Embed Size (px)
Citation preview
DFID Nepal:Contribution to improved Contribution to improved health outcomes
British Embassy21 02 201121.02.2011
Slide 1
Content
• Health outcomes in Nepal – particularly Reproductive and Maternal Health (RMH)P d t f DFID N l i• Programmes and outcomes of DFID Nepal – an overview
• DFID support to health, particularly RMH• Future challenges
Slide 2
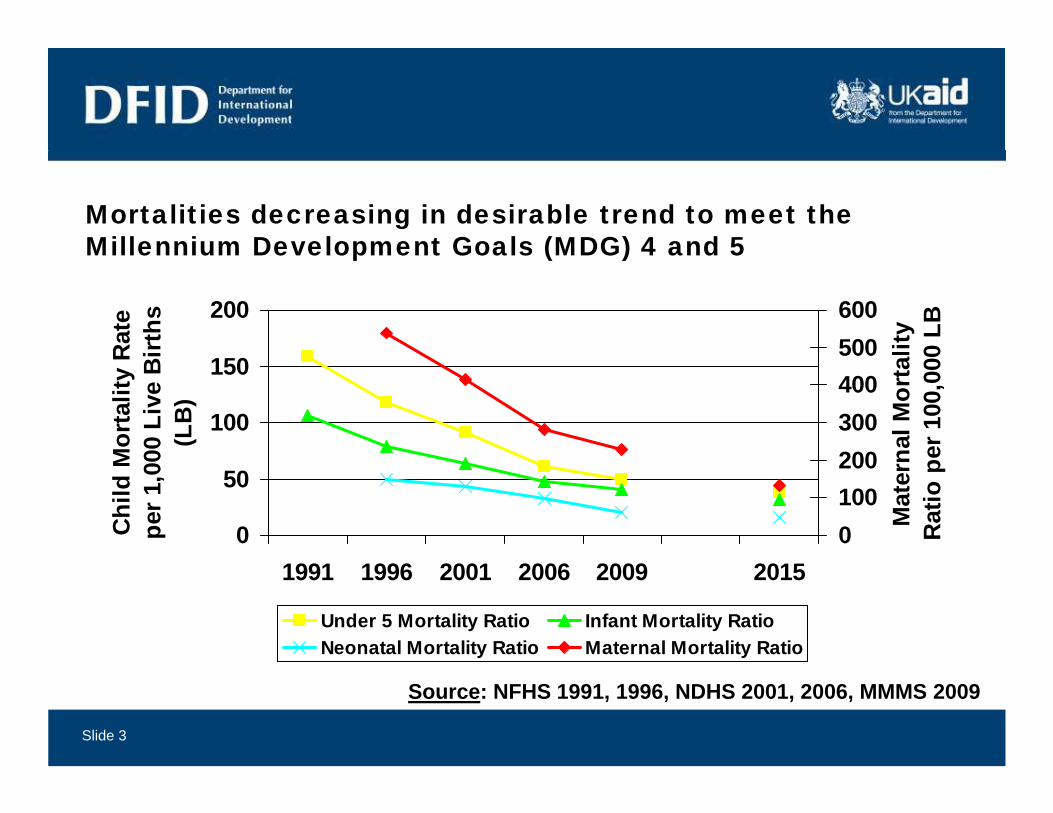
Mortalities decreasing in desirable trend to meet the Millennium Development Goals (MDG) 4 and 5Millennium Development Goals (MDG) 4 and 5
200
Rat
e irt
hs
500600
lity
0 LB
100
150
Mor
talit
y R
00 L
ive
Bi
(LB
)
200300400500
nal M
orta
er 1
00,0
0 0
0
50
Chi
ld M
per 1
,00
0100200
Mat
ern
Rat
io p
1991 1996 2001 2006 2009 2015
Under 5 Mortality Ratio Infant Mortality RatioNeonatal Mortality Ratio Maternal Mortality Ratio
Slide 3
Source: NFHS 1991, 1996, NDHS 2001, 2006, MMMS 2009
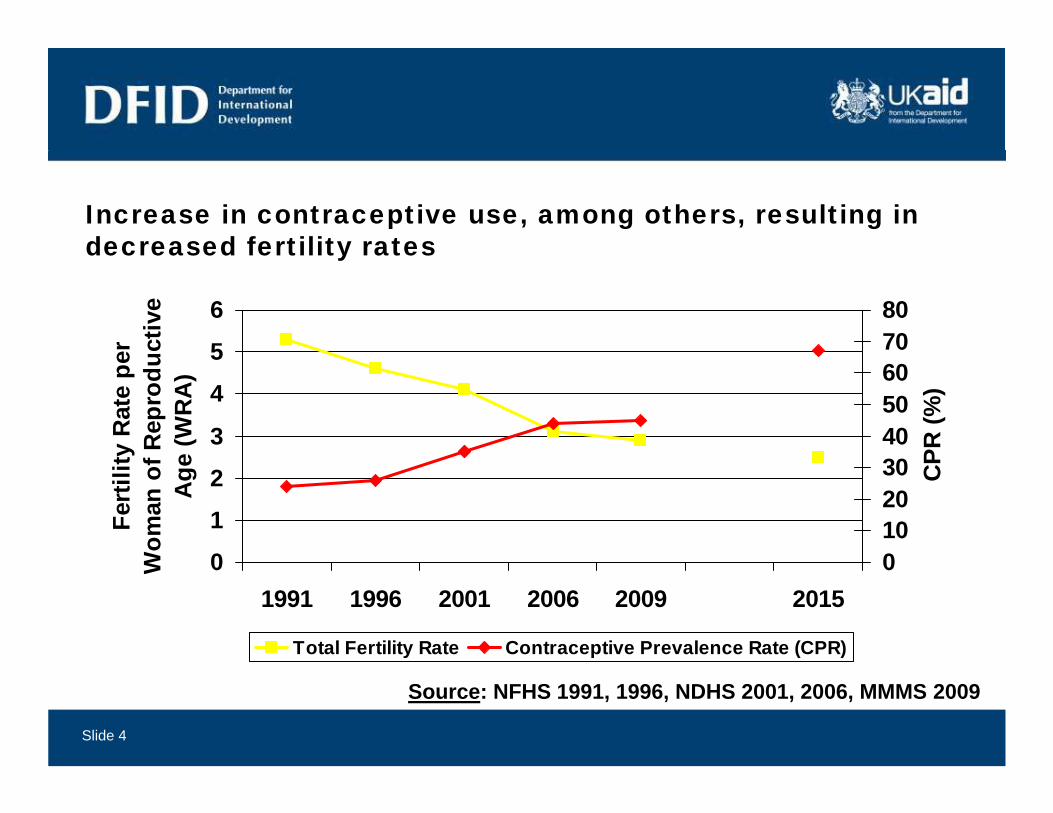
Increase in contraceptive use, among others, resulting in decreased fertility ratesdecreased fertility rates
5
6
er
uctiv
e
7080
3
4
5
ty R
ate
pef R
epro
due
(WR
A)
405060
PR (%
)
0
1
2
Fert
ilit
Wom
an o
fA
ge
0102030 C
P
01991 1996 2001 2006 2009 2015
W 0
Total Fertility Rate Contraceptive Prevalence Rate (CPR)
Slide 4
Source: NFHS 1991, 1996, NDHS 2001, 2006, MMMS 2009
However, access to services is unequal…
• In 2005 19% of births were assisted by skilled birth attendants (NDHS 2006 – now estimated at 30%) but:
– Women educated to secondary level are 8x as likely to benefit fromWomen educated to secondary level are 8x as likely to benefit from an attended delivery as women with no education
– The richest fifth of women are 12x as likely to benefit from an attended delivery as the poorest fifthattended delivery as the poorest fifth
– Town and city dwellers are 3.5x as likely to benefit from an attended delivery as rural dwellers
– Central hill dwellers are 2 5x as likely to benefit from an attended– Central hill dwellers are 2.5x as likely to benefit from an attended delivery as far western mountain dwellers
• 28% of women attend 4 or more antenatal care visits (NDHS 2006) b t t 2 hi h i b th i l
Slide 5
2006), but rates are 2x as high in urban than in rural areas.
… and outcomes are also unequal
• Maternal mortality is 2x to 3x higher among Muslims, Terai/ Madhesis and Dalits (marginalised groups) than Brahmin/ Chhetris and Newars (advantaged caste groups) (MMMS 2009).
• Fertility rates in urban areas are a third lower than rural;• Fertility rates in urban areas are a third lower than rural; education to secondary level is associated with a 50% drop in a woman’s fertility rate; and the richest fifth have a fertility
t th fifth l th th t fifth (NDHS 2006)rate three fifths lower than the poorest fifth (NDHS 2006).• Unmet need for family planning is the reverse (NDHS 2006).
Slide 6
DFID Nepal – Our Operational Plan 2011-2015
B d tBudget: - approx £60m per year (first two years)- over £100m per year (in the next two years)p y ( y )
Vision:Plan focuses on a twin track approach of supporting the development of a lasting political settlement and tackling extreme poverty. Delivery of broad based poverty reduction even under increasing fragility.In all areas there will be specific measures to ensure interventions
Slide 7
In all areas there will be specific measures to ensure interventions to improve the lives of girls and women.
The Operation Plan Pillars
Wealth Creation Governance and SecuritySecurity
Climate ChangeClimate Change and Disaster
Risk Reduction
Direct Delivery of the MDGs
Slide 8
Programme Priorities in Each Pillar
Wealth Creation
•Rural infrastructure•Market Development •Access to Finance•SkillsSkills•Macro-economic reform
Climate Change • ForestryClimate Change and
Disaster Risk Reduction
• Climate Change• Disaster Risk Reduction
Slide 9
Governance •Peace processand
Security
Peace process•Local development •Security and justice•Gender and Inclusion (GBV)PFM & A ti ti•PFM & Anti-corruption
Di t D liDirect Delivery of the MDGs •Health, HIV & Nutrition
•Education•Water and Sanitation
Slide 10
Key results targets: 2011-2015
We will:
• get 34,000 more children into primary educationget 34,000 more children into primary education• ensure 22,400 children complete primary education• provide financial services, ie savings, credit, insurance to 1000,000
people• build & maintain 4,232 km roads.• ensure 110,000 more people will have access to toilets by 2015• enable one million adults to hold decision makers to account
support free and fair elections for 18m people• support free and fair elections for 18m people. • give 22,000 women access to informal justice (paralegals)• help 25,000 women have safe childbirth
Slide 11
DFID Nepal – Support to health (1)• Our approach has evolved over time:Our approach has evolved over time:
– During the civil war (1997-2004), project approach;– Early days of the peace settlement and increasing stability in
Government (2004-2010), mixture of project and programme ( ), p j p gapproach;
– Currently, programme approach (2010-2015), i.e. working closely with Government and providing direct funding to the health system.
• Priority areas:– Reproductive and Maternal Health NutritionReproductive and Maternal Health, Nutrition– Addressing inequalities (gender and social group) and improved
governance of the health system (efficient procurement, better public financial management and anti-corruption)
Slide 12
g )
DFID Nepal – Support to health (2)
1997 2004: Funding: £25 7 million• 1997-2004: Funding: £25.7 million– National Safer Motherhood Project; District Health Strengthening
Project, Reproductive Health Programme; Support to National TB programme Polio Eradication Programmeprogramme, Polio Eradication Programme
• 2004-2010: Funding: £71.5 million (including HIV/AIDS)– Support to Nepal Health Sector Programme (Sector Budget
Support and Technical Assistance)Support and Technical Assistance)– Support to Safer Motherhood Programme (Technical/Financial
Assistance)• 2010 2015: Funding: £77 million• 2010-2015: Funding: £77 million
– Support to Nepal Health Sector Programme 2 (Sector Budget Support, 6% of the sector budget, and Technical Assistance)Additional programmes in HIV/AIDS and family planning (FP)
Slide 13
– Additional programmes in HIV/AIDS and family planning (FP) proposed
DFID Nepal – key reproductive and maternal health achievements
• Safe Abortion Programme – since Mar 2004– Safe abortion legalised in 2002– Safe services available since 2004 – covers all 75 districts now– >300k women utilized service until Jun 2009; Quality high
• Safe Delivery Incentive Programme (initially Maternity y g ( y yIncentive Scheme) – since Jul 2005
– Financial incentives to mothers and service providers– Free delivery care in low human development index (HDI) districts y p ( )
only• Aama Programme – since Jan 2009
– Financial incentives to mothers and service providers
Slide 14
Financial incentives to mothers and service providers– Free delivery care and reimbursement of delivery costs to facility
The innovative cash incentive scheme and free delivery has yielded results… y y
A h b l l ti f A SSMP J 2010
Slide 15
- As shown by early evaluation of Aama programme, SSMP Jun 2010
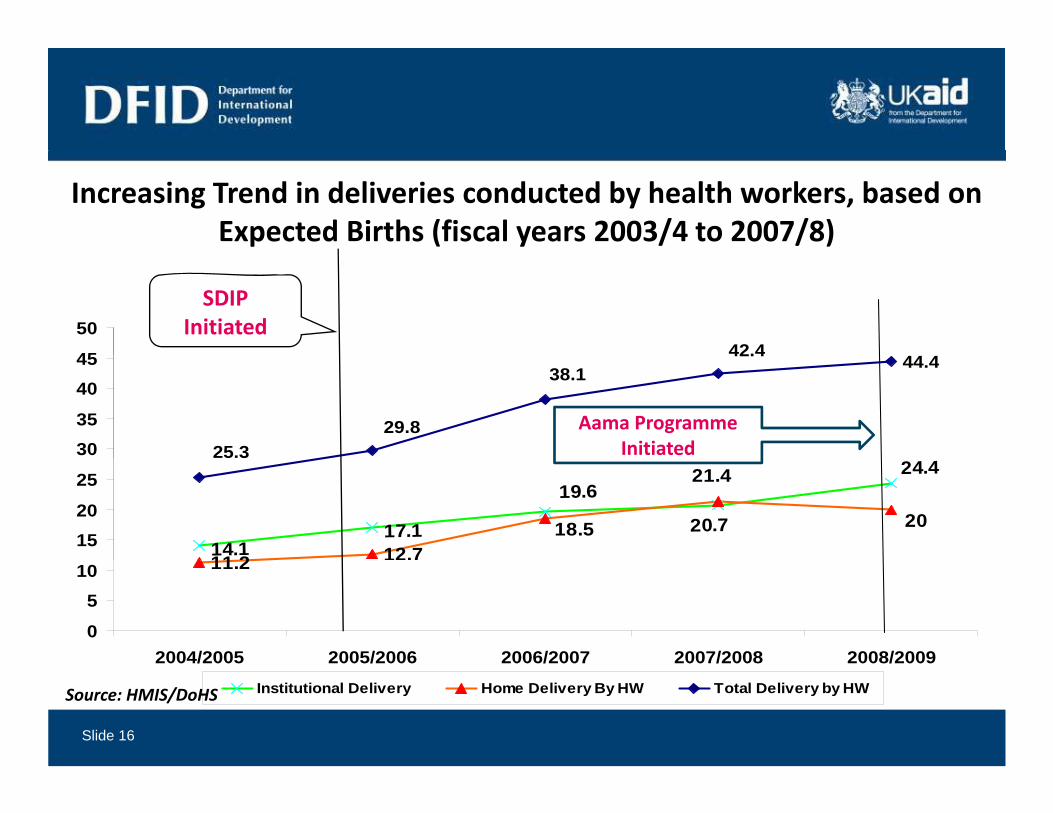
Increasing Trend in deliveries conducted by health workers, based on Expected Births (fiscal years 2003/4 to 2007/8)
44 442.445
50SDIP
Initiated44.4
25.329.8
38.142.4
3035
4045
Aama Programme Initiated
14.117.1
11 2 12.7
19.6
20.7
24.4
18.5
21.4
20
5 3
1520
25
11.2
0
510
2004/2005 2005/2006 2006/2007 2007/2008 2008/2009
Slide 16
2004/2005 2005/2006 2006/2007 2007/2008 2008/2009Institutional Delivery Home Delivery By HW Total Delivery by HWSource: HMIS/DoHS
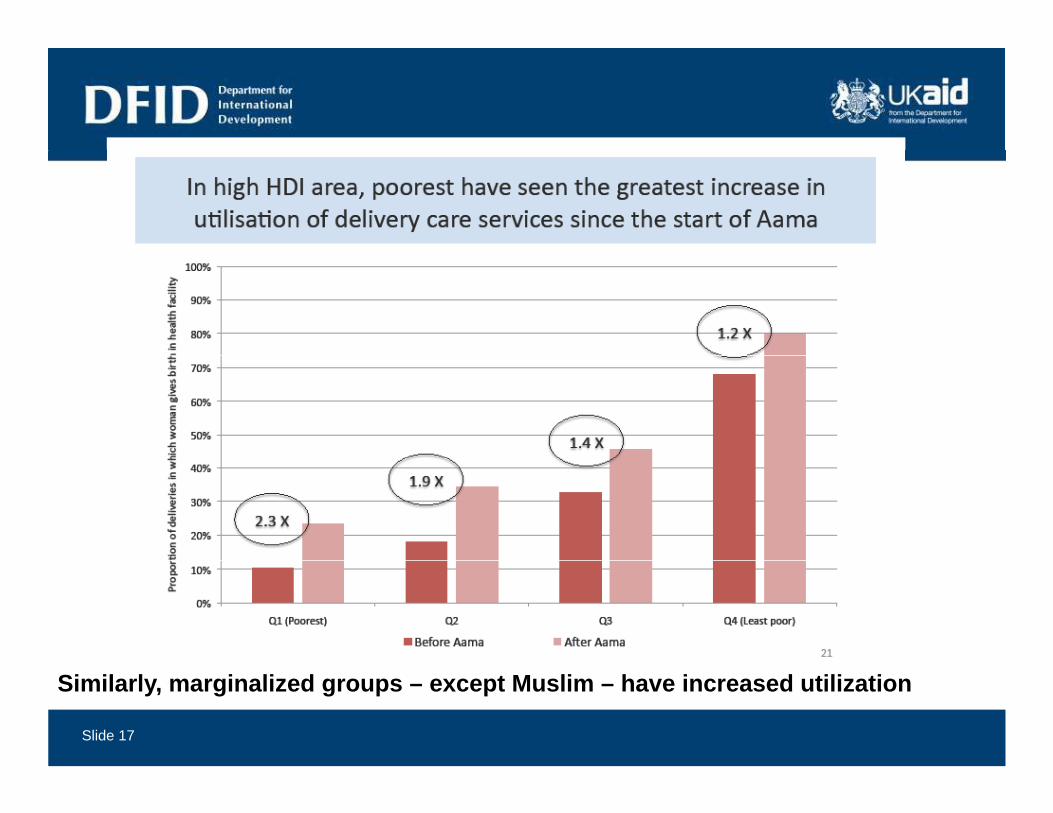
Slide 17
Similarly, marginalized groups – except Muslim – have increased utilization
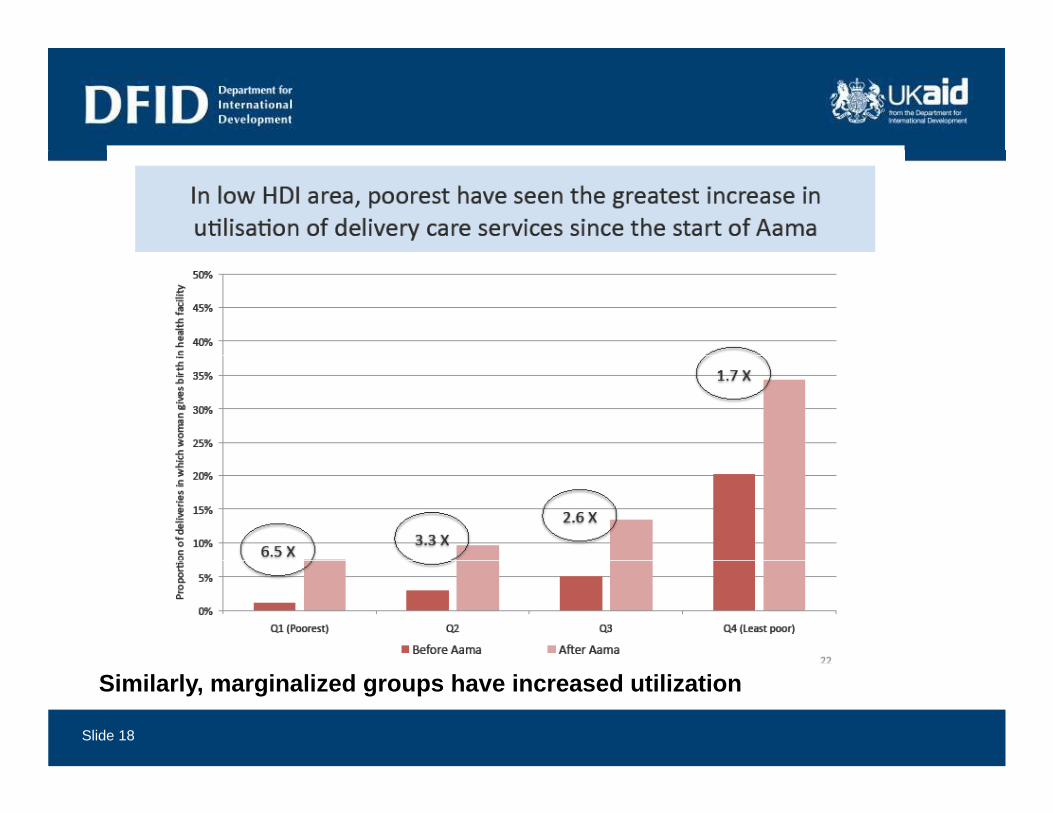
Slide 18
Similarly, marginalized groups have increased utilization
Future challenges• Closing the equity gap by stratifying interventions more intelligently
(eg, currently Aama payment higher for mountain dwellers)• Ensuring right people are in the right place at the right time, with
adequate tools human resource drugs and logistics publicadequate tools – human resource, drugs and logistics, public financial management, governance
• Harnessing the significant capacity of private providers and improving regulationimproving regulation
• Safer motherhood: Improving quality of care, transport and referral options, especially in remote areas
• FP/reproductive health: FP method mix, advising those seeking p , g gsafe abortion about FP methods
• DFID contributed to Nepal’s impressive health outcomes –
Slide 19
achievement of MDG 4 & 5 is likely – however challenges remain.
Leading the UK government’s fight against world poverty
LONDON1 Palace Street
Tel: +44 (0) 20 7023 0000
1 Palace StreetLondonSW1E 5HE
EAST KILBRIDE Tel: +44 (0) 20 7023 0000Fax: +44 (0) 20 7023 0016Website: www.dfid.gov.ukE-mail: [email protected]
EAST KILBRIDEAbercrombie HouseEaglesham RoadEast Kilbride
Public Enquiry Point: 0845 300 4100If calling from abroad: +44 1355 84 3132
GlasgowG75 8EA
Slide 20





























