Embed Size (px)
Citation preview
DOI: 10.1002/cmdc.201000259
Developments in Nonsteroidal Antiandrogens Targetingthe Androgen ReceptorBo Liu,[a] Lei Su,[b] Jingkun Geng,[a] Junjie Liu,[a] and Guisen Zhao*[a]
Introduction
The burden of prostate cancer (PCa) in the world is significant;PCa remains the most frequently diagnosed noncutaneous ma-lignancy and remains the second leading cause of cancer-relat-ed deaths among men in Western countries.[1] In 2009, approxi-mately 192 280 men were diagnosed with PCa, and 27 360men were estimated to die from the disease.[1] The risk factorin PCa includes, but is not limited to, race, geography, age andgene rearrangements.[2] Though patients with PCa initially re-spond to androgen-deprivation therapy, they inevitably relapseto castration-resistant prostate cancer (CRPC) within 18–24months. CRPC is incurable,[3] and it is acknowledged that an-drogen and androgen signaling still play the most influentialrole in the development of PCa. Thus, the treatment of PCa byinhibiting the function of the androgen receptor (AR) remainsa standard strategy. Although drugs such as R-bicalutamideand flutamide have been used in the past to inhibit thegrowth of PCa tumors, eventually the cancer becomes refracto-ry to available AR antagonists. Therefore, new rational ap-proaches and new drugs for the treatment of PCa are needed.
This review will focus primarily on the new nonsteroidalcompounds that have evolved from classical drugs. These newdrugs include bicalutamide derivatives, isoxazolones, pyrrolecarboxamides, pyridines and N-arylpiperazine derivatives,imide-based analogues, hydantoin derivatives, carborane-con-taining derivatives, and organometallic-containing derivatives.We will provide research-related reference materials for thedesign of new antiprostate cancer drugs.
The Structure of the Androgen Receptor andits Gene
The AR is a ligand-induced transcription factor belonging tothe steroid and nuclear receptor superfamily, which includesmore than 100 members with five known vertebrate steroid re-ceptors (androgen receptor (AR), estrogen receptor (ER), pro-gesterone receptor (PR), glucocorticoid receptor (GR) and min-eralocorticoid receptor (MR)),[4] and the number is still increas-ing.
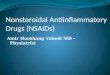
AR is a 110 kDa nuclear receptor coded by the AR gene,which contains eight exons located on Xq11–12.[5] In commonwith other members of the nuclear of transcription factors, theAR is constructed from three principal series of functional do-mains (Figure 1): a hypervariable N-terminal transactivationdomain (NTD) encoded by exon 1; a central, highly conservedDNA-binding domain (DBD) encoded by exons 2 and 3, which
can recognize and bind to a specific DNA sequence that con-stitutes the androgen response element; a large C-terminalligand-binding domain (LBD) encoded by another five exons.Moreover, there is a short hinge-region linker between theDBD and the LBD that contains a nuclear localization signal(NLS) assisting AR in locating a specific site of the relevantDNA and promoting gene transcription.[4, 6] In addition, thereare two transcriptional activation functions, the N-terminal acti-vation function 1 (AF1) and the C-terminal activation function 2(AF2). AR has a three-dimensional structure similar to those ofthe other steroid receptors, ER, PR, GR, MR, and a sequencethat is highly homologous to that of PR. These similarities canobviously explain the phenomenon of cross-reactivity duringthe clinical treatment of PCa.
The Function of the Androgen Receptor
Androgen and the AR signaling pathway play an importantrole in the male secondary sexual characteristics and in the de-velopment and functions of the prostate. Abnormalities of theAR gene and protein can lead to the occurrence of many dis-eases, including PCa, androgen insensitivity syndrome,[7] malebreast cancer,[8] and muscular dystrophy.[9]
In prostate tissue, testosterone and dihydrotestosterone(DHT) are endogenous ligands of AR. Testosterone is usuallyconverted to dihydrotestosterone (DHT) by 5a-reductase. Tes-tosterone and DHT can bind to AR as ligands, while DHT has ahigher affinity profile. Before binding to its ligands, the inactive
[a] B. Liu, J. Geng, J. Liu, Prof. G. ZhaoSchool of Pharmaceutical Sciences, Shandong UniversityJinan, Shandong, 250012 (P. R. China)Fax: (+ 86) 531-8838-2009E-mail : [email protected]
[b] L. SuShandong Institute of Commerce and TechnologyJinan, Shandong, 250103 (P. R. China)
Figure 1. The structure of the androgen receptor gene and protein (adaptedfrom Reference [4]).
ChemMedChem 2010, 5, 1651 – 1661 � 2010 Wiley-VCH Verlag GmbH & Co. KGaA, Weinheim 1651

AR is located in the cytoplasm binding to chaperone heatshock proteins (HSPs), such as HSP90. Once the AR binds tothe endogenous androgens, such as DHT, some of HSPs disso-ciate from the AR. At the same time, there is a conformationalchange in the AR; then the AR translocates to the nucleus as ahomodimer mediated by the NLS. Subsequently, ligand-activat-ed AR binds to specific androgen response elements in theDNA, recruits coregulatory proteins to the promoter of andro-gen-responsive genes, and ultimately coactivates the transcrip-tion of these genes (Figure 2).[10]
Nonsteroidal Antiandrogens
Since the growth of prostate and primary prostate tumors, andthe inhibition of apoptosis, depend largely on androgens,[11]
the early standard therapy, such as castration proposed byHuggins and Hodges in the early 1940s, relied on removing an-drogens.[12] Subsequently, surgical castration or the use of lutei-nizing-hormone-releasing hormone (medical castration), incombination with antiandrogens for advanced prostate cancerwere used widely. Although most patients initially respondedto this therapy, eventually, clinically fatal androgen-independ-ent disease (also known as castration-resistant cancer) devel-oped frequently.[13] In addition, some undesirable side effectsrelated to the conventional hormone therapy, such as de-creased libido and impotence, hot flashes, lethargy and muscleweakness were also reported.[14] Although the precise mecha-nism remains unclear,[15] several have been proposed regardingthe causes of castration-resistant cancer, and these hypothesesconverged at the level of the AR.[16] Moreover, the mutation oramplification of the AR was sufficient to lead the PCa to con-vert from the hormone-sensitive to the hormone-refractorystage.[17] Thus, we can conclude that the AR is a central themein the progression of prostate cancer, and targeting the AR re-mains a hot research topic in the design and development ofantiprostate cancer drugs.
Currently, the antiandrogens can be classified as steroidaland nonsteroidal based on their structures. However, poor se-lectivity and pharmacokinetic properties, and low oral bioavail-ability, as well as side effects, such as potential hepatotoxicityand cross-reactivity with other steroid receptors, have limitedthe use of many steroidal AR antagonists, while nonsteroidalantagonists can overcome these problems to a degree. For ex-ample, flutamide (1) and the corresponding metabolite hydroxy-
flutamide (4), R-bicalutamide (2) and nilutamide (3), have beenapproved as the first-generation typical antiandrogens for ad-vanced PCa or hyperplasia in 1989, 1995 and 1996, respective-ly.[18] Though these compounds can extend the life of patients
in some case, there are still some side effects, especially hepa-totoxicity, that limits their use in patients.[19] Interestingly, allthese drugs have been ultimately observed to convert to ago-nists in clinical use.[20] Thus, it is necessary to design and syn-thesize new nonsteroidal antiandrogens for the treatment ofadvanced PCa. This paper will review the design strategy ofdifferent types of antiandrogens targeting the AR, as well astheir representative compounds, most of which have not yetbeen evaluated clinically but have shown potent antiandrogenactivity in vitro and in preclinical trials.
Bicalutamide derivatives
Among the three clinical drugs referred to above, R-bicalut-amide (2) has fewer side effects, and it is the most extensivelystudied.[21] Some studies have indicated that relatively simpleoptimization of R-bicalutamide (2) can yield nonsteroidal ago-nists with high binding affinity because of the stereoselectiveand regioselective binding to the AR. This can be achievedwithout producing antagonists, since the drug activity is sensi-tive to small changes in the structure.[18b, 22] Substituting the ar-omatic B-ring, or replacing the sulfonyl functionality withsulfur, oxygen or nitrogen is not a desirable strategy to obtaina promising antiandrogen. Most of the simply modified bi-calutamide derivatives with partial agonist activity can targetAR in different tissues to achieve desirable AR action, minimiz-ing undesirable side effects. They act as selective androgen re-ceptor modulators (SARMs) for the treatment of androgen-de-pendent diseases, such as muscle wasting, osteoporosis,benign prostatic hyperplasia and PCa.[23] The SARMs have beenpreviously reviewed extensively.[24]
The cocrystal structure of R-bicalutamide (2) interacting withthe mutant W741L AR LBD has been solved.[18a] The three-dimensional structure demonstrates that this mutation canconfer agonist activity to R-bicalutamide (2), and lead to clini-cal antiandrogen withdrawal syndrome, wherein antiandrogen-resistant patients show symptomatic improvement after cessa-tion of antiandrogen treatment. In the cocrystal structure, the
Figure 2. The androgen receptor signaling pathway.
1652 www.chemmedchem.org � 2010 Wiley-VCH Verlag GmbH & Co. KGaA, Weinheim ChemMedChem 2010, 5, 1651 – 1661
MED G. Zhao et al.
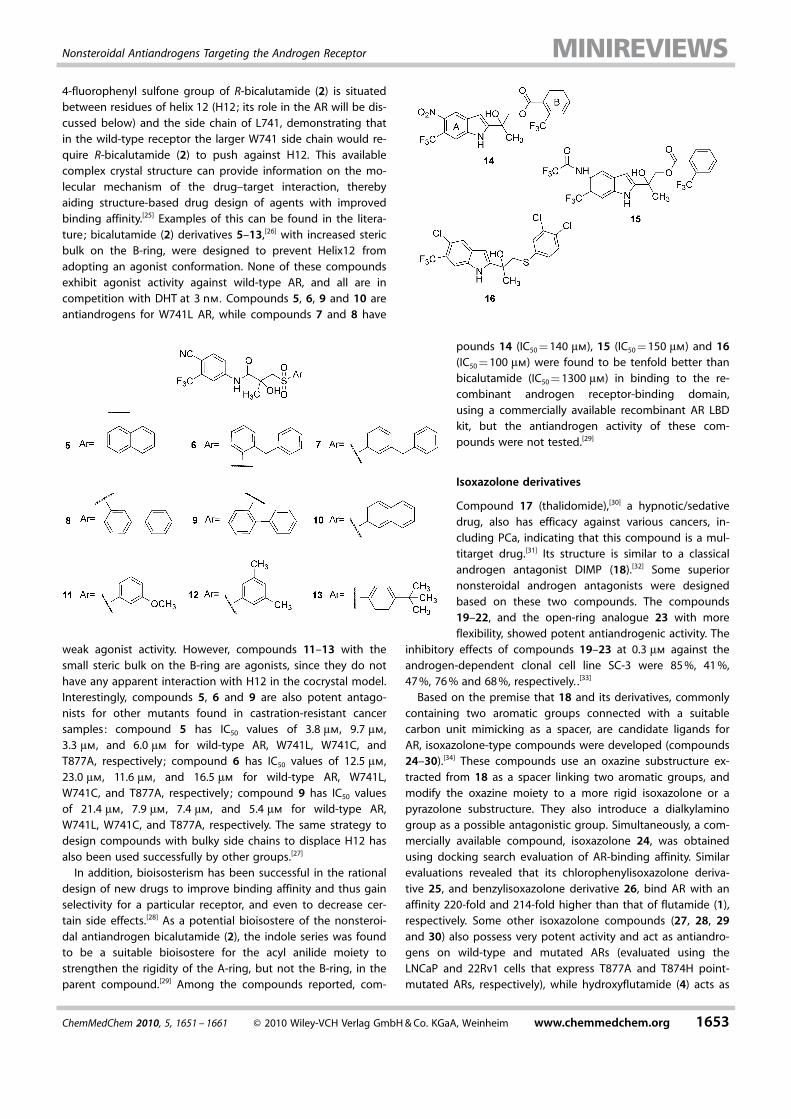
4-fluorophenyl sulfone group of R-bicalutamide (2) is situatedbetween residues of helix 12 (H12; its role in the AR will be dis-cussed below) and the side chain of L741, demonstrating thatin the wild-type receptor the larger W741 side chain would re-quire R-bicalutamide (2) to push against H12. This availablecomplex crystal structure can provide information on the mo-lecular mechanism of the drug–target interaction, therebyaiding structure-based drug design of agents with improvedbinding affinity.[25] Examples of this can be found in the litera-ture; bicalutamide (2) derivatives 5–13,[26] with increased stericbulk on the B-ring, were designed to prevent Helix12 fromadopting an agonist conformation. None of these compoundsexhibit agonist activity against wild-type AR, and all are incompetition with DHT at 3 nm. Compounds 5, 6, 9 and 10 areantiandrogens for W741L AR, while compounds 7 and 8 have
weak agonist activity. However, compounds 11–13 with thesmall steric bulk on the B-ring are agonists, since they do nothave any apparent interaction with H12 in the cocrystal model.Interestingly, compounds 5, 6 and 9 are also potent antago-nists for other mutants found in castration-resistant cancersamples: compound 5 has IC50 values of 3.8 mm, 9.7 mm,3.3 mm, and 6.0 mm for wild-type AR, W741L, W741C, andT877A, respectively; compound 6 has IC50 values of 12.5 mm,23.0 mm, 11.6 mm, and 16.5 mm for wild-type AR, W741L,W741C, and T877A, respectively ; compound 9 has IC50 valuesof 21.4 mm, 7.9 mm, 7.4 mm, and 5.4 mm for wild-type AR,W741L, W741C, and T877A, respectively. The same strategy todesign compounds with bulky side chains to displace H12 hasalso been used successfully by other groups.[27]
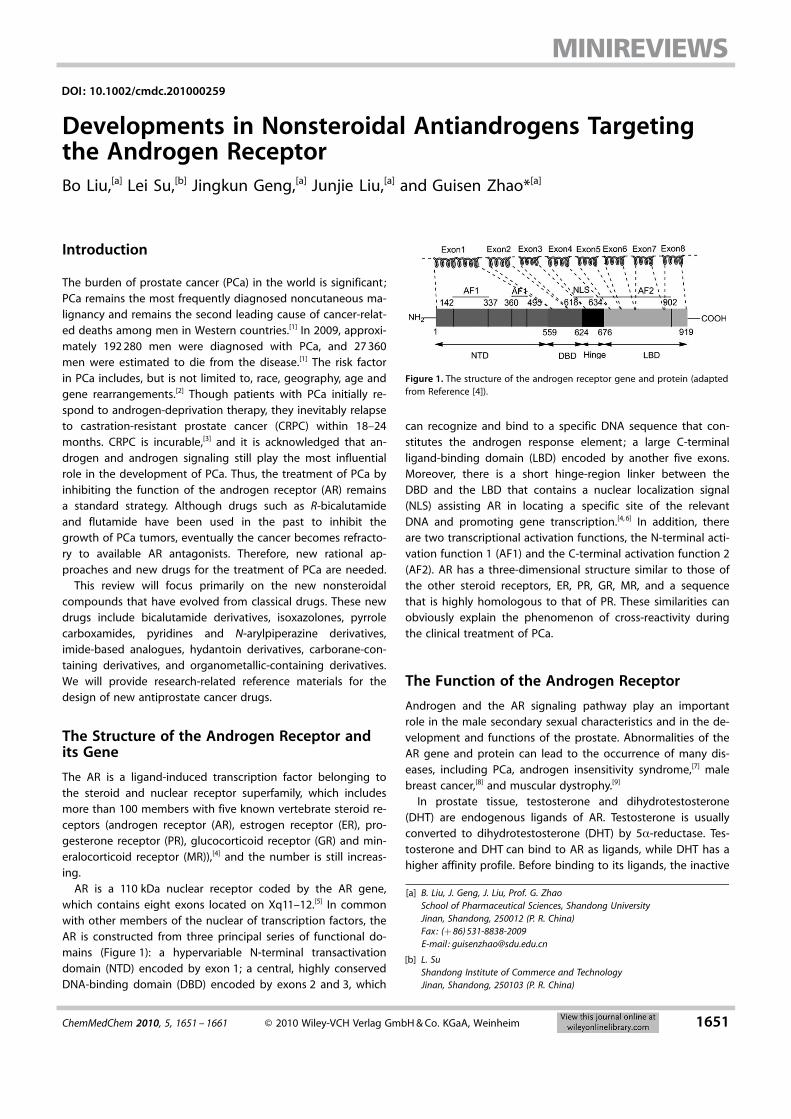
In addition, bioisosterism has been successful in the rationaldesign of new drugs to improve binding affinity and thus gainselectivity for a particular receptor, and even to decrease cer-tain side effects.[28] As a potential bioisostere of the nonsteroi-dal antiandrogen bicalutamide (2), the indole series was foundto be a suitable bioisostere for the acyl anilide moiety tostrengthen the rigidity of the A-ring, but not the B-ring, in theparent compound.[29] Among the compounds reported, com-
pounds 14 (IC50 = 140 mm), 15 (IC50 = 150 mm) and 16(IC50 = 100 mm) were found to be tenfold better thanbicalutamide (IC50 = 1300 mm) in binding to the re-combinant androgen receptor-binding domain,using a commercially available recombinant AR LBDkit, but the antiandrogen activity of these com-pounds were not tested.[29]
Isoxazolone derivatives
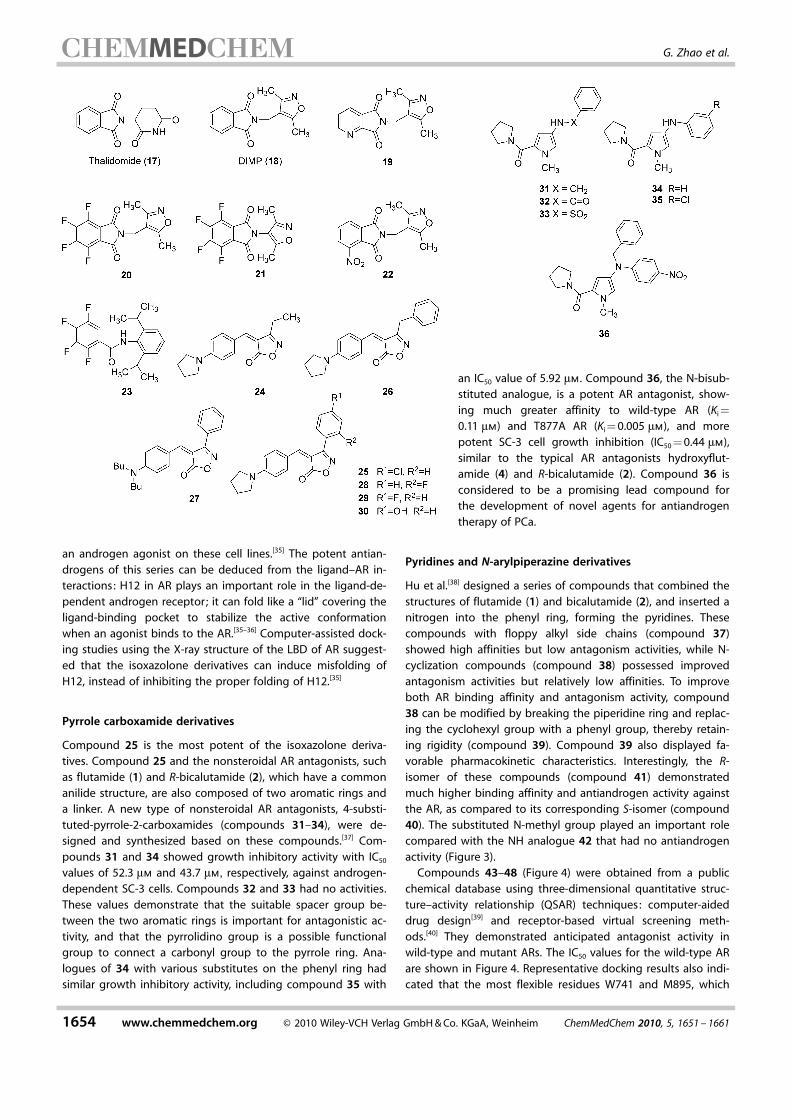
Compound 17 (thalidomide),[30] a hypnotic/sedativedrug, also has efficacy against various cancers, in-cluding PCa, indicating that this compound is a mul-titarget drug.[31] Its structure is similar to a classicalandrogen antagonist DIMP (18).[32] Some superiornonsteroidal androgen antagonists were designedbased on these two compounds. The compounds19–22, and the open-ring analogue 23 with moreflexibility, showed potent antiandrogenic activity. The
inhibitory effects of compounds 19–23 at 0.3 mm against theandrogen-dependent clonal cell line SC-3 were 85 %, 41 %,47 %, 76 % and 68 %, respectively. .[33]
Based on the premise that 18 and its derivatives, commonlycontaining two aromatic groups connected with a suitablecarbon unit mimicking as a spacer, are candidate ligands forAR, isoxazolone-type compounds were developed (compounds24–30).[34] These compounds use an oxazine substructure ex-tracted from 18 as a spacer linking two aromatic groups, andmodify the oxazine moiety to a more rigid isoxazolone or apyrazolone substructure. They also introduce a dialkylaminogroup as a possible antagonistic group. Simultaneously, a com-mercially available compound, isoxazolone 24, was obtainedusing docking search evaluation of AR-binding affinity. Similarevaluations revealed that its chlorophenylisoxazolone deriva-tive 25, and benzylisoxazolone derivative 26, bind AR with anaffinity 220-fold and 214-fold higher than that of flutamide (1),respectively. Some other isoxazolone compounds (27, 28, 29and 30) also possess very potent activity and act as antiandro-gens on wild-type and mutated ARs (evaluated using theLNCaP and 22Rv1 cells that express T877A and T874H point-mutated ARs, respectively), while hydroxyflutamide (4) acts as
ChemMedChem 2010, 5, 1651 – 1661 � 2010 Wiley-VCH Verlag GmbH & Co. KGaA, Weinheim www.chemmedchem.org 1653
Nonsteroidal Antiandrogens Targeting the Androgen Receptor
an androgen agonist on these cell lines.[35] The potent antian-drogens of this series can be deduced from the ligand–AR in-teractions: H12 in AR plays an important role in the ligand-de-pendent androgen receptor; it can fold like a “lid” covering theligand-binding pocket to stabilize the active conformationwhen an agonist binds to the AR.[35–36] Computer-assisted dock-ing studies using the X-ray structure of the LBD of AR suggest-ed that the isoxazolone derivatives can induce misfolding ofH12, instead of inhibiting the proper folding of H12.[35]
Pyrrole carboxamide derivatives
Compound 25 is the most potent of the isoxazolone deriva-tives. Compound 25 and the nonsteroidal AR antagonists, suchas flutamide (1) and R-bicalutamide (2), which have a commonanilide structure, are also composed of two aromatic rings anda linker. A new type of nonsteroidal AR antagonists, 4-substi-tuted-pyrrole-2-carboxamides (compounds 31–34), were de-signed and synthesized based on these compounds.[37] Com-pounds 31 and 34 showed growth inhibitory activity with IC50
values of 52.3 mm and 43.7 mm, respectively, against androgen-dependent SC-3 cells. Compounds 32 and 33 had no activities.These values demonstrate that the suitable spacer group be-tween the two aromatic rings is important for antagonistic ac-tivity, and that the pyrrolidino group is a possible functionalgroup to connect a carbonyl group to the pyrrole ring. Ana-logues of 34 with various substitutes on the phenyl ring hadsimilar growth inhibitory activity, including compound 35 with
an IC50 value of 5.92 mm. Compound 36, the N-bisub-stituted analogue, is a potent AR antagonist, show-ing much greater affinity to wild-type AR (Ki =
0.11 mm) and T877A AR (Ki = 0.005 mm), and morepotent SC-3 cell growth inhibition (IC50 = 0.44 mm),similar to the typical AR antagonists hydroxyflut-amide (4) and R-bicalutamide (2). Compound 36 isconsidered to be a promising lead compound forthe development of novel agents for antiandrogentherapy of PCa.
Pyridines and N-arylpiperazine derivatives
Hu et al.[38] designed a series of compounds that combined thestructures of flutamide (1) and bicalutamide (2), and inserted anitrogen into the phenyl ring, forming the pyridines. Thesecompounds with floppy alkyl side chains (compound 37)showed high affinities but low antagonism activities, while N-cyclization compounds (compound 38) possessed improvedantagonism activities but relatively low affinities. To improveboth AR binding affinity and antagonism activity, compound38 can be modified by breaking the piperidine ring and replac-ing the cyclohexyl group with a phenyl group, thereby retain-ing rigidity (compound 39). Compound 39 also displayed fa-vorable pharmacokinetic characteristics. Interestingly, the R-isomer of these compounds (compound 41) demonstratedmuch higher binding affinity and antiandrogen activity againstthe AR, as compared to its corresponding S-isomer (compound40). The substituted N-methyl group played an important rolecompared with the NH analogue 42 that had no antiandrogenactivity (Figure 3).
Compounds 43–48 (Figure 4) were obtained from a publicchemical database using three-dimensional quantitative struc-ture–activity relationship (QSAR) techniques: computer-aideddrug design[39] and receptor-based virtual screening meth-ods.[40] They demonstrated anticipated antagonist activity inwild-type and mutant ARs. The IC50 values for the wild-type ARare shown in Figure 4. Representative docking results also indi-cated that the most flexible residues W741 and M895, which
1654 www.chemmedchem.org � 2010 Wiley-VCH Verlag GmbH & Co. KGaA, Weinheim ChemMedChem 2010, 5, 1651 – 1661
MED G. Zhao et al.
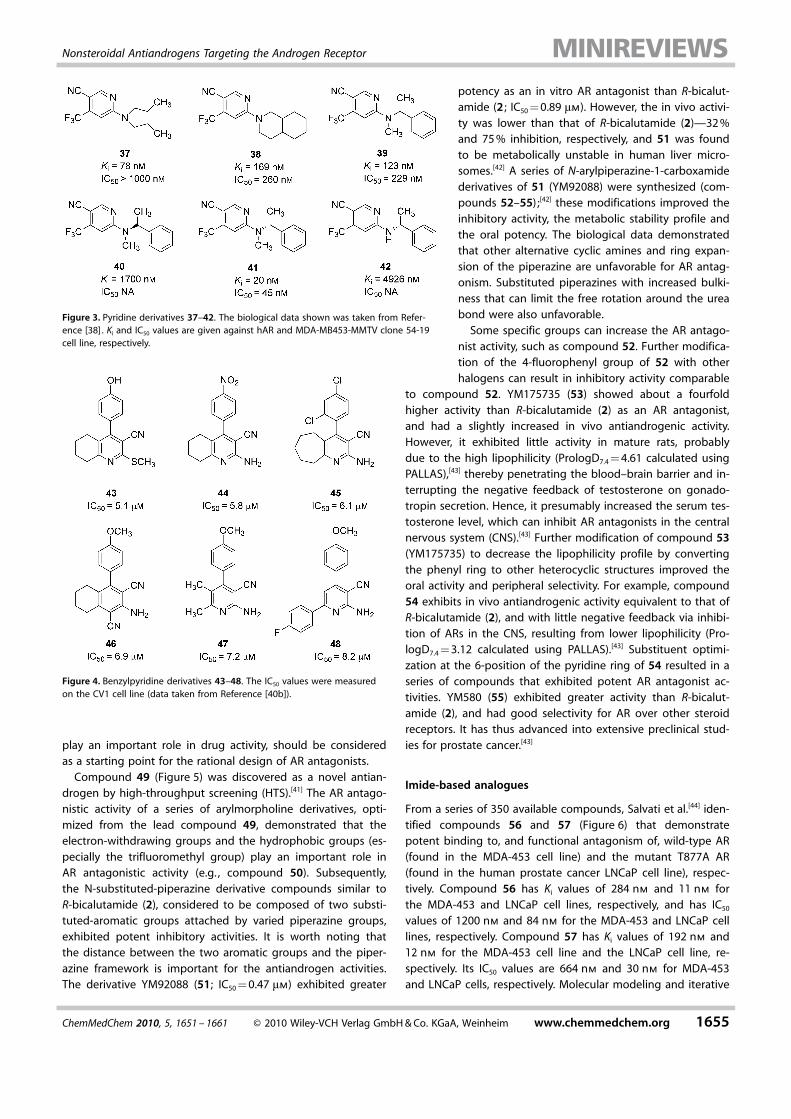
play an important role in drug activity, should be consideredas a starting point for the rational design of AR antagonists.
Compound 49 (Figure 5) was discovered as a novel antian-drogen by high-throughput screening (HTS).[41] The AR antago-nistic activity of a series of arylmorpholine derivatives, opti-mized from the lead compound 49, demonstrated that theelectron-withdrawing groups and the hydrophobic groups (es-pecially the trifluoromethyl group) play an important role inAR antagonistic activity (e.g. , compound 50). Subsequently,the N-substituted-piperazine derivative compounds similar toR-bicalutamide (2), considered to be composed of two substi-tuted-aromatic groups attached by varied piperazine groups,exhibited potent inhibitory activities. It is worth noting thatthe distance between the two aromatic groups and the piper-azine framework is important for the antiandrogen activities.The derivative YM92088 (51; IC50 = 0.47 mm) exhibited greater
potency as an in vitro AR antagonist than R-bicalut-amide (2 ; IC50 = 0.89 mm). However, the in vivo activi-ty was lower than that of R-bicalutamide (2)—32 %and 75 % inhibition, respectively, and 51 was foundto be metabolically unstable in human liver micro-somes.[42] A series of N-arylpiperazine-1-carboxamidederivatives of 51 (YM92088) were synthesized (com-pounds 52–55) ;[42] these modifications improved theinhibitory activity, the metabolic stability profile andthe oral potency. The biological data demonstratedthat other alternative cyclic amines and ring expan-sion of the piperazine are unfavorable for AR antag-onism. Substituted piperazines with increased bulki-ness that can limit the free rotation around the ureabond were also unfavorable.
Some specific groups can increase the AR antago-nist activity, such as compound 52. Further modifica-tion of the 4-fluorophenyl group of 52 with otherhalogens can result in inhibitory activity comparable
to compound 52. YM175735 (53) showed about a fourfoldhigher activity than R-bicalutamide (2) as an AR antagonist,and had a slightly increased in vivo antiandrogenic activity.However, it exhibited little activity in mature rats, probablydue to the high lipophilicity (PrologD7.4 = 4.61 calculated usingPALLAS),[43] thereby penetrating the blood–brain barrier and in-terrupting the negative feedback of testosterone on gonado-tropin secretion. Hence, it presumably increased the serum tes-tosterone level, which can inhibit AR antagonists in the centralnervous system (CNS).[43] Further modification of compound 53(YM175735) to decrease the lipophilicity profile by convertingthe phenyl ring to other heterocyclic structures improved theoral activity and peripheral selectivity. For example, compound54 exhibits in vivo antiandrogenic activity equivalent to that ofR-bicalutamide (2), and with little negative feedback via inhibi-tion of ARs in the CNS, resulting from lower lipophilicity (Pro-logD7.4 = 3.12 calculated using PALLAS).[43] Substituent optimi-zation at the 6-position of the pyridine ring of 54 resulted in aseries of compounds that exhibited potent AR antagonist ac-tivities. YM580 (55) exhibited greater activity than R-bicalut-amide (2), and had good selectivity for AR over other steroidreceptors. It has thus advanced into extensive preclinical stud-ies for prostate cancer.[43]
Imide-based analogues
From a series of 350 available compounds, Salvati et al.[44] iden-tified compounds 56 and 57 (Figure 6) that demonstratepotent binding to, and functional antagonism of, wild-type AR(found in the MDA-453 cell line) and the mutant T877A AR(found in the human prostate cancer LNCaP cell line), respec-tively. Compound 56 has Ki values of 284 nm and 11 nm forthe MDA-453 and LNCaP cell lines, respectively, and has IC50
values of 1200 nm and 84 nm for the MDA-453 and LNCaP celllines, respectively. Compound 57 has Ki values of 192 nm and12 nm for the MDA-453 cell line and the LNCaP cell line, re-spectively. Its IC50 values are 664 nm and 30 nm for MDA-453and LNCaP cells, respectively. Molecular modeling and iterative
Figure 3. Pyridine derivatives 37–42. The biological data shown was taken from Refer-ence [38] . Ki and IC50 values are given against hAR and MDA-MB453-MMTV clone 54-19cell line, respectively.
Figure 4. Benzylpyridine derivatives 43–48. The IC50 values were measuredon the CV1 cell line (data taken from Reference [40b]).
ChemMedChem 2010, 5, 1651 – 1661 � 2010 Wiley-VCH Verlag GmbH & Co. KGaA, Weinheim www.chemmedchem.org 1655
Nonsteroidal Antiandrogens Targeting the Androgen Receptor
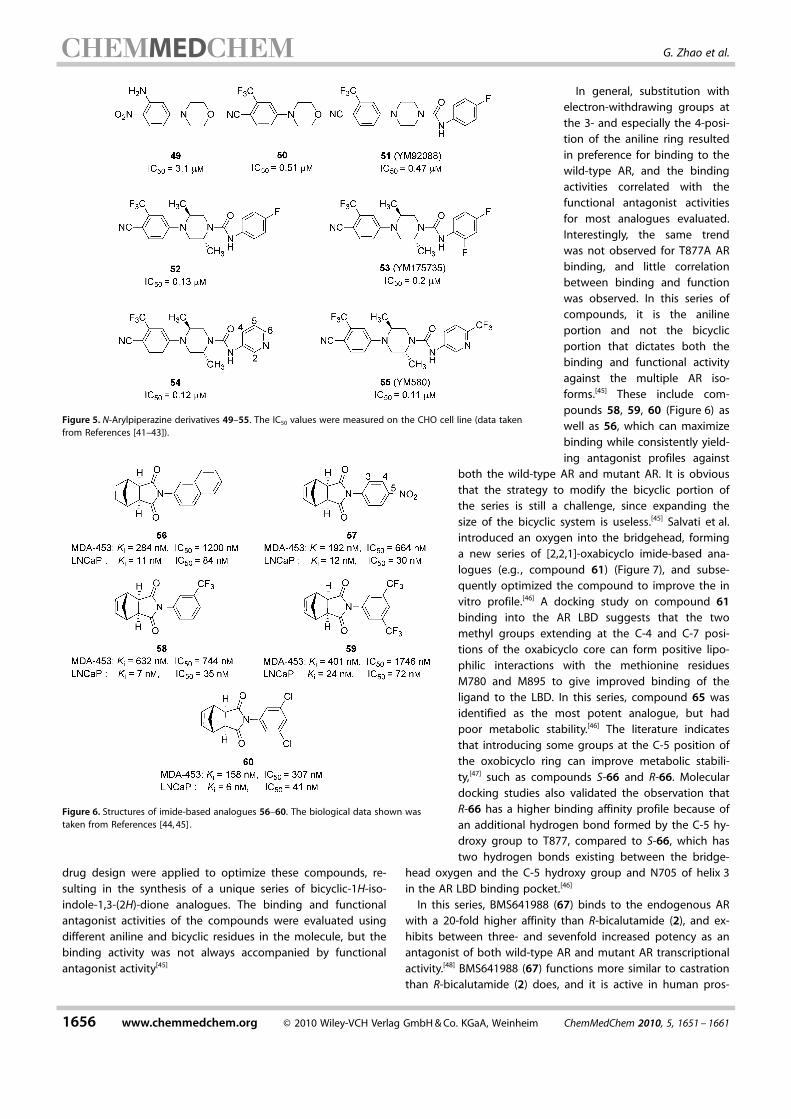
drug design were applied to optimize these compounds, re-sulting in the synthesis of a unique series of bicyclic-1H-iso-indole-1,3-(2H)-dione analogues. The binding and functionalantagonist activities of the compounds were evaluated usingdifferent aniline and bicyclic residues in the molecule, but thebinding activity was not always accompanied by functionalantagonist activity[45]
In general, substitution withelectron-withdrawing groups atthe 3- and especially the 4-posi-tion of the aniline ring resultedin preference for binding to thewild-type AR, and the bindingactivities correlated with thefunctional antagonist activitiesfor most analogues evaluated.Interestingly, the same trendwas not observed for T877A ARbinding, and little correlationbetween binding and functionwas observed. In this series ofcompounds, it is the anilineportion and not the bicyclicportion that dictates both thebinding and functional activityagainst the multiple AR iso-forms.[45] These include com-pounds 58, 59, 60 (Figure 6) aswell as 56, which can maximizebinding while consistently yield-ing antagonist profiles against
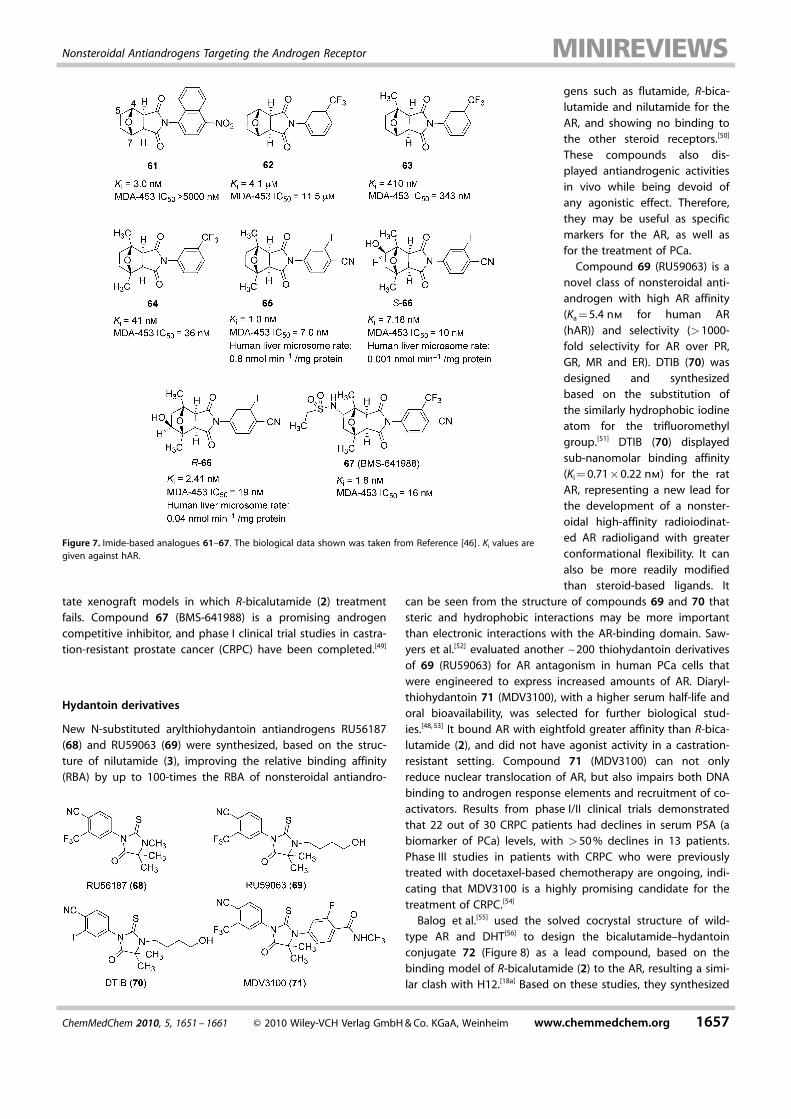
both the wild-type AR and mutant AR. It is obviousthat the strategy to modify the bicyclic portion ofthe series is still a challenge, since expanding thesize of the bicyclic system is useless.[45] Salvati et al.introduced an oxygen into the bridgehead, forminga new series of [2,2,1]-oxabicyclo imide-based ana-logues (e.g. , compound 61) (Figure 7), and subse-quently optimized the compound to improve the invitro profile.[46] A docking study on compound 61binding into the AR LBD suggests that the twomethyl groups extending at the C-4 and C-7 posi-tions of the oxabicyclo core can form positive lipo-philic interactions with the methionine residuesM780 and M895 to give improved binding of theligand to the LBD. In this series, compound 65 wasidentified as the most potent analogue, but hadpoor metabolic stability.[46] The literature indicatesthat introducing some groups at the C-5 position ofthe oxobicyclo ring can improve metabolic stabili-ty,[47] such as compounds S-66 and R-66. Moleculardocking studies also validated the observation thatR-66 has a higher binding affinity profile because ofan additional hydrogen bond formed by the C-5 hy-droxy group to T877, compared to S-66, which hastwo hydrogen bonds existing between the bridge-
head oxygen and the C-5 hydroxy group and N705 of helix 3in the AR LBD binding pocket.[46]
In this series, BMS641988 (67) binds to the endogenous ARwith a 20-fold higher affinity than R-bicalutamide (2), and ex-hibits between three- and sevenfold increased potency as anantagonist of both wild-type AR and mutant AR transcriptionalactivity.[48] BMS641988 (67) functions more similar to castrationthan R-bicalutamide (2) does, and it is active in human pros-
Figure 5. N-Arylpiperazine derivatives 49–55. The IC50 values were measured on the CHO cell line (data takenfrom References [41–43]).
Figure 6. Structures of imide-based analogues 56–60. The biological data shown wastaken from References [44, 45] .
1656 www.chemmedchem.org � 2010 Wiley-VCH Verlag GmbH & Co. KGaA, Weinheim ChemMedChem 2010, 5, 1651 – 1661
MED G. Zhao et al.
tate xenograft models in which R-bicalutamide (2) treatmentfails. Compound 67 (BMS-641988) is a promising androgencompetitive inhibitor, and phase I clinical trial studies in castra-tion-resistant prostate cancer (CRPC) have been completed.[49]
Hydantoin derivatives
New N-substituted arylthiohydantoin antiandrogens RU56187(68) and RU59063 (69) were synthesized, based on the struc-ture of nilutamide (3), improving the relative binding affinity(RBA) by up to 100-times the RBA of nonsteroidal antiandro-
gens such as flutamide, R-bica-lutamide and nilutamide for theAR, and showing no binding tothe other steroid receptors.[50]
These compounds also dis-played antiandrogenic activitiesin vivo while being devoid ofany agonistic effect. Therefore,they may be useful as specificmarkers for the AR, as well asfor the treatment of PCa.
Compound 69 (RU59063) is anovel class of nonsteroidal anti-androgen with high AR affinity(Ka = 5.4 nm for human AR(hAR)) and selectivity (>1000-fold selectivity for AR over PR,GR, MR and ER). DTIB (70) wasdesigned and synthesizedbased on the substitution ofthe similarly hydrophobic iodineatom for the trifluoromethylgroup.[51] DTIB (70) displayedsub-nanomolar binding affinity(Ki = 0.71�0.22 nm) for the ratAR, representing a new lead forthe development of a nonster-oidal high-affinity radioiodinat-ed AR radioligand with greaterconformational flexibility. It canalso be more readily modifiedthan steroid-based ligands. It
can be seen from the structure of compounds 69 and 70 thatsteric and hydrophobic interactions may be more importantthan electronic interactions with the AR-binding domain. Saw-yers et al.[52] evaluated another ~200 thiohydantoin derivativesof 69 (RU59063) for AR antagonism in human PCa cells thatwere engineered to express increased amounts of AR. Diaryl-thiohydantoin 71 (MDV3100), with a higher serum half-life andoral bioavailability, was selected for further biological stud-ies.[48, 53] It bound AR with eightfold greater affinity than R-bica-lutamide (2), and did not have agonist activity in a castration-resistant setting. Compound 71 (MDV3100) can not onlyreduce nuclear translocation of AR, but also impairs both DNAbinding to androgen response elements and recruitment of co-activators. Results from phase I/II clinical trials demonstratedthat 22 out of 30 CRPC patients had declines in serum PSA (abiomarker of PCa) levels, with >50 % declines in 13 patients.Phase III studies in patients with CRPC who were previouslytreated with docetaxel-based chemotherapy are ongoing, indi-cating that MDV3100 is a highly promising candidate for thetreatment of CRPC.[54]
Balog et al.[55] used the solved cocrystal structure of wild-type AR and DHT[56] to design the bicalutamide–hydantoinconjugate 72 (Figure 8) as a lead compound, based on thebinding model of R-bicalutamide (2) to the AR, resulting a simi-lar clash with H12.[18a] Based on these studies, they synthesized
Figure 7. Imide-based analogues 61–67. The biological data shown was taken from Reference [46] . Ki values aregiven against hAR.
ChemMedChem 2010, 5, 1651 – 1661 � 2010 Wiley-VCH Verlag GmbH & Co. KGaA, Weinheim www.chemmedchem.org 1657
Nonsteroidal Antiandrogens Targeting the Androgen Receptor
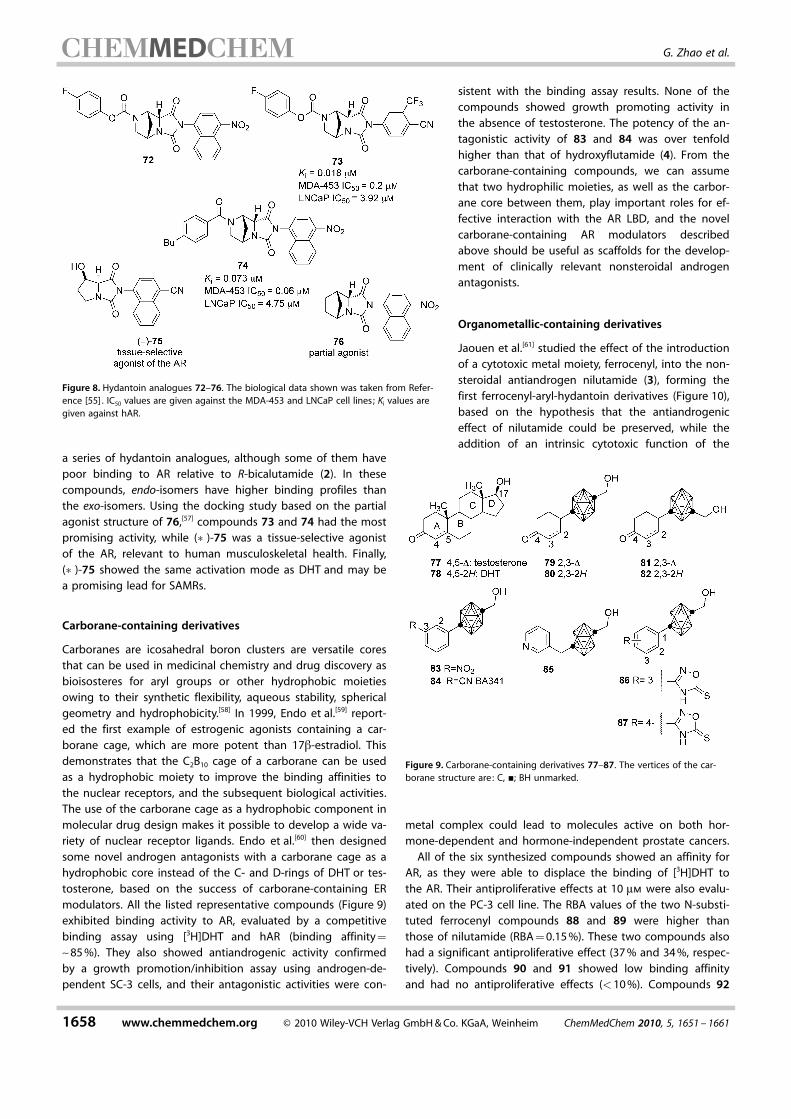
a series of hydantoin analogues, although some of them havepoor binding to AR relative to R-bicalutamide (2). In thesecompounds, endo-isomers have higher binding profiles thanthe exo-isomers. Using the docking study based on the partialagonist structure of 76,[57] compounds 73 and 74 had the mostpromising activity, while (�)-75 was a tissue-selective agonistof the AR, relevant to human musculoskeletal health. Finally,(�)-75 showed the same activation mode as DHT and may bea promising lead for SAMRs.
Carborane-containing derivatives
Carboranes are icosahedral boron clusters are versatile coresthat can be used in medicinal chemistry and drug discovery asbioisosteres for aryl groups or other hydrophobic moietiesowing to their synthetic flexibility, aqueous stability, sphericalgeometry and hydrophobicity.[58] In 1999, Endo et al.[59] report-ed the first example of estrogenic agonists containing a car-borane cage, which are more potent than 17b-estradiol. Thisdemonstrates that the C2B10 cage of a carborane can be usedas a hydrophobic moiety to improve the binding affinities tothe nuclear receptors, and the subsequent biological activities.The use of the carborane cage as a hydrophobic component inmolecular drug design makes it possible to develop a wide va-riety of nuclear receptor ligands. Endo et al.[60] then designedsome novel androgen antagonists with a carborane cage as ahydrophobic core instead of the C- and D-rings of DHT or tes-tosterone, based on the success of carborane-containing ERmodulators. All the listed representative compounds (Figure 9)exhibited binding activity to AR, evaluated by a competitivebinding assay using [3H]DHT and hAR (binding affinity=
~85 %). They also showed antiandrogenic activity confirmedby a growth promotion/inhibition assay using androgen-de-pendent SC-3 cells, and their antagonistic activities were con-
sistent with the binding assay results. None of thecompounds showed growth promoting activity inthe absence of testosterone. The potency of the an-tagonistic activity of 83 and 84 was over tenfoldhigher than that of hydroxyflutamide (4). From thecarborane-containing compounds, we can assumethat two hydrophilic moieties, as well as the carbor-ane core between them, play important roles for ef-fective interaction with the AR LBD, and the novelcarborane-containing AR modulators describedabove should be useful as scaffolds for the develop-ment of clinically relevant nonsteroidal androgenantagonists.
Organometallic-containing derivatives
Jaouen et al.[61] studied the effect of the introductionof a cytotoxic metal moiety, ferrocenyl, into the non-steroidal antiandrogen nilutamide (3), forming thefirst ferrocenyl-aryl-hydantoin derivatives (Figure 10),based on the hypothesis that the antiandrogeniceffect of nilutamide could be preserved, while theaddition of an intrinsic cytotoxic function of the
metal complex could lead to molecules active on both hor-mone-dependent and hormone-independent prostate cancers.
All of the six synthesized compounds showed an affinity forAR, as they were able to displace the binding of [3H]DHT tothe AR. Their antiproliferative effects at 10 mm were also evalu-ated on the PC-3 cell line. The RBA values of the two N-substi-tuted ferrocenyl compounds 88 and 89 were higher thanthose of nilutamide (RBA = 0.15 %). These two compounds alsohad a significant antiproliferative effect (37 % and 34 %, respec-tively). Compounds 90 and 91 showed low binding affinityand had no antiproliferative effects (<10 %). Compounds 92
Figure 8. Hydantoin analogues 72–76. The biological data shown was taken from Refer-ence [55] . IC50 values are given against the MDA-453 and LNCaP cell lines; Ki values aregiven against hAR.
Figure 9. Carborane-containing derivatives 77–87. The vertices of the car-borane structure are: C, &; BH unmarked.
1658 www.chemmedchem.org � 2010 Wiley-VCH Verlag GmbH & Co. KGaA, Weinheim ChemMedChem 2010, 5, 1651 – 1661
MED G. Zhao et al.
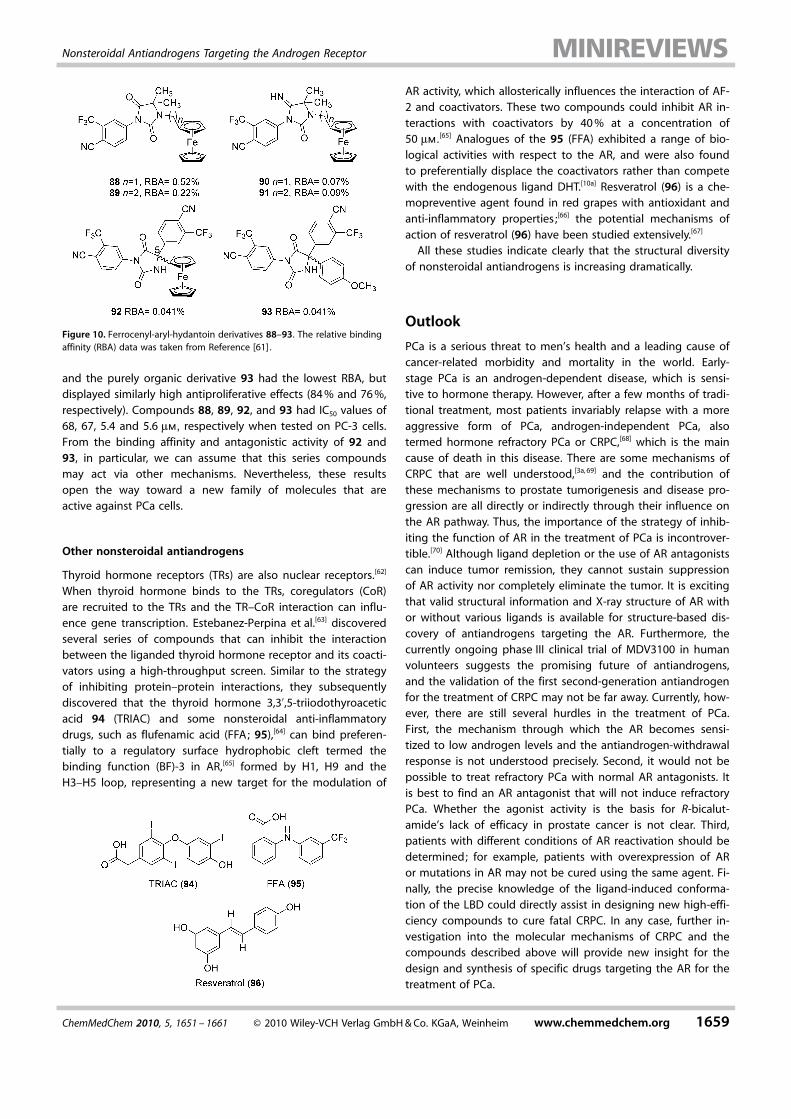
and the purely organic derivative 93 had the lowest RBA, butdisplayed similarly high antiproliferative effects (84 % and 76 %,respectively). Compounds 88, 89, 92, and 93 had IC50 values of68, 67, 5.4 and 5.6 mm, respectively when tested on PC-3 cells.From the binding affinity and antagonistic activity of 92 and93, in particular, we can assume that this series compoundsmay act via other mechanisms. Nevertheless, these resultsopen the way toward a new family of molecules that areactive against PCa cells.
Other nonsteroidal antiandrogens
Thyroid hormone receptors (TRs) are also nuclear receptors.[62]
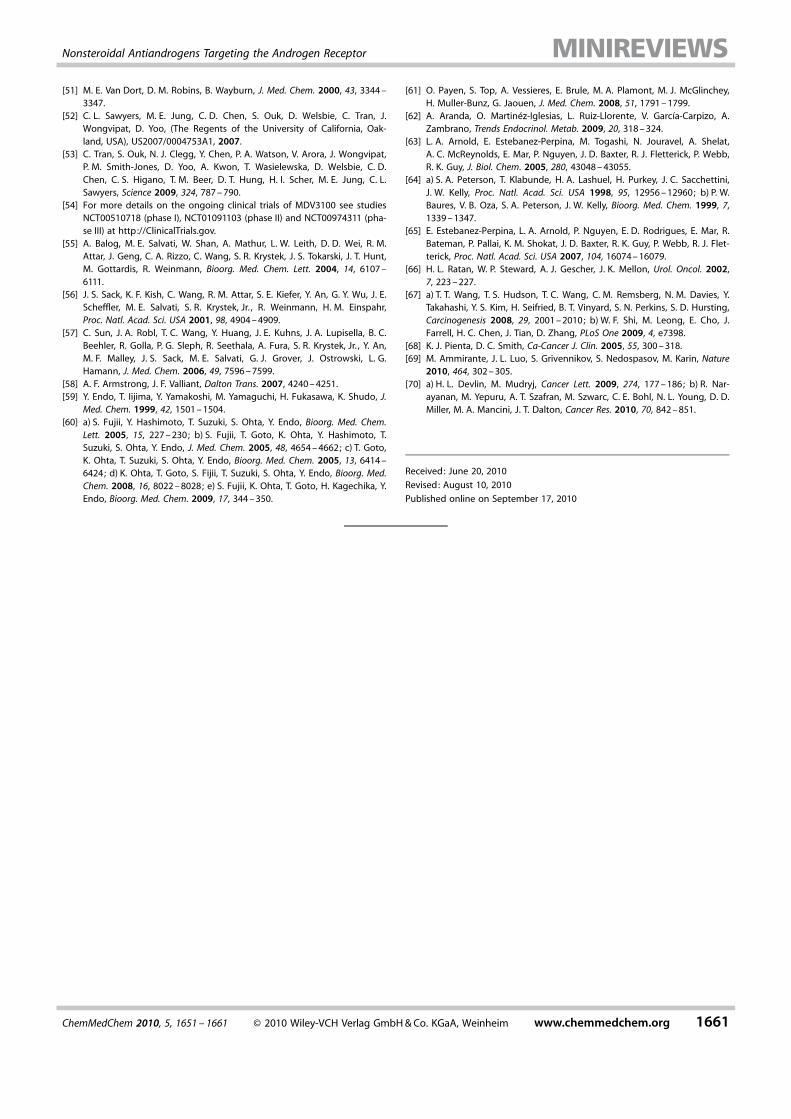
When thyroid hormone binds to the TRs, coregulators (CoR)are recruited to the TRs and the TR–CoR interaction can influ-ence gene transcription. Estebanez-Perpina et al.[63] discoveredseveral series of compounds that can inhibit the interactionbetween the liganded thyroid hormone receptor and its coacti-vators using a high-throughput screen. Similar to the strategyof inhibiting protein–protein interactions, they subsequentlydiscovered that the thyroid hormone 3,3’,5-triiodothyroaceticacid 94 (TRIAC) and some nonsteroidal anti-inflammatorydrugs, such as flufenamic acid (FFA; 95),[64] can bind preferen-tially to a regulatory surface hydrophobic cleft termed thebinding function (BF)-3 in AR,[65] formed by H1, H9 and theH3–H5 loop, representing a new target for the modulation of
AR activity, which allosterically influences the interaction of AF-2 and coactivators. These two compounds could inhibit AR in-teractions with coactivators by 40 % at a concentration of50 mm.
[65] Analogues of the 95 (FFA) exhibited a range of bio-logical activities with respect to the AR, and were also foundto preferentially displace the coactivators rather than competewith the endogenous ligand DHT.[10a] Resveratrol (96) is a che-mopreventive agent found in red grapes with antioxidant andanti-inflammatory properties ;[66] the potential mechanisms ofaction of resveratrol (96) have been studied extensively.[67]
All these studies indicate clearly that the structural diversityof nonsteroidal antiandrogens is increasing dramatically.
Outlook
PCa is a serious threat to men’s health and a leading cause ofcancer-related morbidity and mortality in the world. Early-stage PCa is an androgen-dependent disease, which is sensi-tive to hormone therapy. However, after a few months of tradi-tional treatment, most patients invariably relapse with a moreaggressive form of PCa, androgen-independent PCa, alsotermed hormone refractory PCa or CRPC,[68] which is the maincause of death in this disease. There are some mechanisms ofCRPC that are well understood,[3a, 69] and the contribution ofthese mechanisms to prostate tumorigenesis and disease pro-gression are all directly or indirectly through their influence onthe AR pathway. Thus, the importance of the strategy of inhib-iting the function of AR in the treatment of PCa is incontrover-tible.[70] Although ligand depletion or the use of AR antagonistscan induce tumor remission, they cannot sustain suppressionof AR activity nor completely eliminate the tumor. It is excitingthat valid structural information and X-ray structure of AR withor without various ligands is available for structure-based dis-covery of antiandrogens targeting the AR. Furthermore, thecurrently ongoing phase III clinical trial of MDV3100 in humanvolunteers suggests the promising future of antiandrogens,and the validation of the first second-generation antiandrogenfor the treatment of CRPC may not be far away. Currently, how-ever, there are still several hurdles in the treatment of PCa.First, the mechanism through which the AR becomes sensi-tized to low androgen levels and the antiandrogen-withdrawalresponse is not understood precisely. Second, it would not bepossible to treat refractory PCa with normal AR antagonists. Itis best to find an AR antagonist that will not induce refractoryPCa. Whether the agonist activity is the basis for R-bicalut-amide’s lack of efficacy in prostate cancer is not clear. Third,patients with different conditions of AR reactivation should bedetermined; for example, patients with overexpression of ARor mutations in AR may not be cured using the same agent. Fi-nally, the precise knowledge of the ligand-induced conforma-tion of the LBD could directly assist in designing new high-effi-ciency compounds to cure fatal CRPC. In any case, further in-vestigation into the molecular mechanisms of CRPC and thecompounds described above will provide new insight for thedesign and synthesis of specific drugs targeting the AR for thetreatment of PCa.
Figure 10. Ferrocenyl-aryl-hydantoin derivatives 88–93. The relative bindingaffinity (RBA) data was taken from Reference [61] .
ChemMedChem 2010, 5, 1651 – 1661 � 2010 Wiley-VCH Verlag GmbH & Co. KGaA, Weinheim www.chemmedchem.org 1659
Nonsteroidal Antiandrogens Targeting the Androgen Receptor

Acknowledgements
This work was supported by the National Natural Science Foun-dation of China (No. 20872082) and the Shandong Natural Sci-ence Foundation (No. Y2007C060).
Keywords: androgen signaling · drug design · nonsteroidalantiandrogens · prostate cancer · receptors
[1] A. Jemal, R. Siegel, E. Ward, Y. Hao, J. Xu, M. J. Thun, Ca-Cancer J. Clin.2009, 59, 225 – 249.
[2] C. M. Zeigler-Johnson, H. Rennert, R. D. Mittal, M. Jalloh, R. Sachdeva,S. B. Malkowicz, A. Mandhani, B. Mittal, S. M. Gueye, T. R. Rebbeck, Can.J. Urol. 2008, 15, 4056 – 4064.
[3] a) T. M. Morgan, T. D. Koreckij, E. Corey, Curr Cancer Drug Targets. 2009,9, 237 – 249; b) J. C. Yang, J. H. Ok, J. E. Busby, A. D. Borowsky, H. J.Kung, C. P. Evans, Cancer Res. 2009, 69, 151 – 160.
[4] W. Gao, C. E. Bohl, J. T. Dalton, Chem. Rev. 2005, 105, 3352 – 3370.[5] Y. Chen, C. L. Sawyers, H. I. Scher, Curr. Opin. Pharmacol. 2008, 8, 440 –
448.[6] F. Wang, X. Q. Liu, H. Li, K. N. Liang, J. N. Miner, M. Hong, E. A. Kallel, A.
van Oeveren, L. Zhi, T. Jiang, Acta Crystallogr. , Sect. F: Struct. Biol. Cryst.Commun. 2006, 62, 1067 – 1071.
[7] H. L. Rong, N. Suzuki, A. Imai, Eur. J. Obstet. Gynecol. Reprod. Biol. 2010,148, 53 – 55.
[8] K. Tiefenbacher, G. Daxenbichler, Breast Care 2008, 3, 325 – 331.[9] H. J. Ting, C. Chang, J. Steroid Biochem. Mol. Biol. 2008, 111, 157 – 163.
[10] a) C. F�au, L. A. Arnold, A. Kosinski, F. Zhu, M. Connelly, R. K. Guy, ACSChem. Biol. 2009, 4, 834 – 843; b) M. L. Cutress, H. C. Whitaker, I. G. Mills,M. Stewart, D. E. Neal, J. Cell Sci. 2008, 121, 957 – 968.
[11] R. M. Evans, Science 1988, 240, 889 – 895.[12] M. J. Linja, T. Visakorpi, J. Steroid Biochem. Mol. Biol. 2004, 92, 255 – 264.[13] P. Westin, P. Stattin, J. E. Damber, A. Bergh, Am. J. Pathol. 1995, 146,
1368 – 1375.[14] D. K. Ornstein, G. S. Rao, B. Johnson, E. T. Charlton, G. L. Andriole, Urolo-
gy 1996, 48, 901 – 905.[15] X. Yuan, S. P. Balk, Urol. Oncol. 2009, 27, 36 – 41.[16] a) K. E. Knudsen, H. I. Scher, Clin. Cancer Res. 2009, 15, 4792 – 4798;
b) S. S. Dutt, A. C. Gao, Future Oncol. 2009, 5, 1403 – 1413; c) N. Sharifi,W. L. Dahut, W. D. Figg, BJU Int. 2008, 101, 271 – 274; d) R. B. Montgom-ery, E. A. Mostaghel, R. Vessella, D. L. Hess, T. F. Kalhorn, C. S. Higano,L. D. True, P. S. Nelson, Cancer Res. 2008, 68, 4447 – 4454.
[17] M. E. Grossmann, H. Huang, D. J. Tindall, J. Natl. Cancer Inst. 2001, 93,1687 – 1697.
[18] a) C. E. Bohl, W. Gao, D. D. Miller, C. E. Bell, J. T. Dalton, Proc. Natl. Acad.Sci. USA 2005, 102, 6201 – 6206; b) J. T. Dalton, A. Mukherjee, Z. Zhu, L.Kirkovsky, D. D. Miller, Biochem. Biophys. Res. Commun. 1998, 244, 1 – 4.
[19] a) A. Decensi, D. Guarneri, M. C. Paoletti, J. M. Lalanne, F. Merlo, F. Boc-cardo, Eur. J. Cancer 1991, 27, 1100 – 1104; b) D. Fau, D. Eugene, A.Berson, P. Letteron, B. Fromenty, C. Fisch, D. Pessayre, J. Pharmacol. Exp.Ther. 1994, 269, 954 – 962; c) R. Kashimshetty, V. G. Desai, V. M. Kale, T.Lee, C. L. Moland, W. S. Branham, L. S. New, E. C. Chan, H. Younis, U. A.Boelsterli, Toxicol. Appl. Pharmacol. 2009, 238, 150 – 159.
[20] W. K. Kelly, H. I. Scher, J. Urol. 1993, 149, 607 – 609.[21] G. J. Kolvenbag, G. R. Blackledge, K. Gotting-Smith, Prostate 1998, 34,
61 – 72.[22] a) L. Kirkovsky, A. Mukherjee, D. Yin, J. T. Dalton, D. D. Miller, J. Med.
Chem. 2000, 43, 581 – 590; b) C. A. Marhefka, W. Gao, K. Chung, J. Kim, Y.He, D. Yin, C. Bohl, J. T. Dalton, D. D. Miller, J. Med. Chem. 2004, 47,993 – 998; c) C. E. Bohl, C. Chang, M. L. Mohler, J. Chen, D. D. Miller, P. W.Swaan, J. T. Dalton, J. Med. Chem. 2004, 47, 3765 – 3776; d) D. Yin, Y. He,M. A. Perera, S. S. Hong, C. Marhefka, N. Stourman, L. Kirkovsky, D. D.Miller, J. T. Dalton, Mol. Pharmacol. 2003, 63, 211 – 223.
[23] A. Negro-Vilar, J. Clin. Endocrinol. Metab. 1999, 84, 3459 – 3462.[24] a) X. Zhang, J. C. Lanter, Z. Sui, Expert Opin. Ther. Pat. 2009, 19, 1239 –
1258; b) M. Thevis, W. Sch�nzer, Handb. Exp. Pharmacol. 2009, 195, 99 –126; c) J. O. Jones, Expert Opin. Drug Discovery 2009, 4, 981 – 993.
[25] C. E. Bohl, Z. Wu, J. Chen, M. L. Mohler, J. Yang, D. J. Hwang, S. Mustafa,D. D. Miller, C. E. Bell, J. T. Dalton, Bioorg. Med. Chem. Lett. 2008, 18,5567 – 5570.
[26] P. L. McGinley, J. T. Koh, J. Am. Chem. Soc. 2007, 129, 3822 – 3823.[27] J. M. Zhou, G. Y. Geng, Q. W. Shi, F. Sauriol, J. H. Wu, J. Med. Chem. 2009,
52, 5546 – 5550.[28] L. M. Lima, E. J. Barreiro, Curr. Med. Chem. 2005, 12, 23 – 49.[29] J. C. Lanter, J. J. Fiordeliso, G. F. Allan, A. Musto, W. Hahn do, Z. Sui,
Bioorg. Med. Chem. Lett. 2006, 16, 5646 – 5649.[30] Y. Hashimoto, Arch. Pharm. 2008, 341, 536 – 547.[31] S. Romero, G. Stanton, J. DeFelice, F. Schreiber, R. Rago, M. Fishman,
Urol. Oncol. 2007, 13, 284 – 290.[32] A. Boris, J. W. Scott, L. DeMartino, D. C. Cox, Acta Endocrinol. 1973, 72,
604 – 614.[33] a) Y. Hashimoto, Mini-Rev. Med. Chem. 2002, 2, 543 – 551; b) Y. Hashimo-
to, Bioorg. Med. Chem. 2002, 10, 461 – 479.[34] T. Ishioka, A. Kubo, Y. Koiso, K. Nagasawa, A. Itai, Y. Hashimoto, Bioorg.
Med. Chem. 2002, 10, 1555 – 1566.[35] T. Ishioka, A. Tanatani, K. Nagasawa, Y. Hashimoto, Bioorg. Med. Chem.
Lett. 2003, 13, 2655 – 2658.[36] J. M. Wurtz, W. Bourguet, J. P. Renaud, V. Vivat, P. Chambon, D. Moras, H.
Gronemeyer, Nat. Struct. Biol. 1996, 3, 87 – 94.[37] a) K. Wakabayashi, H. Miyachi, Y. Hashimoto, A. Tanatani, Bioorg. Med.
Chem. 2005, 13, 2837 – 2846; b) K. Wakabayashi, K. Imai, H. Miyachi, Y.Hashimoto, A. Tanatani, Bioorg. Med. Chem. 2008, 16, 6799 – 6812.
[38] L. Y. Hu, H. J. Lei, D. Du, T. R. Johnson, V. Fedij, C. Kostlan, W. S. Yue, M.Lovdahl, J. J. Li, M. Carroll, D. Dettling, J. Asbill, C. Fan, K. Wade, D. Poca-lyko, K. Lapham, R. Yalamanchili, B. Samas, D. Vrieze, S. Ciotti, T. Krieger-Burke, D. Sliskovic, H. Welgus, Bioorg. Med. Chem. Lett. 2007, 17, 5693 –5697.
[39] D. Joseph-McCarthy, Pharmacol. Ther. 1999, 84, 179 – 191.[40] a) A. A. Sçderholm, P. T. Lehtovuori, T. H. Nyrçnen, J. Med. Chem. 2005,
48, 917 – 925; b) A. A. Sçderholm, J. Viili�inen, P. T. Lehtovuori, H. Eskeli-nen, D. Roell, A. Baniahmad, T. H. Nyrçnen, J. Chem. Inf. Model. 2008, 48,1882 – 1890.
[41] I. Kinoyama, N. Taniguchi, T. Yoden, H. Koutoku, T. Furutani, M. Kudoh,M. Okada, Chem. Pharm. Bull. 2004, 52, 1330 – 1333.
[42] I. Kinoyama, N. Taniguchi, E. Kawaminami, E. Nozawa, H. Koutoku, T. Fur-utani, M. Kudoh, M. Okada, Chem. Pharm. Bull. 2005, 53, 402 – 409.
[43] I. Kinoyama, N. Taniguchi, A. Toyoshima, E. Nozawa, T. Kamikubo, M. Im-amura, A. Matsuhisa, K. Samizu, E. Kawanimani, T. Niimi, N. Hamada, H.Koutoku, T. Furutani, M. Kudoh, M. Okada, M. Ohta, S. Tsukamoto, J.Med. Chem. 2006, 49, 716 – 726.
[44] M. E. Salvati, A. Balog, D. D. Wei, D. Pickering, R. M. Attar, J. Geng, C. A.Rizzo, J. T. Hunt, M. M. Gottardis, R. Weinmann, R. Martinez, Bioorg. Med.Chem. Lett. 2005, 15, 389 – 393.
[45] M. E. Salvati, A. Balog, W. Shan, D. D. Wei, D. Pickering, R. M. Attar, J.Geng, C. A. Rizzo, M. M. Gottardis, R. Weinmann, S. R. Krystek, J. Sack, Y.An, K. Kish, Bioorg. Med. Chem. Lett. 2005, 15, 271 – 276.
[46] M. E. Salvati, A. Balog, W. Shan, R. Rampulla, S. Giese, T. Mitt, J. A. Furch,G. D. Vite, R. M. Attar, M. Jure-Kunkel, J. Geng, C. A. Rizzo, M. M. Gottar-dis, S. R. Krystek, J. Gougoutas, M. A. Galella, M. Obermeier, A. Fura, G.Chandrasena, Bioorg. Med. Chem. Lett. 2008, 18, 1910 – 1915.
[47] M. E. Salvati, J. A. Balog, D. A. Pickering, S. Giese, A. Fura, W. Li, R. N.Patel, R. L. Hanson, T. Mitt, J. Y. Roberge, J. R. Corte, S. H. Spergel, R. A.Rampulla, R. N. Misra, H.-Y. Xiao, (Bristol–Myers Squibb Co., Princeton,NJ, USA), US/7141578B2, 2006.
[48] a) M. Salvati, R. M. Attar, A. Balog, J. Dell-John, M. Jure-Kunke, S. Krystek,M. Obermeier, T. R. Spires, G. Vite, M. Gottardis, EJC Suppl. 2008, 6, 50;b) R. M. Attar, M. Jure-Kunkel, A. Balog, M. E. Cvijic, J. Dell-John, C. A.Rizzo, L. Schweizer, T. E. Spires, J. S. Platero, M. Obermeier, W. Shan,M. E. Salvati, W. R. Foster, J. Dinchuk, S. J. Chen, G. Vite, R. Kramer, M. M.Gottardis, Cancer Res. 2009, 69, 6522 – 6530.
[49] ClinicalTrials.gov, a service of the National Institutes of Health (USA), isa registry of federally and privately supported clinical trials conductedin the United States and around the world. For more details on therecent phase I clinical trials of BMS-641988 see studies NCT00644488and NCT00326586 at http://ClinicalTrials.gov.
[50] G. Teutsch, F. Goubet, T. Battmann, A. Bonfils, F. Bouchoux, E. Cerede, D.Gofflo, M. Gaillard-Kelly, D. Philibert, J. Steroid Biochem. Mol. Biol. 1994,48, 111 – 119.
1660 www.chemmedchem.org � 2010 Wiley-VCH Verlag GmbH & Co. KGaA, Weinheim ChemMedChem 2010, 5, 1651 – 1661
MED G. Zhao et al.
[51] M. E. Van Dort, D. M. Robins, B. Wayburn, J. Med. Chem. 2000, 43, 3344 –3347.
[52] C. L. Sawyers, M. E. Jung, C. D. Chen, S. Ouk, D. Welsbie, C. Tran, J.Wongvipat, D. Yoo, (The Regents of the University of California, Oak-land, USA), US2007/0004753A1, 2007.
[53] C. Tran, S. Ouk, N. J. Clegg, Y. Chen, P. A. Watson, V. Arora, J. Wongvipat,P. M. Smith-Jones, D. Yoo, A. Kwon, T. Wasielewska, D. Welsbie, C. D.Chen, C. S. Higano, T. M. Beer, D. T. Hung, H. I. Scher, M. E. Jung, C. L.Sawyers, Science 2009, 324, 787 – 790.
[54] For more details on the ongoing clinical trials of MDV3100 see studiesNCT00510718 (phase I), NCT01091103 (phase II) and NCT00974311 (pha-se III) at http://ClinicalTrials.gov.
[55] A. Balog, M. E. Salvati, W. Shan, A. Mathur, L. W. Leith, D. D. Wei, R. M.Attar, J. Geng, C. A. Rizzo, C. Wang, S. R. Krystek, J. S. Tokarski, J. T. Hunt,M. Gottardis, R. Weinmann, Bioorg. Med. Chem. Lett. 2004, 14, 6107 –6111.
[56] J. S. Sack, K. F. Kish, C. Wang, R. M. Attar, S. E. Kiefer, Y. An, G. Y. Wu, J. E.Scheffler, M. E. Salvati, S. R. Krystek, Jr. , R. Weinmann, H. M. Einspahr,Proc. Natl. Acad. Sci. USA 2001, 98, 4904 – 4909.
[57] C. Sun, J. A. Robl, T. C. Wang, Y. Huang, J. E. Kuhns, J. A. Lupisella, B. C.Beehler, R. Golla, P. G. Sleph, R. Seethala, A. Fura, S. R. Krystek, Jr. , Y. An,M. F. Malley, J. S. Sack, M. E. Salvati, G. J. Grover, J. Ostrowski, L. G.Hamann, J. Med. Chem. 2006, 49, 7596 – 7599.
[58] A. F. Armstrong, J. F. Valliant, Dalton Trans. 2007, 4240 – 4251.[59] Y. Endo, T. Iijima, Y. Yamakoshi, M. Yamaguchi, H. Fukasawa, K. Shudo, J.
Med. Chem. 1999, 42, 1501 – 1504.[60] a) S. Fujii, Y. Hashimoto, T. Suzuki, S. Ohta, Y. Endo, Bioorg. Med. Chem.
Lett. 2005, 15, 227 – 230; b) S. Fujii, T. Goto, K. Ohta, Y. Hashimoto, T.Suzuki, S. Ohta, Y. Endo, J. Med. Chem. 2005, 48, 4654 – 4662; c) T. Goto,K. Ohta, T. Suzuki, S. Ohta, Y. Endo, Bioorg. Med. Chem. 2005, 13, 6414 –6424; d) K. Ohta, T. Goto, S. Fijii, T. Suzuki, S. Ohta, Y. Endo, Bioorg. Med.Chem. 2008, 16, 8022 – 8028; e) S. Fujii, K. Ohta, T. Goto, H. Kagechika, Y.Endo, Bioorg. Med. Chem. 2009, 17, 344 – 350.
[61] O. Payen, S. Top, A. Vessieres, E. Brule, M. A. Plamont, M. J. McGlinchey,H. Muller-Bunz, G. Jaouen, J. Med. Chem. 2008, 51, 1791 – 1799.
[62] A. Aranda, O. Martin�z-Iglesias, L. Ruiz-Llorente, V. Garc�a-Carpizo, A.Zambrano, Trends Endocrinol. Metab. 2009, 20, 318 – 324.
[63] L. A. Arnold, E. Estebanez-Perpina, M. Togashi, N. Jouravel, A. Shelat,A. C. McReynolds, E. Mar, P. Nguyen, J. D. Baxter, R. J. Fletterick, P. Webb,R. K. Guy, J. Biol. Chem. 2005, 280, 43048 – 43055.
[64] a) S. A. Peterson, T. Klabunde, H. A. Lashuel, H. Purkey, J. C. Sacchettini,J. W. Kelly, Proc. Natl. Acad. Sci. USA 1998, 95, 12956 – 12960; b) P. W.Baures, V. B. Oza, S. A. Peterson, J. W. Kelly, Bioorg. Med. Chem. 1999, 7,1339 – 1347.
[65] E. Estebanez-Perpina, L. A. Arnold, P. Nguyen, E. D. Rodrigues, E. Mar, R.Bateman, P. Pallai, K. M. Shokat, J. D. Baxter, R. K. Guy, P. Webb, R. J. Flet-terick, Proc. Natl. Acad. Sci. USA 2007, 104, 16074 – 16079.
[66] H. L. Ratan, W. P. Steward, A. J. Gescher, J. K. Mellon, Urol. Oncol. 2002,7, 223 – 227.
[67] a) T. T. Wang, T. S. Hudson, T. C. Wang, C. M. Remsberg, N. M. Davies, Y.Takahashi, Y. S. Kim, H. Seifried, B. T. Vinyard, S. N. Perkins, S. D. Hursting,Carcinogenesis 2008, 29, 2001 – 2010; b) W. F. Shi, M. Leong, E. Cho, J.Farrell, H. C. Chen, J. Tian, D. Zhang, PLoS One 2009, 4, e7398.
[68] K. J. Pienta, D. C. Smith, Ca-Cancer J. Clin. 2005, 55, 300 – 318.[69] M. Ammirante, J. L. Luo, S. Grivennikov, S. Nedospasov, M. Karin, Nature
2010, 464, 302 – 305.[70] a) H. L. Devlin, M. Mudryj, Cancer Lett. 2009, 274, 177 – 186; b) R. Nar-
ayanan, M. Yepuru, A. T. Szafran, M. Szwarc, C. E. Bohl, N. L. Young, D. D.Miller, M. A. Mancini, J. T. Dalton, Cancer Res. 2010, 70, 842 – 851.
Received: June 20, 2010
Revised: August 10, 2010
Published online on September 17, 2010
ChemMedChem 2010, 5, 1651 – 1661 � 2010 Wiley-VCH Verlag GmbH & Co. KGaA, Weinheim www.chemmedchem.org 1661
Nonsteroidal Antiandrogens Targeting the Androgen Receptor