Embed Size (px)
Citation preview
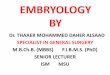
(End 3rd wk WIUL) Angiogenic cells appear from splanchnic mesoderm and gives rise to 2 primitive endocardial tubes (cephalic end), 2 dorsal aortae (caudal). Lateral flexion allows the 2 tubes to fuse in the midline (d17-22).
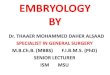
1 - Initially, Heart consists of a simple tube, ancored at one end by the differentiating arterial trunks and at the other by extensive venous channels which drain into the atrium.
2 - Being fixed at both ends, cardiac tubes grows rapidly in length (simultaneous growth in the primitive ventricle & bulbus cordis) and the embroynic ventricle is bent into a C-shaped loop to the right of the midline.
Primitive Ventricle (anterior&lateral growth) Right & Left Ventricle Primitive Atrium (Posteriorly) Right & Left Atrium
The primitive ventricle displaces the bulbous cordis superiorly.
DEVELOPMENT OF THE HEART
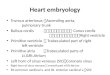
3 - As Development continues, the ventricular region swings back to midline and expands&grows in length, covering the atrium and great veins
Extensive sacculations will eventually become the R Atrium & L Atrium. The future left ventricle lies left to the interventricular groove and the embryonic right ventricular region communicates with the truncus arteriosus.
A 4 chambered heart is formed from this convoluted tube by the formation of septa.
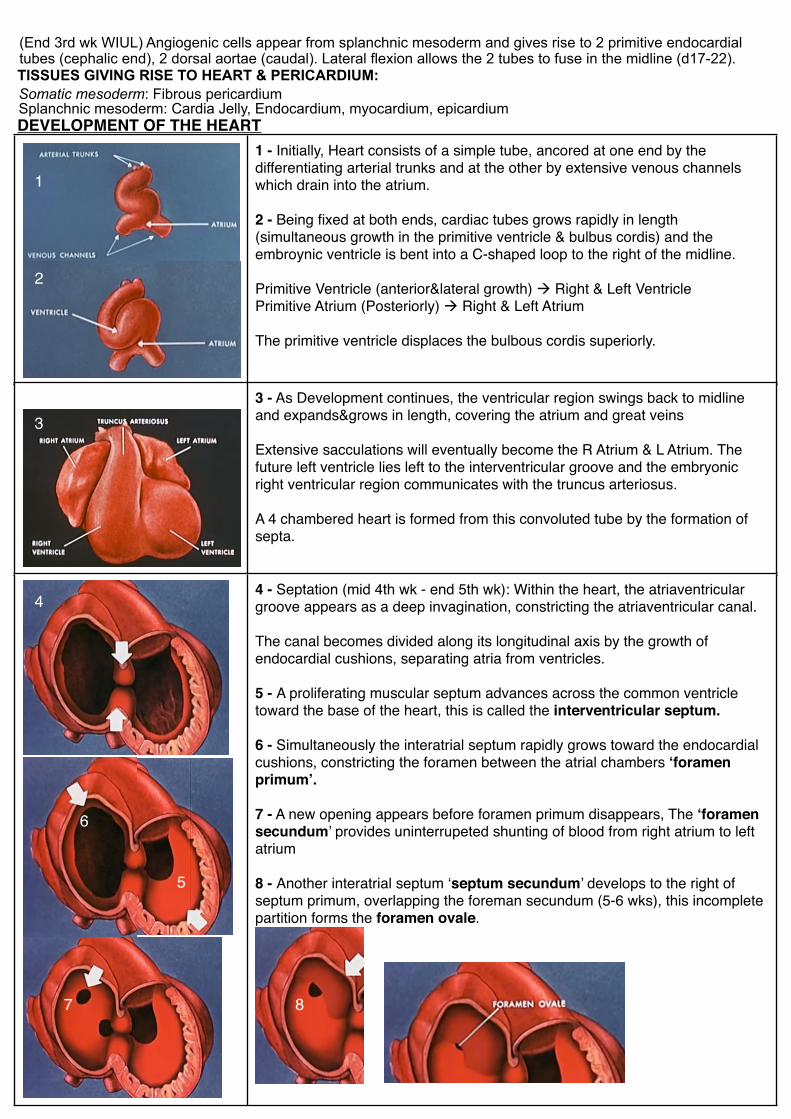
4 - Septation (mid 4th wk - end 5th wk): Within the heart, the atriaventricular groove appears as a deep invagination, constricting the atriaventricular canal.
The canal becomes divided along its longitudinal axis by the growth of endocardial cushions, separating atria from ventricles.
5 - A proliferating muscular septum advances across the common ventricle toward the base of the heart, this is called the interventricular septum.
6 - Simultaneously the interatrial septum rapidly grows toward the endocardial cushions, constricting the foramen between the atrial chambers ‘foramen primum’.
7 - A new opening appears before foramen primum disappears, The ‘foramen secundum’ provides uninterrupeted shunting of blood from right atrium to left atrium
8 - Another interatrial septum ‘septum secundum’ develops to the right of septum primum, overlapping the foreman secundum (5-6 wks), this incomplete partition forms the foramen ovale.
TISSUES GIVING RISE TO HEART & PERICARDIUM: Somatic mesoderm: Fibrous pericardiumSplanchnic mesoderm: Cardia Jelly, Endocardium, myocardium, epicardium
1
2
3
4
5
6
7 8
1
2
3
AV
5
4
6
7
8
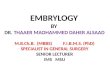
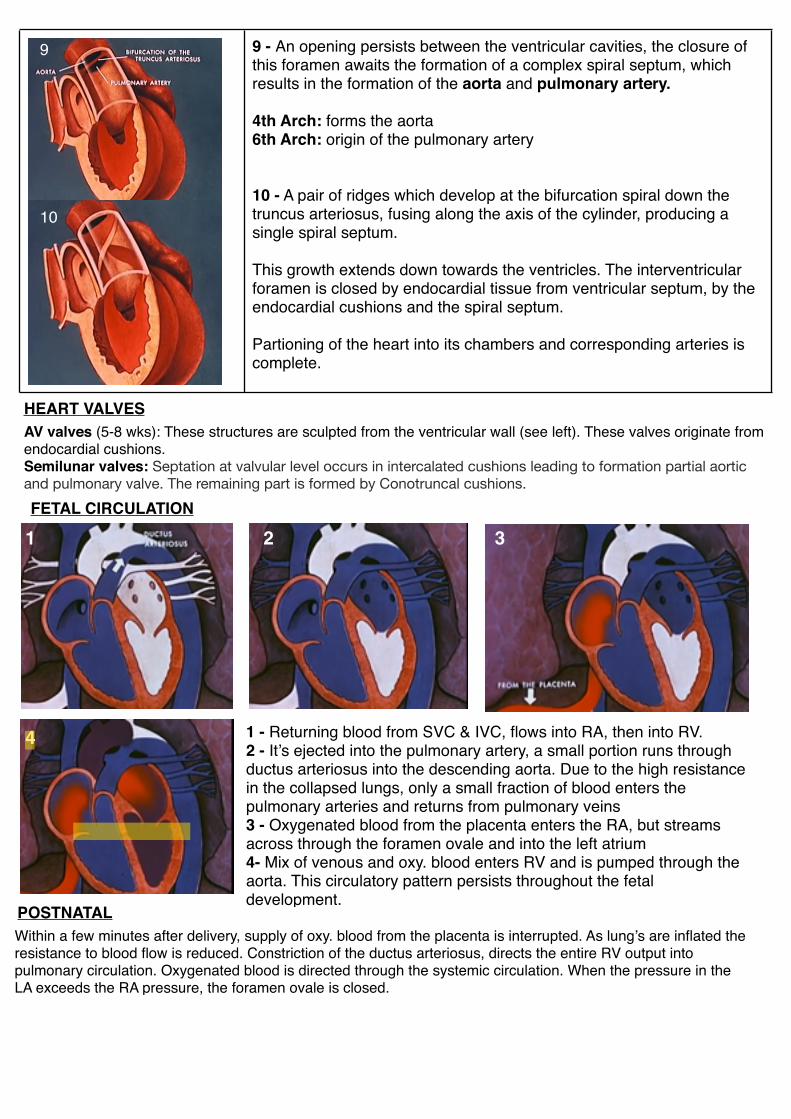
9 - An opening persists between the ventricular cavities, the closure of this foramen awaits the formation of a complex spiral septum, which results in the formation of the aorta and pulmonary artery.
4th Arch: forms the aorta 6th Arch: origin of the pulmonary artery
10 - A pair of ridges which develop at the bifurcation spiral down the truncus arteriosus, fusing along the axis of the cylinder, producing a single spiral septum.
This growth extends down towards the ventricles. The interventricular foramen is closed by endocardial tissue from ventricular septum, by the endocardial cushions and the spiral septum.
Partioning of the heart into its chambers and corresponding arteries is complete.
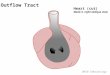
FETAL CIRCULATION
1 2 3
4 1 - Returning blood from SVC & IVC, flows into RA, then into RV. 2 - It’s ejected into the pulmonary artery, a small portion runs through ductus arteriosus into the descending aorta. Due to the high resistance in the collapsed lungs, only a small fraction of blood enters the pulmonary arteries and returns from pulmonary veins3 - Oxygenated blood from the placenta enters the RA, but streams across through the foramen ovale and into the left atrium4- Mix of venous and oxy. blood enters RV and is pumped through the aorta. This circulatory pattern persists throughout the fetal development.
POSTNATALWithin a few minutes after delivery, supply of oxy. blood from the placenta is interrupted. As lung’s are inflated the resistance to blood flow is reduced. Constriction of the ductus arteriosus, directs the entire RV output into pulmonary circulation. Oxygenated blood is directed through the systemic circulation. When the pressure in the LA exceeds the RA pressure, the foramen ovale is closed.
HEART VALVESAV valves (5-8 wks): These structures are sculpted from the ventricular wall (see left). These valves originate from endocardial cushions.Semilunar valves: Septation at valvular level occurs in intercalated cushions leading to formation partial aortic and pulmonary valve. The remaining part is formed by Conotruncal cushions.
9
10