Embed Size (px)
Citation preview

HAL Id: tel-00862466https://tel.archives-ouvertes.fr/tel-00862466
Submitted on 16 Sep 2013
HAL is a multi-disciplinary open accessarchive for the deposit and dissemination of sci-entific research documents, whether they are pub-lished or not. The documents may come fromteaching and research institutions in France orabroad, or from public or private research centers.
L’archive ouverte pluridisciplinaire HAL, estdestinée au dépôt et à la diffusion de documentsscientifiques de niveau recherche, publiés ou non,émanant des établissements d’enseignement et derecherche français ou étrangers, des laboratoirespublics ou privés.
Développement du pancréas humain embryonnaire exvivo / in vivo : La greffe musculaire : un nouveau
modèle d’étude longitudinale et dynamiqueCarmen Capito
To cite this version:Carmen Capito. Développement du pancréas humain embryonnaire ex vivo / in vivo : La greffemusculaire : un nouveau modèle d’étude longitudinale et dynamique. Médecine humaine et pathologie.Université René Descartes - Paris V, 2013. Français. <NNT : 2013PA05T015>. <tel-00862466>

- Année
�
���������ABC���AD��EC����A
�����������A���B�CDE������������AB�AB����������AB�
A
CDE�F�����������������D����������
����������������E�E�����E�E��
���������������F����� �������E�������!F���"D�����F����������F�����
������#����
FA����F������
F����A��A��E���C�A��A�E���E��A��A�CA���A��A��A�CA�C��A
D��E������A�AB�����������D�����������AA
D�����A�C�A�C��C��A�E�C���C��A
Présentée et soutenue publiquement le 26 juin 2013
Devant un jury composé de :
���������AB�CADE��F������� � � � ����A��D�����������������A��ACD��AD���E������� � � � �C����������������ADA ���!����"AE�#�F������� � �C���������
������"�����#C$$�D�E������� � � � %&C�ADC���������DD��$A�����$�'�(��E��F������� � � %&C�ADC����������C��C�$�)*�C�+�CDDE������� � � �A��*����������,���

- Année
�
�
�
���������
�
�������� ��� ��D������ �� �D�D!� ��� �A� ���A�"�#� �A� ���$�"���D����������A�D�����%�D� � D������ ���
��&���$$������$A���A�D%���"��AD������� �A�����$������'$�������A������$"'�D�$A�"��� D%����
�����A�A�D������$A���A�����$�����&���$$������A$$��"����"�A$���D%����D���&A����(��������#�
A���� %��� �A� �������� )��A� ��� �� ���� ��� �A� �������� )��A� "��AD��� $A�A ���� ��� A��� ���)�� ���
�D�D�D�����#� ���AD������������ D��D%������ A������������D!!��������A%���������� ������$*���(�
+,A)����������'��*�����-$�D����A�-� �)������ #���$A�D�����A��D���"��AD�#��,A�$A��$��D�����
�-A�������AD���������&���$$������$A���A�D%���"��AD��.��%����$�����(�EA�������A)�A��D�#�D��A�
����$�����������&A�D���������*������-��� �!!�����$A���A���D��A����"��AD��������A��A$�����
��A��� ��� ���D�� D������D����$�������� /F�E(� ��� A� ���� �������� %��� ����D��D� $�����AD�� ���
��A$D����� �������)��� ���� ��A$��� ��� ��&���$$������ �����D��� "��AD�(� 0�A���D��� ��� �D��� ���
�!!���D�D�AD������$���D)D�D����������D!D�������&���$$�����#����A������$A�D�!���D���&DA��(��
EA��� ��� �A&AD�#� ����� A&���� ��&���$$�� ��� &A�D��� ��� ���&�A�� �D��� ��� �!!�� �A��� ��� �������
�%������D%��#�$�����D�$������$������$�!D�D��(��������#����������������%��D������$���D)����������
���$A���A��"��AD��$A�D����������A�� ��D%��� ���E�E������A�D�A�������A��!������ *�������D��
$A���������D&D��#�A$*��D�.���D����D���������A������D���&DA����A������ �!!��(�F�����*������ �!!��
�A������������������������&�����A$$��"��$�����A�������&D�A ���������������� D���D�A���#��A���
���%������� D�� ��AD�� $���D)��� ������D�� �A� � ��A�D��� ��� ���AD��� *���� ��� ��� ��&��D� ���
���AD�����D ������A%�����$A����� *����A$$������A$$�����$A����&D������D!!��������A�������
��&���$$������
�
�D�����1��A����)'��D��$A���A����&���$�����D��A��-�&D&�2D��&D&���������
�
�)��A������
�
3"D���� �$�A�D�� "��A�� ����D�� ����D��� "A&�� $��D����� ����� ���$AD����� )��4���� ������ A���
"��A�� $A���A�D�� ��&���$����#� �"�� �A�5� �!� A� �)���� �-$�D����A�� �'����� "A�� ���� $��D�����
���AD���� �-A�D�A�D��� �!� "��A�� $A���A�D�� ��&���$����(� 3�� $�&D����'� ��&���$��� A� -��� A!��
������ �!� D��A���� "��A�� !��A�� $A���A�� A!���� ����� �"�� 5D���'� �A$����� �!� D������
D����$������ �D��#� 4"D�"� A���4��� �"�� ��&���$����� �!� "��A�� $A���A�D�� )��A� �����(� 1��#� 4��
���$A��� �"�� ��&���$����� �!� "��A�� A��� ��D��� !��A�� $A���A�D�� A!��� �D�"�� ����� �5����A��
��������$D�'�D�����������"����A���A$����(�3���������A�����"A��"��A��$A���A�D��)��A������
��&���$����� �����6� )��"� )'� �D!!����DA�D��� �!� $A���A�D�� $� ��D���� A��� )'� $��D!�A�D��� �!�
��&���$D� � )��A� �����(� � �"�� ��$�!D�DA�� ���A�D����!� �"�� �5����A��������� A!�� A��� D��� �A�D�� A������
$��D����� D�� &D&�� ����D&D������DA���� ���� �A��!��4"D�"� �A ����� �$��D!D�� �����(� �"D�������� �!�
�� A!������ ����� �"�� �5����A�� ������� �$D�'�D��� D�� A� ��4� A$$�A�"� !�� ��� D���D�A�� ����D��#�
4"D�"� A���4�� ���A�D7��� �A�D$��A�D��� ��� �����D��� �"�� � ��A�D��� �!� "��A�� $A���A�D��
��&���$����(�
�
�
8�������������
�A���A�#�E�&���$$�����#��A�� ��*��#�9��� �!!�#�
�
:�'4������
�A���A�#�E�&���$����#��A�� ����D�#�9��� A!��

�
�������������
A mon jury de thèse :
Je tiens en premier lieu à remercier Raphael Scharfmann, mon directeur de thèse :
tu m’as accueillie dans ton laboratoire il y a un peu plus de 4 ans. Après deux ans à
plein temps, j’ai dû reprendre mes activités cliniques. Concilier le clinicat et la thèse
n’a pas été chose facile mais tu as fait preuve de patience à mon égard et surtout tu
as su trouver les bonnes personnes pour m’aider à achever ce travail. J’ai beaucoup
appris à ton contact, notamment une certaine rigueur de raisonnement que j’espère
pouvoir retranscrire dans mon activité clinique mais aussi dans mon activité de
recherche à venir qui, je l’espère, passera par la poursuite d’une collaboration avec
ton équipe.
Au moment d’achever la première étape de mon parcours académique scientifique,
je tiens à remercier Monsieur Yves Aigrain, de m’avoir donné l’opportunité de
réaliser cette thèse, en me présentant à Raphael mais aussi en me libérant, autant
que possible, de mes activités cliniques ces deux dernières années. Je vous remercie
aussi d’avoir accepté de présider cette thèse. J’espère poursuivre cette activité de
recherche au sein de votre équipe médicale.
Je vous remercie Christian Pinset d’avoir pris sur votre temps pour rapporter cette
thèse et je suis fière de vous compter parmi les membres de mon jury.
Je tiens à remercier Dominique Berrebi d’avoir accepté de rapporter cette thèse :
chère Dominique, pendant mon passage à Robert Debré, j’ai eu la joie de travailler
avec toi au quotidien et de me rendre compte de la grande chance qu’avaient les
équipes chirurgicales de cet hôpital de te compter à leur côté.

�
Je tiens à remercier Roberto Mallone d’avoir accepter d’examiner ce travail. Vos
travaux sur l’immunopathologie du diabète et sa génétique me rendent fière de vous
compter dans mon jury de thèse.
Madame Delezoïde, vous ne vous souvenez certainement pas mais, encore jeune
étudiante de médecine, j’attendais vos cours d’embryologie avec impatience et, en y
assistant, découvrait la « magie » de cette spécialité. Si certains enseignants sont
capables de transmettre leur passion pour leur spécialité, vous comptez certainement
parmi ceux là et, pour moi, aux toutes premières places. J’ai découvert et pris goût à
l’embryologie avec vous et je vous redis encore la fierté que j’ai de vous compter
dans les membres de mon jury.
Aux collègues du laboratoire :
Je tiens en premier à remercier Marie Thérèse Gage Soufflot : chère MT, si ce
surnom d’agent secret que je t’ai donnée te va si bien (en tout cas je trouve !!!) c’est
que tu es capable, en un temps record, d’extraire des données majeures d’un fouillis
de manip générées par une thésarde dans le rush tous les lundi….. Je me dois d’une
idée initiale et le reste je te le dois. Je tiens vraiment à t’exprimer ici toute ma
reconnaissance (éternelle….) pour l’aide apportée pour l’analyse de ce nouveau
modèle.
Virginie Aiello Lorenzo : tu m’as fait faire mes premiers pas à l’animalerie des
SCID, tu m’as appris que même si ce n’était que des souris il fallait respecter
certaines règles, tu m’as montré comment greffer sous la capsule rénale (si fine !!!!)
les pancréas fœtaux. Tu m’as accompagnée ensuite pour les greffes musculaires, tu
m’as montré comment disséquer des E12 de souris (si petits pancréas !!!!), nous
avons tâtonné ensemble sur les moyens de greffer et surtout retrouver… ces E12
dans le quadriceps des souris. Ce projet a démarré avec toi et je te dois beaucoup
beaucoup beaucoup…. De plus, tu as toujours été une oreille attentive à mes excès
d’enthousiasme scientifique en sachant les modérer par ton expérience et les pousser
quand j’en avais besoin. Raphael a de la chance de te compter dans son équipe et
j’ai de la chance de te compter parmi mes amies…..

�
Séverine Pechberty, ma voisine puis mon amie de paillasse, un puits de
connaissance tant théorique que pratique. Je ne pensais pas qu’il était nécessaire de
comprendre en détail les moindres étapes d’une manip avant de t’entendre
m’expliquer les choses. Tu as écouté mes angoisses, mes craintes pendant 4 ans. Tu
as aussi partagé mes joies au labo, en France et ailleurs… Raphael a de la chance
de te compter dans son équipe, même si ces derniers temps nous ne sommes plus sur
le même site…Miss you…
Je tiens aussi à remercier les autres membres du laboratoire avec lesquels j’ai
toujours eu beaucoup de plaisir à me retrouver et qui m’ont, chacun à leur niveau,
apporté beaucoup, et particulièrement Latif, scientifique passionné et à qui je
souhaite toute la réussite qu’il mérite ; Olivier, ta connaissance scientifique n’a
d’égal que ta qualité d’enseignant et j’espère vraiment avoir la possibilité un jour de
collaborer avec toi sur toutes ces molécules fluorescentes et tous ces virus aux noms
quelquefois obscurs que tu maîtrises si bien ; Bertrand, ton flegme apparent est
inversement proportionnel à tes qualités scientifiques ; Estelle, nous avons beaucoup
échangé sur l’Hôpital et les difficultés de concilier la Recherche et la Clinique, je te
souhaite beaucoup de joies dans tes nouvelles fonctions nantaises ; Fanny, l’année a
été difficile pour toutes les deux, plus que quelques semaines avant que « i wish you
nothing but the best… » ; Olivia, Mylène, Kanetee, Djalee, Vikash, Ghislaine,
Samia, Masaya, Andrea, Kathleen, Elodie, Aurore.
Aux collègues hospitaliers :
Monsieur Alaa Elghoneimi, merci de m’avoir donné l’opportunité de poursuivre ce
travail pendant mon clinicat dans votre service et merci encore à vous et à votre
brillante équipe pour votre enseignement.
Madame Sabine Sarnacki, j’ai réalisé mon master 2 sous votre direction il y a
maintenant quelques années, sur un sujet fort interessant et qui, je l’espère, profitera
à de nombreuses petites patientes. Je vous remercie de votre confiance d’alors et
j’espère que nous continuerons à échanger à l’interface de la Science et de la
Clinique.

�
Monsieur Christophe Chardot, ces presque deux années à tes côtés au « theater »
comme disent les anglais m’ont permis d’avancer tant sur le plan clinique que
scientifique. Cette exigence dont tu fais preuve vis-à-vis de toi et des patients est une
qualité qui m’a certainement servi à structurer ce travail au moment où il en avait
besoin.
A mes cochefs pendant ces trois dernières années : Béné, Elodie et Audrey pour
m’avoir aidée pour l’organisation de mon temps scientifique. Audrey tu as été
particulièrement précieuse en ces derniers instants. Je suis ton obligée jusqu'à la fin
de mes jours.
A mes internes, sans la compétence desquels je n’aurais pas pu arriver au bout de ce
travail. Je pense particulièrement à Liza, Benoit, Jérome, Sara, Aias aka « et
voilà ! », Erik aka young Padawan, Maddalena aka fireball, Lara aka Lara Kroft.
A mes rencontres scientifiques :
Au moment où j’achève l’écriture de cette thèse je ne peux m’empecher de penser à
vous Mesdames Nadine Binart et Luisa Dandolo. Si j’ai un jour décidé de
poursuivre une aventure scientifique, c’est parce que lors de mon Master 2 j’ai pu
bénéficier de votre enseignement. Ce dernier m’a rendu les méandres de la Science
moins obscurs mais surtout m’a fait prendre conscience, par la passion que vous
mettez à l’enseigner, qu’il n’est finalement de limite que l’imagination dans votre
discipline. Je vous dois tant….
A mes amies de toujours :
Julie, Pascale, Karine, je n’ai pas été très disponible pour nous ces dernières années
mais vous avez toujours été là pour partager mes doutes mais aussi mes joies…, la
vie quoi…. Il faut dire que entre la côte est africaine et la côte est américaine, vous
m’avez laissée bien seule dans l’ancien monde……Julie, merci de ton aide pour
finaliser ce travail et cela, surtout sous le soleil d’Hawaï, je sais ce que cela t’a
coûté… Moi, perso, j’aurais refusé….

�
A mes parents :
Sans vous, vos conseils, vos encouragements incessants, votre parcours qui est un
exemple à mes yeux, je ne serais jamais allée aussi loin….. Akewani …. Maman,
sans ton aide précieuse pendant les congés de maternité et en ces derniers instants je
n’aurai certainement pas pu finir ce travail.

�
�������������������������������������ABC��D��E������F��������������������A�FF��������A�C�����
�CC���������CBE�����C�BC����BE���������CBE���BC���E��BC�����
����E���������C����
�
�������� ������ ������ ������ ���������!������!������!������!��CB������BC��A������

�
�
�������������ABA�CC��DEF����C���F���E��������C���EF���D�����CC����DEF����C����E�B���
�B�C������B�F���B�������F�E����C�F���E�������������F���E���������C����E�B��� �
���C��!FC����C��!FC����C��!FC����C��!FC�����
����
����
����
����
����
����
����

�
����
����
����
����
����
����
����
����
����
����
����
����
����
����
����
����
����
����
����
����
����
���������������������A�B�������C�
D��E���F�����C�D�E���C����EE����
"E����#��"E����#��"E����#��"E����#������

� �������
��
A����B��CDD��E�C��F� ������������������������������������������������������������������������������� ������
������������ ������������������������������������������������������������������������������������������������������������ ������
Chronologie du développement du pancréas............................................................ - 14 - Embryologie pancréatique humaine ....................................................................................... - 14 - Embryologie pancréatique murine (la souris)......................................................................... - 23 -
Embryogenèse moléculaire endocrine : les données murines comparativement aux
données humaines ....................................................................................................... - 25 - Les facteurs de transcription clés de la morphogenèse pancréatique précoce ....................... - 26 - Les facteurs de transcription clés de la différenciation du lignage endocrine ........................ - 33 - Les facteurs solubles............................................................................................................... - 36 -
Les modèles d’étude du développement pancréatique humain .............................. - 39 -
Rationnel du travail de thèse...................................................................................... - 44 -
������ ��������������������������������������������������������������������������������������������������������������������� ��!"��
Article : Le muscle représente un site de greffe permissif pour le développement du
pancréas immature humain ....................................................................................... - 48 - 1. Stratégie et méthode...................................................................................................... - 48 - 2. Résumé des résultats ..................................................................................................... - 50 -
B����������#��$#��%#���&#� �������������������������������������������������������������������������������������� "'
Le choix du site musculaire .............................................................................................80
Les potentielles applications cliniques de la greffe intramusculaire ...........................81
Discussion des résultats obtenus et des questions soulevées par ces résultats ...........83
Le transfert de gènes et les applications potentielles pour l’étude du développement pancréatique .....................................................................................................................85
��(��#��#��)�)���*� %+�,�#� ��������������������������������������������������������������������������������� -'
C��#.#� �������������������������������������������������������������������������������������������������������������������������� ''
�

�����������
A����B��CDD��E�C��F������A��BCDE��F�����C���B�FC��E�����A��DF���C�E��C��������E����A��BCDE��C���B�FC��E��� �A���C����E����E���ED���!E��� ��"�A��DF���C�E�"�C��������E��#$#�A�%��CB�#E�C��$����#E�C��%&�A�%��E�&�����'E�CB�����EC��(��A�(�������E��CD��E���)*+A�)�CDE�!���*��,���-B�����)$./�A�)�0�!E�$C�1ED�.!!���/���E���������+*+A�+C���������*��,���-�B����*�#A�*����!��E��F�#�D��'F���E�*+�A�*�EE��+����E�BE�������EC��*2A�*��B�2C���E�*$3"A�*$3B��E�"��������E��#)/�A�#�C�����D�)����BE���-�/��C����#$ %4A�#�!E�����'E�E�4�#+A�#E����B��E��B�E���+�B����.##A�.�DC���#ED'E#�'�./�A�.����C��!����.�/A�.�D�BED�����C���E���/�E!BE����25A�2��B1�5���&5�6A�&����C���5��E���C��E�E��C����E�6���'�*7A�E���'F�C�E�7�2 A�2��E���ED���!E��� ��� A���C�ED��� ��(�A�����!E���E�(��C���E�B�C����� �A����B�E��CB����DE������!E��� �-�B��������A������E��CDE����B�F��C��E��"+���A����B�E��CB�"����B�C��C���+�B��������������A������E�����!E���������EC�����"A��E8E��E�"����B�C��C����/(.�A��E8E�E�B�!�C�ED�C!!����DE-CBCE�B��/��A��E!�C�E�DE�DE8E����E!E���/5 4�A�/�6�9�E��DE�E�!C�C�'��E'C���6:�����4�/##A�/��CB�#ED'E#�'�"'A�"����'F�C��E���������

�����7�����
���
�������������������
������������ABCDEFC����BACA���������D��E������������ED��B�A�B������D��BA�������A�
ED�A���BC� ����D���������BC���B�ED�CA��������AB�E��C�� �����D����E��D�E��C�E� ������C��E��
����A���C�����A����� ���� �����A��� ��� ��B�ED��� �C� ���E� �D�������E� ���� ���E������
C�DE����CA����� ABB���BC�����B���CE������E������ ��������������E�B���E��C� ����������AB��
��EC���BC� �B� �E�B�� B���E�� ��� �A�A�AC������ �B� ��EC�AB� B���E�� ��� ��BBD��� AB�A���BC�
D������BC� ���� �A��DE�B������E��D��� �BCE�� ���� ��� ����� !�� ��B�A�BC� ��B����� ��BCAB��E� ���
�D�������E� ���� ��CA��� BD�����AE��� �� ���� DC������ "���� ����B��� ��B�� ��CC�� ABCE����CA�B��
����EC�E�������BBD��������E�B����A������D���������BC���B�ED�CA��������AB���A����EAB��
"���� ���E��E�B�� ����A� ����E����B ��� ��E� �B� ��E��BC� ���D����AE��� "���� �A���C�E�B��
�B��AC��������CA����DC������C���������D���������BC���B�ED�CA��������AB��C��B�AB�B����
�ABAE�B����E��#����E����E�CA�BB���������CE���A����

�����;�����
Chronologie du développement du pancréas �
Embryologie pancréatique humaine
��� ���-C��DE����7<!E��E!�C�E�DE�DF8E����E!E���9/�:=� �E�����C��-E�C��E���E!�������C�E��
9E��������E=�EB�������E=�!E�������E:������DF-C�C�=����B���DE�E���!C�E�E�����BE�>�����C��D��
�?�D� DE�#E��E�=� �@E!������ 8�� B�!!E�BE�� ��� DF�C!C���C��A� (E��E�BC� �E��� �B�E8FE� ���
B����� DE� ��� ;<!E� /�� E�� � �E�!E�� ��� !C�E� E�� ���BE� DE� �@C��E��C�� ��C!C�C-� � 9���F�CE��=�
!��E�=�E������F�CE��:������������C���C���DE��@E��������E�E��>�BE����DE�������C��E����E��
��E!C<�E�� F���B�E�� DE� ��!��E��� ��'��E�A� �C��C=� D<�� ��� -C�� DE� ��� ;<!E� /�� DF!���E�
�@E!����'E�<�E� ���B�F��C��E� >� ����C�� D@��E� ��E!C<�E� F8�'C���C��� E�D�DE�!C��E�
������C������ D���� ��E� �F'C��� ��FDF-C�CE� >� ��� ����CE� B��D��E� DE� �@C��E��C�� ��C!C�C-�
���F�CE��=�>��@�����F�D��DC8E��CB��E��F���C��EA��E�����'E������B�F��C��E�D������9+C'��E�
�:A� "�<�� ���CDE!E��� ���<�=� 8�� ������C��E� ��E� DE��C<!E� F8�'C���C��� E�� �C����C���
8E�����E�BE��E�-�C��E���F'<�E!E��������B��D��E=�B���E�E��DE������DE����8F�CB��E��C�C�C�E�E��
D���� �@��'�E� -��!F� E���E� �E� B����� B���FD���E� 98�CE� DE� D��C��'E� DE�� ��B�� �C�C�C�E�� E��
���8E���BE�D��-�CE:�E���E�D��DF��!A��E�����'E������B�F��C��E�8E�����A�(E������'E����
F�C��F�C���� 8���� ����C-F�E�� ��� �EC�� D�� !F�E�B��!E� E�8C�������� 9�E��EB�C8E!E���
!F�E�B��!E�D������E��8E�����:A��
�
�
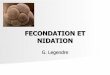
-AB����.A�(�������'CE�E���B�F!��C���C���D��DF8E����E!E���
���B�F��C��E���!�C����
9�@���<���CDCE�����C�E��=�CE���&CB�E��������=���C�C��E�����E���=�3�C8E��C�F�
���C��D:�
Ebauche hépatique
Vésicule biliaire
Ebauche ventrale
Ebauche dorsale
Canal cholédoque
Canal de Wirsung
Canal de Santorini
duodénum
estomac

�����E�����
��� B����� DE� ��� F<!E� /�� E�� >� ��� -�8E��� D@��E� B��C����BE� DC--F�E��CE��E� DE�� DC--F�E����
�E'!E���� C��E��C����=�DE��!��8E!E����DE� �����C��� 8���� �!E�E�� �E�����'E���8E������
�GHI�E�����C<�E�D��D��DF��!����B����B��E��E��DE������D������'E���D�����A�$��-��C���
DE�BE��DE�������'E����8��B����C��E�����'���DE����B�F��C��E�DF-C�C�C8E=�E�B�J��FE�D����
�E�B�D�E�D��DF����E��E�����FE�D@����C����!F�E�B��!��E���DE��EA�$@F���B�E�D�����E=����
��������'E=�D���E����������CE���C�BC���E�DE����'���DE�9�K�E=�B�����E����E�E:�E���@F���B�E�
8E�����E=� ������ >� E��E=� �E� ���BE����� ��BC������ ��� B��B�E�� D�� ���B�F��A� (E��E� -��C���
�����C������C�>�����F��C���DE��8�CE��E�B�F��CBE��D�����B�F���D������9B�����DE�/�����C�C:�
E��D�����B�F���8E������ 9B�����DE�LC����':� 9+C'��E��:A������4HM�DE�� B��=� �E� B�����DE�
/�����C�C� �F'�E��E� ���� ��� ����CE� DC����E� ���� �������� ��� -���� ������ ��E� ��� ����CE�
����C!��E�-��C���E��8EB��E�B��������B�F��C��E�8E�����A�(E�DE��CE��E���D<�����-��!��C���
E�� B���C��C�F� �8EB� �E� B����� B���FD���E� E�� B����C��E=� ��E� -�C�� �EN�� �E� D��C��'E� D��
����'E���D�����=��E�B��������B�F��C��E���C�BC���A�3�C����B���FD���E=�C����E�BE��E���D����
�E�D��DF��!�����C8E���DE��@�!����E��F��������B�F��C��E�DE�D��E�A��
�
�
�
�E� ��� F<!E� >� ��� 4<!E� /�=� �@E!����'E�<�E� ���B�F��C��E� E��� !����FE� ���� ��E�
����C-F���C��� F�C��F�C��E� ��� �EC�� D�� !F�E�B��!E� �8EB� ��'!E����C��� D�� ����� DE��
���'F�C�E���� ���B�F��C��E�A� (E�� BE����E�� !���C���E��E�� �@��'��C�E��� E�� ����B���E��
��E�D��B�����C�E�� ��� �EC�� D�� !F�E�B��!E� E�� 8���� E���C�E� �E� DC--F�E�BCE�� E�� � DE���
�C'�FE��A�����C'�FE�E��B�C�E�9B������E�B�F�E����E���BC�C=�44M�DE����'���DE:=�E������C'�FE�
E�D�B�C�E� 9C����� DE� $��'E�����=� �M� DE� ��� '���DE� 9�C��CADB� #�� ��� *�$$�=� � �//�=�
DiabetologiaO��C��CADB�#�����*�$$�=���//0=�Dev.Dyn.:A�
�
-AB����/�A�+��C���DE��B���������B�F��C��E��
��A�B������BBE���C�E�DE�
/�����C�C�%A�(�������C�BC����DE�
LC����'��$E�B�����DE�/�����C�C��E����E��C��E��D�����������CE�DC����E�B�!!E�
�B�F!��C�F�CBCA�

�����F�����
�
�
���<��BE��E�����E�D@E!����'E�<�E�D@E�8C����G��E!�C�E�=����E���E�D������E�����E�DE�
B��C����BE�E��DE�!������C�����'��C��E�D�����E�����BE�����8�����E�������C8�E���E�D����
����E����D��FE�DE����8CE�-?���EA�
�
/��� �E� ����� E��B�C�E=� D<�� ��E� �E�� B������ ���B�F��C��E�� ��C�BC����� ����� ����B�F�=� 8���
DF!���E�����!������C����BC��C�E�E������������C������B�F��C��EA�$@�BC����E���B����C��F�DE�
�� ���E�� BE�����C�E�� 94HM� DE� ��� '���DE� ���B�F��C��E:�A� �E�� BE����E�� �BC�E��E�� E�� �E��
BE����E��BE������BC�E��E��9+C'��E�7:A�/C��@��C'C�E�E���E��P�E�DE�BE��DE��C<�E���E��E�������
F��BCDF��B�E0��E�!��C�=�C����E������E�B��E�!�C���B�E0��@#�!!EA��.��E���>����E���F��!�C���
��@��E� BE���C�E� �C��F�����E� ������E� ��@E��E�� ������CE��� B���E����D�E� >� DE�� BE����E��
���'F�C��CBE������EC��D�����B�F����D���E�9�$���$CD��#��������*�$$�=� ��/��=�Semin.Cell
Dev.Biol.:A� (EBC� E��� ����E��=� E���E� ����E=� ���� DE��� ���E�8��C����A� �E� ����� DE�
����C-F���C��� DE� BE�� BE����E�� E��� ��<�� F�E8F� ���<�� ���B�F��EB��!CE� ��� DE����B�C���
!FDCB�!E��E��E� D�� ���B�F��� B�E0� �E� !��C�� E�� BE���C�E�� � DE� BE�� BE����E�=� D���� �E�
���B�F����D���E=� '��DE�����E�E���E��C���DE�!����E����E!�������C�E�� �E����E�/5 4A�
$E�� BE����E�� �BC�E��E�� ������ >� E��E�� ���� ����� �P�E� ��C�BC���� DE� �EB�F�E�� ��� BE���C��
��!��E�D@E�0�!E�����DE�����E�0�!E�� 9���E�FE������C� 0�!�'E�E�:�DC'E��C8E�A�5��E��
DC��C�'�E� �����E� B��F'��CE��A� �E�� �E��CD��E�� 9E�D��E��CD��E��A� �����C��'<�E=�
-AB����0A�3�������E����B�F��C��E�
�9��C�CE��CA=��C��DE����A�E��B���A�#C�����'CE�!��FB���C�E=�E<!E�FDC�C��=�&�������44Q:�

�����Q�����
���E������E=� �������F��E� )=� 1���CB�FC�E� E�� 1���CB�FC��'<�E�O� E���E��CD��E��A�
����!C���E��CD��E�� E�� ���B�������E��CD��E�� �� E�� %:=� �@R��!����E=� �E�� E�0�!E��
��B�E����C��E�� 9�C����B�E��E� �� E�� DE�����C����B�E��E� .:=� E�� �E�� E�0�!E�� �C�����C��E��
9�����������C���E� ��=� �C���E�B��C���E� DF�E�DE��E=� B�������� E��E�� �C���E:A� � $@����E�
B�!����C!E���E��B�C�E�E����E��F�E��F������@����E�D�B���A�(E��C�B���E����D�>�����F��C���
DE��@E��E!��E�DE��B�������E�!E������ �E�D��C��'E�DE��DC--F�E���� �����E���BC��C�E�A�(E��
B���������B�F��C��E�������'F�F���E!E���B����F��������C��E�E������������C�C�������EC��DE�
�@����E�F�C��F�C��� B�����C�E�A� �E�� B��D�C��� �E������� �E�!C�������� B����B��DE���BC�C� �����
���E�F�� B��D�C��� C��E�B���C�E�=� BE�� DE��CE��� �E� D��C����� D���� �E�� B��D�C���
C����������C�E�� ��C8C� DE�� B��D�C��� C��E�������C�E�� E�� E�-C�� D�� B����� ���B�F��C��E�
��C�BC�������B�����DE�LC����'=���C��E� BE��E�D���� �SC��E��C�A��C��C��E��BE����E��B�����C�E��
9��� D�B���E�:� ���� DE��� ��C�BC���E�� -��B�C����A� ��� �FB�F�C��� DE� -��CDE� �CB�E� E�� C����
�CB�������E� ��C� �E�!E�� DE� DC��E�� E�� ��!����E�� �E�� E�0�!E�� DC'E��C8E�� D@��C'C�E�
�BC��C�E=�E���E�����������DE�BE���B����B�F��C��E�B����@���D��DF��!A���
�
/����E������E�D�B�C�E=�C����F�F�!����F���E�D<��G/��������C��E�����E����E!C<�E��BE����E��
E�D�B�C�E�=� ���E�=� C���FE�� ��� �E'����FE�� E�� �E�C��� �!��� ��� B����B�� DE�� B������
��C!��DC���� 9��$C1�#�� ��� *�$$�=� � �///=�Diabetes:A� (E�� ��E!C<�E�� BE����E�=� 8��FE�� >�
DC�����C��E� ����� ��C�BC���E!E��� DE�� BE����E�� R� ��C� �E�8E��� B��E���C!E�� DC--F�E��E��
���!��E�� E�� ����!!E��� �@C����C�E� E�� ��� ��!�������C�EA� �<�� ��� 4E!E� /�=� ��� �E�
DF��!��E��������E���HM�DE�BE��BE����E����!C��E����O����!�B��C�F�DE��BE����E��E�D�B�C�E��
�F�-��!FE���@E���C!�����������@��E����!��E�A����E���E�D������E�����E�D@E�����C���
E�D�B�C�E� ���CDE� E�� DE� !������C��� 9�C��CADB�#�� ��� *�$$�=� � �//�=�Diabetologia:A� ����
�C��E���=�����F����C�C���DE�BE��BE����E��E�D�B�C�E��C�C�C��E������EC��D���C�������B�F��C��E�
E��� �E!�������EA� )�� E--E�=� ��� �F�'F�<�E� E�D�B�C�E�DF!���E� ��� BE���E�DE� ��� '���DE=� >�
DC����BE�D��!F�E�B��!E�DE��E���C�E�����E��E����B�F��A�$@E���CB��C���>�BE����E����E8�E�
����� ���A� (E�� BE����E�� �E� �E'����E��� E�� T����� DE� $��'E�����=� ��C�F� -��B�C���E��E� D��
���B�F��� E�D�B�C�EA� )�� E--E�=� C�� �� F�F� DF!����F� ��E� �E�� BE����E�� B����C������ ��� C����
���8E��CE��� DE� ���'F�C�E���� !���C��E�� E�� ���� DE� ��� DC8C�C��� D@��� �����'F�C�E���
B�!!�����9)*�C�+�CDD�������*�$$�=� ��//-=�PLoS.One.:A������C��E���=� �E� -�C��E� �����DE�
����C-F���C���DE��BE����E��E�D�B�C�E��>�BE����DE�9����C-F���C���U�A�7�EM=��E��EB�C8E!E���
>�G�E����/�=�!�����'E�2CFQ�O�7M�E���E��Q�E��7��/��O�E���M�E���F�C�DE��F������E�9��$C1�
#�����*�$$�=���///=�DiabetesO�2C�����)�������*�$$�=���///=�Diabetes:�E���E��-�8E���D@��E�

�����G�����
E�����C���D�������E�D�B�C�E�'�JBE�>���E�����C-F���C���C!�������E�DE�����'F�C�E����E��
��������DC8C�C���DE�BE����E��E�D�B�C�E��!����E��9+C'��E�;:A��
�
�
�
$@T���� �C��C� -��!F� E��� B����C��F� DE� E� ���E�� BE�����C�E��� DC��C�B��� D���� �E�� �������C����
�E��EB�C8E�� 8���� 8��CE�� E�� -��B�C��� D�� �E!���A� �E�� BE����E�� U� 9�EB�F����� �@C����C�E� E��
�E��F�E������EH�GHM�DE��BE����E��E�D�B�C�E�:=��E��BE����E��R�9�EB�F������E�'��B�'��=��E��
��E!C<�E�� >� ������C��E� ����� D�� DF8E����E!E��=� �E�7HM�DE�� BE����E�� E�D�B�C�E�:=� �E��
BE����E��V� 9�EB�F����� ��� ��!�������C�E=�����M�DE��BE����E��E�D�B�C�E�:=� �E��BE����E�����
9�EB�F����� �E� �����E��CDE� ���B�F��C��E=� ��EM� DE�� BE����E�� E�D�B�C�E�:� E�� �E�� ���E��
BE����E�� W� 9�EB�F����� ��� '��E�C�E=� ���8���� B�E���C!E�� �E� '��B�'��=� >� �@J'E� �D���E�
9�CB�C��2�� ��� *�$$�=� � �/��=�Cell Tissue Res.:A� $�� �������C��� DE�� BE����E��β� E��α� �E���
!�B��C��C�E!E��� E�� -�8E��� DE�� ��E!C<�E�� �E�D���� ��� 8CE� -?���E� ������ ��E� BE� ��������
�E�D� 8E��� �@F��C�C��E� >� �@J'E� �D���E� 9�C"���C� 3�� ��� *�$$�=� � �//1=�
Proc.Natl.Acad.Sci.U.S.A:A�)������E=� ��� ��B��C���C���DE�BE��DC--F�E�������E��BE�����C�E��
D�����@T����8��CE��E�����E��E��<BE��!�C������C��E!��E���C���8EB��E��E!��A��C��C�����EC��DE�
�@C������!�C��-?�����E��BE����E���������'��C�FE��B�!!E���C��A����BE���E����'E�DE�BE����E��
U� E�����F� DE�� ����E�� ���E�� BE�����C�E�� E�D�B�C�E�A� (E��E� ��B�C�EB���E� DE� �@T���� 8�� �E�
!�DC-CE��>��@J'E��D���E���C���E�����F'C����C���C���C�C�C��E�DC�����T��E���@C����B���E����D�
�����>����E�B�E8K��E!E���DE��DC--F�E�������E��BE�����C�E��9+C'��E�E:A�
�
-AB����4������C-��C���DE��BE����E������!�C�E��E����E�E��
�����������E���!��E�DE���BE�������'����E�
E�����EBC-CE����DE�����DE�B����E�B�����E�
�9�2���E!�/��E��B���A��C��E�E�=�
�HHH:�

�����4�����
�
$���C'�C-CB��C�������C���'C��E�DE�BE��8��C��C����DE��F'C����C���C����@E�������E�B��E��CE��
B����EA��
/��� �E� ����� �����C���C-=� DE� ��� ��C����BE� >� �@J'E� �D���E=� ��� !���E� BE�����C�E� E�D�B�C�E�
��'!E��E����'�E��C8E!E���E������!!E������!���E�UA�(E��E�DE��C<�E�E���BE��E���C���F�F�
�E������F��DCFE�B�E0��@#�!!EA��C��C=��E��T������F�������������!�B��C��C�E!E���DE��E�C�E�
��C��E�E��8�������'�E��C8E!E����@F��--E�������F��CB��C���U�9+C'��E�F:A�
�
�
�
�
-AB����5�����EB��E����C��E�DE��C�����DE�$��'E������DE�����F�C�DE��F������E����@J'E�
�D���E�.!!����C���B�C!CE�C����C�E�9!�����:�E���E!������C�E�
�9&ECE��CC�E��B���=��HHG=�
�C��E�E�:�
6$���+œ�C$� 6$���C��$���
.����C�EX�'��B�'��X�#�EB����-AB����7����B�C�EB���E�DE��’C����DE�$��'E������B�E0��E�-œ�����DE�����E!�C�E��
D’�!é�����éE�E��B�E0��’�D���E�.!!���-����E�BE�BE�.����C�E�
9���'E:=�*��B�'���98E��:��
9����EE���E�����E��E��E��/B���-!�������E��B���A=��HHG=�
�����5�E:�

�����H�����
(EBC�E���B��-C�!F������@���E�BE�D@��'!E����C���D����!��E�D@T������8EB��@J'E���������E�
�@�� ����BCE� ��E� ��'!E����C��� DE� ��� !���E� BE�����C�E� U� 9#�A��� 8�� 8�� ��� *�$$�=� � �//-=�
Diabetes:�9+C'��E�Q:A��
�
�
�
(E��E� ��'!E����C��� E��� C!�������E� ��� B����� DE�� 7� ��E!C<�E�� ���FE�� DE� 8CE� ��C�� 8��
���'�E��C8E!E��� DC!C��E�� B����@� >� ��� �C8E��� ������ ������� DE� �E��G� ���� 9+C'��E� G:A�
(EBC�E���B���F�F�����C8E���DE��F��CB��C���DE��BE����E��U����<�������C����BE�92C�����)����
���*�$$�=� ��///=�DiabetesO�#�A���8��8�����*�$$�=� ��//-=�DiabetesO�2�$1C�DA����9�����*�$$�=��
�/��=�Diabetes:A��
-AB����:���)8����C���D����!��E��������D@C�����DE�$��'E������E��DE����!���E�BE�����C�E�U��DE�����F�C�DE��F������E����@J'E��D���E�
��9&ECE��CC�E��B���=��HHG=�
�C��E�E�:�

�����������
�
+C���E!E��=� �E� ���B�F��� �D���E� B�!����E��� E�8C���� ����!C��C���� D@T����� B����C��F�� DE�
�HHH� >� 7HHH� BE����E�=� D@��E� ��C��E� 8��C���� DE� �HH� >� 4HHY!=� �F����C�� ��� �EC�� D�� �C����
���B�F��C��E�E��B�C�E�E�� C��C'�F��������� �F�E��� B��C���C�E� �CB�EA�$@C����C�E� 9���!��E�
����'��BF!C���E:=� �E� '��B�'��� 9���!��E� ���E�'��BF!C���E:=� ��� ��!�������C�E�
9���!��E�C��C�C��CBE�DE�����FB�F�C���D@C����C�E�E��'��B�'��=�DE����B�����B�C���D��!��B�E�
�C��E=� DE� ��� �FB�F�C��� �BCDE� '����C��E:� E�� ��� '��E�C�E� 9���!��E� �F'�����CBE� DE� ���
�FB�F�C���D@C����C�E=�E���B�C�����E�C'<�E�9�C�C�;�����*�$$�=� ��//-=�Curr.Diabetes Rev.::�
B��E��� ��� �P�E� BE������ D���� ��� �F'����C��� D�� !F�����C�!E� F�E�'F�C��E� E��
��C�BC���E!E���BE��C�D��'��B��EA�$E������E��CDE����B�F��C��E�������>���C�B��E�����P�E�
-AB����<�������C-F���C���DE��BE����E��U�DE�����F�C�DE��F������E����@J'E��D���E�
.!!���-����E�BE�BE�C����C�E�98E��:�E��2CFQ�9���'E=�
!����E���DE�����C-F���C��:��
9�@���<��&ECE��CC�E��B���=��HHG=��C��E�E�:�

�����������
D@C��C�C�C���DE� ��� �FB�F�C������B�F��C��E�E��B�C�E=�DE� ��C!����C���DE� ���8CD��'E�DE� ���
8F�CB��E��C�C�C�E=�DE���C!����C���DE����!���CBC�F�C��E��C���E�E������E��B�C�������E�C'<�EA��
�

�����7�����
Embryologie pancréatique murine (la souris)
�
(�!!E� B�E0� �@#�!!E=� �E� ���B�F��� �E� DF8E����E� >� ����C�� D@��E� �F'C��� ��FDF-C�CE� DE�
�@C��E��C����C!C�C-����F�CE��=�>��������CE���������B��D��EA�$E����E!CE���F�F!E����E��-�8E���
DE�BE�DF8E����E!E��������8C�C��E�����B����E!�������C�E�4�9)4:=�����C8E���DE��@C��E��C��
��C!C�C-����F�CE��=��8EB��@F!E�'E�BE�D@��E���E!C<�E�F8�'C���C���D�����E���C��>�)4AE�DE�
�@F8�'C���C���8E�����E�����EC��D��!F�E�B��!E�E�8C�������A�$E�DF8E����E!E���>�����C��
DE� BE� ���DE��E���K��E� �F���F�E��DE���F���E�����E�FE��A� �����E!C<�E� �����C�C��� � 9)4AE�
)��AE:�E�����DE��C<!E������C�C���9)�7AE�)�FAE:�9�A*�������=�����*�$$�=� ��'"�=�Dev.Biol.:A�
$�� ��E!C<�E� �����C�C��� 8�� B���E����D�E� >� ��E� �F�C�DE� D@C��E��E� ����C-F���C��� DE��
���'F�C�E�������B�F��C��E����C��@��'��C�E���E��B��D������C��E��B������C��E�B���EB�F��
9�@����E� ���B�F��C��E:� >� ����C�� DE���E��� 8���� F!E�'E�� �E�� DC--F�E���� ���E�� BE�����C�E��
���B�F��C��E��A�
�
�� BE� ���DE=� C�� E�C��E���E���E�� BE����E��E�D�B�C�E��F����E��8C�C��E�=� E��E��CE��E!E���DE�
���E�α,�B���E����D����>�DE��BE����E��C!!����E�=���C��E�8E���B��E���C!E���@C����C�E����
���'��E�C�E�E����C������8��FE��>�DC�����T��E� �����DE�����DE�����F�CE���� 9������C����=�=��
�///=� Development:A� .�� �E��E� �F��!�C��� ��E� �E��� �P�E� �@E��� ���� B��C�A� �� )��AE=� ���
�����C��� DE� �@E���!�B� E�� D�� D��DF��!� �E�!E�� D@�!E�E�� �E�� DE��� ����'E����
F�C��F�C�������B����B��>����-�BE�D�����E���C��C��E��E�D��D��DF��!A�(E��DE��CE���-C�C�����
DE� -��C���E�� 8E��� )�GA� � ����� �E� !K!E� �E!��=� ���� �E� ����� E��B�C�E=� �E�� ��E!C<�E��
BE����E�� �BC��C�E�� ����� 8C�C��E�� �8EB� �@E���E��C��� C!�������E� DE� (��� >� )��AE� � ��C��
D@�!����E�D<��)�7AEA�$E�� BE����E��E�D�B�C�E��!����E�=������� � >� E��E�=� 8����������T��E�
����� DE� ��� � DE��C<!E� �����C�C��� >� ����C�� D@)�7AE=� �F�C�DE� ��C� B���E����D� >� ���
��FBC-CB��C���DE�����'F�C�E����8E����E��DC--F�E�����C'��'E�����B�F��C��E�A� �)���E�)�7AE�
E�� )�EAE� � ��'!E��E� �E� ����� DE� BE����E�� α� E�� β� DC--F�E�BCFE�O� >� )�EAE� �E�� ��E!C<�E��
BE����E���E��������C��E��A��)���E�)�;�E��)�G=��E��BE����E��E�D�B�C�E���E��E'����E���E��
T���� DE� $��'E�����A� )�-C�=� B���E� �8���� ��� ��C����BE� >� )�G=� �E�� BE����E�� �EB�F����� �E�
�����E��CDE� ���B�F��C��E� ������C��E��A� .�� E��� >� ���E�� ��E� BE�� BE����E�� ��� �E!��E���
DF�C8E�������!�B��C�F�DE��BE����E��ε�B�!!E��@������''F�F��E�����8����D@���E��E��B���A�����
D����C8C�DE��C'��'E�9�D���=�����*�$$�=���/��=�PLoS.One.:A����@J'E��D���E=�����������C���
DE�� DC--F�E��E�� BE����E�� B�!������� �@T���� E��� ��� ��C8���E�A�β� 9QH�GHM:=�α� � 9�E��GM:=�δ�

�����;�����
9Z�HM:=����E��BE����E�����E��ε�9�C"���C�3�����*�$$�=� ��//1=�Proc.Natl.Acad.Sci.U.S.A:A�
(E� DE��CE�� E��� ��'��C�F� �8EB� ��� ������ BE������ DE� BE����E�� β� E�� E�� �F�C��F�CE� ��E�
B������E�DE������E�����E��BE�����C�E��9+C'��E�4:A�
�
�
�
�
$E����B�F����D���E�!��C��B�!����E����HHH�>��HHH�T�����E�=�B�!!E�B�E0��@#�!!E=�BE��
DE��CE���8�����@F��--E�����<�������C����BE���������C-F���C����8EB�����CB�>�;��E!�C�E��
DE� 8CE� 96DC�C� �� ��� *�$$�=� � �//-=� Proc.Natl.Acad.Sci.U.S.A:A� /@�'C������ D��
B�!����C!E���E��B�C�E=�E��DE�����D���C!C�'���C�DC--<�E=��E��F���E�������CDE��C��E�A�
�
�
�
-AB����>����B�C�EB���E�DE��’C����DE�$��'E������!��C���D���EA�.!!���-����E�BE�BE�.����C�E�
9���'E:=�*��B�'���98E��:��
.����C�EX�'��B�'��X�#�EB����

�����E�����
Embryogenèse moléculaire endocrine : les données murines comparativement aux données humaines �(�E0� �E� ���'E��� ��� '���D� ��!��E� DSC�-��!��C���� ����� DC����C��E�A� )�� E--E�=� �E��
E��F�CE�BE��DE�DC�����C���'F�C��E�9�E��E�E��'�C��DE�-��B�C��:=��E��F��DE��DE��C'��'E�E��
�E�� F��DE�� DE�� ��F�����E�� DE� BE���C���!�D<�E�� 'F�F�C��E�� ���� �E�!C�� DE� DFD�C�E� �E�
�F�E��� DE� �F'����C��� �����B�C��C���E��E� 9-�B�E���� DE� �����B�C��C��:� E�� ����B�C�E�
9-�B�E���� ������E�:� ��C� B����P�E� ��� DF�E�!C���C��� DE� �@E�D�DE�!E� ���B�F��C��E=� ���
��FBC-CB��C���E�D�B�C�E�E��E�-C�����DC--F�E�BC��C���E�����!������C���DE��DC--F�E�������E��
BE�����C�E�� B����C������ �@T���A� � ���� ������� D���� BE� B���C��E� E����E�� �E�� D���FE�� DE�
DF8E����E!E��� B����� B�E0� ��� ����C�� E�=� ����D� E��E�� E�C��E��=� E����E�� BE��E�� B�E0�
�@#�!!E�9+C'��E��H:A�
�
-AB����.?���F8E����E!E������B�F��C��E�B�E0��������C��
�95�C8E��2���C��1C�C&�E��B���A=�
�HHG=�*E�E���E8:��

�����F�����
Les facteurs de transcription clés de la morphogenèse pancréatique précoce
�
(�!!E� DC�� ��FBFDE!!E��=� �@�����C�C��� DE�� DE��� ����'E���� ���B�F��C��E��
��C!��DC���� B���E����D� >� ��� ����C-F���C��=� E�� ��E� �F'C��� ��FDF-C�CE� DE� �@C��E��C��
���F�CE��=� DE� BE����E�� � E�D�DE�!C��E�A� (@E��� ����� �E� B����P�E� ����B�C�E� DE� -�B�E����
������E�� �EB�F�F�� ���� �E�� �C����� E�8C��������� 9����B���DE=� BE����E�� E�D���F�C��E�=�
!F�E�B��!E:=���E�BE��E��F'C���E�D�DE�!C��E�8����E�D�E���E�DE��C�FE����B�F��C��EA�
(EBC��E�-�C�������@�B�C8��C���DE��@E���E��C���D@��E�B��B�DE�DE�-�B�E����DE������B�C��C��A�
9+C'��E� ��:� 3�E� �C'�����E� !��FB���C�E� 8�� D��B� DF-C�C�� BE�� BE����E�� ���'F�C��CBE��
���B�F��C��E��!���C���E��E��E��BE��E�BC��E�!�DC-CE���D�����E��E!��������BE��BE����E���E�
��FBC-CE���������E��DC--F�E�����C'��'E�����B�F��C��E�AA�
�
$���E8�E���C���C���E��E�������E������C8E�!�C����F�E��E������BE���C����!��E�DE�-�B�E����
DE� �����B�C��C��� !�BE���� ��� DF8E����E!E��� ���B�F��C��E� '������ ��C�� �����
��FBC-C��E!E��=� ��� DF8E����E!E��� UA� �C��C=� �E�� ���'F�C�E���� C�C�C���� D�� ���B�F��� �E�
DF-C�C��E��� ���� �@E���E��C��� DE� ;� -�B�E���� DE� �����B�C��C��� � B�FA� �D��� 9���B�E��CB�
���DE���� ��!E��� � -�B���� �:=� #���4� � 9#�!E����� 'E�E� 4:� =� ��-��X�;G� 9���B�E���
��EBC-CB������B�C��C���+�B�����=�R������C��:�E���E��-�B�E����*����;�E��FA�(E�����'F�C�E�����
���B�F��C��E�� E���C!E����� E�B��E� D@����E�� -�B�E���� DE� �����B�C��C��� �E�!E������
���'�E��C8E!E��� �@��CE����C��� 8E��� �E� �C'��'E� E�D�B�C�E� ��� E��B�C�EA� ���!C� BE���BC=�
1�FA��92��E���ED���!E�����FA�:=��1��A��9��E���ED���!E������A�:�E��/��4�9/�6�9�E��
DE�E�!C�C�'��E'C���6�����4:A�(E��DE��CE��������E���C!F��D����DE��BE����E����C�'��DE���
E�B��E����B���B�<�E�!���C���E��A�
�

�����Q�����
�
�
��&.� E��� ��� -�B�E��� DE� �����B�C��C��� >� ��!F�D�!�C�E� D���� �@C!������BE� D���� �E�
DF8E����E!E������B�F��C��E�9=��DC���8�����*�$$�=� ��''�=�Mol.Endocrinol.O�#A$$���������
���*�$$�=� ��''!=�EMBO J.:� �����B�E0� �@#�!!E���E�B�E0� �������C�=���F�F�DF!����FE�����
�@������E�DE��!����C������!�0�'��E��DE�BE�'<�E�D�����E��DE���E��<BE�A�)��E--E�=��E�25�
!��C�� B��D�C�� >� ��E� �'F�F�CE� D�� ���B�F��� 98�D���D� 8�� ��� *�$$�=� � �''!=�Nature:A� $E��
����'E���� ���B�F��C��E�� �E� -��!E��� !�C�� �E��E��� >� ��� ���DE� ��DC!E���C�E=� E��
�E��E!E��� ��E���E�� BE����E�� E�D�B�C�E�� C!!����E�� �EB�F����� D�� '��B�'��� ��� DE�
�@C����C�E���������E�8FE�A�(E��D���FE����''<�E���D@�C��E������E� �E����E!C<�E��BE����E��
E�D�B�C�E�� ���E�8FE�� �E�D���� �@E!����'E�<�E� ���B�F��C��E� 9B-� �����=� �����C�C���
��C!�C�E� B�E0� ��� ����C�:� �@���� �������E!E��� ���� ��� !K!E� ��C'C�E� ��E� �E�� BE����E��
E�D�B�C�E��!����E��������C����������� ���D�D���� �E�DF8E����E!E��A�$��%��&������'��
��C�CA�B��� �DC�C�����%���C����B��AC����B��A�� C��BD�B�C�����E���DBD�A����B�ED�CA����
(��((#���B��C��#�����������''"��Nat.Genet.)����E����������DC�C��DCDE�%���C����������B��AC���
�B��A�� C��*+,-.�(��((#���B��C�� #�� ������� � �''" ��Nat.Genet.)� �D��� E��� E���C!F� D<��
)GAE�D���� �E�� �F'C������F��!��C8E�����B�F��C��E��DE� �@E�D�DE�!EA�#E��E��=� E���HHH�
9������C� ��� =�=� � �///=�Development:=� �� DF!����F� ���� DE�� E��F�CE�BE�� DE� ��C8C� DE�
�C'��'E���E��@E��E!��E�DE��BE����E�����B�F��C��E��DF�C8�C��DE����'E�C�E�����D��[A������
-AB����..���+�B�E����DE������B�C��C�����é�CD����à����Dé�E�!C���C������B�é��C��E���C��à����DC--é�E�BC��C������B�DE�B���E���DE��-�B�E����DE������B�C��C��A�������E�9E�D�DE�!E�DE��’C��E��C����C!C�C-:���E��9E�D�DE�!E����B�E��C��E:���C��9���'E�C�E����E�D�B�C�E����EB�BE�:�����'E9���'E�C�E����E�D�B�C�E�:����'E�9BE����E���:��
95�C8E��2���C��1C�C&�E��B���A=��HHG=�*E�E���E8:�

�����G�����
���D=��@E���E��C���DE�BE�-�B�E����E����E���EC�������BE����E��U�D�����E���E��E��C��B��E������
�P�E� D@�B�C8��E��� �����B�C��C���E�� D�� '<�E� DE� �@C����C�E� 93�$���D� ��� ��� *�$$�=� � �''�=�
EMBO J.:=�E��>���E���E�� � BE����E��V� 9#A$$������������*�$$�=� ��''!=�EMBO J.:A� ������BE��
BE����E�=� �@E���E��C��� �����C���C8E� DE� �D��� �E��� ����� F�E8FE� ��E� D���� �E�� BE����E��
���'F�C��CBE�=�B���B�F�C��C��E���C��E���8C�C��E������D��!�����'E�C!!����C���B�C!C��E�
DE���C����� -?����A��D���E���D��B�����B�E���!�BE���D��DF8E����E!E������B�F��C��E�>�
����C�� DE�� F���B�E�� E�D�DE�!C��E�� E�� B��E� ����C� ��� �P�E� ��F���DF����� D���� ���
DC--F�E�BC��C���E�����!������C���DE��BE����E��UA�!����C���B�C�E�������B�������B�ED�������AB�
����C��A����E�A�C���B���#�E���A�B���EC�����/,01����BA���������������������C�����9��A�"��B�
��� ��� *�$$�=� � �///=�DiabetesO��C��CADB�#�� ��� *�$$�=� � �//0=�Dev.Dyn.:��'��E2��������CC��
�#�E���A�B���E�A�C�BC����C��B��E��AB��BB�����
�
�$&!>�@���#D&.AE�-�B�E���DE������B�C��C���DE����E��#$#�9%��CB�#E�C��$����#E�C�:=�E���
DF�EB�F��8�����D���D<��)G�����C8E���DE��������B���DE=�DE��@F���B�E�D�����E���C��D����
�@F���B�E�8E�����E�9=A�������*�$$�=���'''=�Nat.Genet.:A���)��AE�����E���E��C���DFB�C�E�E��
DE8CE��� �E���EC��E�����BE����E��UA�3�E��E��E�DE� -��B�C���D��'<�E� C�D�C�� B�E0� ��� ����C��
��E��'F�F�CE�D�����B�F���D��������������E��E����B�F���8E�������E�DF8E����E�!�C���8EB�
��� ��!��E� �FD�C�� DE� BE����E�� U� E�� DE�� T����� D@��B�C�EB���E� !�DC-CFEA� La fenêtre
d'expression de Hlxb9 est aussi extrêmement importante puisque son expression prolongée
perturbe le développement exocrine et endocrine, et s'accompagne d'une différenciation des
cellules de l'épithélium pancréatique en cellules intestinales.(E� -�B�E��� �� D��B� ��� �P�E�
!�BE���D���������FBC-CB��C���DE���@E�D�DE�!E�D������8E�����E�DE��C�FE����B�F��C��E�E�=�
��������D=�D�����E�DF8E����E!E���E�����DC--F�E�BC��C���DE��BE����E��UA� �.��-�������E����E�
�@E���E��C���DE�BE�-�B�E���F��������E0����'E�D�������������F'C���D@C��F�K�=�C��E�����<���E��
��C�C�F� E�� �C���B�C!CE� B�!!E�!����E��� ��FB�BE� D�� DF8E����E!E������B�F��C��EA� � !��
��C� ����A� �� B�C�E� ���� ���� ��C�CA�B�� ��� ��� � B�� ��BC� �D�EAC��� ���%� �&����� �C� ��BC� ��
��EA�AB����B� ��B�E���������A�BC��B����DBD�A�� ���ED����ECA������ �B����E���A�����C��B��
�CDB���� �B�E��C����3� ��� ��B�E���� ��� $�EE�EAB�� (��#����#� ��� #�� ������� � �//1��
J.Pediatr.Surg.4� ��#����#� ��� #�� ������� � �//-�� Hum.Mutat.)�� �� B�CE�� ��BB�A���B���� ����
��CA�BC�� B�� �ED��BC�BC� ���� ��� �A�� C��� ��A�� ���� DC����� ��� ����EC�� �� ��B�� C�E��� ��BC�
�B��E��E�E�����B�E���B����ED�����BC��5�BB���B���C�������(D���#(����C��#�����������/����
Diabetes Metab)�BC�E����ECD����������B���CA�BC���EC��E���B����C�CA�B�����%���C�����

�����4�����
��� � B�� ����A�����BC� E����B������ ��B� �A�� C�� BD�B�C��� ��B�� �B����A����E������A����
�����B�ED����B�A����EA�����
�
��+.CB�4<=��������E�-�B�E���DE������B�C��C���DE����E��#$#=�E���E���E�����E��E��C�������
�E�DF8E����E!E���D��BE�8E�E��E��D�����B�F��A�.��-��B�C���E�D�����E�B�D�E�D@���B�!��E�E�
�F�F����C!F�C��E�A� ��-�A� � ����� �E� ���B�F��� C�� E��� E���C!F� D<�� )4=� �8EB� �D��=� �����
D@����D� D���� �@F���B�E� D�����E� ��C�� �@F���B�E� 8E�����E� ��C�� D���� �E�� BE����E��
���'F�C��CBE�����B�F��C��E��92CCCB�*�A�������*�$$�=���//�=�Nat.Genet.:A���������D=�8E���
)��E=� � ����E���E��C�����'!E��E���!�C�� BE��E�BC� � �E��� �E���EC��E�>� �������CE� �E�!C���E�
DE�� ����B�E�� DE� �@����E� ���B�F��C��E� ��C�� E���C�E� ���� BE����E�� �BC��C�E�=� D����
�E���E��E��C��B����P�E��� �@E���E��C���DE��'<�E��DE��E�0�!E��DC'E��C8E��9=A��������*�$$�=��
�//�=�J.Biol.Chem.:A���FBE!!E��=�C����F�F�DF!����F���E�#��%4�F��C����E�DE��BC��E��DE�
BE� '<�E=� �8EB� �D��� E��1�FA�� 9+C'��E� ��:=� E�� BE��E� �B�C��� �E�!E����C�� DE� ����C�C�E�� ���
�������C���DE�����'F�C�E�����E��D��B����B��C����BE�DE�BE�����=�F�F!E���C�DC��E�����E�>�
�@���E��C��� D@��E� �������C��� E�D�B�C�E� ��--C����E� 9;������D� 9�� ��� *�$$�=� � �/��=�
Mol.Cell Biol.:A�
�
�
�
�$E������C��1��B1����������BE�'<�E���F�E��E�����E���������CE����B�F��C��E��8EB���E�
���E�BE� B�!��<�E� DE� BE����E�� E��B�C�E�� ������ ��E� ��E���E�� BE����E�� E�D�B�C�E��
�E��C��E��A� ��� �����=� BE� -�B�E��� E��� C!�������� D���� ��� ��FBC-CB��C��� E�� �E�!�C��CE�� DE��
-AB����./���F�E���DE��-�B�E����DE������B�C��C���
!�C��E���������������C���DE����'F�C�E����
�9"��!�����A�E��B���A=���H��=�
&��A(E���%C��A:�

����7H�����
���'F�C�E�������B�F��C��E�=�E��D�������DC--F�E�BC��C���D���C'��'E�E��B�C�EA�.���E��E!��E�
���� C�DC��E�����E� >� �@E���E��C��� DE�� ���'F�C�E���� E�D�B�C�E�� ��C���E� D���� �E� 25� C��
�E��C��E� ��E���E�� BE����E�� E�D�B�C�E�A� $��%� �&����� ���� ��C�CA�B�� ����%���C��� ���
/671������CA���BC����B��A�� C��BD�B�C��������AD��������B����A���B��E����A�����(#����2�
3����#�����������//!��Nat.Genet.)��
�
DC�C�4����5�������CE��E��� >� ��E� -�!C��E� DE� -�B�E���� DE� �����B�C��C��� >� D�C'�� DE� 0C�B�
B�����E�DE��E� �CE��>� � �@���������E��F��E�BE�B���E�����B�!�������� �E�!��C-�*���"��A�
5�� E�� DF��!��E� F� !E!��E�A� *���;� E��� E���C!F� D���� �SE�D�DE�!E� ��C!C�C-� E�� ���
BE���C�� ��!��E� D@��'��E�� E�� -��!��C��� �E�� ��E� �E� B?��=� �E� -�CE=� �SC��E��C�� '�K�E� E�� �E�
���B�F��A�$E������C��*���;�25�!E��E���E���E�)QAE�E��)4AE� � 92������;�����*�$$�=� ��''"=�
Genes Dev.:A� � *���� F=� ������ >� ��C=� E��� E���C!F�D���� ��� '���DE���C!C�C8E=� �S�������\DE=�
�@C��E��C�=� �E�!��B�E=� �E�B?��=�E�� �E����!���92�A�'���������*�$$�=� ��//�=�Development:A�
$E������C��*���F�25�!E��E�������C���<����FB�BE!E���E���E�)EAE�E��)QAEA�$@E���E��C���
DE�BE��DE���-�B�E����E����E����8FE�D�����E��F���B�E�����B�F��C��E��D�����E�E��8E�����E�
E��B����B��C�E����8EB��D���E����-���>�)4AEA��(E��E�E���E��C����E�!�C��CE����E�D��������E�
��� �����C�C��� ��C!�C�E� ��C�� 8�� �E� �E���EC�D�E� ���'�E��C8E!E��A� �C��C=� >� )�FAE=� *���;�
�@E����E����8F���@����E���F!C�F��DE� �@����E����B�F��C��E�D���� �E� �E��C��C�E��BC��C�EA���
)�GAE=���E���E��BE����E���BC��C�E��B���C��E���E�B��E�>�E���C!E��*���;A�����@J'E��D���E=�
F����'E!E��=��E��BE����E���BC��C�E���@E���C!E��������BE�-�B�E���!�C��E���E8��B�E�C��E���
�E����8F�D������E���E��BE����E��α�E��β .�/@�'C������DE�*���F=�>�)��AE=�����E���E��C���E���
�E����8FE� D���� �E�� BE����E�� E���C!���� 1��A�� E�� '�7� !�C�� ����C� D���� �E�� BE����E��
D�B���E�� E�� DF8E����E!E��� ������ ��@C�� DE8CE��� E�B��� DE�� BE����E�� �BC��C�E�� E��
DF8E����E!E��A� ���� �C��E���=� C�� �� F�F� DF!����F=� '�JBE� >� DE�� 25� B��DC�C���E��� DE� BE��
DE���'<�E��>�����C��D@�������<!E�(�E�����������E�B����P�E�D�����!��E����D��=���E��E�2��
���B�F��C��E� ��FB�BE� DE� �@��� ��� �@����E� DE� BE�� '<�E�� �E� B��D�C��C�� ��@>� DE� �F'<�E��
���!��CE��D�����B�F���>��@J'E��D���EA�)���E8��B�E��E�D����E�25�B��DC�C���E��������C��>�
��E� �'F�F�CE����B�F��C��E����� ���E�BE�D@E�����C���D������� DE�����'F�C�E�����D��[�
9E�CD�)�����*�$$�=� ��/��=�J.Clin.Invest:A�$��%��&������'�B�������B��C�������(A �*��C��#��
4�� #�� ������� � �/���� Nat.Genet.)� �BC� �A�� �B� D�A��B��� ���%� 18� ��CA�BC�� �ED��BC�BC� �B�
�A�� C�� BD�B�C��� ����� ��DBD�A�� ��B�ED�CA���� �C� ���E� ��EC�AB�� ���� ��E�A���C�A���
�����AD����������C�CA�B���DCDE�%���C������9�6�:�� �C��C� �@������ C���--C���BE� DE� �@��� ���
�@����E�DE��-�B�E����*�"��B��D�C��>������F�����E����B�F��C��E��F8<�E�B�E0��@#�!!E=�

����7������
��������E�B�E0��������C��BEBC��@E��������E�B��A�)��E--E��C��E����FBE���C�E�D@�8�C�����D����E�
2��DE�*���;�E��F���������E�C����E��'F�F�CE����B�F��C��E�B�!��<�EA�$@E��E!��E�DE�BE��
D���FE�� ����� E�� -�8E��� D@��� �P�E� C!�������� DE� BE��E� -�!C��E� DE� -�B�E���� DE�
�����B�C��C���D�����������C-F���C���D�������DE����'F�C�E����E��E���C�E����DC--F�E�BC��C���
E�D�B�C�E� E�� E��B�C�E� �8EB� ��E� -��B�C��� DC--F�E��CE��E� �������E!E��� E���E� �E�� DE���
E��<BE�A��
�
91&/�/�E��� ��� ����E� -�B�E��� DE� �����B�C��C��� >� ��!F�D�!�C�E� D���� �@E���E��C��� E���
DF�EB�FE�D<��)4AE�D�����E������'E�������B�F��C��E������EC��DE�����'F�C�E�����D���[A�
)���C�E=� ���<��)��AE=� C�� E�����C��E!E���!�C��E���D���� �E�����'F�C�E����E�D�B�C�E��>��
DE�� �C8E���� D@E���E��C��� ����� F�E8FE�� ��@C�C�C��E!E��� 9)��++��������� ��� *�$$�=� ��''"=�
Nat.Genet.O�)*�CA�'B�"�$�F��#�����*�$$�=� ��///=�DevelopmentO�3$A����2�C�AD�1A�8��#��
���*�$$�=���//-=�Genes Dev.:�E�=���������D�DE8CE����C!C�F�>�����E���E��BE����E��E�D�B�C�E��
>� �SE�BE��C��� DE�� BE����E�� DE���� 9)����$� =�� ��� *�$$�=� � �''-=� Development:A� ����� �E�
���B�F����D���E=�1��A��B��E�����P�E�!�BE���D�����E�!�C��CE��DE��SCDE��C�F�DE��BE����E��
U� 9�C�A'CD� 8��!����� *�$$�=� ��/��=�Genes Dev.:A� $E�2��!��C����F�E��E���E� ���E�BE�DE�
BE����E�� U� DC--F�E�BCFE�=� ��E� DC!C���C��� D�� ��!��E� DE� BE����E�� R� E�� ��� E�� ��E�
��'!E����C��� DE�� BE����E�� W� 9��C������ =�� ��� *�$$�=� � �//!=�Proc.Natl.Acad.Sci.U.S.A:=�
��''F�����D@�C��E������E��E��BE����E��W�E��U�������CE���DF�C8E��D@�����FB���E���B�!!��A��
$E��BE����E��V��E�����������--EB�FE��D����BE�!�D<�EA�
(E�-�B�E�����D��B�����P�E�!�BE���D���������FBC-CB��C���E�����!������C���D���C'��'E�U�E��
BE���C�E!E�������C�D�������'E�<�E�DE��BE����E��R�E����A�����B����C�CA�B�������� B��B��
DCD�E�CE���D���B���C�����A����B�ED�CA���������AB����B�CE����BB�A���B����
�
91&5�.� E��� ��� -�B�E��� DE� �����B�C��C��� >� ��!F�D�!�C�E� D���� �@E���E��C��� E����
�����C��C�E!E��� DF�EB�FE� >� )GAQE� D���� ��� �F'C��� ��F��!��C8E� 8E�����E� DE� �@C��E��C��
��C!C�C-=� D���� �E� D�!�C�E� �D��A� .�� E��� ���� �C��E���� E���C!F� ��� �C8E��� DE� ��� �F'C���
8E�����E�D�����E��E�����E��D�����E�!F�E�B��!E��F�C�?�����'CE��E����F�'����C��EA���)4=�
��E���E��BE����E��D������'E���D�������B�!!E�BE���>��@E���C!E����������E��@E���E��C���
�@F�EC���E��8E�����A�DE���)�HAE=��@E���E��C���8E�����E��F������C��E��>�BE����DE�C�������'E�
�E���C�E��D@E���E��C���DE���-���E���D��A� �3��B������������D=�C��DE8CE��� �C!C�F�>��������CE�
BE�����E� DE� �@F�C��F�C�!� ����D� ��-��� E��� �E����8F� >� ��� �F�C��F�CE� DE� �@F�C��F�C�!=� ���
�C8E��� DE�� E���F!C�F�� DE� �@����E� ���B�F��C��EA� DE��� )�7AE��;AE=� BE���C�E�� BE����E��

����7������
BE�����E�� E���C!E��� DE�� �C8E���� ����� F�E8F�� DE� ��� ����FC�E� E�� B���E����DE��� �����
��FB���E����DE��BE����E��UA�������@T����!����E=��@E���E��C���DE�1�FA��E����E���EC��E�����
BE����E��UA� � (E� '<�E� �� E��� �F'��F� E���E� ����E�����1��A�� E���D��� 9GC�C�C�������*�$$�=��
�///=�J.Biol.Chem.:A��/����P�E�E���B��C����D�������DC--F�E�BC��C���U������DE���������C�C���
�EB��D�C�E� ��C���E� �E�25�!��C�� D�� '<�E� ��F�E��E� ��E� ���E�BE� D@E�����C��� D�� �����
E�D�B�C�E�U������DE���������C�C����EB��D�C�EA�E��E��C��E�D�����E����B�F�����E���E���E��
���E��BE����E��UA�$@E--E��C�B�!��E��DE����!����C��������E� �C'��'E�U��@E���C��E������E�-�C��
��@�������E� -�B�E���DE� BE��E� -�!C��E=�D���� ��� -��B�C��� �E!��E�K��E� ��<�� �ED��D���E�DE�
BE��E�DE�FA�=�E���E���C!F�D�����E��!K!E��DF��C��D�����E����B�F���A�91&5�/A��/C��E�25�DE�
1�FA�� �@�� ��E� �E�� D@E--E�� ���� �E� ���B�F��� �D���E=� ��E� B��DF��F�C��� �� ��� E--E�� �����
C!�������� ���� ��� �FD�B�C���D�������U� 9��D��$�A��2��������*�$$�=� ��//0=�Development:�
���� �������� ���2��1�FA�� �E��A� �E� ����� C�� �� F�F� �FBE!!E��� DF!����F� ��E� �E� '�C�� DE�
-��B�C���D��'<�E�1�FA��D��������������C�����F�E�D�B�C�E�F��C����--C������������CE��E��
�@E��E!��E� DE�� ��FB���E���� 8E��� ��� �C'��'E� U� 9)*�C++��� �� %�� ��� *�$$�=� � �/��=�
PLoS.Genet.:A� !��B�������������C�CA�B������AB���E����B�����������A�� C���D�EAC��������
;��E����B�CE����BB�A���B����
�
)�&>�E������!E!��E�DE� ��� ���E�-�!C��E�DE�� -�B�E����DE� �����B�C��C���>�#&*����A�)��
DE�����DE������P�E�D�����@E!����'E�<�E����B�F��C��E=�C��B��E�����C�����P�E�!�BE���D����
��� B���D��'E�<�E� E�� D���� ���DF�E�!C���C��� �E��E��E� D���� �E� �E���!��EA��E���!��E���
!E!��E��DE����-�!C��E�/��������E���C!F��D�����E����B�F���E��DF8E����E!E����!�C��BE�
DE��CE���E!��E��8�C����E����BE������C!�������E���E��E������E�A�.��E���E���C!F�E���E�)4�
E�� )��AE� D���� �E� D�!�C�E� DE� �D��� 9)������� ��� �� ��� *�$$�=� � �//"=�
Proc.Natl.Acad.Sci.U.S.A:A� .�� !����E� D��B� �E�� BE����E�� ���'F�C��CBE�� ���B�F��C��E�A�
/����P�E�D����BE��E��BC�E���DE�!�C��E�C���@CDE��C�F�DE�����'F�C�E����!���C���E�����-C��DE�
�E�!E���E� �E��� E�����C��� ����� DE� ��� �����C�C��� ��C!�C�EA� (EBC� �� F�F� DF!����F� E��
F��DC�����E���F�����E�DE����B�F���E!�������C�E��D�����@E���E��C���DE�/��4��8�C��F�F�
��FBC-C��E!E��� ����CE� D���� �E� D�!�C�E� �D��A� (E�� ���B�F��� ��F�E��E��� ��E�
��'!E����C��� DE� �@�������E� E�� ��E� DC!C���C��� DE� ��� ����C-F���C��� DE�� ���'F�C�E����
�D��[A�(EBC�E�������BCF�>���E���������CE����B�F��C��E�E����E���'!E����C���DE��BE����E��
R����� ���DE����FB�BE�� ��''F�������E�DC--F�E�BC��C�����F!����FE�DE� BE�����'F�C�E����
93$A����2�C�AD�1A�8��#�����*�$$�=� ��//-=�Genes Dev.:A�(E�DE��CE����C��=�B�!!E�������E�
8E��������������D=���''<�E���E�/��4�B��E�����P�E=��������DE����FB�BE�=�D�����E�!�C��CE��

����77�����
DE����8�CE���B���B�C8E�D�����E�����'F�C�E�������B�F��C��E�A�3���E����������D=�/��4�E���
E���C!F�D���� �E��BE����E��'�7[=�'<�E�!�BE���D��DF8E����E!E���E�D�B�C�EA� .���F'��E�
���C�C8E!E��� �@E���E��C��� DE� BE� DE��CE�� E�� �E� -C����� >� ���� ���!��E��� 9=�DD�-�� ��� ���
*�$$�=���//"=�Proc.Natl.Acad.Sci.U.S.A:=���''F�������E�/��4�������C�����P�E��F'����E���
D�� DF8E����E!E��� E�D�B�C�EA� ����� ��� �������'CE� ��!�C�E=� �@C��B�C8��C��� D�� '<�E�
B��D�C��>���E�D������CE�B�!��!F�C��E�E����E��F8E��C����E��E��E�B�!��<�E��������CE��E�
B�E0� �E�����CE����;F 6A�,�B�������DEA����������ACCDE�C�E���A��B��C������D�EAC����B������A�AC��
��� B��� ��BB�A���B����� ������A�CA�B� ����� �B� �A�� C��� !�� ���C� B�C�E� BD�B��AB�� ����
����DE�B�������A����������B��BC��B���D�����BC���������DEA����BD�B�C������B��<=�<8>�����
���� �C� �AB�A��B��� DC�BC� ��� 1?@=====� B�A���B���� ���� �DEA��� ��� ��E�A��BC�� ��BC� E�E��� �C�
���EC�����
�
Les facteurs de transcription clés de la différenciation du lignage endocrine
�$�� ��FBC-CB��C��� E�D�B�C�E� E��� C�C�CFE����� �@E���E��C��� �����C��C�E�D@��� -�B�E��� B�E-� DE�
���E� �F�CBE� ���B�E� �F�CBE=� D����B�DAD0� @9BD0AA� (E� '<�E� !����E� ��� �������C��� DE��
���'F�C�E����>�DE��C�FE�E�D�B�C�E�9D��D�����*�$$�=� ��//�=�Development:A�.��E���DF�EB�F�
D<��)GAE�D�������E���E��BE����E��DE��@F�C��F�C�!����B�F��C��E���F��!��C-�D�������D��[�
!�C�� ����C=� >� BE� ���DE=� D���� DE�� BE����E�� �D���=� ��''F����� ��E� ��E���E�� BE����E��
E�D�B�C�E�� ��FB�BE�� �E� DC--F�E�BCE��� C�DF�E�D�!!E��� DE� �D��A� )��E�� B���E����DE���
�������E!E��� ���� BE����E�� E�D�B�C�E�� C!!����E�=� ���!C��E�=� DFB�C�E�� ����� ����A� ����
�C��E����BEBC�E���C��E�����C��������C�D�����E�25�!��C���D�������E������E�8E����E���E��
BE����E�� E�D�B�C�E�� C!!����E�A� � �� )4AE� ��E���E�� BE����E�� DE� �@F���B�E� 8E�����E�
E���C!E���'�7A� �DE���)��AE=� ����E���E��C����E� �C!C�E�E��E��CE��E!E���D���� �������CE�
BE�����E�DE��@F�C��F�C�!����B�F��C��E=�E��!K!E��E!�����E�1��A�����FA��>�E���E��C���
F�E8FEA� '�7� � ��F�E��E� ��� �CB� � D@E���E��C��� >� )�EAE� ��C�� � ���� E���E��C��� DFB�C�E�
���'�E��C8E!E���B����@>�DE8E�C������E�>������C����BEA�$���F'����C���DE�BE�'<�E�E���!���
B�����!�C���E!��E�-�C�E�C��E�8E�C��DE��'<�E����<����C��C��C�E���E����E�#+�U�9'<�E�D��
DC��<�E�&5�6�:=�#E���9E--EB�E���DE� ���8�CE���B��D���������DC�B��E�������������:�E��
/��4=�E���E�����E�A�9+C'��E��7:�
�

����7;�����
��
�
���� �C��E���=� BE� '<�E� E��� E���C!F� D���� �E�� BE����E�� ���'F�C��CBE�� E��E��E�D�B�C�E�� E��
D������E���E�����'F�C�E�����E������������EC��D�����E��E����A�$E�25�!��C�������C��>�
DE�� ����C�� D���� �E� ���B�F��� �E� B���CE��� ���� D@T����� DE� $��'E������ � E�� ��B��E� BE����E�
E�D�B�C�E�9D�C�C��$�D�����*�$$�=���///=�Proc.Natl.Acad.Sci.U.S.A:A�$��%��&�������B��
��C�CA�B� �A�����A���� AB��CA��BC� ��� � � B�� ��B��AC� �� �B� �A�� C�� BD�B�C��� ������
�������E�CA�B��A���CA��� (��)���� )#5 �� F�� #�� ������� � �/����Diabetes4�$���#6� �� ��� #��
������� � �/���� J.Clin.Endocrinol.Metab)�� ���� �C��E���� C�� �� F�F� !����F� ��E� �E�� BE����E��
E���C!����'�7� �E��F�E��E���DE����FB���E����E�D�B�C�E����C���E���� 9���B�C'�������
*�$$�=� ��//'=�Development:�B�����E��DE��E�DC--F�E�BCE��E�� ����DE�������E� ���C�BC�����
���E��BE����C�E��E�D�B�C�E��9R=�U=�V�E����:���������E� �E� �C'��'E�DE��BE����E��W��@E�������
E�B��E� B��C�E!E��� F��BCDFA� $E�� �C'����� ��C� C�-��E�BE��� ��� DC--F�E�BC��C��� DE�� BE����E��
'�7�8E����@��E�����@����E�DE���C'�FE��E�D�B�C�E���E��E���E�B��E�-����A�F��!�C��=�DE��
E��F�CE�BE�� DE� �FE���E��C��� >� DC--F�E����!�!E���� D�� DF8E����E!E��� DE�'�7� D����
DE�� ���B�F��� '�7�25� ���� �E�!C�� DE� !E���E� E�� �8���� �E� �P�E� �������E� D�� �C!C�'�
D@E���E��C��� D���� �@��CE����C��� ��F-F�E��CE��E� 8E��� �@��E� ��� �@����E� DE�� �C'�FE��
E�D�B�C�E�A�)��E--E�=�D����BE�!�D<�E=� ����FE���E��C�����FB�BE�DE�'�7�9)GAQ:�B��D�C��
!�B��C��C�E!E���>����DF8E����E!E���R���������E�����FE���E��C������<��)��AE�B��D�C��
E��E��CE��E!E���>� ��� -��!��C���DE�BE����E��U�E����=�E��E�B��E������ ���D�9])�;AE:�>�DE��
BE����E���V�98��CD���D�2�������*�$$�=���//"=�Dev.Cell:A��
�
�
-AB����.0����F�E���DE��-�B�E����DE������B�C��C���B�����������@E���E��C���DE�
'�7��
�95�C8E��2���C��1C�C&�E��B���A=��HHG=�*E�E���E8:�

����7E�����
�+&5�@��B�$C�����+C*����E�"�&�"AD�ADBA�
$�� DFB��8E��E� DE� BE� -�B�E��� ���� � �-���� /� E�� B���A� � 9+�C"� )�� ��� *�$$�=� � �//-=�
BMC.Evol.Biol.:� E��� �FBE��EA� �<�� )QAE=� C�� E��� ���'E!E��� E���C!F� D���� �@E��E!��E� DE�
�@E�D�DE�!EA�^�����C��D@)4=�����E���E��C����E��E���EC������'�E��C8E!E��A��C��C�>�)�H=�
��� �E����8E� ���� E���E��C��� ����FC��E� � D���� ��E���E�� BE����E�� DE�� ����'E����
���B�F��C��E��D�������E��8E�������E��DE��@C��E��C�A���BE����DE��E��BE����E���-�F[��E�B��
E���C!E��� ���� �D��� !�C�� B��E���C!E��� 1��A�� E�� '�7A� )��E�� B���E����DE��� ����
BE����E��E�D�B�C�E�� C!!����E��D����������8����DFB>�DC�B��F���FBFDE!!E��A�^�����C��
D@)�EAE=�D�������E��CB�DE�DC--F�E�BC��C���E�D�B�C�E�9�CB�DE�'�7[:=��-�F�B����B��C�E��8EB�
'�7[�D������E�����CE�DE�����'F�C�E����E�D�B�C�E��E���@E���E��C����E�B�E8��B�E��8EB�
1��A�=�1�FA��E���D��A���)�GAE=��-�F�E���E���C!F�D��������E���E��BE����E��E�D�B�C�E��E��
BE��E� E���E��C��� E��� !�C��E��E� >� �@J'E� �D���EA� $E� 2�� !��C�� D�� '<�E� ��F�E��E� ���
���B�F���DF����8��DE�BE����E��E�D�B�C�E��!����E��E�BE��F��E��BE����E����A��E�������E��
����CBE������F�E��E�����E����F�CE�DC'E��C8E��E��������E�DE� �E���DFB<����FB�BEA� �$��%�
�&������ ��� �F��� ��DB�C���� �����DCD� ��B�� ��������A�� ��� ��� �D�A����� �A�A�AE�� �C� �B��
�A�EE�D������������E�CA�B���DCD�E�CE���D������AD���������C�CA�B�����A70:�(7��+���D��#��
���������/�/��Nature)���
�
)�� �8��� DE� '�7� E�� �-�F=� ����CE���� B�!�C��C����� DE� -�B�E���� DE� �����B�C��C��� 8����
��F�CDE�� >� ��� DC--F�E�BC��C��� ��FBC-C��E� DE�� �C'�FE�� E�D�B�C�E�� � E�� >� �E��� ����C�C�F�
9)��++������������*�$$�=� ��''"=�Nat.Genet.O�!�D�3���CD�9�����*�$$�=� ��/��=�Diabetes
Res.Clin.Pract.:A�$E��-�B�E�����E�������F��DCF�������A� �E��'<�E���C&4� �9��C�ED�����'E�E�
;:�E���E�9��C����E����E���ED���!E�����'E�E:���C�8������CE��E��D���������E!CE���E!����
�E�� BE����E��'�7[� ��C�� 8E������ �C'��'E�UXV���� 8E������ �C'��'ERX�����C�� ��� �F��E�BE�
D@E���E��C��� DE�� '<�E�� �C&5=� 91&� 9�A�� E�� FA�=� B-� �����:=� 9�����.� @E���'E�CB�
DC--E�E��C��C��� -�B���� �)=� 6�&.� ��� /� 9.�����C�����E� ��!E����� ����EC��:=� 6�$.� @.����C��
'E�E� E����BE�� ����EC� 1)� E�� #C+� 9!��B�������E����CB� -C������B�!�� ��B�'E�E�
��!���'�'E�E����E��%A���C�8�����E�!E���E����DC--F�E�BC��C����E�!C���E�E�����!������C���
DE� �@T���A� $�� -C'��E� BC�DE������ 9+C'��E� �;:� �FB��C���E� �E�� D���FE�� �B��E��E�� DE� ���
�CF���B�CE�D@E���E��C���DE�BE��DC--F�E����-�B�E����DE������B�C��C��A�
�

����7F�����
�
Les facteurs solubles
��E� ��!��E��� -�B�E���� C����� D�� !F��DE�!E� E�� DE� �@EB��DE�!E� �DB�BE���� �����
�FBE���C�E��>�DC--F�E��E��F���E��D��DF8E����E!E������B�F��C��E�B�E0��������C�A� �$E���
�B�C����E�-�C���������!�DE�����B�C�E�E��������C��������F'����C���DE��DC--F�E����-�B�E����DE�
�����B�C��C����8�����FBFDE!!E��A��
• $����E!C<�E�F���E�B���E����D�>������FBC-CB��C���D��D�!�C�E����B�F��C��EA�)��E�
�FBE��C�E� �@E��C�B�C��� DE� ��� 8�CE� #ED'E��'� D���� BE��E� �F'C��� DE� �@E�D�DE�!E=�
�@�B�C��� DE� -�B�E���� DE� B��C����BE� DE� ���E� +'-� E�� "*+U� E�� E�-C�� �@�B�C��� DE�
-�B�E����E�D���E�C���A��
• $��DE��CE!E�E���E� E��� ��� B��C����BE�D������� DE����'F�C�E���=� ��C� E��=� ������ >�
E��E=�������E�B����P�E�DE��8�CE��+'-=���B�=�L��=�)*+�E��"*+UA��
• )�� E�-C�� ��� DE��C<�E� F���E� B���E����D� >� ��� ��FBC-CB��C��� D�� �C'��'E� E�� >� ���
!������C�����C������������E�B����P�E�DE��8�CE��"*+U�E��)*+�93$A����2�C�AD�1A�8��
#�����*�$$�=���//-=�Genes Dev.:A��
���� ������� DF��C��E�� BC�DE������ ��E���E�� ��E�� DE� BE�� 8�CE�A� ����� BE� B���C��E=� �E��
D���FE�� B�E0� �@#�!!E� ����� ���E�� E�� ����� E��E��CE��E!E��� C���E�� DE� B�����E�� DE�
���B�F���-?����A��
�-�FX�
-AB����.4���(��B�DE�DE��-�B�E����DE������B�C��C���B����P��������
DC--E�E�BC��C���DE��DC--F�E�����C'��'E��
E�D�B�C�E���
9D@���<��%E��5��!���=��H�7=��C��E�E���E��
B�C�CB����B�:�

����7Q�����
$��8�CE�#ED'E��'�
�
.�� �� F�F�DF!����F���E� �������B���DE=���E!CE�� ��������DE� �@E�D�DE�!E�D������D���� ���
�F'C��� ��F��!��C8E� ���B�F��C��E� D�����E� 9+C'��E� �E:=� C��C��C�� ��� �C'���C���C���
#ED'E��'�9C��C�C�C���DE��@���DE��E��E--EB�E����A����CB��ED'E��':�D����BE��E��F'C�������
�E� �C�C�� D@���!�C��� DE��� -�B�E����A� �@�B�C8C�E� U%� 9-�!C��E� "*+U:� E�� +'-�� 92A��)��2�� ���
*�$$�=� ��''-=�Proc.Natl.Acad.Sci.U.S.AO���"��1�#�����*�$$�=� ��''-=�Genes Dev.:A�(E��E�
C��C�C�C��� DE� #ED'E��'� �E�!E�� �@�B�C8��C��� DE� �@E���E��C��� DE� �D��� D���� �@F���B�E�
���B�F��C��E� D�����E� E�� �C��C� �E� DF!����'E� DE� ��� !�����'E�<�E� ���B�F��C��EA�
$@F���B�E�8E�����E=�������>�E��E=�D�C�� �����C����!�����'E�<�E�>� �@C��C�C�C���DE� ���8�CE�
#ED'E��'A�(E��E�BC�E����E�-�C��DE����B��C����BE�D��DC8E��CB��E��F���C��E���C�8���E�!E���E�
D@F��C'�E�� �@E�D�DE�!E� ��F��!��C-� ���B�F��C��E� 8E������ DE� ��� �F'C��� D��!F��DE�!E�
B��DC���E� �CB�E� E�� -�B�E���� +'-� ���� #ED'E��'� 9�����*�� D�� ��� *�$$�=� � �//�=�
Development:A���������D�D�����E�DF8E����E!E������B�F��C��E=�BE��E�8�CE�#ED'E��'�E���
�EE���C!FE�D�����E����B�F����������D@)�7AE�9��"��1�#�����*�$$�=� ��''-=�Genes Dev.:A�
�� BE� ���DE� �E� �C8E��� D@E���E��C��� DE� DE��� DE� �E�� E--EB�E���� 9.�DC��� #ED'��'� E��
���B�ED�:� B��E� ��� �P�E� DE� �F'����C��� D�� ����� DE� ���'F�C�E���� �D��[� E�� ��C!������
�@E���E��C�������!!E���DE�+'-�H������E�!F�E�B��!E��F�C����B�F��C��EA��
�
�
�
$E���C'�����E�D���F�C����
�
DE��� )4=� ��E� -�C�� �@E���E��C��� D�����E� DE� �D��� C�D�C�E� ���� ��� ����B���DE=� BE��E�BC�
�@F��C'�E�DE� �@E�D�DE�!E����B�F��C��E� ����� �@E--E��DE� ��� -��C���DE��������E��D�����E�A��
-AB����.7���$E�����������DE�
�@E�D�DE�!E�E��DE��������B���DE��8�������
DF�C!C���C����
9#E���1�&A�E��B���A=���44G=�*E�E���E8:�

����7G�����
$E��BE����E��E�D���F�C��E��C�D�C�E����������@E���E��C���DE���-���E��!�C��CE��E���BE��E�DE�
�D���9=C������%�����*�$$�=���//�=�Science:A����
�
$���C'���C���C��������E��+'-�E�����8�CE���B��
�
5����DFB>�8��������������E��@���DE��!E!��E��DE�BE��E�-�!C��E�9+'-�:�B���C������P�E�D����
��� ��FBC-CB��C��� DE� ��� �F'C��� ���B�F��C��EA� ����� ���D=� �@E�����C��� D�� ����� DE��
���'F�C�E�������B�F��C��E���E�D���� ��� �����C�C�����C!�C�E� E��� ����� �E� B����P�E� E���E�
����E�DE�+'-�H� 9-C���������'��,��� -�B�����H:A� (E� -�B�E���DE� B��C����BE=� �EB�F�F����� �E�
!F�E�B��!E��F�C���B�F��C��E=���F�E��E���E��B�C��� ��FBC-C��E� ���� �������C-F���C���DE�
BE����E�� ���'F�C��CBE�� F�C��F�C��E�� E���C!���� /�#1� (��� ��#�� 8�� #�� ������� � �'''��
Proc.Natl.Acad.Sci.U.S.A4�D+��+ �� C�� #�� ������� � �//���Development)�� '�� ����E�C�AE��
������A�� �� ��� ��BCE�E� ���B� ���CA��BC� ���� D�������� ��B�ED�CA����� ���E��BB�AE��� ���
E�B���E� ��� ����AB��� �B� �ED��B��� ��� 7��1=�� �B� �����AC� ��CA��E� ��� �E��A�DE�CA�B� ����
�E��DBAC��E����B�ED�CA�����������BC�E����E�B���E����C��B���������������BC�E����������
��� ���������B���A� ����D�������AC� (9#� 8�� #�� ������� � �//0��Diabetologia4�C�� ��� ��� #�� ��������
�//"��Diabetes)�� �@����E�� F��DE�� ���� DF!����F� ��S��E� C!�������E� ����CE� DE� BE��E�
�B�C��� DE� +'-�H� F��C�� �E� -�C�� DE� �@�B�C8��C��� DE� ��� 8�CE� ��B�� D���� �@F�C��F�C�!=�
�����C������ >� �@E���E��C��� DE� #E��� 9#�C��� ��D� E����BE�� �-� ���C�� � �:� ��C� ��F8CE��� ���
DC--F�E�BC��C�����FB�BE�E�D�B�C�E�E�� C��C����� �@E���E��C���DE�'�7A�#E���������C���E�
�B�C���DE���E8E��C���DE����DC--F�E�BC��C���E��B�C�E���FB�BE�E��C��C�������-��A�(E��DE���
F�F!E�����E�!E��E����C��C���E�����E�E�����C���D������'E������B�F��C��E�9#���C�B��
=��������*�$$�=� ��//�=�Proc.Natl.Acad.Sci.U.S.AO�%�DA�-�����*�$$�=� ��//!=�DevelopmentO�
#A�C$$���-�����*�$$�=���//1=�Int.J.Dev.Biol.:]�.��E���C!��������DE����E����E��@E--E��DE�BE��E�
8�CE� DE� �C'���C���C��� E���!��C!��� ���� �E�� BE����E�� �D��[� ��� B����B�� D��!F�E�B��!E�
�E�C���B�E��C��E�E���E���!�C���C!�������E�D�����E�BE���E�DE��@F�C��F�C�!=�>�DC����BE�D��
!F�E�B��!EA�(EBC� E���C��E��������C� ��� DC--F�E�BC��C��� E�D�B�C�E�DF!���E� ��� BE���E�
DE����'���DE=�B�!!E�8����FBFDE!!E��A��
�
�
�
�

����74�����
Les modèles d’étude du développement pancréatique humain
�
��� B����� DE�� DE��C<�E�� ���FE�=� DE�� ���'�<�� !�BE���� ���� F�F� �BB�!��C�� D���� ���
DE�B�C��C���DE��F���E����C��F'C��E����@����'E�<�E����B�F��C��E�!��C�EA�(EBC�E����E��-�C��
D�� DF8E����E!E��� DS�����B�E�� DE� ����� E�� ����� �E��C�E��E�� E�� ����C��C��FE�=�
����!!E����E��F��DE��DE��C'��'E�>�����C��DE�����C�������'F�C��E���8EB�'�C������E��E�DE�
-��B�C���� �����E�� ��� C�D�B�C��E�� '�JBE� ���� ����<!E�� ��C�C����� ��� �EB�!�C���E� (�E� ���
�@C�D�B�C���D@E���E��C�������DE�����C�E��E���������C�C�C�F�D@C��E���!��E�E��D@���E�8E���E��
E--E��� DE� BE�� !�DC-CB��C���� >� DE�� ���DE�� ��FBC�� D�� DF8E����E!E��A� )�� ����E=� �E��
!F���DE�� D@F��DE� C�� 8C���� �E� ����� ���� E�� �E��E� ��C���E� �E� �C!C�'� DE� DF8E����E!E���
B�E0� �E� ���'E��� �E�!E�� D@���E�8E�=� E�� B�����E=� �E�� E--E��� DE� -�B�E���� ������E�� ���� BE�
DF8E����E!E��A�(E���EB��C��E��!��C�E���@����DE��C!C�E���E��@C!�'C���C�����!�C�E�E��
�E�� ���'�<�� �EB�����'C��E�A� )�� �E8��B�E=� �E�� D���FE�� ���� �E� DF8E����E!E��� D��
���B�F��� ��!�C�� �E��E��� ���E�A� 3�E� �C!C���C��� !�BE��E� >� BE��E� B����C����BE� E���
�SC�B���BC�F�DE���C8�E����'C��DC���E!E��� ����DE�!�DC-CE�� C��8C8���E��DC--F�E��E��F���E��
DF8E����E!E����E�� �8EB� �E�� !�D<�E�� DF8E����F�� B����S>� ��F�E��A� 3�E� DE��C<!E�
�C!C���C����E��E����DC--CB���F�DS�BB<�������C�����E!�������C�E�����-?�����B���E����D����
>�DE�����DE����FBC-C��E��D��DF8E����E!E���E�������C�F�E��E������C�F���--C����E�A��
�
$E�����8����C�C�C����D@E!������'CE�DE�B�C��C8E���!�C�E������E�!C��DE�!E���E�E�����BE�
�E�� DC--F�E��E�� F���E�� DE� ��� '��������C��� E�� �E� DE8E�C�� DE�� DC--F�E���� -E�C��E���
��C!��DC���� 9E�D������E=� EB�������E=� !F�������E:A� .��� ���� ����C� �E�!C�� DE� DF-C�C�� ���
B�������'CE�DE� BE� DF8E����E!E��A� .�� �E��E��F��!�C�����E� BE��� �E��F�E��E���E� F��DE�
!�������'C��E� ��<�� � ����C��E� ��C� �E� �E��� �E�!E���E� DE� DFB����E�� ��FBC�F!E��� �E��
�B�E����!��FB���C�E��E���E�����P�E��D����BE�����BE����A��E�����=��@���E��C���DE��C�����DE�
����E� ����C�F� ���� DC--F�E���� ���DE�� DE� DF8E����E!E��� E�� �E� B�!�������� ��B��� �C�C��
����C��E� D@������E� E��� -C���E!E��� ���E0� DC--CBC�EA� )�� E--E�� �@�BB<�� ���� �C�����
E!�������C�E�� ��� -?����� E��� F8CDE!!E��� B���E� �E�� �C�FE� E�� D���� �E� B�D�E� DE��
��������C�E�� DE� -?���������'CE� ���� DF-C�C�C��� �E�� -?���� ������F�� ����� C�����
D@C��E�����C���� ��F���E��C��E�� DE� '����E��E� �����!��-��!��C��A� � .�� �E��E� �F��!�C���
��E� �E�� C�-��!��C���� ���E��E�� ���� BE�F� �E�� ���E�� DE� �@F��DE� DE�� !FB��C�!E�� DE�
��FBC-CB��C���E���F'C����C���C���D@��'��E�E��E�-C��DE�DC--F�E�BC��C���E��!������C��A��
�

����;H�����
����� �E� !K!E� ��D�E� D@CDFE=� �@F��DE� DE�� ��F�����E�� ����BCF�� >� DE�� !����C���� DE�
BE���C��� '<�E�� E�� ����C��E� B�C�C��E� �E�!E�� DE� B��-C�!E�� ��� D@C�-C�!E�� �E�� D���FE��
C���E��DE�����EB�E�B�E�B�E0��E����'E��A�(E��E������B�E����E�!C������!!E���DE�!E���E�
E��F8CDE�BE�DE��DC--F�E�BE���C'�C-CB��C8E��E���E��E��DE���E��<BE��D���������DC�B��E�����
�������C�A��E�������E��B���F��E�BE��-C�E��DE�BE��!����C���������E����B�F����E��E�8E���
K��E�E�����FE����E�����DE���E�����C���'C��E�����'�C�����C���E��@�BB<�������C�����!��F�=�
�����DE����C�����F8CDE��E�=��@E����������B���������C��EA�
�
�����DF����E��BE�� �C!C���C���=� �E� ��������C�E�D@�BB�EC���@E�������B�F�DE��C�� �E�DF�����>�
DF8E����E�� DE�� !�D<�E�� D@F��DE� D�� DF8E����E!E��� E�� DE� ��� DC--F�E�BC��C���
���B�F��C��E� E�D�B�C�E� >� ����C�� DE� �C����� E!�������C�E�� ��� -?����� !��C��� ���
��!�C��� � 9#A�C$$��� -�� ��� *�$$�=� � �''-=� J.Cell Biol.O� #A�C$$��� -�� ��� *�$$�=� � �'''=�
Proc.Natl.Acad.Sci.U.S.AO�!����CD������*�$$�=� ��//�=�DevelopmentO��C��CADB�#�����
*�$$�=� � �//�=� DiabetologiaO� %$B�C'A� =�� ��� *�$$�=� � �//�=� Proc.Natl.Acad.Sci.U.S.AO�
�C��CADB�#�����*�$$�=���//0=�Dev.Dyn.:A�$E�����B�F�����!�C���C!!����E����������E���=�
���<�������C���C����D!C�C�����C8E�E�� B���E��E!E���DE�����CE��E�=�����DC��EB�C��� �����
����E��C��B���C�E�D��!��F�CE��E!�������C�E����-?����C����D@C��E�����C���8������C�E�DE�
'����E��E�9.D*:A�(E��E�!F���DE�D���E��BB<��>�DE�����B�F���D�����E�����DE���E�8E����E�
�C��E�� E���E�F/��E�� ��/�=� D��E� �C!C�E�DE� �@.D*� E��+���BEA�������C�� DE� BE�����B�F��� �E�
��������C�E� ��C�C�E� DE��� ���E�� D@�����B�E��A� ��E� �����B�E� C�� 8C���� E�� ��E� �����B�E�
DF8E����E!E����E���E��8C8�XC��8C8���A�$E��!F���DE��C��8C������������FE���������!C�E�E��
B�����E� DE� -��'!E���� DE� BE�� ���B�F��� ���� DE�� ��������� DE� ���E� -C���E� -�������� >�
�@C��E�-�BE� �C���C��CDE� ��� E�� !���CBE� ���CDE� ���E� B����'<�E� ��� !���C'E�A� $@�8����'E�
��F��C��E�DE� BE��E� �����B�E� E��� DE����8�C�� C!�'C�E��DE�� E��F�CE�BE���E�!E������DE�
�E��E�� �@E--E�� DE� BE���C��� -�B�E���� ������E�� ���� �E� DF8E����E!E��� E�D�B�C�EA�
&���E��E��E!E��=� B�����C�E!E��� ��� !�D<�E� !��C�� �_� �E� �C!C�'� DE� DF8E����E!E���
B����� �E�!E�� �@���E��C��� D@C�-��!��C���� D���� DE�� DF��C�� ���CDE�=� �E� DF8E����E!E���
��!�C���@F���������������CE�����E!�C�E�=� C���@E�����������C��E�DE�!�C��E�C��E��B�����E�
BE�� -��'!E���� ���B�F��C��E�� C!!����E�� ��� DE�>� DE� �H� B����� D���� ����E� E��F�CE�BE�
9+C'��E��F:A�$E��D���FE�����8����K��E����E��E�������DE�-�C���C!C�FE�A�
�

����;������
�
�
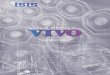
�$�� DE��C<!E� �����B�E� D@F��DE� DE� BE�� ���B�F��� ��!�C��� E��� ��E� �����B�E� DC�E� ��E��
8C8�XC�� 8C8���A� ��� DF����DE�� ���FE��GH=�%E����D�)A�"�B�� 9;�*��!��%����� *�$$�=� ��'-!=�
DiabetesO� ;�*�� !�� %�� ��� *�$$�=� � �'-0=� Transplant.Proc.O� ;�*�� !�� %�� ��� *�$$�=� � �'--=�
Transplantation:� �8�C�� !C�� ��� ��C��� ��� !�D<�E� DE� '�E--E� DE� -��'!E���� DE� ���B�F���
-?�����E�������B����F��B�E0��������C���C!!����DF-CBCE��E���DEA�.����C�C��C��DE�����B�F���
E���E� �;� E�� �G/�� E�� ���E�8�C�� ��E� ��'!E����C��� DE� ��� !���E� β� � !�C�� E�� �����C�F�
C���--C����E�����������������C8E������E�D�A�/E�����@���E������8��B����C���C�������C8E���
����� B����F� F��C�� ����� -�C��E� ����� ����E�C�� ��� DF8E����E!E��� ���B�F��C��E� B�!��E�A�
(E��E�F��C�E�DFBCD��D��B�DE�!�DC-CE���E��C�E�DE�'�E--E�E���E������DC--F�E��E�����E����C8E��
�E����E�A����B�����E��F���E=��E�-�CE�E��������E�E��DF!����<�E�����E����B�����E��F���E�F��C��
����C�E�������E�!C��C-����DF8E����E!E���E�D�B�C�EA�$@��E�DE��'���DE��B�C�C��E��DE�BE��
���8����F��C���@��C�C���C���DE����B�F���>�DE�����DE����<�����DC-��D��DF8E����E!E����8EB�
�@C!����C�C�C�F� D��B� DE� B��B���E� ������ >� ��� ����C�C�C�F� D@���E�C�� ��� DF8E����E!E���
E�D�B�C�E� >� ����C�� DE� ���'F�C�E���� ���B�F��C��E�A� (E� �C�E� DE� '�E--E� �8�C�� F�F� ����C�
��FBFDE!!E�����C�C�FE=�D����D@����E��F��C�E�=������'�E--E��DE��T�����!����E����!�C���
���!��C��� E�� DE�����B�F��� -?�����!��C��� 9#�D�CDC�%�����*�$$�=� ��''�=�J.Clin.InvestO�
�C�C$$A���#�� ��� *�$$�=� � �''0=�Transplantation:. (E��E� �EB��C��E� �� F�F� �E��C�E� D���� �E�
ins-cpa-Hoechst gluc-pdx1-Hoechst
J0
J20
J40
-AB�����.5�����B�F������!�C��DE��H�/�=�B�����E�����-C���E�-��������.!!���-����E�BE�BE�'��B�'���9'��B:=�C����CC�E�9C��:=�B���9B�������E��CD��E��=�!����E����BC��C�E:�E���D��A����DE�>�DE�C�H=����DE��C�F�BE�����C�E��D���[�DFB��C��D����C��E!E���E��������E�8E���B��E�BE����E�E�D�B�C�E�!����EA��

����;������
��������C�E� D@�BB�EC�� >� ����C�� DE� �HH�=� ���� (����C�'� E�� B���A� �8EB� ����� ��C�BC���E��
!�DC-CB��C����A�C:��@��C�C���C���DE����B�F���C!!����E��E!�������C�E�����-?�����9E���E�
Q� E�� ��/�:� ��FB�BE�� ���� �������� ���� ���8���� C�C�C���� DE�%A)A� "�B�� CC:� �@��C�C���C��� DE�
����C�� C!!����C�B�!�F�E��E� /(.�� 9�C��CADB� #�� ��� *�$$�=� � �//�=� Diabetologia:A� $E�
B��C�� D�� �C�E� �E��C�� >� �@C!������BE� DE� ��� 8��B����C���C��� �F���E� E�� �E� B���B�<�E�
BC�B���B�C�� DE� BE�� E���BE� E���E� �E� ���E�B��!E� E�� ��� B�����EA� (����C�'� E�� B���A� ����
DF!����F���E�BE�!�D<�E�DE�����C������!��C�FE����FB��C����C���@E��E!��E�DE��F���E��D��
DF8E����E!E���E�D�B�C�E�E��E��B�C�E�E����E�BE��'�E--����F��CE���B�����E��DE��F'��E��
E--CB�BE!E������'��BF!CE�DE�����C�����<��DF��F�C���D����������C-A� �(E�!�D<�E����C��C�
�E�!C�� D@�BB�!��E�� ��� BE���C�� ��!��E� DE� D���FE�� D@���E�8��C��� ���� �E�� DC--F�E����
���DE�� DE� DF8E����E!E��� D�� ���B�F��� ��!�C�� 9�C��CADB� #�� ��� *�$$�=� � �//�=�
DiabetologiaO� �C��CADB� #�� ��� *�$$�=� � �//0=� Dev.Dyn.O� �C��CADB� #�� ��� *�$$�=� � �//0=�
Diabetologia:A� ����� ���D=� C�� �� ����C� �E�!C�� ��� ��������C�E� DE� B�FE�� ��� !�D<�E� DE�
���B�F��� �����'F�C��E� ����CE�� ���� �����D�B�C��� 8C���E� DE� '<�E�� D@C��F�K�� D���� �E�
���B�F��� DC���BCF� �8���� ��� '�E--E� 9)*�C�+�CDD� ��� ��� *�$$�=� � �//-=� PLoS.One.:A� $��
!F���DE� B���C��E� E�� ��E� DC���BC��C��� !FB��C��E� ��F�����E� D�� ���B�F��=� ��C�� ��E�
C�B����C���DE�����8EB���E������C���DE��E��C8C����C��F'��������'<�E��������E���������E�
B����P�E�D@������!��E���D@C��F�K�A��
��BE� B���=�E��>�����E�B����C����BE=� BE�!�D<�E��E��F�E��E� �@��C��E�!�D<�E�DE���C8C�D��
DF8E����E!E���E�D�B�C�E�D�����B�F�����!�C��D�����DE�E!�������C�E�������DE�-?����
�E�!C���A� "���E-�C�=� ��� '�E--E� ����� ��� B�����E� �F���E� �E��E� �EB��C��E!E��� DC--CBC�E=�
B��������'E� E�� �@E��� �8F�FE� K��E� ���!�D<�E� DC--CBC�E� >�!��C���E�� ���� �E�� B�����C��E��
C��F�E��E�������E�������C�����F!�D���!C��E��C�D�C�E�������E�DF8E����E!E���DE�BE��
'����'�E--�������B����B��D���EC��E��DE��������F���E�9+C'��E��Q:A�

����;7�����
�
��������������������
-AB�����.:A�*�E--E�DE����B�F�����!�C�������
���B�����E��F���E��
�A����B�F���E!�������C�E�DE�G/��%A�Q�B��������<��'�E--E�(A���!�C�����<��'�E--E��A�F�!�C�����<��'�E--E�)A�4�!�C�����<��'�E--E�
�9�(����C�'�&�E��B���A=��HH�=��C��E����'C�:�

����;;�����
Rationnel du travail de thèse
���
%CE�� ��E� �E�� !�D<�E�� !��C��� ���� ���'E!E��� B����C��F� >� ����E� B�!��F�E��C��� DE��
���BE����� 'F�F�C��E�� E�� !��FB���C�E�� ��C� ��F�CDE��� >� ��� DE��C�FE� ���B�F��C��E=� �E�
�F�E���E�� �E��C!C�'�D@E���E��C���DE��-�B�E����DE������B�C��C���E��DE��-�B�E����������E��
B����P������E�DF8E����E!E�����!�C��������E��B������E��F��DCF�A��E���!��E������EB���
�E!��E��� �F��!�C��� B���E�8F�� E���E� �E�� ���'E���� E�� �E�� ��!�C��=� D�� !�C��� ����
��E!CE��� ���DE�� DE� DF8E����E!E��� D�� ���B�F��A� ���� E�E!��E=� DC--F�E���� ��'�!E����
���8E�����DE� �@F��DE�DE��DC��<�E���F�����������DE��DC��<�E��D�� ��BE�� BE��E� 9&5�6:�
B��-C�!E��� ��E� �� �=� �"+��� E�� *7� B��E��� DE�� �P�E�� �C!C��C�E�� ��� B����� D��
DF8E����E!E������B�F��C��E�D�����E��DE���E��<BE�A�&�C��D@����E��D���FE��������E���
DE�� F�F!E���� E�� -�8E��� DE� DC--F�E�BE�� !�BE���� ���� �E� �P�E� DE� BE���C��� -�B�E���� DE�
�����B�C��C�����C��'C��CE�����FB�BE!E���D�����E�DF8E����E!E������B�F��C��E����D����
���DC--F�E�BC��C���DE��DC--F�E�����C'��'E��E�D�B�C�E�A�����E��E��B���A�9�����$$�������*�$$�=��
�/��=�Diabetologia:=�D������E�F��DE�DE������B�C���!E�DE��DC--F�E�������E��BE�����C�E��
���B�F��C��E����!�C��� �D���E�=� ����!C�� E�� F8CDE�BE���E� E���E��C���DC--F�E��CE��E�DE�
&�+%�D�����E��BE����E��α�E��β�!��C�E��E����!�C�E��9B-�-C'��E:A�(E�-�B�E���F��C��B����@>�
��F�E���DF-C�C�B�!!E����!����E���DE����DC--F�E�BC��C���DE����BE����E�α�B�E0��������C��
9��D���6�����*�$$�=���//1=�Diabetes:�E�����E���DE����BE����E�βA�(�E0��@#�!!E=��E�����E����
����!C��E��F8CDE�BE���E�E���E��C���DE�&�+%�D�����E��BE����E��β�>�����C8E���F��C8��E���
>� BE��C� ���E�8F� D���� �E�� BE����E�� α=� ��''F����� �C��C� ��� �P�E� DE� BE� DE��CE�� D���� ���
DC--F�E�BC��C���βA��3������E�E�E!��E�E���������F������E����8�C��B�C�C��E�DE�$��'�����E��E��
B���A� 9=CDB�� $$�D� ��� ��� *�$$�=� � �/��=� Nat.Genet.:� DC�B��F� ����� ����=� ��C=� B�E0� DE��
���CE���� ��F�E������ ��� DC��<�E� �F������� �8EB� �'F�F�CE� ���B�F��C��E=� ���� !C�� E��
F8CDE�BE� DE��!����C���� �F�F��0�'��E�� C��B�C8���CBE�� DE�*�"�F� ������ ��E� BE��!K!E��
!����C����B�E0��������C���@�����C��E����������!K!E���F�����EA�)��E--E�=� �E�25�!��C��
DE� *�"�F� E��� ��FB�BE!E��� �F���� E�� �@C��B�C8��C��� ��FBC-C��E� D�� '<�E� ���� ��� ����<!E�
(�E����=�D�����E��BE����E���D����@C�D�C������������F�����E����B�F��C��E�����C�D����C��EA�
(E�� DE��� E�E!��E�� ������E��� DE�� ��'�!E���� -����� ����� �E��E�� ��E� �@E!����'E�<�E�
���B�F��C��E���!�C�E��E���C������B�!��<�E!E����E��������B����@>���F�E���DFB�C��B�E0�
�������C�A��@����E��DC--F�E�BE��E�C��E���E�B��E�E���E� �E��DE���E��<BE�A������BE��E� �C��E�
����E������C8E=�����E�����B���E���E��DC--F�E�BE��D@��B�C�EB���E�DE��@T����D�����E����B�F���

����;E�����
��!�C��E���E����B�F���!��C��9B-�-C'��E:=�����E��C����BE�DE��@E���E��C���DE��� ��D�����E�
���B�F���E��B�C�E���!�C���D���E� ���������E�BE��E�BC�DC�����T��B�E0� �������C���D���E=� ���
�������C���DE��BE����E��B����C�������@T�����D���E=�E���E������DE�����C-F���C���DE��BE����E��β�
!����E�� ����� F�E8F� B�E0� ��� ����C�� ���� �������� >� �@#�!!EA "���E�� BE�� D���FE�� �����
���������D@��E�C!������BE�B��C���E�>��@�E��E��_��@����@��CE��E�8E��������F���CE�BE�����C�E�
D���� �E� ���C�E!E��� D�� DC��<�EA� )�� E--E�=� ����� ����CE�� BE��E� C���--C���BE� ���B�F��C��E�
E�D�B�C�E=� �E����F���E��C��E��DF8E����FE���B��E��E!E���-�������E��>���E������F'CE�DE�
�����C���C��� BE��E�� ��<�� E--CB�BE� !�C�� ��C� DE!E��E� ����EC'����E� E�� ���� DF-C�C�C���
C!���-�C�E� ��C���@C�� �@�'C�� D@���EC�D�E� ��E� � ��!F�����CE� E�� �E� �����C������ ����
!FB��C�!E�� DE� �F'����C��� E���K!E!E��� ��FBC�� E�� B���C���� DE� BE��E� '���DEA� $E��
B�!��CB��C���� >� ���'� �E�!E� ����� D@�C��E���� ���CDE!E��� �ED������E�� B�E0� �E�� ���CE����
���� B�!��C����A� �E� BE� -�C�=� DE� ���8E��E�� �����F'CE�� ��F���E��C��E�� ���FE�� ���� ���
��F���CE� BE�����C�E� ���� F�F� DF8E����FE�� BE�� 7H� DE��C<�E�� ���FE�A� �B��C��� E�� B���A�
DFB�C8C�E��=� E�� �4QQ=� ��� ��E!C<�E� ����'�E--E� D@T����� DE� $��'E������ 99C�C�ACD� 8�� )�� ���
*�$$�=� � �'""=� Transplant.Proc.:A� (E��E� �EB��C��E� E��� !�C��E����� ��C�C�FE� DE� !��C<�E�
�E���D�B�C��E� B�E0� BE���C��� ���CE���� DC��F�C��E�� � 92�����$�D� !�� ��� *�$$�=� � �''-=�
DiabetologiaO�)�C�A�����#�����*�$$�=� ��///=�Diabetes Technol.Ther.O�)�C�A�����#�����
*�$$�=� � �///=� N.Engl.J.Med.:� !�C�� B�!����E� �F��!�C��� DE�� B�����C��E�� ��C� �����
E��E��CE��E!E��� DE� ���C�� ��D�E��A� �E� ���C�E!E��� C!!��������E��E��=� ��� D��FE� DE� 8CE�
�C!C�FE�DE��'�E--����E���E�-�C��E���!��E�DE�D���E����B�!���F�������!��E�����EBE8E����
���E��CE��� 9�������2�� 6�� ��� *�$$�=� � �//!=� J.Clin.InvestO� )�C�A�����#�� ��� *�$$�=� � �//1=�
N.Engl.J.Med.:A�.��E�C��E���F��C��E!E�������CE���������F'CE��������!��C-CE�����!���E�DE�
BE����E��β�-��B�C���E��E�A�C:��B�C8E���������C-F���C���DE��BE����E��β���FE�C�����E��9�������
��� *�$$�=� � �//!=�Nature:� CC:� 'F�F�E�� DE� ���8E��E�� BE����E��β� -��B�C���E��E�� >� ����C�� DE�
BE����E�� ���B�E�� E!�������C�E�� ���C���E��E�� 9�H����� 2�� �� ��� *�$$�=� � �//0=�
Nat.Biotechnol.O��H����� 2�� �� ��� *�$$�=� � �//1=�Nat.Biotechnol.O� 2���D� %�� ��� *�$$�=��
�//-=�Nat.Biotechnol.:O� CCC:� C�D�C�E� ��� �F'F�F���C��� DE� ���'F�C�E������F�E���� D���� �E�
���B�F��� �D���E� E�� BE����E��β� 9E��E�� ��� *�$$�=� � �//-=�Cell:A� $��!C�E� E��?�8�E� DE� BE��
���8E��E�� �����B�E�� ��F���E��C��E�� ����E� ���� DE�� F��DE�� �����-��DCE�� DE��
!FB��C�!E��DE��F'����C���D��DF8E����E!E���D�����B�F�����!�C��E�����B�!��F�E��C���
DE��!FB��C�!E��DE��F'����C���DE����!���E�DE��BE����E��β�E���F�C�DE���F�E�����������EA��
�-C��DE��E�!E���E�D@�8��BE���������B�!��F�E��C���DE�BE��!FB��C�!E�=�C��E���C!��������
DE��E�D��E��D@���C�������C��E�-��!�������E�BE�����C�C�F��B�E0��E����'E��A�(@E���D����BE��E�

����;F�����
���C��E���E�������8�����F-�FB�C�>��@CDFE��DE��E�D�E������D���!C��E��E�!�D<�E�DE�'�E--E�
DE����B�F�����!�C����C�C�F������E���������C�EA�
�

����;Q�����
������ ����������
,�B�� ��� CE���A��� B���� ���B�� �D������D� �C� ���A�D� �B� B������ ��CA�� �DC���� ���
�D���������BC� ��B�ED�CA���� ����AB� �� ��ECAE� ��� �E������ ��� ��B�ED��� A���C�E���� �B�
��CE���B�������B���D��BCED���A����C�����A��������ED�E��B���B�ED�������AB���ECA������BC�
CE�B��DBA���� AB� �A��� �B� ED��A��BC� ��� CE�B���EC� ��� � B��� �D�AD� ��E� ��BCA�AE���� "����
�ED��BC�B��A�A�����ED���C�C���������E�����B�ED���D��C�B����;�A�B�B�����ECA����ED���AC���BC�
��B��������������CE����#���

����;G�����
Article : Le muscle représente un site de greffe permissif pour le développement du pancréas immature humain
�
�
1. Stratégie et méthode
��������� DE� �@E��F�CE�BE� D�� ��������C�E� D@�BB�EC�� ���� ��� '�E--E� DE� ���B�F���
E!�������C�E�� ��!�C��� E�� !��C��� ����� ��� B�����E� �F���E=� ����� �8���� DF8E����F� E��
8��CDF�����C�E����E����C-�DE�'�E--E�DE�����B�F���E!�������C�E��DE�BE��DE���E��<BE�������
�SE�C!��C�!� DE�� !��B�E�� ���E�E��C��E�� DE� ��� B�C��EA� 3�C�C����� BE� !�D<�E� ����� �8����
���E�8F��E��F���E��DE����DC--F�E�BC��C���E�D�B�C�E��E��������F��SE���E��C���DE�-�B�E����
DE� �����B�C��C��� B�F�� ��C� ��F�CDE��� >� BE� DF8E����E!E��A� ����� -C�C�=� ����� �8����
DF!����F� ��� -�C���C�C�F� D�� � �����-E��� DE� '<�E� ��C�� 8C8���� ���� �@SC��E�!FDC�C�E� DE�
�E��C8C������������DE��'<�E���������E����������E�B����P�E�DE����!��E������FBC-C��E�A�
$E�����B�F�����C�C�F��F��CE���C���F����C��>�����C��DE�����C��'E�����E��>�)��AE���C��>�����C��
D�� !��F�CE�� E!�������C�E� C���� D@C��E�����C��� 8������C�E� DE� '����E��E� E���E� Q� E�� 4�
�E!�C�E��DE�DF8E����E!E��=�E��B��-��!C�F��8EB���� �F'C����C���-���N�C�E�E��8C'�E���E��
����DC�EB�C8E��DE�����E�C���C���C��A��
�
$E�� ��C!���� �EBE8E���� F��CE��� DE�� ����C�� C!!����C�B�!�F�E��E�� /(.�� DE� F� >� G�
�E!�C�E��DE�8CE�!�C��E��E��D����DE��B��DC�C����D@F�E8�'E���F�C�E�A������ ���'�E--E=� �E��
����C��F��CE�����E���F�CFE���8EB����!F���'E�1F��!C�E�X�����0C�EA� 95mg/ml ketamine et
0.5mg/ml xylazine, injection intraperitoneale). Les pancréas F��CE��� E���C�E� C!�����F�� 9��
����'�E--E:=������!CB���B��E=���C����������B�����E��F���E�B�!!E�DFB�C����FBFDE!!E���
9�C��CADB�#�����*�$$�=���//�=�Diabetologia:���C��������@E�C!��C�!�!��B���C�E�D���CBE���
-F!��������D��'���D�-E��CE��9+C'��E��G:A��
�

����;4�����
�
�
^�DC--F�E�����E!��=��E��'�E--����F��CE�����F�E8F��E��������F������C!!����C���B�C!CE����
!CB���B��CE� F�EB����C��EA� (E���C��� ��C!���� -��E��� ���!C�� >� DE�� �E���� -��B�C���E����
9�E���D@���E�'��BF!CE����8���FE��C������F�C���F��E�E���E����DE�DE����B�C���D�����B�F���
3 mois post greffe
6 mois post greffe
-AB����.<��*�E--E�DE����B�F�����!�C��C!!����E�D�����E�
!��B�E���

����EH�����
DE� �@��C!��� �EBE8E��� ���� �������E:� �-C�� D@F8���E�� ��� ����C�F� D�� DF8E����E!E��� D��
'�E--��A� )�-C�=� D@����E�� ��C!���� -��E��� ��C�C�F�� ����� DF8E����E�� ��� !F���DE� DE�
�����-E���DE�'<�EA��
���
2. Résumé des résultats
�
D��CD��C���D��!�D<�E�DE�'�E--E�C����!��B���C�E�
�A ����� ��� ��E!CE�� � �E!��� ����� �8���� DF!����F� ��E� ��� '�E--E� D���� �E� !��B�E� DE�
���B�F��� !��C��� >� )��AE� � DE� DF8E����E!E��� � �����C���C�� >� ��� DF8E����E!E���
F��C8��E���>����'�E--E���������B�����E��F���EA�$E������C��F��CE�����B�C-CFE��>�C�E�E���E��
'�E--���� ��F�E8F�� ����� ������E� 9-C'��E� �:A� $E�� BE����E�� E�D�B�C�E�� �@F��CE��� �CE��
DF8E����FE�����<��BE��E��F�C�DE�DE�'�E--E=�E�����E��E��E���!�����'E������@C����C�E�E��
�E�'��B�'���E���E�����'��C���C���E��T�����8EB����BE���E�β�E�����!���E���B����C��F�DE��
����E��BE����E��E�D�B�C�E�=�B�!!E�D�����E����B�F���!��C���D���E�9B-A�C����D�B�C��:A��
�
�A ���� �8���� E���C�E� �F��C�F� BE��E� B�!����C���� �8EB� DE�� ���B�F��� E!�������C�E��
��!�C��� >� Q/�� '�E--F�� �E�D���� 7� !�C�� � E�� �8���� �����C� >� ��� !K!E� B��B���C���
9-C'��E��:A��$E��T�����F��CE���B����C��F��DE��DC--F�E�������E��BE�����C�E�����E�D��=��8EB�
��E���B�C�EB���E�E�B��E�-?���E�>��7��E!�C�E����C��F8����������'�E��C8E!E���8E���
�@��B�C�EB���E��D���E�9+C'��E�/�:A��
�
7A $�� ��E��C��� ��C8���E� F��C�� DE� ��8�C�� �C� BE�� '�E--���� ��!�C��� F��CE��� B�����E�� DE�
�F'��E�����'��BF!CE�DE������C��'�JBE�>�����FB�F�C���D@C����C�E���!�C�EA������BE�-�C�E=�
������8�����F��C�F�DE������E��D@E��F�CE�BE��A���E���E!C<�E���C�B���C���C��>�DF���C�E�
�E����B�F���E�D�'<�E�DE��������C�������@�������E����C�E������B�!���F����D����������
��E����CBC�F���FBC-C��E����� �E��BE����E��β�DE����'E���E�������E--E�������E��BE����E��β�
��!�C�E�A�(E�B�!���F�E�����C�C�F������C�D�C�E����DC��<�E�B�E0��E����'E��A�����BE��E�
�����B�E�������8����DF!����F���E=���E���E��B��������<���@C�BEB�C���D@�������E=��E��
����C��D�����E�'�E--����8�C�����DF8E����E!E������C�-�C��������C8�CE���>��F'��E���E���
'��BF!CE�9-C'��E�/�:A�$��DE��C<!E�E��F�CE�BE�D@F8�����C���DE��������C�F�D��'�E--������
B���C��F� E�� ��� �E��� D@���E�'��BF!CE� ���8���FE� ���� 8�CE� C����� �F�C���F��EA� $E��
����C���8EB����DF8E����E!E��� C���--C�����D��'�E--����8�CE���������-C��'��BF!C��E�

����E������
�����!����� >� ��8�C�� ��E� -���E� ��'!E����C��� DE� ��� '��BF!CE� 7H� !C���E�� ���<��
�@C�BEB�C��� ����� ��'!E����C��� DE� �@C����C�F!CE� ��!�C�EA� )�� �E8��B�E=� �E�� ����C��
��F�E������ ��� DF8E����E!E��� ���!��CE��� D�� '�E--��� F��CE��� D���� ��� F����
D@���E�C����C�C�!E� B�!!E� E�� ���E��E� �@���E�BE� DE� 8��C��C���� '��BF!C��E�� ���<��
B���'E� E�� '��B��EA� (EBC� F��C�� B���F�F� >� DE�� �FB�F�C���� D@C����C�E� ��!�C�E�
C!�������E��E�!C���E�����<�����B���'E�E��'��B��EA�9-C'��E���������CFE=���F�E��FE�E��
�E!�����E�-C'��E�/;:A��
�
;A $@������E� E�� !CB���B��CE� F�EB����C��E� DE�� BE����E�� E�D�B�C�E�� ���<�� G� !�C�� DE�
DF8E����E!E��� B��-C�!�C�� ��� ����C�F� DE� DF8E����E!E��� ��C���E� ��� ����B���E� DE��
'�����E���α�E��β�F��C��BE��E�DE�BE����E��!����E��9-C'��E�7:A�
�
������E�D��DF8E����E!E���E�D�B�C�E��
���� ����� ��!!E�� E���C�E� C��F�E��F�� >� �@E���E��C��� DE� 7� � -�B�E���� DE� �����B�C��C���
B�F��A��� �=�*7�E��2 �A�A� ��C��C�������8����F����C������BE��7� -�B�E�����������E���
D@E���E��C���D�����E����B�F���E��DF8E����E!E��A���
�
�A )��!E������� �������C-F���C���DE��BE����E���� �[�>�DC--F�E�������DE�����<�����'�E--E�
DE����B�F�����!�C��9�FM�2CFQ[X�D��[����<�����E!�C�E��DE�DF8E����E!E��=�G=7M�
���<���7��E!�C�E��E��7AFM����<��FH��E!�C�E�:=�������8����B��-C�!F� �E��D���FE��
E!������'C��E�� DE� �����C�C��� ��C!�C�E� 9����C-F���C��� D�� ����� �D��[:� E�� DE�
�����C�C��� �EB��D�C�E� 9DC!C���C��� ���'�E��C8E� DE� BE��E� ����C-F���C��� ����� �E���E��
D������E�����E�DE�DC--F�E�BC��C���BE�����C�E:�9+C'��E�;:A� � .��E���>����E���F��!�C���
��E� �E�� B�C--�E�� DE� ����C-F���C��� DE�� BE����E�� �� �� >� FH� �E!�C�E�� ����� ��<��
���F�CE����>�BE���DE��BE����E�����!K!E����DE�9HAFQM=�-C'��E�Q%:A�.���E!��E�D��B�
��E� �@E��E!��E�D��!�����'E��� �����E�8F��@E��� ���� �E���EC��� >� ��� BE����E�βA� (EBC�
B��-C�!E� C�DC�EB�E!E��� ������C�����E��� ��'��DE=� B�E0� �@#�!�C�=���E�E���E��C���
D���� �E� �C���� D�B���� ���B�F��C��EA� ���� �@�8���� ���� �����C-CF� ��� ����C-F���C���
D�B���E�!�C�� C�� E��� �������E� ��E� ��� ��!!E� DE�� B�C--�E�� DE� ����C-F���C��� DE� BE�� ��
B���C�'E���� E���C��E��� �E�� �C8E���� F�E8F�� E�B��E� ���E�8F�� E�� -C�� DE�
DF8E����E!E��A�
�

����E������
�A $@������E�D������E���D@E���E��C���DE�� -�B�E����DE� �����B�C��C���DE�DC--F�E�BC��C���
E�D�B�C�E� �E�!E�� DE� B��B���E� ��E�'�7� E��� E���C!F� ���!�C��� D<�� 4/�� 9Q[�:� E��
B����E��F�9�4[Q:�/��9+C'��E�E:A��E����!K!E�!��C<�E=�2 �A��E���E���C!F�D�����E��
��E!C<�E�� BE����E�� E�D�B�C�E�� E�� DF8E����E!E��=� �C��C� ��E� D���� DE� ��!��E��E��
BE����E��E�B��E�C�DC--F�E�BCFE��9-C'��E�F:�E��BE���B����E��F/�����!�C��A��
�
.�D�B�C���DE������'E�<�E�����C�BEB�C����E��C8C���E�D�����E�'�E--������B�F��C��E�
�����������!!E��-C���E!E���DE!��DF���SC��F��C������C��E�DE�BC��E����FBC-C��E!E����E��
BE����E�� β� E�� �E�� BE����E�� �BC��C�E�� D���� �E�!�D<�E� DE� '�E--E� DF8E����FA� � ���� �8����
C�BEB�F�DC�EB�E!E���D�����E�'�E--���DE����F�����C�����E��C8C���E������������������'<�E�
����BC���� �E�'<�E�DE� ���*+������� �E�B����P�E�D�����!��E��� C����C�E� 9BC���'E�β:����D��
���!��E��� E������E� 9BC���'E� �BC��C�E:A� �� ����C�� DE� Q� B����� ����� C�BEB�C��=� ����� �8����
���E�8F���E�E���E��C���DE�*+����FBC-C��E�DE�����E��BE�����C�E��BC��F��9+C'��E�G�E��/7:A��
�
�

����E7�����
The mouse muscle as an ectopic permissive site for human pancreatic
development
Carmen Capito1, Marie-Thérèse Simon
1, Virginie Aiello
1, Anne Clark
2, Yves
Aigrain3 Philippe Ravassard
4, Raphael Scharfmann
1
1 INSERM U845, Research Center Growth and Signalling, Université Paris
Descartes, Faculté de Médecine Cochin, Paris, France
2 Diabetes Research Laboratories, Oxford Centre for Diabetes, Endocrinology and
Metabolism, Churchill Hospital, Oxford UK
3 Necker Enfants Malades University hospital, Université Paris Descartes, Paris,
France
4 Université Pierre et Marie Curie-Paris 6, Biotechnology and Biotherapy Team,
Centre de Recherche de l’Institut du Cerveau et de la Moelle épinière (CRICM),
UMRS 975, CNRS, UMR 7225, INSERM, U975, Paris, France.
En cours de revue au journal : Diabetes
Abstract
Whilst sporadic human genetic studies
have permitted some comparisons between
rodent and human pancreatic development,
the lack of a robust experimental system
has not permitted detailed examination of
human pancreatic development. We
previously developed a xenograft model of
human fetal pancreas grafted under the
kidney capsule of immune-incompetent
mice, which allowed the development of
human pancreatic beta cells. Here, we
compared development of human fetal
pancreatic grafts at a less complicated and
efficient alternative site under skeletal
muscle epimysium with renal capsule
grafts and with murine muscle or renal
capsule grafts. We demonstrated that
human pancreatic beta cell development
occurs more slowly (weeks) than murine
pancreas (days) both by differentiation of
pancreatic progenitors and by proliferation
of developing beta cells. The superficial
location of the skeletal muscle graft and its
easier access permitted in vivo lentivirus-
mediated gene transfer with a GFP labeled
construct under control of the insulin or
elastase gene promoter which targeted beta
cells and non-endocrine cells respectively.
This model of engraftment under the
skeletal muscle epimysium is a new
approach for longitudinal studies, which
allows localized manipulation to determine
the regulation of human pancreatic
development.
Introduction
Understanding the mechanisms that
control human pancreatic islet
development remains a target for
deciphering the pathophysiological
mechanisms of disease and for developing
innovative therapeutic approaches. In
rodents, genomic gene disruption
experiments have enabled inference of the
transcriptional regulatory network and
paracrine soluble factors that control
pancreas specification and later endocrine
and exocrine fate determinations. In
humans, rare genetic deficiencies are
currently the way that regulatory factors
for pancreatic islet development are
determined.
In rodents, the pancreas-committed
endodermal region of the foregut first
expresses the transcription factor
pancreatic and duodenal homeobox 1
(PDX1); mice and humans deficient in
PDX1 lack a pancreatic gland (1,2). PDX1

��E;���
later becomes restricted to mature
pancreatic delta cells and beta cells where
it activates insulin gene expression (3).
These undifferentiated PDX1+ pancreatic
progenitors proliferate through the
mesenchymal effector FGF10 (4) and
differentiate into endocrine, ductal and
acinar cells. The endocrine specification
rests upon the transient expression of the
basic helix loop helix factor, neurogenin3
(NGN3), and NGN3-deficient mice lack
pancreatic endocrine cells (5). NGN3-
expressing cells are unipotent endocrine
precursors (6) and differentiate into the
four pancreatic endocrine cell types (alpha,
beta, delta and PP cells, producing
respectively glucagon, insulin,
somatostatin and pancreatic polypeptide).
Subsequently, combinations of additional
transcription factors will determine the
specific fate and stability of each
pancreatic endocrine cell type (7). As an
example, NKX2.2 is first expressed in
early mouse pancreatic PDX1+
progenitors. Afterwards it is maintained in
early endocrine progenitors along with
NGN3 (7,8) and later becomes restricted to
endocrine cells (except delta cells) as islets
develop (9). In rodent pancreas, NKX2.2
plays a major role in maintaining beta cell
identity (10).
Less is known on pancreatic
development in human. This is at least in
part due to the difficulty in accessing
properly staged human fetal pancreatic
tissues and to the frequently poor quality of
such tissues. This paucity of information is
also due to the absence of dynamic assays
to follow human beta cell development
from pancreatic progenitors, and to the
lack of assays to genetically modify
pancreatic cells at different stage of their
development. Many aspects seem
conserved between rodent and human
pancreatic development. For example,
different arguments derived from human
genetic studies strongly suggest that PDX1
and NGN3 play similar roles during rodent
and human pancreatic development
(2,11,12). But differences seem to exist on
the pancreatic role of other transcription
factors such as for example MAFB or
GATA family members (13,14). This is
not unexpected since, while rodent and
human adult pancreatic beta cells share a
large number of similarities, a number of
data also indicate marked differences
between species (15,16).
We previously developed and
validated a model of xenograft of human
fetal pancreas under the kidney capsule of
immune-incompetent SCID mice. We
demonstrated that this grafting model was
permissive for proper development of the
fetal tissue into a functional human
endocrine pancreas (17). However,
grafting under the kidney capsule is time-
consuming, limiting the number of SCID
mice to be grafted and the amount of data
to be produced. Moreover, due to its deep
anatomical localization, in close contact to
the kidney parenchyma following grafting,
the growing pancreas is difficult to
genetically modify to examine lineage
tracing or longitudinal transcription factor
expression.
In this context, we have developed an
alternative site by grafting human fetal
pancreas under the epimysium of the thigh
muscle. Using this model we have
examined in detail the major steps and
transcription factor expression that take
place during human pancreatic
development. Finally, we have
demonstrated the feasibility of cell-type,
specific virus-mediated gene transfer to
allow lineage tracing to observe islet and
non-endocrine cell development in human
fetal pancreas.
Research Design and Methods
Mouse and human pancreases Pregnant Swiss mice were purchased from
the Janvier breeding center (Janvier, Le
Genest, France). At 12.5 days of gestation
(E12.5), mice were killed by CO2
asphyxiation, according to the guidelines
of the French Animal Care Committee and

��EE���
the embryos were harvested. The dorsal
pancreas was isolated and preserved in
Hank’s balanced salt solution until use.
Human fetal pancreases were extracted
from tissue fragments (18) that were
obtained immediately after elective
termination of pregnancy between 7 and 9
weeks of gestation, in compliance with the
French bioethics legislation. Approval was
obtained from the Agence de Biomedecine,
the French competent authority along with
maternal written consent.
Animals and grafting into SCID mice Severe combined immunodeficiency
(SCID) mice (Charles River, L’arbresle,
France) were kept in isolators supplied
with sterile-filtered, temperature-controlled
air. Cages, bedding and drinking water
were autoclaved. Food was sterilized by X-
ray irradiation. The French animal ethics
committee approved these studies. For
grafting, 6- to 8-week-old SCID mice were
anesthetized with a ketamine/xylazine mix.
Fetal pancreases were implanted (1
pancreas per graft), using a dissecting
microscope, either under the kidney
capsule as previously described (17) or
under the muscle epimysium of either the
biceps femoris or the gluteus superficialis.
At different time points following grafting,
grafts were removed, fixed in formalin
3.7% and embedded in paraffin.
Immunolabelling and quantification
Graft sections (4-5 µm-thick) were
prepared and processed as previously
described (19). The following primary
antibodies were used for immunostaining:
mouse anti-BrdU (Amersham,
Courtaboeuf, France); rabbit anti-
carboxypeptidase A (Biogenesis Ltd,
Poole, UK, 1/600); rabbit anti-GFP
(Abcam, Paris, France, 1/1,000); mouse
anti-glucagon (Sigma, St Louis, MO, USA,
1/2,000); mouse anti-insulin (Sigma,
1/1000); mouse anti-Ki67 (BD, Franklin
Lakes, NJ, USA 1/20); sheep anti- human
NGN3 (R&D systems, Lille, France,
1/400); mouse anti- mouse NGN3 (BCBC,
1/1,000); mouse anti-NKX2.2
(Developmental Studies Hybridoma Bank,
1/50); rabbit anti-pan-cytokeratin (Dako,
Trappes, France 1/500); rabbit anti-PDX1
(1/1,000) (20); mouse anti-somatostatin
(BCBC, 1/500). The secondary antibodies
were: dyelight or FITC conjugated anti-
rabbit antibodies (Beckman Coulter,
Villepinte, France, 1/200); texas red or
FITC anti-mouse antibodies (Beckman
Coulter, 1/200); alexa fluor anti-rabbit
antibodies (Biogenex, Fremont, CA, USA,
1/400). For NGN3, revelation was
performed using the Vectastain ABC kit
(Vector, Malakoff, France).
Cell proliferation For cell proliferation analyses, mice were
injected with bromodeoxyuridine (BrdU,
50 mg/kg) 4 h before being killed. To
measure the proliferation of PDX1+
pancreatic progenitors, we counted the
frequency of BrdU+ nuclei among PDX1+
cells. To measure the proliferation of beta
cells, we counted the frequency of BrdU+
nuclei among insulin+ cells. At least 1,000
cells per graft were counted in each
condition. The same tissues were also
stained with Ki67 antibody and
quantification performed as described
above, as a second readout for cell
proliferation.
Electron microscopy For standard electron microscopy, human
pancreatic grafts were removed, cut into
1mm cubes and fixed overnight in 2.5%
glutaraldehyde in 0.1M phosphate buffer
pH 7.2. For gold immunolabelling the
fixative solution was 2.5%
paraformaldehyde plus 0.5%
glutaraldehyde in 0.1M phosphate buffer
pH 7.2. All fixed specimens were stored at
4°C until processed into resin; Spurr’s
resin (Elektron Technology UK, Stansted
UK), was used for structural observations
and London Resin Gold (LRG) (Elektron
Technology UK) was used for
immunolabelling. Ultrathin (70nm) section
were cut onto nickel grids, contrasted with

��EF���
uranyl acetate and lead citrate and viewed
with a Joel 1010 electron microscope.
LRG sections were immunogold labeled
for insulin using guinea-pig anti-insulin
(Sigma, UK) and protein A gold (British
Biocell International, Cardiff UK)
Induction of diabetes with alloxan To determine the capacity of the human
graft to regulate the glycaemia of the
mouse, grafted (3 months grafts) and non-
grafted (control mice) SCID mice were
injected intravenously with alloxan
(Sigma-Aldrich, 90 mg/kg body weight),
which is known to destroy rodent, but not
human, beta cells (21).Glucose
concentrations were measured on blood
collected from the tail vein, once a week
during 4 weeks, using a portable glucose
meter (OneTouch Vita, Lifescan France,
Issy les Moulineaux, France). To confirm
the contribution of the graft to the
normalization of blood glucose values in
the host, grafts were removed 30 days after
the injection of alloxan and blood glucose
concentrations were measured during one
more week. Circulating insulin
concentrations were measured at day 0
after alloxan injection by Elisa method
(Mercodia insulin Elisa, Human, Mercodia
AB, Uppsala, Sweden).
Lentivirus-mediated gene transfer The lentiviral construct pTRIP
deltaU3.RIP405-GFP has been previously
described (22). The lentiviral construct
pTRIP deltaU3.ElastaseP-GFP was derived
from the pTRIP deltaU3.RIP405-GFP.
Briefly, the insulin promoter was removed
by MluI and BamHI digestion and replaced
by a 500 bp fragment of the Elastase
promoter flanked with the same MluI and
BamHI restriction sites. The Elastase PCR
fragment was amplified using phusion high
fidelity polymerase (Finnzyme) from
Elastase GFP pcDNA3 plasmid kindly
provided by David Tosh (University of
Bath, UK) using forward primer 5’
ACGCGTCAGATCAGCTTATCGTATG
AA 3’ and reverse primer 5’
GGATCCCGAGACCACTGCCCCTTGC
3’. Lentiviral vectors were prepared and
titrated as described (22). Grafted (3-
month grafts) SCID mice were
anesthetized. Hundred micro liters of the
lentiviral vector solutions (105 transduction
units) were injected using 32 gauge
needles into multiple sites of the
developing human pancreas. Pancreases
were harvested at 7, 14 and 30 days
following injections and used for
immunofluorescence analyses.
Results
Development of mouse and human fetal
pancreas upon grafting under the
muscle epimysium or under the kidney
capsule The renal capsule has been widely used as
a grafting site for mature rodent and human
islets and for fetal pancreas (17,23,24). We
first compared the development of mouse
fetal pancreas grafted either under the
kidney capsule (renal graft) or at the level
of the muscle epimysium (muscular graft).
We found that undifferentiated E12.5
pancreases developed efficiently and in a
similar fashion at both sites. Two weeks
following grafting, insulin- and glucagon-
expressing cells were present, forming
islet-like structures with insulin-positive
clusters surrounded by glucagon-
expressing cells (Fig. 1A, D). Insulin-
positive cells expressed PDX1 (Fig. 1B,
E). Duct-like structures also developed
similarly at both sites (Fig. 1A-F).
Interestingly, acinar cells, visualized either
following carboxypeptidase-A staining
(Fig. 1C, F) or following amylase staining
(data not shown), developed at none of the
grafting sites.
We next compared human fetal pancreas
development following grafting under the
muscle epimysium or the kidney capsule.
Three months following grafting, insulin-,
glucagon- and somatostatin-expressing
cells were observed on both sites (Fig. 2A,
B, D, E). Beta cells stained positive for

��EQ���
PDX1 (Fig. 2C, F) and were never found
positive for glucagon (Fig. 2A, D),
supporting the differentiated status of such
newly formed beta cells (25,26). Ductular
structures that stained positive for pan-
cytokeratin were observed on both sites
(Fig. 2G, J). Acinar cells that stained
positive for carboxypeptidase-A developed
from human fetal pancreas grafted on
either site (Fig. 2G, H, J, K). This contrasts
with the findings with grafted mouse
pancreas (Fig. 1C, F).
We then characterized in more detail beta
cells that developed from human fetal
pancreases grafted under the muscle
epimysium. For functional analysis, three
months following grafting, we destroyed
endogenous mouse beta cells with alloxan
(21), which gave rise to increased
glycaemia in non-grafted mice (Fig. S1).
Among five grafted mice, one did not
regulate its glycaemia, had low circulating
human insulin levels and poor beta cell
differentiation (Fig. S1). In four mice,
glycaemia was efficiently regulated with
circulating human insulin levels reaching
0.6ng/ml and efficient beta cell
differentiation (Fig. S1). Of note, all four
mice became hyperglycemic upon after
removal of the grafts.
For morphological analysis, electron
microscopy of the human fetal graft was
performed 8 months after grafting. It
indicated the presence of well-granulated
alpha and beta cells and a developed
capillary network (Fig. 3A). Immunogold-
electron microscopy indicated the presence
of insulin within structurally mature beta-
cell granules (Fig. 3B,C).
These data demonstrated that pancreatic
development of mouse or human pancreas
was similar upon grafting under the muscle
or the kidney capsule. Since grafting at the
muscle site was technically easier, faster
and could potentially allow perturbation
experiments, we thus performed muscular
grafting in the remaining part of this study.
PDX1+ pancreatic progenitors following
grafting
We analyzed the presence of PDX1+
pancreatic progenitors following grafting.
In engrafted mouse fetal pancreas, all
PDX1+ cells stained positive for insulin
two weeks following grafting (Fig. 1E).
This indicated that within two weeks, the
pool of PDX1+/endocrine- negative,
pancreatic progenitors had been depleted.
In contrast, many PDX1+/INS- negative
cells were observed 3 months following
grafting of human fetal pancreas (Fig. 2F).
We next measured the proliferation of
PDX1+ pancreatic progenitors at different
time points following grafting of human
fetal pancreas. Two weeks after grafting,
16% of PDX1+ cells stained positive for
Ki67 and 12% of PDX+ cells stained
positive for BrdU following a 4h pulse
(Fig. 4). These proportions decreased by
nearly two fold 13 weeks following
grafting, and further decreased 60 weeks
following grafting (Fig. 4).
Endocrine progenitors following
grafting We analyzed the expression of NGN3, a
transient marker of endocrine progenitors
(5) following grafting. Two weeks
following grafting of mouse fetal pancreas,
NGN3+ endocrine progenitors were not
observed (Fig. 5A). In grafted human
pancreas, NGN3 was detected at weeks 2,
8, 13 and 19 post-grafting, its expression
being undetectable at weeks 37 and 60
following grafting (Fig. 5B). Thus, NGN3
is expressed during at least 19 weeks in the
grafted human fetal pancreas.
During mouse pancreatic development,
NKX2.2 is expressed in early pancreatic
progenitors and later becomes restricted to
endocrine cells (except delta cells) as islets
develop (9). In grafted human fetal
pancreas, two weeks following grafting,
NKX2.2 was expressed in the first
developing endocrine cells, and also in
many endocrine-negative cells (Fig. 6).
Many NKX2.2+/endocrine- cells remained
present till at least week 19 following
grafting. At later post-grafting time points,
the number of differentiated endocrine

��EG���
cells increased and such cells stained
positive for NKX2.2. In parallel, the
number of NKX2.2+/endocrine-cells
decreased (Fig. 6).
Taken together, such results indicated that
in mouse, the pool of pancreatic and
endocrine progenitors was depleted within
a two week period whereas in human
pancreas, pancreatic and endocrine
progenitors remained present for at least
four months following grafting, creating a
pool of cells giving rise to endocrine cells.
Beta cell proliferation in grafted
pancreases Two weeks following grafting, 8.9% beta
cells that developed from mouse fetal
pancreas incorporated BrdU after a 4h
BrdU pulse and 16.15% beta cells stained
positive for Ki67 (Fig. 7A). In grafted
human fetal pancreas, beta cell
development increased during a 60-week
time period with the development of larger
islet-like structures (Fig. S2). Thirteen
weeks following grafting, 2% beta cells
incorporated BrdU following a 4h pulse
and 3.5% beta cells stained positive for
Ki67 (Fig. 7B). These proportions
measured in grafted human fetal
pancreases were lower than the ones
measured in grafted mouse pancreas and
further decreased by more than 5 fold 60
weeks following grafting (Fig. 7B).
Virus-mediated gene transfer into the
developing human pancreatic cells We finally asked whether it was feasible to
specifically target human pancreatic cell
types in the above-described model of
human fetal pancreas that has developed
under the muscle epimysium. Three
months following grafting of human fetal
pancreases under the muscle epimysium,
we injected within the developing tissue
lentiviral vectors that expressed GFP under
the control of either the insulin promoter or
the elastase promoter. Grafts were
removed and analyzed 7-30 days later.
When GFP was under the control of the
insulin promoter, we labeled insulin+ cells
with this approach (Fig. 8), while
endocrine-negative cells that could
represent nascent acinar cells were labeled
when GFP was under the control of the
elastase promoter (Fig. S3).
Discussion
During the past years, major progress has
been made on understanding factor
controlling mouse pancreatic islet-cell
development. This is at least in part due to
the development of a large number of
innovative approaches, for example
transgenic mice for gain- and loss-of-
function experiments or in vitro assays to
screen for signals that modulate pancreatic
development (27). On the other hand,
information on human pancreatic islet
development remained scarce. A first
major limitation to efficient progress on
human pancreas development is the
inability to longitudinally track or impact
on human pancreas development with
models developed so far. A second
limitation is the difficult access to human
fetal pancreases corresponding to specific
stages of development in large-enough
quantity and quality.
In this work, we developed and validated a
new grafting model for study of human
pancreatic islet development. Moreover,
this model permitted to perform virus-
mediated gene transfer in specific human
pancreatic cell types.
We previously developed a model of
xenograft of human fetal pancreas under
the kidney capsule of SCID mice. This
model was permissive for pancreatic
development and gave rise to functional
human beta cells (17). However, grafting
under the kidney capsule is technically
challenging when performing a large
number of grafts, and time-consuming.
Moreover, our attempts to perform virus-
mediated gene transfer into the developing
human pancreas grafted under the kidney
capsule failed due to difficulties to access

��E4���
the graft and hemodynamic drastic
variations when trying to mobilize the
kidney (data not shown). In this context,
we modified our initial model and used the
muscular site as an alternative. The
muscular site has been used in the past to
graft mature islets. For example the
forearm muscle was used with success in
humans for islet auto-transplantation after
total pancreatectomy for severe hereditary
pancreatitis (28). In addition, a murine
model of islets grafted within the cremaster
muscle was developed and showed an
efficient intra-islet blood supply after two
weeks of engraftment (29). Moreover, islet
injections into biceps femoralis in the rat or
into gracilis muscle in minipig induced a
sustained reversal of diabetes (30,31).
Finally, human islets grafted into the
muscle of the forearm could be imaged,
demonstrating their survival 1 year after
following implantation (32). On the other
hand and to the best of our knowledge, the
muscle has not been used as a grafting site
for undifferentiated fetal pancreas and it
was unknown whether this site was
permissive for proper pancreatic cell
differentiation. Here, we have
demonstrated that rodent and human fetal
pancreas properly develop upon grafting
under the muscle epimysium. This site
could thus represent a new site for grafting
of human pancreatic progenitors. Indeed,
protocols are now available to generate
PDX1+ pancreatic progenitors from hESCs
(33). These progenitors need to be grafted
into mice to differentiate into functional
pancreatic endocrine cells (34). There is
however a recurrent discussion on the best
site for grafting of either mature islets or
pancreatic progenitors that would develop
into functional beta cells (35). In this
context, the muscular epimysium
represents an intersting site as: i)
functional beta cells develop from human
fetal pancreatic progenitors; ii) the
developing graft can be easily removed if
necessary for oncological reasons; iii) it
should be possible to image the developing
beta cells, using approaches similar to the
ones used for imaging beta cells grafted in
muscle forearm (32).
In this model of muscular grafting, within
two weeks following transplantation of a
E12.5 mouse pancreas, differentiated cells
developed, while the pool of PDX1+
pancreatic progenitors was depleted, and
all PDX1+ cells expressed insulin. This
result perfectly fits with rodent data
obtained either in vivo or in vitro (19,36).
In contrast, three months following
grafting of human fetal pancreas, many
PDX1+/Insulin- cells were still observed.
They were efficiently proliferating, based
on both Ki67 staining and BrdU
incorporation. These proliferation indices
decreased at later time points post-grafting.
Taken together, such results suggest that
pancreatic cell differentiation remains
active during a long period in humans. It is
however important to keep into account
that in humans, the presence of
PDX1+/Insulin-negative cells represents an
indirect sign of active differentiation as
PDX1 remains expressed within pancreatic
duct cells during adult life (37). But more
direct arguments indicate that endocrine
cell differentiation takes place during a
long period following grafting of human
fetal pancreas. Two weeks following
grafting of mouse E12.5 pancreas,
endocrine progenitors that expressed the
transient NGN3 marker could not be
observed as is the case in vivo and in in
vitro rodent models (5,19,36). On the other
hand, NGN3-positive cells could be
observed within the grafted human fetal
pancreas up to at least 19 weeks following
engraftment. NGN3 expression was
undetectable 37 and 60 weeks following
grafting. This suggests that the process of
endocrine differentiation occurs over
periods of weeks and is probably finished
at the end of pregnancy in humans. Similar
results were obtained by looking at the
expression of NKX2.2. In rodents,
NKX2.2 is expressed in early pancreatic
progenitors. Its expression is later
maintained in mature endocrine cells (9).

��FH���
In the grafted human fetal pancreas, cells
positive for NKX2.2 but negative for
endocrine markers could be detected for at
least 19 weeks following grafting.
Based on this longitudinal study of PDX1,
NGN3 and NKX2.2 expression patterns in
the grafted human fetal pancreas, we
propose that endocrine cell differentiation
takes place during a long time window
during development. This long time-frame
in humans should be useful to attempt to
capture and amplify in vitro human
pancreatic progenitors as performed in the
case of neural progenitors (38). Moreover,
as previously suggested (14) such long
lasting developmental windows of human
pancreatic development could explain why
haploinsuffficiency of a number of
transcription factors such as GATA6,
HNF1A, HNF1B, and HNF4 cause
diabetes in humans and not in rodents.
Beta cell proliferation in this grafting
model reproduced beta cell proliferation
observed in vivo both for rodent and
human pancreas. This is the case for mouse
E12.5 pancreases engrafted during two
weeks, where 8.9% of beta cells
incorporated BrdU as reported for newborn
mouse pancreas (4). This is also the case
for human fetal pancreases where 2% beta
cells incorporated BrdU 3 months
following grafting with 3.5% beta cells
positive for Ki67. Such levels decreased
one year following grafting with 0.2% beta
cells that incorporated BrdU and 0.7% that
stained positive for Ki67. These data
obtained with Ki67 antibodies are in
accordance to those reported in fetal and
neonatal pancreases at the same
developmental stages (39,40). Of note, the
above-described dynamic model of human
pancreatic development permitted to
further support data obtained with Ki67
antibodies with data obtained following
BrdU injections. To our knowledge, such a
type of experiments on human PDX1+
progenitors or human fetal beta cells
entering the S-phase using BrdU
incorporation had not been described in the
past due to the lack of proper experimental
system. Such a dynamic model of beta cell
proliferation should thus be useful to better
dissect the mechanisms that regulate
human beta cell proliferation during the
perinatal period (41).
Overall, our results demonstrated the
efficiency of the muscular fetal pancreatic
graft model to recapitulate pancreatic
development. The difference observed
between mouse and human pancreatic islet
development after grafting further
emphasizes the specificity of each species
regarding cell differentiation, maturation
and proliferation. The fact that we
successfully performed cell type specific in
vivo lentiviral-mediated gene transfer in
human pancreas grafted under the muscle
epimysium represents a first step to the use
of this model in a dynamic manner for
gain- and loss-of-function experiments.
Author contribution R.S. is guarantor and takes full
responsibility for the manuscript and its
originality. C.C. conceived experiments,
researched data, contributed to the
discussion, and wrote the manuscript. M.-
T.S, V.A. and researched data. A.C
performed the electron microscopy. P.R.
contributed tools. R.S. conceived
experiments, contributed to the discussion
and also wrote the manuscript.
Acknowledgments C.C. was supported by the Fondation pour
la Recherche Médicale and by the
Association des Jeunes Diabétiques. This
work was supported by grants to RS from
the Beta Cell Biology Consortium (grant
1U01DK089571-01), from the 7th
Framework Program of the European
Union under grant agreements n° 241883,
from the Innovative Medicine Initiative
under grant agreement n° 115005, from the
bilateral program Bundesministerium fur
Bildung und Forschung (BMBF) ANR,
convention number 2009 GENO10502 and

��F����
from the Laboratoire d’Excellence
consortium Revive

��F����
��
-AB����.������$����D���+�%./�7��������CD*��C����+�$$�CADB�B�C+�ADB�
&���E�)��AE����B�E��E��,E�E�'��-�ED�EC��E����DE�� ��E�1CD�E�� B�����E� 9��(:������DE��
��E�!��B�E�E�C!��C�!�9��+:A�",��,EE1�����E�=���E�'��-���,E�E��E!�8ED=��EB�C��ED���D�
���C�ED�,C������C�C����C�=��'��B�'��=���� ����D��(������C��DCE�A�`�C�DCB��E��D�B��A�/B��E�
����A��HHY!�
�

��F7���
�
-AB����/������$����D���+����CD�+��C$��CD*��C����+�$$�CADB�B�C+�ADB�
#�!���-E�������B�E��E��,E�E�'��-�ED�EC��E����DE����E�1CD�E��B�����E�9��(=�*�.:������DE��
��E�!��B�E�E�C!��C�!�9��+=�C�$:A�"��EE�!���������E�=���E�'��-���,E�E��E!�8ED=��EB�C��ED�
��D� ���C�ED� ,C��� ���C�C����C�=� �'��B�'��=� ���!�������C�=� ��� �=� �(��� ��D� ����(2�
���C��DCE�A�/B��E�����A��HHY!�
�

��F;���
�
-AB���� 0�� %$�*���D� �A*���*���� CD�� B�$�� A���D�$C"�$$ADB� +��� AD��$AD� AD� ���CD�
�CD*��C��<���D���������B�C+�ADB�AD��1�$��C$����*$��
�A�"�E�'��-��,���,E���8��B����C�ED�,C���B��C����CE��9B��:��DB�BE�������E���BE���A�%E���BE����
,E�E�,E���'�������ED���D�B����C�ED�!C��B���D�C��9!:=�!����E��EB�E�����'�����E��,C���
B����B�E�C��CB�B�������C�E�B��E���-���!����D�������B�E���9C:���D���!E�C!!����E�'�����E��
9����,�:A�!��*��D�C!!������E��C�'�-���C����C��,�����E�E����8E����E��EB�E�����'�����E��C��
�E���BE�����������E���-��!��DB�BE���������BE���A�/B��E������EHH�!A���
�

��FE���
�
-AB����4�����$A+��C�A�D��+���E.I�*�$$��+�$$�CADB�B�C+�ADB��+����CD�+��C$��CD*��C����
�D�����������*$����A���A����
#�!��� -E���� ���B�E��E��,E�E� '��-�ED� ��DE�� ��E�!��B�E� E�C!��C�!A� ��� DC--E�E��� �C!E�
��C����9�=��7���D�FH�,EE1�:=�!CBE�,E�E�C�BEB�ED�,C���%�D3���D���B�C-CBED�;����������E�A�
"�E� '��-��� ,E�E� �E!�8ED=� �EB�C��ED� ��D� ���C�ED� ,C��� ���C��� �=� �2.FQ� ��D� �%�D3�
���C��DCE�A�;����CD�$���E��E�E����C8E����C�C�'�������EE��C!E���C���A�/B��E�����A��HHY!A��
=�C��� �CD�$��a����C-CB��C��� �-� ��E� �������C���� �-� �� �����C�C8E� BE���� �����,E�E� �����
���E��ED�-���EC��E��2CFQ����%�D3A��b�;�'��-����E��'�����E�BE���-���FH�,EE1��,�E�E��b�A�
�

��FF���
�
-AB����7��9D90��&�����A�D�AD�������CD�����CD����*�$C��B�C+���
��&���E�)��AE����B�E��E��,E�E�'��-�ED���DE����E�!��B�E�E�C!��C�!A�",��,EE1�����E�=�
��E�'��-���,E�E��E!�8ED=��EB�C��ED���D����C�ED�,C������C�*7����C��DCE�A�3��'��-�ED�
)�EAE�!���E����B�E���,�����ED���������C�C8E�B������A�/B��E�����A��HHY!�
!��#�!���-E�������B�E��E��,E�E�'��-�ED���DE����E�!��B�E�E�C!��C�!A����DC--E�E����C!E�
��C����9�=�G=��7=��4=�7Q���D�FH�,EE1�:=���E�'��-���,E�E��E!�8ED=��EB�C��ED���D����C�ED�
,C������C�*7����C��DCE�A�%���A��HHY!���D��EY!�C����E�C��E���
�
�
�
�

��FQ���
�
-AB����5���92E/�/��&�����A�D�AD����CD����*�$C��B�C+���
#�!��� -E���� ���B�E��E��,E�E� '��-�ED� ��DE�� ��E�!��B�E� E�C!��C�!A� ��� DC--E�E��� �C!E�
��C����9�=�G=��7=��4=�7Q���D�FH�,EE1�:=���E�'��-���,E�E��E!�8ED=��EB�C��ED���D����C�ED�
,C��� �� B�B1��C�� �-� ���C�C����C�=� '��B�'��=� ��!�������C�� ��D� ���B�E��CB� �����E��CDE�
���C��DCE�� �E8E��ED� C�� '�EE�� ��D� ���C�2 �A�� ���C��DCE�� �E8E��ED� C�� �EDA� /B��E����A�
�HHY!A�
�
�
�
�
�
�
�
�
�
�
�
�
�

��FG���
�
�
-AB���� :�� ���$A+��C�A�D� �+� AD��$ADI� *�$$�� +�$$�CADB� B�C+�ADB� �+� +��C$� �CD*��C����
�D�����������*$����A���A����
&���E� )��AE� @A� ��D� ��!��� -E���� ���B�E��E�� @!A� ,E�E� '��-�ED� ��DE�� ��E� !��B�E�
E�C!��C�!A� ��� DC--E�E��� �C!E� ��C���=� !CBE� ,E�E� C�BEB�ED� ,C��� %�D3� ��D� ��B�C-CBED� ;�
���������E�A�"�E�'��-���,E�E��E!�8ED=��EB�C��ED���D����C�ED�,C������C�C����C�=��2.FQ���D�
�%�D3� ���C��DCE�A� �E��E�E����C8E� �EB�C���� ��E� ��E�E��EDA� ����,�� ��C��� ��� D����E�
���C�ED�BE���A�/B��E�����A��HHY!A�a����C-CB��C����-���E��������C����-�C����C�����C�C8E�BE����
����� ���C�ED� ���C�C8E� -��� EC��E�� 2CFQ� ��� %�D3� ��E� ����� ���,�A� a����C-CB��C��� ,���
�E�-��!ED����7�'��-���-���!���E����B�E��=�;�'��-���-�����!������B�E������,EE1��7���D�
��'��-���-�����!������B�E������,EE1�FHA�
�

��F4���
�
-AB����<��=�D�A�A�������AC����B�D����CD�+���AD�����������$��ADB����CD��CD*��C�A*�
*�$$��+���"��C�*�$$����*A+A*�B�D���&�����A�D�
#�!���-E�������B�E��E��,E�E�'��-�ED���DE����E�!��B�E�E�C!��C�!A�"��EE�!���������E�=�
�E��C8���8EB�����E���E��C�'�*+����DE����E�B��������-���E�C����C�����!��E��,E�E�C�BEB�ED�
C���� ��E�DE8E���C�'�'��-��A�*��-���,E�E����8E��ED�Q=��;���D�7H�D��������� C�BEB�C�����D�
���C�ED�,C������C�C����C����D����C�*+�����C��DCE�A�/B��E�����A��HHY!�
�

��QH���
�

��Q����
-AB����).��-�D*�A�DC$�����$����D���+����CD��CD*��C�A*��CD*��C����B�C+�����D����
�������*$����A���A����
/(.��!CBE�,E�E�EC��E������'��-�ED����'��-�ED���DE����E�!��B�E�E�C!��C�!�,C�����!���
-E���� ���B�E��E�A� "��EE�!������ ���E�=�!CBE�,E�E� C�BEB�ED�,C��� �������� 9��E�� ����,�:A�
*��B�E!C��,���!E����ED���BE���,EE1A����D���H=�����!����!���C����C��,���!E����ED�C��
����'��-�ED���D�'��-�ED�!CBEA� �*��-���E!�8��=����D���7��9-C��ED�����,�:�C�D�BED������CD�
C�B�E��E� C�� ��E� '��B�E!C�� �-� '��-�ED� !CBEA� "�E� �E!�8ED� '��-��� ,E�E� �EB�C��ED� ��D�
���C�ED���C�'����C�C����C����D����C�'��B�'������C��DCE�A�/B��E������b��HHY!A�
�

��Q����
�
-AB���� )/�� ���CD� �CD*��C�A*� ����$����D�� +�$$�CADB� B�C+�ADB� �D���� ���� ���*$��
��A���A�����
#�!��� -E���� ���B�E��E��,E�E� '��-�ED� ��DE�� ��E�!��B�E� E�C!��C�!A� ��� DC--E�E��� �C!E�
��C����9�=��7=���D�FH�,EE1�:=���E�'��-���,E�E��E!�8ED=��EB�C��ED���D����C�ED�,C������C�
C����C�=��'��B�'��=��(�����D��� �����C��DCE�A�/B��E�����A��HHY!�
�

��Q7���
�
-AB���� )0�� =�D�A�A�������AC���� B�D�� ��CD�+��� AD��� ���� ����$��ADB� ���CD�
�CD*��C�A*�*�$$��CA���D-���D��������*�D���$��+������$C��C������������
#�!���-E�������B�E��E��,E�E�'��-�ED���DE����E�!��B�E�E�C!��C�!A�"��EE�!���������E�=�
�E��C8���8EB�����E���E��C�'�*+����DE����E�B��������-���E�E������E����!��E��,E�E�C�BEB�ED�
C������E�DE8E���C�'�'��-��A�*��-���,E�E����8E��ED�Q�D���������C�BEB�C�����D����C�ED�,C���
���C�C����C�=��*+�=����(2���D�(������C��DCE�A�/B��E�����A�EHY!�
�
�
�
�

��Q;���
-AB����)4��
�

��QE���
-AB���� )4�� +����,C�'� �� �F������ -���=� ���E�C�E� ����D� '��B��E� �E8E��� ,E�E�!E����ED� C��
��!��E�� ��1E�� -��!� ��E� ��C�� 8EC�A�*��B��E� C�� ��E�C�E��%/�,��� C�BEB�ED� C�����E�C���E�����
��C�'� �� �������E� '��B��E�!E��E� 95�E���B�� 8C��=� $C-E�B��� +���BE:A� +���!E����E!E��� �-�
.����C��,���!E����ED����)�C���!E���D�9��!���C����C��E�C��=�&E�B�DC���%:A�+����'��-�ED�
!CBE� ,E�E� �����0ED� 9�A�O� �A�O� �A�O� �A7:A� In order to further test the ability of the graft to
respond to acute hyperglycemia, we performed a glucose tolerance test following a 16-hour
fast. Four mice grafted with human fetal pancreas developed during 8 months were submitted
to a high dose of glucose by intraperitoneal injection 9�� !'X'� ��D�� ,EC'��: ��D� ����D�
'��B��E�!E����ED�7H=�FH=���D���H�!C���E���-�E�� ��E� C�BEB�C��A�#�!��� insulin� �EB�E�C���
,��� ����� !E����ED� -��!� ����D� ��!��E�� B���EB�ED� ��� E� ��D� �E� !C���E�� �-�E�� '��B��E�
C�BEB�C��A� One mouse (1.2) was hyperglycemic (up to 300ng/dl) 30 minutes after injection and
this correlated with undetectable human insulin secretion and poor beta cell differentiation. In
three mice, glycemia was regulated thanks to an efficient human insulin secretion (from 4 to
10ng/ml) five minutes after glucose injection�

��QF���
.References
1. Jonsson,J, Carlsson,L, Edlund,T, Edlund,H: Insulin-promoter-factor 1 is required for
pancreas development in mice. Nature 371:606-609, 1994
2. Stoffers,DA, Zinkin,NT, Stanojevic,V, Clarke,WL, Habener,JF: Pancreatic agenesis
attributable to a single nucleotide deletion in the human IPF1 gene coding sequence.
Nat.Genet. 15:106-110, 1997
3. Ohlsson,H, Karlsson,K, Edlund,T: IPF1, a homeodomain-containing transactivator of
the insulin gene. EMBO J. 12:4251-4259, 1993
4. Bhushan,A, Itoh,N, Kato,S, Thiery,JP, Czernichow,P, Bellusci,S, Scharfmann,R:
Fgf10 is essential for maintaining the proliferative capacity of epithelial progenitor
cells during early pancreatic organogenesis. Development 128:5109-5117, 2001
5. Gradwohl,G, Dierich,A, LeMeur,M, Guillemot,F: neurogenin3 is required for the
development of the four endocrine cell lineages of the pancreas.
Proc.Natl.Acad.Sci.U.S.A 97:1607-1611, 2000
6. Desgraz,R, Herrera,PL: Pancreatic neurogenin 3-expressing cells are unipotent islet
precursors. Development 136:3567-3574, 2009
7. Oliver-Krasinski,JM, Stoffers,DA: On the origin of the beta cell. Genes Dev. 22:1998-
2021, 2008
8. Schwitzgebel,VM, Scheel,DW, Conners,JR, Kalamaras,J, Lee,JE, Anderson,DJ,
Sussel,L, Johnson,JD, German,MS: Expression of neurogenin3 reveals an islet cell
precursor population in the pancreas. Development 127:3533-3542, 2000
9. Sussel,L, Kalamaras,J, Hartigan-O'Connor,DJ, Meneses,JJ, Pedersen,RA,
Rubenstein,JL, German,MS: Mice lacking the homeodomain transcription factor
Nkx2.2 have diabetes due to arrested differentiation of pancreatic beta cells.
Development 125:2213-2221, 1998
10. Papizan,JB, Singer,RA, Tschen,SI, Dhawan,S, Friel,JM, Hipkens,SB, Magnuson,MA,
Bhushan,A, Sussel,L: Nkx2.2 repressor complex regulates islet beta-cell specification
and prevents beta-to-alpha-cell reprogramming. Genes Dev. 25:2291-2305, 2011
11. Pinney,SE, Oliver-Krasinski,J, Ernst,L, Hughes,N, Patel,P, Stoffers,DA, Russo,P, De
Leon,DD: Neonatal diabetes and congenital malabsorptive diarrhea attributable to a
novel mutation in the human neurogenin-3 gene coding sequence.
J.Clin.Endocrinol.Metab 96:1960-1965, 2011
12. Rubio-Cabezas,O, Jensen,JN, Hodgson,MI, Codner,E, Ellard,S, Serup,P,
Hattersley,AT: Permanent Neonatal Diabetes and Enteric Anendocrinosis Associated
With Biallelic Mutations in NEUROG3. Diabetes 60:1349-1353, 2011
13. Dorrell,C, Schug,J, Lin,CF, Canaday,PS, Fox,AJ, Smirnova,O, Bonnah,R,
Streeter,PR, Stoeckert,CJ, Jr., Kaestner,KH, Grompe,M: Transcriptomes of the major
human pancreatic cell types. Diabetologia 54:2832-2844, 2011
14. Rodriguez-Segui,S, Akerman,I, Ferrer,J: GATA believe it: new essential regulators of
pancreas development. J.Clin.Invest 122:3469-3471, 2012
15. Rorsman,P, Braun,M: Regulation of insulin secretion in human pancreatic islets.
Annu.Rev.Physiol 75:155-179, 2013
16. Scharfmann,R, Rachdi,L, Ravassard,P: Concise review: in search of unlimited sources
of functional human pancreatic beta cells. Stem Cells Transl.Med. 2:61-67, 2013
17. Castaing,M, Peault,B, Basmaciogullari,A, Casal,I, Czernichow,P, Scharfmann,R:
Blood glucose normalization upon transplantation of human embryonic pancreas into
beta-cell-deficient SCID mice. Diabetologia 44:2066-2076, 2001

��QQ���
18. Polak,M, Bouchareb-Banaei,L, Scharfmann,R, Czernichow,P: Early pattern of
differentiation in the human pancreas. Diabetes 49:225-232, 2000
19. Attali,M, Stetsyuk,V, Basmaciogullari,A, Aiello,V, Zanta-Boussif,MA, Duvillie,B,
Scharfmann,R: Control of beta-cell differentiation by the pancreatic mesenchyme.
Diabetes 56:1248-1258, 2007
20. Duvillie,B, Attali,M, Bounacer,A, Ravassard,P, Basmaciogullari,A, Scharfmann,R:
The mesenchyme controls the timing of pancreatic beta-cell differentiation. Diabetes
55:582-589, 2006
21. Eizirik,DL, Pipeleers,DG, Ling,Z, Welsh,N, Hellerstrom,C, Andersson,A: Major
species differences between humans and rodents in the susceptibility to pancreatic
beta-cell injury. Proc.Natl.Acad.Sci.U.S.A 91:9253-9256, 1994
22. Castaing,M, Guerci,A, Mallet,J, Czernichow,P, Ravassard,P, Scharfmann,R: Efficient
restricted gene expression in beta cells by lentivirus-mediated gene transfer into
pancreatic stem/progenitor cells. Diabetologia 48:709-719, 2005
23. Davalli,AM, Ogawa,Y, Ricordi,C, Scharp,DW, Bonner-Weir,S, Weir,GC: A selective
decrease in the beta cell mass of human islets transplanted into diabetic nude mice.
Transplantation 59:817-820, 1995
24. Montana,E, Bonner-Weir,S, Weir,GC: Beta cell mass and growth after syngeneic islet
cell transplantation in normal and streptozocin diabetic C57BL/6 mice. J.Clin.Invest
91:780-787, 1993
25. De Krijger,RR, Aanstoot,HJ, Kranenburg,G, Reinhard,M, Visser,WJ, Bruining,GJ:
The midgestational human fetal pancreas contains cells coexpressing islet hormones.
Dev.Biol. 153:368-375, 1992
26. Riedel,MJ, Asadi,A, Wang,R, Ao,Z, Warnock,GL, Kieffer,TJ: Immunohistochemical
characterisation of cells co-producing insulin and glucagon in the developing human
pancreas. Diabetologia 55:372-381, 2012
27. Gittes,GK: Developmental biology of the pancreas: a comprehensive review.
Dev.Biol. 326:4-35, 2009
28. Rafael,E, Tibell,A, Ryden,M, Lundgren,T, Savendahl,L, Borgstrom,B, Arnelo,U,
Isaksson,B, Nilsson,B, Korsgren,O, Permert,J: Intramuscular autotransplantation of
pancreatic islets in a 7-year-old child: a 2-year follow-up. Am.J.Transplant. 8:458-462,
2008
29. Christoffersson,G, Henriksnas,J, Johansson,L, Rolny,C, Ahlstrom,H, Caballero-
Corbalan,J, Segersvard,R, Permert,J, Korsgren,O, Carlsson,PO, Phillipson,M: Clinical
and experimental pancreatic islet transplantation to striated muscle: establishment of a
vascular system similar to that in native islets. Diabetes 59:2569-2578, 2010
30. Lund,T, Korsgren,O, Aursnes,IA, Scholz,H, Foss,A: Sustained reversal of diabetes
following islet transplantation to striated musculature in the rat. J.Surg.Res. 160:145-
154, 2010
31. Sterkers,A, Hubert,T, Gmyr,V, Torres,F, Baud,G, Delalleau,N, Vantyghem,MC, Kerr-
Conte,J, Caiazzo,R, Pattou,F: Islet Survival and Function Following Intramuscular
Autotransplantation in the Minipig. Am.J.Transplant. 2013
32. Pattou,F, Kerr-Conte,J, Wild,D: GLP-1-receptor scanning for imaging of human beta
cells transplanted in muscle. N.Engl.J.Med. 363:1289-1290, 2010
33. D'Amour,KA, Bang,AG, Eliazer,S, Kelly,OG, Agulnick,AD, Smart,NG,
Moorman,MA, Kroon,E, Carpenter,MK, Baetge,EE: Production of pancreatic
hormone-expressing endocrine cells from human embryonic stem cells.
Nat.Biotechnol. 24:1392-1401, 2006
34. Kroon,E, Martinson,LA, Kadoya,K, Bang,AG, Kelly,OG, Eliazer,S, Young,H,
Richardson,M, Smart,NG, Cunningham,J, Agulnick,AD, D'Amour,KA,

��QG���
Carpenter,MK, Baetge,EE: Pancreatic endoderm derived from human embryonic stem
cells generates glucose-responsive insulin-secreting cells in vivo. Nat.Biotechnol.
26:443-452, 2008
35. Jacobs-Tulleneers-Thevissen,D, Bartholomeus,K, Suenens,K, Vermeulen,I, Ling,Z,
Hellemans,KH, In't,VP, Pipeleers-Marichal,M, Pipeleers,D: Human islet cell implants
in a nude rat model of diabetes survive better in omentum than in liver with a positive
influence of beta cell number and purity. Diabetologia 53:1690-1699, 2010
36. Jensen,J, Heller,RS, Funder-Nielsen,T, Pedersen,EE, Lindsell,C, Weinmaster,G,
Madsen,OD, Serup,P: Independent development of pancreatic alpha- and beta-cells
from neurogenin3-expressing precursors: a role for the notch pathway in repression of
premature differentiation. Diabetes 49:163-176, 2000
37. Heimberg,H, Bouwens,L, Heremans,Y, Van De,CM, Lefebvre,V, Pipeleers,D: Adult
human pancreatic duct and islet cells exhibit similarities in expression and differences
in phosphorylation and complex formation of the homeodomain protein Ipf-1.
Diabetes 49:571-579, 2000
38. Sun,Y, Pollard,S, Conti,L, Toselli,M, Biella,G, Parkin,G, Willatt,L, Falk,A,
Cattaneo,E, Smith,A: Long-term tripotent differentiation capacity of human neural
stem (NS) cells in adherent culture. Mol.Cell Neurosci. 38:245-258, 2008
39. Kassem,SA, Ariel,I, Thornton,PS, Scheimberg,I, Glaser,B: Beta-cell proliferation and
apoptosis in the developing normal human pancreas and in hyperinsulinism of infancy.
Diabetes 49:1325-1333, 2000
40. Meier,JJ, Butler,AE, Saisho,Y, Monchamp,T, Galasso,R, Bhushan,A, Rizza,RA,
Butler,PC: Beta-cell replication is the primary mechanism subserving the postnatal
expansion of beta-cell mass in humans. Diabetes 57:1584-1594, 2008
41. Chen,H, Gu,X, Liu,Y, Wang,J, Wirt,SE, Bottino,R, Schorle,H, Sage,J, Kim,SK:
PDGF signalling controls age-dependent proliferation in pancreatic beta-cells. Nature
478:349-355, 2011

��Q4���
B�����������
#���
$#��%#���&#���
�
�
�
�
�
�
$����� �������D���������BC���B�ED�CA��������AB������A�BC�����E��������CA������C����
CE�B��DB ��� AB� �A��� ��C� �B�� B�������� ���E����� ��E��CC�BC� ��B�A����E� �DC��A�E� ���
ED����CA�B������EC�AB��� B�����E������#�DEA�B���������AB���������EC�������B�CA�B�AB��A����!��
��E��C�����A������A�E���������BAE������EC�AB��������������E��D�����E������ B���E����EC��E��
�� �A��DE�BC�� �C����� ��� �D���������BC�� �B�AB�� A�� ���E�� ��� ����A�A�ACD� C�D�EA���� ��� CEA�E�
���A������BC� ���� ��������� �E��DBACEA���� �EC��� ��� CE�B�� B�� �C� ��� ���E��A�E�� ���E� DC���� AB�
�ACE����

��GH���
Le choix du site musculaire
�
$E� ��������C�E� �� ��C�C�F� �E�D���� DE� ��!��E��E�� ���FE�� ��� !�D<�E� DE� �F��'�E--E� DE�
���B�F����E!�������C�E���!�C����������B�����E��F���E�DE�����C��/(.�A�.����F�F�DF!����F�
��E� BE�!�D<�E� �FB��C����C�� �@E��E!��E� D�� DF8E����E!E��� E�D�B�C�E� �E�� ��@���E�8F� AB�
�C�E�� 9�C��CADB�#�� ��� *�$$�=� � �//�=�Diabetologia:A� (E�E�D���=� ��� ��C�BC���E� �C!C���C���
�F�CDE�D�����E��DC--CB���F��>�!�DC-CE��'F�F�C��E!E����E�����B�F���'�E--F��E����C����DE����
�C����C��� �����!C��E� D�� '�E--��=� ��� B����B�� D�� �EC�A�&E�� �E����C8E������� E--EB��E�� D��
�����-E��� DE� '<�E�� D���� BE�!�D<�E� ���� C�BEB�C���� � DC�EB�E�� D���� �@���<�E� �F���E=� ���<��
B��!��'E=� � ���� FB���F� >� B���E� DE�� B�����C��E�� � �F!�D���!C��E�� C�D�C�E�� ���� ���
!��C�C���C��=����DC��EB�C���E���E�B����P�E�D���FDCB��E��F���A�����8���C����D��B�����8E��
��E����E����C8E��������-�BC�E��� B�E0� �E��E�C�� ��C!��A��E�� ���8������F�C!C��C�E��DE�'�E--E�
!��B���C�E���E�B@�C��F��C�F��>�����C��DE��C'�FE��BE�����C�E��β�C�����D@C����C��!E��DE�����C��
9�C'�FE�&C�F:�E��DE�����9�C'�FE�C���:��9��!C��C���DE�BE����E��&C�F����C����'�E--FE��D�����E�
!��B�E� D���� ��� E�����'E� DE� !���C'E�:� !@�8�CE��� �E�!C�� DE� �E��E�� ��E� �E� !��B�E�
���8�C��K��E�����C�E��BBE��E���DE�����E�����C�F����C���E=���������DE��E�B����=�B@���E��C��
���C����C��!E�8��B����C�F�C�D�C�������E�����'��BF!CE��F���E�B�E0��������C�A��E�����=�E��
B�C�C��E� ��!�C�E=� C�� �8�C�� F�F� !����F� ��S��E� ����'�E--E� C����!��B���C�E� D@T�����
���B�F��C��E��B�E0���E�E�-����DE�Q������8�C����E�!C��DE��FD�C�E��E���E��C���E��C����C�E�
DE�BE��E�BC����<�����B�F��EB��!CE������E����������B�F��C�E��F�FDC��C�E��F8<�E�9�C+C�$�%��
��� *�$$�=� ��//-=�Am.J.Transplant.:A� $@F��C�E� �8�C�� E����C�� �E�� T����� DE� $��'E������ DE� ���
���CE��E�>�����C��DE� ����C<BE�DE����B�F��EB��!CE�E�� �E�� ��C� �8�C�� '�E--F��D���� �E�!��B�E�
���B�C���DC��C��DE� �@�8��������=�Q���E��E����������DA����<��DE�������DE���C8C=� �E��C8E���
������ E�� ��C!��F� DE� �E��CDE� (=� !����E��� C�DC�EB�� DE� ��� �FB�F�C��� D@C����C�E=� �E��<�E���
�����E�� E�� C��� ���E�8<�E��� ��E� DC!C���C��� ���'�E��C8E� DE� �E�� �E��C��� E�� C����C�E��
E��'<�EA���������D=���E�����E�F��C�E�DF!�����C�=�B�E0�������CE���DE�;G����=�������8CE�DE��
T�������������<������'�E--E� C����!��B���C�E� � 9�C�����-�����*�$$�=� ��/�/=�N.Engl.J.Med.:A�
(E�� DE��� F��DE�� ��''F��CE��� -���E!E��� ��E� �E� !��B�E� ���8�C�� K��E� ��� �C�E� �BBE��E���
E--CBCE��� ����� ��� '�E--EA� .�� �E���C�� � >� ��8�C�� �C� �@��� ���8�C�� ���E�C�� ��� DF8E����E!E���
E�D�B�C�E�B�!��E��>�����C��DE�BE����E�DE�'�E--EA�(E����8�C�����E�!C��DE�B��-C�!E��BE��E�
������<�E�C�C�C��EA�
�

��G����
Les potentielles applications cliniques de la greffe intramusculaire
$E���F����������E�������8�������E�����C��C���E��E�����8����DE���-�E��E��B���A��E���������E��
B���A� 9�C+C�$� %�� ��� *�$$�=� � �//-=� Am.J.Transplant.O� �C����� -�� ��� *�$$�=� � �/�/=�
N.Engl.J.Med.:� ��''<�E��� ��E� BE� �C�E� !��B���C�E� �E��� �E��F�E��E�� ��E� ���E����C8E�
C��F�E�����E=�B���!�C���C�8��C8E=�>����'�E--E�D@T�����D�����E�����<!E�8EC�E�������E�98EC�E�
��C�BC���E� C��C'����� �E� -�CE� E�� ��C� ��C�� DE� ��� �F��C��� DE�� 8EC�E�� DE� D��C��'E� D�� ���E�
DC'E��C-� E�� DE� ��� ���E:A� (E��E� � �EB�E�B�E� DE� �C�E�� E������F���C��E�� DE� '�E--E� D���� ���
��F���CE�BE�����C�E�D��DC��<�E��E�����E���E��C���D@�B����C�F���C���E���E���F��������>����'�
�E�!E�DE��B�����E��DE����CE�����������F�F-CBCF�D@��E�����'�E--E�D@T�����D���� �E�����<!E�
����E� ����� !�C��� ���!E��E���� ��@���E�D�� � 9)�C�A��� �� #�� ��� *�$$�=� � �//1=�
N.Engl.J.Med.:A� (EBC� �CE��� >� ����CE���� ��C����A� C:� ��� DE����B�C��� ��FB�BE� DE� BE�� T�����
C�BEB�F������ �E�� BE����E�� C�-��!!���C�E�� BC�B�����E�� 9#�"��B�=�����*�$$�=� ��//�=�LancetO�
2���B��D�3�����*�$$�=���//-=�Diabetologia:=�CC:��SC���--C���BE�DE��E8��B����C���C����E--CB�BE�
E����FB�BE�DE�BE��DE��CE���9#C�����D�D�����*�$$�=���//�=�DiabetesO����A���++�����D�D�����
*�$$�=� � �/�/=�Diabetes:� E�=� ����� C���CF����=� CCC:� ��E� ���E��CE��E� ���CBC�F� C����� �F���C��E�
DC�EB�E�DE�BE��T�����9!�C�BC�C�������*�$$�=���//!=�Diabetes:�E������C���E���!�����D�����E�
-�CE� �EBE8E��� 9���"��C�1A� -�� ��� *�$$�=� � �//1=� Cancer Res.:A� $�� ��E��C��� DE� ���
�E8��B����C���C�����F�F����C�FE������@F��C�E�DE���-�E��E��B���A�9���A���++�����D�D�����*�$$�=��
�/�/=�Diabetes:A� .�������DF!����F=� >�����C��DE� �@F��DE�DE� ��� �E8��B����C���C���DE�� T������
�F��'�E--F��D���� �E�!��B�E����D���� �E� -�CE�B�E0� �������C�� �E��D@C���������'�E--F��D���� �E�
!��B�E�B�E0��@#�!!E=���E����DE��C�F�B��C���C�E����E��E��E�B��������<��'�E--E�!��B���C�E�
F��C��CDE��C��E�>�BE��E�DE��T�����C���C��=�BE���C��@E��������E�B������<��'�E--E��F���C��EA��(E�
�F��������E��F�E��E�E�B��E������'�!E���-����������E��E����E��E��C�E�!��B���C�E�������C��
K��E� ��E� ���E����C8E� 8��CDE� D���� BE� ���E� DE� ��F���CE� BE�����C�EA� .�� �E��E� �F��!�C��� >�
DF�E�!C�E�=�D���� �E� B�D�E�D@����'�E--E�� B�E0� �@#�!!E=� �C� �E��!FB��C�!E�� C!!��C��C�E��
!C��E��BE��D�����E�!��B�E��@E����C�E���������E�DE����B�C�����������CDE�DE��T�����B�!���F�
����C�E��F���C��EA��
�
)������E=��C� �@����'�E--E�D@T�����E���������FE�>�BE���C������CE����DC��F�C��E��DE����E��=� C��
�E��E���@C���@����������--C��!!E���DE�D���E������������������������E��CE����EBE8E���A�3��
��BEB�C-�DE����B�!!�����F��BCE��C-C��E�E���D��B�DE�DF8E����E��DE������BE�����E����C8E��
DE� BE����E�� βA� ����� BE� B���E��E=� �E�� BE����E�� ���B�E�� E!�������C�E�� ��!�C�E�� 9�)/(:�

��G����
�E��F�E��E�����E�����BE����E��CE��E�E��DE�������B��E��E�C��E���!�C��E����������'F�F�E��
DE�����'F�C�E�������B�F��C��E���� �[�>�����C��DE��)/(�9�H�����2�������*�$$�=���//0=�
Nat.Biotechnol.O��H�����2�������*�$$�=���//1=�Nat.Biotechnol.:A�C����E��>�C���@������F�F�
����C��E�D@C�D�C�E=�C��8C���=���E�DC--F�E�BC��C���DE�BE�����'F�C�E����E��BE����E��β�!����E��
-��B�C���E��E�� !�C�=� C�� �� F�F� DF!����F� ��@C��� � ���8�CE��� �E� DC--F�E�BCE�� E�� BE����E�� β�
!����E�����<��'�E--E����������B�����E��F���E�DE�����C��C!!����C�B�!�F�E��E��92���D�%��
���*�$$�=� ��//-=�Nat.Biotechnol.:A� .�� �� �� �D��B� ����E���E�DC�B���C��� ���� �E� �C�E�DE�'�E--E�
CDF���D��������E���EB�C8E=��E���K��E������C���C���C�E=�DE������B��E��DE���F���CE�BE�����C�E�>�
����C�� DE� BE�� ���'F�C�E���A� 3�E� DE�� ��C�BC���E�� �����F!��C��E�� ����E8FE�� ���� BE��E�
�����B�E�E����E��C���E�B��BC����'C��E����E��CE��DE��E��������B��E����C���E�A�C:�C���@�'C��C��
DE�'�E--E��DE��BE����E������C���E��E���� �[��������CE����E��CC:� C���E����E��C��E��DE���)/�
���� �����-��!FE�� E�� ���'F�C�E���� �� �[� D���� �E�� ��F�����C���� BE�����C�E�� ����
�E��C�C�C�F�C�B�!��<�E�DE��!F���DE��DE���C�BE�����C�EA��@�C��E����2�����)�E��B���A=�D�����E���
F��DE� C�� 8C8�� ���� �!C�� E�� F8CDE�BE� �=�M�DE� �F����!E�� C!!����E�� DF8E����F�� D���� �E�
'�E--��� E�� �7=�M�DE� �F����!E��!����E�A�)����E����� E�� B�!��E� BE� �C���E=� �E� -�CE� ��� �E�
�EC���E!��E���D��'E�E���B����E��E���C��D��'�E--��=������DE����C�������B���'C��E�=��E��C��
B�!��E�EA� �E� ����� ��� E�8��C��E!E��� ��!����� DE� BE�� DE��� ��'��E�� ������C�� �8�C�� DE��
B���F��E�BE�� ��<�� �FB����C8E�� ����� � BE�� ���CE���A� (�!!E� �E�� �F�������� ���E���� D����
����E� ���8�C�� DF!����E��� ��@C�� E��� ����C��E� D@���E�C�� ��E� DC--F�E�BC��C��� CDE��C��E� DE��
���'F�C�E���� ���B�F��C��E�=� >� ����C�� DE� ���B�F��� E!�������C�E�=� ����� ����� ��� B�����E�
�F���E� ��E� D���� �E� !��B�E=� BE� DE��CE�� DE8CE��� ��� B��DCD��� C��F�E�����=� D���� BE��E�
���C��E=���C���E�-�BC�E�>����8EC��E��9E��B�C�C��E����E��C!�'E�CE:A�/����E������B�C�C��E=�E��
����E=� �E� DF8E����E!E��� ��!����� ��C!C�C-� 9��!E��� !��C'�E� ��C!C�C8E:� ��� �EB��D�C�E�
9!F������E�:�D���� �E�!��B�E�E���E�BE��C���E��>� �@�'E��D���E�B�����C�E!E������ -�CE�9�C�E�
DE� !F������E� -�F��E��:A� (E��� �E��F�E��E� E�B��E� ��� ��'�!E��� E�� -�8E��� DE� BE� �C�E�
���E����C-A� � )�-C�=� ��E� B�C���'CE� D@E�F�<�E� >� BE� �C8E��� �E��C�� !�C��� DC--CBC�E� E�� !�C���
�C���FE���������������������E���C�E��F��DCF��B����@>���F�E��A��
�
�
�
�

��G7���
Discussion des résultats obtenus et des questions soulevées par ces résultats
����� �SE��E!��E=� ���� �F�������� ���� B��-C�!F� �SE--CB�BC�F� DE� BE� !�D<�E� DE� '�E--E�
C����!��B���C�E�DE����B�F����������FB��C���E���E�DF8E����E!E���E�D�B�C�E����!��A�$E��
DC--F�E�BE�����E�8FE�����<��'�E--E�E���E��E�DF8E����E!E��� �D�����B�F���!��C��E��BE��C�
D�� ���B�F��� ��!�C�� ����C'�E��� E�� ����E� ��� ��FBC-CBC�F� DE� B����E� E��<BE� ���� ���
DC--F�E�BC��C��� BE�����C�E=� ��� !������C��� E�� ��� ����C-F���C��� DE�� DC--F�E��E�� �C'�FE��
���B�F��C��E�A��
�
.�� E��� C��F�E������ DE� ���E�=� ���� E�E!��E=� ��E� ��� �C'�FE� E��B�C�E� �@E��� ��EC�E!E���
DF8E����FE�D�����E��'�E--E��DE��C�������!�C���B�!�����C8E!E��������'�E--E��DE��C�����DE�
����C�=� D���� �E���E��E�� ��B��E� BE����E� �!����E����C�C8E��@�� F�F� �E����8FE� >� ��� -C��DE� ���
�F�C�DE� DE� '�E--EA� $�� ��C���� DE� BE��E� DC--F�E�BE� �SE��� ���� B��C�EA� $E�� D���FE�� ���� �E�
DF8E����E!E��� D�� ���B�F��� E��B�C�E� F����� E�B��E� ���E�� D���� ��� �C��F�����E=� �E��
������<�E�� ����� ��!��E��E�A� 5�� ������C�� �E� DE!��DE�� �C� BE��E� DC--F�E�BE� �SE��� ����
�E��E!E���D�E�>� ���DC--F�E�BE�DE� �C!C�'�DE�DF8E����E!E���E���E� �E��DE���E��<BE������
���������������DE�����E�8F�A�)��E--E�=���C���E��E�DF8E����E!E���D�����B�F���DE�����C��
��E�D����BE�E����H�B�����E�����B���E�C���D������<!E�D�B�������D��DF��!��E��E����D�C��
����D��������E�!�D<�E=��E���K��E���E� BE�� BE����E���BC�E��E�� �E� �����DF8E����FE��!�C��
��E� BE� B���C�'E��� BE�����C�E� ����C�� ���C� ��E� �������E� �EB��D�C�E� >� ��E� ����DC'E��C���
���B�F��C��E�DE8�����@C!����C�C�C�F�D@E�B�F�E���E����E�0�!E��D�������BC�B�C���E�!F���EA��
(E��E����E�BE�DE�B���E�C���D������<!E�D�B�����E�!��C-E��E=�D��������E�!�D<�E�������E�
D������CE�1���C��E�D�B���E������D�����E��'�E--����!��C�����E�BE�����!�C��A�.��E�C��E����
!�D<�E�!��C��DE�D������CE�D�B���E���FB�BE��8EB�DF8E����E!E���1���C��E�B�����C�E�����
!����C��� C��B�C8���CBE� C����� ���B�F��C��E� D@��� -�B�E��� DE� �����B�C��C��� >� ��!F��
D�!�C�E�A� ������� 9�����E��� ��!E����� ����EC�� �:� (E��E� F��DE� DF!����E=� E���E� ����E=�
��E� ��� D������CE� 1���C��E� C�D�C�� ��E� ���F-�B�C��� DE�� BE����E�� �BC��C�E�� �8EB� �E� �E!���
9G�������$CD��8��8�����*�$$�=���/��=�Gastroenterology:A��E�����=��E�-�C����E�D�������'�E--E�
DE� ���B�F��� ��!�C��� �E�� BE����E�� �BC�E��E�� ����� ��F�E��E�� B����@>���� ���DE� ���DC-� 9FH�
�E!�C�E��DE�DF8E����E!E���D��'�E--��:=�!�C���E!��E��@C��E��!�C�D�E������C�F� ��8EB� �E�
�E!��� 9B-A� -C'��E� /�=� ���CB�E:=� E��� �E��� K��E� E�� -�8E��� DE� ��� ��E!C<�E� ������<�EA� .�� E���
����C��E� ��E� ���� �E� ���'� �E�!E� ��� �@���E�8E��C�� ����� DE� BE����E�� �BC��C�E�� � D���� �E��
'�E--���� ��!�C��� E�� ��E� B�E0� ��� ����C�� BE� �C!C�'� E��� ��<�� B����A�&���E��E��E!E��� ���

��G;���
��C8C���������'�DE��'�E--������!�C����E����E��E�8C��'E���E�B�E0��E��E�C����C!����>�B���E�
DE����B��C����BE�DFB>�C!�������E�D��'�E--�����!�C�����<������=�DE����������DE��FB�F�C���
D@C����C�E� ��!�C�E� C�D�C����� ��� F���� ����'��BF!C��E� ���'�E��C-� B�E0� ��� ����C��
�EBE8E��E=� E�� E�-C�� DE� ��� ���8CE� �����E��E� DE� ��� ����C�� DE� ��������C�E� �@E�BFD���� ��E�
���E!E��������>������X�A�3�E�����E�������<�E��E��C����E��@���E�BE�DE�B���E�C���C�C�C��E�
DE� �@����E� ���B�F��C��E� E��� >� �@��C'C�E� D@��E� D��'F�F�CE� D�B���E� C�D�C����� E���C�E� ��E�
�'F�F�CE� �BC��C�EA� 3�E� DE��C<�E� ������<�E� �E��C�� E�-C�� ��E� �E�� !FB��C�!E�� � D��
DF8E����E!E���E��B�C�E�DC--F�E���E���E��E��DE���E��<BE��E����E�����E�!�D<�E�DE�'�E--E�
�E� ��C�� ���� �E�!C��C-� ����� �E� DF8E����E!E��� �BC��C�E� >� ����C�� DE� ���B�F��� C!!����E��
!��C��A��
����� �8��BE�� ���� BE��E� ��E��C��=� C�� B��8CE��� DE� B�!!E�BE�� ���� E��!C�E�� �E�
DF8E����E!E��� E��B�C�E� >� DE�� ��C���� C��E�!FDC�C�E�� E���E� CH� E�� C�E� ���<�� '�E--E� DE�
���B�F���!��C��A�(E����C����-E������@��BE��DE����8����D�����E����C�E��DE�BE����8�C�A �
�
3�� ����E� ��C��� C��F�E������ B��BE��E� �E�� DC--F�E�BE�� D@E���E��C��� DE� �� �� ���E�8FE��
D��������E�F��DEA���������E�D�����E��'�E--E��DE����B�F���!��C��=�DE����E!�C�E�����<�����
'�E--E=� ����E�� �E�� � BE����E�� �� ��[� B��E���C!E��� �SC����C�E� B�!!E�D���� �E� ���B�F��� DE�
����C���D���E=��E��'�E--E��DE����B�F�����!�C��������E�!C��DE�B��-C�!E������E��C����BE�DE�
�@E���E��C��� DE� �� �� E�� DE����� D�� D�!�C�E� E�D�B�C�E� 9��A�"��B���� ��� *�$$�=� � �///=�
DiabetesO��C��CADB�#�����*�$$�=���//0=�Diabetologia:A�(E���C����E��F�E��E���E�DC--F�E�BE�
!�BE��E� E���E� �E�� �� E��<BE�� ��� B����� D�� DF8E����E!E��=� E�� �E� �P�E� DE� �� ��D���� BE��
BE����E�� D�B���E�� �E��E� >� DF�E�!C�E�A� )�� E--E�� ��� �E��� �E� DE!��DE�� �C=� ���� BE��E�
E���E��C��� �E��C�����E=� �E�� BE����E�� D�B���E�� �E� B���E�8E��� ���� DE�� B���B�<�E��
E!�������C�E��B�E0��@#�!!EA�
����� �8��BE�� ���� BE���C��=� .�� -��D��C�� D���������E!CE�� �E!���DF�E�!C�E�=� >� DC--F�E����
���DE�� 9��FB�BE�� E�� ���DC-�:=� �E�� -�B�E����DE� �����B�C��C��� B��E���C!F�� �8EB��� ��D����
�E�� BE����E�� ���� E�D�B�C�E�A� .�� -��D��C�� ����!!E��� F��DCE�� �@E���E��C��� DE� �"+��=�
*�"�;=� *�"�F� E�� ��5 �A� (E�� DE��� DE��CE��� -�B�E���� �E!��E��� �����'E�� �E�� !K!E��
�E��C��C�E�� ��E� �� �� B�E0� ��� ����C�A� � )�� E--E�=� ���<�� ��E� F���E� D@E���E��C��� ��C��C��E�
D���� �@F���B�E� ���B�F��C��E=� BE��E� BC� �E� �E���EC��� ���� BE����E�� D�B���E�� E�� ����
���'F�C�E���� E�D�B�C�E�� 9B-A� C����D�B�C��:A� 3�E� DE��C<!E� F���E� �E��C�� D@����C��E�� ���
�EB��C��E� DE� �����-E��� DE� '<�E� �8EB� BE��E� -�C�� ��� �����'<�E� *+�� ����� �E� B����P�E� D��
���!��E��� �� �� E�� ��C8�E=� >� DE�� ���DE�� DC--F�E���=� �E� DE8E�C�� DE� BE�� ���'F�C�E����

��GE���
C�C�C���A�5��������C������C�E�8C��'E��DE������D�C�E�DE���'<�E���������E����B�D���������
DE��� ����FC�E�� DE� -����E�BE�BE� DC--F�E��E� ����� �E� B����P�E� DE� DE��� � ���!��E����
DC--F�E���� 9�� �� E�� *�"�F� ���� E�E!��E:� �-C�� DE� ���8�C�� ��C8�E� B��B�C��E!E���
�@E���E��C���DE���'<�E��D@C��F�K�A�
�
3�� DE��CE�� ��C��� D@C��F�K�� �E��C�� DE� ������C8�E� ��� B���B�F�C���C��� DE�� ��������
D@E���E��C��� DE� *7� E�� 2 �A�A� ����� BE� ���8�C�=� B�!!E� �� �� �E��F�E���C�� ���
!����E��� !�C��� �E��C�E��� DE�� BE����E�� ���'F�C��CBE�� >� DE�� ���DE�� ���DC-�� D��
DF8E����E!E��=�������8������C8C� ���BC�F�C��E�DE� �*7�E��2 �A�A����<��7Q��E!�C�E�=�
��B��E� �BE����E�*7[��@E������E�8FE�E�� �E�����!��E� � �E!��E�DFB>� -���E!E���DC!C��F�
���<���4��E!�C�E��DE�'�E--EA��(EBC���''<�E���E��E����BE�����DE�DC--F�E�BC��C���E�D�B�C�E�
E����������E!E����E�!C�F��8�������-C��D�����C�C<!E���C!E���E�DE�'E����C�����C���E�*7�
E��E����E�-�B�E���DE������B�C��C���C�C�C��E��A��
����� ���E�C�� DE�� D���FE�� ����� ��FBC�E�=� C�� B��8CE��� DE� �F��C�E�� DE�� B�!���'E�� � DE��
BE����E�� *7� ���� DC--F�E���� ���DE�A� $@��E� DE�� �C!C���C���� !�BE��E�� >� BE��� ����� �E�
!�!E���E������DC--CB���F�DE��F��C�E��DE��@C!!���-����E�BE�BE�DE�����C�F��8EB��@���CB�����
���C� *7� ��E� ����� ��C�C����A� $E�� B��!�����'E�� ����� DE� -�C�� DC--CBC�E�� >� �F��C�E�� �����
�@C������A�.���E��C��D@�C��E��������C�C��F�E������DE�DF�E�!C�E���E����E��CE��DE�����C-F���C���
DE� BE�� BE����E�A� � ����� ����CE�� BE�� DC--CB���F�� �EB��C��E�� B��B��B���E��E�=� ��� ������C��
�F��C�E�� BE� ���8�C�� �8EB�2 �A�=� -�B�E���DC�EB�E!E���E���8���DE�*7�D���� ��� �C'�FE�βA�
)�-C�� C�� -��D��C�� ����C� �@����B�E�� >� B��-C�!E�� �E� ����E��� D@E���E��C��� DE�� ����E��
!����E���� E�D�B�C�E�� 9�+ F=� �� =� E���E� ����E�:� !�C�� ����C� DE�� -�B�E���� DE�
�����B�C��C�����FB�BE��9/5 4=�& �=�*�"�F:A�
�
�
Le transfert de gènes et les applications potentielles pour l’étude du développement pancréatique
���� �8���� �F��C�F� �8EB� ��BB<�� �E� �����-E��� DE� '<�E�� C�� 8C8�=� >� 7�!�C������� '�E--E=�����
C�BEB�C���� �E��C8C���E�� DC�EB�E�� D���� �E� '�E--��A� ��� ��F�����E� ����� �8C���� E����F� DE�
�F��C�E�=� D���� BE�!�D<�E�!��B���C�E=� DE�� C�BEB�C���� C����8EC�E��E�� >�����C�� DE� ��� 8EC�E�
C�C���E�E��E��E�E��E��!�C��E������E��8�C��E����C�C���E��B��!�F���E�D�����H�!C���E�A�$E��
�F�������� E�� !��C<�E� DE� �����D�B�C��� �@F��CE��� '�<�E� !EC��E���� ��E� BE��� ���E���� ����

��GF���
C�BEB�C���DC�EB�E�D���� �E� '�E--��A� (E���C��� E��� DC--CBC�E� >� E���C��E�A� ���� ������ �E� ����� DE�
�����D�B�C��� E��� E�B��E� -�C��E�D���� �E�� B��DC�C������C�C�FE��D���� BE� ���8�C�A� .�� B��8CE���
D��B� D@E����E�� D@�!F�C��E�� BE� ��C���A� C:� E�� ���C!C����� �E�� B��DC�C���� E��F�C!E����E��
9��'!E��E�� ��� B��BE�����C��� 8C���E=� B��!��'E� �E� ����� ���'� ����C��E� E�� B��� D@C�BEB�C����
C����8EC�E��E=� B��C�C�� DE�� ����C�� �EBE8E��E�� D���� �@C!!����C�B�!�F�E�BE� DC--<�E� E��
-��B�C���D�����E�DE�8EB�E�����C�C�F:�CC:�E��B��C�C�������E�8EB�E���8C�����E�!CE����D���F����
���E�DE���E��C�������FE�A�
�
���!C��E��8EB�E����C��F'���C-�=� �E�B��C��D@���8EB�E���DE����E��E��C8C�����E��C�����-�C����E�
����� �����C�C���� � C�C�C��E!E��� C�-EB�E�� �����E!E��� DE�� BE����E��β� D���� ��� �����CF�F�E���
D@K��E�-�C��E!E�������C-F����E�A�(E��8EB�E�����E��C8C������E�8E���C�-EB�E��������E��BE����E��
��CE�BE��E�� ��E� �E�� BE����E�� E�� DC8C�C��� ������ ��E� �E�� ����E�� 8EB�E���� �F���8C�����
�E�!E��E�����E�C��F'���C��������E����'F��!E�DE��S�P�E�!�C���E��E�8E���C�-EB�E����E��E��
BE����E��E��DC8C�C��A�������E�����DE�BC��E��DE��BE����E��E�D�B�C�E���8EB����-�C��E������DE�
����C-F���C��=�BE��DE��CE����@F��CE��������������CF�A�)���E8��B�E=�F�����D@��C�C���C��������
-�BC�E� ��E� �E�� �E��C8C���=� � C�� '��DE� ����E� �E��� ���BE� ����D� ����� 8��D����� C�-EB�E�� DE��
���'F�C�E�������B�F��C��E�=�>�-���������DE�����C-F���C��A��
�
3�� ����E� ���E� DE� 8EB�E��� ����E�� ����� �8���� �F-�FB�C� ����� �E�� ��D� 9�DE�������BC��ED�
8C���:A� � (E�� DE��CE��� ���� ��� ����CB����C�F� D@K��E� DE� �E�C��� 8C���=� ���� C��F'���C-�� !�C��
�����E�� E�� �����!C��C��E�� >� ��� DE�BE�D��BE=� �E�� �����'<�E�� ����� �@#�!!E� E�� E�-C��
���8����C�-EB�E����<��E--CB�BE!E���DE��BE����E��E��B�B�E������CE�BE��E�A���E������C��E�C��E=�
�E�����E���������E=���E�BE���C�E���FBC-CBC�F��C�����C�EA�.����F�F�DF!����F=�����E�E!��E=���E�
�E�� ��DF=� ��DG� E�� ��D4� �E�!E���CE��� ��E� C�-EB�C��� E--CB�BE� E�� �����E� DE�� BE����E��
E��B�C�E�� E�� E�D�B�C�E�� ���B�F��C��E�� 9GCDB��� ��� ��� *�$$�=� � �//!=�Hum.Gene Ther.O�
8A��D�'� F�� ��� *�$$�=� � �/��=� Diabetologia:A� � )�� ����E� �E�� ��DF� �E!��E��=� D���� �E�
B�!����C!E��� E��B�C�E=� ���8�C�� C�-EB�E�� ��FBC-C��E!E��� �E�� BE����E�� D�B���E�� �����
C�-EB�C����BC��C�E�98A��D�'�F�����*�$$�=���/��=�Diabetologia:A��������E�������B�E��DE���C8C�
DE� �C'�FE� ��E� ����� �����C����� DF8E����E�� ����E�� BE�� B���B�F�C��C��E�� -���� DE� BE��
8EB�E����DE��B��DCD������<��C��F�E�������B���D@��C�C���C��������-�BC�E�E��������FB��C�FE=�E��
D@E���E��C��������E�������E��C�C�����E��CE��E!E���C�D�C��������@C��F'���C���8C���E�B�!!E�
B@E��� �E�B����8EB��E���F���8C���A� �$���E��E��E���CB�C����F��!�C����E��E������C��E�!��C!��E�
D�������'<�E�����F=���C�E���DE���-�C��C�-F�CE��E�>�BE��E�DE���F���8C���A��

��GQ���
����� ���B��F'��CE�DE��8EB�E�������� C��F'���C-�=� C����������C� �E���DF��8C���A�(E��DE��CE���
�E�!E��E��� DE� �����D�C�E� ��<�� E--CB�BE!E��� �E�� BE����E�� E�� C�DF�E�D�!!E��� D�� B�B�E�
BE�����C�EA�)������E=� �E�� �����DE����D�B�C�����<��F�E8F���E�!E��E���D@���E�C�� -�BC�E!E���
DE�� B��BE�����C���� ��<�� C!�������E�� DE� 8EB�E��A� )�� E�-C�� C��� �E�8E��� C��F'�E�� DE��
�����'<�E��DE���<��'���DE���C��E=��E�D�����@E���E��C������B����E�DE�����CE���������'<�E��
-�C����E�A� )�� �E8��B�E=� BE�� 8C���� �E� ����� ���� C��F'���C-�� E�� �E� �E�!E��E��� ��@��E�
E���E��C��� �����C��C�E� D���� ��� BE����E=� ���� �����!C��C��E� ���� BE����E�� -C��E�A� (E� ���E�
D@�����B�E� ������C�=� D���� ����E� !�D<�E=� >� DE�� ���DE�� ��FBC�� D�� DF8E����E!E��=�
�E�!E���E��@E���E��C���D�������BE����E�BC��E�D@���-�B�E�������FC��E��E�������E������D@���
��� C��E�-F������-C��D@E��������E�� �E��B���F��E�BE������ �E�DF8E����E!E��A�(E� ���E�DE�
8C�����E�������C�K��E���C�C�F������C���E��DE��BE����E�����FBC-C��E�=�>�������DE���FBC��DE��E���
DF8E����E!E��� C�� 8C8�=� ���� B���!F��CE� DE� -���� 9+�(/:A� (EBC� �E��C�� C��F�E������
����!!E��� ����� BE���C��� -�B�E���� �E��� ��E� �E�� -�B�E���� ��FB�BE�� DE� DF8E����E!E���
E�D�B�C�EA� 5�� �E��� ���� E�E!��E� !E���E� E�� ���BE� ��� �����B��E� D@C�BEB�C���=� D����
DC--F�E����'�E--����>�DE�� ���DE����FBC�=�D@�DF��8C��������������� �����'<�E�*+������� �E�
B����P�E�D�����!��E���*7A����<���;�=� ��� DC���BC��C���D�����B�F��� E�� �E� �����'E� ���
+�(/�DE���������C���!���BE�����C�E�DE8��C���E�!E���E�D@C���E���E��BE����E��*+�[X*7[A�
(E� ���E� D@�����B�E� �E�!E����C�� D@C���E�� BE�� BE����E�� >� DC--F�E���� ���DE�� DE�
DF8E����E!E���E��D@F��DCE������E�E!��E��@F8����C���DE��E��������B�C���!E�������������>�
���B�������'CE�DF8E����E!E����EA�)�����D���F���@C����F�F�!����F�B�E0��������C����E�BE��
BE����E�� F��CE��� DE�� ���'F�C�E���� ��C���E���� ��FDE��C�F�� 9���B�C'� ��� ��� *�$$�=� � �//'=�
Development:=� ���� DE�� !FB��C�!E�� E�B��E� C�B�����=� >� D���E�� ��E� �E��E� BE����E�
E�D�B�C�E=� BE� ���E� D@�����B�E� ������C�� �E�!E���E� D@�8��BE�� D���� BE� D�!�C�E� B�E0�
�@#�!!E� E�� DF�E�!C����� ��E��� ����� �E�� -�B�E���� ��C� C�D�C�E��� �E� B��C�� D�� �C'��'E�
E�D�B�C�EA�3�E�����E���C�C���C�������C��E�DE���DF��8C�����E��C��D@E����E��DE��F��C�E��DE�
��� �����DC--F�E�BC��C��� � BE�����C�E� AB��A��� � D���� �E�� '�E--������!�C��A� � )�� E--E�=� c���� E��
B���<'�E�� 9J���� K�� ��� *�$$�=� � �//-=� Nature:� ���� DF!����F� ��� ����C�C�C�F� DE�
�����DC--F�E�BCE�� DE�� BE����E�� �BC��C�E�� E�� BE����E�� β� ���� C�BEB�C���� D@��� B�B1��C��
�DF��8C���� ���������� �E�� -�B�E����DE� �����B�C��C���'�7=��D���E��&�-�=� AB��A��=� D���� �E�
���B�F���DE�����C���D���E�A������BE� ���8�C�=� �E�����E�������CE��E��=�>�����C��DE�BE����E��
�BC��C�E�� !����E�=� DE�� BE����E�� β� E���C!���� DE�� ����FC�E�� DE� !����C�F� DE� BE� ���E�
BE�����C�E�E�����D�C���������!!E���DE��@C����C�E�>�DE���C8E����CDE��C��E��>�BE��C�DE��β�
DE��T����A�(E��E�E��F�CE�BE���''<�E���E�����FE���E��C���DE�'<�E��E!�������C�E��D�����E�

��GG���
���B�F����E����E�!E���E�DE��E���'��!!E��DE��BE����E��DC--F�E�BCFE�A�(�E0��@#�!!E=�BE�
���E�DE�DF!��B�E��E��C����E������B�E���<��C���8���E�E������������C�E�C����E����E��DE�
DF!����E���C�BE����E�D@E��F�CE�BE�E����E���D�B�C��E�D����DE��'�E--������!�C���AB��A��A��
�
�
�
��
%D�*�D*$��A�DE�D����������D��C��A��C�������$���C�B���D���D�*���CA���������
��B��� � ��� $LAD���M�� ��� *�� D����C�� ���,$�� ����� $L������ ��� ����$������D��
�CD*��C�A ��� ��� ��� ���� ����D�A�$$��� C��$A*C�A�D�� *$ADA ���� �CD�� $C� ����C�A��
*�$$�$CA�������AC",����9���� ����CA��D��������A���� *�� ��C�CA$� �D� C����+�D�A��CD��
$����A++���D����������*�A�����&����������������D��CAD�A��*�D�AD�����LC�B��D����$C�
��DDCA��CD*�� ���� ��*CDA����� ����A�CD�� N� $C� ����AD��� ���� �A++���D��� $ABDCB���
�CD*��C�A ������
�
�
�
��������
������FE��B�F��$���F����%�D�EB�E��$��&���E�DE���B�������E���CC�����E�'���E��B����DE�����F(� �
)E�*F������F�)E�*F������F�)E�*F������F�)E�*F������F������
�

��G4���
���(��#��#��
)�)���*� %+�,�#��

��4H���
�-���=/A=�/E!E�EB=$A=�(��=CA/A=���D�(�E�=A�9�HHG:A�.DE��C-CB��C�����D�B����B�E�C0��C����-���8E����!����C���E���EBC-CB��+ ������B�C��C���-�B����A�%&(A�)8��A�%C��A�D=���FA�
���E�=$A=�#C��=CA"A=�*����=/A=�&�'�����=&A�A=���D�/���E�=$A�9�H��:A�*��E�C��E���E��C���C����E�!���E����B�E���DE-C�E������C��E�!���C���E������'E�C�����������C��A��$�/A�5�EA�E=�EE�H�FA�
����E�=.A=�$E�$��=CA=�#��'=6A=�)�'��0C=$A=�/B�C��E�=CA(A=�#E�DE����=)A=�/�����C�ED�=%A=���D�/�EC�=�A�9�HHF:A�&�-%A�����B�C8������-���E�'��B�'���'E�E�E���E��ED�C��DE8E���C�'�C��E�����������D��E���BE���A��C��E�E��88=��4Q�7H;A�
�����C=&A=�/�E����1=DA=�%��!�BC�'�����C=�A=��CE���=DA=�c�����%����C-=&A�A=���8C��CE=%A=���D�/B���-!���=�A�9�HHQ:A�(��������-��E���BE���DC--E�E��C��C��������E����B�E��CB�!E�E�B��!EA��C��E�E��8:=���;G���EGA�
%E��5��!��=A=�(�����E�=&A=�DCEC��=�A=��-EC-E�=�A=����E��E=A=�*BE��E�=)A=�+���C�E=%A=��8��C�=+A=���D�(����!���=�A�9�H�7:A�+��!����B�E��CB�C��E��-��!��C�������E���BE����E'E�E���C��A��C��E�E���E�A�(�C�A����B�A�
%���'�8�=�A=�/E�C��=�A�A=��B1E�!��="A)A=�����=)A�A=�����=%ALA=�$�1E�=CA�A=���D�/���C��=�A&A�9�HH;:A���E8��E�BE��-��E���CB���E����C���-�E��C��E��������������C�����D�C����E���C������'��-��-��B�C��A��C��E�E��8@=��7����7�QA�
%������=�A=�.���=A=�2���=/A=�"�CE��=CA�A=�(0E��CB��,=�A=�%E����BC=/A=���D�/B���-!���=�A�9�HH�:A�+'-�H�C��E��E��C���-���!�C���C�C�'���E�����C-E���C8E�B���BC����-�E�C��E�C������'E�C����BE����D��C�'�E��������B�E��CB���'���'E�E�C�A��E8E���!E���1FD=�E�H4�E��QA�
%���E-��D=�A=�D�C�����=)A=���C�C��E=CA=�/1���E1=%A=�$���E��=/A=�6E�'�=$A=�#��8�E��=&A=�(�8E=#A=�%��C��=2A=�/B���-!���=�A=�����1=&A=���D���������=&A=�+��'�E�=�A=���D�D��C���C�E=&A�9�H�7:A�"����B�C��C���-�B����'E�E�& ��C������8E��B���E��-��E�!��E����E�������DC��E�E��C����B�����'�C�E����-�!C��A��C��E�E��&E���A�
(���E��=5A=�%E�!��=�A&A=�2E����=A/A=��CB��DC=(A=�%E�''�E�=�A5A=���D�(�CBED�=�A�9�HHF:A�"�E���C��E�B�����B�C�EB���E��-���!������B�E��CB�C��E�������C!��CB��C����-���C��E��BE���-��B�C��A����BA����A��B�DA�/BCA�3A�/A���1=@=��77;��774A�
(����C�'=&A=���8C��CE=%A=�a�E!E�E��=)A=�%��!�BC�'�����C=�A=���D�/B���-!���=�A�9�HHE:A�)��8C8��������C���-��BC������D�E�D�B�C�E�BE���DE8E���!E���C����E���!���E!�����CB����B�E��A��E8A����A�F@.=�774�7;EA�
(����C�'=&A=�*�E�BC=�A=�&���E�=CA=�(0E��CB��,=�A=���8�����D=�A=���D�/B���-!���=�A�9�HHE:A�)--CBCE����E���CB�ED�'E�E�E���E��C���C���E���BE��������E��C8C����!EDC��ED�'E�E������-E��C�������B�E��CB���E!X���'E�C����BE���A��C��E����'C��.D=�QH4�Q�4A�
(����C�'=&A=��E����=%A=�%��!�BC�'�����C=�A=�(����=.A=�(0E��CB��,=�A=���D�/B���-!���=�A�9�HH�:A�%���D�'��B��E����!��C0��C��������������������C����-���!���E!�����CB����B�E���C�����E���BE���DE-CBCE���/(.��!CBEA��C��E����'C��..=��HFF��HQFA�

��4����
(��C���--E�����=*A=�#E��C1����=CA=�C��������=$A=������=(A=��������!=#A=�(�����E���(�������=CA=�/E'E��8��D=�A=��E�!E��=CA=�2���'�E�=5A=�(�������=�A5A=���D���C��C����=&A�9�H�H:A�(�C�CB�����D�E��E�C!E��������B�E��CB�C��E��������������C���������C��ED�!��B�EA�E�����C��!E����-���8��B���������E!��C!C������������C�����C8E�C��E��A��C��E�E��8<=��EF4��EQGA�
(�E8E���D=&A#A=�/�,�E�=CA&A=��-E�C1=/A=�CE��E�=CA=���D�$E�B�=/A�A�9�H��:A�)��B�C�E�����'E�CE�A������E�DE8E���!E����-����B�E��CB��BC���=�D�B������D�BE�����BC����BE���A�/E!C�A�(E����E8A�%C��A�F@=�Q���Q�4A�
(�E����E=(A=��E�E�=�A=�/����8C��E=�A=�cE���=&A=��!CE�=CA=�C���E��=+A=��E8C����=6A=�%����=$A=�&���CB�=�A=�C�����+E1E�E=(A=���D�$����E�=/A�9�HHG:A�/�EB���!��-�#$ %4�'E�E�!����C����C��(�����C������D��!E���D�'E�����E���E�����E�B���E���C��A�#�!A�&����A�F<=�4H7�4�HA�
(�E����E=(A=�cE���=&A=�C���E��=+A=�/����B1C=/A=��E8C����=6A=�$����E�=/A=���D�C�����+E1E�E=(A�9�HHF:A�E,�B�C�CB�����D���E���E��CB��E���EB�C8E��C��(�����C������D��!E�9���D���-��4�B��E�:A�CA��EDC���A�/��'A�.1=���F��7�A�
�S�!���=2A�A=��'���CB1=�A�A=�)�C�0E�=/A=�2E���=5A*A=�2����=)A=���D�%�E�'E=)A)A�9�HHE:A�)--CBCE���DC--E�E��C��C����-���!���E!�����CB���E!�BE�������DE-C�C�C8E�E�D�DE�!A���A�%C��EB����A�F@=��E7;��E;�A�
�S�!���=2A�A=�%��'=�A*A=�)�C�0E�=/A=�2E���=5A*A=��'���CB1=�A�A=�/!���=A*A=�&���!��=&A�A=�2����=)A=�(���E��E�=&A2A=���D�%�E�'E=)A)A�9�HHF:A����D�B�C����-����B�E��CB����!��E�E���E��C�'�E�D�B�C�E�BE����-��!���!���E!�����CB���E!�BE���A���A�%C��EB����A�F.=��74���;H�A�
��8���C=�A&A=�5'�,�=6A=��CB��DC=(A=�/B����=�ALA=�%���E��LEC�=/A=���D�LEC�=*A(A�9�44E:A����E�EB�C8E�DEB�E��E�C����E��E���BE���!�����-���!���C��E�������������ED�C����DC��E�CB���DE�!CBEA�"�����������C���8<=�G�Q�G�HA�
�E�'��0=�A���D�#E��E��=�A$A�9�HH4:A����B�E��CB��E���'E�C��7�E���E��C�'�BE������E���C���E���C��E����EB������A��E8E���!E���1@:=�7EFQ�7EQ;A�
�E���B�=*A=�C��'=CA=�c�E�'=&A=�$���=CA=���D�c��E�=2A/A�9�HH�:A����C���E��C�����EB�������������C���-������B�E�����D��C8E��,C��C����E�E!�����CB�E�D�DE�!A��E8E���!E���1FD=�GQ��GG�A�
��!���,�1C=+A=�&���CE�=(A=���D�)8E��=&A�9�HHF:A�#E����BE��������E�����!��C�D�BED������,���!�E�����B�E��CB�C��E��������������C������C!!��E�DC��E�CB�%%X�-D�����A�(��BE���E�A�::=��G77��G;7A�
���=6A=�%��,�=CA=�&���C�E0=5A.A=���D�&E����=�A�A�9�HH;:A��D�������B�E��CB��E���BE������E�-��!ED�����E�-�D���CB��C�������E���������E!�BE���DC--E�E��C��C��A�����E�.F<=�;��;FA�

��4����
����E��=(A=�/B��'=CA=�$C�=(A+A=�(���D��=�A/A=�+��=�ACA=�/!C���8�=5A=�%�����=�A=�/��EE�E�=�A�A=�/��EB1E��=(ACA=�C�A=�2�E���E�=2A#A=���D�*��!�E=&A�9�H��:A�"����B�C���!E���-���E�!�B�����!������B�E��CB�BE������E�A��C��E����'C��8.=��G7���G;;A�
)�'��0C=$A=�(����&E�E��=(A=�(0E��CB��,=�A=���D�/B���-!���=�A�9�HH�:A����E�-���+*+��...��!EDC��ED��C'�����C��B�������C�'����B�E��CB�E�D�B�C�E����'E�C����BE�������C-E���C��A����BA����A��B�DA�/BCA�3A�/A���<<=�7GG;�7GG4A�
)��C=+A=�*����=%A=�%C��1C�=�ADA=�$C�=CALA=����E��=&A�A=�6�= A=�&�B�����D=�ACA=�(C8C�=(A.A=��E��=+A A=���B1=&A�A=�%���=�ALA=���D�$E�B�=/A�A�9�HH;:A���B��C��C�C�����-��-��B�C�����D��BC����BE���DC--E�E��C��C���C��DE8E���C�'�!���E���D�0E���-C������B�E��A��E8E���!E���1@1=�;��7�;��;A�
*��D,���=*A=��CE�CB�=�A=�$E&E��=&A=���D�*�C��E!��=+A�9�HHH:A��E���'E�C�7�C���E��C�ED�-�����E�DE8E���!E����-���E�-����E�D�B�C�E�BE����C�E�'E���-���E����B�E��A����BA����A��B�DA�/BCA�3A�/A���<E=��FHQ��F��A�
*�=*A=�������1�C�E=CA=���D�&E����=�A�A�9�HH�:A��C�EB��E8CDE�BE�-�����E����B�E��CB��C�E�'EA�*7[�BE������E�C��E�����'E�C�������D���E�DC��C�B��-��!�D�B�����'E�C����A��E8E���!E���1F<=��;;Q��;EQA�
#E���1=&A=�2C!=/A2A=���D�&E����=�A�A�9�44G:A����B���D��E��E��C����-�E�D�DE�!���/��CB��ED'E��'��E�!C������B�E���DE8E���!E��A�*E�E���E8A�1F=��QHE��Q�7A�
#EC!�E�'=#A=�%��,E��=$A=�#E�E!���=6A=�D����E=(A&A=�$E-E�8�E=DA=���D��C�E�EE��=�A�9�HHH:A��D������!������B�E��CB�D�B����D�C��E��BE����E��C�C���C!C���C�CE��C��E���E��C�����D�DC--E�E�BE��C��������������C�����D�B�!��E��-��!��C����-���E���!E�D�!�C������EC��.�-��A��C��E�E��.<=�EQ��EQ4A�
#E��E�EC�=2A�A=�E����=/A%A=�2������D�=2A=�#E��C�'�=CA(A=�)�CB���=CA=���D�/��DE�=&A�9�HHE:A�2 F������B�C��C���-�B�����B�C8C���C���E��C�ED�-������������D��E���BE���DE8E���!E���C����E����B�E��A��E8E���!E���1@F=�7�74�7�;4A�
#E��E��=�A$A�9�HHH:A��D����C����C�����D�'��B�'������D�BC�'�BE����DC--E�E��C��E�-��!��,��C�DE�E�DE���BE����C�E�'E�A��E8E���!E���1FE=��7�Q��7��A�
.��D�=�A=�CE���E�=(A=�2������=#A=�+�BC���C=6A=�$E8C�E=CA=�&��C��=�A=�/���!�=�A=���D�%���E��LEC�=/A�9�HHG:A�(�����CB�����D���E�..����C�C8E����B�E��CB�BE������E����'E�C�����-��������E�D�B�C�E���D�E��B�C�E����B�E����-�E���C���A����BA����A��B�DA�/BCA�3A�/A���1=8=��44�E��44�4A�
CC!E�E0=DA=������=)A=�&�����=(A=��'�D�=CA=�(��E����=�A=�5��B�=&A=�&���0=/A=�/���8E��=�A=���D�%��B�=+A�9�H���:A�.��8C8��'E�E�CB�E�'C�EE�C�'��-�!��C�E����B�E��CB��E���BE����!EDC��ED�����C�'�E������DED��DE�������BC��ED�8C����8EB������-��E�����E��F=�G���D�4A��C��E����'C��8.=��HQE��HGFA�

��47���
C��������=2A�A=�������=3A=�C��D��=A=�*�=*A=�%EE�!���=+A=�*��D,���=*A=���D�*���C��%�����=�A�9�HHQ:A�"E!������B��������-��E���'E�C�7��B�C8C���C�����B�E������'E�C������E8E����B�!�E�E�BE�,C�D�,��-�����E�'E�E���C����-�DC--E�E���E�D�B�C�E�BE������E�A��E8A�(E���1F=�;EQ�;FEA�
C������=CA=�(�������=$A=�)D���D="A=���D�)D���D=#A�9�44;:A�.����C�����!��E��-�B������C���E��C�ED�-������B�E���DE8E���!E���C��!CBEA�����E�@E1=�FHF�FH4A�
2���E!=/A�A=���CE�=.A=�"�������=�A/A=�/B�EC!�E�'=.A=���D�*���E�=%A�9�HHH:A�%E���BE�������C-E���C�����D��������C��C����E�DE8E���C�'����!�����!������B�E�����D�C�����E�C����C�C�!��-�C�-��B�A��C��E�E��.<=��7�E��777A�
2�,�'�B�C=6A=�(���E�=%A=�*�����=&A=����=&A=�&�B�����D=�ACA=���D�L�C'��=(ADA�9�HH�:A�"�E����E��-���E������B�C��C������E'���������-���C��B��8E��C�'�C��E��C����������B�E��CB����'E�C����A���A�*E�E�A�@F=���G��7;A�
2ECB0E�=�A=�8���"���=&A=�&ECBE��=(A=�����=&A=�"C���E�=�A=�*���8E�D=+A=���D�2��������1C�=&A�9�HH�:A�"�E������B�C��C���-�B����*�"�F�C��E��E��C���-�������B�C�'�!�����'E�E�C����D�E�C��E�C���BE���DC--E�E��C��C���D��C�'�-E�������!������DE8E���!E��A��E8E���!E���1FD=�EH7�E��A�
2E�!E��E�=%A=�$C�'=cA=�*����=+A2A=��E�8���=*A=�%��,E��=$A=�*����C�'=�A=�#E�D�CEB1�=(A=��C�E�EE���&��CB���=&A=�D���/B���8E�DCB1=(A=�/��!E��=2A=���D��C�E�EE��=�A*A�9�44G:A�.!�������C����-�����D��DC0ED��E���BE���'��-���C�����C8E���E'!E����-�.��&����CE���A�'��-����D��EBC�CE����B����B�E�C��CB��C���,��B��E���-�C����C��C�DE�E�DE�BE���DE��!�C��E���BE�C!!��������E��C���-�����C���1CD�E��'��-�A��C��E����'C��.1=�;E��;E4A�
2C!=/A2A���D�&E����=�A�A�9�44G:A����B�E���DE8E���!E���C�����!��ED����B�B����!C�E=����ED'E��'��C'���C�'�C��C�C���A����BA����A��B�DA�/BCA�3A�/A���<8=��7H7F��7H;�A�
2���'�E�=5A=�$��D'�E�="A=�+E��DC�=&A=�+���=�A=�.��1����=%A=��E�!E��=CA=��E�����=A#A=���-�E�=)A=���DE�=&A=�/��!E��=2A=�"C�E��=�A=�"�-8E���=*A=���D�C�����=%A�9�HHG:A�5��C!C�C�'�C��E��E�'��-�!E���C��B�C�CB���-�����BBE��-���B�C�CB���C��E��������������C��A��C��E����'C��81=���Q��7�A�
2����=)A=�&���C����=$A�A=�2�D���=2A=�%��'=�A*A=�2E���=5A*A=�)�C�0E�=/A=�6���'=#A=��CB���D���=&A=�/!���=A*A=�(���C�'��!=CA=��'���CB1=�A�A=��S�!���=2A�A=�(���E��E�=&A2A=���D�%�E�'E=)A)A�9�HHG:A����B�E��CB�E�D�DE�!�DE�C8ED�-��!���!���E!�����CB���E!�BE����'E�E���E��'��B��E��E�����C8E�C����C���EB�E�C�'�BE����C��8C8�A���A�%C��EB����A�F:=�;;7�;E�A�
2��1���C=�AA=�&C0��B�C=)A%A=�5B���=�A*A=���D�/�E,���=�A+A�9�H��:A�#�!����E���BE�������C-E���C�����D�C����BE��������C'���C�'A�D�C8C�'�C����E�D��1�,C�����������D�!��A��C��E�E��:1=���HE����7A�

��4;���
2��=(A"A=�&���C�E�=)A)A=�����D����=�A=�/C'�C��=2A=�$�=&A&A=����!�BE1=&A/A=�/��D�C�=(A=���D�$ECDE�=CA&A�9�44Q:A�*�"�;������B�C��C���-�B����C���E��C�ED�-���8E������!�����'E�E�C����D��E�������E�-��!��C��A�*E�E���E8A�11=��H;G��HFHA�
$�!!E��=)A=�(�E�8E�=5A=���D�&E����=�A�9�HH�:A�.�D�B�C����-����B�E��CB�DC--E�E��C��C�������C'�����-��!�����D�8E��E��A�/BCE�BE�F<.=�EF;�EFQA�
$��'�=�A#A=�+����'��=/A)A=�/��,�/!C��=(A=��E�+���B�=)A=��1E�!��=.A=�(��,E��=�A=�+E��E�=CA=�#���E���E�=�A"A=���D�)����D=/A�9�H��:A�*�"�F������C���--CBCE�B��B���E�����B�E��CB��'E�E�C��C����!���A���A�*E�E�A�..=��H���A�
$E����D=CA=��EE��=%A=�C������="A=�+E��E�C=2A=�$EE=/A=���D�&���!C��=&A�A�9�447:A�(����B�E�C0��C����-���!�������C��������B�C8��C�'�-�B�����=�����8E����!E�����-�B�����������C!����E����!�������C��E���E��C���C�����B�E��CB�C��E��BE���A�&��A�)�D�B�C���A�E=���QE���G7A�
$C=#A=����E�=/A=�CE��E��="A&A=���D�)D���D=#A�9�444:A�/E�EB�C8E��'E�E�C���-���E�D���������B�E���C��!CBE���B1C�'���!E�����'E�E�#���4A���A�*E�E�A�F@=�FQ�QHA�
$C�=6A=�&�B�����D=�ACA=���D�/,C-�=*A#A�9�HH�:A�����C�DC�'���D������B�C��C������B�C8��C���������� �A�% ��A&)./�����C!E����D�B���E���C���,C��������B�E�����EBC-CB����CB��E�C��������E�C��B�!��E�A�CA�%C��A�(�E!A�FE:=��Q4GE��Q447A�
$���=+A(A=�/!C��=/A%A=�LC����=&A)A=�6��'=2A6A=�E1�E�=A=���D�*E�!��=&A/A�9�HHQ:A�/��4�B���DC���E���������B�C��C������E�,��1�C�����B�E��CB����'E�C����BE���A����BA����A��B�DA�/BCA�3A�/A���1=.=��HEHH��HEHEA�
&�������=*A=�C������=$A=���D�(�������=�A5A�9�HH�:A��EB�E��ED�8��B�����DE��C���C��!���E����B�E��CB�C��E����-�E��������������C��A��C��E�E��81=��7F���7FFA�
&ECE�=CACA=�%���E�=�A)A=�/�C���=6A=�&��B��!�="A=�*������=�A=�%������=�A=��C00�=�A�A=���D�%���E�=�A(A�9�HHG:A�%E���BE����E��CB��C���C����E���C!����!EB���C�!�����E�8C�'���E�����������E�����C����-��E���BE���!����C����!���A��C��E�E��8E=��EG;��E4;A�
&C��E�=(A�A=�&B*E�EE=�A)A=�C�A=���D�#��E�E�=CA+A�9�44;:A�.� ��A����E,���!E�D�!�C�������B�C��C���-�B����E���E��ED�C���������B�E��CB�C��E�����D�D��DE��!������������B�C8��E����E���!�������C��'E�EA�)&%5�CA�1@=���;E���EFA�
&C����E�=+A=�%���E�C��="A=�(0E��CB��,=�A=���D�/B���-!���=�A�9�44G:A�"*+��E�����������1E�����E�C��!�����'E�E�C���-���E����B�E��CB�C��E����-�$��'E���������B�������C�'���E��B�C8C����-���E�!���C��!E���������EC���E�&&���A�CA�(E���%C��A�1.@=�G�Q�G7FA�
&C����E�=+A=�(0E��CB��,=�A=�50�1C=2A=�.���=A=���D�/B���-!���=�A�9�444�:A�/C'���C�'������'��-C���������'��,���-�B�����EBE����������������1E�����E�C����E�DE8E���!E����-���E�E��B�C�E����B�E��A����BA����A��B�DA�/BCA�3A�/A���<:=�F�FQ�F�Q�A�

��4E���
&C����E�=+A=�$�!���E=$A=�(�����=�A=���D�C���C=�A$A�9�HHF:A�.��E�������E�,EE��+*+�H���D���B���C'����C�'�C���E��C�ED�-�����E��E�-��E�E,����-����B�E��CB����'E�C����A�.��A�CA��E8A�%C��A�8==��Q��FA�
&��E�'=$A=�C��������=#A=�$�1C�C��=�A=�%E��E=(A=�+���=�A=�2���E�=�A=�5������=5A=�/��!E��=2A=�"C�E��=�A=�"�-8E���=*A=�)�'�E=*A=�C�����=)A2A=�2���'�E�=5A=���D�C�����=%A�9�HH�:A����D�B�C����-��C���E�-�B����������B�E��CB�C��E��BE�����������C''E���-�DE��C!E���������!���CB��E�B�C����C��B�C�CB���C��E��������������C��A�$��BE��@:==��H74��H;EA�
&������=)A=�%���E��LEC�=/A=���D�LEC�=*A(A�9�447:A�%E���BE���!������D�'��,����-�E�����'E�ECB�C��E��BE���������������C���C�����!�����D����E���0�BC��DC��E�CB�(EQ%$XF�!CBEA�CA�(�C�A�.�8E���<1=�QGH�QGQA�
&�����'�=$A(A=�/���'E�=%AcA=�2,��=2A&A=���D�&E����=�A�A�9�HH7:A���B���C'���C�'�B��������!���C��E���E����-����B�E��CB�DC--E�E��C��C��A����BA����A��B�DA�/BCA�3A�/A���1===��;4�H��;4�EA�
�B��C��=CA/A=�/���E����D=�A)A=�&����=�ACA=�/�E--E�=&ALA=�/C!!���=�A$A=���D�*�E�0=+A(A�9�4QQ:A�#�!���C��E��������������C��A�����E�C!C������E����A�"���������A����BA�<=��77��7FA�
5������=#A=�2�������=2A=���D�)D���D="A�9�447:A�.�+�=�����!E�D�!�C��B����C�C�'�������B�C8������-���E�C����C��'E�EA�)&%5�CA�1F=�;�E��;�E4A�
5�C8E��2���C��1C=CA&A���D�/��--E��=�A�A�9�HHG:A�5����E���C'C���-���E��E���BE��A�*E�E���E8A�FF=��44G��H��A�
���C0��=CA%A=�/C�'E�=�A�A=�"�B�E�=/A.A=����,��=/A=�+�CE�=CA&A=�#C�1E��=/A%A=�&�'�����=&A�A=�%������=�A=���D�/���E�=$A�9�H��:A�1��A���E��E�����B�!��E���E'����E��C��E���E���BE�����EBC-CB��C�����D���E8E�����E������������BE����E���'��!!C�'A�*E�E���E8A�F8=���4���7HEA�
������=+A=�2E���(���E=CA=���D�LC�D=�A�9�H�H:A�*$�����EBE������B���C�'�-���C!�'C�'��-���!����E���BE��������������ED�C��!��B�EA�A�)�'�A�CA�&EDA�@:@=���G4���4HA�
�CB�E�=�A$A=�(���1=LA�A=�LC��C�!�=�A#A=���D�����E�=LACA�9�4Q�:A�������������B������������C���-���E�DE8E���C�'�E!�����CB����B�E��A��E8A�%C��A�F<=�;7F�;FQA�
�C��E�=/A)A=�5�C8E��2���C��1C=CA=�)����=$A=�#�'�E�=A=����E�=�A=�/��--E��=�A�A=������=�A=���D��E�$E��=�A�A�9�H��:A�E�������DC��E�E����D�B��'E�C����!���������C8E�DC����E������C������E��������8E��!����C���C����E���!����E���'E�C��7�'E�E�B�DC�'��E��E�BEA�CA�(�C�A�)�D�B�C���A�&E����<:=��4FH��4FEA�
����1=&A=�%��B���E��%���EC=$A=�/B���-!���=�A=���D�(0E��CB��,=�A�9�HHH�:A�)���������E����-�DC--E�E��C��C���C����E���!������B�E��A��C��E�E��.<=���E��7�A�

��4F���
���D�=(A$A=���'��%E����D=�A)A=�)�'��0C=$A=�/�����C�ED�=%A=���D�/���E�=$A�9�HH;:A�*��E�C��BE�����E���BE�C����C�����D�BC�'��E���BE����C���,��!���E�!�DE����-����B�E���DE8E���!E��A����BA����A��B�DA�/BCA�3A�/A���1=1=��4�;��4�4A�
��-�E�=)A=�"C�E��=�A=���DE�=&A=�$��D'�E�="A=�/�8E�D���=$A=�%��'����!=%A=����E��=3A=�.��1����=%A=�C�����=%A=�2���'�E�=5A=���D��E�!E��=CA�9�HHG:A�.����!��B���������������������C����-����B�E��CB�C��E���C����Q��E�����D�B�C�DA������E���-����,���A��!A�CA�"���������A�D=�;EG�;F�A�
��'���=2A=�*���E'�=�A=�/B��0EB=CA6A=�*��BC��(�����E��="A=���D�&��E�=*A�9�H�7:A��C--E�E���'��E�C����B��C���C���C���D������!�����D�����E�D�B�C�E����B�E��A�(E���"C���E��E�A�
����E�=2A.A���D�#�����=�A&A�9�HH;:A�(����E�'E��-�BC�'�C��E��������������C���-�����E���E��!E����-����E���DC��E�E��!E��C���A�CA�(�C�A�.�8E���11.=�GQQ�GG7A�
���C��(��E0��=5A=�CE��E�=CAA=�#�D'���=&A.A=�(�D�E�=)A=�)����D=/A=�/E���=�A=���D�#���E���E�=�A"A�9�H��:A��E�!��E���E��������C��E�E����D�)��E�CB���E�D�B�C���C������BC��ED�LC���%C���E�CB�&����C����C��)3�5*7A��C��E�E��:==��7;4��7E7A�
/B��--E�=�A)A=�"�����=%A$A=�%E������E�=CA�A=�$C�=CA=�"���E�=+A=�6���=LA=�CC��=6A=�2�E���E�=2A#A=�#E��E��=�A$A=�&�'�����=&A�A=�&��=(A$A=���D�/��DE�=&A�9�H�7:A�1�FA��B����������'E�E��E'���������E�,��1��E��C�ED�-���E�����C��C�'���D�!�C���C�C�'����B�E��CB�%E���BE���CDE��C��A��$�/A�*E�E�A�<=�E�HH7�Q;A�
/B���-!���=�A=� C��= A=�#EC!�E�'=#A=�&���E�=CA=���D���8�����D=�A�9�HHG:A�%E���BE����,C��C���C�'�E���!���C��E�����C'C���E�-��!�!���C��E����'E�C����A��$�/A�5�EA�@=�E7EE4A�
/B�,C�0'E�E�=DA&A=�/B�EE�=�ALA=�(���E��=CA�A=�2���!����=CA=�$EE=CA)A=���DE����=�ACA=�/���E�=$A=�C������=CA�A=���D�*E�!��=&A/A�9�HHH:A�)���E��C����-��E���'E�C�7��E8E�������C��E��BE�����EB�������������C���C����E����B�E��A��E8E���!E���1FE=�7E77�7E;�A�
/E��CB1=*A/A=�%��1E�=2A"A=�/����E��CB1����=.A=�+�EC�B�!���=(A=�(��E!��=�ACA=�*���E��=(A=�*����=�A$A=�)D'�C��=)A$A=�#���E���E�=�A"A=�LE����E�=�A2A=�*��D,C�=*A=���D�#�������=�A/A�9�HH;:A�&����C����C���"+���B���E����B�E��CB���D�BE�E�E������'E�E�C�A���A�*E�E�A�@:=��7H���7HEA�
/E�!���=�A�A=�+�E�DE=2A2A=�"���=&AA=�&��E�=)A)A=�CE��E�=CA=�2C��=�A=�/B�E�E�=*A=���D�/��DE�=&A�9�HHQ:A�/5 4�C���E��C�ED�-���!�C��E���BE��-���E����B�E��CB����'E�C����BE�������A����BA����A��B�DA�/BCA�3A�/A���1=.=��GFE��GQHA�
/���C��=�A&A���D�$�1E�=CA�A�9�HHH:A�+����E���E�D��C��C��E��BE���������������C��A��C��E�E��"EB����A�"�E�A�F=�;;4�;E�A�
/���C��=�A&A=�$�1E�=CA�A=�����=)A�A=�2������=*A/A=�"���=)A=�L����B1=*A$A=�2�E�E!��=A&A=���D���B���E=�ADA�9�HHH:A�.��E��������������C���C���E8E�����CE����,C������E���DC��E�E��

��4Q���
!E��C������C�'���'��B�B���CB�CD�-�EE�C!!��������E��C8E��E'C!E�A�A�)�'�A�CA�&EDA�@.@=��7H��7GA�
/���C��=�A&A=��CB��DC=(A=�#E�C�'=%ACA=���B�C�B����=#A=�$C�D���D=�A=����E�����=�A�A=�/EBB�C=�A=�%�E�DE�=&A�A=�%E��E�="A=�%�E����=�A(A=�(�'�CE��=)A=���EB��D��=�A=�����=)A�A=��C&E�B��C�=%A=�&��E�=�A=�������1�=2A/A=��EE!�=CA�A=�%�E�0E�=�A*A=�%E���00C=+A=�+���D="A=�2��D��,�!�=�A=�/���E����D=�A)A=�)C�E������=*A=�/E'��=&A=���EC1��C�C�=CA=�2������=*A/A=�%�����=+A%A=�DC8C���=$A=�/E�-E���&��'��C�=DA=�%��E����E=CA=���D�$�1E�=CA�A�9�HHF:A�.��E����C�������C����-���E�)D!�����������B���-���C��E��������������C��A�A�)�'�A�CA�&EDA�@88=��7�G��77HA�
/!C��=/A%A=�a�=#AaA=�"��E�=A=�2C��C!���=A6A=�/B�EE�=�ALA=�$�=6A=����B�=�A&A=�*����=�A=�L��'=CA=�$���=+A(A=�&C�����1�="A=�&C�B�E��=CA=�/EE�1E=�A=��E�C�=CA=�D��DE��)CB�DE�=/A=�����!�,CB0=&A=�2�BE�=A=�LEC��=CA=��E���D=&A)A=�*E��C�E=&A=�#���E�=.A=��E,��=2A=�#���E���E�=�A"A=�L��'=�A=�LC����=&A)A=�C������=CA�A=�����B�����1��=(A=���D�*E�!��=&A/A�9�H�H:A��-�F�DC�EB���C��E��-��!��C�����D�C����C�����D�B�C���C��!CBE���D���!���A�����E�.:@=�QQE�QGHA�
/��--E��=�A�A=�+E��E�=CA=�(���1E=LA$A=���D�#��E�E�=CA+A�9�44Q:A�)��������E�����E�..�DC��E�E��!E��C����9&5�6;:��C�1ED����.�+�A���A�*E�E�A�1E=��7G��74A�
/��--E��=�A�A=�cC�1C�=A"A=�/����BE8CB=DA=�(���1E=LA$A=���D�#��E�E�=CA+A�9�44Q�:A����B�E��CB��'E�E�C������C������E�������C�'�E���B�E��CDE�DE�E�C���C����E���!���.�+��'E�E�B�DC�'��E��E�BEA���A�*E�E�A�18=��HF���HA�
/���E�=$A=�2���!����=CA=�#���C'���5S(�����=�ACA=�&E�E�E�=CACA=��EDE��E�=�A�A=����E���EC�=CA$A=���D�*E�!��=&A/A�9�44G:A�&CBE���B1C�'���E���!E�D�!�C�������B�C��C���-�B����1��A����8E�DC��E�E��D�E�������E��ED�DC--E�E��C��C����-����B�E��CB��E���BE���A��E8E���!E���1F8=����7�����A�
"��!����=A=�*E�C��=)A=�/B�EC�E��=�A=�%�B�E�=�A=���D�*���C��%�����=�A�9�H��:A�������-C�C�'���D�B���!��C��C!!�����EBC�C���C����E��E�BC�'��E8E���������"+�������C�C0E�����B�E������'E�C����CDE��C���8C����E�B��������-�& �X#$ %4���D����E�,��1��-����E�������B�C��C���-�B����A�&��A�(E���%C��A�@F=���G4���44A�
"�B�=%A)A=�'=�A%A=�C��E�=�A=���D�"����E=CA�A�9�4G;:A�#C�����'CB�DC--E�E��C��C����-���!���-E�������B�E��CB�E������������������ED�C������DE�!CBEA��C��E�E��@@=���GH���GQA�
"�B�=%A)A=�5�'E���=2ACA=���D�"����E=CA�A�9�4GG:A���!��C0��C����-�����D�'��B��E��E8E���C�����DC��E�CB���DE�!CBE������!���-E�������B�E����-�E��C�D�B�C����-�DC��E�E�A�"�����������C���.:=�FHG�F��A�
"�B�=%A)A���D�"����E=CA�A�9�4GE:A�#�!���-E�������B�E��CB�E�������A���EC���C�����'CB�DE8E���!E����-�E��������������C���C������DE�!CBEA�"���������A����BA�1E=��Q7;��Q7GA�

��4G���
L��'=�A6A=��E�'=�A�A=�)�����D�=�A=�/���!="A�A=���D�2��=&A�A�9�HH;:A�(�!���C�����-��DE��8C������D��DE�������BC��ED�8C����8EB�����-������B�E��CB�'E�E�DE�C8E���C��8C8�A�#�!A�*E�E�"�E�A�18=�;HE�;�7A�
L���D�=#A=�&C�!C��=�A*A=�$E��'=CA=���D�*E�!��=&A/A�9�HHH:A�"����B�C��C�������D���������C������E'����C����-��E���BE���DC--E�E��C��C���-�B����1�FA�A�CA�%C��A�(�E!A�FE8=�7;��;�7;�7HA�
LE��!��E���D=CACA=�2C�CB=*A=�/����C�=(A=�/C�!�=/A=�%��C�=CA=��E�'=CA=�#��8E�=A=���D�/�����C�ED�=%A�9�H��:A����B�E�����EBC-CB�DE�E�C����-��������--EB���DE8E���!E�����D�DC���������!E�����C���-���E�E��B�C�E����B�E��A�*�����E��E����'��1.F=�444��HH4A�
�= A=��S#�1E�=CA=�/���'E=*A=�%���E=/A=��E�$E�=A=� C��= A=�D����E=(A&A=�&E��C�0E�=*A=�$C�'=cA=��C�E�EE��=�A=�%��,E��=$A=�/B���-!���=�A=�*��D,���=*A=���D�#EC!�E�'=#A�9�HHG:A�%E���BE����B����E�'E�E���ED�-��!�E�D�'E��������'E�C�����C��C�B��ED��D����!���E����B�E��A�(E���1@F=��4Q��HQA�
���=/A=�%���1=&ACA=��EB1E�=2ACA=�%����E=&A�A=����B��=/A�A=�#��E=&A�A=�&�B�����D=�ACA=���D�/���E�=$A�9�H��:A����B�E�����EBC-CB�DE�E�C����-�!���E�*���;���D�*���F�B���E�����B�E��CB��'E�E�C�A�CA�(�C�A�.�8E���1FF=�7E�F�7E�GA�
6�D�="A=��E0�1C=2A=�/��E=#A=�2�C0�!C=&A=���!DC�D��B=%A=��1���=&A=���D�2�1EC=&A�9�HHG:A�*��E�C���E'����E��C����C���E�E��E���D�'��BE!C�A�����C���'CB������E���D���E���E��CB����E��C��A�(���A��C��E�E���E8A�.=��G��7A�
6E=+A=���8C��CE=%A=���D�/B���-!���=�A�9�HHE:A�+C���������'��,���-�B�����Q���D��H���E�E���E��ED�C����E���!���E!�����CB����B�E��CB�!E�E�B��!E���D����!��E���E�����C-E���C����-�E!�����CB����B�E��CB�E�C��E�C���BE���A��C��E����'C��.D=��QQ��G�A�
c���=aA=�%��,�=CA=�2����E1=�A=���B�'����=CA=���D�&E����=�A�A�9�HHG:A�.��8C8���E���'��!!C�'��-��D�������B�E��CB�E��B�C�E�BE��������E���BE���A�����E�.88=�F�Q�F7�A��

��44���
C��#.#��
� �
�
�
�
� ,�B����CC����ECA����BC�E��E���D�������A��DE�BC���ECA�������ABA���������AD��������E�����
��� C� ����6������BC��B�E����EC������ �����EAB���ABA������B�DBAC������C�����A����ECA���A E��
��� B������� BD� �C� ���E� ��������� ��� �EA��� �B� ���E��� ��AE�E�A����� ���C� ����BAE� B������AE���
*�B�CE���A����ABA�������B���������AB��������E����BC��DBD�A�A�E������CC��C� ����C�B�������B��
ABACAD� �B� �E�;�C� ��� ����E�C�AE��� �B��E�� �ED�A�AB�AE��� ��E� ��� �ED�CA�B� ��B� ��� ���
�����EAB���ABA���������ECAE�������B�ED����GC��#����

Value of 18F–fluoro-L-dopa PET
in the Preoperative Localization
of Focal Lesions in Congenital
Hyperinsulinism1
Carmen Capito, MD
Naziha Khen-Dunlop, MD
Maria-Joao Ribeiro, MD, PhD
Francis Brunelle, MD
Yves Aigrain, MD
Celia Cretolle, MD, PhD
Francis Jaubert, MD
Pascale De Lonlay, MD, PhD
Claire Nihoul-Fekete, MD
Purpose: To retrospectively compare fluorine 18 (18F) fluoro-L-dopapositron emission tomography (PET) and pancreatic ve-nous sampling (PVS) in the preoperative differentiation ofdiffuse from focal congenital hyperinsulinism (CHI) andlocalization of focal lesions.
Materials and
Methods:
This study was approved by the institutional ethical com-mittee, and informed consent for the research study wasobtained from the parents of all subjects. Fifty-one pa-tients evaluated for focal CHI between January 1, 1995,and January 31, 2008, were included. Thirty five under-went PVS evaluation alone, and 16 underwent a PET eval-uation alone. The sensitivity values of each technique forthe diagnosis and localization of focal lesions were com-pared in regard to results of surgery and pathologic analy-ses. In each patient, perioperative treatment was re-viewed, and the presence of postoperative hypoglycemiawas assessed as evidence of incomplete resection. Com-parisons of the sensitivity values and recurrence rateswere performed by using the Fisher exact test in regard tothe number of patients. Comparisons of median age,weight, or number of biopsies were performed with atwo-tailed unpaired Mann-Whitney U test. A differencewith P , .05 was considered significant.
Results: For PVS and PET groups, there was no error in differentiat-ing focal from diffuse forms. PVS was not completed in fourof 35 patients. In 27 (87%) of 31 patients in whom PVS wascompleted and 13 (81%) of 16 patients in whom PET wascompleted, preoperative localization of the focal lesion was inaccordance with the surgical findings (P 5 .7). Although notsignificant, the number of biopsies performed before discov-ering the focal lesion was higher in the PET group comparedwith the PVS group (P 5 .06). Inadequate localization oc-curred in two (6%) patients in the PVS group and five (31%)patients in the PET group at initial preoperative imagingstudy; these patients underwent repeat surgery for residualCHI (P 5 .03).
Conclusion: 18F–fluoro-L-dopa PET is equivalent to PVS in the charac-terization of CHI but does not provide localization of thelesion as precisely as does PVS.
r RSNA, 2009
1 From the Departments of Pediatric Surgery (C. Capito,
N.K., Y.A., C. Cretolle, C.N.), Radiology (F.B.), Pathology
(F.J.), and Pediatrics (P.D.L.), Necker-Enfants Malades
Hospital, AP-HP, 149 rue de Sevres 75015 Paris, France;
and Biomedical Imaging Institute, Life Sciences Division
CEA, Frederic Joliot Hospital, Orsay, France (M.J.R.). Re-
ceived August 18, 2008; revision requested October 25;
final revision received February 26, 2009; accepted
March 17; final version accepted June 1. Address corre-
spondence to C. Capito (e-mail: carmendoc@hotmail
.com).
R RSNA, 2009
OR
IGIN
AL
RE
SE
AR
CH
nN
UC
LEA
RM
ED
ICIN
E
216 radiology.rsna.org ▪ Radiology: Volume 253: Number 1—October 2009
Note: This copy is for your personal, non-commercial use only. To order presentation-ready copies for
distribution to your colleagues or clients, use the Radiology Reprints form at the end of this article.

Congenital hyperinsulinism (CHI) isthe major cause of pediatric postna-tal persistent hypoglycemia and oc-
curs with an estimated incidence of one in30 000 to one in 50 000 live births innorthern countries (Europe, Canada,United States) (1). This abnormality ischaracterized by inappropriate insulinrelease, and early diagnosis and treat-ment are required to prevent severeneurologic damage (2). Histopathologi-cally, two major forms have been de-scribed: diffuse and focal (3,4). The dif-fuse form is characterized by dysregula-tion of insulin secretion that involves allthe pancreatic b cells. Treatment is gen-erally medical, but in rare cases whenthis treatment fails, near-total pancrea-tectomy is required (5). Pancreatec-tomy, the only procedure that can pre-vent hypoglycemia, results in iatrogenicdiabetes mellitus as a consequence ofthe procedure (6). In the focal form,insulin secretion dysregulation is local-ized to one region of the pancreas (7,8),and children with the focal form can becured by using complete resection of thefocal lesion (9,10). In cases of residualdisease, postoperative recurrence of hy-poglycemia will occur.
The clinical presentations of the twoforms are indistinguishable. Consequently,after correction of hypoglycemia and main-tenance of normal glucose levels, the ma-jor challenges in the treatment of childrenwith this abnormality are to characterizethe histopathologic form and, in childrenwith the focal form, to localize the lesionprior to surgery. Until 2002, pancreaticvenous sampling (PVS) by using catheter-ization of the portal system was themethod of choice for the diagnosis of thefocal form. By producing a detailed vascu-lar pancreatic map of the insulin concen-tration in each region of the pancreas,
this imaging study allows accurate diagno-sis and precise anatomic localization offocal lesions (11). However, it is invasiveand technically difficult to perform (12).Positron emission tomography (PET)with fluorine 18 (18F) fluoro-L-dopa wasintroduced in Necker-Enfants MaladesHospital (Paris, France) in 2002. Thisfunctional imaging study requires only pe-ripheral venous access and does not re-quire the patient to be hypoglycemic atthe time of the study. The study is basedon the capability of neuroendocrine cellsto take up L-DOPA and convert it to dopa-mine by decarboxylation (13). Research-ers reported that 18F–fluoro-L-dopa PEThas been shown to aid in the accuratedifferentiation of focal from diffuse forms(14,15), but the precision of the anatomiclocalization is limited by the spatial reso-lution of the nuclear technique itself(16,17). The purpose of our study was toretrospectively compare 18F–fluoro-L-dopaPET and PVS for the preoperative differ-entiation of diffuse from focal CHI and forlocalization of focal lesions.
Materials and Methods
Patients
The institutional ethics committee ofNecker-Enfants Malades Hospital ap-proved this retrospective study, and in-formed consent was obtained from theparents for clinical and research studies.
We retrospectively reviewed the surgicaland pathologic results in 51 patients whowere suspected of having and weretreated for focal CHI between January 1,1995, and January 31, 2008. These pa-tients were suspected of having a preop-erative diagnosis of focal CHI, in view ofthe resistance to medical treatment andthe findings at PVS or PET, which sug-gested a focal lesion. In all patients, sur-gical and pathologic results served as thereference standard for the diagnosis ofeither the diffuse or the focal form and fordetermination of the exact location of thelesion. Thirty-five patients underwentPVS evaluation between January 1, 1995,and March 31, 2002, and 16 children un-derwent an 18F–fluoro-L-dopa PET evalu-ation between November 1, 2002, andJanuary 31, 2008. Sixteen male patientsand 19 female patients underwent PVS,whereas 13 male patients and three fe-male patients were examined by usingPET. These differences in sex were notsignificant. The median age at diagnosis ofCHI was 1 day, with an age range of1–270 days for the PVS group and an agerange of 1–150 days for the PET group,and the difference between the groupswas not substantial. Respective medianage and weight at the time of radiologicevaluation were 5 months and 6.7 kgin the PVS group and 3 months and 7.1 kgin the PET group. The differences be-tween the groups were not significant(age, P 5 .06; weight, P 5 .8).
Published online before print
10.1148/radiol.2532081445
Radiology 2009; 253:216–222
Abbreviations:
CHI 5 congenital hyperinsulinism
PVS 5 pancreatic venous sampling
ROI 5 region of interest
SUV 5 standardized uptake value
Author contributions:
Guarantors of integrity of entire study, C. Capito, N.K., C.
Cretolle, P.D.L., C.N.; study concepts/study design or data
acquisition or data analysis/interpretation, all authors;
manuscript drafting or manuscript revision for important
intellectual content, all authors; manuscript final version
approval, all authors; literature research, C. Capito,
M.J.R., F.B., Y.A., F.J.; clinical studies, all authors; statis-
tical analysis, C. Capito, M.J.R., Y.A.; and manuscript
editing, C. Capito, N.K., M.J.R., F.B., Y.A., C.N.
Authors stated no financial relationship to disclose.
Advance in Knowledge
n The results of this study suggestthat albeit 18F–fluoro-L-dopa PETis an excellent examination for thecharacterization of the morpho-logic type of congenital hyperinsu-linism (focal vs diffuse), it fails toallow precise localization of thelesion for the surgeon.
Implications for Patient Care
n Children with focal forms of hy-perinsulinism can be cured withcomplete resection of the focallesion.
n The limitations of 18F–fluoro-L-dopa PET examination must beconsidered when planning surgeryto avoid unnecessary extendedpancreatic resections and to pre-vent long-term pancreatic insuffi-ciency.
n Improvements in spatial resolu-tion of the PET signal and the useof hybrid machines, such as PET/CT, may be helpful in obtainingbetter anatomic localization, per-mitting organ-sparing surgery.
NUCLEAR MEDICINE: 18F–fluoro-L-dopa PET for Congenital Hyperinsulinism Capito et al
Radiology: Volume 253: Number 1—October 2009 ▪ radiology.rsna.org 217

PVS Studies
The PVS studies (12) were performed byone author (F.B., with 10 years of experi-ence), who was the initiator of the tech-nique in Necker-Enfants Malades Hospi-tal. All medical treatments were stopped5 days before the examination. With ad-ministration of a general anesthetic, thepatients were maintained in a hypoglyce-mic state, with a venous blood glucoselevel between 2 and 3 mmol/L, and retro-grade transhepatic catheterization of theportal system was performed. At least 10venous blood samples from throughoutthe pancreatic venous network were col-lected for measurements of plasma glu-cose, insulin, and C-peptide levels. Dur-ing phlebography, a pancreatic venousmap of insulin levels was obtained (Fig 1).This map allowed the localization of thefocal lesion by using a simultaneous com-parison of the insulin–C-peptide ratiosand glucose levels at different anatomiclocations. A focal lesion was character-ized by an increase in insulin–C-peptideratios in one or two contiguous locations,when low levels of insulin and C-peptidewere obtained in the remaining gland. Indiffuse forms, insulin and C-peptide levelswere increased throughout the gland. Theratio of C-peptide to insulin was calculatedin each sample. Near a focal lesion, thisratio was about 1.0 (meaning that the levelsfor secretion of C-peptide and insulin by theb cells were the same), and it increased asthe distance from the lesion increased.
18F–fluoro-L-dopa PET Studies
The 18F–fluoro-L-dopa PET studies (18)were performed by an author (M.J.R.,with 7 years of experience), who was theinitiator of the technique in Necker-En-fants Malades Hospital. Intravenous injec-tion of 18F–fluoro-L-dopa (mean dose ofradioactivity injected, 4.2 MBq per kilo-gram of body weight 6 1.0 [standard de-viation]) was performed, and a thoraco-abdominal PET scan (three-dimensionalacquisition mode) was begun between 45and 65 minutes after radiotracer injec-tion. Depending on the height of the child,data were acquired in two to four bedpositions. The data sets were correctedfor scatter by using a model-based correc-tion, allowing simulation of a map of sin-gle scatter events. The images were re-
constructed by using an attenuation-weighted ordered subset expectationmaximization iterative algorithm, withfour iterations and six subsets. The finalspatial resolution in reconstructed imageswas approximately 6 mm. Three regionsof interest (ROIs) were identified in theright, middle, and left areas of the pan-creas; these areas corresponded to thehead (right side of the spine) (Fig 2), body(in front of the spine) (Fig 3), and tail (leftside of the spine) (Fig 4), respectively.The sizes of these ROIs varied from onechild to another; that is why the spine wasthe major anatomic landmark for inter-preting the location of the lesion. Themean radioactivity concentration in eachROI (in becquerels per milliliter), mea-sured at 60 minutes after injection, wasdivided by the injected dose of the radio-tracer (in becquerels) and was correctedfor the radioactive decay between injec-tion and scan start times and body weight(in grams) to calculate standardized up-take values (SUVs). Next, values for theratio between the SUV of the region
where the lesion is located and the meanpancreatic SUV were calculated. In dif-fuse forms, the values for the ratio be-tween the SUV of the region where thelesion is located and the mean pancreaticSUV are about 1.0. In contrast, in focalforms, the values for the the ratio be-tween the SUV of the region where thelesion is located and the mean pancreaticSUV are between 1.2 and 2.0. We consid-ered that an abnormal focal 18F–fluoro-L-dopa uptake for the pancreatic regionshould be reflected by a ratio between theSUV of each of the three ROIs and themean pancreatic SUV to be greater than1.2. The radiotracer has an early biliaryexcretion and late urinary elimination(gallbladder, liver, followed by kidneysand bladder, high signals during the ex-amination).
Surgery
In cases of radiologically confirmed focalCHI, partial elective pancreatectomywas recommended. Meticulous inspec-tion of the anterior wall of the pancreas
Figure 1
Figure 1: Vascular pancreatic map shows insulin concentrations in 3-month-old male infant with focal
CHI. Low levels of insulin were observed in all but one point of splenic vein (circled box with numbers). This
location was associated with hypersecretion of insulin (serum insulin level, 407 mIU/L [2827 pmol/L]), si-
multaneous hypoglycemia (serum glucose level, 1.9 mmol/L), and insulin–C-peptide ratio of 1.4. Results of
this examination were highly suggestive of focal lesion in distal body of pancreas. Values in each box repre-
sent serum glucose level (in millimoles per liter), serum insulin level (in milli–international units per liter),
and insulin–C-peptide ratio, from top to bottom. To convert values for serum insulin level to Systeme Interna-
tional units (in picomoles per liter), multiply by 6.945.
NUCLEAR MEDICINE: 18F–fluoro-L-dopa PET for Congenital Hyperinsulinism Capito et al
218 radiology.rsna.org ▪ Radiology: Volume 253: Number 1—October 2009

was performed, with a search for an obvi-ous lesion in the area suggested by thefindings at the preoperative radiologic ex-amination (head, body, or tail). Three bi-opsy specimens were taken in the threemorphologic areas of the pancreas forpathologic confirmation of the focal formof the disease (endocrine cells with abun-dant cytoplasm and large irregular nucleiin the pathologic zone and resting b cellswith small nuclei outside the focal lesion).Analyses were performed by one author(F.J., with 20 years of experience). If nolesion was seen on the anterior wall, thepancreas was mobilized from tail to headand inspected on the posterior wall. Ifthere was still no obvious lesion, multiplebiopsies were performed, first in the areasuggested by findings at imaging and then,if needed, at different points throughoutthe gland. For each biopsy, a contempo-raneous pathologic examination was per-formed until the focal lesion was found.After resection of the lesion, specimenswere examined from an adequate marginof normal tissue. The surgical procedurewas always performed by the same team(C.N. and Y.A., with 20 years of experi-ence in CHI surgery).
Evaluation
The surgical treatment (number of biop-sies performed before finding the focallesion and the size of the pancreas re-sected during surgery) and postopera-tive outcomes in the group of patientswho underwent preoperative PVS werecompared with postoperative outcomesin the group of patients who underwentpreoperative PET for evaluation. Pan-creatic resections for focal lesions var-ied from resection of a single well-delin-eated lesion to resections of one or mul-
tiple pancreatic areas. A resection wasjudged as complete if there was no post-operative recurrence of hypoglycemia.A resection was judged as incomplete ifthere was recurrence of hypoglycemia.In cases of incomplete resection, a sec-ond radiologic examination (the sameas initially performed) was performedto locate the persisting focus.
Statistical Analysis
Quantitative data were expressed withmedians and ranges. Diagnostic sensi-tivity of each examination was definedas the ratio of the number of patients inwhom a diagnosis of the focal form wasdetermined by using PVS or PET and inwhom the diagnosis was confirmed by us-ing surgery and pathologic analysis to thetotal number of patients in each group(PVS or PET). Accuracy or sensitivity forlocalization was defined as the ratio of thenumber of patients with correct localiza-tion of the lesion by using PVS or PETcompared with correct surgical localiza-tion to the total number of patients ineach group (PVS or PET). Comparisonsof sensitivity values and recurrence rateswere performed by using the Fisher exacttest, regarding the number of patients.Comparisons of median age, weight, ornumber of biopsies were performed witha two-tailed unpaired Mann-Whitney U
test. A difference with a P value of lessthan .05 was considered significant. Thestatistical analysis was performed withsoftware (StatView for Windows, version5.0; SAS Institute, Cary, NC).
Results
Diagnostic Sensitivity: Focal versus
Diffuse Form
PVS was successfully performed in 31patients. In four other patients, the ex-amination was not completed becauseof difficulties in maintaining the patientsin a stable hypoglycemic state during theexamination or because of an inability toperform transhepatic pancreatic cathe-terization. These four patients were, then,excluded from the rest of the analysis. PETexaminations were successfully completedin all patients examined, uneventfully.
Thus, as summarized in Table 1, the
Figure 2
Figure 2: Transverse 18F–fluoro-L-dopa PET
image in 6-month-old male infant shows focal lesion
(arrow) in head of pancreas. Diagnosis was con-
firmed at surgery. Focal lesion corresponds to large
uptake region localized in front of and on right side of
spine. Large posterior regions of increased uptake
correspond to kidneys. Despite poor spatial resolu-
tion of images, lesion was accurately localized by
using PET and was removed completely.
Figure 3
Figure 3: Transverse 18F–fluoro-L-dopa PET
image in 4-month-old male infant shows focal
lesion (arrow) in body of pancreas, localized in
front of spine.
Figure 4
Figure 4: Transverse 18F–fluoro-L-dopa PET
image in 5-month-old male infant shows focal
lesion (arrow) in tail of pancreas (far from spine,
on left side of spine).
Table 1
Diagnostic Sensitivity of PVS and PET
for Focal CHI
Clinical Data
PVS
Group
PET
Group
No. of patients 35 16
No. with diagnosis of focal
form 31 16
No. with procedure failure 4 0
No. with erroneous diagnosis 0 0
NUCLEAR MEDICINE: 18F–fluoro-L-dopa PET for Congenital Hyperinsulinism Capito et al
Radiology: Volume 253: Number 1—October 2009 ▪ radiology.rsna.org 219

diagnostic sensitivity for distinguishing be-tween the focal and the diffuse forms wasexcellent (100%) for both PVS and PETgroups. There was no error in differentiat-ing the focal form from the diffuse form.
Accuracy of Approximate Localization of
Focal Lesions
Because precise localization was notpossible with PET imaging alone, thesensitivity values of the preoperative ra-diologic localization with PVS and PETwere compared for the three major pan-creatic areas (head, body, tail).
During surgery, macroscopic focal le-sions were seen in 24 (77%) of 31 pa-tients in the PVS group and in 11 (69%) of16 patients in the PET group. In 27 (87%)of 31 patients in the PVS group and in 13(81%) of 16 patients in the PET group,preoperative localization of the lesion wasperformed, in accordance with the surgi-cal findings. In 74% (35 of 47) of ourpatients, the lesion was visualized at sur-gery, and this factor helped in the perfor-mance of the resection, and the use of thefindings from pathologic analysis was offurther assistance. The radiologic and
surgical features of the four patients inthe PVS group in whom misdiagnoses oflocalization occurred are summarized inTable 2. The three cases of misdiagnosisin the PET group are described in Figures5–7. There was no significant differencebetween the two groups in the accuracyof localization of focal lesions (P 5 .7).
The median number of biopsies weperformed before we discovered thefocal lesion was higher in the PETgroup (median number, six; range,1–12) than it was in the PVS group(median number, three; range, 0–12),
Figures 5–7
Figures 5: Coronal 18F–fluoro-L-dopa PET image shows inaccurate localization of focal lesion in 2-month-old female infant. Results suggested focal form (FF) le-
sion in body of pancreas (arrow). Perioperative findings indicated bifocal form with one lesion in inferior part of head of pancreas and another in wall of descending duo-
denum. Repeat surgery was performed because of incomplete resection of this bifocal lesion initially.
Figure 6: Coronal 18F–fluoro-L-dopa PET image shows inaccurate localization of focal form (FF) lesion in 2-month-old male infant. Results suggested focal lesion in
body of pancreas (red arrow). Gallbladder signal (green arrow) was well identified. Lesion was not identified during surgical procedure, and body of pancreas was re-
sected, as pointed out by using PET. After persistent hypoglycemia was noted postoperatively, this patient underwent repeat surgery, and focal lesion in head of pancreas
was resected.
Figure 7: Coronal 18F–fluoro-L-dopa PET image shows inaccurate localization of focal form (FF) lesion (red arrow) in 5-month-old male infant. Results suggested
focal lesion in body of pancreas. Common bile duct (CBD) and right ureter (green arrows) were well identified because they were abnormally dilated. After persistent hy-
poglycemia was noted postoperatively, this patient underwent repeat surgery, and focal lesion in head of pancreas was resected.
Table 2
Misdiagnoses at PVS
Patient No./Sex/Age (mo) Pancreatic Location at PVS Pancreatic Location at Perioperative Localization Extent of Resection
1/M/5 Head Body (lesion seen) Elective resection; patient was cured
2/F/7 Head Body (lesion seen) Elective resection; patient was cured
3/F/4 Body Tail (lesion seen) Elective resection; patient was cured
4/F/7 Body Lesion not seen and not found perioperatively; recurrence,
with localization in head at postoperative PVS
Resection of body and tail and secondary near-total
pancreatectomy; patient was cured
NUCLEAR MEDICINE: 18F–fluoro-L-dopa PET for Congenital Hyperinsulinism Capito et al
220 radiology.rsna.org ▪ Radiology: Volume 253: Number 1—October 2009

although the difference between thegroups was not significant (P 5 .06).
In the PVS group, two (6%) patientsunderwent further surgery for residualCHI, which was diagnosed after recur-rence of hypoglycemia. In one case, thisrecurrence resulted from incomplete re-section of the lesion, although findingsfrom an intraoperative pathologic exami-nation suggested free margins; the resec-tion was completed during a second pro-cedure. In the other case, partial resec-tion was performed, without successfulpreoperative localization of the lesion (pa-tient 4, Table 2); a second procedure wasperformed successfully.
In the group examined by usingPET, five (31%) patients underwent fur-ther surgery for residual CHI, whichwas diagnosed after recurrence of hypo-glycemia. In three of these patients, thefirst resection did not include the entirelesion, although the intraoperative patho-logic examination results suggested freemargins. The resection was completedwith a second procedure. In two otherpatients, the lesion was not found duringthe initial surgical procedure, when resec-tion of the region identified by using PETwas performed. After early recurrence ofhypoglycemia, these two patients under-went a second PET examination, whichconfirmed the persistence of focal dis-ease. The resection was successfully com-pleted during a second surgical proce-dure.
Of the 47 children in this study, 40(85%) were cured after the initial surgi-cal procedure, However the reexplora-tion rate was significantly higher in thePET group (P 5 .03).
Discussion
18F–fluoro-L-dopa PET is now the imagingmethod of choice for the examination ofpatients with CHI (13–15). Unlike PVS,PET evaluation can be performed easily,does not require patients to be anesthe-tized or hypoglycemic during the exami-nation, and does not require suspensionof medical treatment prior to examina-tion. Moreover, the radiation dose islower (1 mSv/kg for PVS vs 0.4 mSv/kgfor PET), and there is no associated riskof deep venous thrombosis. The only lim-
itation of this technique is that the radio-tracer is not available in all PET centers.
If one considers the approximate lo-calization of the focal lesion, with the pan-creas divided into three main areas, theresults of PET and PVS were comparable(81% and 87%, respectively, of lesionscorrectly identified). This finding con-firms that 18F–fluoro-L-dopa PET is notonly an accurate noninvasive techniquefor diagnosing focal forms of CHI but alsoa good examination for initial localizationof the pancreatic focal lesion (17). Theaim of surgery is to completely removethe lesion, while sparing as much of thepancreas as possible to prevent long-termpancreatic insufficiency. However, whenwe compared PET with PVS, we foundthat the lack of precision in the localiza-tion of the lesion by using PET can haveadverse consequences for both surgeonand patient: In this study, the repeat sur-gery rate was five times higher in the PETgroup.
Preoperative visualization of these fo-cal lesions is difficult because of theirsmall size (mean length, 10 mm) (17).Identification of these focal lesions is alsodifficult because their texture may beidentical to that of the surrounding nor-mal gland and because they occur eithersuperficially or deep within the pancreaticgland and may not be readily visible. In74% (35 of 47) of our patients, the lesionwas visualized at surgery, and this factorhelped in the performance of the resec-tion, and the use of the findings frompathologic analysis was of further assis-tance. For patients in whom the lesioncould not be seen macroscopically duringsurgery, the results of preoperative radio-logic studies and intraoperative histologicstudies were essential in guiding the re-section.
As with all functional imaging, 18F–fluoro-L-dopa PET demonstrates a bio-logical activity, and in this case, it is theactivity of hyperactive b cells in the pan-creas. The signal seen is proportional tothe activity rather than to the size of thelesion (13). Moreover, precise anatomiclandmarks, usually used in conventionalimaging, are not apparent (19,20). Whenwe compared 18F–fluoro-L-dopa PETwith PVS, the major limitation of PETwas its limited spatial resolution. Be-
cause PVS can be used to screen theentire pancreatic venous network, it al-lows precise anatomic localization of thefocal lesion. Although the difference interms of accuracy of approximate local-ization (P 5 .7) between the two tech-niques was not significant (probably be-cause of insufficient power, given thesmall number of patients), we found adifference, although not significant (P 5
.06), in the number of biopsies that hadto be performed during surgery. Thisdifference may be the consequence ofgreater difficulties in precisely locatingthe lesion with PET, despite the appar-ent comparable rate of “approximate”localization by using the three pancre-atic areas (head, body, and tail). Thisstudy had several shortcomings. Be-cause of its retrospective nature and thesmall number of patients in each group,this study failed to display significantdifferences between PVS and PETgroups concerning the accurate localiza-tion of focal lesions. Nevertheless, therepeat surgery rate in the patients in thePET group was significantly higher, sug-gesting better outcomes in patientstreated with PVS. This finding is favor-able in regard to the use of hybrid ma-chines, such as PET/computed tomog-raphy, which will permit better ana-tomic localization and more precisedelineation of focal CHI (19–22).
In conclusion, 18F–fluoro-L-dopa PETis an excellent way to differentiate focalfrom diffuse CHI, but this techniquefails to give precise localization of thelesion, partly because of the absence offixed anatomic landmarks (such as thecommon bile duct, splenic and mesen-teric blood vessels, spleen, and duode-num).
References
1. De Leon DD, Stanley CA. Mechanisms of
disease: advances in diagnosis and treatment
of hyperinsulinism in neonates. Nat Clin
Pract Endocrinol Metab 2007;3(1):57–68.
2. Menni F, de Lonlay P, Sevin C, et al. Neuro-
logic outcomes of 90 neonates and infants
with persistent hyperinsulinemic hypoglyce-
mia. Pediatrics 2001;107(3):476–479.
3. Goossens A, Gepts W, Saudubray JM, et al.
Diffuse and focal nesidioblastosis: a clinico-
pathological study of 24 patients with persis-
NUCLEAR MEDICINE: 18F–fluoro-L-dopa PET for Congenital Hyperinsulinism Capito et al
Radiology: Volume 253: Number 1—October 2009 ▪ radiology.rsna.org 221

tent neonatal hyperinsulinemic hypoglyce-
mia. Am J Surg Pathol 1989;13(9):766–775.
4. Sempoux C, Guiot Y, Jaubert F, Rahier J.
Focal and diffuse forms of congenital
hyperinsulinism: the keys for differential di-
agnosis. Endocr Pathol 2004;15(3):241–246.
5. Fekete CN, de Lonlay P, Jaubert F, Rahier J,
Brunelle F, Saudubray JM. The surgical man-
agement of congenital hyperinsulinemic hy-
poglycemia in infancy. J Pediatr Surg 2004;
39(3):267–269.
6. Cherian MP, Abduljabbar MA. Persistent
hyperinsulinemic hypoglycemia of infancy
(PHHI): long-term outcome following 95%
pancreatectomy. J Pediatr Endocrinol Metab
2005;18(12):1441–1448.
7. Giurgea I, Bellanne-Chantelot C, Ribeiro M,
et al. Molecular mechanisms of neonatal hy-
perinsulinism. Horm Res 2006;66(6):289–
296.
8. Sempoux C, Guiot Y, Dahan K, et al. The
focal form of persistent hyperinsulinemic hy-
poglycemia of infancy: morphological and
molecular studies show structural and func-
tional differences with insulinoma. Diabetes
2003;52(3):784–794.
9. Adzick NS, Thornton PS, Stanley CA, Kaye
RD, Ruchelli E. A multidisciplinary approach
to the focal form of congenital hyperinsulin-
ism leads to successful treatment by partial
pancreatectomy. J Pediatr Surg 2004;39(3):
270–275.
10. Cretolle C, de Lonlay P, Sauvat F, et al.
Congenital hyperinsulinism of infancy: surgi-
cal treatment in 60 cases of focal form [in
French]. Arch Pediatr 2005;12(3):258–263.
11. Dubois J, Brunelle F, Touati G, et al. Hyper-
insulinism in children: diagnostic value of
pancreatic venous sampling correlated with
clinical, pathological and surgical outcome in
25 cases. Pediatr Radiol 1995;25(7):512–
516.
12. Brunelle F, Negre V, Barth MO, et al. Pan-
creatic venous samplings in infants and chil-
dren with primary hyperinsulinism. Pediatr
Radiol 1989;19(2):100–103.
13. Ahlstrom H, Eriksson B, Bergstrom M, Bjurl-
ing P, Långstrom B, Oberg K. Pancreatic
neuroendocrine tumors: diagnosis with PET.
Radiology 1995;195(2):333–337.
14. Hardy OT, Hernandez-Pampaloni M, Saffer
JR, et al. Diagnosis and localization of focal
congenital hyperinsulinism by 18F-fluoro-
dopa PET scan. J Pediatr 2007;150(2):140–
145.
15. Ribeiro MJ, De Lonlay P, Delzescaux T, et al.
Characterization of hyperinsulinism in in-
fancy assessed with PET and 18F-fluoro-L-
DOPA. J Nucl Med 2005;46(4):560–566.
16. Von Schulthess GK, Hany TF. Imaging and
PET-PET/CT imaging. J Radiol 2008;89(3 pt
2):438–447.
17. Mohnike K, Blankenstein O, Minn H,
Mohnike W, Fuchtner F, Otonkoski T.
[18F]-DOPA positron emission tomogra-
phy for preoperative localization in con-
genital hyperinsulinism. Horm Res 2008;
70(2):65–72.
18. Mohnike K, Blankenstein O, Christesen
HT, et al. Proposal for a standardized pro-
tocol for 18F-DOPA-PET (PET/CT) in con-
genital hyperinsulinism. Horm Res 2006;
66(1):40–42.
19. Blodgett TM, Meltzer CC, Townsend DW.
PET/CT: form and function. Radiology 2007;
242(2):360–385.
20. von Schulthess GK, Steinert HC, Hany TF.
Integrated PET/CT: current applications and
future directions. Radiology 2006;238(2):
405–422.
21. Barthlen W, Blankenstein O, Mau H, et al.
Evaluation of [18F]Fluoro-L-DOPA positron
emission tomography-computed tomogra-
phy for surgery in focal congenital hyperinsu-
linism. J Clin Endocrinol Metab 2008;93(3):
869–875.
22. Subramaniam RM, Karantanis D, Peller PJ.
[18F]Fluoro-L-dopa PET/CT in congenital
hyperinsulinism. J Comput Assist Tomogr
2007;31(5):770–772.
NUCLEAR MEDICINE: 18F–fluoro-L-dopa PET for Congenital Hyperinsulinism Capito et al
222 radiology.rsna.org ▪ Radiology: Volume 253: Number 1—October 2009

Morphological Mosaicism of the Pancreatic Islets:
A Novel Anatomopathological Form of Persistent
Hyperinsulinemic Hypoglycemia of Infancy
C. Sempoux, C. Capito, C. Bellanne-Chantelot, V. Verkarre, P. de Lonlay,Y. Aigrain, C. Fekete, Y. Guiot, and J. Rahier
Department of Pathology (C.S., Y.G., J.R.), Cliniques Universitaires Saint Luc, 1200 Brussels, Belgium;
Departments of Pediatric Surgery (C.C., Y.A., C.F.) and Pathology (V.V.), Unite 845 Institut National de la
Sante et de la Recherche Medicale (C.C.), and Reference Center of Metabolic Diseases (P.d.L.) Assistance
Publique-Hopitaux de Paris (AP-HP) Hopital Necker-Enfants Malades, Universite Paris Descartes, Faculte
de Medecine, 75743 Paris, France; and Department of Genetics (C.B.-C.), AP-HP Groupe Hospitalier
Pitie-Salpetriere, Universite Pierre et Marie Curie, 75651 Paris, France
Background: Morphological studies of the pancreas in persistent hyperinsulinemic hypoglycemia
of infancy (PHHI) have focused on the diagnosis of focal vs. diffuse forms, a distinction that de-
termines the optimal surgical management. ABCC8 or KCNJ11 genomic mutations are present in
most of them.
Aim: Our aim was to report a new form of PHHI with peculiar morphological and clinical
characteristics.
Research Design and Methods: Histopathological review of 217 pancreatic PHHI specimens re-
vealed 16 cases morphologically different from diffuse and focal forms. They were analyzed by
conventional microscopy, quantitative morphometry, immunohistochemistry, and in situ
hybridization.
Results: Their morphological peculiarity was the coexistence of two types of islet: large islets with
cytoplasm-rich b-cells and occasional enlarged nuclei and shrunken islets with b-cells exhibiting
little cytoplasm and small nuclei. In small islets, b-cells had abundant insulin content but limited
amount of Golgi proinsulin. Large islets had low insulin storage and high proinsulin production and
were mostly confined to a few lobules. No evidence for KATP channels involvement or 11p15
deletion was found. Genomic mutations for ABCC8, KCNJ11, and GCK were absent. Patients had
normal birth weight and late hypoglycemia onset and improved with diazoxide. Ten were cured
by limited pancreatectomy. Six recurred after surgery and were medically controlled.
Conclusion: This new form of PHHI is characterized by a morphological mosaicism. Pathologists
should recognize this mosaicism on intraoperative frozen sections because it is often curable by
partial pancreatectomy. The currently unknown genetic background does not involve the classical
genomic mutations responsible for diffuse and focal PHHI. (J Clin Endocrinol Metab 96: 0000–0000,
2011)
Persistent hyperinsulinemic hypoglycemia of infancy
(PHHI), a syndrome that was first recognized by
McQuarrie (1), has been repeatedly attributed to nesidi-
oblastosis, a particular histological feature that is character-
ized by the presence of numerous small clusters of endocrine
cells in the vicinity of the pancreatic ducts (2). Nesidioblas-
tosis was considered a permanent b-cell proliferation, lead-
ing to an increased b-cell mass that was responsible for
ISSN Print 0021-972X ISSN Online 1945-7197
Printed in U.S.A.
Copyright © 2011 by The Endocrine Society
doi: 10.1210/jc.2010-3032 Received December 27, 2010. Accepted August 25, 2011.
Abbreviations: H&E, Hematoxylin and eosin; ISH, in situ hybridization; LOH, loss of
heterozygosity; PET, positron emission tomography; PHHI, persistent hyperinsulinemic hy-
poglycemia of infancy; PVS, pancreatic venous sampling; SUR1, sulfonylurea receptor 1.
O R I G I N A L A R T I C L E
E n d o c r i n e R e s e a r c h
J Clin Endocrinol Metab, December 2011, 96(12):0000–0000 jcem.endojournals.org 1
J Clin Endocrin Metab. First published ahead of print September 28, 2011 as doi:10.1210/jc.2010-3032
Copyright (C) 2011 by The Endocrine Society

hyperinsulinism. However, the proliferation index and the
fractional volume of b-cells are not higher in the pancreas
of hypoglycemic infants than in controls, and nesidioblasto-
sis is not specific to the disease in that it is also observed in the
pancreas of normoglycemic neonates and infants (3, 4).
Since the 1990s, histological retrospective analyses of
case series led several groups to characterize two forms of
PHHI: the focal and the diffuse forms (3–7). In the first
form, a small focal endocrine lesion, often invisible to the
naked eye, is responsible for insulin hypersecretion. This
lesion is an adenomatous hyperplasia made from the con-
fluence of histologically roughly normal islets with few
non-b-cells at the periphery of a b-cell central core. Ab-
normal, large b-cell nuclei are often observed within the
lesion but are not seen outside of the focal lesion where the
islets exhibit small nuclei and less cytoplasm, with evidence
of low proinsulin synthesis. This focal form is curable by a
partial pancreatectomy restricted to the lesion. The second
form is diffuse and involves the whole pancreas. Its histolog-
icalhallmark is thepresenceofabnormally large b-cell nuclei
scatteredthroughoutmost islets (3–6). Inbothforms, infants
have a high birth weight, hypoglycemia occurs in the neo-
natalperiod,anddiazoxide isnearlyalways ineffective (8,9).
Neither clinical nor biological data can be used to differen-
tiate the focal from the diffuse forms. To distinguish the two
forms, portal venous catheterization with selective venous
sampling for insulin measurements (10) and more recently
noninvasive imaging using positron emission tomography
(PET) with [18F]fluoro-L-DOPA (18F-PET) are useful (11,
12). Intraoperative frozen sections are essential, not only to
confirm the diagnosis made based on imaging but also to
determine whether the suspected area effectively corre-
sponds to a focal lesion and is completely resected (13).
The genetic cause of many cases has been identified. In
most diffuse forms, hyperinsulinism is due to inactivating
mutations in ABCC8 or KCNJ11, which are located on
chromosome 11p15 and code for the sulfonylurea recep-
tor 1 (SUR1) and Kir6.2 proteins, respectively, the two
subunits of ATP-sensitive K (KATP) channels, resulting
in abnormal channels (14, 15). In the focal forms, in ad-
dition to a paternally inherited inactivating mutation in
ABCC8 or KCNJ11, there is a loss of heterozygosity in the
11p15 region, leading to the occurrence of focal adeno-
matous hyperplasia because of an imbalance between im-
printed genes involved in cell proliferation (H19 and
IGF2) and a loss of the antiproliferative factor p57 (16–
20). Infrequent cases of congenital hyperinsulinism unre-
lated to KATP channels have also been reported; most of
these cases were sensitive to diazoxide. These cases may be
due to dominant activating mutations of the GLUD1
gene, which codes for glutamate dehydrogenase (21, 22),
or due to activating mutations of GCK, which codes for glu-
cokinase (23, 24); these are two enzymes that are involved in
the metabolic control of insulin secretion. Loss-of-function
mutations in the HADH gene and mutations in HNF4a
can also produce infantile hyperinsulinism (25–29). The
rarity of these forms, which are unrelated to defects of the
KATP channels, explains why exhaustive descriptions of
their pathological characteristics are limited.
Among the 217 cases of operated PHHI that we col-
lected over 25 yr, 16 cases (7.4%) did not fit with the usual
types. They displayed peculiar pancreatic morphologies
and had a distinct clinical presentation, with normal birth
weight in the majority of the cases, a late onset of hyper-
insulinism, and a relative sensitivity to diazoxide. Fur-
thermore, when genetic analyses were performed in
these infants (n 5 13), genomic mutations of ABCC8,
KCNJ11, and GCK were ruled out, and no similar peculiar
pathologies were found in cases with similar mutations. The
aim of the present study is to report the histological charac-
teristicsof thesepatients topermit intraoperative recognition
and diagnosis of this particular form of PHHI that can often
be cured by a limited pancreatectomy.
Materials and Methods
On the basis of their specific histological features alone, we identi-
fied 16 cases of the 217 PHHI pancreases collected during surgery
in several European hospitals since 1976. This study was approved
by the ethical committee of the Universite Catholique de Louvain.
Whenever possible and after obtaining the written informed
consentoftheparents forthegenetic testingoftheirchildren,genetic
analyses were performed to search for ABCC8, KCNJ11, or GCK
genomic mutations. The genetic results of four of these 16 patients
have recently been published in a large series of 109 patients (30);
this previous publication evaluated the incidence and spectrum of
ABCC8 and KCNJ11 mutations in this cohort of PHHI.
Diagnoses of PHHI were made according to the clinical cri-
teria previously reported (8). The infants were considered to be
or to become nonresponsive to diazoxide therapy when 10 mg/
kg z d was insufficient to avoid hypoglycemic events (8).
Preoperative radiological evaluation was performed by pan-
creatic venous sampling (PVS) (10) in 14 cases, by 18F-PET (12,
13, 31) in one case, and with both in the last case.
All samples of partial pancreatectomies were fixed in 4% for-
malin to study SUR1, Ki67, and p57 and to perform molecular
biology investigations, including in situhybridization (ISH) forpro-
insulin mRNA and/or in Bouin’s solution for conventional micros-
copy on hematoxylin and eosin (H&E)-stained sections and the
immunostainingof insulin,proinsulin, somatostatin,andglucagon.
The anomalies were sometimes very small, being limited to
one or a few pancreatic lobules and were not detectable with the
naked eye. Moreover, the areas of interest were sometimes fixed
only in Bouin’s solution. All of the analyses were thus not per-
formed in all of the cases but were performed according to theadequacy of the available material.
The sizes of the b-cell nuclei and the b-cell nuclear crowding
(number of b-cell nuclei per 1000 mm2 of b-cell cytoplasm) were
2 Sempoux et al. Mosaicism in Infantile Hyperinsulinism J Clin Endocrinol Metab, December 2011, 96(12):0000–0000

measured in both types of islet (at least 10 islets in each case)according to themethod previously reported (6)Theareaof theseislets was measured and used to evaluate the differences betweenthe types of islet (Axiovision, Zeiss, Germany).
Immunoperoxidase staining was performed to detect insulin,proinsulin, and somatostatin as well as SUR-1, Ki67, and p57.The source of the antibodies and their dilution for use are givenin Supplemental Table 1 (published on The Endocrine Society’sJournals Online web site at http://jcem.endojournals.org).
Quantifications of Golgi proinsulin (diaminobenzidine) andsomatostatin cells (Fast Red) were performed on paraffin sec-tions. The total immunostained area of each islet was measured,and the coordinates of each islet were stored by an image ana-lyzer (KS-400 system; Zeiss-Vision, Munich, Germany). On thesame slides, insulin was further detected (Fast red), and the totalimmunostained area was measured again. After removal of theFast red staining by washing in alcohol, the Golgi proinsulin areawas measured, and the areas of somatostatin (d-cell area) andinsulin (b-cell area) immunolabeling were calculated. Then, theGolgi proinsulin-to-cytoplasmic insulin area ratio that reflectsthe b-cell synthesis function was calculated as previously re-ported (18) and related to the d-cell-to-b-cell area ratio. Isletsections (n 5 220) from six age-matched normoglycemic con-trols, born to nondiabetic mothers and dead from a disease not
related to the endocrine pancreas, were compared with 300 isletsfrom six infants with islet mosaicism.
The insulincontentofb-cells inboth typesof isletwasquantifiedon paraffin sections by measuring the specific absorbance (OD) on10 islets of each type after immunostaining for insulin according toa method of immunodensitometry previously reported (32).
ISH to detect proinsulin mRNA was performed with a flu-orescein isothiocyanate-labeled probe (final dilution 1:2;NCL-Proins, Novocastra, UK).
For microsatellite analysis, normal and hyperfunctional isletswere microdissected from paraffin sections of three cases (cases 8,12,and15;Table1)usingaPALMMicroLaserSystemspulsed laser(337 nm; Bernied, Germany) coupled to an Axiovert 200 micro-scope (Zeiss, Oberkochen, Germany). Although the morphologywas maintained using formalin, every sixth section from the con-secutive sections was stained with H&E to confirm the identifica-tion of normal and hyperfunctional islet areas. A Picopure DNAextraction kit (Arcturus Bioscience, Mountain View, CA) was usedto extract DNA from microdissected tissues following the manu-facturer’s recommendations. Loss of heterozygosity (LOH) wasstudied with a selection of markers located in the 11p15 region,from telomere to centromere (NCBI database): D11S4046 (0.8Mb), D11S2351 (3.9 Mb), D11S902 (16.3 Mb), and D11S4114(19.5 Mb), as described previously (18). PCR products were ana-
TABLE 1. Clinical data
Case Sex
Birthweight
(percentile)
Age atpresentation
(months)
Preop Dzxtreatment(mg/kg z d)
Localization(PVS or 18F-PET) Surgery Follow-up
1 F 46 3 6.5 Inconclusive (PVS) Partial tail Recurrence controlledby low-dose Dzx
2 F 78 6 10 Focal-corpus (PVS) Partial corpusand tail
Cured
3 M 94 8 10 Focal (PVS) Partial corpusand tail
Cured
4 F 4 5 12 Diffuse (PVS) Partial corpusand tail
Cured
5 F 64 6 15 Focal-tail (PVS) Partial tail Cured6 F 69 3 Sensitive
to DzxFocal (PVS) Partial corpus
and tailCured
7 M 79 4 Transientsensitivity
Tail (PVS) Tail Cured
8 M 48 5 15 Focal-head (PVS) Partial Recurrence controlledby low-dose Dzx
9 M 7 9 10 Focal tail (PVS) Partial tail Cured10 M 40 5.5 12 Focal tail (PVS) Partial tail Recurrence controlled
by low-dose Dzx11 F 51 6 6 Focal tail (PVS) Partial corpus
and tailCured
12 F 86 NN Transientsensitivity
Focal corpus (PVS) Partial corpusand tail
Cured
13 M 48 4 18 Focal corpus and tail(PVS)
Partial corpusand tail
Cured
14 F 90 NN 15 Inconclusive (PVS) Head corpus andtail
Recurrence controlledby low-dose Dzx
15 F Unknown 6 Sensitiveto Dzx
Inconclusive(18F-PET)
Partial head andisthmus
Recurrence controlledby low-dose Dzx
16 M 45 7 Transientsensitivity
Inconclusive(PVS and 18F-PET)
Corpus and tail Recurrence controlledby low-dose Dzx
Cases 4, 6, and 13 were not tested for ABCC8, KCNJ11, and GCK mutations. Mutations in the GDH gene have been ruled out in patients 7, 10,
and 14. Dzx, Diazoxide; F, female; M, male; Preop, preoperative.
J Clin Endocrinol Metab, December 2011, 96(12):0000–0000 jcem.endojournals.org 3

lyzed using ABI Genescan Software. Allelic loss was scored if thearea under the allelic peak was reduced by a minimum of 50%. Apreviously tested focal lesion served as the positive control (casenumber 7 from Ref. 18).
The statistical evaluation of the results was conducted usingthe Fisher’s exact test for the differences in proportions of infantswith high birth weight and by Wilcoxon signed-rank test for allof the other parameters.
Results
Clinical data
The clinical data of the 16 atypical cases retrieved from
the patient files are detailed in Table 1. In most of the cases
(14 of 16), the hypoglycemic events occurred later in life
(median 165 d, range 1–270 d) than those in the classical
focal and diffuse forms, which are almost always diag-
nosed in the neonatal period (8, 9). The birth weights
expressed in percentiles were lower than in the forms pre-
viously reported (z score 5 10.04 vs. 11.36). Only one
patient (6%) had a percentile higher than 90% vs. 46% in
a series of 52 classical PHHI cases reported by de Lonlay-
Debeney et al. (8); this proportion of infants was signifi-
cantly lower than that previously reported (8) (P , 0.001,
Fisher’s exact test). At the onset of disease, all of the infants
were responsive to diazoxide at least for a short period of
treatment. Later, the sensitivity to the drug decreased, and
the infants required progressive and continuous increasing
of the dose, which, in certain infants, finally exceeded the
10 mg/kg z d that is characterized for diazoxide sensitivity
(8). Although they experienced marked improvement
upon diazoxide treatment, most infants remained prone to
occasional hypoglycemic events. This is strikingly dif-
ferent from the classical focal and diffuse forms that are
related to KATP channelopathies, which are almost al-
ways insensitive to diazoxide from birth (8, 9). Insulin
levels after PVS or 18F-PET were suggestive of focal
lesions in 11 cases, diffuse lesions in one case, and in-
conclusive or difficult to interpret in
four other cases.
For one or several reasons (persis-
tence of hypoglycemic events, progres-
sive loss of diazoxide sensitivity, or ma-
jor hypertrichosis and /or because PVS
was suggestive of a localized form), the
patients finally underwent surgery. Af-
ter partial pancreatectomy, 10 were de-
finitively cured. In the six others, hypo-
glycemic events reoccurred in the first
days or weeks after surgery and were
medically treated (Table 1).
Morphology
Conventional microscopy
Macroscopically, the pancreas ap-
peared normal, and no lesions were
identified macroscopically by the sur-
geon during surgery. Several biopsies
(from four to 20) were thus taken by the
surgeon in the area suspected by PVS or18F-PET or in different areas of the
gland when the preoperative localiza-
tion techniques were inconclusive, and
frozen sections were made. After recog-
nition of the abnormal area, biopsies
were taken to ensure that the limits of the
resection were healthy. The typical char-
acteristic of the lesions, already recogniz-
able on frozen sections, were confirmed
after H&E staining; these typical charac-
teristicswere thecoexistenceof twostrik-
FIG. 1. Islet mosaicism. A and B, On H&E-stained sections, the typical feature of this new
form of PHHI was the presence of both large hyperplastic islets with cytoplasm-rich b-cells
exhibiting some enlarged nuclei (A) as well as small shrunken islets that are 2-fold smaller (B);
C and D, after the immunodetection of insulin, the large islets showed a faint diffuse
homogeneous staining (C), whereas the small islets had strong polarized labeling (D); E, the
staining for proinsulin was stronger in large islets, suggesting a high level of function; F, this
staining was limited to a small dot in the small shrunken islets.
4 Sempoux et al. Mosaicism in Infantile Hyperinsulinism J Clin Endocrinol Metab, December 2011, 96(12):0000–0000

inglydifferent typesof islet, resulting inamosaicpattern(Fig.
1, A–F).
Morphometry
Profiles from islets of the first type were 2.06-fold larger
than the second type of islet, with a mean value of 11,407
mm2 (P , 0.01). They contained numerous b-cells with
abundant cytoplasm and sometime large nuclei. However,
these nuclei were rarely as large as those in the classical
diffuse form of the disease (Fig. 1A). The radius of the
b-cell nuclei and the b-cell crowding have been evaluated
on both types of islet (Fig. 2) The b-cell nuclear mean
radius was constantly larger in the hyperplastic type 1
islets than in the small type 2 islets (5.66 6 0.83 vs. 3.85 6
0.21 mm, P , 0.01) (Fig. 2A). The b-cell nuclear crowding
was higher in small type 2 than in hyperplastic type 1 islets
(13.91 6 3.27 vs. 8.88 6 2.56) (Fig. 2B). The hyperplastic
type 1 islets were not observed throughout the whole pan-
creas but were confined to one or some adjacent lobules of
the pancreas (Fig. 3). Certain lobules contained only this
type of islet, but other lobules showed both types of islet.
The islets of the second type were small and appeared
hypotrophic. They contained b-cells with scanty cyto-
plasm and small nuclei and appeared suppressed (Fig. 1B).
This second type of islet was distributed throughout the
whole pancreas.
Immunocytochemistry, ISH, and microsatellite analysis
Immunocytochemistry also revealed striking differ-
ences between both types of islet (Fig. 1, C–F). In the first
type (large islets), the outlines of the islets labeled with
insulin antibody were very regular, and the cytoplasm of
the b-cells was only faintly stained at a very uniform level
(Fig. 1C), whereas the proinsulin antibody gave a strong
labeling, which marked a large Golgi area (Fig. 1E). The
insulin mRNA content, which was demonstrated by ISH,
was also abundant, and only a few somatostatin and glu-
cagon cells were present at the periphery of these islets
(Fig. 4A). In the second type of islet (small shrunken islets),
the staining with the antiinsulin antibody was strong, and
the outlines of the islets were irregular (Fig. 1D), but the
proinsulin antibody labeled only a small dot correspond-
ing to the Golgi area (Fig. 1F). Insulin mRNA labeling was
slightly lower in the islets, and the somatostatin and glu-
cagon cells were much more numerous than in the first
type of islet (Fig. 4B).
p57waspresent inbothtypesof islet (Fig.4,CandD),and
SUR1 immunolabeling had a similar pattern and intensity of
staining in both types of islet, appearing cytoplasmic with a
perimembranous reinforcement (Fig. 4, E and D).
The intensity of the insulin immunolabeling was mea-
sured in both types of islet by immunodensitometry. The
ODof insulin labelingwasalwayshigher in small suppressed
islets than in hyperplastic-hyperactive islets (0.403 1 0.101
vs. 0.288 1 0.093, P , 0.01) (Fig. 2C).
The proinsulin in the Golgi of b-cells, a reflection of
b-cell proinsulin synthesis, was measured in the islets from
normoglycemic patients (n 5 6) and from six cases with
FIG. 2. Nuclear radius, nuclear crowding, and densitometry of insulin.
The two symbols linked by a line represent the mean value of the
parameter measured in large hyperplastic islets (left) and in small
shrunken islets (right) in the same patient. A, Mean radius of 50
selected b-cell nuclei (micrometers) in large hyperplastic and small
shrunken islets; B, b-cell nuclear crowding (number of b-cell nuclei/
1000 mm2 of b-cell cytoplasm); C, specific absorbance (OD) of insulin
labeling (immunodensitometry); means of 10 islets in each islet type
and patients.
FIG. 3. Lobular distribution of large hyperplastic islets. At low
magnification, the lobular topography of hyperplastic-hyperactive islets
was already recognizable (proinsulin immunodetection).
J Clin Endocrinol Metab, December 2011, 96(12):0000–0000 jcem.endojournals.org 5

islet mosaicism, and these measurements were compared
with the amount of d-cells in these islets. For this purpose,
the d-cell-to-b-cell area ratio (area percentage) was mea-
sured in each individual islet and related to the proinsulin
in the Golgi area (expressed as proinsulin-to-b-cell area
percentage) in the same islets. In the controls (Supplemen-
tal Fig. 1A), the d-cell-to-b-cell area ratio varied from
2.4 –119.0%. The Golgi proinsulin-to-insulin area ratio
showed weak variations (0–3.3%). By contrast, in hypo-
glycemic infants with islet mosaicism (Supplemental Fig.
1B), the d-cell-to-b-cell area ratio markedly varied within
the islets (from 0–250%) as did their Golgi proinsulin to
insulin area (from 0–21.6%). In this series of infants,
many islets with low d-cell-to-b-cell area ratios had large
Golgi proinsulin areas, whereas other infants with high
d-cell-to-b-cell area ratios had normal or small Golgi pro-
insulin areas (the small and shrunken islets).
The proliferation index of b-cells was counted in
both types of islet and was found to range 1.12–1.18%
of b-cells in suppressed and hyperplastic islets (not
significant).
Because the purity of the cell population was critical in
LOH detections, both types of islet were microdissected
from the same histological sections, and microsatellite
analysis was performed separately in the three cases (cases
8, 12, and 15). None of these showed an 11p15 LOH
involving imprinted genes in 11p15.5 and ABCC8, IGF2
or H-19, and KCNJ11 (Fig. 5). In patient 8, one marker
was not informative (D11S902); in patient 12, the four
markers were informative; and in patient 15, one marker
was not informative (D11S4114). To confirm that the la-
ser microdissection did not reduce the sensitivity for the
detection of LOH in small microdissected tissues by mic-
rosatellite analysis, a similar procedure was applied in a
case of focal adenomatous hyperplasia, and this procedure
confirmed the 11p15 deletion that was previously dem-
onstrated (case number 7 from Ref. 18) (Fig. 5).
FIG. 4. Insulin mRNA and somatostatin cells, p57, and SUR1. A and B,
Insulin mRNA and somatostatin cells in large hyperplastic islets (A) and
in small shrunken islets (B). Insulin mRNA labeling was darker in the
large hyperplastic islets, whereas d-cells were less numerous
(ISH/immunohistochemistry, differential interference contrast of
Nomarski). C and D, p57 immunodetection in large hyperplastic islets
(C) and in small shrunken islets (D). There were no differences in the
numbers of positive cells or in the intensities of the labeling. E and F,
SUR1 immunodetection showed no difference between the large
hyperplastic islets (E) and the small shrunken islets (F).
FIG. 5. Microsatellite analysis. A, Markers used and their distribution
in the 11p15 region; B and C, tracing corresponding to marker
D11S2351. In contrast to a classical KATP-related focal lesion used as
positive control (B), no LOH was observed in patients with histological
mosaicism (C, case 8). TM, Telomere; CM, centromere.
6 Sempoux et al. Mosaicism in Infantile Hyperinsulinism J Clin Endocrinol Metab, December 2011, 96(12):0000–0000

Discussion
From our careful review of the series of 217 PHHI pa-
tients, we identified 16 cases (7.4%) with a unique pan-
creatic histology characterized by the coexistence of two
different types of islet, a striking mosaic aspect never de-
scribed in normoglycemic infants or in infants suffering
from the diffuse form of PHHI related to ABCC8 or
KCNJ11 mutations; unlike those with the mosaicism,
these pancreases have islets that have the same appear-
ance, with numerous small poorly formed islets and large
b-cell nuclei and cytoplasm (3, 5, 6). The novel mosaic
pattern differs from that of the focal form because of the
absence of adenomatous hyperplasia, but the islets of the
second type (with small nuclei and reduced cytoplasm)
resemble the normal resting islets located outside the focus
of insulin hypersecretion (3, 5, 6, 7, 18).
In the mosaic forms that we analyzed, the hyperactive
islets were located in one or some adjacent lobules. This
focal distribution explains why many cases were cured by
partial pancreatectomy.
The distinct aspects of the two types of islet suggest
major functional differences. The islets of the first type
contain b-cells with large nuclei and cytoplasm, charac-
teristic of hyperactive b-cells. Their proinsulin antibody-
labeled Golgi were large, reflecting a high rate of hormone
synthesis, as confirmed by a stronger labeling for insulin
mRNA by ISH. By contrast, the faint labeling of the an-
tiinsulin antibody suggested that insulin is not stored for
very long but is rapidly released. The islets of the second
type showed the opposite characteristics: small nuclei,
shrunken cytoplasm, and proinsulin-stained Golgi area
restricted to a punctate labeling but strong antiinsulin an-
tibody staining, indicating that these b-cells are resting
with a low production of proinsulin but a high storage of
insulin. This morphological aspect suggested that persis-
tent hypoglycemia inhibits insulin secretion and synthesis
in these b-cells, which implies that they remain normally
regulated.
In most cases, hyperactive islets contain only a few
d-cells compared with resting islets. Our quantitative anal-
ysis of the mosaic cases indicated that proinsulin synthesis
is higher in b-cells from islets with a low d-cell-to-b-cell
area ratio. The absence of d-cells may have a role in in-
fantile hyperinsulinism (33) but has never been demon-
strated in the islets of KATP hyperinsulinemic infants. The
meaningof the decrease in d-cell number in the hyperactive
islets of mosaic cases remains unclear. Suggested previ-
ously but not yet demonstrated (34), intra-insular soma-
tostatin secretion may play a role in the control of insulin
secretion. Furthermore, because the low d-to-b ratio also
observed in certain islets from normoglycemic controls
was not linked to proinsulin overproduction in these
controls, it is unlikely that the hyperproduction of pro-
insulin observed in hyperactive islets is caused by a rel-
ative lack of d-cells.
A lack of expression of the antiproliferative factor p57
has been implicated in the hyperplasia of classic focal le-
sions (17). Obvious expression of p57 in hyperfunctional
as well as resting islets of the mosaic form clearly indicates
that 11p15 LOH is not the cause of the lesion. This ob-
servation was confirmed in three cases using microsatellite
analysis. This new mosaic form of PHHI is thus distinct
and unrelated to the focal form previously described.
Large nuclei in the hyperactive islets should not be mis-
taken for a diffuse pathology (which would lead to ag-
gressive management) because they are restricted to a few
lobules and are mixed with small resting islets, a feature
never observed in the diffuse form of PHHI.
Interestingly, the clinical characteristics of these pa-
tients are also different from those of diffuse or focal PHHI
patients. Birth weight, corrected for gestational age and
sex, was indeed lower than that of infants suffering from
diffuse or focal KATP channelopathy (8, 9). This could
suggest that the disease was not present before birth or did
not cause major hyperinsulinism in utero. The observation
that the first symptoms of hypoglycemia occurred or were
recognized only later in life in most cases reinforced this
interpretation. This late onset may also result from the
small size of the lesion or from transient compensation by
physiological adaptive mechanisms.
The patients with mosaic histology shared some clinical
characteristics with infants presenting a loss-of-function
mutation of the HADH gene: a later onset in comparison
with KATP-deficient cases and a certain sensitivity to di-
azoxide. Although we cannot definitely rule out a role for
the HADH gene for now, no particular protein sensitivity
has been found in our mosaic cases, and the decrease in
diazoxide sensitivity with time that we observed has not
been reported in HADH-mutated patients.
In this series, 10 infants were definitively cured by a
partial pancreatectomy, but six were not cured. This could
suggest that their lesion was not localized or less localized
than expected and incompletely resected. In these six
cases, the observation of pancreatic lobules that contain
only healthy islets means that the lesion sparing at least
some lobules is thus a true localized lesion and does not
correspond to a classical diffuse form. It is likely that the
extension of the lesion, and then the difficulty of its re-
section, varies according to the chronology of the somatic
mutation occurrence.
When genetic analyses were performed, genomic
ABCC8 or KCNJ11 mutations were not found, indicating
that this mosaic form was also genetically different from
J Clin Endocrinol Metab, December 2011, 96(12):0000–0000 jcem.endojournals.org 7

those related to KATP channel abnormalities. This is in
agreement with the persistence of a response (although
incomplete) to diazoxide in these cases as well as with the
normal and similar SUR1 immunohistochemical expres-
sion we found in both types of islet. The observation of this
insular mosaicism, together with the lobular distribution
of the abnormalities, could be explained by the occurrence
of specific somatic mutations during the embryonic de-
velopment of the endocrine pancreas. These mutations
have so far not been identified in this series.
Rare cases of PHHI with histology that did not fit with
the classical description of focal or diffuse forms have al-
ready been reported (35, 36). Whether the particular his-
tological features could result from a longer evolution of
the KATP channel deficiency in children were operated on
later in life is unlikely because the usual KATP-deficient
children who are operated on later in life still present nu-
merous abnormal nuclei disseminated throughout the
pancreas and never show a mosaic pattern. The relative
sensitivity to diazoxide and the absence of demonstrated
genomic ABCC8 or KCNJ11 mutations in these patients
also do not favor this hypothesis.
Pancreatic b-cell nuclear enlargement that is found only
in some sections of the pancreas has been recently reported
in a hypoglycemic infant by Hussain et al. (37). That case,
however, completely differs from ours by its mosaic uni-
parental paternal disomy, with the interstitial region of the
uniparental paternal disomy encompassing the KATP
channel genes and including an ABCC8 mutation, which
was not found in the 13 patients we analyzed for genetic
mutations. Furthermore, the patient had a neonatal onset
of hypoglycemia and an immediate and total insensitivity
to diazoxide.
We have identified a new form of PHHI that is char-
acterized by a morphological mosaicism, with particular
histological, immunohistochemical, and clinical charac-
teristics. The abnormal hyperfunctional islets of this form
are most often confined to a few adjacent lobules. The
genetic background of these cases remains unclear, but the
diagnosis of morphological mosaicism should be sus-
pected from the peculiar clinical presentation and can be
confirmed during surgery using intraoperative surgical
frozen sections, with the knowledge that partial pancre-
atectomy may often be sufficient to cure the infant.
Acknowledgments
The authors thank Mrs. J. Marchandise, Mr. S. Godecharles, andMr. S. Lagasse for their skillful technical assistance.
Address all correspondence and requests for reprints to: Prof.Dr. Jacques Rahier, M.D., Ph.D., Department of Pathology, Cli-
niques Universitaires Saint Luc, Avenue Hippocrate 10, 1200Brussels, Belgium. E-mail: [email protected].
This work was supported by Grants 3.4616.05 (to J.R.),9.4559.04 (to C.S.), and 1.5.216.04 (to C.S.) from the FondsNational de la Recherche Scientifique Medicale (Belgium) and byARC Grant 05/10-328 (to C.S.) from the General Direction ofScientific Research of the French Community of Belgium.
Disclosure Summary: The authors have nothing to disclose.
References
1. McQuarrie I 1954 Idiopathic spontaneously occurring hypoglyce-
mia in infants: clinical significance of problem and treatment. Am J
Dis Child 87:399–428
2. Landau H, Perlman M, Meyer S, Isacsohn M, Krausz M, Mayan H,
Lijovetzky G, Schiller M 1982 Persistent neonatal hypoglycemia due
to hyperinsulinism: medical aspects. Pediatrics 70:440–446
3. Rahier J, Falt K, Muntefering H, Becker K, Gepts W, Falkmer S 1984
The basic structural lesion of persistent neonatal hypoglycaemia
with hyperinsulinism: deficiency of pancreatic D cells or hyperac-
tivity of B cells? Diabetologia 26:282–289
4. Rahier J, Guiot Y, Sempoux C 2000 Persistent hyperinsulinaemic
hypoglycaemia of infancy: a heterogeneous syndrome unrelated to
nesidioblastosis. Arch Dis Child Fetal Neonatal Ed 82: F108–F112
5. Goossens A, Gepts W, Saudubray JM, Bonnefont JP, Nihoul-Fekete,
Heitz PU, Kloppel G 1989 Diffuse and focal nesidioblastosis. A
clinicopathological study of 24 patients with persistent neonatal
hyperinsulinemic hypoglycemia. Am J Surg Pathol 13:766–775
6. Sempoux C, Guiot Y, Lefevre A, Nihoul-Fekete C, Jaubert F,
Saudubray JM, Rahier J 1998 Neonatal hyperinsulinemic hypogly-
cemia: heterogeneity of the syndrome and keys for differential di-
agnosis. J Clin Endocrinol Metab 83:1455–1461
7. Suchi M, MacMullen CM, Thornton PS, Adzick NS, Ganguly A,
Ruchelli ED, Stanley CA 2006 Molecular and immunohistochemical
analyses of the focal form of congenital hyperinsulinism. Mod
Pathol 19:122–129
8. de Lonlay-Debeney P, Poggi-Travert F, Fournet JC, Sempoux C, Vici
CD, Brunelle F, Touati G, Rahier J, Junien C, Nihoul-Fekete C,
Robert JJ, Saudubray JM 1999 Clinical features of 52 neonates with
hyperinsulinism. N Engl J Med 340:1169–1175
9. de Lonlay P, Fournet JC, Touati G, Groos MS, Martin D, Sevin C,
Delagne V, Mayaud C, Chigot V, Sempoux C, Brusset MC, Laborde
K, Bellane-Chantelot C, Vassault A, Rahier J, Junien C, Brunelle F,
Nihoul-Fekete C, Saudubray JM, Robert JJ 2002 Heterogeneity of
persistent hyperinsulinaemic hypoglycaemia. A series of 175 cases.
Eur J Pediatr 161:37–48
10. Brunelle F, Negre V, Barth MO, Fekete CN, Czernichow P,
Saudubray JM, Kuntz F, Tach T, Lallemand D 1989 Pancreatic
venous samplings in infants and children with primary hyperinsulin-
ism. Pediatr Radiol 19:100–103
11. Otonkoski T, Nanto-Salonen K, Seppanen M, Veijola R, Huopio H,
Hussain K, Tapanainen P, Eskola O, Parkkola R, Ekstrom K, Guiot
Y, Rahier J, Laakso M, Rintala R, Nuutila P, Minn H 2006 Non-
invasive diagnosis of focal hyperinsulinism of infancy with [18F]-
DOPA positron emission tomography. Diabetes 55:13–18
12. Mohnike K, Blankenstein O, Christesen HT, De Lonlay J, Hussain
K, Koopmans KP, Minn H, Mohnike W, Mutair A, Otonkoski T,
Rahier J, Ribeiro M, Schoenle E, Fekete CN 2006 Proposal for a
standardized protocol for 18F-DOPA-PET (PET/CT) in congenital
hyperinsulinism. Horm Res 66:40–42
13. Rahier J, Sempoux C, Fournet JC, Poggi F, Brunelle F, Nihoul-
Fekete C, Saudubray JM, Jaubert F 1998 Partial or near-total pan-
createctomy for persistent neonatal hyperinsulinaemic hypoglycae-
mia: the pathologist’s role. Histopathology 32:15–19
14. Thomas PM, Cote GJ, Wohllk N, Haddad B, Mathew PM, Rabl W,
8 Sempoux et al. Mosaicism in Infantile Hyperinsulinism J Clin Endocrinol Metab, December 2011, 96(12):0000–0000

Aguilar-Bryan L, Gagel RF, Bryan J 1995 Mutations in the sulfo-
nylurea receptor gene in familial persistent hyperinsulinemic hypo-
glycemia of infancy. Science 268:426–429
15. Ryan F, Devaney D, Joyce C, Nestorowicz A, Permutt MA, Glaser
B, Barton DE, Thornton PS 1998 Hyperinsulinism: molecular ae-
tiology of focal disease. Arch Dis Child 79:445–447
16. de Lonlay P, Fournet JC, Rahier J, Gross-Morand MS, Poggi-Tra-
vert F, Foussier V, Bonnefont JP, Brusset MC, Brunelle F, Robert JJ,
Nihoul-Fekete C, Saudubray JM, Junien C 1997 Somatic deletion of
the imprinted 11p15 region in sporadic persistent hyperinsulinemic
hypoglycemia of infancy is specific of focal adenomatous hyperpla-
sia and endorses partial pancreatectomy. J Clin Invest 100:802–807
17. Kassem SA, Ariel I, Thornton PS, Hussain K, Smith V, Lindley KJ,
Aynsley-Green A, Glaser B 2001 p57(KIP2) expression in normal
islet cells and in hyperinsulinism of infancy. Diabetes 50:2763–2769
18. Sempoux C, Guiot Y, Dahan K, Moulin P, Stevens M, Lambot V, de
Lonlay P, Fournet JC, Junien C, Jaubert F, Nihoul-Fekete C,
Saudubray JM, Rahier J 2003 The focal form of persistent hyper-
insulinemic hypoglycemia of infancy: morphological and molecular
studies show structural and functional differences with insulinoma.
Diabetes 52:784–794
19. Verkarre V, Fournet JC, de Lonlay P, Gross-Morand MS, Devillers
M, Rahier J, Brunelle F, Robert JJ, Nihoul-Fekete C, Saudubray JM,
Junien C 1998 Paternal mutation of the sulfonylurea receptor
(SUR1) gene and maternal loss of 11p15 imprinted genes lead to
persistent hyperinsulinism in focal adenomatous hyperplasia. J Clin
Invest 102:1286–1291
20. Fournet JC, Mayaud C, de Lonlay P, Gross-Morand MS, Verkarre
V, Castanet M, Devillers M, Rahier J, Brunelle F, Robert JJ, Nihoul-
Fekete C, Saudubray JM, Junien C 2001 Unbalanced expression of
11p15 imprinted genes in focal form of congenital hyperinsulinism:
association with a reduction to homozygosity of a mutation in
ABCC8 or KCNJ11. Am J Pathol 158:2177–2184
21. Stanley CA, Fang J, Kutyna K, Hsu BY, Ming JE, Glaser B, Poncz M
2000 Molecular basis and characterization of the hyperinsulinism/
hyperammonemia syndrome: predominance of mutations in exons
11 and 12 of the glutamate dehydrogenase gene. HI/HA Contrib-
uting Investigators. Diabetes 49:667–673
22. Stanley CA, Lieu YK, Hsu BY, Burlina AB, Greenberg CR, Hop-
wood NJ, Perlman K, Rich BH, Zammarchi E, Poncz M 1998 Hy-
perinsulinism and hyperammonemia in infants with regulatory mu-
tations of the glutamate dehydrogenase gene. N Engl J Med 338:
1352–1357
23. Cuesta-Munoz AL, Huopio H, Otonkoski T, Gomez-Zumaquero
JM, Nanto-Salonen K, Rahier J, Lopez-Enriquez S, García-Gimeno
MA, Sanz P, Soriguer FC, Laakso M 2004 Severe persistent hyper-
insulinemic hypoglycemia due to a de novo glucokinase mutation.
Diabetes 53:2164–2168
24. Sayed S, Langdon DR, Odili S, Chen P, Buettger C, Schiffman AB,
Suchi M, Taub R, Grimsby J, Matschinsky FM, Stanley CA 2009
Extremes of clinical and enzymatic phenotypes in children with hy-
perinsulinism caused by glucokinase activating mutations. Diabetes
58:1419–1427
25. Clayton PT, Eaton S, Aynsley-Green A, Edginton M, Hussain K,
Krywawych S, Datta V, Malingre HE, Berger R, van den Berg IE2001 Hyperinsulinism in short-chain L-3-hydroxyacyl-CoA dehy-drogenase deficiency reveals the importance of b-oxidation in in-sulin secretion. J Clin Invest 108:457–465
26. Molven A, Matre GE, Duran M, Wanders RJ, Rishaug U, NjølstadPR, Jellum E, Søvik O 2004 Familial hyperinsulinemic hypoglyce-mia caused by a defect in the SCHAD enzyme of mitochondrial fattyacid oxidation. Diabetes 53:221–227
27. Li C, Chen P, Palladino A, Narayan S, Russell LK, Sayed S, XiongG, Chen J, Stokes D, Butt YM, Jones PM, Collins HW, Cohen NA,Cohen AS, Nissim I, Smith TJ, Strauss AW, Matschinsky FM, Ben-nett MJ, Stanley CA 2010 Mechanism of hyperinsulinism in short-chain 3-hydroxyacyl-CoA dehydrogenase deficiency involves acti-vation of glutamate dehydrogenase. J Biol Chem 285:31806–31818
28. Pearson ER, Boj SF, Steele AM, Barrett T, Stals K, Shield JP, EllardS, Ferrer J, Hattersley AT 2007 Macrosomia and hyperinsulinaemichypoglycaemia in patients with heterozygous mutations in theHNF4A gene. PLoS Med 4:e118
29. Fajans SS, Bell GI 2007 Macrosomia and neonatal hypoglycaemiain RW pedigree subjects with a mutation (Q268X) in the gene en-coding hepatocyte nuclear factor 4alpha (HNF4A). Diabetologia50:2600–2601
30. Bellanne-Chantelot C, Saint-Martin C, Ribeiro MJ, Vaury C,Verkarre V, Arnoux JB, Valayannopoulos V, Gobrecht S, SempouxC, Rahier J, Fournet JC, Jaubert F, Aigrain Y, Nihoul-Fekete C, deLonlay P 2010 ABCC8 and KCNJ11 molecular spectrum of 109patients with diazoxide-unresponsive congenital hyperinsulinism.J Med Genet 47:752–759
31. Ribeiro MJ, Boddaert N, Bellanne-Chantelot C, Bourgeois S, Va-layannopoulos V, Delzescaux T, Jaubert F, Nihoul-Fekete C,Brunelle F, De Lonlay P 2007 The added value of [18F]fluoro-L-DOPA PET in the diagnosis of hyperinsulinism of infancy: a retro-spective study involving 49 children. Eur J Nucl Med Mol Imaging34:2120–2128
32. Rahier J, Stevens M, de Menten Y, Henquin JC 1989 Determinationof antigen concentration in tissue sections by immunodensitometry.Lab Invest 61:357–363
33. Bishop AE, Polak JM, Chesa PG, Timson CM, Bryant MG, BloomSR 1981 Decrease of pancreatic somatostatin in neonatal nesidi-oblastosis. Diabetes 30:122–126
34. Orci L, Unger RH 1975 Functional subdivision of islets of Langer-hans and possible role of D cells. Lancet 2:1243–1244
35. Sempoux C, Guiot Y, Cosgrove K, Nenquin M, de Lonlay P,Saudubray JM, Fekete C, Robert JJ, Brunelle F, Dunne M, HenquinJC, Rahier J 2002 A new morphological form of persistent hyper-insulinaemic hypoglycaemia of infancy: correlation with clinical andphysiological data. Horm Res 58(Suppl 2):44 (Abstract P1-146)
36. Suchi M, Thornton PS, Adzick NS, MacMullen C, Ganguly A, Stan-ley CA, Ruchelli ED 2004 Congenital hyperinsulinism: intraoper-ative biopsy interpretation can direct the extent of pancreatectomy.Am J Surg Pathol 28:1326–1335
37. Hussain K, Flanagan SE, Smith VV, Ashworth M, Day M, Pierro A,Ellard S 2008 An ABCC8 gene mutation and mosaic uniparentalisodisomy resulting in atypical diffuse congenital hyperinsulinism.Diabetes 57:259–263
J Clin Endocrinol Metab, December 2011, 96(12):0000–0000 jcem.endojournals.org 9

The surgical management of atypical forms of congenital
hyperinsulinism
Carmen Capito, MD,a Pascale de Lonlay, MD, PhD,b Virginie Verkarre, MD,c
Francis Jaubert, MD,c Jacques Rahier, MD,d Claire Nihoul-Fékété, MD,a
Yves Aigrain, MDa
From the aDepartment of Pediatric Surgery, AP-HP Hôpital Necker-Enfants Malades, Université Paris Descartes, Paris,
France;bReference Center of Metabolic Diseases, AP-HP Hôpital Necker-Enfants Malades, Université Paris Descartes, Paris,
France;cDepartment of Pathology, AP-HP Hôpital Necker-Enfants Malades, Université Paris Descartes, Paris, France; and thedDepartment of Pathology, Cliniques Universitaires, St-Luc, Louivain University, Brussels, Belgium
Beyond the 2 classical forms of congenital hyperinsulinism, focal and diffuse, we report our experience
on the surgical treatment of atypical forms. We define 2 subtypes among these atypical forms of
hyperinsulinism: in case of a giant focal form the surgical strategy is the same as in focal forms. In case
of hyperinsulinism caused by a mosaic, our experience suggests the benefit of a limited resection from
the tail to the body of the pancreas.
© 2011 Elsevier Inc. All rights reserved.
KEYWORDSHyperinsulinism;
Atypical forms;
Surgery
Therapeutic management of congenital hyperInsulinism
(CHI) may be challenging.1,2 Some patients (43% in our
experience) will require surgical treatment because of the
inability to medically control the disease and avoid delete-
rious hypoglycemic episodes.2-4 Histologic classification of
CHI includes 2 major forms: diffuse forms, which are char-
acterized by hyperfunction of every islet of Langerhans, and
focal forms, which correspond to an adenomatous hyper-
plasia and are smaller than 15 mm with resting islets outside
the lesion.2,5-7 Diffuse forms, which are uncontrollable by
medical treatment, will require a near total pancreatectomy,
with unpredictable postoperative results.2 Focal forms, as
we proposed a few years ago,8 can be cured by complete
resection of the lesion with pancreatic-sparing surgery when
possible (efficient peroperative pathologic examination on
frozen sections for free margins). A third group correspond-
ing to rare case reports in the literature9 includes what is
generally called atypical forms, which are defined as non-
focal and nondiffuse forms on histologic reports. These
atypical forms are not homogeneous, and we have been able
to identify 2 varieties: segmental mosaic forms and exten-
sive focal forms.
Materials and methods
From 1991 to 2009, 427 children were managed for CHI in
our center. They all presented with hypoglycemia less than
3 mmol/L associated with inappropriate plasma insulin lev-
els. Among them, 184 patients were operated on for CHI
resistant to medical treatment. Before surgery, a radiologi-
cal evaluation was performed by pancreatic venous cathe-
Address reprint requests and correspondence: Yves Aigrain, MD,
Service de Chirurgie Pédiatrique, 149 Hôpital Necker Enfants-Malades rue
de Sèvres, 75743 Paris Cedex 15 France.
E-mail: [email protected].
1055-8586/$ -see front matter © 2011 Elsevier Inc. All rights reserved.
doi:10.1053/j.sempedsurg.2010.10.003
Seminars in Pediatric Surgery (2011) 20, 54-55

terization sampling10 or, after 2002, 18-fluoro-L-Dopa
positron-emission tomography scanning.11 These examina-
tions permitted us to diagnose the histologic classical form
of CHI and, in case of focal forms, to locate the lesion and
guide the surgical procedure.12 The indications for surgery
were assumed in every case of focal CHI, and a partial
elective pancreatectomy was performed.8,13 Diffuse lesions
were operated whenever complete suppression of hypogly-
cemia was not achieved by a medical treatment compatible
with home management. A near-total pancreatectomy was
performed, leaving only the pancreatic tissue in the concav-
ity of the duodenum and containing the choledocal duct.13
The operative protocol consisted in all cases of an inspec-
tion of the anterior wall of the gland searching for an
obvious lesion. Three biopsies were taken in the 3 morpho-
logic areas of the pancreas for pathologic confirmation of
histologic form of the disease on frozen sections. Focal form
is defined as an adenomatous hyperplasia smaller than 15
mm and made by endocrine cells with an abundant cyto-
plasm and large irregular nuclei in the hyperinsulinic zone
and resting b cells with little nuclei outside the focal lesion.
Diffuse forms are defined as hyper function of every islet of
Langerhans within the pancreas. Those islets include abnor-
mal beta cells with giant nuclei. Atypical forms were de-
scribed as nonfocal and nondiffuse form. After surgery,
specimens were examined from a confirmation of the his-
tologic form and an adequate margin of normal tissue. We
will focus on the surgical treatment of patients whose patho-
logic report was atypical because lesions encountered were
not in accordance with the classical definition of focal or
diffuse forms.
Results and conclusions
Histopathological results
The review of the pathologic reports allows separating the
patients into 2 groups. The first group has pathologic fea-
tures that were similar to classical focal forms but the size
of the lesion was much larger than 15 mm as classically
described in typical focal forms. We called this pathologic
entity “extensive focal form.” In the second group the pan-
creatic architecture was normal but the coexistence of hyper
functional islets with some abnormal giant beta cell nuclei,
and resting small and round islets (mosaicism), in a seg-
mental distribution. Because of this segmental distribution
and the mixed lesion with parts of diffuse (hyper functional
islets) and focal lesion (resting islets) we called this form
“segmental mosaic form.”
Extensive focal forms
In this group the surgical procedure consists in the resection
of the focal lesion. The main difference with the classic
focal forms concern the number of biopsies needed to reach
free margins, the length of surgery and the amount of
pancreatic tissue removed. Moreover, a redo procedure with
further resection due to persistent hypoglycemia is more
frequent in this group of patients.
Segmental mosaic forms
Anatomical location of the lesion involved in most cases the
tail and body of the pancreas. That is why we strongly
advocate a partial resection starting from the left to the
portal vein. Even in cases where this limited procedure does
not completely cure the hypoglycemia, most patients are
improved by the limited resection and few will require a
redo procedure.
References
1. Hussain K. Diagnosis and management of hyperinsulinaemic hypo-
glycaemia of infancy. Horm Res 2008;69:2-13.
2. Lonlay-Debeney P, Poggi-Travert F, Fournet JC, et al. Clinical fea-
tures of 52 neonates with hyperinsulinism. N Engl J Med 1999;340:
1169-75.
3. Kapoor RR, Flanagan SE, James C, et al. Hyperinsulinaemic hypo-
glycaemia. Arch Dis Child 2009;94:450-7.
4. Menni F, de Lonlay P, Sevin C, et al. Neurologic outcomes of 90
neonates and infants with persistent hyperinsulinemic hypoglycemia.
Pediatrics 2001;107:476-9.
5. De Leon DD, Stanley CA. Mechanisms of disease: Advances in
diagnosis and treatment of hyperinsulinism in neonates. Nat Clin Pract
Endocrinol Metab 2007;3:57-68.
6. Sempoux C, Guiot Y, Dahan K, et al. The focal form of persistent
hyperinsulinemic hypoglycemia of infancy: morphological and molec-
ular studies show structural and functional differences with insuli-
noma. Diabetes 2003;52:784-94.
7. Sempoux C, Guiot Y, Jaubert F, Rahier J. Focal and diffuse forms of
congenital hyperinsulinism: the keys for differential diagnosis. Endocr
Pathol 2004;15:241-46.
8. Cretolle C, Fekete CN, Jan D, et al. Partial elective pancreatectomy is
curative in focal form of permanent hyperinsulinemic hypoglycaemia
in infancy: A report of 45 cases from 1983 to 2000. J Pediatr Surg
2002;37:155-8.
9. Hussain K, Flanagan SE, Smith VV, et al. An ABCC8 gene mutation
and mosaic uniparental isodisomy resulting in atypical diffuse con-
genital hyperinsulinism. Diabetes 2008;57:259-63.
10. Brunelle F, Negre V, Barth MO, et al. Pancreatic venous samplings in
infants and children with primary hyperinsulinism. Pediatr Radiol
1989;19:100-3.
11. Ribeiro MJ, de Lonlay P, Delzescaux T, et al. Characterization of
hyperinsulinism in infancy assessed with PET and 18F-fluoro-L-dopa.
J Nucl Med 2005;46:560-6.
12. Capito C, Khen-Dunlop N, Ribeiro MJ, et al. Value of 18F-fluoro-L-
dopa PET in the preoperative localization of focal lesions in congenital
hyperinsulinism. Radiology 2009;253:216-22.
13. Fekete CN, de Lonlay P, Jaubert F, et al. The surgical management of
congenital hyperinsulinemic hypoglycemia in infancy. J Pediatr Surg
2004;39:267-9.
55Capito et al Surgical Management of Atypical Forms of CIH