Embed Size (px)
Citation preview
Devising an Algorithm for early recognition & management of
Urinary Retention in the Rotunda Hospital
Mary O’Reilly Midwifery Practice Co-ordinator
26th April 2016
Urinary Retention • Defined as the inability to completely or partially empty the bladder.
Overt
• Symptomatic inability to void spontaneously within six hours of birth or removal of IDC.
– Straining to void/decreased sensation to void
Covert
• Non symptomatic increased post void residual volumes >150mls after birth or removal of IDC.
– May be passing small volumes
• Common in the pregnancy/ post natal period
– Incidence varies from 0.05 to 37%
– Short term complications – Recurrent UTI’s
– Long term complications – Permanent voiding dysfunction (Lim 2010)
Risk factors for urinary retention • Primiparity
• Epidural
• Episiotomy
• Assisted birth
• Prolonged 1st and 2nd stage of labour
• Baby birth weight >4kg
• Perineal trauma and pain
• Over distension of bladder >700mls during delivery
• Communication barriers (Yip et al 2005)
Clinical Audit
Urinary Retention
• Key findings: Inconsistency in diagnosis and management
• Conflict between midwives and doctors regarding treatment
PLAN: Standardized evidence based approach for management
Review of the literature and develop an algorithm to guide decision making
Education package for clinical department staff
GOAL: Decrease Urinary Retention and long term damage for the women
Re-audit: 6 month period following education to assess improvement in uniformity of management
Why an Algorithm • Method for solving a problem or
achieving a specific goal. It has one or more finite steps
• A systematic process consisting of an ordered sequence of steps, each step depending on the outcome of the previous one
• Use has been identified as an effective method to impart knowledge and guide decision making (Rathbun & Sahd 2009)
Development
– Multidisciplinary team involved
– The algorithm defined UR and post void residual, voiding efficiency, when and how to assess the patient, when to catheterize and success
– Review of previous cases of UR, feedback from midwifery and medical staff, literature search
– User friendly and easy access of algorithm for all staff
Implementation – Midwifery staff engaged with in- service education,
• Physiology of the urinary tract
• Normal voiding function
• Complications and techniques to monitor and diagnose malfunction of voiding process
– Communication with the medics - awareness of algorithm
• Lead champions identified at ward level
• Involvement of multidisciplinary team
• Education of patient
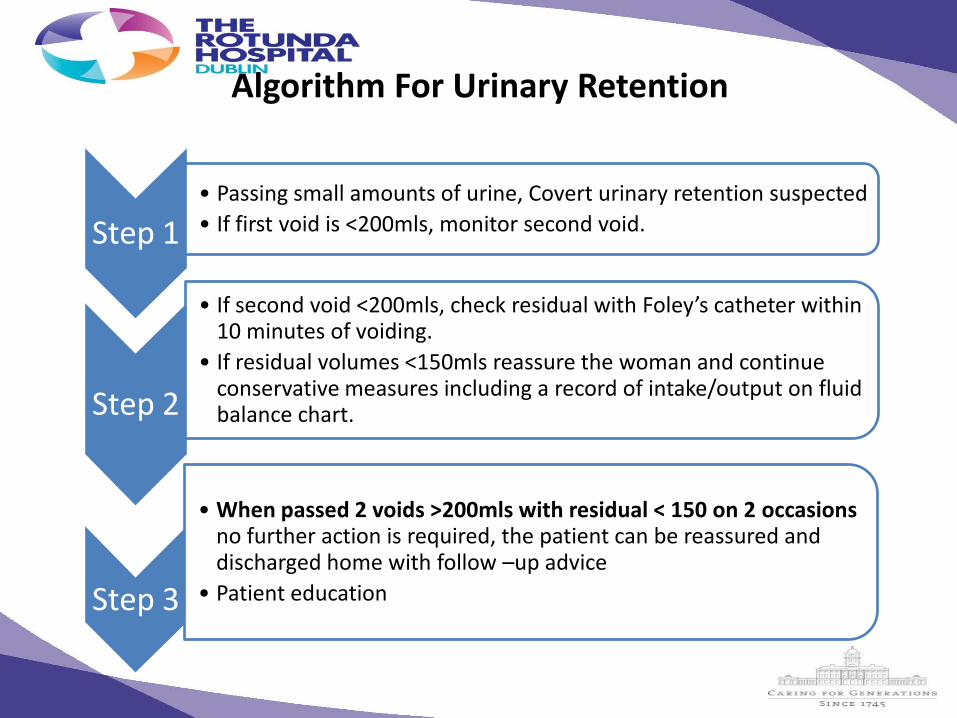
Algorithm For Urinary Retention
Step 1 • Passing small amounts of urine, Covert urinary retention suspected
• If first void is <200mls, monitor second void.
Step 2
• If second void <200mls, check residual with Foley’s catheter within 10 minutes of voiding.
• If residual volumes <150mls reassure the woman and continue conservative measures including a record of intake/output on fluid balance chart.
Step 3
• When passed 2 voids >200mls with residual < 150 on 2 occasions no further action is required, the patient can be reassured and discharged home with follow –up advice
• Patient education
Evaluation
Use of the algorithm was evaluated by:
1. Time of first void following birth of baby
2. Measurement of the 1st two voids
3. Measurement of residual urine
4. Use of continuous/ intermittent catheterisation
5. Measurement of voiding efficiency
6. Urinary retention greater than 500mls
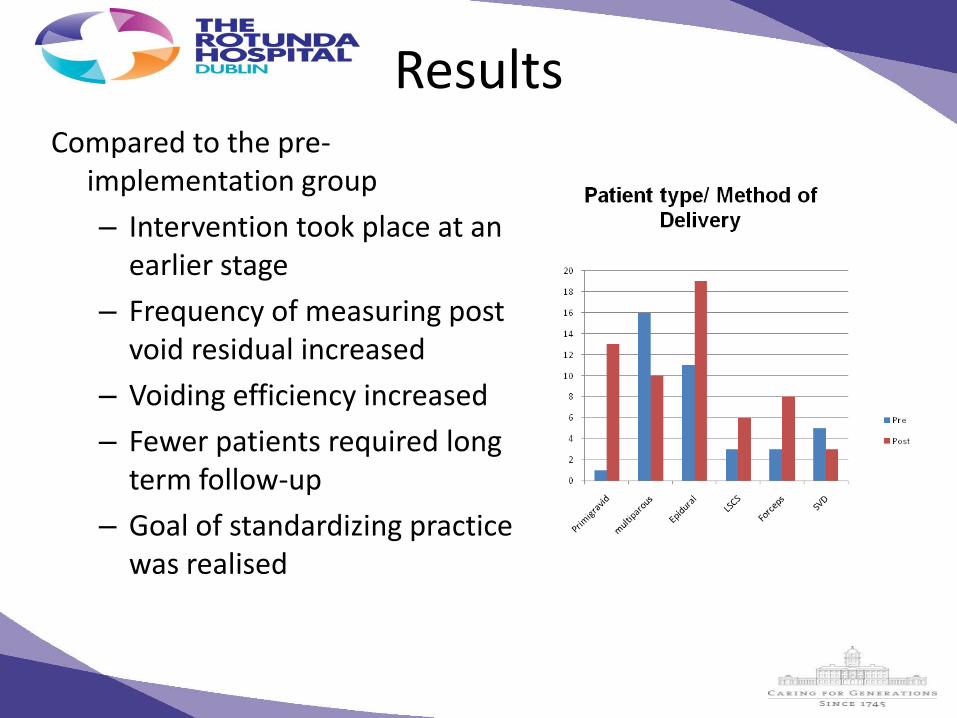
Results Compared to the pre-
implementation group
– Intervention took place at an earlier stage
– Frequency of measuring post void residual increased
– Voiding efficiency increased
– Fewer patients required long term follow-up
– Goal of standardizing practice was realised
Challenges
• Limited availability of staff to attend education
• Documentation
• Requires ongoing analysis for sustainable change in practice and outcomes
Conclusions
• Since the introduction of the algorithm significant improvement in the management of urinary retention
• Decision aid for better safer care
• Facilitates translation of evidence into midwifery practice at the bedside
• Enhanced clinical decision making
• Use as a teaching tool
References • Lim JL. Post-partum voiding dysfunction and urinary retention. Aust N Z J
Obstet Gynaecol. 2010;50:502–5.
• Rathbun, M C & Ruth-Sahd, LA (2009) Algorithmic tools for interpreting vital signs. Journal of Nursing Education 48(7) 395-400
• Yip, S., Sahota, D., Pang, M., & Chang, A. (2005). Screening test model using duration of labour for the detection of postpartum urinary retention. Neurology and Urodynamics, 24, 248-253
• Yip, S., Sahota, D., Pang, M., & Chang, A. (2004). Postpartum urinary retention. Acta Obstetricia et Gynacologica Scandinavica, 83, 887-891