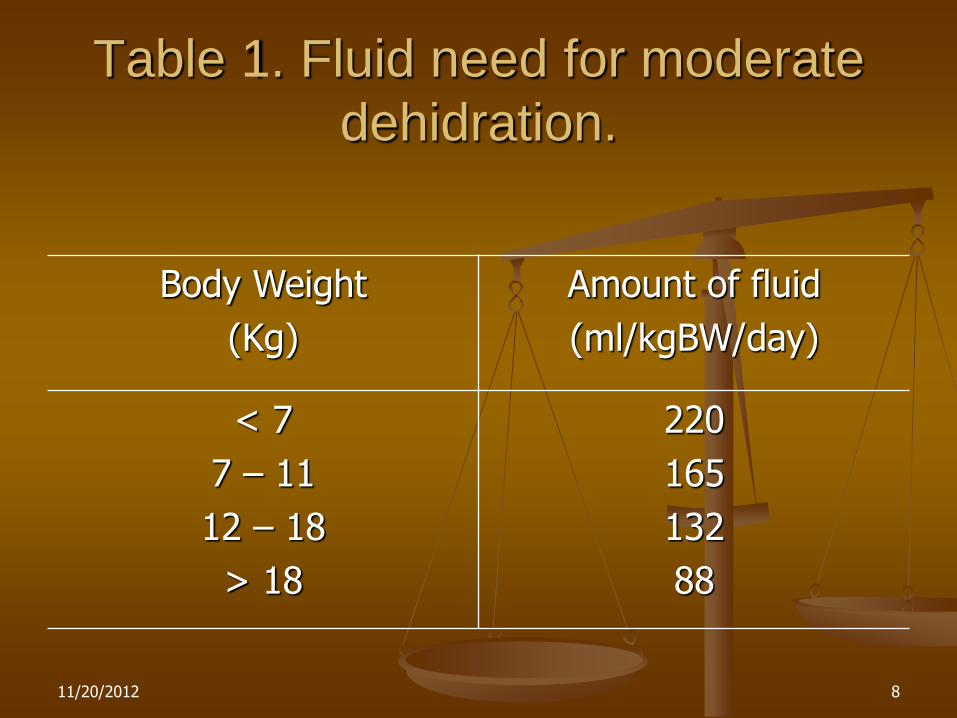
Table 1. Fluid need for moderate
dehidration.
Body Weight
(Kg)
Amount of fluid
(ml/kgBW/day)
< 7
7 – 11
12 – 18
> 18
220
165
132
88
11/20/2012 8
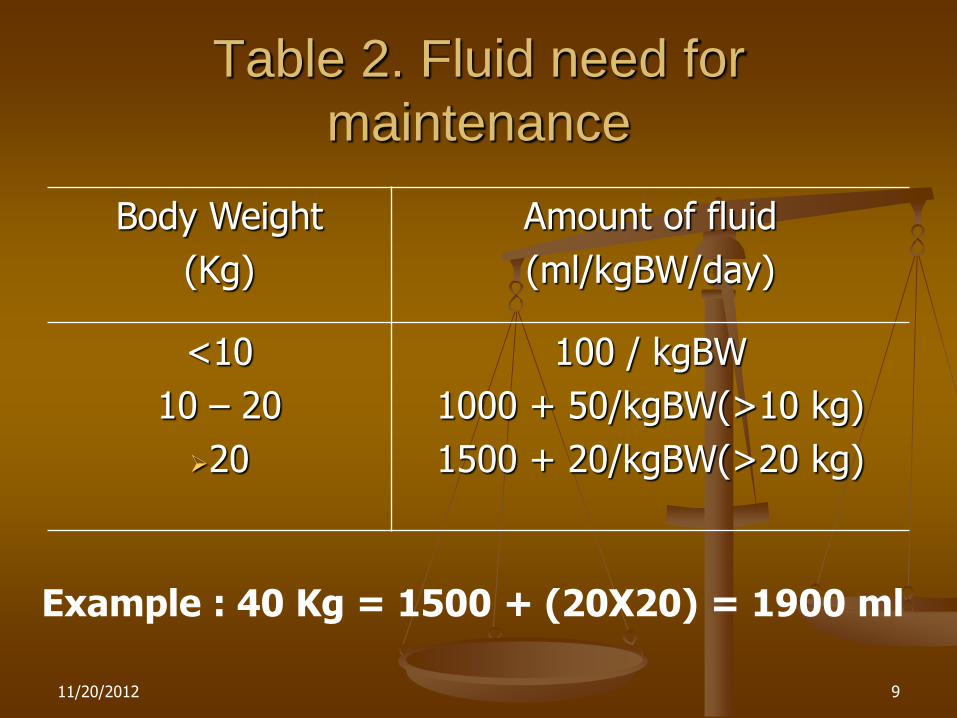
Table 2. Fluid need for
maintenance
Body Weight
(Kg)
Amount of fluid
(ml/kgBW/day)
<10
10 – 20
20
100 / kgBW
1000 + 50/kgBW(>10 kg)
1500 + 20/kgBW(>20 kg)
Example : 40 Kg = 1500 + (20X20) = 1900 ml
11/20/2012 9
Temperature leakage Reconvalescen reabsorbtion of fluid Sign + symptom of shock
hospitalization Fluid Recommended (WHO)
Cristaloid : RL – RL-D5% RA – RA-D5% NaCl 0.9 % - NaCl 0.9%-D5% Colloid : Plasma Dextran L 40 HAES Gelofusin Gelofundin
11/20/2012 10
DSS
Shock emergency – fluid recovery 48 hours
Replacement of plasma volume
Cristaloid : 20 ml/kgBW/30 min
Still Shock : Koloid 10 – 20 ml/kgBW/h
Maximal 30 ml/kgBW
Improvement : Cristaloid 10 – 20 ml/kgBW/h
Still syok, PCV bleeding blood
PCV > 40 blood 10 ml/kgBW/h
Massive bleeding blood 20 ml/kgBW/h
Improvement Cristaloid
11/20/2012 11
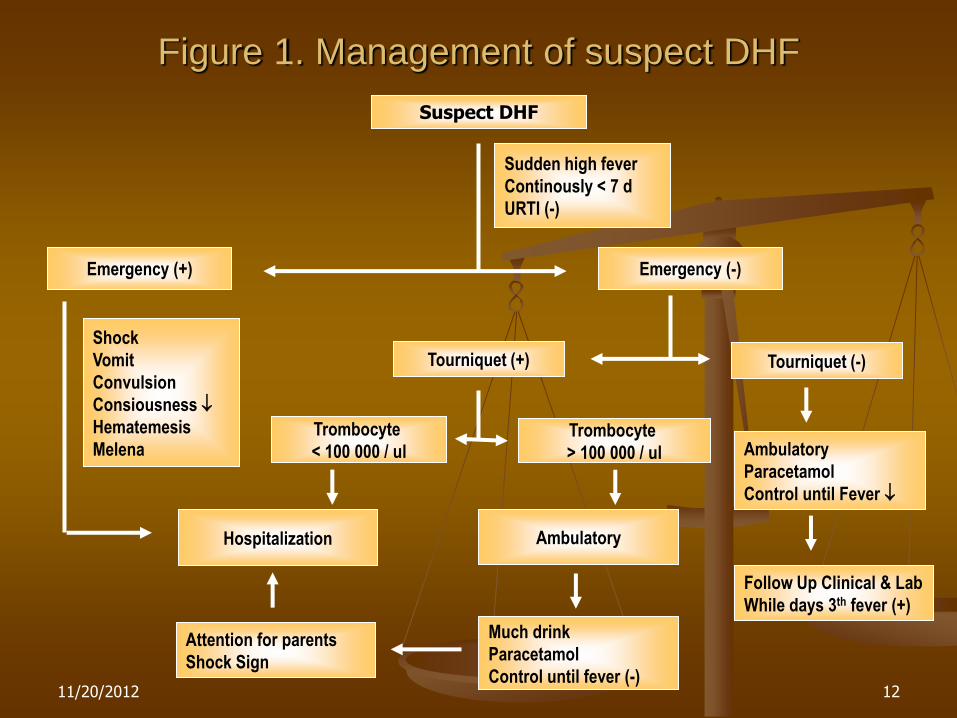
Figure 1. Management of suspect DHF
Suspect DHF
Sudden high fever
Continously < 7 d
URTI (-)
Emergency (-) Emergency (+)
Shock
Vomit
Convulsion
Consiousness
Hematemesis
Melena Ambulatory
Paracetamol
Control until Fever
Tourniquet (+) Tourniquet (-)
Follow Up Clinical & Lab
While days 3th fever (+)
Attention for parents
Shock Sign
Trombocyte
> 100 000 / ul
Trombocyte
< 100 000 / ul
Hospitalization
Much drink
Paracetamol
Control until fever (-)
Ambulatory
11/20/2012 12
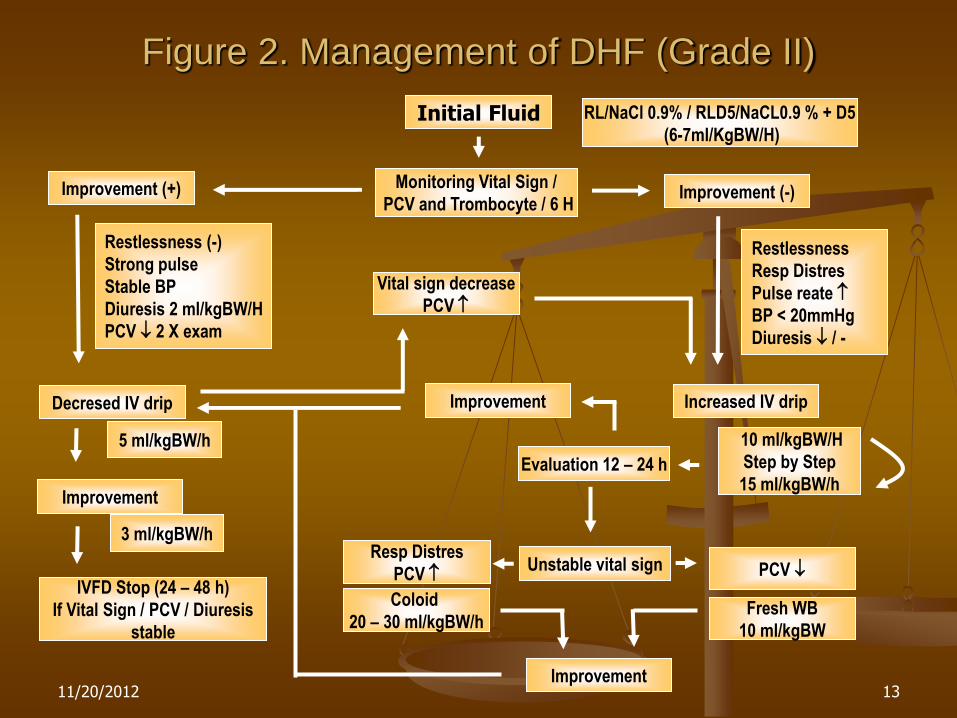
Figure 2. Management of DHF (Grade II)
Initial Fluid RL/NaCl 0.9% / RLD5/NaCL0.9 % + D5
(6-7ml/KgBW/H)
Decresed IV drip
Monitoring Vital Sign /
PCV and Trombocyte / 6 H
Restlessness (-)
Strong pulse
Stable BP
Diuresis 2 ml/kgBW/H
PCV 2 X exam
Improvement (+) Improvement (-)
Restlessness
Resp Distres
Pulse reate
BP < 20mmHg
Diuresis / -
10 ml/kgBW/H
Step by Step
15 ml/kgBW/h
Increased IV drip
Evaluation 12 – 24 h
Improvement
Unstable vital sign Resp Distres
PCV PCV
Coloid
20 – 30 ml/kgBW/h Fresh WB
10 ml/kgBW
Improvement
Improvement
Vital sign decrease
PCV
IVFD Stop (24 – 48 h)
If Vital Sign / PCV / Diuresis
stable
5 ml/kgBW/h
3 ml/kgBW/h
11/20/2012 13
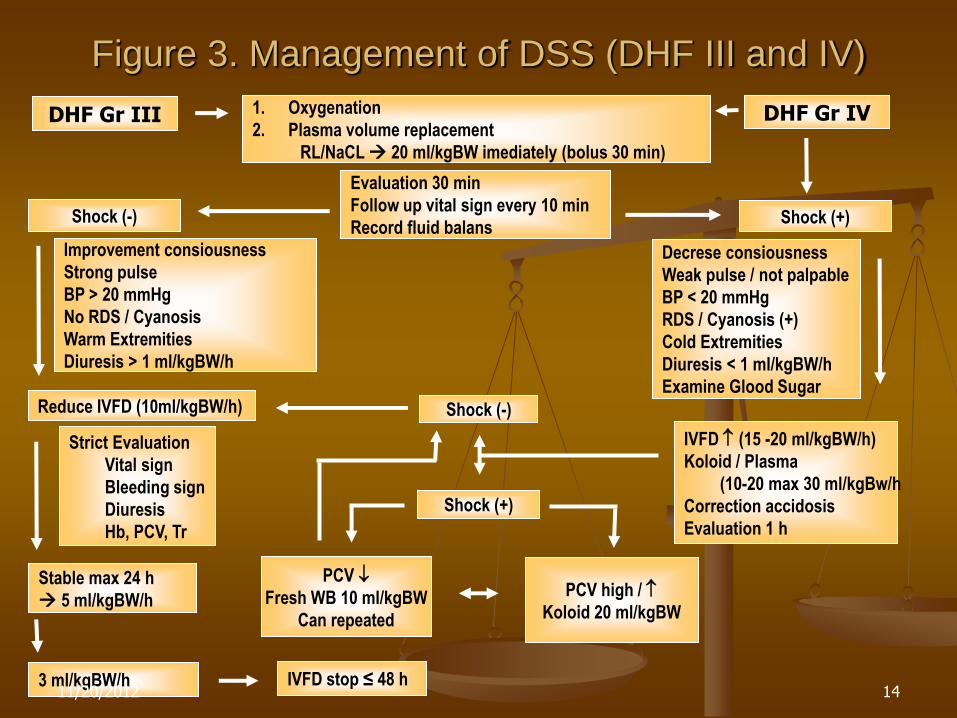
Figure 3. Management of DSS (DHF III and IV)
DHF Gr III 1. Oxygenation
2. Plasma volume replacement
RL/NaCL 20 ml/kgBW imediately (bolus 30 min)
Evaluation 30 min
Follow up vital sign every 10 min
Record fluid balans Shock (-) Shock (+)
DHF Gr IV
Improvement consiousness
Strong pulse
BP > 20 mmHg
No RDS / Cyanosis
Warm Extremities
Diuresis > 1 ml/kgBW/h
Decrese consiousness
Weak pulse / not palpable
BP < 20 mmHg
RDS / Cyanosis (+)
Cold Extremities
Diuresis < 1 ml/kgBW/h
Examine Glood Sugar Reduce IVFD (10ml/kgBW/h)
IVFD (15 -20 ml/kgBW/h)
Koloid / Plasma
(10-20 max 30 ml/kgBw/h
Correction accidosis
Evaluation 1 h
Shock (+)
Shock (-)
PCV high /
Koloid 20 ml/kgBW
PCV
Fresh WB 10 ml/kgBW
Can repeated
Strict Evaluation
Vital sign
Bleeding sign
Diuresis
Hb, PCV, Tr
Stable max 24 h
5 ml/kgBW/h
3 ml/kgBW/h IVFD stop ≤ 48 h 11/20/2012 14
COMPLICATIONS
Electrolyte Imbalance Hyponatremia
Hypocalcemia
Fluid overload Early IVFD
Hypotonic Solution
Not IVFD
Not Use Colloidal Sol / Plasma
Not Give blood transf
Not Calculate IVFD 11/20/2012 15
Signs and Symptoms of Fluid Overload
RSD, Dyspnea and Tachypnea
Massive acites
Rapid Pulse
↓ Pulse pressure
Crepitation/Ronchi
Porr tissue perfusion
COMPLICATIONS
11/20/2012 16
Management of fluid overload
Change IV to Dextrans 40
Urinary Catheter
Furosemide 1 mg/kgBW, IV
Still Shock Dextrans 40, 10 mg/kgBW in 10-15 min
Record Urine output
Furosemide may repeat if still RDS
CVP if not Response furosemide
Ventilatory support
Pleural/peritoneal tapping
COMPLICATIONS
11/20/2012 17
Unusual manifestation of DHF
Less than 5% of patient
Encephalopathy/encephalitis
Hepatic failure
Renal failure
Dual infections
Underlying conditions
COMPLICATIONS
11/20/2012 18
Signs and Symptoms of Fluid Overload
Prolonged shock
Acute hemolysis + Hb uria
G6PD
Hemoglobinopathy
Management of acute hemolysis + Hb Uria
Transfussion PRC of FWB
IVFD according the stage
Alkaline urine
COMPLICATIONS
11/20/2012 19
Dual Infections
Associate :
GI, Salmonella
RI, Pneumonia
Urinary infections
Skin + soft tissue inf
Nosocomial
Thrombophlebitis
Pneumonia
UTI (Catheter)
Others
Transfussion reaction
Hepatitis
Massive GI Hem
Drugs reactions
COMPLICATIONS
11/20/2012 20
Common causes of encephalopathy
Hepatic encephalopathy Severeshock
Inborn error of metab
Hepatotoxic drugs
Underlying liver diseases
Electrolyte imbalance
Metabolic distrubance (hypoglycemia)
Intracranial bleeding
Cerebral thrombosis/ischemia
COMPLICATIONS
11/20/2012 21
Management of DHF hepatic encephalopathy
Maintain oxygenation
Prevent ↑ intracranial press : Restrict IV
Furosemide + / dexamethasone
↓ Amonia production
Vit K1 3-10 mg IV
Correct metab acidosis
PRC if indicated
Antibiotic
H2 Blocker if massive GI Bleeding
Avoid unnecessary drugs
Exchange tranf if needed
Dyalisis if needed
Branch – chain aminoacid
COMPLICATIONS
11/20/2012 22
INDICATION FOR DISCHARGE
Not fever in 24 h
Good appetite
Good general condition
Diuresis
Normal PCV (38 – 40)
≥ 2 days after shock
No dyspnea
Platelet > 50 000/mm3
No complication
11/20/2012 23
CAUSES OF DEATH
Prolonged shock
Fluid overload
Massive bleeding
Unusual manifestation
11/20/2012 24

11/20/2012 25





























