-
8/12/2019 Dexamethasone for the Prevention of Recurrent
Laryngeal Nerve Palsy After Thyroid Surgery
1/8
ORIGINAL ARTICLE
Dexamethasone for the Prevention of RecurrentLaryngeal Nerve
Palsy and Other ComplicationsAfter Thyroid Surgery
A Randomized Double-Blind Placebo-Controlled Trial
Mario Schietroma, MD; Emanuela Marina Cecilia, MD; Francesco
Carlei, MD; Federico Sista, MD;Giuseppe De Santis, MD; Laura
Lancione, MD; Gianfranco Amicucci, MD
Importance : Recurrent laryngealnerve dysfunction
andhypoparathyroidism are well-recognized, importantcom-plications
of thyroid surgery. The duration of convales-cence after
noncomplicated thyroid operation may de-pend on several factors, of
which pain andfatigue are themost important. Nausea and vomiting
occur mainly on
theday of operation. Glucocorticoids arewell known fortheir
analgesic , ant i- inf lammatory, immune-modulating andantiemetic
effects. However, there is littleinformation in the literature on
theuse of steroids in thy-roid surgery, andthe information that is
available is con-flicting.
Objective : To investigate whether preoperative dexa-methasone
could improve surgical outcome in patientsundergoing thyroid
surgery.
Design : A randomized double-blind placebo-controlled trial. A
30-day follow-up for morbidity wasperformed in all cases.
Setting : All patients were hospitalized in a public
hos-pital.
Participants : From June 2008 through August 2011,328 patients
were randomized to receive either intrave-nous dexamethasone, 8
mg,administered90 minutesbe-fore skin incision, or saline solution
(placebo).
Interventions : Intravenous dexamethasone, 8 mg.
Main Outcomes and Measures : The primary endpoints were
temporary or permanent recurrent laryn-geal nerve palsy. Transient
and definitive hypoparathy-
roidism, pain and fatigue scores, nausea, and the num-ber of
vomiting episodes were also registered.Preoperativelyand at several
timesduringthe first 24post-operative hours, we measured C-reactive
protein, inter-leukin 6, and interleukin 1 levels.
Results : In the dexamethasone group, the rate of tem-porary
recurrent laryngeal nerve palsy (4.9%) was sig-nificantly lower
compared with theplacebo group (8.4%)(P=.04). Also, postoperative
transient biochemical hy-poparathyroidism occurred more frequently
in the pla-cebo group (37.0%) than in the dexamethasone
group(12.8%). Dexamethasone use significantly reduced
post-operative levels of C-reactive protein ( P=.01) and
inter-leukin6 andinterleukin1 (P=.02), fatigue ( P=.01),andoverall
pain during the first 24 postoperative hours(P=.04), as well as the
total analgesic (ketorolac tro-methamine) requirement ( P=.04).
Dexamethasone usealso reduced nausea and vomiting on the day of
opera-tion ( P=.045).
Conclusions and Relevance : Preoperative adminis-tration of
dexamethasone, 8 mg, reduced postoperativetemporary recurrent
laryngeal nerve palsy and hypo-parathyroidism rates and reduced
pain, fatigue, nausea,and vomitingafter thyroid surgery. However,
these datarequire further analysis in randomized
prospectivestudies.
Trial Registration : clinicaltrials.gov
Identifier:NCT01690806
JAMA Otolaryngol Head Neck Surg. 2013;139(5):471-478
T OTAL THYROIDECTOMY OR thyroidlobectomyhasbeenacceptedas
thecurrent sur-gical therapyforbenignandmalignant thyroidal
disor-ders, 1-5 but extensive resection might in-crease the risk of
postoperative complica-tions. 6,7 Recurrent laryngeal nerve
(RLN)dysfunction and hypoparathyroidism are
well-recognized, important complica-tions of thyroid surgery. 8
Complicationrates of thyroidectomy have a varyingrangefor
bothRLNinjury(0% to14%)andpermanent hypoparathyroidism (1% to11%).
9 Paralysisof vocal cords maycauseserious phonatory, respiratory,
and psy-chological problemsthat limit workingca-pacities and
quality of life of the pa-
Author Affiliations:Department of Surgery,University of LAquila,
Abruzzo,Italy.
JAMA OTOLARYNGOL HEAD NECK SURG/ VOL 139 (NO. 5), MAY 2013
WWW.JAMAOTO.COM471
2013 American Medical Association. All rights reserved.
wnloaded From: http://archotol.jamanetwork.com/ on
06/15/2013
-
8/12/2019 Dexamethasone for the Prevention of Recurrent
Laryngeal Nerve Palsy After Thyroid Surgery
2/8
tients. 5 Complications especially related to the RLN
andparathyroid glands can be prevented with the appropri-ate
surgical technique during total thyroidectomy.
The surgical technique is one of the important fac-torsaffecting
the outcome of thyroidectomy. 7 In thepast,most surgeons avoided
dissections in close proximity tothe RLN to prevent its injury.
Recently, endocrine sur-geons consider this unacceptable. The
identification andpreservation of the RLN are essential to avoid
its in-
jury.10
Meticulous hemostasis and delicate technique arerequired to
prevent nerve injury. Once found, the nerve,with all the identified
branches, must be followed supe-riorly through the entire course
until it enters the lar-ynx. 11 This surgical technique, which
requires more dis-sections, mayharm the RLNand parathyroid glands.
7 Infact, recurrent laryngeal nerve palsy (RLNP) may
resultfromdirect mechanicaldamagewithout disruption.Thisdisparity
between anatomic neural integrity and actualRLN function probably
results from trauma to the in-tact nerve. Nerve manipulation during
thyroid surgerymaycause neural edema andconsequent dysfunction,
re-sulting in anything from neurapraxia to axonotmesis.
The duration of convalescence after noncomplicated
thyroid operationmay dependonseveral factors, ofwhichpain,
fatigue, and sociocultural factors are the most im-portant. Pain
and fatigue are most intense on the day of operation and the
following day. Nausea and vomitingoccur mainlyon the day
ofoperation and only rarelycon-tribute to prolonged
convalescence.
Glucocorticoids are well known for their
analgesic,anti-inflammatory, immune-modulating, and anti-emetic
effects, although the mechanism by which glu-cocorticoidsexert
their actionis yet tobeclarified. 12 Thereare both experimental and
clinical data supporting thenotion that the steroid administration
may prevent or re-duce neural edema. 13-15 Patientswith
idiopathicfacialpalsyhave shown improved facial nerve function
after an em-
pirical course of corticosteroids.16,17
Several random-ized clinical trials in many different major
andminor sur-gical procedures have been conducted to examine
theeffects of a perioperative single-dose glucocorticoid
ad-ministration on surgical outcome. 18 The overall resultson
postoperative outcome have either been positive andin favor of
glucocorticoid use, with postoperative nau-sea andvomiting and pain
outcome parameters most sig-nificantly
improved,orshownnodifferencebetween studygroups. 18-21
Regardingtheuseof steroids in thyroid surgery, thereis little
information in the literature, and the informa-tion that is
available is conflicting. In their book, Lore etal22 have mentioned
the benefit of intraoperative ste-
roids in thyroid surgery. Wang et al23
reported a studythat found no statistically significant benefit.
We undertook the present studyto investigatewhether
preoperative use of dexamethasone could improve surgi-caloutcome
in patients undergoing either total thyroidec-tomy or total
lobectomywith routine identificationofRLN.Our primary end points
were to evaluate the role of dexa-methasone in preventing or
treating postoperative RLNPand in preventing hypoparathyroidism. We
also investi-gated the effects of dexamethasone on pain, fatigue,
nau-sea, vomiting, and the duration of convalescence.
METHODS
From June 2008 through August 2011, 336 patients were
ran-domized. Exclusion criteria were American Society of
Anesthe-siologists (ASA) physical class III or IV, age older than
75 years,and pregnancy. Patients were not included if they had
chronicpain due to a disease other than thyroid disease; if they
had anysigns of renal, hepatic, and immunological disease; if they
re-ceivedopioidsor tranquilizers( 1 week of treatmentbeforethy-
roidectomy); if they spoke only a foreign language or had
men-tal disorders; or if they had a history of alcohol or drug
abuse.Finally,because the developmentof
surgicalcomplicationsmightinfluence thechosenoutcome parameters, we
decided before thestart of the study to exclude these patients, and
the results wereanalyzed according to the protocol. The study
protocol was ap-proved by the ethical committee of the Faculty of
Medicine of the University of L Aquila, and all patients gave their
written in-formed consent to participate in the study.
Patients were followed from the day before the operationand
daily during the first postoperative week. The day of op-eration
was defined as day 0 and the first day after operationas day 1, the
second day after as day 2, and so on.
A 30-dayfollow-up formorbidity wasperformed in allcases.The
present study included several contacts between patientsand study
observers during the first postoperative 24-hour pe-riod.
Total thyroidectomy or lobectomywas performedby a tech-nique of
capsular dissection. The delicate technique was per-formed by
seeking, identifying, and exposing the RLN with allbranches and
following its coursewith careuntil it enteredlar-ynx. When
dissection proceeded to the ligament of Berry area,RLN was
identified where it coursed through the ligament orclose to it.
Wherea large thyroidmassor substernal goiter wasencountered, RLN
was identified and traced from the recur-rent nerve triangle, as
advocated by Lore .24 However, specialcare wasnot given to identify
superior laryngeal nerves. All theparathyroid glands were
identified, if possible.
Allpatients were operated on by 2 surgeons (M.S. and G.A.).All
patients received preoperative and postoperative flexible
la-ryngoscopic examinationsof thevocalcords. If vocal cord palsywas
identified, initial follow-up examinations were performedweekly and
then every 3 to 4 weeks thereafter until recovery;the dysfunction
was considered permanent if it persisted after6 months. Patients
were excluded from the study if they hadpreoperative RLNP or nerves
encased by cancer, in whichcasethe nerves were intentionally
removed.Postoperatively total se-rum calcium concentrations were
obtained at 24, 48, and 72hours (also at 96 and 120 hours in
patients with hypocalce-mia). Hypocalcemia was defined as at least
1 serum calciummeasurement below 8.1 mg/dL (reference range,
8.1-10.4 mg/ dL) (to convert to millimoles per liter, multiply by
0.25). Oralcalcium supplementation with or without vitamin D
analoguewas given if patients developed symptomatic hypocalcemia
orwhen the serum calcium level was less than 8.1 mg/dL. An
in-travenous calcium gluconate, 10%, infusion was administered
for significant hypocalcemic symptoms or when oral therapyproved
inefficacious. Patients were discharged when the se-rum calcium
level was higher than 8.1 mg/dL. Hypocalcemiawas considered
permanent if it persisted after 6 months.
All patients received general anesthesia similarly.
Preanes-thesia wasaccomplished withatropinesulfate,0.01mg/kg,
pluspromethazine hydrochloride, 0.5 mg/kg; induction with so-dium
thiopental, 5 mg/kg, and atracurium besylate, 0.5 mg/ kg; and
tracheal intubation and assisted ventilation with ni-trogen dioxide
and oxygen in a 2:1 ratio. After intubation,anesthesia
wasmaintained with oxygenin air, sevoflurane,andremifentanil
hydrochloride, 0.25 g/kg/min.
JAMA OTOLARYNGOL HEAD NECK SURG/ VOL 139 (NO. 5), MAY 2013
WWW.JAMAOTO.COM472
2013 American Medical Association. All rights reserved.
wnloaded From: http://archotol.jamanetwork.com/ on
06/15/2013
-
8/12/2019 Dexamethasone for the Prevention of Recurrent
Laryngeal Nerve Palsy After Thyroid Surgery
3/8
Amoxicillin-clavulanic acid, 2200 mg, was given at the
be-ginning of surgery. In the postoperative anesthesia care
unit(PACU), vital signs (blood pressure, pulse, respiration,
pulseoximetry, and adequate answering) were monitored every
15minutes by a consultant. Patients were discharged from thePACU
when vital signs were normalized. We used a prophy-lactic
multimodal analgesic technique for treatment of post-operative
pain. Thus, patients received incisional local anes-thetics using15
mL(75mg)of bupivacainehydrochloride, 0.5%.Intravenous ketorolac
tromethamine, 30 mg, was adminis-
tered every 6 hours on the first day after operation, and
after-wards,on demand. Intravenous ondansetron hydrochloride,
4mg,wasadministered forantiemetic treatment on demand. Painwas
registered preoperatively, several times during the first
24postoperative hours, and daily during the first
postoperativeweek. Pain was measured on a visual analog scale (VAS)
withend points labeled no pain, and worst possible pain, andona
verbal rating scale(VRS)(0=no pain; 1= lightpain; 2= mod-erate
pain; and 3=severe pain). Moreover, the pain was re-corded at rest
(supine position) and during mobilization (su-pine to sitting
position) preoperatively and 1, 2, 3, 6, and 24hours after
operation (ie, investigator-recorded instant painscores). In
addition, the patients themselves registered the pain(VAS and VRS)
(self-reported registration). Self-reported reg-istrations were
completed the day before operation (at 8 PM),on the day of
operation (at 6 hours preoperatively and then at6 hours
postoperatively, both the investigator-recorded in-stantpain score
andthe patients self-registered pain score wererecorded), and daily
until postoperative day 7 at 8 PM. At thesame intervals, patients
also rated fatigue on a 10-point ordi-nal scale (1=fit;
10=fatigued). 25 Patients were instructed thatself-reported
registrations should coverpainand fatigue withinthe period since
the last measurements.
Patients evaluated nausea and vomiting over 2 postopera-tive
intervals: 0 through 6 hours and 6 through 24 hours afteroperation.
26 Nausea was rated on a VRS (0=no nausea; 1= mildnausea;
2=moderate nausea; and 3=severe nausea), and thenumber of vomiting
episodes were registered (0=no episodes[none]; 1=1 episode [mild];
2 =2 or 3 episodes [moderate];3= 3 episodes [severe]).
Serialvenous blood samples were taken at 0, 30,60, 90, 120,and
180 minutes, at 12 and 24 hours, and then dailyuntil post-operative
day 6. The plasma concentration of C-reactive pro-tein (CRP) was
measured using a competitive CRP enzyme-linked immunosorbent assay
(ELISA) kit.
Serum concentration of interleukin 1 (IL-1 ) and interleu-kin 6
(IL-6) were measured using a quantitative sandwichELISA kit
(R&D System) according to the manufacturers de-scription
(ranges: IL-1 , 3.9-250 pg/mL 1; and IL-6, 3.13-300pg/mL
1).Serumsamples (100 L)were dispensedinto thewellsof 96-well
microtiter plates, which had been coated with therelevant
monoclonal cytokine antibody. After incubation for2 hours at room
temperature, unbound proteins were washedaway fromthe wells, to
which subsequently an enzyme-linkedantibody was added and
directedagainst the relevant cytokinefor another 2 hours at room
temperature. After further rinsing
to remove unbound antibody, a substrate solution was addedto
each well, and the mixture was incubated for 20 minutes at37 C. The
reaction was terminated with the addition of a stopsolution.
Adsorption was determined by using an ELISA platereading at 450 nm.
Serial dilution of the relevant recombinantcytokine provided the
standard curve. Assays were performedon duplicate samples. Samples
were diluted appropriately withthe diluent providedin the kit if
the levels of neat sampleswerebeyond the linear measuring
range.
Patients were randomized by means of a sealed envelopemethod (on
the basis of a block-randomized computer-generated list), and the
randomization code was kept un-
known to any of the investigators until the study was com-plete.
Patients were randomized to receive intravenousdexamethasone, 8 mg
(Decadron; Merck Sharp& Dohme), 90-minutes before skin
incision,or saline placebo. Thedrug or pla-cebo solution was drawn
into a syringe by a nurse not partici-pating in the study and was
delivered to the investigator (M.S.)who was outside the medicine
room and unaware of the con-tent. The saline and dexamethasone
solutions appeared trans-parent and completely identical at the
time the syringes weregiven to the investigator. Thus, the
patients, the anesthesiolo-
gist, the surgeon, and the study observer were all blinded
withrespect to the study group. The study drug was administeredto
the patient within 5 minutes after being drawn into the
sy-ringes.
For statistical analyses, we used the Mann-Whitney, Fried-man,
Fisher exact, 2, Spearman rank correlation coefficientand log-rank
tests whenappropriate. Postoperative 24-hour re-sults were
specifically analyzed for intergroup differences. Inaddition,
postoperative fatigue and pain scores from repeatedassessments at
different time points were added together forintergroup comparison
(added total painscores and added totalfatigue scores).
Nausea and vomiting scores were evaluated separately forthe 0-
through 6-hour period and the 6- through 24-hour pe-riod. From each
period, thehighest severity score andthe high-est incidence of
nausea and vomiting were used as a measureof nauseaand/or vomiting
forthe entire24-hour period. P .05was considered statistically
significant. Data are given as me-dian (range) if not stated
otherwise.
RESULTS
A total of 328 patients were available for analysis(Table 1 ); 8
patients (4 in each treatment group) wereexcluded from the study.
There were 163 patients in thedexamethasone group and 165 in the
placebo group(Table 1).
The overall risk of temporary RLNP was 6.7% (22 of 328) and
permanent RLNP was 1.2% (4 of 328)
(Table 2 ). The risk of temporary and permanent
RLNPinthedexamethasonegroupwas 4.9% (8of163)and 1.2%(2 of 163),
respectively. The risk of temporary and per-manent RLNP in
theplacebo group was 8.4% (14 of 165)and 1.2% (2 of 165),
respectively (Table 2). In the dexa-methasone group, the rate of
temporary RLNP was sig-nificantly lower compared with the placebo
group(Table2) ( P = .04, Mann-Whitney test), whereas the
dif-ference did not reach statistical significancebetween the2
groups for permanent RLNP ( P = .20). Among the 22patients who had
temporary RLNP, the recovery timesranged from7 to 41 days (mean,
24.2 days) and from 18to 72 days (mean, 48.6 days) for patients
with or with-out preoperative dexamethasone, respectively ( P =
.048
Mann-Whitney test). Postoperative transient biochemi-cal
hypoparathyroidism occurred more frequently in theplacebo group
thanin thedexamethasonegroup (Table2).In the dexamethasone group
and placebo group, 21(12.8%)and61 (37%) patients, respectively,
requiredoralcalcium carbonate supplementation postoperatively,
al-though these patients showed no clinical symptoms of
hypocalcemia. This difference was statistically signifi-cant ( P =
.045) (Table2).The lowest serum calcium levelwas 7.2 mg/dL in the
placebo group vs 7.6 mg/dL in thedexamethasone group. Also,
postoperative definitive hy-
JAMA OTOLARYNGOL HEAD NECK SURG/ VOL 139 (NO. 5), MAY 2013
WWW.JAMAOTO.COM473
2013 American Medical Association. All rights reserved.
wnloaded From: http://archotol.jamanetwork.com/ on
06/15/2013
-
8/12/2019 Dexamethasone for the Prevention of Recurrent
Laryngeal Nerve Palsy After Thyroid Surgery
4/8
poparathyroidism occurred more frequently in the pla-
cebo group (4 patients [2.4%]) than in the dexametha-sone group
(3 patients [1.8%]), but this difference wasnot statistically
significant ( P = .97).
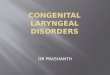
Fatigueincreased significantly inboth groups( P .01,Friedman
test) ( Figure 1 A). In the dexamethasonegroup, fatigue scores were
significantly lower 24 hoursafter operation ( P .01, Mann-Whitney
test) andthroughout the postoperative week compared with theplacebo
group ( P = .01, Friedman test). The added me-dian total
postoperative fatigue scores were 28 (range,10-62) in the
dexamethasone group and 39 (range, 16-64) in the placebo group ( P
= .01, Mann-Whitney test).
In the dexamethasone group, self-reported VASscoresfor pain were
significantly lower on day 1 after operation
compared with the placebo group (Figure 1B) ( P =
.04,Mann-Whitney test). The added median total VAS scoresof pain
(covering the first postoperative week) were 52(range, 0-251)
inthedexamethasonegroupand148 (range,13-406) intheplacebogroup( P
.05,Mann-Whitneytest).In both treatment groups, self-reported
scores of pain in-creased duringthefirstpostoperative week ( P
.01,Fried-man test), but differences between groupsdidnot
changesignificantly duringthetest period( P =
.12,Friedmantest).
Nine patients in the dexamethasone group and 21 intheplacebo
grouprequired 1 ormore supplementarydoses
of ketorolacduring their hospital stay ( P = .10, Fisher ex-act
test),with a significantly lower totaldose in thedexa-methasone
group ( P = .04,Mann-Whitneytest)(Table 1).Spearman correlation
coefficients for the association be-tween the total dose of
postoperative supplementary an-algesic during hospital stay and
pain (first 24-hour pe-riod) were 0.53 ( P = .01) and 0.58 ( P =
.01) for thedexamethasone and placebo groups, respectively.
Afterhospitaldischarge, 2 patients in thedexamethasone group
and 9 in the placebo group required supplementary an-algesic (in
total, analgesics were taken 18 times by11dif-ferent patients [ P =
.08, Fisher exact test]).
During the first 6 postoperative hours, the incidenceand
severity of nausea wassignificantly lower ( P = .045,
2 test and Mann-Whitney test) in the dexamethasonegroup,
andvomiting wassignificantly reduced during theentire 0 through
24-hour period compared with pla-cebo( P = .045, 2 test
andMann-Whitney test).Eight pa-tients in the dexamethasone group vs
21 in the placebogroup received intravenous ondansetron for
antiemetictreatment once or multiple times during their
hospitalstay (P = .11, Fisher exact test) (Table 1).
SerumCRPlevel increasedsignificantly in both treat-
ment groups during the study period ( P = .01, Fried-man test),
but the increase was significantly higher in theplacebo group ( P =
.01, Friedman test) (Figure 1C).
Before the operation, serum IL-1 or IL-6 levelswerenot
significantlydifferent between the2 groups. Figure 2shows
thechronological changes in serumIL-1 andIL-6levelsafter surgery.
In theplacebo group, theserumIL-1and IL-6 levelsbegan to
significantly increase as early as1 hour from thebeginning of
operation, revealinga peakat the sixth hour (approximately 4 hours
after opera-tion) and, thereafter, declining to preoperative levels
by6 days. However, in the dexamethasone group, the in-crease in the
serum IL-1 and IL-6 levels was delayedand the peak values were
significantly lower in the pla-
cebo group ( P .05, Friedman test).Noapparent signs
ofadverseeffectsof thestudy drugswere observed. Four patients in
each group were ex-cluded from the study. In the dexamethasone
group, 2patients had preoperative RLNP and 2 patients devel-oped a
wound infection. In the placebo group, 2 pa-tients had the RLN
encased by cancer and 2 patients de-veloped a wound infection.
Thus, 4 patients (2 from eachstudy group) developed postoperative
wound infec-tions.
DISCUSSION
The identification, careful exposure, and preservation of the
RLN throughout its course are important to preventnerve injury. 11
Theapproach for the identificationof theRLN during surgery on the
thyroid gland was describedin some previousstudies. 11,27,28
Although Bergamaschi etal29 reported that the RLN identification
failed to reduceinjury rate, there are many studies demonstrating a
sig-nificant decrease in the rate of RLN injury
maintainedbytheidentification of thenerve. 5-7,27,30
WagnerandSeiler 7reported that in total thyroidectomy the permanent
in- jury rate significantly increased from 3.8% to 7% when
Table 1. Characteristics of Patients in the Dexamethasoneand
Placebo Groups
Characteristic
DexamethasoneGroup
(n = 163)
PlaceboGroup
(n = 165)
Sex, No.Male 64 66Female 99 99
Age, mean (range), y 49 (28-67) 46 (25-66)Thyroid disease, No.
(%)MNG 99 (10.7) 102 (61.8)Toxic MNG 25 (15.3) 24 (14.5)Graves
disease 16 (9.8) 16 (9.6)Papillary carcinoma 12 (7.3) 13
(7.8)Follicular carcinoma 5 (3) 5 (3)Recurrent MNG 6 (3.6) 5
(3)
Types of thyroid surgeryTotal thyroidectomy 125 (76.6) 128
(77.5)Lobectomy 38 (23.3) 37 (22.4)
ASAI 106 104II 57 61
Duration of surgery, mean(range), min
57 (33-102) 56 (35-98)
Total thyroidectomy 71 (50-102) 69 (51-98)Lobectomy 38 (33-61)
36 (35-58)
Stay in hospital, d 2 2Patients requiring ketorolac
tromethamine, No.9a,b 21a
Patients requiring ondansetron,No.
8c 21c
Abbreviations: ASA, American Society of Anesthesiologists;
MNG,multinodular goiter.
aP = .10, Fisher exact test.bThere was a significantly lower
total dose in the dexamethasone group
(P = .04, Mann-Whitney test).cP = .11, Fisher exact test.
JAMA OTOLARYNGOL HEAD NECK SURG/ VOL 139 (NO. 5), MAY 2013
WWW.JAMAOTO.COM474
2013 American Medical Association. All rights reserved.
wnloaded From: http://archotol.jamanetwork.com/ on
06/15/2013
-
8/12/2019 Dexamethasone for the Prevention of Recurrent
Laryngeal Nerve Palsy After Thyroid Surgery
5/8
the nerve wasnot identified. Ma ttiget al 27 demonstrated
that routine preparation of the RLN decreased the per-manent
injury rate from 5.99% to 0.88%.Empirically, some surgeons use
steroids during thy-
roid operations inanattempt to reducepostoperative neu-ral edema
resulting from inevitable nerve manipulationduring identification
of RLN, as well as to promote re-covery of nerve function when
nerve paralysis occurs.However, there have only been few published
data con-cerning the efficacyof preoperativeor intraoperative
ste-roid use in the management or prevention of nerve dys-function
resulting from operation. Wang et al 23 used a
single intravenous dose of intraoperative corticoste-
roids (100-mg hydrocortisone) and concluded that in-traoperative
steroids didnot produce benefit in terms of reducing postoperative
temporary and permanentRLNP rates, but it did shorten the recovery
time for pa-tients with temporary RLNP. This study was prospec-tive
but not randomized. On the contrary, Lore et al22said that the rate
of temporary RLNP can be reducedfrom 9% to 2.6% with the use of
preoperative or/and in-traoperative steroids. In addition, the use
of steroids re-duces the longest duration of temporary vocal cord
pa-ralysis from 9 to 2 months.
Table 2. Recurrent Laryngeal Nerve Palsy and
Hypoparathyroidism
Variable
Patients, No. (%)
P ValueDexamethasone Group
(n = 163)Placebo Group
(n = 165)Total
(n = 328)
Recurrent laryngeal nerve palsyTransient 8 (4.9) 14 (8.4) 22
(6.7) .04Permanent 2 (1.2) 2 (1.2) 4 (1.2) .20
Hypoparathyroidism
Transient 21 (12.8) 61 (37.0) 82 (25.0) .045Permanent 3 (1.8) 4
(2.4) 7 (2.1) .97
0Preop
10
9
1 0
- P o
i n t
O r d
i n a l
S c a
l e
Days After Operation
3
Placebo
Placebo
Placebo
Dexamethasone
Dexamethasone
Dexamethasone
4
5
6
7
8
2
1
A
1
2 3 4 5 6 7
0Preop
9
P l a s m a
C R P L e v e l
, m g
/ d L
Time After Beginning the Operation
3
4
5
6
7
8
2
1
C
1 h 2 h 3 h 4 h 5 h 6 h 24 h 2 d 3 d 6 d 12 d
0Preop
35
V i s u a l
A n a l o g u e
S c a
l e
Days After Operation
15
20
25
30
10
5
B
1 2 3 4 5 6 7
Figure 1. Changes in fatigue and overall pain scores and serum
C-reactive protein (CRP) levels. A, Changes in fatigue scores
(10-point ordinal scale: 1 = fit,4 = slightly tired, 7 = tired, and
10 = fatigued) in patients receiving placebo or dexamethasone.
Patients who received dexamethasone were significantly lessfatigued
on postoperative day 1 (* P .01). B, Changes in overall pain scores
(visual analog scale) in patients receiving placebo or
dexamethasone. Patients whoreceived dexamethasone experienced
significantly less overall pain on postoperative day 1(* P .05). C,
Changes in serum CRP levels in patients receivingplacebo or
dexamethasone. The increase in CRP level was significantly higher
in the placebo group (* P = .01). Preop indicates preoperation. For
CRP, to convertmilligrams per deciliter to nanomoles per liter,
multiply by 95.24.
JAMA OTOLARYNGOL HEAD NECK SURG/ VOL 139 (NO. 5), MAY 2013
WWW.JAMAOTO.COM475
2013 American Medical Association. All rights reserved.
wnloaded From: http://archotol.jamanetwork.com/ on
06/15/2013
-
8/12/2019 Dexamethasone for the Prevention of Recurrent
Laryngeal Nerve Palsy After Thyroid Surgery
6/8
-
8/12/2019 Dexamethasone for the Prevention of Recurrent
Laryngeal Nerve Palsy After Thyroid Surgery
7/8
Kehlet 18 provide a comprehensive review of these trialsand
endorse the use of a single-dose preoperative ste-roid. As an
immune modulation strategy, such therapyappears to shift the
balance of inflammation in favor of anti-inflammatorymediators in a
variety of surgical pro-cedures. Some aspects of cardiac 41 and
pulmonary func-tion 42 have been shown to improve, but usually in
smallstudies with insufficient statistical power to detect
reli-able clinical differences. Trials aimed at evaluating ad-
verse effects of preoperativesingle-dose steroids have alsobeen
inconclusive becauseof size and design. When con-sidered together,
however, it appears that this therapy(dexamethasone, 8 mg) is safe;
it particularly does notincrease complications one might expect,
such as infec-tions and impaired wound healing. A recent
meta-analysis 43 concluded thatperioperative administrationof
high-dosemethylprednisolone (30-35mg/kg), a dose ap-proximately 50
times thedose used in our study, was notassociated with significant
adverse effects. In our study,we found no apparent adverse effects
or complicationscaused by dexamethasone treatment because only 2
pa-tients in each surgical group developed a postoperativewound
infection. It also appears that the timing of ste-
roid administration is important (1-2 hours preopera-tively) if
excess inflammatoryactivationsand relatedpost-operative morbidity
are to be attenuated.
The analgesic effect of glucocorticoid is provided byinhibiting
phospholipase enzymes and, accordingly,blocking both the
cyclooxygenase and the lipoxygenasepathway in the inflammatory
chain reaction, 12 as well assuppressing tissuelevelsofbradykinin
44 andreleasing neu-ropeptides from nerve endings, 45 both of which
may en-hance nociception in inflamed tissue and the surgicalwound.
In the present study, dexamethasone reducedpain. Our results are in
accordance with the analgesiceffect of dexamethasone, 8 mg, in
patients undergoinggynecologic operation 46 and dental extractions.
47 Inare-
cent review18
regardingtheeffects of perioperative single-dose glucocorticoid
administration, randomized trialsfrom several minor and major
surgical procedures wereanalyzed. 18 The authors concluded that
glucocorticoidadministration in major abdominal surgery probably
hasno or limited analgesic effect, but may have an analgesiceffect
in minor surgical procedures, and that glucocor-ticoid
administration definitely has an analgesic effect indental surgery.
18
The incidence andseverityof postoperative nausea andvomiting
have been significantly decreased by preopera-tive single-dose
steroid administration in several stud-ies.19 This
canbeexplainedbya central antiemetic mecha-nism involving
endogenous prostaglandin and opioid
production.19
In a recent meta-analysis of 17 randomizedclinical trials, a
single dose of dexamethasone in combi-nation with 5-HT 3 receptor
antagonists significantly re-duced postoperative nauseaand
vomitingcompared withplacebo, but the optimal dose of this
combination needstobe identified. 19 Furthermore, therole
ofconcomitant useof 5-HT3 receptor antagonist remains to be
clarified. 20,48-50
In the present study, intravenous dexamethasone wasadministered
90 minutes before skin incision. Glucocor-ticoidsbindto the
intracellular glucocorticoid receptor,andeffects arepredominantly
mediated throughanalteredpro-
tein synthesis via gene transcription. 51 Therefore, the on-set
of biological action is generally 1 to 2 hours, depend-ing on the
route of administration. 12 Unfortunately,
moststudieshaveadministeredglucocorticoids immediatelybe-fore
induction of anesthesia, 18 includingtheother trials
inpatientsundergoing laparoscopiccholecystectomy. 48-50 Be-cause
activations of the early mediators of the metabolicresponse to
surgery occur immediately after the surgicalincision,administration
ofglucocorticoids1 to2 hourspre-
operatively may be important to achieve the full postop-erative
benefit of the treatment. 52In conclusion, we demonstrated that a
single dose of
preoperative dexamethasone (administered 90 minutesbefore skin
incision) was effective in preventing tempo-rary RLNP during
thyroid operation and in reducing theduration of temporary RLNP.
This is especially impor-tant for the patients with locally
advanced cancer, pa-tients with Graves disease, and patients
undergoing re-operation in which the incidence of RLNP may be
tripleor more. 7,53-57 Also postoperative transient
biochemicalhypoparathyroidism occurred less frequently with
pre-operative single-dose dexamethasone.
Moreover, dexamethasone improved surgicaloutcome
after thyroid surgery in terms of significantly less pain,
fa-tigue,nausea, andvomiting, andpatientsresumed their
rec-reationalactivity significantly fastercomparedwith
thepla-cebogroup.Thissimpletherapy,in theabsence
ofincreasedmorbidity from
thesingledoseofsteroids,warrantsbroaderapplication in thyroid
surgery.
Submitted for Publication: April 20, 2012; final revi-sion
received July 17, 2012; acceptedFebruary14, 2013.Correspondence:
Mario Schietroma,MD, Universit de-gli Studi di LAquila, Facolt di
Medicina e Chirurgia,Dipartimento di Scienze Chirurgiche, Presso
OspedaleS. Salvatore, Edificio Delta 6, 67100 Coppito (AQ),
Italy([email protected]).Author Contributions: Dr Schietroma
had full access toall the data in the study and takes
responsibility for theintegrity of the data and the accuracy of the
data analy-sis. Study concept and design: Carlei. Acquisition of
data:Cecilia, Sista, De Santis, and Lancione. Analysis and
in-terpretation of data: Schietroma and Amicucci. Draftingof the
manuscript: Cecilia, Sista, De Santis, and Lanci-one. Critical
revision of the manuscript for important in-tellectual content:
Schietroma, Carlei, and Amicucci. Sta-tistical analysis: De Santis
and Lancione. Administrative,technical, and material support:
Schietroma, Cecilia,Car-lei, Sista, and Amicucci.Conflict of
Interest Disclosures: None reported.
REFERENCES
1. Bron LP, O BrienCJ. Totalthyroidectomy for clinically benign
disease of the thy-roid gland. Br J Surg . 2004;91(5):569-574.
2. Dener C. Complication rates after operations for benign
thyroid disease. Acta Otolaryngol . 2002;122(6):679-683.
3. Erog luA, Unal M, Kocaog lu H. Totalthyroidectomyfor
differentiated thyroid car-cinoma: primary and secondary
operations. Eur J Surg Oncol . 1998;24(4):283-287.
4. RosatoL, AveniaN, Bernante P,et al.Complicationsof thyroid
surgery: analysisof a multicentricstudy on 14,934 patientsoperated
on in Italy over5 years.World J Surg . 2004;28(3):271-276.
JAMA OTOLARYNGOL HEAD NECK SURG/ VOL 139 (NO. 5), MAY 2013
WWW.JAMAOTO.COM477
2013 American Medical Association. All rights reserved.
wnloaded From: http://archotol.jamanetwork.com/ on
06/15/2013
-
8/12/2019 Dexamethasone for the Prevention of Recurrent
Laryngeal Nerve Palsy After Thyroid Surgery
8/8
5. Sturniolo G, D Alia C, Tonante A, Gagliano E, Taranto F, Lo
Schiavo MG. The re-current laryngeal nerve related to thyroid
surgery. Am J Surg . 1999;177(6):485-488.
6. Thomusch O, Sekulla C, Dralle H. Is primary total
thyroidectomy justified in be-nign multinodular goiter? results of
a prospective quality assurance study of 45hospitals offering
different levels of care [in German]. Chirurg .
2003;74(5):437-443.
7. Wagner HE,Seiler C. Recurrentlaryngeal nerve palsy
afterthyroidgland surgery.Br J Surg . 1994;81(2):226-228.
8. McHenry CR. Patient volumes and complications in thyroid
surgery. Br J Surg .2002;89(7):821-823.
9. Harness JK, Fung L, Thompson NW, Burney RE, McLeod MK. Total
thyroidec-tomy: complications and technique. World J Surg .
1986;10(5):781-786.
10. Hisham AN, Lukman MR. Recurrent laryngeal nerve in thyroid
surgery: a criticalappraisal. ANZ J Surg . 2002;72(12):887-889.
11. Ardito G, Revelli L, D Alatri L, Lerro V, Guidi ML, Ardito
F. Revisited anatomy ofthe recurrent laryngeal nerves. Am J Surg .
2004;187(2):249-253.
12. Sapolsky RM, Romero LM, Munck AU. How do glucocorticoids
influence stressresponses? integrating permissive, suppressive,
stimulatory, and preparativeactions. Endocr Rev .
2000;21(1):55-89.
13. Jones KJ, Drengler SM, Oblinger MM. Gonadal steroid
regulation of growth-associated protein GAP-43 mRNA expression in
axotomized hamster facial mo-tor neurons. Neurochem Res .
1997;22(11):1367-1374.
14. Bansberg SF, McCaffrey TV. The effect of systemic
triamcinolone acetonide onnerve repair. Otolaryngol Head Neck Surg
. 1987;96(2):158-164.
15. Lipton R, McCaffrey TV, Ellis J. The beneficial effect of
triamcinolone acetonideon nerve repair with autogenous grafts.
Otolaryngol Head Neck Surg . 1986;94(3):310-315.
16. Stankiewicz JA. A review of the published data on steroids
and idiopathic facialparalysis. Otolaryngol Head Neck Surg .
1987;97(5):481-486.
17. Austin JR, Peskind SP, Austin SG, Rice DH. Idiopathic facial
nerve paralysis: arandomized double blind controlled study of
placebo versus prednisone.Laryngoscope .
1993;103(12):1326-1333.
18. Holte K, Kehlet H. Perioperative
single-doseglucocorticoidadministration:patho-physiologic effects
and clinical implications. J Am Coll Surg .
2002;195(5):694-712.
19. Henzi I, Walder B, Tramr MR. Dexamethasone for the
prevention of postopera-tive nausea and vomiting: a quantitative
systematic review. Anesth Analg . 2000;90(1):186-194.
20. Fujii Y, Saitoh Y, Tanaka H, Toyooka H.
Granisetron/dexamethasone combina-tion for the prevention of
postoperative nausea and vomiting after
laparoscopiccholecystectomy. Eur J Anaesthesiol .
2000;17(1):64-68.
21. Schietroma M, Giuliani M, Zoccali G, et al. How does
dexamethasone influencesurgicaloutcome after
laparoscopicNissenfundoplication? a randomized double-blind
placebo-controlled trial. Updates Surg . 2010;62(1):47-54.
22. Lore JM Jr, Farrell M, Castillo MB, . Endocrine surgery. In:
LorJM Jr, MedinaJE, eds. An Atlas of Head and Neck Surgery. 4th ed.
Philadelphia, PA: Elsevier;2005:963-965.
23. Wang LF, Lee KW, Kuo WR, Wu CW, Lu SP, Chiang FY. The
efficacy of intraop-erative corticosteroids in recurrent laryngeal
nerve palsy after thyroid surgery.World J Surg .
2006;30(3):299-303.
24. Lore JM Jr. Practical anatomical considerations in thyroid
tumor surgery. Arch Otolaryngol . 1983;109(9):568-574.
25. ChristensenT, Stage JG,Galbo H, Christensen NJ,Kehlet H.
Fatigue andcardiacand endocrinemetabolic response to exercise
afterabdominal surgery. Surgery .1989;105(1):46-50.
26. Greif R, Laciny S, Rapf B, Hickle RS, Sessler DI.
Supplemental oxygen reducesthe incidence of postoperative nausea
and vomiting. Anesthesiology . 1999;91(5):1246-1252.
27. Ma ttig H, Bildat D, Metzger B. Reducing the rate of
recurrent nerve paralysis byroutine exposure of the nerves in
thyroid gland operations [in German]. Zen- tralbl Chir .
1998;123(1):17-20.
28. Pimpl W, RiegerR, Waclawiczek HW,MeiserG, Zukriegel M,
BoecklO. Techniqueof recurrent laryngeal nerve exposure within the
scope of interventions of the thy-roid gland [in German]. Wien Klin
Wochenschr . 1992;104(15):439-442.
29. BergamaschiR, BecouarnG, Ronceray J, Arnaud JP.Morbidityof
thyroidsurgery.Am J Surg . 1998;176(1):71-75.
30. Hermann M, Alk G, Roka R, Glaser K, Freissmuth M. Laryngeal
recurrent nerveinjury in surgery for benign thyroid diseases:
effect of nerve dissection and im-pact of individual surgeon in
more than 27,000 nerves at risk. Ann Surg .
2002;235(2):261-268.
31. Vittimberga FJ Jr, Foley DP, Meyers WC, Callery MP.
Laparoscopic surgery andthe systemic immune response. Ann Surg .
1998;227(3):326-334.
32. Mayers I, Johnson D. The nonspecific inflammatory response
to injury. Can J Anaesth . 1998;45(9):871-879.
33. GuptaA, WatsonDI. Effectof laparoscopy onimmune function.BrJ
Surg . 2001;88(10):1296-1306.
34. Cruickshank AM, Fraser WD, Burns HJ, Van Damme J, Shenkin A.
Response ofserum interleukin-6 in patients undergoing elective
surgery of varying severity.Clin Sci (Lond) .
1990;79(2):161-165.
35. Perlmutter DH, Dinarello CA, Punsal PI, Colten HR.
Cachectin/tumor necrosisfactor regulates hepatic acute-phase gene
expression. J Clin Invest . 1986;78(5):1349-1354.
36. Sakamoto K, Arakawa H, Mita S, et al. Elevation of
circulating interleukin 6 aftersurgery: factors influencing the
serum level. Cytokine . 1994;6(2):181-186.
37. Ohzato H, Yoshizaki K, Nishimoto N, et al. Interleukin-6 as
a new indicator ofinflammatory status: detection of serum levels of
interleukin-6 and C-reactiveprotein after surgery. Surgery .
1992;111(2):201-209.
38. Spa th-Schwalbe E, Hansen K, Schmidt F, et al. Acute effects
of recombinant hu-man interleukin-6 on endocrine and central
nervous sleep functions in healthymen. J Clin Endocrinol Metab .
1998;83(5):1573-1579.
39. Nagelschmidt M, Fu ZX, Saad S, Dimmeler S, Neugebauer E.
Preoperative highdose methylprednisolone improves patients outcome
after abdominal surgery.Eur J Surg . 1999;165(10):971-978.
40. Schulze S, Andersen J, Overgaard H, et al. Effect of
prednisolone on the sys-temic response and wound healing after
colonic surgery. Arch Surg . 1997;132(2):129-135.
41. Yared JP, Starr NJ, Torres FK, et al. Effects of single
dose, postinduction dexa-methasone on recovery after cardiac
surgery. Ann Thorac Surg . 2000;69(5):1420-1424.
42. Bigler D, Jonsson T, Olsen J, Brene J, Sander-Jensen K. The
effect of preop-
erativemethylprednisoloneon pulmonary functionand painafterlung
operations.J Thorac Cardiovasc Surg . 1996;112(1):142-145.43.
Sauerland S, Nagelschmidt M, Mallmann P, Neugebauer EA. Risks and
benefits
of preoperative high dose methylprednisolone in surgical
patients: a systematicreview. Drug Saf . 2000;23(5):449-461.
44. Hargreaves KM, Costello A. Glucocorticoids suppress levels
of immunoreactivebradykinin in inflamed tissue as evaluated by
microdialysis probes. Clin Phar- macol Ther .
1990;48(2):168-178.
45. HongD, ByersMR, Oswald RJ.Dexamethasonetreatmentreduces
sensory neu-ropeptides and nerve sprouting reactions in injured
teeth. Pain . 1993;55(2):171-181.
46. McKenzie R, TantisiraB, Karambelkar DJ, Riley TJ,
AbdelhadyH. Comparisonofondansetron with ondansetron plus
dexamethasone in the prevention of post-operative nausea and
vomiting. Anesth Analg . 1994;79(5):961-964.
47. Baxendale BR, Vater M, Lavery KM. Dexamethasone reduces pain
and swellingfollowing extraction of third molar teeth. Anaesthesia
. 1993;48(11):961-964.
48. Coloma M, White PF, Markowitz SD, et al. Dexamethasone in
combination with
dolasetron forprophylaxis inthe ambulatory setting:effecton
outcomeafter lapa-roscopic cholecystectomy. Anesthesiology .
2002;96(6):1346-1350.
49. Wang JJ, Ho ST, Liu YH, et al. Dexamethasone reduces nausea
and vomitingafter laparoscopic cholecystectomy. Br J Anaesth .
1999;83(5):772-775.
50. Wang JJ, Ho ST, Uen YH, et al. Small-dose dexamethasone
reduces nausea andvomiting after laparoscopic cholecystectomy: a
comparison of tropisetron withsaline. Anesth Analg .
2002;95(1):229-232.
51. Donnelly LE, Newton R, Kennedy GE, et al. Anti-inflammatory
effects of resve-ratrol in lungepithelialcells:
molecularmechanisms.AmJ Physiol Lung Cell Mol Physiol .
2004;287(4):L774-L783.
52. Wang JJ, Ho ST, Tzeng JI, Tang CS. The effect of timing of
dexamethasone ad-ministration on its efficacy as a prophylactic
antiemetic for postoperative nau-sea and vomiting. Anesth Analg .
2000;91(1):136-139.
53. Chiang FY, Wang LF, Huang YF, Lee KW, Kuo WR. Recurrent
laryngeal nervepalsy after thyroidectomy with routine
identification of the recurrent laryngealnerve. Surgery .
2005;137(3):342-347.
54. Razack MS, Lore JM Jr, Lippes HA, Schaefer DP, Rassael H.
Total thyroidec-tomy for Graves disease. Head Neck .
1997;19(5):378-383.
55. Agarwal A, Mishra SK. Role of surgery in the management of
Graves disease.J Indian Med Assoc . 2001;99(5):252, 254-256.
56. Steurer M, Passler C, Denk DM, Schneider B, Niederle B,
Bigenzahn W. Advan-tages of recurrent laryngeal nerve
identification in thyroidectomy and parathy-roidectomy and the
importance of preoperative and postoperative laryngo-scopic
examination in more than 1000 nerves at risk. Laryngoscope .
2002;112(1):124-133.
57. Flynn MB, Lyons KJ, Tarter JW, Ragsdale TL. Local
complications after surgicalresection for thyroid carcinoma. Am J
Surg . 1994;168(5):404-407.
JAMA OTOLARYNGOL HEAD NECK SURG/ VOL 139 (NO. 5), MAY 2013
WWW.JAMAOTO.COM478
2013 American Medical Association. All rights reserved.