Embed Size (px)
Citation preview

DGH v Tertiary InterventionDGH v Tertiary InterventionIs there really a conflict?Is there really a conflict?
“The BCIS Perspective”“The BCIS Perspective”
Dr Martyn ThomasDr Martyn Thomas
Kings College HospitalKings College Hospital
BCIS PresidentBCIS President

MY CONFLICTSOF INTEREST ARE:
Research Support: Boston Scientific, Cordis and Medtronic
Advisory Board for: Boston, Cordis, Abbott, Lilly and Nycomed.

DGH v Tertiary InterventionDGH v Tertiary Intervention(p.s. surgical v non surgical(p.s. surgical v non surgical
centres!)centres!)Is there really a conflict?Is there really a conflict?“The BCIS Perspective”“The BCIS Perspective”
• What “experience” do I have to give What “experience” do I have to give such a talk?such a talk?
- BCIS President- BCIS President
- Currently perform PCI at Kings College - Currently perform PCI at Kings College Hospital (Teriary) Hospital (Teriary) AND AND the “Mayday the “Mayday Hospital” (DGH). Gives some Hospital” (DGH). Gives some perspective!!perspective!!

DGH v Tertiary InterventionDGH v Tertiary InterventionIs there really a conflict?Is there really a conflict?
“The BCIS Perspective”“The BCIS Perspective”
Where does the UK stand in Where does the UK stand in worldwide terms with regard worldwide terms with regard
to revascularisation??to revascularisation??

Total UK PCI Total UK PCI ProceduresProceduresYear Centres Total
Procedures Rate per million Increase
(%) 1991 52 9,933 174 1992 52 11,575 203 16.5 1993 53 12,937 227 11.8 1994 54 14,624 256 13.0 1995 54 17,344 304 18.6 1996 53 20,511 359 18.1 1997 58 22,902 402 11.7 1998 61 24,899 437 8.7 1999 63 28,133 494 13 2000 66 33,652 590 20 2001 64 38,992 664 12.5 2002 64 44,913 759 14.3 2003 73 53,261 894 17.8 2004 77 62,780 1050 17.4 2005 83 70,142 1165 11.0
2005 data: Ludman

A worldwide perspective.A worldwide perspective.
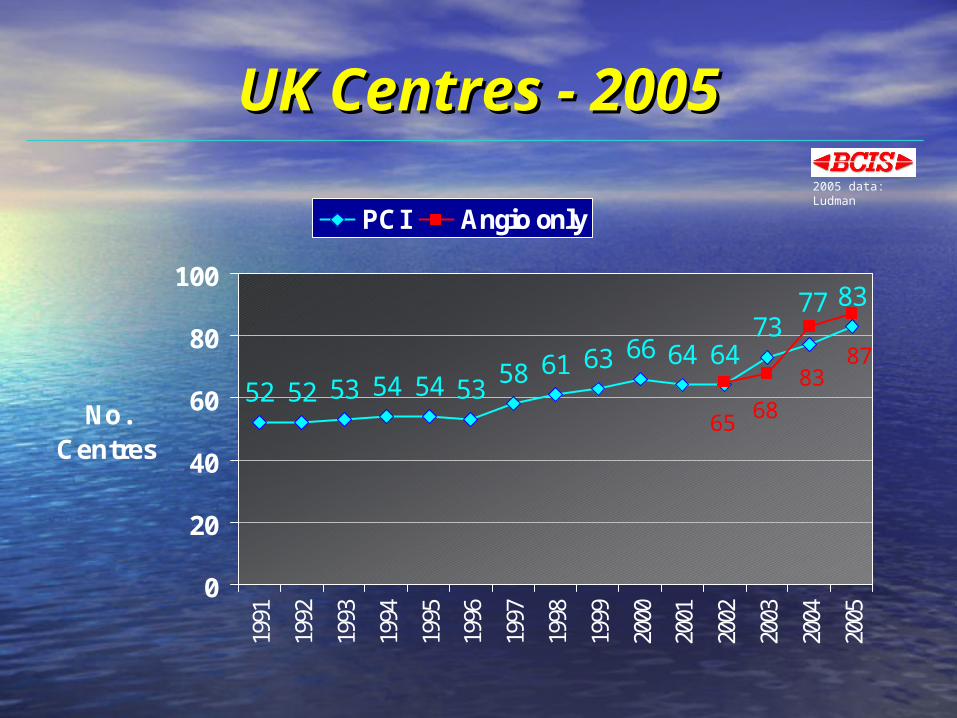
UK Centres - 2005UK Centres - 2005
52 52 53 54 54 5358 61 63 66 64 64
738377
87
6568
83
0
20
40
60
80
10019
91
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
No.Centres
PCI Angio only
2005 data: Ludman

What are the current What are the current guidelines:guidelines:
for a new PCI centre?for a new PCI centre?

What are the current What are the current guidelines:guidelines:
for an operator?for an operator?

Number of PCIs performed in 2005Number of PCIs performed in 2005((per NHS Centre)per NHS Centre)
0
500
1000
1500
2000
2500
3000
Num
ber
of P
CIs
Individual Centres
2005 data: Ludman
Data from: all 65 NHS centres
Mean = 1028

Surgical CoverSurgical Cover

Surgical coverSurgical cover

YearYear
% % ProcedurProcedur
eeSuccessSuccess
% QMI % QMI % Re PCI for % Re PCI for acute closure acute closure % Em. CABG% Em. CABG Mortality Mortality
(%)(%)
19951995 8989 1.41.4 1.91.9 0.690.6919961996 9090 1.41.4 1.71.7 0.720.7219971997 9292 1.21.2 1.11.1 0.890.8919981998 9292 0.80.8 0.70.7 0.800.80
19991999 9090 0.570.57 0.480.48 0.610.61
20002000 9292 0.60.6 0.40.4 0.640.64
20012001 9494 0.50.5 0.40.4 0.750.75
20022002 9292(51 of 64)(51 of 64)
0.570.57(49 of (49 of
64)64)
0.330.33(50 of 64)(50 of 64)
0.280.28(53 of 64)(53 of 64)
0.540.54(53 of 64)(53 of 64)
20032003 9292(62 of 73)(62 of 73)
0.360.36(56 of (56 of
73)73)
0.170.17(62 of 73)(62 of 73)
0.290.29(64 of 73)(64 of 73)
0.530.53(64 of 73)(64 of 73)
20042004 93.593.5(63 of 78)(63 of 78)
0.300.30(57 of (57 of
78)78)
0.300.30(61 of 78)(61 of 78)
0.210.21(64 of 78)(64 of 78)
0.560.56(66 of 78)(66 of 78)
20052005 90.290.2 0.240.24 0.120.12 0.590.59
MACE (2005) - All PCIsMACE (2005) - All PCIsAll Data from CCAD + Form CAll Data from CCAD + Form C
2005 data: Ludman

Surgical CoverSurgical Cover(all 83 NHS and Private Centres)(all 83 NHS and Private Centres)
On siteOn site Off siteOff siteNo of centresNo of centres 5454
(65%)(65%)
2929(35%)(35%)
No. of PCI No. of PCI (% of total)(% of total) 57,54557,545(82%)(82%)
12,62212,622(18%)(18%)
Mean No. PCI per Mean No. PCI per centre centre 1065.61065.6 435.2435.2
PCIs per PCIs per interventionistinterventionist(all 65 NHS centres only):(all 65 NHS centres only):
167.4167.4 114.4114.4
2005 data: Ludman

Tertiary (Surgical) and DGH (Non-Surgical) Tertiary (Surgical) and DGH (Non-Surgical) centres receiving BCIS visits since 2004 (the centres receiving BCIS visits since 2004 (the
“Truth!”.“Truth!”.
1:20 is aSurgical centre!
Tertiary (surgical centre) Tertiary (surgical centre) ParanoiaParanoia
Where is all the work?Where is all the work?What will we do?What will we do?


The Model (DOH)The Model (DOH)
• 3 levels of revascularisation tested; 3 levels of revascularisation tested; 1900, 2200 and 2500 per million, by 1900, 2200 and 2500 per million, by 20152015
• 7.2% increase in ICDs, reaching 7.2% increase in ICDs, reaching latest NICE guidelines by 2015.latest NICE guidelines by 2015.
• A range of 5-15% increase in A range of 5-15% increase in interventions for EP/arrythmias.interventions for EP/arrythmias.

•NB: BCS 2004 NB: BCS 2004 proposed 2200-3300 proposed 2200-3300
per million for PCI per million for PCI alone!!alone!!
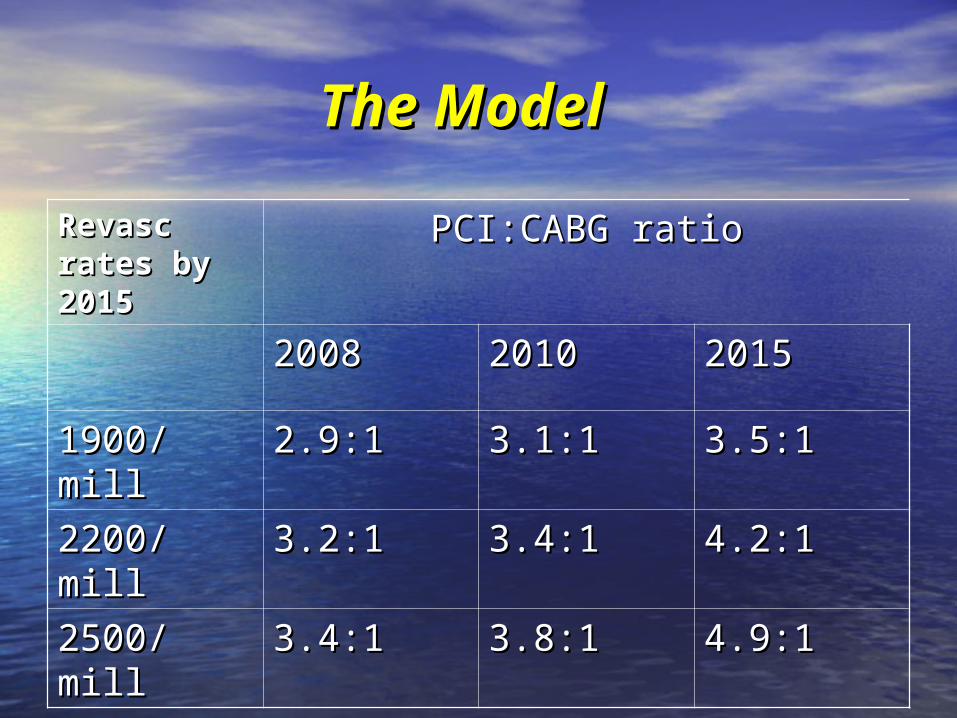
The ModelThe Model
Revasc Revasc rates by rates by 20152015
PCI:CABG ratioPCI:CABG ratio
20082008 20102010 20152015
1900/mill1900/mill 2.9:12.9:1 3.1:13.1:1 3.5:13.5:1
2200/mill2200/mill 3.2:13.2:1 3.4:13.4:1 4.2:14.2:1
2500/mill2500/mill 3.4:13.4:1 3.8:13.8:1 4.9:14.9:1

Where will PCI take place in Where will PCI take place in the future?the future?
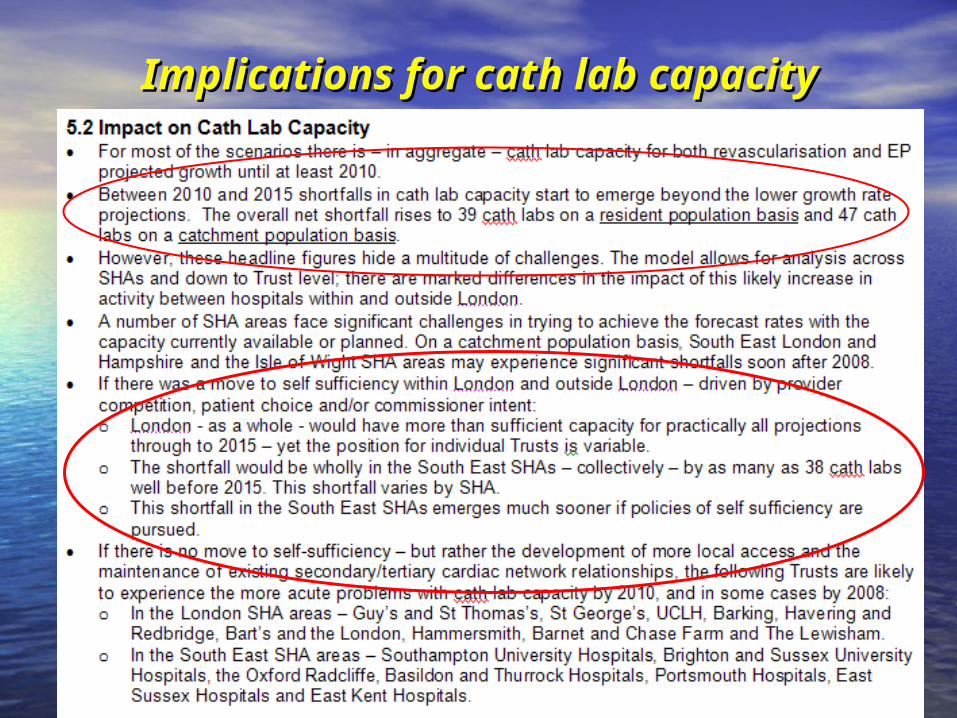
Implications for cath lab capacityImplications for cath lab capacity

Potential growth areasPotential growth areas? For the surgical centres? For the surgical centres
• ““Hole” closure: PFO, ASD etc.Hole” closure: PFO, ASD etc.
• Percutaneous Valve therapy.Percutaneous Valve therapy.
• Intramyocardial injection therapyIntramyocardial injection therapy
• ““Gene/cell” therapy.Gene/cell” therapy.

Specific “issues” with a Specific “issues” with a change toward PCI in non-change toward PCI in non-
surgical centressurgical centres(not outcome related!)(not outcome related!)
• Changes needed in the organisation Changes needed in the organisation of some interventional research.of some interventional research.
• Case Mix (the Tariff).Case Mix (the Tariff).

Interventional ResearchInterventional ResearchConsequences of a Consequences of a “devolved service”“devolved service”
• Currently a “handful” of surgical centres have Currently a “handful” of surgical centres have the infra-structure, and perform international the infra-structure, and perform international multicentre randomised trials and registries.multicentre randomised trials and registries.
• For FIM type cases this requires relatively For FIM type cases this requires relatively straightforward lesions………..these will be straightforward lesions………..these will be increasingly rare in the surgical centres.increasingly rare in the surgical centres.
• A change of infra-structure/research staff etc A change of infra-structure/research staff etc will therefore be necessary for this activity to will therefore be necessary for this activity to continue. continue.

The TariffThe TariffProblems of Case MixProblems of Case Mix
• E15: Percutaneous coronary interventionE15: Percutaneous coronary intervention• Elective £3660Elective £3660• Non-elective £4758Non-elective £4758• CABG elective £7195CABG elective £7195• CABG non elective £8748CABG non elective £8748
• Kings MFF 1.3Kings MFF 1.3• +16% uplift+16% uplift
• Leads to PCI elective=£5519 and PCI non Leads to PCI elective=£5519 and PCI non elective=£7175elective=£7175

Tertiary centre: year 1Tertiary centre: year 1100 cases referred from DGH100 cases referred from DGH60% unstable and 40% stable60% unstable and 40% stable
25% multiple stents25% multiple stents• Simple elective: make £500, Complex elective: lose £1000Simple elective: make £500, Complex elective: lose £1000• Simple non-elective: make £1,500, Complex non-elective: Simple non-elective: make £1,500, Complex non-elective:
lose 1,500lose 1,500
• Revenue:Revenue:• Simple non-elective: +£67,500Simple non-elective: +£67,500• Complex non-elective: -£22,500Complex non-elective: -£22,500• Simple elective: +£15,000Simple elective: +£15,000• Complex elective: -£10,000Complex elective: -£10,000
• Net income= +£50,000Net income= +£50,000

Tertiary centre: year 2Tertiary centre: year 225 cases referred from DGH25 cases referred from DGH
(all complex), 75 cases done in (all complex), 75 cases done in non surgical centre.non surgical centre.
• Non-surgical centre:Non-surgical centre:• Simple non-elective: +£67,500Simple non-elective: +£67,500• Simple complex: +£15,000Simple complex: +£15,000• Revenue: +£82,500Revenue: +£82,500
• Tertiary centre:Tertiary centre:• Complex non-elective: -£22,500Complex non-elective: -£22,500• Complex elective: -£10,000Complex elective: -£10,000• Revenue: -£32,500Revenue: -£32,500

Potential consequences of the Potential consequences of the Tariff and non-surgical centre Tariff and non-surgical centre
PCI.PCI.• Potential diversion of Potential diversion of
revascularisation toward surgery revascularisation toward surgery because of “skewed” case mix because of “skewed” case mix leading to PCI being non-viable.leading to PCI being non-viable.
• Potential of “profiteering” of DGH at Potential of “profiteering” of DGH at the expense of Quality.the expense of Quality.

Personnel view!!Personnel view!!
• Fully supportive of non-surgical Fully supportive of non-surgical centre PCI, as long as volume and centre PCI, as long as volume and expertise are maintained. expertise are maintained.
• Here are the last x2 cases at the Here are the last x2 cases at the Mayday………….last Thursday.Mayday………….last Thursday.

ConclusionsConclusions Training and experience has more influence Training and experience has more influence
on outcome of PCI than location.on outcome of PCI than location. As long as individual and institutional As long as individual and institutional
volumes are maintained BCIS fully supports volumes are maintained BCIS fully supports the development of non-surgical centre PCI.the development of non-surgical centre PCI.
Strong links between the surgical centre Strong links between the surgical centre and non-surgical centre with exchange of and non-surgical centre with exchange of personnel and audit data in both directions personnel and audit data in both directions is essential.is essential.
Achievement of “European” type rates of Achievement of “European” type rates of revascularisation cannot be done without revascularisation cannot be done without full use of the non-surgical cath labs. full use of the non-surgical cath labs.

ConclusionsConclusions Development of research infrastructure within Development of research infrastructure within
the non-surgical centres should be the non-surgical centres should be encouraged.encouraged.
Surgical centre operators should be Surgical centre operators should be encouraged to “support” non-surgical encouraged to “support” non-surgical centres, including performing PCI sessions.centres, including performing PCI sessions.
Some form of tariff sharing may be required Some form of tariff sharing may be required across Networks to make all units viable and across Networks to make all units viable and to avoid distortion of clinical practice for to avoid distortion of clinical practice for financial reasons.financial reasons.





























