Embed Size (px)
Citation preview

Thorax 1992;47:1019-1024
Development of a shuttle walking test of disabilityin patients with chronic airways obstruction
Sally J Singh, Michael D L Morgan, Shona Scott, Denise Walters, Adrianne E Hardman
1019
AbstractBackground The aim was to develop astandardised and externally paced fieldwalking test, incorporating an incre-mental and progressive structure, toassess functional capacity in patients withchronic airways obstruction.Methods The usefulness oftwo differentshuttle walking test protocols wasexamined in two separate groups ofpatients. The initial 10 level protocol(group A, n = 10) and a subsequent,modified, 12 level protocol (group B,n = 10) differed in the number ofincrements and in the speeds of walking.Patients performed three shuttle walkingtests one week apart. Then the perfor-mance ofpatients (group C, n = 15) in thesix minute walking test was comparedwith that in the second (modified) shuttlewalking test protocol. Heart rate wasrecorded during all the exercise tests witha short range telemetry device.Results The 12 level modified protocolprovided a measure of functionalcapacity in patients with a wide range ofdisability and was reproducible after justone practice walk; the mean differencebetween trial 2 v 3 was -2-0 (95% CI -21'9to 17-9) m.There was a significant relation between
the distance walked in the six minutewalking test and the shuttle walking test(rho = 0 68) but the six minute walkingtest appeared to overestimate the extentof disability in some patients. The shuttletest provoked a graded cardiovascularresponse not evident in the six minutetest. Moreover, the maximal heart ratesattained were significantly higher forthe shuttle walking test than for the sixminute test.Conclusions The shuttle walking testconstitutes a standardised incrementalfield walking test that provokes a symp-tom limited maximal performance. Itprovides an objective measurement ofdisability and allows direct comparisonof patients' performance.
(Thorax 1992;47:1019-1024)
Objective measures of disability are importantfor the assessment and clinical management ofpatients with chronic airways obstruction. Aslaboratory assessment is not widely available
and may be expensive and intimidating to thepatient, field tests of walking ability are oftenused. These usually comprise a self paced testin which the patient walks as far as possible ineither six or twelve minutes.' 2 Although attrac-tive, these protocols are difficult to standardiseand may be influenced by motivation andencouragement.' In addition, their very sim-plicity limits the information that can beobtained from them about the physiologicaland symptomatic changes that occur duringexercise.4 The purpose of this study was todevelop a simple, standardised test of disabilitythat overcomes these limitations to determinefunctional capacity in patients with chronicairways obstruction.
Exercise tests based on a single work ratemay add little to the studies performed at rest.5The proposed test therefore is incremental andprogressive, stressing the individual to a symp-tom limited maximal performance. Theprotocol was modified from that of a progres-sive, externally paced 20 metre shuttle runningtest, widely used as a field test of functionalcapacity in athletes.6 Our test requires thepatient to walk up and down a 10 m course,with the walking speed dictated by a prerecor-ded audio signal played on a cassette recorder.In the first instance a downgraded 10 levelprotocol was used, the speed of walking beingproportional to the speeds of running used inthe Leger and Lambert shuttle test. Evaluationof the performance of a group of patients usingthis protocol led to the development of amodified, 12 level protocol. This used a greaterrange of walking speeds to accommodatepatients with minimal disability as well as thosemore severely disabled.This paper, firstly, examines the feasibility
and reproducibility of shuttle walking testprotocols and, secondly, compares patients'performance in the modified (second) shuttlewalking test with that in the standard sixminute walking test.
MethodsPATIENTSThe patients were recruited from medical clin-ics and given a full explanation before informedconsent was obtained. Patients known to behypoxic with cor pulmonale or ischaemic heartdisease were excluded, as were subjects withneurological or locomotor disorders. Patientshad no alteration made to their medicationduring the study.Three groups of patients were recruited on
the basis of convenience. Groups A (n = 10)
Department ofRespiratory Medicine,Glenfield GeneralHospital, LeicesterLE3 9QPS J Singh,M D L Morgan,D WaltersDepartment ofPhysical Educationand Sports Science,LoughboroughUniversity,LoughboroughLEll 3TUS ScottA E HardmanReprint requests to:S J SinghReceived 13 August 1991Returned to authors3 December 1991Revised version received26 February 1992Accepted 23 June 1992
on February 20, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.47.12.1019 on 1 D
ecember 1992. D
ownloaded from

Singh, Morgan, Scott, Walters, Hardman
Table I Physical characteristics of the three groups ofpatients
Age (y):Group n (M:F) mean (range) FEV, (I)BI'7S
A 10 (9:1) 64 (54-73) 0 50 (0 36-145)B 10 (6:4) 63 (52-74) 1-10 (0 60-210)C 15 (10:5) 64 (45-71) 1 20 (0 50-285)
and B (n = 10) participated in thereproducibility studies of the downgraded andmodified shuttle walking protocols respectively,and group C (n = 15) was recruited for thecomparison of the shuttle walking test with thesix minute walking test. Table 1 shows thephysical characteristics of the three groups.The study was approved by the local ethical
committee.
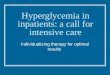
EXERCISE TEST PROCEDURESShuttle walking testThe shuttle walking test required the patient towalk up and down a 10 m course. The coursewas identified by two cones inset 0 5 m fromeither end to avoid the need for abrupt changesin direction (fig 1). The speed at which thepatient walked was dictated by an audio signalplayed on a tape cassette, originally generatedfrom a BBC microcomputer. The accuracy ofthe timed signal was ensured by the inclusionon the tape of a calibration period of oneminute.The explanation to the patient was standar-
dised and played from the tape before the startof the test. The patient was advised: "Walk at asteady pace, aiming to turn around when youhear the signal. You should continue to walkuntil you feel that you are unable to maintainthe required speed without becoming undulybreathless."The start of the test was indicated by a triple
bleep. Thereafter the tape emitted a singlebleep at regular intervals, at which point thesubject attempted to be at the opposite end ofthe course-that is, by the time the patientheard the signal he should be turning round thecone to proceed back down the course. Eachminute the speed of walking was increased by asmall increment. For example, in the modifiedprotocol the increase was 0-17 m/s each min-ute, so the patient was required to walk
Table 2 The shuttle walk protocols
Downgraded protocol Modified protocol
Speed SpeedNo of shuttles No of shuttles
Level m/s mph per level m/s mph per level
1 0-62 1-39 3 0 50 1 12 32 072 1 61 4 067 1 50 43 082 1 83 4 084 1 88 54 092 206 5 1 01 226 65 1-02 228 6 1 18 264 76 112 251 6 135 302 87 1-22 2-73 7 1 52 340 98 132 295 7 169 378 109 1-42 3 18 8 1 86 4 16 1110 1-52 340 9 203 454 1211 2 20 4-92 1312 237 530 14
progressively faster. A change of speed to thenext level was indicated by a triple bleep fromthe tape recorder.The first speed of walking was referred to as
level 1, the second as level 2, and so on. Eachlevel lasted for one minute and the tape contin-ued for 10 levels in the downgraded protocoland for 12 in the modified protocol. Thenumber of shuttles (10 m lengths) in each levelwas dictated by the walking speed at that level(table 2). For example, the modified shuttlewalking test protocol required the patient tocomplete three shuttles in the first level. Thenumber of shuttles the patient was required tocomplete within consecutive levels increasedby one-that is, for level 2 four shuttles, forlevel 3 five shuttles, and so on. Figure 2 showsthe total number of shuttles completed at theend of each level. To help the patient toestablish the routine of the test and the first,very slow, speed of walking, the operatorwalked alongside for the first minute. Thepatient had 20 seconds to complete each of thethree shuttles in the first minute. After this firstminute patients paced themselves to coordinatetheir walking speed with the timed signals.When patients reached the cone before thesignal, they were instructed to remain until thesignal indicated that they could proceed withthe test. The operator sat alongside the 10 mcourse and no encouragement was given. Theonly verbal contact was the advice given eachminute to increase the walking speed slightly.All patients found it easy to pace themselvesand no difficulties were encountered in ad-ministering the test.The end of the test was determined by either
(a) the patient, when he or she was too breath-less to maintain the required speed or (b) theoperator, if the patient failed to complete ashuttle in the time allowed (that is, was morethan 0 5 m away from the cone when the bleepsounded) or (c) attainment of 85% of thepredicted maximal heart rate derived from theformula [210 - (0-65 x age)].Downgraded shuttle walking test The initialstudy used a protocol for which the timings ofthe speeds and signals were simply down-graded from the speeds used by Leger andLambert in the 20 metre shuttle running test.6The starting speed was 0-62 m/s and the testcontinued for a maximum of 10 levels-that is,for 10 minutes. The increase per level was0-10 m/s, resulting in a final speed of 1-52 m/s(3A4 mph) (table 2). If the patients were capablethey completed nine shuttles (90 m) in the lastminute of the test. This protocol was examinedwith the patients in group A.Modified shuttle walking test After analysis ofthe results of the downgraded protocol amodified shuttle walking protocol was adopted.The timings of the signals for this protocolwere modified from the 10 level protocol de-scribed above-specifically there was a slowerstart (0 50 m/s) than in the downgradedprotocol but the increments of 0-17 m/s eachminute were slightly greater. The timed signalsfor this modified protocol continued for 12minutes, the final speed (level 12) being 2-37m/s (5 3 mph) (table 2). If the patients were
Figure I Diagram of theshuttle walk
1020
on February 20, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.47.12.1019 on 1 D
ecember 1992. D
ownloaded from

Development of a shuttle walking test of disability in patients with chronic airways obstruction
110 -
100 -
90
80
70
60
50
40
30
20
10
00 1 2 3 4 5 6 7 8 9 10 1 1 12
Completed levels
Figure 2 Cumulative number of shuttles (10 m lengths) completed at the end of eachlevel (modified protocol).
capable of reaching this speed they wouldcomplete 14 shuttles (140 m) in the final min-ute. This protocol was examined in a separategroup of patients, group B.Reproducibility of the shuttle walking test Theprocedure adopted for examining thereproducibility of both the downgraded andthe modified protocol was the same. Patientsmade three visits to the hospital, at intervals ofone week and at the same time of day. Theyreceived no bronchodilators for three hoursbefore the test, but took all other medicines asusual. The baseline measurements at each visitincluded spirometry (FEVy and FVC), theBorg breathlessness scale,7 heart rate, and com-pletion of the Chronic Respiratory DiseaseQuestionnaire.' Heart rate was monitoredthroughout the exercise by a short rangetelemetry device (Polar Electro Sports TesterPE3000). Reproducibility was examined bycomparing the distances recorded for each ofthe three trials.
Six minute walking testThe six minute walking test was conductedalong a 45 m hospital corridor. The operatorsat half way along the corridor in a visibleposition, issuing standardised instructions andencouragement-either "You're doing well"or "Keep up the good work"-as the patientpassed.3
Comparison of the shuttle and the six minutewalking testsFifteen patients consented to take part in thecomparison of the two tests (group C). Theprotocol for the modified shuttle walk was usedfor this study. The reproducibility studyshowed that only one practice of this shuttletest was necessary.Two practice six minute walks were per-
formed to counteract any learning or trainingeffect.39 The result of the third trial was used in
Table 3 Reproducibility studies on the shuttle walking test
Downgraded protocol (group A) Modified protocol (group B)
Trial r d (m) (95% CI(m)) r d (m) (95" CI (m))
1 v 2 0-95 0 (-388 to 38 8) 0-98 -31 (-49-0 to 13-0)1v3 0-94 -13 (-280 to6-0) 099 -33 (-481to179)2v3 0-99 -11 (-53-0to31-6) 098 -2 (-21-9to179)
the analysis. Three visits were required, withthe same baseline measurements as before.Visit 1 comprised two six minute walking testsand one shuttle walking test, with at least 45minutes' rest between each exercise test. Forvisits 2 and 3 a randomised balanced design wasused, with one shuttle walking test followedone week later by a six minute walking test orvice versa.
STATISTICAL ANALYSISStatistical analysis was carried out according tothe recommendations of Bland and Altman,'0with the CIA software package VI 1 and theMinitab V7O statistical package for IBM com-patibile computers to assess the agreementbetween the tests. Relationships between per-formance in the three trials of groups A and Bwere evaluated by means of the Pearsonproduct moment coefficient. Relationships bet-ween performance and Borg scores in theshuttle test and the six minute walking testwere evaluated by using Spearman's rho (p). A5% level of significance was used throughout.
ResultsThere was no significant difference in the scor-ing of the four components of the ChronicRespiratory Disease Questionnaire betweenthe three separate visits for groups A, B, or C.All the patients were clinically stable through-out the trial (FEV1 values remained similarwithin each group). The patients were there-fore both physically and psychologically stableduring the study.No patients were excluded or withdrew from
the study of either the downgraded or themodified protocol. The patients did not find itdifficult to pace themselves correctly. Nor wasany patient "disqualified" because the speed ofwalking was misjudged. The agreement be-tween trials was examined in two different ways.The starting point was to examine the relation-ships between distances walked in trials 1, 2,and 3. In addition, the agreement between theresults of the three trials was examined on thebasis of the mean difference (d) and the 95%(CI) for this bias'0 (table 3).
REPRODUCIBILITY STUDIESDowngraded shuttle walking protocol (group A)The distance walked ranged from 20 to510 m-that is, the end of the 10 levelprotocol-with a mean distance of 211, 211,and 222 m for trials 1, 2 and 3 (fig 3A). Therewas no significant difference in performancebetween trials. The relationship between per-formance in the three trials was strong (table 3).The mean maximal heart rate attained was 114,111, and III beats/min for trials 1, 2, and 3respectively (fig 3B).
Modified shuttle walking protocol (group B)Distances walked ranged from 90 to 520 m-that is, from level 2 plus two shuttles of level 3to the end of level 8-with mean values of 345,376, and 378 m for the three trials (fig 3A). Nopatient completed this 12 level protocol. Therewas a significant difference in patients' per-
1021
on February 20, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.47.12.1019 on 1 D
ecember 1992. D
ownloaded from

Singh, Morgan, Scott, Walters, Hardman
Figure 3 A-Mean(SE) distances walked inthe shuttle walking test:groups A and B. B-Mean (SE) heart rateduring the shuttle walkingtest: groups A and B.
a'i T n a 3I-'i Trial 2,i3ta
G~~.,roup
Predicted maximum heart
rate for 64 year old
Group B
formance between trials 1 and 2 but not be-tween trials 2 and 3, suggesting a small trainingor learning effect. Mean maximal heart rateswere 125, 128, and 127 beats/min for trials 1, 2,and 3 (fig 3B). The relationships between thedistances walked on each trial were strong(table 3)-for example, r = 0-98 for trial 2 vtrial 3. Table 3 shows that for 95 patients out of100 the recorded walking distance in trial 3would be within -21-9 to 17 9 m of thatrecorded for trial 2. The mean difference be-tween these two trials was -2 m.As with other studies examining patients'
performance,I 1112 there was a poor correlationwith patients' lung function values. For FEV, vwalking distance r = 0-51, 0 22, and 0-25 fortrials 1, 2, and 3.
COMPARISON OF THE SHUTTLE AND THE SIXMINUTE WALKING TEST (GROUP C)The results of the second shuttle test (modifiedprotocol) and the third six minute walking testwere used for the comparison of the two tests.The distance recorded for the shuttle testrepresents completed shuttles only. Therelationship between performance (distancecompleted) in the six minute walking test and inthe shuttle test was moderate (fig 4, p = 0-68).
In nine of the 15 patients the maximal heart
E
(u
4-
to
.0U,(U.to
co
I
150 -
140 -
130 -
120 -
110 -
100 -
90-
80-
6 min/i* 6 min/2
**-*o -- Shuttle/l***ao.. Shuttle/2
0 2 4 6Time (min)
8 10
Figure 5 Heart rate responses during the shuttlewalking test and the six minute walkfor tworepresentative patients from group C.
rate was greater for the shuttle test than for thesix minute walking test. The correlation be-tween heart rates for the two different tests wasmoderate (r = 0-76). The mean maximal heartrate was 9 beats/min higher in the shuttle testthan in the six minute walking test (95% CI 1 to18 beats/min). Figure 5 shows the heart raterecorded at the end of every minute of each testfor two representative patients. This shows agraded cardiovascular response to the shuttletest, which was not observed in the six minutewalking test. The mean increase from restingheart rate values was significantly smaller forthe six minute walking test (41 (SD 22), range8-86 (beats/min) than the shuttle walking test(55 (21), 29-91 beats/min).The Borg breathlessness scale rating7 was
higher at the end of the shuttle walking testthan at the end of the six minute walking test innine out of 15 patients. Two patients reportedgreater breathlessness after the six minutewalking test and one of these patients had ahigher level of perceived breathlessness at reston the day of the six minute walking test thanon the day of the shuttle test (scores 4 and 0 5).The correlation of the Borg breathlessnessscale responses at the end ofthe shuttle walkingtest and of the six minute walking test wasp = 0-64. The maximum recorded Borg scalescores were nine for the shuttle test and sevenfor the six minute walking test (not in the samepatient).
Figure 4 Distanceswalked in the shuttlewalking test and the sixminute walking test:group C.
0
00
Qo
00
0
400 500Shuttle walk (m)
DiscussionThe performance of patients with chronicairways obstruction is limited by breathless-
0 ness that is due to a mixture of functionalabnormalities. The limitation to individualperformance cannot, however, be predicted bythe measurement of these factors alone. 13'Observation of the exercise response hastherefore become the basis of objective assess-
rho 0-68 ment of disability both to stress the cardio-respiratory system and to evaluate reserve
, , capacity.600 700 It has been proposed that day to day
activities are mostly of an irregular nature, a
700 -
E 600-(U3@ 500-
.E
.x 400-Un
80
300
vv, ,
.1m)
1022
.,
:.
on February 20, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.47.12.1019 on 1 D
ecember 1992. D
ownloaded from

Development of a shuttle walking test of disability in patients with chronic airways obstruction
steady state rarely being achieved.14 Con-sequently, patients' symptoms are probablymore likely to be revealed or identified duringan incremental exercise test rather than a selfpaced exercise test. The six and 12 minute testshave no standardised pace or incrementalfacility. Whether the cardiorespiratory systemis stressed maximally depends on the manner inwhich the test is conducted and the amount ofencouragement offered. Inconsistencies of thisnature probably contribute to the considerablevariation in the walking performance reportedfor clinically similar groups ofpatients betweenstudies.4"5'6 This makes it difficult to makevalid comparisons between studies.The shuttle test fulfils the basic criteria for an
exercise test for pateints with chronic airwaysobstruction. It is based on a familiar activityand, unlike cycle ergometry or treadmill walk-ing, is simple for both the operator and thepatient. It requires minimal equipment and hasthe advantage that it is standardised, incremen-tal, and externally paced, diminishing the effectof the operator's influence.Although the operator walks alongside for
the first minute in the shuttle walking test thisdoes not encourage the patient to walk fasterbecause pacing is imposed by the audio signal.It does, however, help the patient to establishthe slowest speed of walking and thereforecreates the base speed on which to increasespeed. In the first minute it was usually neces-sary to slow the patient down as the lessseverely affected patients found it difficult towalk slowly enough. Although the operatorthen sits alongside the course noencouragement is offered and his or herinfluence is minimised because the externalpacing does not allow the patient to walk faster.
External pacing allows valid intersubject andintrasubject comparison. Patients who havecompleted 500 m in an incremental walkingtest have experienced a similar "work rate/stress." This is not necessarily the case forpatients completing similar distances in the selfpaced six or 12 minute walking tests andtherefore any conclusions regarding their re-spective functional capacities would be invalid.It has been suggested that the habitual natureof walking may prevent a self paced test fromfully showing the possible beneficial effects ofany treatment.'2 The shuttle test may enablemore effective comparison of different ap-proaches to patients' management and treat-ment than has previously been possible withexisting field exercise tests. Interestingly, theone patient who performed strikingly better inthe shuttle test than in the six minute walkingtest (fig 4) found it difficult to pace himself forthe six minute walking test on all threeoccasions. The extent of his disability wasshown more clearly by the shuttle test than bythe traditional six minute walking test.Examining the results from the downgraded
protocol we thought that the development ofanalternative protocol would be appropriate.This conclusion was based on two observa-tions. Firstly, the FEV, values ofgroup A werelow (mean value 05 1) and, secondly, onepatient from group A completed the 10 level
protocol. These two factors indicate that thepatient suffering from mild chronic airwaysobstruction would probably complete thecourse with relative ease. An extended protocolwas therefore required to evoke a symptomlimited maximal performance in these patients.Secondly, a slower start was clearly necessaryto accommodate the more severely affectedpatient. We identified the modified 12 levelprotocol as a suitable shuttle walking testprotocol for assessing functional capacity in awide range of patients with chronic airwaysobstruction, with a greater increase of walkingspeed to stress the more able patients as well asa slower start than the downgraded protocol tocater for the more severely affected patients. Ameasure of functional capacity can be thereforeobtained in most patients with the modifiedshuttle walking protocol. The reproducibilityof the shuttle walking test can be examined andreinforced by using the results of bothprotocols as the structure and procedure ofthese externally paced walking tests were thesame. Consequently, the modified protocol wasused for the second stage of the study. Further-more, only one practice walk appeared to benecessary. The patients in group B performingthis modified protocol walked significantly fur-ther in the second and third trial than in thefirst, suggesting that meaningful results can beobtained after just one practice walk.Reproducible results are obtained regardless ofwhether the patient completes one level (oneminute) or 12 levels (12 minutes).The defined speeds of walking in the shuttle
test ensure that the work load increases in amanner that provides an incremental and quan-titatively similar cardiorespiratory stress for allthe patients. The heart rate response (fig 5)provides evidence of this graded cardiovascularresponse, not observed in the six minute walk-ing test. The shuttle test, unlike the six ortwelve minute walking tests, where effort maybe maximal from the start, stresses the patientprogressively to a symptom limited maximum.This gradual increase in exercise intensityincreases the safety of the test. Consequently,the shuttle test may reveal cardiovascularlimitations to exercise and may have the poten-tial for use as an exercise test for conditionsother than lung disease. Secondly, the shuttletest can yield an outcome measure that is easilyapplied to exercise rehabilitation for patientswith both cardiac and respiratory conditions.The mean maximal heart rates obtained in ourpatients (fig 3B), however, are clearly lowerthan would be expected for the median age ofthe group, which is consistent with a ven-tilatory limit to functional capacity in thesegroups. We anticipate that the shuttle walkingtest will have a role in the prescription ofexercise in this group ofpatients. By calibratinga patient's response to the test (heart rate, Borgscale) a suitable walking speed can be judgedfor a training programme.
It has been reported that an externally pacedstep test is a reproducible and standardisedmethod of assessing functional capacity innormal subjects.'7 The performance of patientswith severe chronic airways obstruction in a
1023
on February 20, 2020 by guest. P
rotected by copyright.http://thorax.bm
j.com/
Thorax: first published as 10.1136/thx.47.12.1019 on 1 D
ecember 1992. D
ownloaded from

Singh, Morgan, Scott, Walters, Hardman
paced step test, however, shows a pronouncedlearning effect.'2 A 96% improvement in per-formance over the first four tests has beenreported. In the same study patients were alsoobserved to have a lower ventilatory responseand therefore maximal oxygen uptake (Vo2max) response to a self paced walking test thanto the paced step test. This indicates thatpatients tend to select a speed that is comfort-able rather than stress themselves with a symp-tom limited performance. They wouldconsequently fall short of attaining their Vo2max in a self paced walking test.The step and the shuttle walking test both
use less space than a self paced corridor test.Stepping may not be a familiar activity andcoordination may be difficult for this group ofpatients. Limitation to this type ofexercise mayin practice be muscle weakness or sorenessrather than ventilation. In addition, the steptest appears to have poor reproducibility. 12 Theshuttle walking test offers an alternative to theself paced walking test and the paced step testand is a substitute for both.The modified shuttle walking test we have
described is, after one practise walk, areproducible, easily administered, standard-ised exercise test of functional capacity inpatients with chronic airways obstruction. Werecommend its use for the objective assessmentof patients with a wide range of respiratorydisability.
The shuttle walking test tape and instruction leaflet maybe obtained from the department of respiratorymedicine, Glenfield General Hospital, Leicester LE39QP.
S J S is supported by the Trent regional research scheme.
1 McGavin CR, Gupta SP, McHardy GJR. Twelve-minutewalking test for assessing disability in chronic bronchitis.BMJ 1976;i:822-3.
2 Butland RJA, Gross ER, Pang J, Woodcock AA, GeddesDM. Two-, six-, and 12-minute walking tests in res-piratory diseases. BMJ 1982;284:1607-8.
3 Guyatt GH, Pugsley SO, Sullivan MJ, Thompson PJ,Berman LB, Jones NL, et al. Effect of encouragement onwalking test performance. Thorax 1984;39:818-22.
4 Beaumont A, Cockcroft A, Guz A. A self paced treadmillwalking test for breathless patients. Thorax 1985;40:459-64.
5 Jones NL. Clinical exercise testing. 3rd ed, Philadelphia:Saunders, 1988.
6 Leger LA, Lambert J. A maximal multistage 20-m shuttlerun test to predict Vo, max. Eur J Appl Physiol 1982;49:1-12.
7 Borg GAV. Psychophysical basis of perceived exertion. MedSci Sports Exerc 1982;14:377-81.
8 Guyatt GH, Berman LB, Townsend M, Pugsley SO,Chambers LW. A measure of the quality of life for clinicaltrials in chronic lung disease. Thorax 1987;42:773-8.
9 Mungall IPF, Hainsworth R. Assessment of respiratoryfunction in patients with chronic obstructive airwaysdisease. Thorax 1979;34:254-8.
10 Bland JM, Altman DG. Statistical methods for assessingagreement between two methods of clinical measurement.Lancet 1986;i:307-10.
11 Knox AJ, Morrison JFJ, Muers MF. Reproducibility ofwalking test results in chronic obstructive airways disease.Thorax 1988;43:388-92.
12 Swinburn CR, Wakefield JM, Jones PW. Performance,ventilation, and oxygen consumption in three differenttypes of exercise test in patients with chronic obstructivelung disease. Thorax 1985;40:581-6.
13 Anonymous. Assessing respiratory disablement [editorial].Lancet 1987;i:726-7.
14 Spiro SG. Exercise testing in clinical medicine. Br J DisChest 1977;71:145-72.
15 Swerts PMJ, Mosert R, Wouters EFM. Comparison ofcorridor and treadmill walking in patients with severechronic obstructive pulmonary disease. Phys Ther1990;70:439-42.
16 McGavin CR, Artvinli M, Naoe H, McHardy GJR. Dysp-noea, disability, and distance walked: comparison ofestimates of exercise performance in respiratory disease.BMJ 1978;ii:241-3.
17 Jones PW, Wakefield JM, Kontaki E. A simple and portablepaced step test for the reproducible measurements ofventilation and oxygen consumption during exercise.Thorax 1987;42:136-43.
1024 on F
ebruary 20, 2020 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.47.12.1019 on 1 Decem
ber 1992. Dow
nloaded from