-
8/20/2019 Dexamethasone Dose Attenuates Pain on Injection.87
1/13
Letters to the Editor
AIS’ Current Role in Anesthesiology RiskManagement Remains
Uncertain
To the Editor:
I read with interest the article by Dr. Feldman (1). Despite the
author’seffort to address an important topic, the approach to
answering thiscomplex question has resulted in a potentially
misleading conclusion.The article indicates that departments using
AIS find that it does notinterfere with “risk management.” In
addition, in the opinion of someof the surveyed departments,
electronic records have been helpful indisposing of potential and
actual malpractice actions more favorably.Unfortunately, there are
substantial limitations in the study method-ology that preclude
definite conclusions. This is due in part to manycurrently
unresolved issues associated with the intermeshing of med-ical
informatics and anesthesiology. A number of these issues are
enumerated below.First, there is still much to learn about
managing biosignals
transduced to a real-time monitor, let alone a written record
withstored data. For example, at this time all biosignals are
analog innature. These signals must be electronically converted to
digitalsignals to be recorded by a PC (or any computer) (2). In
additionthere are real-time data sampling and data quantification
prob-lems that can significantly alter read-out values (2).
Conse-quently, data printed on a written record from stored
computerdata is, by its intrinsic nature, data that has been
manipulatedinto a form that may or may not be sufficiently accurate
to reflectthe clinical situation in real time. This problem of
computer datamanipulation is a limitation that is similar to the
current handwritten record. It is not possible to know from the
informationpresented whether the AIS surveyed are actually more
accuratethan a written record.
Second, this paper does not define the term “risk
management.”Risk management, as a field of study, incorporates
specific methodsfor identifying and managing issues in an attempt
to decrease notonly the risk of lawsuits but also for identifying
and mitigatingmany other types of liability issues (3). In any
JCAHO accreditedinstitution, risk management methods are regularly
applied to prob-lems in the medical setting not related to provider
negligence.Perhaps substituting the words “decrease in liability”
or “decreas-ing liability” for “risk management,” in this article,
would producea more understandable (but not more valid)
interpretation of thesurvey data. Absent a specific definition of
“risk management” inthe questionnaire, the respondents are left to
apply their own inter-pretation to a term with several contextual
definitions, which pro-foundly confounds our ability to interpret
the survey results.
Third, the survey asks the questionnaire respondents to come toa
legal conclusion about whether the increase in quality of docu-
mentation (which is presumed but not established by
objectiveevidence) made a difference in legal actions such as
voluntarilydismissing a suit or settling a suit by somehow
decreasing liability.It seems exceedingly unlikely that the
respondents to this surveycould definitively know the plaintiff’s
actual reasoning for droppingor settling a suit and whether it was
actually related to AIS, sincemost physicians do not understand the
potential legal proof prob-lems associated with these electronic
records. The AIS are propri-etary and they vary significantly
because there is no establishedstandard for these systems. More
importantly, using AIS is not thestandard of care currently. A
well-qualified attorney could (andlikely would) raise substantial
questions about the accuracy and thevalidity of any (AIS) system
based on the aforementioned factors.Therefore, depending on the
relationship between the anesthesiarecord and the particular
liability issue in question, the use of AIScould influence the
decision of opposing counsel in either direction:
to pursue or reject a claim, depending on the nature of the
injurysustained and the ability to prove the relationship (in legal
terms,the attachment of liability) between the presumed negligence
andthe injury (proximate cause).
Fourth, this paper speculates incorrectly that any additional
datanot printed on the anesthesia record may, in the future, be
intro-duced into a legal proceeding in a manner that might be
determined
by the institution or department in question. To suggest
that a set of circumstances would arise where part of the
record could be vol-untarily withheld is incorrect. Any additional
data archived in anelectronic database of the AIS is now and will
in the future be legallyavailable for analysis in any litigation. A
patient’s record and alldata contained therein belong to the
patient (4). The complete recordcannot be sequestered or remain
undisclosed without creating asituation where the institution
and/or the physician are in contemptof the court.
The methodology of this paper severely constrains our ability
to
derive meaningful conclusions about AIS and its role in
liabilityreduction and risk management. Additional investigation
that ad-dresses the issues noted above will be required before we
can makea valid determination of the utility of AIS for liability
reduction andrisk management.
Philip Edward Lane, MD , JD , MPH,
MBADepartment of AnesthesiologyRush University Medical
CenterChicago, IL
[email protected]
References1. Feldman JM. Do anesthesia information systems (AIS)
increase malpractice exposure?
Results of a survey. Anesth Analg 2004;99:840–3.2. Van Bemmel
JH, Musen MA. Eds. Biosignal analysis in handbook of medical
infor-
matics. New York: Springer, 1997:120–5.3. Vincent C. The
development of clinical risk management. In: Clinical risk
manage-
ment. London: BMJ Books, 2001:45–60.
4. Available
at http://www.hhs.gov/ocr/hipaa/consumer_summary.pdf .
DOI: 10.1213/01.ANE.0000151477.28089.88
In Response:
In Dr. Lane’s letter on my article (1), he writes that the
“paperseverely constrains our ability to derive meaningful
conclusionsabout AIS and its role in liability reduction and risk
management.”I agree that the question of the impact of AIS on
malpracticeexposure remains open and that the information available
from thearticle is not definitive. Any survey has major sampling
limitationsand more importantly, the investigator cannot control
the quality of the data collected. Dr. Lane does however seem
to have misinter-preted some of the information presented in the
article that I wouldlike to reiterate.
In the introduction to the article, I described opposing
argumentssupporting the contentions that AIS increase and decrease
malprac-
tice exposure. One of my primary goals in this study was to
findevidence supporting either one of these arguments as they
haveheretofore been based solely on opinion. Unfortunately,
evidencefrom legal precedent could not be identified and the survey
was theonly instrument for collecting any form of data. Of the
departmentsresponding to the survey, there was not one report that
the AISincreased malpractice exposure. As I stated in the article,
“Theresults of the survey lend credibility to the argument that AIS
helpto reduce malpractice exposure.” This conclusion was not
intendedto be a definitive statement about the role of AIS in
malpracticeexposure, only an assessment of the evidence collected
by thesurvey.
Dr. Lane also seemed to misinterpret the discussion
regardingdiscoverability of electronic data. This is a very
important point thatis worthy of clarification. The article clearly
states that a highresolution electronic version of the data
collected during anesthesia
©2005 by the International Anesthesia Research Society Anesth
Analg 2005;100:1537–49 1537
-
8/20/2019 Dexamethasone Dose Attenuates Pain on Injection.87
2/13
is created by the AIS in addition to the printed version placed
in thepatient’s medical record. Although I could not find evidence
to datethat the electronic data has been part of the discovery
process, thereis no question in my mind that it will be in the
future. As AIS areadopted, risk managers will need to consider not
only the impact of the printed record on malpractice exposure
but also the impact of the high-resolution electronic
archive.
Not only are AIS proliferating, there is momentum building onthe
national level to make the entire patient record electronic. Wewill
undoubtedly have to address not only the malpractice impli-cations,
but also all of the complexities that will be introduced bythis
technology. I certainly look forward to more definitive
evidencefrom actual malpractice proceedings to document the role of
AIS inthe malpractice process and to continued constructive
dialogue onthis important question.
Jeffrey M. Feldman, MD, MSEDepartment of
AnesthesiologyChildren’s Hospital of PhiladelphiaPhiladelphia,
PA
[email protected]
Reference1. Feldman JM. Do anesthesia information systems (AIS)
increase malpractice exposure?
Results of a survey. Anesth Analg 2004;99:840–3.
Effects of Hydroxyethyl Starch and Calciumon Platelet
ActivationTo the Editor:
I read with great interest the article by Deusch et al. (1)
whereincitrate anticoagulated blood diluted 20% with Hextend®
(AbbottLaboratories, Chicago, IL) had greater platelet activation
than otherhydroxyethyl starch solutions devoid of calcium.
Furthermore,
blood samples diluted with a 600 kd-containing
hydroxyethylstarch solution with addition of calcium equivalent to
Hextend®
also had an increase in platelet activation. My concern with
theseresults was that blood sample calcium concentrations could
besufficiently increased by Hextend® to initiated thrombin
generation.
To test this, pooled, citrated control plasma (Trinity Biotech,
Ven-tura, CA) was either undiluted, diluted 20% with 6% hetastarch
in0.9% NaCl (Abbott) or with Hextend® (n 3 per condition) at
roomtemperature for 5 min prior to calcium determination with
ananalyzer (model 1306, Instrumentation Laboratory, Lexington,
MA).Calcium values were as follows (mM): undiluted
0.02 0.01,hetastarch 0.01 0.00, Hextend® 0.04 0.01.
One-way analysisof variance demonstrated that the plasma diluted
with Hextend®
had a significantly greater calcium concentration than the
otherfluids. Nevertheless, this concentration is far below the
thresholdrequired for thrombin generation. What other mechanism
underlyingcalcium-mediated platelet activation would the authors
suggest?
Another issue is the citation by Deusch and colleagues (1) of
astudy wherein Hextend® administration resulted in enhanced
he-mostasis assessed by thrombelastography (decreased R time) in
arabbit model of hemorrhagic shock (2). Deusch et al. (1) in
their
discussion imply that our findings were explained by calcium
con-tained in Hextend®—a conclusion that is not true, as
Hextend®
decreased endogenous heparinoid release and did not affect
bloodcalcium concentration (2). In fact, there has never been a
significantchange in blood calcium concentration documented in any
of our invivo rabbit studies involving hemodilution
(3,4). However, while40% dilution with Hextend® did not change R
values (3), 75%dilution did significantly decrease R values in
rabbits (4).
Vance G. Nielsen, MDDepartment of AnesthesiologyThe
University of Alabama at BirminghamBirmingham,
[email protected]
References1. Deusch E, Thaler U, Kozek-Langenecker SA. The
effects of high molecular weight
hydroxyethyl starch solutions on platelets. Anesth Analg
2004;99:665–8.2. Nielsen VG. Resuscitation with Hextend® decreases
endogenous circulating heparin
activity and accelerates clot initiation after hemorrhage in the
rabbit. Anesth Analg2001;93:1106–10.
3. McCammon AT, Wright JP, Figueroa M, Nielsen VG. Hemodilution
with albumin, butnot Hextend®, results in hypercoagulability as
assessed by thrombelastography inrabbits: role of heparin-dependent
serpins and factor VIII complex. Anesth Analg2002;95:844–50.
4. Nielsen VG, Baird MS. Extreme hemodilution in rabbits: an
in vitro and in vivothrombelastographic
analysis. Anesth Analg 2000;90:541–5.
DOI: 10.1213/01.ANE.0000149041.17161.FF
In Response:
Thank you for the opportunity to respond to the comments of
Dr.Nielsen to our article (1).
Enhanced hemostasis may result from an increase in
procoagulantssuch as activated platelets or increased levels of
ionized calcium, adecrease in anticoagulants such as
heparin-dependent serpins, or acombination of both. The novel
hetastarch diluted in a balanced elec-trolyte formulation
containing calcium, lactate buffer, and a physio-logic level of
glucose (Hextend®) has been reported to enhance hemo-stasis: lower
thromboelastographic R values were found in patientsreceiving
Hextend® compared with hetastarch in saline (2). Similarly,lower R
times were observed by Nielsen et al. after 75% in vitro dilutionof
blood with Hextend® (3) and after about 40% isovolemic
hemodi-lution in rabbits (4) when compared with albumin. The
underlyingmechanisms for enhanced dynamic clot formation after
Hextend® still
remain unclear. Among other factors, ionized calcium levels
affect Rtime. In vitro 75% hemodilution using albumin
significantly deceasedcalcium concentrations and prolonged R time,
which was reversible bycalcium supplementation (3). In contrast to
albumin, isovolemic he-modilution using Hextend® containing calcium
in the commerciallyavailable solution resulted in no decrease in
calcium levels (3–5). Sim-ilarly, Hextend-treated patients required
less intraoperative calciumand were less likely to receive calcium
supplementation than patientstreated with hetastarch in saline (2).
In his letter, Dr. Nielsen stated thatwe misinterpreted his studies
in our discussion section (1). However,the discussion on the
importance of calciumin facilitating hemostasis wasclearly related
to our study results performed in citrated whole blood.
R time is also dependent on platelet procoagulant activity.
Our invitro experiments demonstrated an increase in
platelet activationafter incubation of citrated whole blood with
Hextend® and indicatethat this effect is, at least in part, due to
the solvent of Hextend®
containing calcium (1). Maintenance of calcium
concentrationwithin physiological ranges and acid-base balance may
attenuatefluid-specific pharmacodynamic effects of Hextend® on
platelets.Nielsen questions in his letter this potential mechanism
by demon-strating some data on low calcium levels achieved after
in vitroHextend® dilution that were below the threshold for
plasma clottingkinetics. To the best of our knowledge a calcium
level threshold forcalcium-mediated platelet activation has not
been determined. Cal-cium is the key second messenger in platelets
and although notdetermined in detail so far, a high sensitivity of
platelets to theextracellular electrolyte milieu can be
anticipated.
R time is further dependent on anticoagulants. Since in
vitroexperiments exclude many compensatory changes such as
antico-agulant production, secretion, and removal, as well as
modifyingmechanisms of the endothelium, our findings are not likely
to berelated to anticoagulant activities. In vivo, however,
the decrease in
heparin-dependent serpin activities in the presence of
Hextend
®
asreported by Nielsen et al. (4,5) has to be considered as a
cause of enhanced hemostasis.
E. Deusch, MDS. Kozek-Langenecker, MD
Medical University of ViennaVienna,
[email protected]
References1. Deusch E, Thaler U, Kozek-Langenecker S. The
effects of high molecular weight
hydroxyethyl starch solutions on platelets. Anesth Analg
2004;99:665–8.2. Gan TJ, Bennett-Guerrero E, Phillips-Bute B, et
al. Hextend, a physiologically balanced
plasma expander for large volume use in major surgery: a
randomized phase IIIclinical trial. Anesth Analg 1999;88:992–8.
3. Nielsen VG, Baird MS. Extreme hemodilution in rabbits: an in
vitro and in vivothrombelastographic analysis. Anesth Analg
2000;90:541–5.
4. Nielsen VG. Resuscitation with Hextend® decreases endogenous
circulating heparinactivity and accelerates clot initiation after
hemorrhage in the rabbit. Anesth Analg
2001;93:1106–10.
1538 LETTERS TO THE EDITOR ANESTH
ANALG2005;100:1537–49
-
8/20/2019 Dexamethasone Dose Attenuates Pain on Injection.87
3/13
5. McCammon AT, Wright JP, Figueroa M, Nielsen VG. Hemodilution
with albumin, but notHextend®, results in hypercoagulability as
assessed by thrombelastography in rabbits: roleof heparin-dependent
serpins and factor VIII complex. Anesth Analg 2002:95:844–50.
Skin Sensitivity to Rocuronium and
Vecuronium: Prick-Tests Are NotIntradermal TestTo the
Editor:
We read with interest the study by Dhonneur et al. (1). The
authorsreport a 50% and 40% incidence of positive skin reaction to
undilutedrocuronium and vecuronium, respectively. They state that
these resultsare in contradiction with the recent guidelines
published by the SociétéFrançaise d’Anesthésie et de
Réanimation (SFAR) (2). Unfortunately,these authors did not follow
the recommendations for positivity crite-ria established by SFAR.
In these guidelines, the criterion of a positiveprick test is
theappearance ofan edematous whealwitha diameterat least3 mm
greater than that induced by the negative control solution.
Incontrast, for Dhonneur et al., the association of a wheal and a
flare definesa positive skin reaction irrespective of their size.
Moreover, by injecting 50L, the authors confuse prick-testing which
corresponds to an injection of a volume of 20 nL, and
intradermal testing which requires an injection of 20 to 50
L. Use of completely different criteria and administration of
atleast 1000-fold more allergen than recommended by SFAR may
explainthe unexpected high proportion of positive reactions
observed.
The authors state that their observations are supported by
arecent Scandinavian report (3). Unfortunately, in the latter no
pos-itive prick test to undiluted rocuronium or cisatracurium was
re-ported. Similarly, other large studies from the literature
publishedin different countries are in contradiction with Dhonneur
et al.’sresults (4,5). The authors also claim that their results
are in line withthose reported by Levy et al. (6). Unfortunately,
no prick-test wasperformed in this study.
Finally, Dhonneur et al. suggest that their findings may
explainthe intriguingly high incidence of allergic reactions in
France andcall into doubt whether NMBDs are the main cause of
anaphylaxisduring anesthesia (7,8). However, anaphylactic reactions
to anes-
thetic drugs have been reported in Australia, New Zealand,
theUnited Kingdom, Norway, Belgium, and Spain with a similar
esti-mated incidence, and in all these studies, NMBDs are the
mostcommon cause of anaphylaxis during anesthesia.
In conclusion, the results reported by Dhonneur et al. are, in
ouropinion, in contradiction with the literature, and we do not
believethat they support the conclusion drawn by these authors
regardingthe reality of the risk of anaphylaxis during
anesthesia.
P. M. Mertes, MD, PhDM. C. Laxenaire,Department of
Anesthesia and Intensive CareUniversity Hospital of Nancy,
France
[email protected]
J. M. Malinovsky, MD , PhDDepartment of
Anesthesia and Intensive CareUniversity Hospital of Reims,
France
E. Florvaag, MDLaboratory of Clinical Biochemistry
Haukeland University HospitalBergen, Norway
D. A. Moneret-Vautrin, MDDepartment of
AllergologyUniversity Hospital of Nancy, France
References1. Dhonneur G, Combes X, Chassard D, Merle JC. Skin
sensitivity to rocuronium and
vecuronium: a randomized controlled prick-testing study in
healthy volunteers.Anesth Analg 2004;98:986–9.
2. Reducing the risk of anaphylaxis during anaesthesia
[abbreviated text]. Ann Fr AnesthReanim 2002;21(Suppl
1):7s–23s.
3. Berg CM, Heier T, Wilhelmsen V, Florvaag E. Rocuronium and
cisatracurium-positiveskin tests in non-allergic volunteers:
determination of drug concentration thresholdsusing a dilution
titration technique. Acta Anaesthesiol Scand 2003;47:576–82.
4. Leynadier F, Sansarricq M, Didier JM, Dry J. Prick tests in
the diagnosis of anaphylaxis
to general anaesthetics. Br J Anaesth 1987;59:683–9.
5. Fisher MM, Bowey CJ. Intradermal compared with prick testing
in the diagnosis of anaesthetic allergy. Br J Anaesth
1997;79:59– 63.
6. Levy JH, Gottge M, Szlam F, et al. Weal and flare responses
to intradermal rocuroniumand cisatracurium in humans. Br J Anaesth
2000;85:844–9.
7. Laxenaire M, Mertes PM, Groupe d’Etudes des Reactions
Anaphylactoides Peranes-thesiques. Anaphylaxis during
anaesthesia: results of a 2 year survey in France. Br JAnaesth
2001;87:549–58.
8. Mertes PM, Alla F, Laxenaire MC, Anaphylactic and
anaphylactoid reactions occurringduring anesthesia in France in
1999 –2000. Anesthesiology 2003;99:536–45
DOI: 10.1213/01.ANE.0000149043.37250.61
In Response:
I want to thank Mertes et al. for offering such an important
tribuneto argue comments and remarks about the results, methodology
anddiscussion of our study (1). Before giving a point-by-point
responseto Mertes et al., I would like to specify that I am not an
expert inimmunology and I do not make a living in the
neuromuscular
blocking drugs nor the allergy industry.Regarding the
Methods section, Mertes et al. suggests that we
“confused prick testing and intradermal testing.” This remark is
notacceptable and I believe that the title of this letter is
inappropriate.We did not perform any injection of any sort but just
applied GoodClinical Practice (GCP) recommendations for prick
testing. GCPsare GCPs! A single investigator working in the
cosmetic departmentof one of the most important French CRO
performed all prick tests.A calibrated 50-L drop of a solution is
placed on the skin on theforearm that is pricked with a
commercially available device: 1-mmtip at 1 mm deep 20 nL of active
substance delivered. Under theseconditions, the amount of active
substance, rather than “allergen,” isstrictly linked to the
concentration of the contact solution.
The present letter also states that we did not follow the
recom-mendations for “positivity” criteria established by SFAR. Of
course,we did not. We challenged the skin of selected healthy
volunteers,and we defined arbitrarily in the Methods section our
criteria of positive skin reaction. Indeed, the association of
a wheal and flarecharacterized in our study a positive reaction
irrespective of theirsize. As written in the introduction section,
“this study was per-formed to determine the concentration-response
curves for pricktests with rocuronium and vecuronium in healthy
volunteers” butnot to diagnose allergy. We did investigate the
relationship betweendose of relaxants and skin responses looking at
a nonspecific effect
of aminosteroid drugs that we characterized for the flare
responses.Our results are not disputable because of the study
design.Regarding the Discussion section, we never affirmed that
our
results were “in contradiction with the recent guidelines
published by the SFAR but rather that ”our observations
contrast“ with theFrench group’s estimation of normally nonreactive
concentration of rocuronium and vecuronium. Guidelines are
guidelines and ourresults cannot be in contradiction with
guidelines. On the otherhand, our results question the pertinence
of recommendations forclinical diagnosis of allergy. Discussion and
interpretation of ourresults is based on these recommendations.
To putour results in perspective,we strictly applied the
onecriterionfor positive prick test proposed by the French group
recalled by Merteset al. in this letter: an edematous wheal with a
diameter at least 3 mmgreater than that induced by the negative
control solution. Calculationof the area of a wheal reaction is
linked to its diameter. Since none of
our volunteers reacted to the negative control solution, all
prick-testswere considered positive if the surface of the wheal was
greater than7 mm2 [ * (3.0/2) (2)]. To
assess the quality of our results, weapplied other criteria for
positive prick tests (some are proposed in Eu-rope, other in the
United States) such as comparing individual weal orflare surface
ratios between that of the positive control and active
dilutedsolutions of relaxants. Interestingly, this quality control
procedure dem-onstrated that wherever the cursor is placed, there
are at least 15% of thevolunteers being significantly responsive to
undiluted rocuronium andvecuronium, respectively. Although allergy
is of rare occurrence in anes-thesia, I am convincedthat a rate
offalse positive10%is unacceptable fora diagnostic test. Even under
this new insight our conclusion remainspertinent, prick tests to
undiluted stock solutions of aminosteroids musclerelaxants should
not be used to diagnose or confirm allergy.
Although, the formulation is awkward, our results confirm
theobservations of both Berg et al. (2) and Levy et al. (3) that
demon-
strated frequent false positive rate associated with “skin
testing”
ANESTH ANALG LETTERS TO THE EDITOR
15392005;100:1537–49
-
8/20/2019 Dexamethasone Dose Attenuates Pain on Injection.87
4/13
and pleaded in their respective papers for a clinically
applicablediscriminant test technique able to separate true
positive tests fromfalse positive tests. Moreover, I cannot
understand how our resultscan be in contradiction with other large
studies published in differ-ent countries such as that of Fisher et
al. (4) and Leynadier et al. (5),since these studies were performed
in patients suspected or knownto be allergic but not in healthy
volunteers.
As all clinicians, I am still waiting for an important study
includ-ing a large cohort of healthy volunteers from several
countries andof different skin colors tested to determine real skin
sensitivity toNMBAs, unless this study has already been performed
in France butnot published. Unfortunately, in the absence of such
major study for
better application of skin testing and validation of other
diagnosticapproach of allergy to anesthetic drugs, it is not
certain that we aremaking the correct diagnostic of allergy to
rocuronium and vecu-ronium using prick responses to undiluted stock
solutions.
We are aware that the French group has performed an immense
taskin the area of allergy and largely “sensitized” all
anesthesiologists (notonly French professionals) to this risk. We
are better prepared for suchrisk, and special operating diagnostic
and therapeutic procedures arenow systematically applied in case of
suspicion of an allergic accident.The French group did a great job
for patients’ security. We accept thefact that neuromuscular
blocking drugs are probably the most com-
mon cause of anaphylaxis during anesthesia. However, real
incidenceof allergy is difficult to establish and do vary among
countries. Report-ing problems pollute the numerator, and the
denominator is highlyvariable. Dr. Levy (6) suggested in an
editorial that the only way toexplain this widely divergent
perspective is to understand how thediagnosis is made and to define
threshold skin tests concentrations.This was our main goal.
We believe that there is now probably enough material that
callsinto question the past practice of skin testing in anesthesia
for ourFrench eminent specialists, the leaders in this area, to
manageindisputable international studies and propose
worldwide-agreedguidelines for the diagnostic of allergy in
anesthesia.
We also believe that stigmatizing neuromuscular blocking drugsor
dealing with fear of allergy is an attitude that promotes
“epider-mic reactions” and blocks off the potential allergic risk
of otherdrugs used in the clinical practice of anesthesia.
Gilles Dhonneur, MDDepartment of Anesthesia and Critical
Care Medicine Henri Mondor University Hospital of
CréteilUniversity of Paris XII Val-de-MarneSchool of Medicine of
CréteilCrétei l, France
[email protected]
References1. Dhonneur G, Combes X, Chassard D, Merle JC. Skin
sensitivity to rocuronium and
vecuronium: a randomized controlled prick-testing study in
healthy volunteers.Anesth Analg 2004;98:986–9.
2. Berg CM, Heier T, Wilhelmsen V, Florvaag E. Rocuronium and
cisatracurium-positiveskin tests in non-allergic volunteers:
determination of drug concentration thresholdsusing a dilution
titration technique. Acta Anaesthesiol Scand 2003;47:576–82.
3. Levy JH, Gottge M, Szlam F, et al. Weal and flare responses
to intradermal rocuroniumand cisatracurium in humans. Br J Anaesth
2000;85:844–9.
4. Fisher MM, Bowey CJ. Intradermal compared with prick testing
in the diagnosis of anaesthetic allergy. Br J Anaesth
1997;79:59– 63.
5. Leynadier F, Sansarricq M, Didier JM, Dry J. Prick tests in
the diagnosis of anaphylaxis
to general anaesthetics. Br J Anaesth 1987;59:683–9.6. JH Levy.
Anaphylactic reactions to neuromuscular blocking drugs: are we
making thecorrect diagnosis. Anesth Analg 2005;98:881–2.
Local Anesthetics for Breakthrough Pain inPatients Receiving
Intrathecal Treatment forCancer Pain ManagementTo the Editor:
Neuraxial administration of drugs is often used to optimize the
treat-ment in patients no longer responsive to systemic analgesics
(1). De-spite optimal analgesia, patients may suffer from
fluctuations in painintensity (breakthrough pain) (2). This
condition is challenging forphysician, as no specific indications
have been provided for patients
receiving a continuous spinal drug combination. We report three
casesof patients selected for intrathecal therapy, implanted with a
port-system and an external pump, and presenting breakthrough
episodestreated by the use of local anesthetics as needed. The
first patient, a57-year-old male, with colon cancer was admitted
for abdominal paindue to extensive visceral involvement. The second
patient was a 40-year-old female, admitted for unbearable pain due
to pelvic relapse of
colon cancer, presenting multiple metastases (spleen, pancreas,
leftcolon, presacral area, left ischiorectal fossa, bladder, left
ala ilii, abdom-inal wall, ureter, lung, and liver). She complained
of abdominal-pelvicpain with irradiation to the left leg, with a
mixed component, visceral,neuropathic, and somatic. The third
patient, a 76-year-old male withlung cancer, was admitted for
vertebral, chest wall, and shoulder pain,irradiated to the left
arm, which increased in intensity on movementdue to chest wall
involvement. An intrathecal catheter was introducedat the level of
corresponding segmental area and connected with asubcutaneous port
placed in the anterior thoracic wall, after tunnelingthe catheter
subcutaneously. The proper position of the catheter tipwas checked
by contrast medium injection. These patients received anintrathecal
mixture containing morphine and levobupivacaine, indoses of 25–80
mg and 6–40 mg, respectively, with a mean infusionrate of
levobupivacaine of 37 mg/day (about 1.5 mg/h), allowing
anacceptable basal pain relief (4 on a numerical scale of 0–10).
Episodes
of breakthrough pain, unresponsive to large doses of systemic
opioids,were relieved by intrathecal boluses of about 1.25 mg (0.5
mL of levobupivacaine), by a three-way stopcock placed in the
external sys-tem, close to the port. This means that the dose
required to treat
breakthrough events was approximately the hourly dose. No
infectionsigns or important hemodynamic changes were observed,
despite therepeated boluses. Of interest, the treatment was
subsequently main-tained at home by properly instructed relatives,
without reportingcomplications for a survival time of 10, 45, 32
days, respectively. Thisis the first report on the use of local
anesthetics as an intrathecal bolusfor treating breakthrough pain
in cancer patients receiving a spinalanalgesic treatment. This
treatment should be reserved to very selectedpopulation, providing
the best methods to prevent the risk of infectiondue to the high
rate of manipulations.
Sebastiano Mercadante, MDPatrizia Ferrera, MD
Patrizia Villari, MD Anesthesia and Intensive Care
UnitPain Relief and Palliative Care UnitLa Maddalena Cancer
CenterPalermo, [email protected]
Edoardo Arcuri, MDIntensive Care and Pain Therapy
UnitNational Cancer Institute Regina ElenaRome, Italy
References1. Mercadante S. Problems of long-term spinal opioid
treatment in advanced cancer
patients. Pain 1999;79:1–13.2. Portenoy RK, Hagen NA.
Breakthrough pain: definition, prevalence, and characteris-
tics. Pain 1990;41:273–81.
DOI: 10.1213/01.ANE.0000149045.24425.68
An Uncommon Complication of ThoracicEpidural Anesthesia: Pleural
PunctureTo the Editor:
Thoracic epidural analgesia is commonly used to provide
perioper-ative analgesia in patients undergoing thoracic surgery,
and pleuralpuncture by the needle or the catheter is an uncommon
and alife-threatening complication (1–4).
A 67-year-old female patient, body mass index 36 kg/m2
(weight,105 kg; height, 170 cm) was scheduled for lobectomy. The
awakepatient was placed in the left lateral decubitus position. An
18-gauge Tuohy needle was inserted at the T6–7 interspace with
amidline approach. Technical difficulties were encountered
becauseof poor body landmarks and decreased resistance of the
deeper
1540 LETTERS TO THE EDITOR ANESTH
ANALG2005;100:1537–49
-
8/20/2019 Dexamethasone Dose Attenuates Pain on Injection.87
5/13
tissue levels. On the fourth attempt, a loss of resistance to
saline wasdetected, and the epidural catheter was threaded easily.
No chestsymptoms were observed. Ten milliliters of 0.25%
bupivacaine and100 g fentanyl were injected from the
catheter. Unfortunately,there was not enough time to assess the
level of sensory block beforethe induction. When the chest cavity
was entered, the epiduralcatheter was found penetrating the
parietal pleura in close proxim-ity to both the spine and the
thoracic aorta (Fig. 1). There was noobvious bleeding or injury to
the lung. The catheter was withdrawnand the postoperative course
was uncomplicated.
Only few cases about the misplacement of the thoracic
catheter
into the pleural cavity have been reported in the literature
(1–4). Inmost of these case reports, the paramedian approach was
usedduring needle insertion (1–4). Our case report is the only one
inwhich the midline approach was used. The paramedian approach
tothe thoracic epidural space is thought to have fewer potential
tech-nical problems but a higher complication rate; therefore, it
is be-lieved that the use of the midline approach may minimize the
risk(2). However our case report showed that the midline approach
isnot free from complications. Sprung et al. (5) investigated the
factorsthat may predict the difficulty of performing neuraxial
blocks andconcluded that the quality of body landmarks was the most
signif-icant independent predictor of difficulty and the obese
patients hadthe highest incidence of having poor landmarks.
In conclusion, in obese patients with poor body landmarks, the
sensorylevel of analgesia should be assessed preoperatively or the
correct place-ment of the catheter should be verified by
radiography to decrease the
incidence of technique-related complications during epidural
analgesia.Zeynep Eti, MD*Tunç Laçin, MD†Bedrettin
Yıldızeli, MD†Varlık Dogan, MD*F. Yılmaz Gögüs,
MD*Mustafa Yüksel, MD†*Departments of Anesthesiology
and †Thoracic Surgery
Medical Faculty of Marmara UniversityIstanbul,
[email protected]
References1. Furuya A, Takashi M, Ozaki M, Kumazawa T.
Interpleural misplacement of an
epidural catheter. J Clin Anesth 1998;10:425–6.2. Patt RB, Reddy
S, Wu CL, Catania JA. Pneumothorax as a consequence of thoracic
subarachnoid block. Anesth Analg 1994;78:160–2.3. Grieve PP,
Whitta RKS. Pleural puncture: an unusual complication of a
thoracic
epidural. Anesth Intensive Care 2004;32:113–6.
4. Koch J, Nielsen JU. Rare misplacements of epidural catheters.
Anesthesiology 1986;65:556–7.5. Sprung J, Bourke DL, Grass J, et
al. Predicting the difficult neuraxial block: a prospec-
tive study. Anesth Analg 1999;89:384–9.
DOI: 10.1213/01.ANE.0000149046.59469.48
Measurement of Isoflurane and DesfluraneDegradationTo the
Editor:
Laster et al. (1) suggest that only small amounts of isoflurane
and desflu-rane are degraded in their studies of anesthetic
absorbent fires. The mon-itoring device used for anesthetic
concentrations was a monochromaticinfrared monitor (RGM 5250,
Ohmeda, Louisville, CO), which is prone tointerference becausethe
infraredabsorbance is measured at a single wave-length. The
reported anesthetic concentration is based on a
user-enteredcalibration factor for each anesthetic. Because
trifluoromethane (CHF3) isproduced during the breakdown of
isoflurane and desflurane (2), andinterferes with anesthetic drug
monitoring (3), CHF3 may cause falselyelevated reported
concentrations of the selected anesthetic. Calcula-tions (not
shown) based on our study (3) demonstrate that the RGM5250 monitor
reports approximately 0.9% isoflurane or 1.2% desfluranefor each 1%
CHF3. The breakdown of 1 mole isoflurane or desfluraneproduces 0.23
and 0.84 moles of CHF3, respectively. Therefore, thereported
concentration of isoflurane is falsely elevated by about 21%and
desflurane by about 98% of the degraded amount due to
theinterference of CHF3. Thus, little if any change in reported
desfluraneconcentration can result. Although the ratio of the
amount of CHF3produced for each mole of anesthetic degraded depends
somewhat onreaction temperature (4), it is probable that little, if
any, decrease in theconcentration of desflurane can be detected by
the RGM 5250 monitor
because of the interference of CHF3. Figure 5 in Laster et
al.’s article (1)may indicate little to no desflurane degradation
as a result, and thediscrepancy at the initial measurement may be
due to temperaturedependence, since the absorbent is under 25°C at
that time.
Marshall B. Dunning III, PhD , MSDivision of
Pulmonary/Critical Care [email protected]
Harvey J. Woehlck, MDDepartment of Anesthesiology
Medical College of Wisconsin
Milwaukee, WI
Figure 1. Thoracic epidural catheter lying in the chest
cavity.
ANESTH ANALG LETTERS TO THE EDITOR
15412005;100:1537–49
-
8/20/2019 Dexamethasone Dose Attenuates Pain on Injection.87
6/13
References1. Laster M, Roth P, Eger EI II. Fires from the
interaction of anesthetics with desiccated
absorbent. Anesth Analg 2004;99:769–74.2. Eger EI II, Strum D.
The absorption and degradation of isoflurane and I-653 by dry
soda lime at various temperatures. Anesth Analg
1987;66:1312–5.3. Woehlck HJ, Dunning MB III, et al. The response
of anesthetic agent monitors to
trifluoromethane warns of the presence of carbon monoxide from
anesthetic break-down. J Clin Monit 1997;13:149–55.
4. Woehlck HJ, Dunning M III, Nithipatikom K, et al. Mass
spectrometry provides
warning of carbon monoxide exposure via trifluoromethane.
Anesthesiology 1996;84:1489–93.
DOI: 10.1213/01.ANE.0000149047.06813.41
In Response:
Dunning and Woehlck have correctly taken us to task for
neglectingthe effect of desflurane degradation products on the RGM
5250 de-termination of desflurane (and isoflurane) concentration.
Using gaschromatography, we confirmed the correctness of their
criticism bymeasuring the concentrations of desflurane in the
presence of des-iccated Baralyme®. Duplicate measurements (two
runs) suppliedthe data for desflurane presented in Figure 1. As in
the previousstudy (1), peak temperatures of 100°C were reached
20–30 min afterinitiating delivery of 9% desflurane. Temperatures
declined there-after, despite appreciable continuing desflurane
degradation for upto an hour of desflurane delivery.
Although the data presented in Figure 1 quantitatively differ
greatlyfrom the data presented in a similar figure in ouroriginal
report (Fig. 5)(1), the qualitative implications are unchanged.
Degradation of desflu-rane, and to a lesser extent isoflurane, is
not sustained. In contrast,degradation of sevoflurane continues at
appreciable levels for theduration of sevoflurane administration
(note that data for the full2 hours are not presented because fire
occurred in one run, andinclusion of those data would skew the
results). The data fordesfluraneand isoflurane are consistent with
an action of potassium hydroxide
(KOH) on these anesthetics. The limited presence of KOH (5% of
base),and its consequent rapid depletion, restricts the degradation
of desflu-rane and isoflurane. Degradation of desflurane decreases
faster thandegradation of isoflurane because the concentration of
desflurane isthree times greater, thus exhausting the stores of KOH
sooner. Thecontinuing degradation of sevoflurane suggests that
barium hydroxideand/or calcium hydroxide, as well as KOH, degrade
sevoflurane.
The important message of our previous report (1) remains
un-changed by the present correction. Sevoflurane degradation by
desic-cated Baralyme® can lead to temperatures exceeding 150°C and
to firein the anesthetic circuit. In contrast, degradation of
desflurane andisoflurane by desiccated Baralyme® leads to lower
temperatures (peaksof 100°C), and these lower temperaturesdo not
lead to fire. As an aside,we note that a concern that fires from
sevoflurane degradation may bemore likely with Baralyme® than soda
lime has resulted in the with-drawal of desiccated Baralyme® from
commercial use. Whether thisproblem extends to soda lime remains to
be determined.
[Dr. Eger is a paid consultant to Baxter Healthcare, the
manufac-turer of desflurane.]
Michael J. Laster, DVMPatricia Roth, MDEdmond I
Eger II, MDDepartment of Anaesthesia
University of California, San FranciscoSan Francisco,
[email protected]
Reference1. Laster M, Roth P, Eger EI II. Fires from the
interaction of anesthetics with desiccated
absorbent. Anesth Analg 2004;99:769–74.
Cervical Plexus Block ProvidesPostoperative Analgesia After
ClavicleSurgeryTo the Editor:
We report a case of successful postoperative analgesia after
clavic-
ular open reduction and internal fixation (ORIF) using a
cervicalplexus block (CPB). While an interscalene block could
provideanalgesia, at the price of motor and sensory blockade of the
upperextremity, using a CPB, to our knowledge, has not been
described
before.A healthy 49-year-old woman undergoing right
clavicular ORIF
was given preoperatively a deep (C2–C4) and superficial CPB
ac-cording to the classic approach (1) using 0.5% bupivacaine.
Thesurgical procedure was performed under general anesthesia.
Fol-lowing awakening from general anesthesia, the patient was
pain-free until 14 hours postoperatively. She then took one dose of
oralanalgesics before discharge.
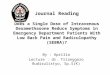
The innervation of the clavicle and the overlying skin
variesdepending on the source in the literature between C3 and C6.
Figure1 summarizes the dermatome distributions published by
severalauthors. The clavicle itself has been reported to be
innervated either
by C4, or by C5 and C6 (subclavian nerve).This case
demonstrates that a cervical plexus block can provideanalgesia
after clavicle ORIF. It remains to be determined whether aCPB could
be used as a sole anesthetic for clavicle ORIF in
selectedpatients.
Daniel S. Choi, MD , MBAArthur Atchabahian,
MDAnthony R. Brown, MDDepartment of AnesthesiologyColumbia
University College of Physicians and SurgeonsNew York,
NY [email protected]
References1. Adriani J. Blocking of spinal nerves. In: Adriani
J, ed. Labat’s Regional anesthesia:
techniques and clinical applications. St. Louis: Warren H.
Green, 1985:236–54.2. Foerster O. The dermatomes in man. Brain
1933;56:1–39.3. Head H, Campbell AW. The pathology of herpes zoster
and its bearing on sensory
localization. Brain 1900;23:353–523.
Figure 1. Degradation of 1.5 MAC (2.8%) sevoflurane exceeds
deg-radation of 1.5 MAC isoflurane (1.8%), which, in turn,
exceedsdegradation of 1.5 MAC desflurane (9%). Percent degradation
wascalculated as 100 times (the difference between the delivered
andend-tidal concentrations) divided by the delivered
concentration.Concentrations in the case of desflurane were
measured by gaschromatography, whereas concentrations of
sevoflurane and isoflu-rane were measured by the Ohmeda RGM 5250
(Louisville, CO). Forthe reasons offered by Dunning and Woehlck,
the values for isoflu-
rane probably are underestimated.
1542 LETTERS TO THE EDITOR ANESTH
ANALG2005;100:1537–49
-
8/20/2019 Dexamethasone Dose Attenuates Pain on Injection.87
7/13
4. Bonica JJ. Applied anatomy relevant to pain. In: Bonica JJ,
ed. Management of pain. 2nded. Malvern: Lea & Febiger,
1990:133–58.
5. Keegan JJ, Garrett FD. The segmental distribution of the
cutaneous nerves in the limbsof man. Anat Rec 1948;102:409–37.
DOI: 10.1213/01.ANE.0000149049.08815.00
Dangerous Design Flaw in the Ohmeda
Aespire Anesthesia SystemTo the Editor:
We believe there is a dangerous design flaw in the Ohmeda
AespireAnesthesia system (Datex-Ohmeda, Helsinki, Finland.).
Althoughthis narrative is being prepared as part of a larger
article on anes-thesia machine design and safety, we feel that this
matter is urgentenough to warrant expedited notification of the
readership.
Recently during a routine anesthetic, one of our most
experiencedCRNA’s called for engineering assistance when the Model
7100ventilator on a new Aespire anesthesia machine began to
intermit-tently fail. During normal controlled ventilation of an
adult patient,the ventilator would periodically shut down and a
sustained pres-sure alarm would flash. After switching to bag
ventilation, theventilator would reset and then function for
several minutes until itagain repeated the failure cycle. The
machine was removed from
service and evaluated by biomedical engineering. They found
that
the machine would indeed abruptly shut off the ventilator and
flasha sustained pressure alarm while maintaining a pressure of
approx-imately 9 cm H2O in the circuit. The system would reset
after severalminutes of hand ventilation by bag. On further
examination it wasfound that the waste gas scavenging system’s flow
regulator had
been turned nearly to off. On the Aespire system this is
located,along with the scavenger bag, in a difficult to access
location behindthe left rear leg of the machine. It was determined
that the lowsuction flow allowed waste gas to accumulate in the bag
and when
the pressure reached 9 cm H2O in the bag, the ventilator was
shutoff and the pressure was maintained throughout the patient
circuit.We initially assumed this was simply a manufacturing
defect, butwere very confused by the fact that, even if a defective
pressurerelease valve was not venting waste gas to the atmosphere,
why wasthe waste gas scavenging system linked to the ventilator?
Afterextensive discussion with Ohmeda’s technical services office,
wewere informed that this was, in fact, purposely designed to
functionin the manner we encountered! Apparently, the rationale for
thisdesign is that, in the event of low suction flow and a buildup
of gasin the waste system, it is preferable to shut off ventilation
and holdthe patient at 9 cm of CPAP, rather than vent the gas to
the roomand contaminate the atmosphere. Ohmeda states that the
thresholdfor ventilator shutoff is 7.5 cm H2O, but may vary with
fresh gasflow. When we advised Ohmeda that this was unacceptable,
theyoffered a choice of replacement valves that would either
convert the
system to a full passive unsuctioned or full unregulated
active
Figure 1. Dermatome distributions determined by different
methods: A, Foerster’s map, constructedusing stimulation of nerve
stumps and observing forvasodilatation (2). B, Head’s diagram, from
observation of patients with herpes zoster lesions (3). C, Bonica’s
map, developed “on the basis of personalobservation and data
published by others” (4). D, Keegan’s chart, established on the
pattern of hypoalgesia following loss of a single nerve root
(5).
ANESTH ANALG LETTERS TO THE EDITOR
15432005;100:1537–49
-
8/20/2019 Dexamethasone Dose Attenuates Pain on Injection.87
8/13
suctioned mode. (Strangely, the full active system still had a
flowregulator on the suction hose near the line connector.)
We have subsequently filed an FDA Form 3500 expressing
ourconcern about this design feature. Representatives from Ohmeda
ad-vise us that this is supplied as standard because some surgical
facilitiesare unable to generate the suction flow required for
proper evacuationof the system and do not want the full active
system. Until recently,
anesthesia machine design and appearance has largely reflected
safetyinnovations as a result of lessons learned through clinical
misadven-ture. Newer systems, however, are sleeker and more
esthetically pleas-ing, while hiding crucial components, such as
flow sensors, unidirec-tional valves, and waste gas scavenging
systems. This is, in essence, atriumph of style over safety.
Furthermore, the desire to accommodatehypothetical fears of trace
anesthesia gas in the OR atmosphere hastrumped the very real hazard
to individual patients of interruptedventilation and sustained
airway pressure. Users of the Aespire anes-thesia system should be
aware of this design issue and take care to besure waste gas is
evacuated appropriately. On their newest model, theADU, this full
suction system is the only available waste gas scaveng-ing
system.
George Mychaskiw II, DOProfessor of Anesthesiology
Steve Morris
Director, Perioperative Biomedical EngineeringDepartment of
AnesthesiologyUniversity of Mississippi School of Medicine
Jackson, MS [email protected]
DOI: 10.1213/01.ANE.0000149050.32419.20
How Likely Is Awareness DuringAnesthesia?To the Editor:
The report by Sebel et al. (1) provides data on an issue of
greatconcern to anesthetists. In a prospective study using a
structured
interview, the investigators identified 25 cases of awareness
duringanesthesia in 19,575 patients for an incidence of 0.13%. In
support of their finding, this incidence parallels the
incidence found in severalother similar studies cited by the
authors. They added that theirestimate of the incidence was
relatively conservative and suggestedthe possibility that the true
incidence might be closer to 0.36%. Wesuggest that a contrary
interpretation is possible.
1. The investigators appear to define awareness by both
objectiveand subjective criteria: the “recalled event was confirmed
by attend-ing personnel (objective criteria), or the investigators
were con-vinced that the memory was real, but no confirmation could
beobtained (subjective criteria).” Awareness during anesthesia is
dif-ficult to certify objectively. In our view it requires
remembrance of an event by the patient that uniquely connects
that remembrance toan event unequivocally occurring during
anesthesia/surgery. Thereport by Saucier et al. supplies such an
example (2). In the study bySebel et al., the patient who “heard
the doctor ask for a stent whichwas identified by a number” meets
this criterion, assuming that thesurgeon corroborated the
remembrance. However, the patient whosaid she had an out of body
experience provides subjective evi-dence. It would be helpful to
know how many of the experiences inTable 4 in their article were
corroborated by the surgeons/operatingroom staff and which relied
solely on convincing the investigators.
2. Awareness during anesthesia (especially during surgery) may
bedifficult to distinguish from awareness (remembrance) during
awak-ening or in the Post Anesthesia Care Unit (PACU). Could the
surgeonsindicate the timing of the remembrance of the voice that
said that “thedoctor forgot to connect the catheter of the bag; the
floor was full of urine. Other jumbled conversations, someone
was angry and yellingabout it.” (“Yelling”? In a hospital in North
America?) Without objec-tive confirmation of the time of this
conversation, we can only conjec-ture whether this represents
recall of an event during surgery, emer-gence from anesthesia, or
in the PACU.
3. In the same vein, the authors observed that “we
interviewedpatients in the PACU and again after seven days because
it has previ-ously been demonstrated that approximately 35% of
cases are detectedonly at a delayed postoperative interview (3).
Approximately one half of the cases in our study were detected
only at the second interview.”Is it possible that repeated
interviews of patients who knew they wereparticipating in a study
of awareness falsely (albeit unconsciously)
increased the incidence of patients’ self-reports?4. We do not
know the number of patients in the present study
only given anesthesia with an IV anesthetic and thus cannot
assignan incidence of awareness during one form of anesthesia (IV)
versusanother (potent inhaled anesthetic) or, indeed, to one as
opposed toanother inhaled anesthetic. This would be useful to know.
Is recallmore likely during IV versus inhaled anesthesia? If so, is
the studypopulation representative of the surgical population as a
whole, inits proportion of patients receiving IV versus inhaled
anesthesia?Five of the 25 cases were found in patients who did not
receive apotent inhaled anesthetic. In an additional 5 or 6
patients, remem-
brance appears to have taken place during induction of
anesthesia,again in the probable absence of a potent inhaled
anesthetic. Be-cause anesthesia solely with IV anesthetics is less
usual in NorthAmerica, and assuming the study population reflects
this practice, itappears that awareness is more likely in patients
given general
anesthesia with an IV anesthetic.5. The authors note that others
have found an incidence of aware-ness 64% greater (0.18% versus
0.11%) in the presence of neuromus-cular blockade (3).
Approximately 80% of the patients with aware-ness in the present
study had neuromuscular blocking drugs, andhalf these patients had
a sense of paralysis as part of their remem-
brance of awareness. Paralysis is not anesthesia, and 20
of thepatients in the present study may not have been adequately
anes-thetized. Of the 5 patients who were not given
neuromuscular
blocking drugs, and thus were presumably adequately
anesthe-tized, one had an out of body experience (see above), one
felt a tubein her throat and did not know if surgery was ongoing
(was thisawakening during intubation?), one was concerned about
spilturine (see above), one heard the doctor ask for a stent (see
above),and one having a procedure for cervical stenosis had a
“sensation of two flat surfaces moving on each other leaving
sharp, intense pain;felt sensation in the neck, sensation of
choking and felt bone beingcut away from the neck” (but despite the
report of noxious sensa-tions there is no mention of movement in
this unparalyzed patient).Apart from the patient whose surgeon
asked for a stent, it is notclear to us that the remaining
unparalyzed patients rememberedevents during anesthesia.
6. The authors explored several risk factors for awareness.
Wewould have benefited from an evaluation of two that were
nottested: 1. Did the choice of anesthetic affect the incidence of
aware-ness (IV versus inhaled)? 2. Did the use of neuromuscular
blockingdrugs increase the risk of awareness? These may be factors
of particular importance because, unlike demographic factors,
they areunder the control of the anesthetist.
We suggest that the report by Sebel et al. (1) may overestimate
theincidence of awareness during anesthesia. We suggest that
patientsadequately anesthetized with a potent inhaled anesthetic
(i.e., des-flurane, isoflurane, or sevoflurane at 0.5 MAC or
greater) have an
incidence of awareness that is vanishingly small.Dr. Eger is a
paid consultant to Baxter Healthcare Corp, the
manufacturer of desflurane.
Edmond I Eger II, MD James M. Sonner,
MDDepartment of Anesthesia and Perioperative CareUniversity of
California, San FranciscoSan Francisco,
[email protected]
References1. Sebel PS, Bowdle TA, Ghoneim MM, et al. The
incidence of awareness during anes-
thesia: a multicenter United States study. Anesth Analg
2004;99:833–9.2. Saucier N, Walts LF, Moreland JR. Patient
awareness during nitrous oxide, oxygen,
and halothane anesthesia. Anesth Analg 1983;62:239– 40.3. Sandin
RH, Enlund G, Samuelsson P, Lennmarken C. Awareness during
anaesthesia:
a prospective case study. Lancet 2000;355:707–11.
DOI: 10.1213/01.ANE.0000151467.79077.08
1544 LETTERS TO THE EDITOR ANESTH
ANALG2005;100:1537–49
-
8/20/2019 Dexamethasone Dose Attenuates Pain on Injection.87
9/13
In Response:
Drs. Eger and Sonner have raised interesting and worthwhile
ques-tions about our study that also pertain to most studies of
intraop-erative awareness.
Their first point is that the patient’s remembrance of
intraop-erative awareness should be unequivocally linked to an
intraop-erative event that can be corroborated. We agree that this
is themost convincing kind of evidence to have in a case of
intraoper-ative awareness. However, if we were to adhere to this
very highstandard of evidence, we would almost certainly
underestimatethe incidence of intraoperative awareness. Since the
patient’sinternal experience is subjective, it is impossible to
know the“true” incidence of intraoperative awareness. The most
inclusivestandard of evidence forintraoperativeawareness would be
simply thepatient’s belief that he or she was awake during surgery.
If the patient
believes t hat he or she was awake during surgery, and
there is noevidence to the contrary, how can we know that he or she
wasnot?
Because of the difficulty in judging the likelihood of
intraopera-tive awareness based on patients’ descriptions, we
divided thereports in our study into 2 categories, likely awareness
and possibleawareness, based on the investigators’ assessments of
the reports.Realizing the subjective nature of this data analysis,
we deliberately
published the descriptions of the likely awareness cases for
thereaders to judge on their own. We believe that the incidence
of awareness that we have reported is a reasonable estimate
and isunlikely to either greatly overestimate or underestimate the
trueincidence.
Eger and Sonner ask whether interviewing the patients in thePACU
and then at a later time might cause patients to falsely
reportintraoperative awareness. This seems unlikely to us. There
wascertainly no benefit of any kind to be gained for the patients
indoing so. The questions, which were repeated in the second
inter-view, may “jog” the patients’ memories by their repetition
but theydo not contain leading information that might cause “false”
mem-ories. The second interview was included specifically because
of previous studies showing that patients may not report an
episode of intraoperative awareness immediately following
surgery (1,2).
Eger and Sonner ask whether recall is more likely during IV
versus inhaled anesthesia. Unfortunately, because this study
wasnot designed to examine the effects of different anesthetic
drugs, thedrug data collected by the study are incomplete and we
are not ableto answer this interesting question.
Eger and Sonner state that the “5 patients [with putative
intraoper-ative awareness] who were not given neuromuscular
blocking drug-s. . .were presumably adequately anesthetized”. We
presume theymean because the patients had not received
neuromuscular blockingdrugs,and were apparently not movingduring
anesthesia, the patientsmust have been adequately anesthetized. We
do not agree with thisconcept. Reports of intraoperative awareness
occur in the absence of obvious clues to awareness, including
the absence of movement, tachy-cardia or hypertension, so the
absence of movement does not guaran-tee that the patient is
adequately anesthetized or will not have intra-operative awareness.
In fact, in the very case report cited by Drs. Egerand Sonner, a
patient not receiving neuromuscular blocking drugs had
a well-corroborated episode of intraoperative awareness without
anyapparent movement noticed by the anesthesiologist (3).Finally,
Drs. Eger and Sonner state that patients receiving potent
inhaled anesthetics at 0.5 MAC or greater have a “vanishingly
small”incidence of awareness. We are not sure what “vanishingly
small”means, but we believe that an incidence of intraoperative
awareness of 0.1%, or 1 in a 1,000 should be improved upon,
and there is little doubtthat patients would agree with us. We are
not aware of the evidencethat 0.5 MAC end tidal agent results in a
“vanishingly small” incidenceof awareness during surgery. While
isoflurane at 0.45 MAC preventedrecall in volunteers given verbal
stimuli, the authors noted that“whether the arousing effect of
surgery may increase the anestheticconcentrations required to
prevent conscious and unconscious mem-ory is not known” (4). Since
there are many cases of intraoperativeawareness that have been
reported in the presence of what appeared tothe anesthesiologist to
be adequate doses of potent volatile agent, and
because there is such enormous biological variation in
response to
anesthetic agents, we would advise caution in relying on any
particular“recipe” of drug or dose for avoiding intraoperative
awareness.
T. Andrew Bowdle, MD , PhDUniversity of Washington
Medical CenterSeattle, WA
Peter S. Sebel, MB BS, PhD, MBAEmory
University School of Medicine
Atlanta, GA [email protected]
Mohamed M. Ghoneim, MDUniversity of IowaIowa City, IA
Ira J. Rampil, MDSUNY Stony Brook, NY
Roger E. Padilla, MD Memorial Sloan-Kettering Cancer
CenterNew York, NY
Tong Joo Gan, MB BS, FRCA, FFARCSDuke
UniversityDurham, NC
Karen B. Domino, MD , MPH Harborview Medical
CenterSeattle, WA
References1. Sandin RH, Enlund G, Samuelsson P, Lennmarken C.
Awareness during anaesthesia:
a prospective case study. Lancet 2000;355:707–11.2. Nordstrom O,
Englstrom AM, Persson S, Sandin R. Incidence of awareness in total
iv
anaesthesia based on propofol, alfentanil and neuromuscular
blockade. Acta Anaes-thesiol Scand 1997;41:978– 84.
3. Saucier N, Walts LF, Moreland JR. Patient awareness during
nitrous oxide, oxygen andhalothane anesthesia. Anesth Analg
1983;62:239– 40.
4. Dwyer R, Bennett HL, Eger EI, Heilbron D. Effects of
isoflurane and nitrous oxide insubanesthetic concentrations on
memory and responsiveness in volunteers. Anesthe-siology
1992;77:888–92.
Concern About the Safety of IntrocanSafety® Intravenous
Catheters
To the Editor:Leading health care and health care worker safety
authorities, includ-ing the Association for Professionals in
Infection Control and Epide-miology, Occupational Safety and Health
Administration, and Centersfor Disease Control and Prevention have
advocated the adoption of passive sharps safety devices (1).
The passive Introcan Safety® IVCatheter (B. Braun Medical Inc.,
Bethlehem, PA) was purchased at ourinstitution to minimize
accidental needle sticks without requiring user
Figure 1. Introcan® Safety IV Catheter (22 gauge, 1 inch)
withseveral protuberances on the external surface.
ANESTH ANALG LETTERS TO THE EDITOR
15452005;100:1537–49
-
8/20/2019 Dexamethasone Dose Attenuates Pain on Injection.87
10/13
activation and to increase safety for both health care workers
andpatients. With the use of the FEP (hexafluoropropylene and
polytetra-fluoroethylene) catheters, we frequently noticed that
there are protu-
berances on the external surface of these IV catheters
(Fig. 1). Althoughno immediate adverse effect would be noticed,
this observation wouldremain a concern. FEP is associated with more
local tissuereaction thanpercutaneous venous (2), silicone (3), and
vialon (4–6) catheters. More
worrisome is that these particles observed on the external
surface of theFEP Introcan Safety® IV catheters can be detached
upon rubbing theexternal surface of the catheter and have the
potential to flow into the
bloodstream, in which case the consequences although not
docu-mented, may be at the least undesirable.
Claude Abdallah, MD , MScDivision of
AnesthesiologyChildren’s National Medical CenterWashington,
[email protected]
References1. Needle points: An AFSCME guide to sharps safety.
Washington, DC: American
Federation of State, County and Municipal Employees, 2002:1.2.
Reynolds J. Comparison of percutaneous venous catheters and Teflon
catheters for
intravenous therapy in neonates. Neonatal Netw 1993;12:33–9.3.
Reynolds JV, Walsh K, Ruigrok J, Hyland JM. Randomised comparison
of silicone
versus Teflon cannulas for peripheral intravenous nutrition. Ann
R Coll Surg Engl
1995;77:447–9.4. Jacquot C, Fauvage B, Bru JP. Peripheral venous
catheterization: influence of catheter
composition on the occurrence of thrombophlebitis. Ann Fr Anesth
Reanim 1989;8:620– 4.5. Gaukroger PB, Roberts JG, Manners TA.
Infusion thrombophlebitis: a prospective
comparison of 645 Vialon and Teflon cannulae in anaesthetic and
postoperative use.Anaesth Intensive Care 1988;16:265–71.
6. McKee JM, Shell JA, Warren TA, Campbell VP. Complications of
intravenous therapy:a randomized prospective study—Vialon vs.
Teflon. J Intraven Nurs 1989;12:288–95.
DOI: 10.1213/01.ANE.0000151469.79550.12
Can Capnography Substitute forAuscultation in Sedation Cases?To
the Editor:
Soto et al. (1) found that the frequent apneas that occurred
during IV
sedation were readily detected by capnography but “none
weredetected by the anesthesia providers.” This is not surprising,
sincethe anesthesia providers were not using continuous
auscultation,and thus were constrained to recognize apnea visually.
Had theyused a simple precordial stethoscope placed in the
suprasternalnotch, I suspect that not only would all cases have
been detected,
but also before the 20-second lapse required for a
CO2-based apneaalarm. Conceivably, an obstructive apnea lasting
more than 20seconds could evolve to negative pressure pulmonary
edema.
Auscultation is effective in detecting partial airway
obstruction,which often precedes complete obstruction, and
hypoventilationpreceding central apnea. Diminished and absent
breath sounds areimportant findings! Of course, auscultation is not
subject to lapseswhile the machine recalibrates.
Although modern electronic monitors have brought basic
physi-ology into clinical management, they still do not substitute
for the
basic vigilance principle to “always stay in contact with
the patient.”Possibilities include visual inspection, auscultation,
hand on a
breathing bag, or voice contact during light sedation. The
authorsdismissed auscultation by noting that its use has been
declining inrecent years. Their conclusion urging research into
methods todiagnose antecedents of adverse outcomes might include
teachingeffective “hands-on” vigilance skills. Continuous
auscultation witha well-fitted earpiece is unencumbering and best
of all, providesabundant, free information about the patient not as
easily obtainedotherwise.
Quentin A. Fisher, MD, FAAPProfessor of Anesthesia
and PediatricsDirector, Pediatric Anesthesia
Medstar-Georgetown University HospitalWashington, DC
[email protected]
Dr. Soto does not wish to respond.
Reference1. Soto RG, Fu ES, Vila H Jr, Miguel RV. Capnography
accurately detects apnea during
monitored anesthesia care. Anesth Analg 2004;99:379– 82
DOI: 10.1213/01.ANE.0000151470.50760.4A
Accidental Epidural Injection of PancuroniumTo the
Editor:
A 41-year-old man, 51 kg, ASA status I, was scheduled for
antero-posterior resection due to cancer of the rectum. Combined
epidural-general anesthesia was planned. The epidural catheter was
success-fully placed at L2–3 interspace through the 18-gauge Tuohy
needleafter the “ loss of resistance to air technique.”
Before induction of general anesthesia, pancuronium (4 mg)
wasaccidentally injected through epidural catheter instead of
fentanyl100 g.
After induction of general anesthesia with thiopental 5
mg/kg,
the syringe of pancuronium that was prepared for intubation
wasfound to be empty. The trachea was then intubated after
IVpancuronium 0.1 mg/kg and anesthesia was maintained withN2O,
O2, halothane. Neuromuscular blockade was monitored
byacceleromyography using train-of-four (TOF-watch®,
Organon(Ireland) Ltd, Swords, Dublin, Ireland) mode. The operation
wasuneventful and lasted for 3 h. No added neuromuscular
blockadefor the entire procedure after the first dose. The patient
started to
breath spontaneously during suturing the skin.
Neuromuscular blockade was reversed with IV neosti gmine 0.04
mg/kg andatropine 0.02 mg/kg at the end of the operation. TOF
ratios were0.4 after 10 min and 0.86 after 25 min, respectively.
The tracheawas extubated 30 min later.
He was discharged from the PACU at the 7th postoperative
hourwithout any adverse effects and from the hospital on the
14thpostoperative day. He had been followed up for 2 months and
there
were no clinical signs of neurotoxicity.Local anesthetics,
opioids, and steroids are commonly injectedinto the epidural space
in medical practice. In the history of regionalanesthesia, various
substances have been accidentally injected intoepidural space, with
consequences ranging from no clinical effect toirreversible
paralysis (1–4). To our knowledge, no data about acci-dental
injection of pancuronium through an epidural catheter inhuman were
documented in the literature. In this report, we admin-istered
pancuronium both IV and epidurally. We found that thetime from
injection of pancuronium epidurally to recovery at TOFratio of 0.86
was 230 min while the action of pancuronium injectedIV was normally
lasted for 60–90 min (5). No data on the rate of absorption of
pancuronium from the epidural space was found inthe literature.
Neuromuscular blocking drugs cause excitement andseizures when
introduced into the central nervous system (6–8).Acute intrathecal
administration of these drugs leads to dose-
dependent central nervous system effects in the rat (6). Because
noclinical or experimental data exist about interaction between
pan-curonium and other drugs injected epidurally, no other
drugsshould be given at this site.
Although we injected saline into the epidural space to
acceleratesystemic absorption of pancuronium (“volume effect”),
there is nosufficient evidence in the literature that this maneuver
is effective (9).
In conclusion, the anesthesiologist must be careful during
admin-istration of the anesthesia, as human error can be
catastrophic to thecare of patients.
Janjira Krataijan, MDNawal Laeni,
MDDepartment of AnesthesiologyFaculty of MedicinePrince of Songkla
University
Hadyai, [email protected]
1546 LETTERS TO THE EDITOR ANESTH
ANALG2005;100:1537–49
-
8/20/2019 Dexamethasone Dose Attenuates Pain on Injection.87
11/13
References1. Shanker KB, Palkar NV, Nishkala R. Paraplegia
following epidural potassium chloride.
Anaesthesia 1985;40:45–7.2. Dahl JB, Jacobsen JB. Accidental
epidural narcotic overdose. Anesth Analg 1990;70:
321–2.3. Dror A, Henriksen E. Accidental epidural magnesium
sulfate injection. Anesth Analg
1987;66:1020–1.4. Whiteley MH, Laurito CE. Neurologic symptoms
after accidental administration of
epidural glucose. Anesth Analg 1997;84:216–7.
5. Savarese JJ, Caldwell JE, Lien CA, Miller RD. Neuromuscular
blockade. In: Miller RD,ed. Anesthesia. 5th ed. Philadelphia:
Churchill Livingstone, 2000:412–90.
6. Szenhradszky J, Trevor AJ, Bickler P. Central nervous system
effects of intrathecalmuscle relaxants in rats. Anesth Analg
1993;76:1304–9.
7. Cardone C, Szenohradszky J, Yost S, Bickler PE. Activation of
brain acetylcholinereceptors by neuromuscular blocking drugs: a
possible mechanism of neurotoxicity.Anesthesiology
1994;80:1155–61.
8. Scheepestra GL, Vree TB, Crul JF. Convulsive effects and
pharmacokinetics of lau-danosine in the rats. Eur J Anaesthesiol
1986;3:371–83.
9. Kostopanagiotou G, Mylona M, Massoura L, Siafaka I.
Accidental epidural injection of vecuronium. Anesth Analg
2000;91:1550–1
DOI: 10.1213/01.ANE.0000151471.73967.52
Peripheral Nerve Blocks for PostoperativePain Relief After Total
Knee Replacement:
More Questions Than AnswersTo the Editor:
Singelyn et al. (1) reported that a continuous three-in-one
femoralnerve block (CFNB) would facilitate rehabilitation after
total kneereplacement (TKR). While some authors argue that it would
be essen-tial to add an obturator nerve block to the CFNB, others
have reportedthat over 80% of the patients had better postoperative
analgesia whena continuous sciatic nerve block is added to a CFNB
(2,3).
We have compared continuous posterior lumbar (psoas
com-partment) blocks (CPCB) and CFNB with a simple morphine IVPCA
in a randomized prospective study that included 60
patientsundergoing TKR (4). The obturator nerve was blocked in a
sig-nificantly higher percentage of patients with the CPCB
technique(90 vs 47%), but during the first 48 h, morphine
consumption wasthe same for the two types of continuous nerve
blocks (36.1
25.8 vs 37.3 34.7 mg, mean sd). Verbal analogical pain
scoresmeasured at rest (6, 24, and 48 h) and during physiotherapy
werealso comparable for these two groups (4). Although our studywas
not designed to compare the effects of these two regionalanesthesia
techniques on rehabilitation, from the data that can
beretrospectively retrieved from the charts of these patients one
cansee that the difference in the amplitude of the knee flexion
between the CFNB group and the PCA group was small and
didnot last beyond the first few days and that there was
absolutelyno trend toward a faster rehabilitation in the CPCB group
com-pared with the CFNB group (Fig. 1). Furthermore, the number
of patients who achieved a 90-degree flexion at 7 days (PCA:
58.3%,CFNB: 66.7%, and CPCB: 60%) and the length of
hospitalization(PCA: 7 days [5–30 days], CFNB: 7 days [5–13 days],
and CPCB:7 days [5–15 days], median [range]) was not improved by
any of the two regional anesthesia techniques.
Since there is an inherent risk of complication with any
techniqueand because the addition of any of them would, at least
theoreti-cally, increase the number of related complications, it
would appearessential to evaluate the real benefits of these
proposed combina-tions of peripheral nerve blocks (single shot or
continuous) not onlyin term of reduced need for opioids
administration, but also in theirreal ability to facilitate
rehabilitation.
Joanne Guay, MD, FRCPClinical Associate
Professor, AnesthesiaUniversity of Montreal
Montreal, Quebec, Canada [email protected]
Drs. Singelyn and Bouziz do not wish to respond.
References1. Singelyn FJ, Deyaert M, Joris D, et al. Effects of
intravenous patient-controlled anal-
gesia with morphine, continuous epidural analgesia, and
continuous three-in-one block on postoperative pain and knee
rehabilitation after unilateral total knee arthro-plasty Anesth
Analg 1998;87:88–92.
2. Macalou D, Trueck S, Meuret P, et al. Postoperative analgesia
after total knee replace-ment: the effect of an obturator nerve
block added to the femoral 3-in-1 nerve blockAnesth Analg
2004;99:251–4.
3. Ben-David B, Schmalenberger K, Chelly JE. Analgesia after
total knee arthroplasty: iscontinuous sciatic blockade needed in
addition to continuous femoral blockade?Anesth Analg
2004;98:747–9.
4. Kaloul I, Guay J, Côt é C, Fallaha M. The posterior lumbar
ple xus (psoas compartment)and the three-in-one femoral nerve block
provide similar postoperative analgesia aftertotal knee
replacement. Can J Anaesth 2004;51:45–51.
DOI: 10.1213/01.ANE.0000151472.37849.81
In Response:
Dr. Guay’s recent paper on analgesia following total knee
re-placement (1) demonstrated (a) approximately a 50% reduction
inopiate consumption with both CFNB and CPCP, (b) a small but
statistically insignificant further reduction in opiate
consumptionwith CPCB versus CFNB, (c) a significant reduction in
VAS scoreat rest with both techniques, (d) a small but
statistically insignificantfurther reduction in VAS with CPCB
versus CFNB, and(e) no reduction in VAS with physical therapy. We
accept these data asvalid and feel they support our own experience
and published work(2). That is, we agree with and accept the
conclusion that beyond theanalgesia of femoral blockade, obturator
blockademakes only a limitedcontribution to analgesia following
TKR.
However, Dr. Guay would have been wise to limit her conclu-sions
to the question posed by their study—as to the relative anal-gesic
contribution of obturator blockade. We believe that their
pa-tients’ opiate needs would have been much further reduced and
theanalgesia during PT far more effective had they added
continuoussciatic blockade to their protocol. Furthermore, neural
blockadedoes not alter the inflammatory response and sensitization
(central
or peripheral) and will be far more effective if combined with
COX-2
Figure 1. Effects of postoperative analgesic technique on
the recoveryof knee flexion after total knee replacement.
Retrospective data re-trieved from patients’ charts. PCA: IV
morphine patient controlledanalgesia (PCA) alone; CFNB: IV morphine
PCA plus continuousthree-in-one femoral nerve block; CPCB: IV
morphine PCA plus continu-
ous posterior lumbar plexus (psoas compartment) block. Mean
sd
.
ANESTH ANALG LETTERS TO THE EDITOR
15472005;100:1537–49
-
8/20/2019 Dexamethasone Dose Attenuates Pain on Injection.87
12/13
inhibition (3). Where Dr. Guay sees a failed technique (neural
block-ade) we see a failure to use the technique properly. One may
not beable to travel far in a car with one wheel, but that does not
leavewalking as the only option. One might try attaching the other
wheels.
More disturbing than extrapolating beyond the limits of her
workis Dr. Guay’s use of dubious retrospective “outcome data.” This
isworse than meaningless. It is misleading. For example, how do
we
know that the physical therapists didn’t actually measure but
sim-ply approximated flexion? Would that not lead to fairly
routinizedcharting, thus making any comparative data worthless? The
ex-tremely long hospitalizations of 7 days suggests that hospital
staywas dictated by standard practice rather than by a set of
dischargecriteria, thus debasing any conclusion as to the influence
of analge-sia technique on hospital length of stay. As she herself
noted, theirstudy was not designed to assess rehabilitation. That
was correct.She should have heeded her own caution.
On the basis of false extrapolation, meaningless data, and
suppo-sition (as to complications), Dr. Guay would admonish us to
recon-sider the use of neural blockade as a postoperative analgesic
tech-nique. We would admonish her to be more careful with such
baseless, sweeping, and hubristic commentary.
Bruce Ben-David, MD Jacques E. Chelly, MD,
PhD , MBA
Department of AnesthesiologyUniversity of Pittsburgh Medical
CentersPittsburgh, [email protected]
References1. Kaloul I, Guay J, Côt é C, Fallaha M. The
posterior lumbar ple xus (psoas compartment)
and the three-in-one femoral nerve block provide similar
postoperative analgesia aftertotal knee replacement. Can J Anaesth
2004;51:45–51.
2. Ben-David B, Schmalenberger K, Chelly JE. Analgesia after
total knee arthroplasty: iscontinuous sciatic blockade needed in
addition to continuous femoral blockade:Anesth Analg
2004;98:747–9.
3. Buvanendran A, Kroin JS, Tuman KJ, et al. Effects of
perioperative administration of aselective cyclooxygenase 2
inhibitor on pain management and recovery of functionafter knee
replacement: a randomized controlled trial. JAMA
2003;290:2411–8.
Does Paralysis Contribute to AwarenessUnder Anesthesia?To the
Editor:
Sebel et al. (1). deserve commendation for their prospective
study of awareness during general anesthesia. The study
validated someclinical suspicions (sicker patients undergoing
emergent operationsare at high risk) but not others (females are
not at higher risk; theeffect of BIS monitoring is
undetectable).
One clinical suspicion was not directly addressed. Many
clini-cians believe an unparalyzed patient is the best protection
againstrecall: presumably an inadequately anesthetized patient will
move,provoking more anesthetic before recall occurs. However, this
ismerely intuition. Table 4 in their article lists the 25 patients
withfrank recall. Four patients did not receive muscle relaxants
while 19(80%) did (one patient lacked documentation). If the
authors candetermine what percentage of all participating patients
receivedmuscle relaxants, they may provide a long-awaited answer to
sup-plant a clinical practice based on faith alone.
Samuel Metz, MDOregon Anesthesiology GroupPortland,
[email protected]
Reference1. Sebel PS, Bowdle TA, Ghoneim MM, et al. The
incidence of awareness during anes-
thesia: multicenter United States study. Anesth Analg
2004;99:833–9
DOI: 10.1213/01.ANE.0000151474.73594.80
In Response:
We thank Dr. Metz for his interest in our study and question
concern-ing the relationship of awareness under general anesthesia
and neu-romuscular blockade. As Dr. Metz points out, 5 patients in
our study
had intraoperative awareness despite the lack of neuromuscular
block-ing agents. Although our study was not designed to evaluate
therelationship of awareness with anesthetic agents, our limited
data forapproximately half of the study patients suggests that
neuromuscular
blockade was used in 65% percent of the study patients.The
fact that awareness can occur in a patient who is fully capable
of movement is well described in a study of nearly 12,000
Swedish
patients by Sandin et al. (1). The incidence of awareness was
0.10%in the absence of neuromuscular blocking drugs (4 patients),
com-pared with 0.18% in the presence of neuromuscular blockade
(14patients). In addition, other studies have observed awareness
andrecall in the absence of neuromuscular blockade (2). While
nonpara-lyzed patients may recall intraoperative events, they may
less likelyto describe severe pain or anxiety than patients who are
incapable of movement. Sandin et al. (1) found that none of
the 4 nonparalyzedpatients had anxiety during the period of recall
or postoperativenightmares and anxiety. However, the long-term
outcome of pa-tients with intraoperative awareness is unclear, as
these investiga-tors found a surprising number of psychological
sequelae afterintraoperative awareness in a 2-year postoperative
follow-up of their patients (3). In fact, two of the patients
who had been awareduring nonrelaxant anesthesia and had denied
nightmares in theimmediate postoperative period, developed moderate
symptoms of
posttraumatic stress disorder.Thus, awareness with recall during
general anesthesia can occurin the absence of neuromuscular
blockade. While these episodesmay be associated with less pain or
anxiety than in the paralyzedpatient, the ultimate psychological
outcome is unclear.
Peter S. Sebel, MB BS, PhD, MBAEmory
University School of Medicine
Atlanta, GA [email protected]
T. Andrew Bowdle, MD , PhDUniversity of Washington
Medical CenterSeattle, WA
Mohamed M. Ghoneim, MDUniversity of IowaIowa City, IA
Ira J. Rampil, MD
State University of New York Stony Brook, NY
Roger E. Padilla, MD Memorial Sloan-Kettering Cancer
CenterNew York, NY
Tong Joo Gan, MB BS, FRCA, FFARCSIDuke
UniversityDurham, NC
Karen B. Domino, MD , MPH Harborview Medical
CenterSeattle, WA
References1. Sandin RH, Enlund G, Samuelsson P, Lennmarken C.
Awareness during anaesthesia:
a prospective case study. Lancet 2000;355:707–11.2. Wennervirta
J, Ranta SOV, Hynynen M. Awareness and recall in outpatient
anesthesia.
Anesth Analg 2002;95:72–7.3. Lennmarken C, Bildfors K, Enlund G,
et al. Victims of awareness. Acta Anaesthesiol
Scand 2002;46:229–31.
Dexamethasone Dose Attenuates Pain onInjection Following
DiazepamHydrochlorideTo the Editor:
To test the hypothesis of whether a prior injection of
dexamethasoneattenuated or abolished pain following diazepam
injection, we con-ducted a randomized, prospective, double-blind,
placebo-controlledclinical trial to compare dexamethasone,
metoclopramide, and nor-mal saline in 120 ASA class I and II men
aged 20–45 years. Thesubjects were randomly allocated into one of
the three groups:
1548 LETTERS TO THE EDITOR ANESTH
ANALG2005;100:1537–49
-
8/20/2019 Dexamethasone Dose Attenuates Pain on Injection.87
13/13
Group 1: 2 mL IV normal saline in one hand and 2 mL
dexa-methasone in the other, simultaneously.
Group 2: 2 mL IV normal saline into one hand and 2 mL
meto-clopramide in the other, simultaneously.
Group 3: 2 mL IV metoclopramide in one hand and 2 mL
dexa-methasone in the other, simultaneously.
After 30 seconds, diazepam hydrochloride was injected
simulta-neously into each of patients’ hand veins, and maximal
VerbalAnalog Scale (VAS) was assessed for discomfort. In Group 1,
themean of VAS for pain was significantly less in dexamethasone
thansaline pretreatment (P 0.001), whereas in Group 2,
metoclopra-mide pretreatment had significantly more effect than
saline in re-ducing pain (P 0.001). In Group 3, the
pain observed on abovescale was significantly less in dexamethasone
than metoclopramide.In conclusion, although both dexamethasone and
metoclopramideproved effective in reducing the severity of pain
following diazepam,the former proved to be more efficacious.
Efficacy of metoclopramidein reducing pain on injection following
diazepam is clear (1).
Ali Movafegh, MDFarid Abolhasan Gharehdaghi,
MDZahid Hussain Khan, MDGita Shoeibi, MD
Department of Anesthesiology and Critical CareDr. Ali Shariati
HospitalTehran University of Medical SciencesTehran, Iran
[email protected]@movafegh.com
Reference1. Majedi H, Rabiee M, Hussain Khan Z, Hassannasab B. A
comparison of metoclopra-
mide and lidocaine for preventing pain on injection on diazepam.
Anesth Analg2002;95:1297–9.
DOI: 10.1213/01.ANE.0000151567.76745.A6
Airway Obstruction Due to a Damage tothe Laryngeal MaskTo the
Editor:
Drs. von Urgern-Sternberg and Erb reported a case of
airwayobstruction during the use of a size 2 laryngeal mask airway
due
to an unnoticed detachment of the cuff weld near the device
tip(1). There have already been several reports of the same
problem(2–4).
The authors were surprised to hear that the manufacturer
claimedthe incident was “user’s fault,” because such a deformity
may occurduring sterilization if air or moisture is in the cuff
(1). If 1–2 mL of air is remaining in the cuff, air may expand
by 20 times (up to
40 mL) during sterilization (5). This volume should be no
problemfor a size 3 or larger (6), but could in theory decrease the
integrity of the cuff of a size 2 or smaller. Water in the
cuff evaporates