Embed Size (px)
Citation preview
DEVELOPMENT OF EARLY MOTHER-PRETERM INFANT ATTACHMENT
COACHING PROGRAM
RUNGLAWON EAMKUSOLKIT
A DISSERTATION SUBMITTED IN PARTIAL FULFILLMENT
OF THE REQUIREMENTS FOR THE DOCTOR DEGREE
OF PHILOSOPHY IN NURSING SCIENCE
(INTERNATIONAL PROGRAM)
FACULTY OF NURSING
BURAPHA UNIVERSITY
AUGUST 2016
COPYRIGHT OF BURAPHA UNIVERSITY

This study was partially supported scholarship from
National Research Council of Thailand
ACKNOWLEDGEMENT
I would especially like to express my sincere gratitude and deep appreciation
to my Principal advisor, Associate Professor Dr.Chintana Wacharasin, for her
valuable supervision that contribute me to be Ph.D., invaluable support throughout the
dissertation process, being the best role model, and affectionate relationship. I am
very thankful to my co-advisor, Associate Professor Dr.Suzanne M. Thoyre from
University of North Carolina, USA. who provided valuable guidance throughout this
study, and very kind supporting while I was in the USA. Special thanks to Professor
Dr.Veena Jirapat from Chulalongkorn University as external committee, for all the
guidance, and valuable advice. I am also very great appreciation to Associate
professor Dr.Wannee Deoisres, graduate representative committee and academic
advisor for all of valuable advice throughout this study. Very thanks for all experts
involved in validating the instruments. I would like special thanks to all nursing
instructors in this curriculum, who taught me to contribute to my professional growth.
Very special thanks to administrators and team members in Boromarajonani
College of Nursing, Nakhon Phanom University that gave the opportunity for me to
study doctoral degree of nursing science, and scholarship supporting. I also would like
to thank the director of nursing, head nurse, and professional nurses of nursery unit,
and Dad and Mom clinic at Nakhon Phanom hospital, who give me permission to
conduct this research. I am gratefully indebted for all mother- preterm infant dyads
and their families who participated in this study. Surely, special thanks to National
Research Council of Thailand that provided financial support for my dissertation.
Finally, I wish to express my deep thanks for my lovely family that consists
of my father; Mr.Thanaphon Panyakullavat, my mother; Mrs.Chutikorn
Panyakullavat, my hasband; Mr.Kritsada Eamkusolkit, my sons; Korawish and
Kongpob Eamkusolkit, my brother; Mr.Thakon Panyakullavat, and my sister; Miss
Monthacha Panyakullavat, that I received endless love, encouragement and invaluable
support . Unforgettable, I offer special thanks to all of my classmates for their best
and warm friendship, supportiveness, and togetherness.
Runglawon Eamkusolkit

v
53810010 MAJOR: NURSING SCIENCE; Ph.D. (NURSING SCIENCE)
KEYWORDS: DEVELOPMENT/ MOTHER-PRETERM INFANT/
ATTACHMENT/ COACHING
RUNGLAWON EAMKUSOLKIT: DEVELOPMENT OF EARLY
MOTHER-PRETERM INFANT ATTACHMENT COACHING PROGRAM.
ADVISORY COMMITTEE: CHINTANA WACHARASIN, Ph.D., SUZANNE M.
THOYRE, Ph.D. 171 P. 2016.
Mother-preterm infant attachment has several potential inhibiting factors. A nursing
intervention to specifically promote mother-preterm infant attachment and lessen those factors
should be implemented. The purposes of this mixed-method embedded experimental design
were to develop the Early Mother-Preterm Infant Attachment Coaching (EMPAC) program
and examine its effect on maternal stress, maternal attachment, and mother-preterm infant
attachment. Participants were recruited by purposive sampling for the qualitative approach,
and randomly assigned 82 voluntary dyads of mothers and babies to the intervention and the
control groups equally for the quantitative approach were employed. Data were carried out in
2015 in Nakhorn Phanom hospital. The experimental group received the EMPAC program of
3 sessions for 10 days and the routine care, while the control group received only routine care.
Research instrument for data collection included the parent stress scale, the parenting stress
index-short form, the maternal attachment inventory and the mother-infant attachment Tool.
Their reliability were .96, .98, .80, and .90, respectively. Content analysis, descriptive
statistics, chi-square test, independent t-test, and repeated measure ANOVA were used to
analyze the data.
Results revealed that from the qualitative part perspective of mothers and health
care providers were that attachment is important and necessary for mothers and preterm
infants since the first week in hospital. The experimental group had significantly lower mean
score of maternal stress and higher mean score of maternal attachment and mother-preterm
infant attachment than in the control group. The EMPAC program could decrease maternal
stress, and increase mother-preterm infant attachment until 1 month corrected age of preterm
infant. The EMPAC program could enhance maternal attachment overtime up to 2 months
corrected age of preterm infants. Therefore, implementation this program at general hospital
is recommended.
vi
CONTENTS
Page
ABSTRACT ............................................................................................................... v
CONTENTS ............................................................................................................... vi
LIST OF TABLES ..................................................................................................... viii
LIST OF FIGURES ................................................................................................... x
CHAPTER
1 INTRODUCTION ............................................................................................. 1
Statements and significance of the problems ............................................. 1
Research objectives .................................................................................... 7
Research hypotheses .................................................................................. 8
Philosophical underpinning ........................................................................ 8
Conceptual framework ............................................................................... 10
Scope of the study ...................................................................................... 13
Definition of terms ..................................................................................... 13
2 LITERATURE REVIEWS ................................................................................ 16
Concept of mother-infant attachment ........................................................ 16
The nature of preterm infant ...................................................................... 29
Mother-preterm infant attachment ............................................................. 34
Factors related with mother-preterm infant attachment ............................. 37
Review of intervention with the mother-preterm infant attachment .......... 40
The nursing coaching model ...................................................................... 43
The early mother-preterm infant attachment coaching (EMPAC)
program ...................................................................................................... 49
3 RESEARCH METHODOLOGY ....................................................................... 51
Research design .......................................................................................... 51
Population and sample ............................................................................... 54
Setting of the study .................................................................................... 56
Instrumentations ......................................................................................... 56
Protection of human rights ......................................................................... 67
Data collection ........................................................................................... 68
vii
CONTENTS (Cont.)
CHAPTER Page
Data analysis .............................................................................................. 75
4 RESULTS .......................................................................................................... 77
Part 1: Development of EMPAC program ................................................. 77
Part 2: Verification the EMPAC program on maternal stress, maternal
attachment, and mother-preterm infant attachment ................................... 86
5 CONCLUSION AND DISCUSSION ................................................................ 104
Summary of the study ................................................................................ 104
Discussion of the research findings ........................................................... 107
Strengths and limitations ............................................................................ 113
Suggestions and recommendations ............................................................ 114
REFERENCES .......................................................................................................... 118
APPENDICES ........................................................................................................... 129
Appendix A ................................................................................................ 130
Appendix B ................................................................................................ 133
Appendix C ................................................................................................ 136
Appendix D ................................................................................................ 139
Appendix E ................................................................................................ 142
Appendix F ................................................................................................. 144
Appendix G ................................................................................................ 146
Appendix H ................................................................................................ 154
Appendix I .................................................................................................. 157
Appendix J ................................................................................................. 159
Appendix K ................................................................................................ 165
Appendix L ................................................................................................ 167
Appendix M ............................................................................................... 169
BIOGRAPHY ............................................................................................................ 171
viii
LIST OF TABLES
Tables Page
3-1 The early mother-preterm infant attachment coaching [EMPAC]
program and the usual care ............................................................................ 63
4-1 Acceptability rating scores of the program .................................................... 85
4-2 The demographic characteristics of mothers in intervention and the control
groups ............................................................................................................. 87
4-3 Compare means of characteristic of mothers between intervention and
the control groups .......................................................................................... 88
4-4 The demographic characteristics of preterm infants in intervention and the
control groups ................................................................................................ 89
4-5 Compare means of characteristic of preterm infants between intervention
and the control groups .................................................................................... 90
4-6 Mean and standard deviation for total and subscale scores, and mean score
difference and standard deviation of maternal stress in the intervention group
and control group ........................................................................................... 93
4-7 Mean and standard deviation of maternal attachment in the intervention
group and control group ................................................................................. 94
4-8 Mean and standard deviation for total and subscale scores, and mean score
difference and standard deviation of mother-preterm infant attachment in the
experimental group and control group ........................................................... 95
4-9 Comparisons of mean scores of maternal stress and maternal attachment the
intervention and the control groups at baseline ............................................. 96
4-10 Comparison of the mean score of maternal stress in hospital at discharge
day of preterm infant between intervention and the control groups .............. 97
4-11 Comparison of mean scores of maternal stress at home at 1 month corrected
age of preterm infants between intervention and the control groups ............. 98
4-12 Comparison of the mean score of mean difference of maternal stress at
home at 1 and 2 months corrected age of preterm infant between
intervention and the control groups ............................................................... 98

ix
LIST OF TABLES (Cont.)
Tables Page
4-13 Comparison the score of maternal attachment between experimental and
control group overtime at pre-intervention, discharge day of preterm infant,
1 month corrected age, and 2 months corrected age of preterm infant .......... 100
4-14 Mean different and compare the maternal attachment over 4 time points
of intervention group by Bonferroni..................................................... 101
4-15 Comparison of mean scores of mother-preterm infant attachment
at 1 month corrected age of preterm infants between intervention and
the control groups .......................................................................................... 102
4-16 Comparison of the mean score of mean difference of mother-preterm
infant attachment between intervention and the control groups at 1 and 2
months corrected age of preterm infant ......................................................... 103

LIST OF FIGURES
Figures Page
1-1 Conceptual framework of EMPAC program ................................................. 12
2-1 Bonding process, attachment process, and mother-infant attachment
process............................................................................................................ 26
3-1 Embedded design: Embedded experimental model ....................................... 52
3-2 Data collection process .................................................................................. 74
4-1 Mother-preterm infant attachment of mothers’, nurses’, and pediatricians’
perspective, Nakhon Phanom hospital ........................................................... 82
4-2 Hospitalized of preterm infants in nursery unit at Nakhon Phanom hospital 84
4-3 The mean score of maternal attachment between experimental and
control group overtime at pre-intervention, discharge day of preterm infant,
1 month corrected age, and 2 months corrected age of preterm infant .......... 101

CHAPTER 1
INTRODUCTION
Statements and significance of the problems
Mother-infant attachment is very important for establishing a basic sense of
trust to the world and developing emotional regulation of newborn via the strong and
satisfactory relationship with his/ her parent and caregivers. Mother-infant attachment
is a reciprocal positive interaction between mother and infant (Goulet, Bell, Tribble,
Paul, & Lang, 1998; Klaus & Kennel, 1982). The infant who experiences a
satisfactory attachment to his/ her mother is more likely to explore the surrounding
environment, using its mother as a secure haven for environmental exploration
(Malekpour, 2007). Through this exploration of the environment, the child gains
greater competence, acquiring greater independence in future experience (Malekpour,
2007). Studies indicated that infants who demonstrate secure attachment would
continue to be secure through childhood and adolescence, eventually becoming
autonomous adults (Goldberg, 2000). Children who have attachment security, have
a stable self-esteem, better self-perception accuracy, greater self-clarity, and a better
organized self-structure than insecure children (Goulet et al., 1998; Wu, 2009).
Furthermore, a mother who experiences a satisfactory attachment to her infant is more
likely to develop the self-confidence of maternal attachment and maternal role (Goulet
et al., 1998). Therefore, if mother and infant have an excellent mother-infant
attachment, this will benefit infant’s psychosocial development and maternal role.
However, mother-infant attachment is difficult to promote in the risk group, especially
in the group of preterm infants (Orapiriyakul, Jirapaet, & Rodcumdee, 2007).
Preterm birth as the unexpectedly early birth that is interrupts the attachment
process. This interruption and the fear for the infant’s safety and well-being may
complicate the mother-preterm infant’s attachment process and also affect the
relationship between the different components of the relationship (Korja et al., 2010).
In addition, at separation, the preterm infant’s cues and behavioral state are often
difficult to read (VandenBerg & Hanson, 2013). As a result, there is less interaction
between the preterm infant and mother; infants tend to be less responsive to social
2
stimulation, and show more gaze aversion than full term infants (DiVitto & Goldberg,
1979). Infants’ poor interactive behavior remained as a significant predictor of child’s
chronic or recurrent health problems during the two years of age (Mantymaa et al.,
2003). Furthermore, several studies found more insecurely attached preterm infants
compared to term born infants (Korja et al., 2010; Mangelsdorf et al., 1996).
Insecure attachment of preterm infants is a negative feeling of interaction
between preterm infant with attachment figure (Ainsworth, Blehar, Waters, & Wall,
1978; Bowlby, 1969). Ainsworth et al. (1978) classified attachment of infant into four
types, namely secure attachment, ambivalent attachment, avoidant attachment, and
disorganization attachment. If infants have ambivalent attachment, they often do not
learn or understand emotions of their own or others. If infants have avoidant
attachment, they develop a sense that they cannot contact with their world, so they
will not engage others. It is likely that these infants will delay in development, passive
behavior, and may confront full-blown reactive attachment disorder. Likewise, if
infants have disorganization attachment, they show no emotional response, and in
fact, they are often described as being emotionally absent (Ainsworth et al., 1978;
Goldberg, 2000). In addition, preterm infant gestational age less than 32 weeks had
disorganized attachment 32 % that more than full term infant had disorganized
attachment 17 % (Wolke, Eryigit-Madzwamuse, & Gutbrod, 2014). Thus, due to the
inability to reach a level of attachment security, preterm infants might be at risk of
various problems such as social-emotional and cognitive development.
Mother is the closest and the most significant attachment figure for preterm
infant. Mother should have high maternal sensitivity which includes mutually give
and take with the preterm infant that is congruent with the preterm infant's cues.
Maternal sensitivity is an important precursor for maternal-infant attachment, infant
attachment security, and infant development (Ainsworth et al., 1978; Bakermans-
Kraneuburg, van Ijzendoorn, & Kroonenberg, 2004; Belsky, 1999; Cassidy & Shaver,
1999; Kalinauskiene et al., 2009; Shin, Park, Ryn, & Seomun, 2008). Maternal
sensitivity is the quality of a mother’s sensitive behaviors that are based on her
abilities to perceive and interpret her infant’s cues and respond to them (Ainsworth
et al., 1978; Shin et al., 2008). A mother’s sensitive behavior must be contingent on
her infant’s behaviors and have the quality of a reciprocal interaction with her infant.
3
It is a dynamic process which accompanies the adaptation and changeability (Shin
et al., 2008). Mothers who show higher maternal sensitivity tend to have higher
maternal attachment and mother-infant attachment (Shin, Park, & Kim, 2006).
However, the mother of the preterm infant has not been able to prepare
herself for separation from the infant (Korja et al., 2009). The interrupted
representation process, a traumatic birth experience, early separation and a fear for the
infant’s safety may inhibit the mother’s attachment process (Korja et al., 2009).
Because of the preterm infant’s life-threatening condition, mothers of preterm infants
may experience uncertainty about his/ her chances of survival. Mothers of preterm
infants have been found to be concerned about becoming too attached for fear of
infant death (Howland, 2007), lower coherence, less acceptance (Korja et al., 2009),
less richness of perceptions, less openness to change, and lower intensity of
involvement (Inwongwan, Lamchang, & Thanasuwan, 2008). All of these conditions
of the hospitalization of preterm infant will be a stressful event for mothers (Engler,
2005). The inability to read the preterm infant's cues or fear of medical equipments
and the uncertain environment of the Neonatal Intensive Care Unit [NICU] increases
maternal stress (Miles, Funk, & Carlson, 1993; Shin et al., 2008). Maternal stress
tends to decrease maternal sensitivity over time (Shin et al., 2008). When mothers
have low sensitivity, the maternal attachment and mother-infant attachment will
decrease (Shin et al., 2008), and the preterm infant is more likely to develop
attachment insecurity. In Thailand, Phatthanasiriwethin (2001) identified that some
mothers have declined to interact with their preterm infants. Mothers did not spend
much time, only 2-5 minutes, at their first visit to their preterm infant. The physically
separating between mother and preterm infant is a causing of stressful situation for
mother (Sannino, Plevani, Bezze, & Cornalba, 2011). In addition, Orapiriyakul et al.
(2007) found that the process of maternal attachment to preterm infants in the NICU
was struggled to get connected. The mothers had difficulties connecting physically
and psychologically with their preterm infants while hospitalized in the NICU.
The process of actions or interactions of maternal attachment to the preterm infants
sequentially consisted of withdrawal contacting, seeking closeness, mutual mother-
preterm infant interacting and committing to mothering, concerning for the preterm
infant, adjusting emotionally to the crisis, supporting connections, life experience and
4
health care system facilitating. Affection of maternal attachment to the preterm infant,
which was disrupted at birth or delayed during early hospitalization in the NICU or
nursery unit, must be resumed to a normal level as quickly as possible. Preterm birth
and hospitalization of the preterm infant in the NICU was a crisis experience for
mothers and their families. Mothers need support from family and health care
providers in order to reduce stress and develop attachment to her preterm infant since
from early state after birth.
As a result, the mother-preterm infant attachment has many inhibiting
factors. The important inhibiting factors include maternal stress (Engler, 2005; Miles
et al., 1993; Shin et al., 2008), lack of understanding of preterm infant's cues (Miles
et al., 1993), less responsiveness of preterm infant (DiVitto & Goldberg, 1979), and
early separation (Korja et al., 2009). Therefore, the nursing intervention to promote
mother-preterm infant attachment should try to minimize barrier factors especially the
barrier from maternal factor. The nursing intervention should decrease maternal stress
and improve the perception of maternal attachment in early period of post-partum in
order to help mother to understand her preterm infant’s cues and develop high
confident to respond and interact with the preterm infant. It will promote the behavior
of attachment between mothers and preterm infants.
Current nursing interventions had rare interventions that related with
maternal stress, maternal attachment, and mother-preterm infant attachment. There
were only eight studies about decreasing maternal stress and promoting maternal
attachment, and mother-preterm infant attachment. However, there were only five
effectiveness studies about decreasing maternal stress and promoting maternal
attachment, and mother-preterm infant attachment. First study, maternal-infant
interaction program (Trisayaluk, 1999) included encouraging mother to interact with
preterm infant by using sensory stimulation 3 times/ week from after birth to two
weeks. This program could enhance maternal attachment after finishing the program
and two weeks after a preterm infant was discharged from hospital. Second study,
multi-modalities sensory stimulation program (Charoensri, 2002), consisted of
auditory, tactile, vestibular, and visual sensory stimulation by mother once a day until
preterm was one month old. This program could promote maternal attachment at one
month old of preterm infant. Third study, mother providing preterm infant massage
5
program (Lokham, 2003) was a massage from mother to preterm infant once a day
from the second visit until preterm infants were about 20 days. This program could
enhance mother-preterm infant attachment after the program completed. Forth study,
video-feedback intervention to promote positive parenting (Kalinauskiene et al., 2009)
included video record and video feedback about mother-infant interaction from seven
to twelve months of age. Mothers would be asked to keep journal about infant crying,
fussing, sleeping, awaking and being satisfied behavioral states, and reactions with
caregivers’during feeding and playing. This program could enhance maternal
sensitivity at 12 months of infant’s age that is benefit for mother-infant attachment.
Final study, mother-infant transaction program (Newnham, Milgrom, & Skouteris,
2009) was consisted of nine sessions that were teaching mother about recognizing
infant’s disorganization/ stress cues, responding to infant’s cues, guiding principle
during care and play, massaging, having kangaroo care in hospital, and home visiting
at one and three months for mutual enjoyment through play. The result found that this
program helped mother reducing stress at three months. Therefore, information could
decrease maternal stress, sensory stimulation and interaction could promote maternal
attachment, and interaction through massage could enhance mother-preterm infant
attachment. This results showed that some of programs could decrease maternal stress
and some could increase maternal attachment or enhance mother-preterm infant
attachment. Yet, there haven’t been the one program that could decrease maternal
stress, promote maternal stress and mother-preterm infant attachment all together.
Moreover, most of the programs were developed by other countries, they might not fit
in our Thai culture because the broader cultural context in which families live that can
influence the formation of attachment (Goldberg, 2000).
The process of maternal-preterm infant attachment was difficultly to get
connection, especially in the early state after birth. Mother and preterm infant’s
bonding process got interrupted from early state after birth causing separation causing
mother’s emotional stress. In addition, mother could not understand her preterm
infant's cues that might decrease maternal sensitivity, and cause difficulty in promoting
maternal attachment and mother-preterm infant attachment. Contemporary interventions
to promote mother-preterm infant attachment were unclear in effectiveness to reduce
maternal stress, and enhance maternal attachment and mother-preterm infant
6
attachment. On top of that, most of programs were developed form other country,
it might not fit with the Thai culture.
Therefore, neonatal nurses need to develop an appropriate nursing
intervention to help Thai mothers reduce maternal stress, and enhance maternal
attachment and mother-preterm infant attachment. New intervention should apply
research evidences integrating contents of interventions such as providing knowledge
about preterm infant's cues, behavior, and need of preterm infant (Newnham et al.,
2009), encouraging mother-preterm infant interaction (Trisayaluk, 1999), guidance
strategies to enhance attachment by multi-modalities sensory stimulation (Charoensri,
2002), and video-feedback (Kalinauskiene et al., 2009). In order to create a new
strong intervention, the protective factors such as family and health care provider’s
support should be integrated in it. Encouragement from father will provide emotional,
information, appraisal support for mother (Tiden, 1985) because spouse was the best
supporter (Klaus & Kennell, 1982). Besides, marital relationship could predict
mother-infant attachment (Soakeaw, 2007). In addition, support from grandmother
will encourage mother to interact confidently with her preterm infant. Moreover,
health care provider is an important social support for mother of preterm infant.
Therefore, it is highly recommended to involve family and caregivers especially
nurses in to the new intervention.
Moreover, new intervention should apply relevant theories that can change
the cognitive, affective, and behavior. It should prepare mother with knowledge about
preterm infant's cues and include strategies to promote attachment, positive emotions,
and competency to attach with her preterm infant. The idea should be in congruence
with the nursing coaching model which could help the coachee to change the thought,
feeling, and improving behavior (Kowalski & Casper, 2007). The coaching model was
significant for improving parent caring practice skill such as enhancing caring practice
skill among parent of children with pneumonia (Apichaiyawat, Lamchang, & Yenbut,
2010), and promoting caring practice skill among parent of children with asthma
(Suksawat, Lamchang, & Jintrawet, 2012). Therefore, nursing coaching model might
be effective for changing emotional, cognitive and behavior of mother in order to
promote mother-preterm infant attachment. Furthermore, the new intervention should
be developed base on the context of the mother-preterm infant attachment in Thailand
7
such as family relationship, culture, belief, daily living, and competency of mothers.
Besides, the new intervention should be developed base on clinical knowledge from
pediatrician, and NICU and nursery nurses (Whittemore & Grey, 2002). Due to the
complex of family and preterm infant situations inherent in the NICU, today more
than ever before, nurses need to be aware and be active facilitators of the attachment
process for these families (Schenk, Kelley, & Schenk, 2005).The new intervention
should be updated and appropriate for mother-preterm infant attachment in NICU and
nursery unit. Therefore, the development of new intervention to enhance mother-
preterm infant attachment should integrate theory, research evidences, clinical
knowledge of pediatrician and NICU nurses, and perspective of mother. The mixed
method design would be applied to deep understanding of context of mother-preterm
infant attachment by qualitative method, and testing the effective of this intervention
by quantitative method.
The purpose of this study was to develop and verify the early mother-
preterm infant attachment coaching [EMPAC] program integrating the concept of
mother-infant attachment and nursing coaching model, research evidences, clinical
knowledge of pediatrician, and nurses, and mother’s perspective. This intervention
also aimed to decrease maternal stress, and enhance maternal attachment and mother-
preterm infant attachment. Also, if preterm infants and mothers developed positive
attachment, preterm would enhance emotional regulation, and beneficial long-term
social-emotional and cognitive functioning (Page, Wilhelm, Gamble, & Card, 2010).
Furthermore, the outcome of this study would help pediatric nurses to have a model of
intervention for promoting mother-preterm infant attachment that fit with the context
of Thai family.
Research objectives
The specific objectives as follows:
1. To develop a mother-preterm infant attachment intervention.
2. To examine the effectiveness of the mother-preterm infant attachment
intervention on maternal stress, maternal attachment, and mother-preterm infant
attachment.
8
Research hypotheses
1. Mothers who received the EMPAC program had significantly lower mean
scores of the maternal stress at hospital on the discharge day than those who did not
receive.
2. Mothers who received the EMPAC program had significantly lower mean
scores of the maternal stress at home on 1 month corrected age of preterm infants than
those who did not receive.
3. Mothers who received the EMPAC program had significantly higher
mean score differences of maternal stress at home between 1 and 2 months corrected
age of preterm infants than those who did not receive.
4. Mothers who received the EMPAC program had significantly higher
mean scores of the maternal attachment on the pre-intervention, discharge day of
preterm infant, and 1 and 2 months corrected age of preterm infants than those who
did not receive.
5. There were significant differences in mean scores of maternal attachment
across the four points of time in experimental group at pre-intervention, discharge day
of preterm infant, and 1 and 2 months corrected age of preterm infants.
6. There were significant differences in mean scores of maternal attachment
between groups and times.
7. Mothers who received the EMPAC program had significantly higher
mean scores of the maternal-preterm infant attachment on 1 month corrected age of
preterm infants than those who did not receive.
8. Mothers who received the EMPAC program had significantly higher
mean score differences of maternal-preterm infant attachment between 1 and 2
months corrected age of preterm infants than those who did not receive.
Philosophical underpinning
The philosophical base to explain the nursing phenomenon is post-
positivism paradigm. Guba (1990) state ontology of post-positivism that is critical
realism-reality but only imperfectly, probabilistically apprehensible and fragmentable.
It focuses on the discovery of a reality characterized by patterns and regularities that
maybe used to describe, explain, and predict phenomenon (Ford-Gilboe, Campbell, &

9
Berman, 1995). Epistemology of post-positivism is modified objectivist that is
objectivity remains a regulatory ideal, but it can only be approximated, with special
emphasis placed on external guardians such as the critical tradition and the critical
community (Guba, 1990; Newman, 1992). The methodology of this study is
manipulate and modified experimental and focusing on falsification of hypotheses
rather than verification (Guba, 1990). Using quantitative and qualitative data help
overcome the limitations of each and provide stronger support for a hypothesis than
could be achieved with either method alone (Ford-Gilboe et al., 1995).
The phenomenon of interest in this study is mother-preterm infant
attachment. I believe that reality of early mother-preterm infant attachment is
probability for enhancing. However, it is imperfectly. Preterm infants have varies
behaviors according to gestational age. They become stress when they have to adjust
to extra uterine life before they are ready. They may have little excess energy for
maintaining muscle tone and poor development of flexion. Preterm infants are easily
exhausted from noise and routing activities. Their responses are varied, including
lowered oxygenation levels and behavior changes. Their cries may be feeble, less alert
and less responsive in interaction (Korja et al., 2010). Moreover, mothers of preterm
infants were inability to read the preterm infants cues and fear of medical equipments
and the uncertain environment of the NICU (Shin et al., 2008). Besides, mothers were
afraid of losing their preterm infants (Danerek & Dykes, 2009) that tend towards
maternal stress and maternal attachment.
Therefore, mothers and preterm infants are having stresses and difficult for
reciprocal relationship that may be unavailable for maternal attachment,
mother-preterm infant attachment, and direct to mother-preterm infant attachment.
However, preterm infants are human being that means they need bonding and
attachment from attachment figure especially from their mothers. Mother-preterm
infant attachment can promote by decreasing maternal stress, stimulating mothers’
bonding in early birth, and continue promoting maternal attachment. Nevertheless,
enhancing mother-preterm attachment can never be fully apprehended. Therefore,
the reality of mother-preterm infant attachment is incompletely understood of this
situation because human nature and family are complexity.

10
Epistemology of this study is come to mean more than directly observable
sense data of objectivist. It includes both perceptions and a symbolic meaning that
may be accessed through self-reports, stories of mother, and observable behavior of
mother-preterm infant attachment after manipulative intervention. Likewise, research
should test falsification of hypothesis by interaction with them by quantitative and
qualitative method. Therefore, methodology of this study will be use mixed method
design for decreasing maternal stress, and promoting maternal attachment and
mother-preterm infant attachment in the complexity of this phenomenon.
Conceptual framework
The conceptual framework of this study applies of the maternal-newborn
attachment concept (Klaus & Kennell, 1982), coaching concept (Kowalski & Casper,
2007), and research evidences. Klaus and Kennel (1982) described that the attachment
between a mother and her infant is a unique relationship that occurs particularly
between two. It will increase when the mother and the infant respond positively to
each other. The process of relationship creation between the mother and the infant
during postpartum period will show the interaction of both the mother to the infant
(touch, eye-to-eye contact, high-pitched voice, entrainment, and heat), and the infant
to the mother (eye-to-eye contact, cry, entrainment). This relationship will be firmly
stable forever that relates to mother’s attention to take care of her child. Behavior of
mother-preterm infant attachment will occur, if mother had a good perception of
maternal attachment, and provide quality interaction with preterm infant. Therefore,
the new intervention should promote mother to provide quality interaction with
preterm infant during postpartum period.
In addition, the coaching concept for nursing (Kowalski & Casper, 2007)
is specific tools and a framework for improving performance that focus on change
cognitive, affective, and behavioral. It consists of three major components: “the
foundation” for the coaching process; “the learning process,” which occurs during
coaching; and “taking action,” which encompasses changes in behavior. This process
can significantly improve future performance. Therefore, the new intervention should
apply coaching model integrating in the program that might enhance the mother-
preterm infant attachment. Moreover, the new intervention should integrate research
11
evidences in the content of intervention such as providing knowledge of preterm
infant's cues, behavior, and need of preterm infant (Newnham et al., 2009), encouraging
mother-preterm infant interaction (Trisayaluk, 1999), guidance the strategies to
enhancing attachment by multi-modalities sensory stimulation (Charoensri, 2002),
and video-feedback (Kalinauskiene et al., 2009). The new intervention, EMPAC
program was developed. The EMPAC program has a five steps that include
1) creating trusting relationship for developing trust between coach with coachee for
establishing and maintain the relationship, 2) understanding context of attachment for
expression mother's feeling about situation of her preterm infant for helping mother to
understand her feeling and her problem in this situation, 3) Setting realistic
expectation for encouragement mother to make a commitment to achieving goal of
promoting attachment for her preterm infant, and encouragement family such as father
or grandmother involvement to help mother to develop an action plan for enhancing
attachment for her preterm infant, 4) supporting information for giving information
about preterm infant’s cue, behavioral state of preterm infant, preterm infant’s need
and how to response to preterm infant’s signals for mother by hand out and
demonstration one by one, 5) reflecting & evaluating for observing, giving positive
reinforcement, and feedback the attachment from mother to her preterm infant by
video feedback. In addition, this step will encourage mother to feedback herself about
her cognitive, affective, and behavior changing to attach her preterm infant. It will
helps mother to learning her preterm infant, understanding her preterm infant’s cue,
decreasing maternal stress, increasing maternal attachment, and changing behavior to
attach her preterm infant. (Figure 1-1)
12
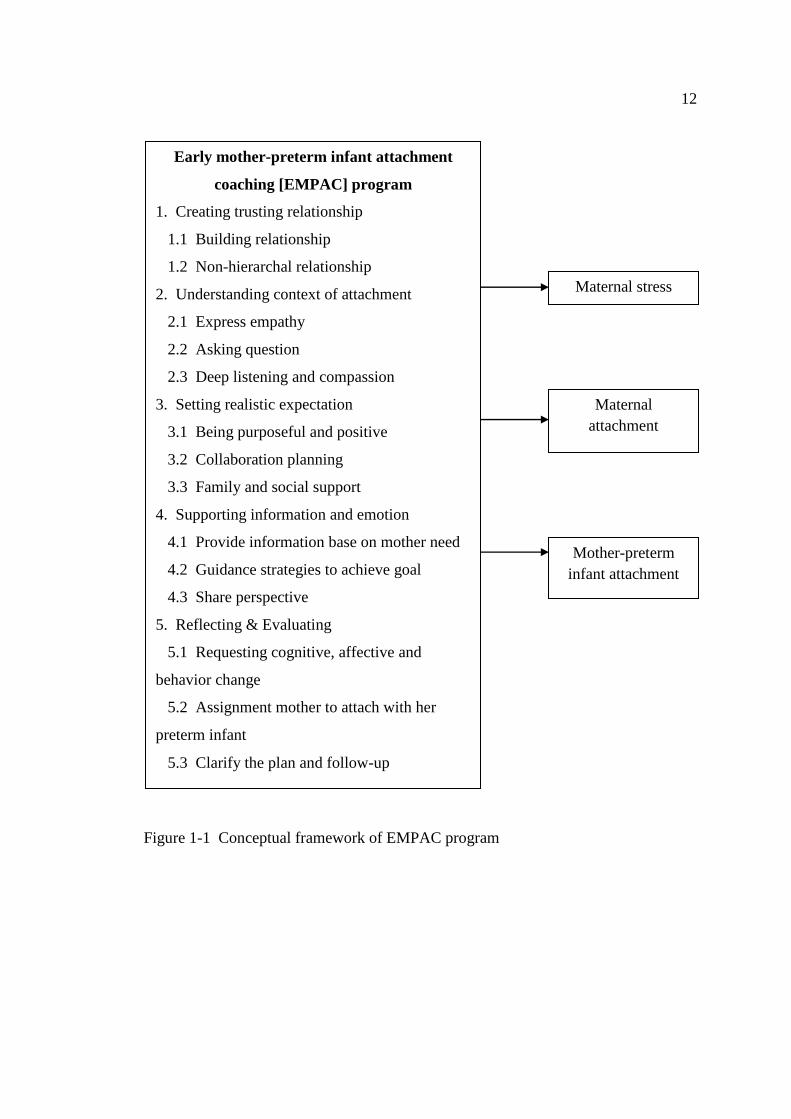
Figure 1-1 Conceptual framework of EMPAC program
Early mother-preterm infant attachment
coaching [EMPAC] program
1. Creating trusting relationship
1.1 Building relationship
1.2 Non-hierarchal relationship
2. Understanding context of attachment
2.1 Express empathy
2.2 Asking question
2.3 Deep listening and compassion
3. Setting realistic expectation
3.1 Being purposeful and positive
3.2 Collaboration planning
3.3 Family and social support
4. Supporting information and emotion
4.1 Provide information base on mother need
4.2 Guidance strategies to achieve goal
4.3 Share perspective
5. Reflecting & Evaluating
5.1 Requesting cognitive, affective and
behavior change
5.2 Assignment mother to attach with her
preterm infant
5.3 Clarify the plan and follow-up
Maternal stress
Maternal
attachment
Mother-preterm
infant attachment
13
Scope of study
The present study was a mixed method study which aim to developed and
examined the EMPAC on maternal stress, maternal attachment, and maternal-infant
attachment. The mother-infant dyads who participated in this program were mothers
who have the preterm infant of gestational age < 35 weeks, body weight between
1,000-2,000 grams and admit in nursery unit at Nakhon Phanom hospital since June
2014-June 2015.
Definition of terms
Early mother-preterm infant attachment coaching [EMPAC] program
referred to nursing intervention that derived from mother-infant attachment model,
coaching model, research evidence, and perspective of mother having preterm infants,
nurses, and Pediatricians. This intervention started since second time when mother
visit her preterm infant until 10 days in hospital with 3 sessions. The process of
intervention for every session had five stages as followed:
1. Creating trusting relationship: Creating trusting that described as
a cocreative relationship. This stage consisted of building relationship, the art of being
present, and non-hierarchal relationship. Coach (researcher) contacted with coachee
(mother) and her family (father or grandmother) since second time when her visit her
preterm for developing trust between coach with coachee for establishing and
maintain the relationship.
2. Understanding context of attachment: It was an individual approach that
approached by expressing empathy, asking question, and deep listening and
compassion. The coach encouraged the coachee to explored and expressed her
feelings and beliefs about illness of preterm infant. The coach ask questions relevant
to the coachee’s ability and infant care needs and problems. The coach provided deep
listening with compassion, and respecting belief and ability of mother. The coach
clarified the problems of attachment for preterm infant and transformed the agenda
in to action step through listening intently, asking powerful question, and serving as
catalyst in moving mother toward to taking attachment and achieving desired solution.
3. Setting realistic expectation: Coach encouraged coachee to made
a commitment to achieving goal of promoting attachment for her preterm infant.
14
In addition, coach encouraged family such as father or grandmother involvement to
help mother to developed an action plan for enhancing attachment for her preterm
infant.
4. Supporting information and emotion: Coach give information about
preterm infant’s cue, behavioral state of preterm infant, preterm infant’s need and how
to response to preterm infant’s signals for coachee by chart desktop of mother-preterm
infant attachment and demonstration that depended on need of mother. It taught one
by one that focused on looking at the mother’s own infant, and talking about her
infant’s cue. In addition, coach gave information depended on mother's questions and
mother' s need.
5. Reflecting and evaluating: Coach became a partner behind coachee when
her interacted with her preterm infant. Coach in this stage observed, gave positive
reinforcement and feedback the attachment from mother to her preterm infant by
video feedback. In addition, coach encouraged coachee to interact with her preterm
infant and feedback herself about her feeling, perception, and behavior changing to
attached her preterm infant.
Maternal stress at hospital was responding of the mother when she could
not cope with the situational stressors due to the preterm infant birth. The stressors of
the preterm infant birth in hospital consisted of stress from sights and sounds in the
NICU and nursery unit, the preterm infant’s appearance, and relationship with the
preterm infant and maternal role. It was measured at the second time visit of mother to
her preterm infant (pre-intervention), and discharge day of preterm infant by using
The parenting stress score: NICU (Miles et al., 1993).
Maternal stress at home was responding of the mother when she could not
cope with the situational stressors due to preterm infant at home. It included maternal
distress, difficult child characteristics, and dysfunctional mother-child interaction.
It was measured at 1 and 2 months corrected age of the preterm infant by using parent
stress index (Abidin, 1990, 1995).
Maternal attachment was a mother’s affection about her relationship with
her preterm infant that included her perception of her infant’s signals, and her
responsiveness to preterm infant. It was measured at second time of mother to visited
her preterm infant (pre-intervention), discharge day of preterm infant, and 1 and 2

15
months corrected age of the preterm infant by using The maternal attachment
inventory (Muller, 1994).
Mother-infant attachment referred to an enduring reciprocal relationship
or interaction between mother and preterm infant. It includes the responsiveness
behavior of mother to preterm infant, and redundant behavior of preterm infant to
mother, when they were interaction with tactile, visual, auditory, and feeding.
It measured at 1 and 2 months corrected age of the preterm infant by using the
mother-infant attachment tool that modified from mother-infant screening tool of
Reiser (1981).

CHAPTER 2
LITERATURE REVIEWS
This chapter, related literature and research are reviewed in the following
seven topics that consist of a) concept of mother-infant attachment, b) the nature of
preterm infant, c) mother-preterm infant attachment, d) factors related to mother-
preterm infant attachment, e) systematic review the interventions of mother-preterm
infant attachment, and d) coaching model, and e) Early mother-preterm infant
attachment coaching [EMPAC] program.
Concept of mother-infant attachment
The mother-infant attachment start with bonding that refers to the rapid
initial attraction felt by parent for his/her infants. It is unidirectional from parent to
infant, and is enhanced when parents and infants are permitted to touch and interact
during a, so-called, sensitive period extending through the first 30-60 minutes after
birth. An enduring bond between a parent and infant promotes attachment (Klaus &
Kennell, 1982). Attachment is an affection tie on the infant to attachment figure.
The significance attachment figure is usually being mother. Infant will response to the
bonding from parent such as a quiet, alert state, seeming or gazing directly at the
parents (Bowlby, 1969). Therefore, the terms of bonding and attachment represent
different concepts. Bonding is the process of the parent's attachment to his/ her infant.
On the other hand, attachment is the process of the infant's attachment to his/ her
attachment figure. Therefore, the concept of mother-infant attachment formulated
from the concept of bonding (Klaus & Kennell, 1982) and attachment (Bowlby, 1969;
Aisworth et al., 1978). However, the concept of maternal infant attachment was of
often used interchangeably with the terms of maternal infant bonding (Kinsey &
Hupcey, 2013)
Klaus and Kennell (1982) defined bonding “as a unique relationship between
people that is specific and endures through time.”
Bowly (1969) defined attachment as an affective tie of infant to attachment
figures, as well as a behavioral system operating in the service of the goal of
17
providing the infant a sense of security.
Mercer and Ferketich (1994) described attachment as “an interactive process
between parents resulting in satisfying experiences and an emotional bond that
motivates parental commitment in caring for the infant.”
Kinsey and Hupcey (2013) define maternal infant bonding is “a process that
includes the emotional tie of a mother to her infant, occurring in the first week or year
of a baby’s life.”
In summary, the concept of maternal infant attachment is frequently defined,
but not consistently across studies. In this study seem to agree that maternal infant
attachment is a process of emotional relationship between mother with her infant that
occur when they are interaction.
The attribution of mother-infant attachment was proximity, reciprocity, and
commitment (Goulet et al., 1998). Proximity means the physical and psychological
experience of the mother being close to infant. The attribution of proximity comprised
three dimensions: contact, emotional state, and individualization. Firstly, contact was
the sensory experiences of touching, holding, and gazing at the infant. Secondly,
emotional state was emerged from the affective experience of the new mother toward
her infant and her maternal role. Finally, individualization of the mother was also
aware of the need to differential the infant's needs from herself, to recognized and
responded appropriately, and making the attachment experience. Reciprocity was the
process by which the capability and behavioral characteristics of the infant's cues
elicit mother response. The infant, the other one in this interaction process, and his
ability to reinforce the mother's care giving efforts contributed to the quality of the
exchanges that take place. This is a process of both mother and infant responding to
the cues of the other, such as the mother responding to the crying cues of the infant,
and the infant giving back cues of satisfaction in response to the mother's efforts.
Commitment referred to the enduring nature of the attachment relationship. Mother
places the infant at the centre of her life and her family. Mother acknowledges her
responsibility for the well-being of her infant and promotes its safety, growth, and
development. In addition to the ability of the mother to find her own way, it integrates
the maternal identity into herself.
18
Maternal attachment process
Maternal attachment refers to the perception of affection tie that a mother
feels toward her infant. This was reflected a developing growth of positive feelings on
the part of the mother toward her infant, and included such dimensions as wanting to
possess, to prolong, or to seek contact, and to be proud of and to love her infant that
developed through their interactions (Carson & Virden, 1984; Gottlieb, 1978).
Maternal attachment is a natural process of motherhood that starts from the
very beginning of pregnancy or even before being pregnant and gradually develops
and increase throughout the time of pregnancy and will lasts a lifetime. Klaus and
Kennell (1982) have listed events that are important to the formation of maternal-
infant attachment in three phases.
1. Prior to pregnancy, mothers-to-be and her families have to start planning
of having a child or more. That is an important point of an impact on maternal-infant
attachment. The mothers begin to expect and imagine what their infants will be like.
At this point they already started developing an attachment with their infants.
However, Klaus and Kennell (1982) stated that the mothers’ past experience with
their own mothers in their childhood were the major determinant in molding maternal
attachment behaviors, while the prenatal attachment process provided the structure for
postnatal maternal attachment.
2. An antepartum period is the first stage of pregnancy when a woman
should come to term with the knowledge that she is going to be a mother. Once
quickening occurs, the infant’s reactions add to her fantasies, as she begins to attach
positive or negative meaning to its movements. By the end of the pregnancy, the
mother may have a lot of imaginations about her infant’s characteristics, such as facial
feature, temperament, strength, sex and size. The mother’s attitudes about the
pregnancy itself may influence her feelings about her infant. Most of woman initially
experience some degree of ambivalence because the infant will impose some changes
in her lifestyle and in her relationship with the father and other family members.
Ambivalence can be intensified by an unplanned or teenage pregnancy. It may also be
intensified by a pregnancy which is likely to impose an emotional, physical or
economic strain on the mother or her family. If the mother is able to resolve the
ambivalence, her feeling about the infant is more likely to be positive which will

19
foster her attachment to the expected infant. On the other hand, if the ambivalence
continues, the mother may have a negative view and attachment to her baby at birth.
3. Intra-partum and post-partum periods, the period of birth is the crucial
time of life, especially the shortly time after birth. It is the time that the maternal-
infant newborn attachment is developed which is the highlight of pregnancy.
According to Klaus and Kennell (1982), this attachment has so strong power that
enable the parent to make unusual sacrifices to care for their baby all day all night.
The time right after birth is a sensitive period. It is the first minute, first hour and first
day of the new life, so this period is important for enhancing mother-infant
attachment. Klaus (2009) presented that the early period after birth was not a “critical”
period but a “sensitive” period for promoting bonding and attachment, respectively.
The attachment still continued until two years later. Troy (1995) examined maternal-
newborn attachment in 67 postpartum mothers and found that there was association
between immediate holding of the newborn after birth, self-esteem and maternal-
newborn attachment. In other word, the mothers who get to hold their babies
immediately after birth have higher level of maternal-newborn attachment which will
lead to positive attachment process.
In conclusion, if mother have positive maternal attachment process, it will
promote a positive attachment process
Infant attachment process
The development of infant attachment includes 4 phases: 1) the initial pre-
attachment phase; 2) the phase of attachment-in-the-making; 3) the phase of clear-cut
attachment; and 4) the phase of goal-corrected partnership (Bowlby, 1969; Ainsworth
et al., 1978).
1. The initial pre-attachment phase. This phase the infant’s motor and signal
systems are already particularly adept at eliciting interest and caregiving from other
humans, ensuring that a number of needs, including proximity, physical contact,
nutrition, and warmth are predictable outcomes (Marvin & Brittner, 1999).
Additionally, infants respond to stimuli in ways which increase their likelihood of
continued contact with other people. At this stage, however, the infant shows
undiscriminating social responsiveness, as the infant lacks the ability to differentiate
between individuals. They will respond to anyone in their vicinity with a number of
20
characteristic behaviors including orienting, tracking with his/her eyes, grasping,
smiling, reaching, or ceasing to cry.
While the infant shows undifferentiated social responsiveness during the
first phase of development, the caregiver is of great importance in the development of
attachment, as it is primarily the caregiver who maintains proximity to the infant and
protects it at this time (Marvin & Britner, 1999). Further, just as infants are biased to
act in ways that evoke caregivers, mothers are biased to behave in particular ways
toward their infants, such as by holding the infant in a face-to-face position likely to
orient him or her to her, as well as allowing the infant to more easily explore her
(Bowlby, 1969). Thus, both infants and caregivers experience a great deal of
interaction during these early months. Through these early interactions and
correspondences between the infants and caregivers that their attachment is gradually
developed and become stronger.
During the first period of life, these patterns of infant-caregiver interaction
are frequently repeated. If the caregiver’s initiation and responses are well attuned to
the infant’s behavior, stable and predictable patterns of interaction may be established.
These patterns of reciprocal infant-caregiver-behavior interaction will gradually
minimize the frequency and intensity of attachment behaviors such as crying.
It should be easier to elicit other behaviors such as smiling or visual orientation.
Given this context, it might be seen as the infant establishes its own behavior and auto
regulation so that stable internal and dyadic rhythms are becoming established
concurrently (Marvin & Britner, 1999). Bowlby (1969, 1982) proposed that in an
environment of evolutionary adaptedness, an environment in which the conditions
were well-suited to those abilities chosen by the process of natural selection.
He suggested that phase I lasted from birth to sometime between 8 and 12 weeks of
age. However, it could last much longer under unfavorable conditions, including
neglect or maltreatment.
2. The phase of attachment-in-the-making. During this phase, the infant
begins to show differential responsiveness and the phase may be operationally defined
in terms of the infant’s differentiating between his most familiar caregivers and others
in directing his or her attachment behaviors (Marvin & Britner, 1999). The infant
generally continues to behave in a friendly and sociable manner toward others, as he
21
or she did during Phase 1, but does so in a more marked fashion toward attachment
figures, such as the mother, than toward others (Bowlby, 1969, 1982). Thus, the infant
responds differently to his or her mother’s voice, maintains a different visual-postural
orientation toward the mother, cries differently when his or her mother departs, ceases
crying differentially according to who holds him, smiles and vocalizes differentially,
and shows differential greetings (Ainsworth et al., 1978). The shift between
undifferentiated responding (characteristic of phase 1) and differentiated responding
(characteristic of phase 2) happens gradually along with some attachment behaviors
showing evidence of differential response before others.
During this phase, the simple behavior systems (characteristic of the phase
1) infant becomes integrated into more complex, chain-linked behavior systems
(Marvin & Britner, 1999). While the caregiver in Phase 1 provides the conditions for
terminating one behavioral link in a chain and activating the next, during phase 2 the
infant assumes much of this control (Marvin & Britner, 1999). For instance, at three
months, the infant’s perception of a bottle or breast may serve as an activating
stimulus for opening the mouth, and often, bringing the hand toward the mouth
(Hetzer & Ripin, 1930 cited in Bowlby, 1969). By four months, the infant’s visual
system begins to activate the motor behavior of reaching for an object and through a
reciprocal feedback process, wherein the infant alternates his or her gaze between the
hand and the object, eventually grasps the object. By five months, the infant will be
skillful at this activity that he or she is able to reach toward and grasp parts of the
mother’s body and clothing while being held (Marvin & Britner, 1999). Thus, the
infant’s behaviors become increasingly complex and self-directed. If simple
preference of one figure over others is the criterion of attachment, then one could
identify a baby as attached to a preferred figure in phase 2. However, it seems that the
infant remains unable to conceive of an attachment figure as someone with an
existence separate from his or her own existence (Marvin & Britner, 1999).
3. The phase of clear-cut attachment, phase 3. During this phase, the infant
is thought to consolidate attachment to its caregiver and it is during this phase that
most experts consider the infant to be “really” attached (Marvin & Britner, 1999).
This phase generally begins around the sixth month of life, although its emergence
may be delayed until after the first birthday in infants who have had little contact with
22
a primary caregiver (Bowlby, 1969, 1982). Phase 3 usually lasts until approximately
24 months (Bowlby, 1969, 1982).
During phase three, the infant’s increasing locomotors abilities enabling him
or her to show further differential behaviors, including approaching, following,
climbing on, exploring, and clinging to the mother preferentially (Ainsworth et al.,
1978), as well as allowing the infant some degree of control over proximity to his or
her attachment figure. Additionally, the infant begins using the mother as a secure
base from which to explore the surrounding environment and a haven of safety to
return to (Bowlby, 1969, 1982). Thus, a delicate balance between exploration and
proximity seeking behaviors remains characteristic of the infant throughout the third
stage.
Thus, the infant now has separate working models from his or her caregiver
consisting of organized cognitive images and plans of the self and other, based on his
or her new ability to operate internally on the images and likely behaviors that became
chain-linked during phase 2 (Marvin & Britner, 1999). Despite these advances, the
internal working models of the infant in phase 3 remain primitive. The infant is still
limited, at least during the early part of the phase, to think about the caregiver and self
in terms of behaviors; the infant does not yet comprehend that the attachment figure
has unique cognitions, perceptions, and goals (Marvin & Britner, 1999). Additionally,
early in the phase, the infant is unable to think about behaviors in terms of long
sequences (Marvin & Britner, 1999). However, with the development of the ability to
think about the caregiver’s likely behavior, the infant’s set-goal becomes partially
regulated by his or her expectations of the mother’s behavior and location. The
infant’s set-goal can be influenced by many factors including his or her physiological
state; the presence or absence of a disturbing event in the environment; assessment of
the caregiver’s attention to the infant; and whether the caregiver is present, departing,
absent, or returning from an absence (Bowlby, 1969, 1982). The infant’s set-goal may
also depend on the dyad’s history of the relatively stable patterns of attachment-
caregiving interactions established throughout this and earlier phases (Marvin &
Britner, 1999).
While increasing signs of attachment to the caregiver are hallmarks of Phase
3, infants during this stage are particularly likely to show wariness when faced with an

23
unfamiliar situation or person. Phase 3 infants are likely to stop exploration when
confronted with a stranger. The infant will remain wary or fearful for several
moments, then either remain stationary or move away from the stranger and toward
the attachment figure. However, they may later approach the stranger and interact
sociably if he or she does not seem threatening (Marvin & Britner, 1999).
4. The phase of a goal-corrected partnership, phase 4. This phase is thought
to begin around 24 months of life at earliest, however, it may emerge closer to 30
months for many children (Bowlby, 1969, 1982). Since the third phase of attachment
development, the infant has begun to be able to predict his/her mother’s movements
and adjust behaviors to her accordingly. During the fourth phase of attachment
development (the goal corrected partnership) is marked by a gradual development of
the infant’s ability to infer something about his or her caregiver’s set-goal and the
plans she/ he is forming to achieve (Bowlby, 1969). The infant is then able to attempt
to change the caregiver’s set-goal to something more closely related to his or her own
goal by utilizing techniques of request or persuasion, rather than merely adjusting his/
her set-goal to suit baby (Ainsworth et al., 1978). The ability to form a plan to change
the set-goal of other’s behavior requires a considerable degree of cognitive
competence such as the ability to see things from another’s point of view. Thus, the
child’s earliest attempts at such plans are often hampered by egocentrism and may
appear primitive or incompetent (Ainsworth et al., 1978). Over time, the child’s
attempts may be either facilitated or hampered by his or her caregivers’ behaviors,
depending on the extent to which they clarify or dissemble their own set goals, or
encourage or discourage the child’s awareness of them (Ainsworth et al., 1978). With
the child’s improving judgment, proximity is maintained by as much by the child as
by the mother (Ainsworth et al., 1978). Thus, the infant shows increasing control over
their own behavior and understanding of the caregiver’s behavior as they progress
through the four phases of attachment development, eventually developing the ability
to independently maintain proximity to the caregiver and act to influence the
caregiver’s set-goal.
In conclusion, the infants are continuing develop the attachment with the
mother or attachment figure since birth. At first, infant does not differentiate one
person from another, and hence responds to mother figure in the same way as infant

24
responds to other person. Infant will show the signals for serving to induce other
people to approach him/ her that for promoting proximity and contact. Then, infant
also becomes able to discriminate between one familiar figure and another at second
phase when 2 month age. During this phase, the infants will be active attachment
behavior with the emergence of coordinate reaching attachment. They can remember
mother or attachment figure at the third phase when second half of the first year. They
can organize relationship at this time. It also show the early birth is a basic period for
develop attachment for the infant in the next phase. Besides, its mention mother is a
significant person for closely relationship with infant.
According to infant have positive attachment from mother, they will develop
secure attachment infants. Attachment security as the infant used the mother as a
secure base for exploration, as expected. That is, when a mother was present, an infant
freely explored the environment, with occasional visual, verbal or physical contact.
When a mother departed, infant’s exploration was diminished. The infant might or
might not cry, but when a mother returned, the infant greeted her positively, and if the
infant was visibly upset, he/ she went to her, was soon comforted and returned to
exploring (Ainsworth et al., 1978). Attachment security shows a positive interaction
between infants as compared with others especially with their mothers. Positive
mother-infant interaction will promote attachment security between mother and the
infant. If infants had experience a satisfactory attachment relationship with their
caregiver, they will allowance for emotional regulation-the expression of feelings,
along with the underlying physiological patterning (Malekpour, 2007). In addition,
attachment security is an important prerequisite to secure attached preschoolers
(Goldberg, 2000) and they continue to be secure through childhood and adolescence,
eventually becoming autonomous adults (Goldberg, 2000). A person with attachment
security will have higher self-esteem, stable self-esteem, better self-perception
accuracy, greater self-clarity, and a better organized self-structure than an insecure
person (Wu, 2009). In addition, the results of attachment security include reducing
infant distress, enhancing emotional regulation, and beneficial long-term to social-
emotional and cognitive functioning (Page et al., 2010). Besides, the nature of the
attachment security influences the child’s trust in that person as an informant
(Corriveau et al., 2009). Therefore, infants who are secure attachment will have
25
physical survival, well-being, and healthy psychological development. Furthermore,
attachment security will provide increasing maternal competence, positively affecting
the infant, and decreasing maternal stress (Korja et al., 2008).
Mother-infant attachment process
Mother-infant attachment is a reciprocal way that occurs in both directions
between mother and infant. It was facilitated by positive feedback, either real or
perceived, from the infant. He/ she had a repertoire of responses called reciprocal
attachment. The infant receives warmth, feeding, and security from mother’s
behavior. The mother accepts the responsibility for the infant’s care and responds to
the child’s need. In return, she receives enjoyment and establishes her identity as a
mother. Both benefit from the formation of irreplaceable linkage continuing long after
the child ceases to be dependent (Murray & McKinney, 2010). Therefore,
mother-infant attachment process is a development of attachment between mother
with infant since post-partum and gradually develops throughout the time and last
long in people's life. This process integrates between bonding process and attachment
process that show in figure 2.
According to Klaus and Kennell (1982), attachment has a strong power for
the parent to enable them to do unusual sacrifices for caring their baby all day all
night. The time immediately after birth is the sensitive period, which is the first
minute, first hour and first day of life. Both the mother and baby have a unique and
active role in creating the reciprocal cues and responsiveness to each other. Therefore,
if health care provider would like to promote mother-infant attachment, it should
promote in the early state after birth that is in the post-partum period of mother
attachment and initial pre-attachment phase of infant attachment. Because of this
period is sensitive or important period for enhancing mother-infant attachment. Klaus
(2009) presented that the early period after birth is not a “critical” period but a
“sensitive” period for promoting bonding and attachment, respectively.
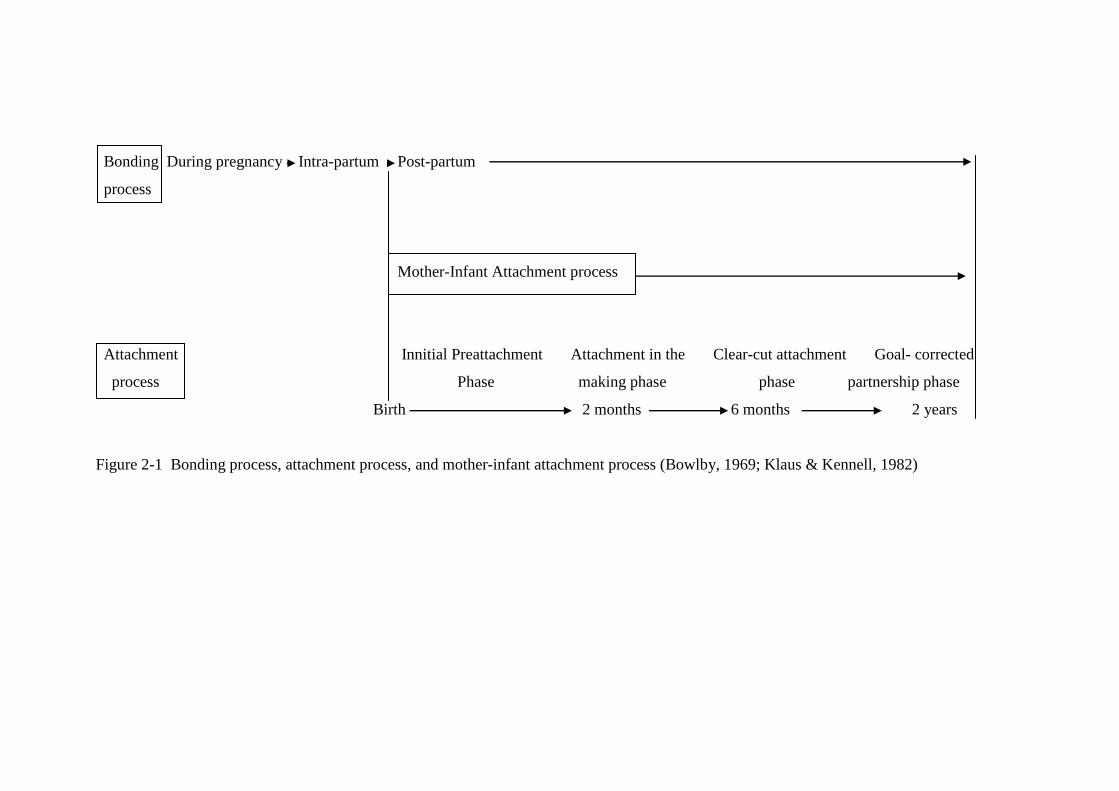
26
Bonding During pregnancy Intra-partum Post-partum
process
Mother-Infant Attachment process
Attachment Innitial Preattachment Attachment in the Clear-cut attachment Goal- corrected
process Phase making phase phase partnership phase
Birth 2 months 6 months 2 years
Figure 2-1 Bonding process, attachment process, and mother-infant attachment process (Bowlby, 1969; Klaus & Kennell, 1982)
27
Maternal-infant attachment can be assessed by observing the interaction
between the mother and the newborn and asking the mother’s perception of her infant.
Maternal interaction could stimulate the newborn, the newborn will response to the
mother. These interactions include touch, eye-to-eye contact, high pitch voice,
entrainment, odor, and skin to skin contact (Klaus & Kennell, 1982).
1. Touch, the most important behavior that serves to bind the mother and
her infant together is the mother’s interest in touching her baby.
2. Eye-to-eye contact, another interaction that mothers and their infant
demonstrate their love to the newborn originates in the eyes. Eye-to-eye contact
affects maternal-infant attachment. Klaus and Kennell (1982) found that several
mothers verbalized and showed their intense interest in waking up their newborns to
see their eyes opening. It makes mothers much closer to their infant with enface
position.
3. High pitch voice, DeCasper and Fifer (1980) have discovered that within
the first three days of life, newborns discriminate between speakers and demonstrate a
preference for the mother’s voice but not the father’s after only limited maternal
exposure. Because female voice higher pitch more than male voice. Besides, neonate
usually alerts, attends and responds to high-pitch voice.
4. Entrainment, human communication is not only sound, but also includes
movement of the body. When an individual speaks, some parts of body obviously
move or sometimes it is unnoticeable. Also the same as the listener, whose movement
get along with the speech. Although the newborn moves the rhythm of mother’s
voice. On the other hand, the newborn’s movements may reward the mother and
stimulate her to continue attach to her baby. Thus, these areas of contact are
interactive.
5. Odor, the olfactory sense helps an infant to identify the mother. An infant
recognizes his/ her mother from the breast milk odor. This affects maternal-infant
attachment.
6. Skin to skin contact, it begins ideally at birth and involves placing the
naked baby, then covered with a warm blanket, prone on the mother’s bare chest.
28
In summary, the maternal-infant attachment form prior to pregnancy to after
birth makes a mother and her newborn love each other. The consequences of the
presence of mother-infant attachment were make a newborn that have security
attachment, grow up with self-reliance, trust, cooperation, and helpfulness to the
others (Ainsworth et al., 1978; Goldberg, 2000). Infants who are cared for in a
relatively consistent and predictable way develop confidence in their ability to have
a positive influence on their environment and are more likely to express their need for
love and security (Goulet et al., 1998). Indeed, it seems that these children
demonstrate greater self-esteem, independence, and competence in relating to other
children (Haney & Durlak, 1998). Moreover, the consequences of mother-infant
attachment were mother grow through the interaction with her infant, which can be
inferred from exchange of positive emotions and mutually satisfying behavior. The
reinforcement of mother's skills in attachment for her infant will increase her self-
esteem and her sense of self-efficacy (Goulet et al., 1998). Strong attachments
between mother and her infant contribute to the prevention of negligence and abuse
(Belsky, 1993).
In contrast, if a mother can not develop attachment to her newborn, the baby
can develop an anxious and insecure attachment, over dependent, or immature (Korja
et al., 2010; Mangelsdorf et al., 1996). Insecurely attached infants were negative
feeling of attachment between infant with attachment figure (Ainsworth et al., 1978).
Ainsworth et al. (1978) classified the type of insecurely attached infant to 3 types that
include ambivalent attachment, avoidant attachment, and disorganization attachment.
If they have ambivalent attachment, they often do not learn or understand emotions of
their own or others. If they have avoidant attachment, they develop a sense that they
cannot impact their world, and thus, do not engage others. These infants are likely to
become delayed developmental, passive behavior, and may develop to full-blown
reactive attachment disorder. Likewise, if they have disorganization attachment, they
show no emotional response, and in facet, they are often described as being
emotionally absent (Ainsworth et al., 1978; Cassidy & shaver, 1999; Fish & Stifter,
1995; Goldberg, 2000; Woodhouse, 2010).
Maternal-infant attachment in preterm infant is poor reciprocity
(Bialoskurski, Cox, & Hayes, 1999) because this relationship was difficult for mothers
29
to progress in their physical and psychological connection with their preterm infants
because of the nature of preterm infant. Several studies found more insecurely
attached preterm infants compared to term born infants (Korja et al., 2010;
Mangelsdorf et al., 1996). In addition, preterm infant gestational age less than 32
weeks had disorganized attachment 32 % that more than full term infant had
disorganized attachment 17 % (Wolke et al., 2014). Therefore, preterm infant are
trend to be a insecure attachment infant.
The nature of preterm infant
Preterm infants, those born before 37 weeks of gestation, are at risk because
the preterm infants appear small and delay developed that are often found to have low
birth weight (Wong, Perry, Hockenberry, & Lowdermilk, 2006). The low birth weight
infant is classification by size to 4 levels of low birth weight infant that consist of low
birth weight [LBW], moderate low birth weight [MLBW], very low birth weight
[VLBW], and very very low birth weight [VVLBW] or extremely low birth weight
[ELBW]. LBW is an infant whose birth weight is less than 2,500 grams regardless of
gestational age. MLBW is an infant whose birth weight is 1,501 to 2,500 grams.
VLBW is an infant whose birth weight is 1,000 to 1,500 grams. ELBW is an infant
whose birth weight is less than 1,000 grams (Wong et al., 2006). Most of preterm
infant will be low birth weight.
The percentage of live births in Thailand that was weight 2,500 grams or less
at birth were 10.8, 11.4, and 11.31 in years 2008 to 2010 respectively (Ministry of
Public Health, 2011). Likewise, Nakhon Phanom hospital preterm infant with low
birth weight rate increase every year, 18.87 and 18.96 percent in 2009 and 2010,
respectively (Nakhon Phanom hospital, 2011). Despite technological and medical
advances, the proportion of preterm births has remained unchanged, whereas the
number of surviving infants has increased dramatically. Infant born at 23-26 weeks,
who usually weigh between 500 and 750 grams, have a 40 %-60 % chance of
survival. Infant born at 27-28 weeks (about 750-1000 grams), have approximately an
85 % chance of survival (Browne, 2003). The first few weeks and/ or months of life
can be a physically stressful experience for preterm infants. General immaturity of
preterm infants can lead to dysfunction in any organ or body system that affects a
30
wide range of problems including respiratory distress syndrome [RDS], patent ductus
arteriosus [PDA], apnea of prematurity, anemia, retinopathy of prematurity [ROP],
infection, poor thermoregulation, hyperbilirubinemia, and immature nervous systems
(Littleton & Engebretson, 2005; Wong et al., 2006). Those preterm infants and low
birth weight infants constitute the high-risk infant group to treat and care. When they
stayed in neonatal intensive care unit [NICU] or Nursery unit, they needed medical
equipment or on incubator that were separated from their mothers. They may exhibit
behavioral responding that reflect lack of energy, or behaviors that the mother may
view as abnormal, disinterest, or rejection (Korja et al., 2010).
Preterm infants had delay of growth and development. Preterm infants are
generally described as less alert and less responsive in interaction than full-term
infants (Korja et al., 2008). Accordingly, they were lower in self-regulation capacities
(Feldman, Weller, Sirota, & Eidleman, 2003; Korja et al., 2008; Korja et al., 2010).
Corrected age for evaluations growth and development of child should evaluated until
two years of age, in order to create real expectations for each child, without under
estimating premature children when comparing them with reference standards. When
assessing growth, this adjustment is necessary to reduce the variation that results from
the rapid growth during the third trimester of pregnancy and the deceleration
postpartum, there by making more accurate evaluations of growth rates and preterm
and those born at less than 28 weeks, it is recommended that corrected age be
employed until three years of age (Rugolo, 2005).
Preterm infants capable of less physiological, motor, and behavioral
organization and modulation because they had neurological immaturity and medical
complications (Als, 1982). Behavioral state of preterm infants was inconsistency by
their neurological immaturity. The ability to go from sleep to wakefulness, and to
maintain longer periods of sleep and wake are complex processes largely under
neurological control (Barnard & Kang, 1987). Therefore, it is important for mother to
learn states of alertness of the preterm infant at the time in order to appropriately
interact with them. When infants receive the positive interaction from mothers in the
appropriate state of behavior, they will console learning and responsive to mother that
will help preterm infant improving the emotional, social, and cognitive development.
31
It is the best to interact with the babies in quiet alert because infant in this state
provide much pleasure and positive feedback for caregivers (Barnard & Kang, 1987).
During this period the baby open eyes and does not move much. He/ She has eye
contact, listen to, and touch his/ her mother. Preterm infant are have 6 characteristics
of behavioral state (Barnard & Kang, 1987) that consist of sleep state and awake state
as follow:
Sleep states
State 1 Deep sleep (quiet sleep) with regular breathing, eyes closed, non
rapid eye movement (non-REM), no spontaneous activity except startles or jerky
movements at quite regular intervals; external stimuli produce startles with some
delay; suppression of startles is rapid, and state changes are less likely than from other
states. Infants will be unresponsive when mothers or caregivers arouse them.
State 2 Light sleep (active sleep) with eyes closed; rapid eye movements can
often be observed under closed lids; low activity level, with random movements and
startles or startle equivalents; movements are likely to be smoother and more
monitored than in State 1; responds to internal and external stimuli with startle
equivalents, often with a resulting change of state. Respirations are irregular, sucking
movements occur off and on. Eye opening may occur briefly at intervals. Light sleep
makes up the highest proportion of newborn sleep and usually precedes wakening.
Due to brief fussy or crying sounds made during this state, mothers who are not aware
that these sounds occur normally may think it is time for feeding and may try to feed
infants before they are ready to eat.
Awake state
State 3 Drowsy or semi-dozing; eyes may be open but dull and heavy-lidded,
or closed, eyelids fluttering; activity level variable, with interspersed, mild startles
from time to time; reactive to sensory stimuli, but response often delayed; state
change after stimulation frequently noted. Movements are usually smooth. From the
drowsy state, infants may return to sleep or awaken further, in order to awaken,
mothers can provide something for infants to see, hear, or suck, as this may arouse
them to a quiet alert state, a more responsive state. Infants left alone without stimuli
may return to sleep state.
32
State 4 Quiet alert; seems to focus invested attention on source of
stimulation, such as an object to be sucked, or a visual or auditory stimulus; impinging
stimuli may break through, but with some delay in response. Motor activity is at a
minimum. There is a kind of glazed look which can be easily broken through in this
state. Infants in this state provide much pleasure and positive feedback for caregivers.
Providing something for infant to see, hear, or suck will often maintain a quiet alert
state.
State 5 Active alert; considerable motor activity, with thrusting movements
of the extremities, and even a few spontaneous startles; reactive to external
stimulation with increase in startles or motor activity, but discrete reactions difficult to
distinguish because of general activity level. Brief fussy vocalizations occur in this
state. Mothers may intervene at this stage to console and to bring infants to a lower
state.
State 6: Crying; characterized by intense crying which is difficult to break
through with stimulation, motor activity is high, breathing more irregular. Crying is
the infant's communication signal. It is a response to unpleasant stimuli from the
environment or from within infants (fatigue, hunger, discomfort). Crying tells that
infants limits have been reached. Sometimes infants can console themselves and
return to lower states. At other times they need help.
It is the best to attachment relationship with the infants in quiet alert. During
this period the infant open eyes and does not move much. He/ She has eye contact,
listen to, and touch his/ her mother. However, most of preterm infants were fussy and
irritable (Talmi & Harmon, 2003). Preterm infants appear to have two problems of
state modulation. First, the immature infant has more total sleep and, in particular,
more day sleep. In addition, they were does not have the energy to wake up and look
at his/ her mothers even for brief periods misses the most basic attachment
opportunities (Barnard & Kang, 1987; Talmi & Harmon, 2003). Moreover, when
mother would like to interact with preterm infant, she should understanding the
preterm infant's cues that consist of engagement cures and disengagement cures.
1. Engagement cues are the appropriate cues for interaction. Preterm infant
will show signals as follow:
33
1.1 Eye becoming wide open and bright as the preterm infant focuses on
the mother.
1.2 Alert face or an animated face with wide open, bright eyes, often
accompanied by gently pursed lips as if the preterm infant were saying "ooh."
1.3 Grasping or holding onto the mother or objects in the environment.
1.4 Hand-to-mouth activity, often accompanied by rooting and sucking
movement. The preterm infant may also suck on his or her fingers.
1.5 Smiling.
1.6 Turning eyes, head, or body toward someone who is talking.
1.7 Smooth motor movements.
2. Disengagement cues are the inappropriate cues for interaction. Preterm
infant will show signals as follow:
2.1 Crying or fussing
2.2 Hiccoughing
2.3 Spitting up or gagging
2.4 Jittery or jerky movement
2.5 Frowning or grimacing
2.6 Becoming red or pale
2.7 Agitated or thrashing movements
2.8 Falling asleep
2.9 Averting the gaze (the infant moves her eyes or head away from the
mother)
Therefore, mother should observe the preterm infant's cues before taking the
interaction. Mother should interact when preterm infant show the engagement cues
that will suitable with infant behavior. This behavior represent that infant prepare for
learning and responsive with other.
However, most of preterm infant with very low birth weight separate with
mother for caring in incubator that can be influence to difficulty in interaction
between mother and preterm infant. Therefore, preterm with very low birth weight are
high risk for manifesting a higher rate of insecure-resistant relationships than the
nearly term infants (Mangelsdorf et al., 1996).
34
Maternal-preterm infant attachment
Premature birth may complicate the development and quality of this
attachment relationship, and possible differences between term and preterm infants
(Meijseen et al., 2010). Several studies found more insecurely attached preterm
infants compared to term born infants (Meijssen et al., 2010). In addition, preterm
infant gestational age less than 32 weeks had disorganized attachment 32 % that more
than full term infant had disorganized attachment 17 % (Wolke et al., 2014) that affect
from mother-preterm infant dyads have many problems which difficult to develop
attachment process between mother with preterm infant that consist of characteristic
of preterm infant, the stress of mother, and policy and environment in hospital.
Preterm infants are generally described as less alert and less responsive in
interaction than full-term infants (Korja et al., 2008). Accordingly, a preterm infant is
lower in self-regulation capacities, as well as the early separation, and decreased
parental touch and contact during postnatal care in the neonatal intensive care unit
(Feldman et al., 2003; Korja et al., 2008; Korja et al., 2010). Thus, natures of preterm
infants are barriers for maternal-preterm infant attachment.
Sitanon (2009) founded that mothers of preterm infant needed to be
addressed or supported to ameliorate improvements in care for their preterm infants,
in order to better support their ability to care for their preterm infants during the
infant’s hospitalization because mother had many stressors. Three main themes were
found for the need of mother. Firstly, they needed to be strong included parental
strengths and building strengths. Secondly, they needed to be there in order to get
closer to their infants. Thirdly, they needed to provide care for infants in order to
protect infants, increase involvements, and take over by the represented 3 stages of
parenting activities in NICU. However, the delivery of a preterm infant is an
unexpected and unprepared event for a mother. Thus, this event causes a mother to
experience uncertainty in the infant’s illness (Jongkae, Thaiyapirom, & Soontornchai,
2008). In addition, more than 50 % of the mothers was stressed out from physiological
stressors (inadequate sleep, worrying about infant’s illness) and extra-personal
situational stressors (exceeding expenditure of the income on taking the premature
infant to follow ups, and low family income) after preterm infant is discharged from
hospital to the home (Inwongwan et al., 2008). Most of the time parents felt stress,
35
uncertainty, anxiety, and fear of becoming too attached to the preterm infant or fear of
losing the baby. (Danerek & Dykes, 2008; Howland, 2007). Moreover, mothers of
preterm infants show lower coherence, less richness of perceptions, less openness to
change, lower intensity of involvement, and less acceptance (Borghini et al., 2006;
Korja et al., 2009). Mothers and fathers of preterm babies also have reduced
interaction with the babies compared to parents of babies born at full term (Danerek &
Dykes, 2008). Hence, those will affect maternal-infant attachment for their preterm
infants.
Likewise, Orapiriyakul et al. (2007) founded the process of maternal
attachment to preterm infants that was “struggling to get connected”. She explained
the mothers progressed in their physical and psychological connection with their
preterm infant with difficulty. The mothers followed to struggling develop their
interaction with the baby and interact with others in order to get connected to their
baby while hospitalized in the NICU. This process composed of 4 phases of
establishing the connections, disrupting of the connection, resuming to get connected
and becoming connected. The process of actions/ interactions of maternal attachment
to the preterm infants in each phase that sequentially were being close to the fetus,
withdrawal contacting, seeking closeness, mutual mother-baby interacting an
committing to mothering, depended upon having concern for the baby, adjusting
emotionally to the crisis, supporting connections, life experience and health care
system facilitating. The purpose of “struggling to get connected” was to resume the
affected maternal attachment to the baby that was disrupted at birth or delayed during
early hospitalization in the NICU to become a normal attachment as quickly as
possible. Preterm birth and hospitalization of the preterm infant in the NICU was
a crisis experience for mothers and their families. Mothers need to be supported in
their emotional stress and concern for the baby and be facilitated in developing
attachment to the preterm infant.
The hospital’s policy and environment may inhibit maternal-infant
attachment for preterm infants. Preterm infants have early separation since their birth
and decrease parental touch and contact during postnatal care in the nursery or NICU
(Feldman et al., 2003; Korja et al., 2008; Orapiriyakul et al., 2007). Besides, the
environment in the nursery or NICU has more overstimulation such as over light,
36
noise, and pain that will make preterm infants stressed and lonely in the incubator or
bassinette (Shah, 2010).
In summary, mother-preterm infant attachment has many problems that start
with the early separation between mother and preterm infant for caring in incubator at
NICU and nursery unit that lack of bonding and attachment on the sensitive period
after birth. Thus, mother-preterm infant attachment is not continuous of maternal
attachment process. Although, mother needs to be parental strength in order to get
closer to preterm infant, providing care and protecting preterm infant (Sitanon, 2009),
however, mother-preterm infant attachment was a struggling process (Orapiriyakul
et al., 2007) because three inhibiting factors inhibit attachment process. Firstly, it is
characteristic of preterm infant that had a less alert and responsiveness, inconsistency
of behavioral state (Korja et al., 2008). It is difficult for mother to understand, and
respond his/ her behavioral. Secondly, it is a mother factors. Mother of preterm infant
has many stress, lack of knowledge, difficult to understand preterm infant's cues and
need, and lack of skill to attach and respond to her preterm infant (Borghini et al.,
2006; Danerek & Dykes, 2008; Howland, 2007; Korja et al., 2009). Finally, it is a
policy and environment in hospital that inhibit attachment process from the early
separation in sensitive period of attachment, and the overstimulation in hospital
(Feldman et al., 2003; Shah, 2010). Therefore, mother will has less interaction with
preterm infant that will decrease attachment between mother and preterm infant.
As a result, the mother-preterm infant attachment has many of inhibiting
factors. The important inhibiting factors include maternal stress (Engler, 2005; Miles
et al., 1993; Shin et al., 2008), lack of understanding of preterm infant's cues (Miles,
Funk, & Carlson, 1993), less responsiveness of preterm infant (DiVitto & Goldberg,
1979), and early separation (Korja et al., 2009). Therefore, the nursing intervention to
promote mother-preterm infant attachment should try to minimize the barrier factors
that are especially barrier from maternal factor. Nurse professional should develop the
nursing intervention for helping mother to attachment with her preterm infant since
early period after birth. Besides, nurse professional should support her emotional for
decrease stress, give information about progression of preterm infant's illness, preterm
infant's cues, preterm infant's need, method of positive interaction with preterm infant
for increasing maternal perception of attachment and enhancing high confident to
37
response and interaction with her preterm infant. It will promote the behavior of
attachment between mothers with preterm infants. Moreover, the new intervention
should develop base on the factors that influence with the mother-preterm infant
attachment.
Factors related with mother-preterm infant attachment
There are several factors related with the mother-preterm infant attachment.
It has 2 directions of factors that consist of inhibiting factors and protective factors for
mother-preterm infant attachment. The details are as follows:
1. Inhibiting factors
1.1 Maternal stress
Lazarus's and Selye's definition stress is the inability to cope with a
perceived (real or imagined) threat to one's mental, physical, emotional, and spiritual
well-being, which results in a series of physiological responses and adaptation
(Seaward, 2011). Thus, maternal stress is an inability of mother to cope with a
perceive threat of preterm infant birth to her emotional and behavior of attachment.
Maternal stress of preterm infant birth as identify consist of stress from sights and
sounds in the NICU and nursery unit, the preterm infant’s appearance, and
relationship with the preterm infant and maternal role (Miles et al., 1993). Maternal
stress results not from a particular life event but from the individual's perception of
that event and of her ability to control and deal with the event (Mercer & Ferketich,
1994). Maternal stress is an important factor to inhibit attachment process. Mother
reported high levels of stress from preterm infant birth because she had high levels of
fear, lack of control and helplessness. Mother needed to receive emotional support
(Walker, 1992). If mother increase the stress, she can delay establishment of a durable
of bonding (Schenk et al., 2005). Therefore, if mother can not coping the stress, she
will difficult to promote attachment for her preterm infant. The representation of
attachment relationship between mother and preterm infant seems to have a special
impact from the adult’s capacity to coping with stress (Wilinger, Diendorfer-Radner,
Wilnauer, Jorgl, & Hager, 2005).
38
1.2 Preterm infant factor
Accordingly, a preterm infant is lower in self-regulation capacities
(Feldman et al., 2002; Korja et al., 2008; Korja et al., 2010). In addition, preterm
infants are generally described as less alert and less responsive in interaction than
full-term infants (Korja et al., 2008). It is difficult for mother to get and understanding
preterm infant behavior and preterm infant need. Mother may attach her preterm
infant which is not congruence with preterm infant need that will make a negative
attachment to her preterm infant.
1.3 Policy and environment in hospital
The hospital’s policy and environment may inhibit maternal-infant
attachment for preterm infants. Preterm infants have early separation since their birth
and decrease parental touch and contact during postnatal care in the nursery or NICU
(Feldman et al., 2003; Korja, et al., 2008; Orapiriyakul et al., 2007). The environment
in the nursery or NICU has more overstimulation such as over light, noise, and pain
that will make preterm infants stressed and lonely in the incubator or bassinette
(Chawaphanth, 2006; Shah, 2010). This is show the attachment process of preterm
infants is difficult to develop because their mother can not interaction with them in the
sensitive period, and they have a many stress from the environment in hospital that
make them less interaction with mother.
2. Protective factors
2.1 Maternal sensitivity
Maternal sensitivity is the quality of a mother’s sensitive behaviors that
are based on her abilities to perceive and interpret her infant’s cues and respond to
them (Ainsworth et al., 1978; Shin et al., 2008). A mother’s sensitive behavior must
be contingent on her infant’s prior behaviors and have the quality of a reciprocal
interaction with her infant. It is a dynamic process which accompanies the adaptation
and changeability (Shin et al., 2008). Maternal sensitivity as a factor influencing to
mother-infant attachment that lead to the development and safety of the infant
(Muller, 1996). Mothers read their infants’ cues and respond to them in a way that
influences the infants’ social development and increases their mutual pleasure
(Heinicke & Guthrie, 1992). Concept analysis of maternal sensitivity presented
mother-infant attachment was a consequence of maternal sensitivity (Shin et al.,
39
2008). Therefore, if mother has more maternal sensitivity, mother-preterm infant
attachment will increase.
2.2 Marital relationship.
Marital relationship is a mother relationship with father that make mother
feels loved, cared for and valued. Therefore, this feeling can be easily extended to the
person around her particularly her infant. Spouse can provide social support in all four
aspects that include emotional, information, appraisal, and instrumental support
(Tiden, 1985). If mother has high level of self-esteem and confidence, she can
concentrate on her mothering role and ready to provide unconditional love to her
newborn (Kluas & Kennell, 1982). Soakeaw (2007) examined the factors that
predicted maternal-newborn attachment, including marital relationship complication
during pregnancy, and separation time. One hundred and ten postpartum mothers who
gave birth through vagina at 36-48 hours postpartum participated in this study. This
result showed that marital relationship was significant predictor of the maternal-infant
attachment. It could predict 13.3 % of variance in maternal-infant attachment. This
could be explained that marital relationship might help the mother feel that they were
loved and cared for. Thus, they could extend their love and care to their infant. It was
congruent with Klaus and Kennell (1982). They stated the most important factor that
affects the maternal-infant attachment was marital relationship because spouse was
the best supporter.
2.3 Social support
Social support refers to the sources provided by other person that usually
used in reference to the support available to or perceived by parent, but a broader view
would encompass support for the young infant. In addition, the social support is
includes family support, friend support, and health care provider support. Most
broadly, social support may act directly to promote health regardless of person's level
of stress by protecting persons from the effects of stress (Walker, 1992). Besides,
social support could enhance mother-infant attachment (Walker, 1992). The social
supports for mother consist of family support, friend support, and health care provider
support.
As mention above, maternal-infant attachment in preterm infants had many
factors inhibiting that included characteristics of preterm infants, maternal stress,

40
policy and environment in hospital. However, new intervention can applies protective
factors to promote mother-preterm infant attachment that include involvement the
family such as father and/ or grandmother to support attachment between mother with
preterm infant, and give information to help mother understanding her preterm infant
that will excess maternal sensitivity to response the positive interaction with preterm
infant. In addition, new intervention should suggestion the method to enhance
attachment for her preterm infant that will help mother feeling high confidence to
attach her preterm infant in the early period after birth. As a result, it will help mother
decreasing maternal stress, increasing maternal attachment, and growing up mother-
preterm infant attachment.
Review of interventions with the mother-preterm infant attachment
There were multi-faceted interventions utilized to attachment focusing on
mother-infant interaction, video-feedback, providing information, multi-modalities
sensory stimulation, and developmental care that as follows:
1. Parent baby interaction program [PBIP] by Johnson et al. (2009) for
improved cognitive and motor development in preterm infants in England. This
program was implemented during preterm infant admission in NICU and up to six
weeks after discharge. It provided parental support during the neonatal period to
facilitate attachment, to enhance parent-infant interaction, to sensitize parents to their
baby’s cues, to facilitate parents’ confidence in indentifying and meeting their baby’s
needs, and to educate parents in developmental care principle. The result showed that
there was no significant effect of the PBIP on cognitive and motor development of
preterm infants at two years. Therefore, this program is not enough to promote
mother-preterm infant attachment. If preterm infants have best attachment from their
mother, they will be a secure attach baby, and they will have a good cognitive and
motor development.
2. Video-feedback Intervention to promote positive parenting [VIPP] by
Kalinauskiene et al. (2009) was used to promote maternal sensitivity and infant
attachment security in Netherlands. This program used only video-feedback about
mother-infant interaction for mother. The result founded that this program could
promote maternal sensitivity at 6 and 12 months but could not promote infant
41
attachment security.
3. Skin-to-skin contact [SSC] by Chiu and Anderson (2009) to promote
mother-preterm interaction in United State. This program was encouraged to begin
experiencing SSC as early, as often, and as long as possible each time. Mothers held
their infants between their breasts with either their hospital gown or their own clothes
and a blanket folded across the infant’s back for warmth. Infants wore a small diaper
and often, a cap. This result revealed that this program had no affect on mother-
preterm infant interaction at 6, 12, and 18 months. Therefore, the skin-to-skin contact
may could not promote mother-preterm infant attachment because it is not affect on
mother-preterm infant interaction.
4. Mother-infant transaction program [MITP] by Newnham et al. (2009)
was used to enhance outcomes of preterm infants and mothers including infant
temperament, infant regulation, mother-infant interaction, infant development, and
parental stress in Australia. This program included nine sessions that were teaching
mothers about recognizing infant’s disorganization/ stress cues, responding to infant’s
cues, principle during care and play, massage, kangaroo care in hospital, and home
visit at one and three months for mutual enjoyment through play. The result found that
MITP helped infants better to be able to self-regulation at three months and improved
communication skill for preterm infant at two years. Moreover, this program could
help mother reducing stress at three months but with no benefit in six months.
However, this program could not promote mother-infant interaction. Therefore, this
program can decrease maternal stress, yet, it is not enough to promote mother-preterm
infant attachment.
5. Infant behavioral assessment and intervention program [IBAIP] by
Meijssen et al. (2011) was used to promote maternal attachment representations in
Netherlands. This program was a post-discharge for preterm infant from birth to 6 to
8 months that helps to sensitized parents to their baby’s responses, in order to assist
parents to support their infant’s self-regulatory efforts, and to adjust the environment
to match the neurobehavioral needs of the infants. The result founded that this
program could not enhance maternal attachment representations. However, this result
found 50 % of the mothers had negative emotions in the first time seeing their babies
due to the fear of small infants. This first negative experiences of mother more often
42
had non-balanced attachment representations. Moreover, the first two weeks at home
found 37 % of mothers reported negative experiences that consisted of feelings of
fear, stress and worries, 28 % of mothers felt ambivalent both negative and positive.
Therefore, early support should address mothers’ feelings during the first contacts
with their baby as well as their first experiences with the baby at home that will
promote balance attachment representation which is secure attachment.
6. Developmental care included the nursing care to activate appropriate
stimulation and protected the overstimulation from the animate and non-animate
environment in the hospital. This intervention comforted preterm infants and reduced
stress that facilitated interaction with parents especially a mother. When a mother and
her infant interact in a positive way, attachment security will emerge. For example,
some research studies about effects of cycled lighting of heart rate, oxygenation, and
weight gain in preterm infant. The result revealed that gradual cycle lighting helped
preterm infants have less stress than in abrupt cycle light environment (Chawaphanth,
2006). If preterm infants have less of stress, they will have a capability to interact with
other that is benefit for promoting mother-preterm infant attachment.
7. Multi-modalities sensory stimulation program by Charoensri (2002) was
used to enhance growth of preterm infants and maternal attachment in Thailand. This
program was included auditory, tactile, vestibular, and visual sensory stimulation by
mother once a day until preterm infant was one month old. This program started with
auditory sensory stimulation that used planning tape music 10 minutes, then,
providing tactile stimulation by gentle strokes through the areas of neck, upper back,
both legs, both arms, and head. After that, vestibular and kinesthetic stimulation was
provides by slowly flexing and extending both legs and arms that followed with re-
tactile again. The last step was visual stimulation by holding for making eye contact
and talking. The result presented that this program could promote growth of preterm
infant and maternal attachment at one month old of preterm infant. Therefore, this
program is benefiting for maternal attachment that trend to enhance mother-preterm
infant attachment.
8. Maternal-infant interaction program by Trisayaluk (1999) for promoting
maternal attachment and growth of preterm infants in Thailand. This program was the
early interaction with sensory stimulation (touching, talking, eye-to-eye contact) and
43
encouragement maternal involvement for caring preterm infant. This program
manipulated three times per week since 24-48 hrs. after birth until two weeks. The
result founded that this program could enhanced maternal attachment at after finishing
program and two weeks after discharge from hospital. Therefore, this program is
benefiting for maternal attachment that trend to enhance mother-preterm infant
attachment.
All programs for promoting maternal-infant attachment benefit for self-
regulation of preterm infant at three months, reduced maternal stress at three months,
enhanced maternal attachment at after finishing program until 1 month old of preterm
infant, increased mother’s sensitivity at 6, 12 months, improved communication skill
of preterm infants at two years (Charoensri, 2002; Kalinauskiene et al., 2009;
Newnham et al., 2009; Trisayaluk, 1999). However, these programs could not directly
promote maternal-preterm infant attachment that may be these programs develop base
on theory for change only behavior of attachment but did not change the feeling of
stress and perception of attachment with attachment behavior together. In addition,
these interventions may lack of perspective from mother and family in that setting to
develop intervention.
The intervention based on the literature review that related to promote
mother-preterm infant attachment is consist of social support, marital relationship,
mother-preterm infant interaction, video-feedback, provide information, multi-
modalities sensory stimulation, and developmental care. In addition, it should select
the theory supporting that can change the cognitive, affective, and behavior. It will
help mother to have knowledge about preterm infant's cues and strategies to promote
attachment, positive emotions, and competency to take care of preterm infant to have
precise attachment. It congruence with the coaching model that is helps the coachee to
change the thought, feeling, and improving behavior (Kowalski & Casper, 2007).
The nursing coaching model
International coach federation defined coaching is partnering with clients in
a thought-provoking and creative process that inspires them to maximize their
personal and professional potential (Cook & Poole, 2011). The use of coaching as a
development process has increased significantly in recent years. Despite the obvious

44
use of the word “coach” in the 1500s as a method of carriage the term was reported to
have been adopted in England in the mid-1830s to refer to an individual who assisted
students in exam preparation (Zeus & Skiffington, 2005). From the late 1880s
coaching was used in the context of sports (Whitmore, 2002). Sport also had a strong
influence on the rise of coaching. In the late 1990s, it was a period for executive
coaching in the business (Performance Coaching International, 2012). Then in 2009,
the chartered institute of personnel and development [CIPD] suggestion that coaching
is becoming a standard management practice.
Nursing profession applies coaching model to develop intervention for many
dimension of nursing care that for improving health behavior (Palmer, Tubbs, &
Whybrow, 2003; Whittemore, Melkus, Sullivan, & Grey, 2004), development clinical
skills (Price, 2009), and health outcome in chronic condition (Vincent & Birkhead,
2013). Besides, the coaching model was significant to improve parent caring practice
skill such as enhancing caring practice skill among parent of children with pneumonia
(Apichaiyawat et al., 2010), and promoting caring practice skill among parent of
children with asthma (Suksawat, Lamchang, & Jintrawet, 2012). The process of
coaching model for change parent caring practice for children was consist of
1) assessment and analysis problem, 2) collaborate planning, 3) implementation
4) evaluation that had coach for supporting of emotion and information (Apichaiyawat
et al., 2010; Suksawat et al., 2012).
Kowalski and Casper (2007) created the nursing coaching model for
improving performance of nurses professional. A concerted effort had been made to
develop not only a coaching model but also the corresponding coaching competencies.
This model focused on change in thoughts, feelings and activities. It was in
congruence with Cook and Poole (2011) who presented many coaches focusing on the
essential concept that thoughts lead to feeling, feelings lead to actions, and actions
lead to results. This model was an explicit step for changing thoughts, feelings and
activities. The techniques of listening, questioning, clarifying and giving feedback
were essential. Therefore, this study has selected the coaching model of Kowalski and
Casper (2007) to apply for its developing structure of the new intervention. This
coaching model consisted of three major components that included “the foundation”
for the coaching process, “the learning process” which occurred during coaching, and
45
“taking action,” which encompassed changes in behavior.
Stage 1: The foundation
The foundation aspect of the coaching process was composed of four
following behaviors: 1) “Building relationships” between the coach and the coachee.
2) “Setting realistic expectations” for the process. 3) “Observing the coachee
behavior” and 4) “Self-reflection on the part of the coach.”
1. Building relationships
The coaching relationship had been described as a co-creative relationship.
The coachee specifically seek a partner to assist in visioning, planning, and achieving
accountability for improving performance. The coach served to clarify and transform
the agenda into action steps through listening intently, asking powerful questions, and
serving as a catalyst in moving the coachee toward taking action and achieving
desired solutions. Unique to the coaching relationship was mutual awareness of
inherent strengths of each other as well as the value of an objective person to reinforce
and assist the coachee in the process of learning and growing through inquiry,
understanding, and shifting identified nonproductive behaviors.
2. Setting realistic expectations
Coach had the primary responsibility that was to listen to the coaching
agenda, to empower the coachee to succeed, and to focus on the coachee’s needs.
The coachee was responsible for implementing the agenda, making a commitment to
achieve goals, providing feedback to the coach regarding what had worked well and
what had not, and participating actively in the coaching session. It was important to
establish relationship and maintaining it.
3. Observing behavior
As the coachee began to describe the agenda for each session, the coach was
provided with information about what the coachee was struggling with or the
coachee’s desired action plan and its development. Listening for missing pieces of a
story or asking for a description of a desired outcome by the coach would illustrate the
coachee’s alternative perspective into mobilizing action. At the same time, the coach
was able to reinforce behavioral strengths that had been described by the coachee.
Reframing events, coachee will identified strengths to leverage, and obstacles to
overcome. Providing multiple options for both changes in perspective and action steps
46
to address the initial agenda was the part of work of the coachee.
4. Use of self-reflection
Listening and reflecting by the coach back to the coachee using the exact
words, sound, feeling of the voice tonality, and energy patterns served to create
feedback and potential prompts for a change in the coachee’s awareness. At the same
time, the coach must also practice self-reflection and review the tonality and
observations made to the coachee. In this reflection, the coach could discover whether
there were other approaches that would be more helpful to the coachee.
In the coaching relationship, both the coach and coachee should understand
the inherent value of honest, confidential conversation as essential for personal growth
and development. Each session could end with a review of what was useful and what
was not for both the coach and the coachee.
Stage 2: The learning process
The learning process occurred during the time frame of this coaching
process, no matter how long the process lasted. It consisted of the art of being
“present,” the method of being purposeful and “positive,” the skill of “asking
questions,” the ability to “listening actively,” and the grace and style to “share
perceptions.”
1. The art of being present
In this session, it was critical to remove unnecessary distractions, such as
forwarding the phone or turning off any devices. It was important to make good eye
contact, face the coachee directly, be emotionally honest, and listen with intelligence
while internalizing and interpreting meaning with compassion and caring. These
attending behaviors were not only important to indicate “presence” but also potent to
build rapport and trust.
2. Being purposeful and positive
The coaching session was for discussions of what was and was not working
for the coachee related to the work environment. This was the reason for developing
an agenda into a format for this session. It was essential to focus on the positive
approaches that worked and brought the coachee success. The coach’s responsibility
was to give reinforcement, however, it was difficult to see the success, the progress, or
the changes. This was one of the reasons to end each session with success that had
47
occurred since the previous session.
3. Asking questions
The most important tool for the coach was the ability to ask powerful and
thought-provoking questions. The purpose of the questions was to discover what the
coachees were thinking both about themselves and others and how they perceived
difficult situation. It was helpful to use open-ended questions that genuinely
persuading sharing such as who, what, when, and where. Followings were an example
of a helpful framework using the vowels A, E, I, O, U.
A = Awareness of what had been noticed;
E = Experience of thoughts and feelings associated with whatever happened;
I = Intention in the situation including the purpose and goal;
O = Ownership of the coachee’s part in the outcome; and
U = Understanding of the situation and the outcomes by the coachee.
Eighty percent of the conversation should be a say of the coachee, while
20 % was the coach’s. This was an indicator of the importance of listening.
4. Active listening
Listening deeply demonstrated respect and built mutual trust through
empathy and sensitivity. To give a total focus on what another human being was
saying was the highest form of recognition and acknowledgement of that particular
person. Many people traveled through life, never felt heard or understood. So, the
coach’s ability to listen intently was a gift to the coachee. Listening deeply could be
known from the ability to reflect back to the coachee not only a summary of what was
said but also an interpretation of the intending meaning. The coachee would be
empowered by deep listening and the follow-up questions that resulted in additional
clarity and understanding.
5. Share perspectives
In this session, it was valuable for the coach to share his/ her observations
and experience with the coachee. The coach needed to be fair, objective, and factual
when sharing perspectives. Usually, it was more useful to use questions that led the
coachee through a process of discovery how to be more successful in approaching
difficult situations, in shifting his or her behaviors, and in working toward meaningful
professional relationships. One thing that should be shared here was what the impact
48
of the coachee’s behavior or activity might have had on the coach if he or she was the
recipient of the behavior or activity.
The coach could make valuable and enlightening connections between the
coachee’s actions and behaviors and their results or outcomes (what happened in the
given situation). Any behavior usually had both healthy and unhealthy (unintended)
consequences. These behaviors could be identified to the coachee. It was also
important to use “I” statements rather than “you” statements. In fact, each of us would
be amazed at the number of “you” statements made each day. Being conscious (and
self-reflective) of vocabulary and how it was used could help the coach be more
successful.
Stage 3: Taking action
This was a process where options were suggested and evaluated, the request
for changes in behavior occurred, the plan was clarified, the action plan follow-up
took place, and there was a clear evidence of support for the coachee in this process.
1. Suggest options
Discovering options could start with the coach asked the coachee for ideas
and suggestions he or she had for a given situation. Since empowerment could be
evolved from encouraging people to engage, to think critically, and to tap their
creativity. It was found that an effective strategy was to ask “what if” questions in an
effort to create options. In addition to asking questions, the coach could also share
his/her experience. Creating more helpful options, so it would provide the coachee
with more choices.
2. Request for behavior change
If options were not implemented or suggestions were not implemented, there
might be an additional issue. First attempt, the coach could review what the agreement
or commitment were to discover what prohibited the agreement from being enacted.
The coach might need to be quite direct in asking for a change in behavior. It was
quite acceptable to tell the truth directly. It was also helpful to ask how the coachee
wanted to handle the situation and offer them alternatives and/or consequences.
3. Clarify the plan and follow-up
It was important that the plan for behavioral change or improvement was
specific and measurable. It was unacceptable and a waste of the coach’s time for the
49
sessions to “drift” with no clear outcomes and objective unmet. The clearer the
specific actions were, the easier it was to evaluate them and to discover what worked
and what did not. To follow-up, the structure designed in the guildlines for the
constructive session allowed for written documentation of the various activities and
plans to make it simple to determine fulfillment.
4. Be supportive
Since this was a voluntary arrangement between the coach and the coachee,
so being supportive was crucial. The coach must be able to convey confidence that the
coachee would be successful according to the plan and the effort. It was helpful to
simply ask, “How can I support you?” “What do you need from me?” Whatever is
within the coach’s control and is reasonable should be implemented. It could be
valuable for the coach to connect with the coachee at these points by just to serve as a
“sounding board” to provide a positive affirmation and to be a “cheer leader.” It was
about being clear that the coachee could do whatever they had set out to accomplish.
Therefore, if new intervention wants new action to promote mother-preterm
infant attachment that will changing feeling, perception, and behavior of attachment.
Also, this study will select this coaching model, mother-infant attachment model, and
evidence based from previous study to develop the new intervention that focus on
decreasing maternal stress, increasing maternal attachment, and enhancing mother-
preterm infant attachment. The new intervention for mother-preterm infant attachment
develop base on theory of coaching model and mother-infant attachment model, and
research evidence that is EMPAC program.
The early mother-preterm infant attachment coaching (EMPAC)
program
This intervention was developed for solving the problem of attachment
among mothers with preterm infants. Most of the previous interventions were
developed based on theoretical support such as teaching about recognizing infant’s
disorganization/ stress cues, responding to infant’s cues, principle during care and
play, massaging, promoting kangaroo care in hospital, stimulating sensory stimulation,
and home visiting (Charoensri, 2002; Kalinauskiene et al., 2009; Lokham, 2004;
Newnham, Milgrom, & Skouteris, 2009; Trisayaluk, 1999). Those might not fit with
50
the context of some families in reality. Literature review showed the previous
interventions did not effectively reduce maternal stress, enhance maternal attachment
and mother-preterm infant attachment.
This proposed intervention is different from the previous interventions
because it integrates qualitative findings (need of mother, culture, belief, daily living
and competency of mother, and perspective of the expertise in this setting) with the
theory, and research evidences to develop the quality intervention that fits the
problems of mother-preterm infant attachment and the context of the family in
Thailand.
First of all, this intervention will be developed by integration of maternal-
infant attachment model of Klaus and Kennel (1982), coaching model of Kowalski
and Casper (2007), research evidences and qualitative findings (phase I). This
intervention is an EMPAC program (Appendix J). Therefore, EMPAC program is
suitable for problems of mother-preterm infant attachment, and the context of Thai
families that will add value and body of knowledge to the area of mother-preterm
infant attachment. Finally, there will be a pilot study to confirm its feasibility,
acceptability, and beneficial outcome.
Moreover, the EMPAC program is an early coaching intervention using
video-feedback that can stimulate mothers’ understanding, planning, implementing,
self-reflecting, and evaluating mother preterm infant attachment by themselves since
early post-partum period. It is hypothesized that it will change their emotion,
perception, and behavior of attachment with her preterm infants.
51
CHAPTER 3
RESEARCH METHODOLOGY
The purpose of this study was to develop a maternal-preterm attachment
intervention and examine the effectiveness of the intervention on maternal stress,
maternal attachment, and maternal-preterm infant attachment.
Research design
A mixed method (embedded experimental model) was employed to develop
an intervention of mother-preterm infant attachment and test its effect on maternal
stress, maternal attachment, and mother-preterm infant attachment. The study
developed the intervention based on theory, research evidence, clinical knowledge
from pediatrician and nurses, and perspective of mothers in the context of family in
Thailand by qualitative methods. Moreover, this study pilot tested the intervention
using qualitative and quantitative data to shape the intervention and to estimate the
outcome. After this, the effectiveness of the intervention was tested with a randomized
control trial that used quantitative methods. After intervention approaches, this
researcher wants to follow up with quantitative outcome and in-depth with
participants who received the treatment for understanding treatment experience of
participants. This process of design was congruence with a mixed method (embedded
experimental model) of Creswell and Plano Clark (2007, 2011) in figure 3-1. The
embedded experimental model that was embeds a qualitative component within a
quantitative design, as in the case of experimental design.
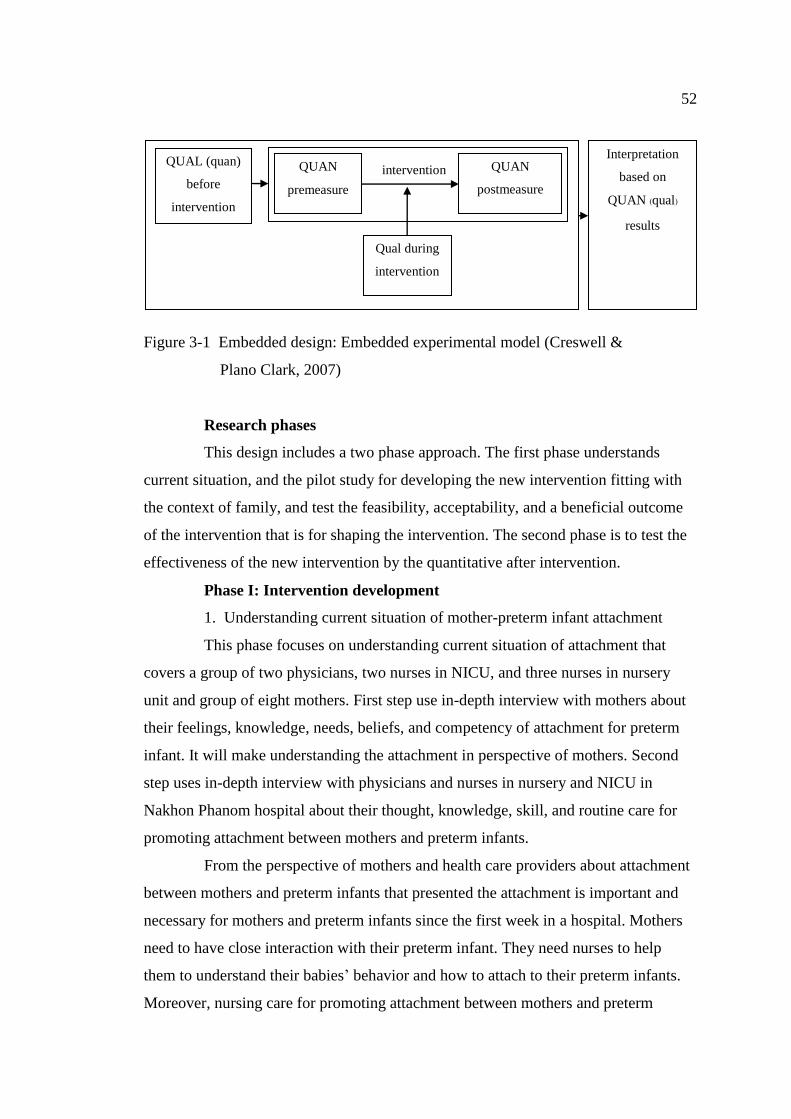
52
Figure 3-1 Embedded design: Embedded experimental model (Creswell &
Plano Clark, 2007)
Research phases
This design includes a two phase approach. The first phase understands
current situation, and the pilot study for developing the new intervention fitting with
the context of family, and test the feasibility, acceptability, and a beneficial outcome
of the intervention that is for shaping the intervention. The second phase is to test the
effectiveness of the new intervention by the quantitative after intervention.
Phase I: Intervention development
1. Understanding current situation of mother-preterm infant attachment
This phase focuses on understanding current situation of attachment that
covers a group of two physicians, two nurses in NICU, and three nurses in nursery
unit and group of eight mothers. First step use in-depth interview with mothers about
their feelings, knowledge, needs, beliefs, and competency of attachment for preterm
infant. It will make understanding the attachment in perspective of mothers. Second
step uses in-depth interview with physicians and nurses in nursery and NICU in
Nakhon Phanom hospital about their thought, knowledge, skill, and routine care for
promoting attachment between mothers and preterm infants.
From the perspective of mothers and health care providers about attachment
between mothers and preterm infants that presented the attachment is important and
necessary for mothers and preterm infants since the first week in a hospital. Mothers
need to have close interaction with their preterm infant. They need nurses to help
them to understand their babies’ behavior and how to attach to their preterm infants.
Moreover, nursing care for promoting attachment between mothers and preterm
QUAN
premeasure
QUAN
postmeasure
Qual during
intervention
premeasure
QUAL (quan)
before
intervention
intervention
Interpretation
based on
QUAN (qual)
results
53
infants need to develop the guideline for nurses that will make sure that mother-
preterm infants have a consistency and quality care for enhancing attachment.
As a result, mothers, preterm infants, nurses, pediatricians, and family were factors
that affect attachment between mothers and preterm infants which showed the
promoting and inhibiting points of attachment for preterm infant.
2. Formulating new intervention
Researcher developed the new intervention based on the integration of
scientific knowledge of theory and research evidence for creating EMPAC program.
Then, new intervention will be integrated the clinical knowledge from physicians and
nurses, and perspective of mothers (Whittemore & Grey, 2002) that is for improving
the EMPAC program fit with the reality of attachment in Thailand.
3. Pilot study
Qualitative and quantitative data were used for revising the EMPAC
program and confirmation about the feasibility, acceptability, and a beneficial
outcome (Thabane et al., 2010). This step started with the selecting 20 mother-preterm
infant dyads (Melnyk & Morrison-Beedy, 2012) who met inclusion criteria in nursery
unit at Nakhon Phanom hospital for enrolling and receiving the EMPAC program.
Then, the researcher conducted an in-depthinterview with participants reflecting the
program after finishing this intervention.
Phase II: Examining new intervention
Examining new intervention for testing the effectiveness of EMPAC
program on maternal stress, maternal attachment, and mother-preterm infant
attachment was applied two-group randomized control trial with long term repeated
measure follow-up (Christensen, 2007; Melnyk & Morrison-Beedy, 2012; Shadish,
Cook, & Campbell, 2002). This design applies for determining both of short and long
term effects of an intervention at discharge day, 1 and 2 months corrected age of
preterm infant, which is important in assessing sustainability of the intervention's
effects on outcomes over time (Melnyk & Morrison-Beedy, 2012).
54
Population and sample
Phase I: Intervention development
Target populations of this study are mothers of preterm infants in the post-
partum period when they visit their babies in the nursery unit and NICU at Nakhon
Phanom hospital. Eight mothers, two pediatricians and five staff nurses working at
NICU and nursery unit of Nakhon Phanom hospital were recruited for the study.
Criteria of samples selection were 1) mothers who have a preterm infant
with gestational age < 35 weeks and 1,000-2,000 grams birth weight and mothers’ age
of more than 20 years. 2) pediatricians and nurses must have at least 2 years
experiences in NICU and nursery unit.Criteria of sample size was determined based
on saturation of data. Eight mothers, two pediatricians, two staff nurses from NICU,
and three staff nurses from Nursery unit of Nakhon Phanom hospital were also
participationsin thisphase.
Phase II: Examining new intervention
Target populations are mother-preterm infant dyads at Nakhon Phanom
hospital when they visit their preterm infant at nursery unit. The number of
populations is 15 cases per month estimating from the previous years (178 cases in
2010, 185 cases in 2011, and 188 cases in 2012).
Inclusion criteria of mothers are: a) being mothers of preterm infant
(determined by diagnosis of pediatrician), b) being more than 20 years of age,
c) appreciating to enroll in this study and not involving alcohol or drugs (assessed by
interview), d) being able to speak, read, write, and understand Thai language.
Inclusion criteria of preterm infants include: a) having gestational age < 35 weeks
based on Ballard score, b) having between 1,000-2,000 grams birth weight, c) caring
in incubator, and d) absence of congenital anomalies such as congenital health
disease, central system disturbance that diagnosis by pediatrician. However, preterm
infants with evidence of severe or acute illness, such as cardiopulmonary arrest,
during the period of this study and the mothers who cannot care for their preterm
infants throughout the study will be excluded from this study because they can not
complete every process of this study, and they may were extraneous variables that
affect the outcomes.
55
The approximate sample size was determined based on the effect size from
the pilot study. The results of the pilot study were founded the effectiveness of
EMPAC program on maternal stress between before and after intervention presented
the effect size was 0.89, and the effectiveness of EMPAC program on maternal
attachment between before and after intervention presented the effect size was 1.12
(Appendix L). This study was selected the lowest effect size because this study testing
the new intervention that might not has the strong effect to the outcome. Therefore,
the effect size of this study was 0.89. A level of significance of .05 (probability of a
type I error) and a power of .80 (1-probability of type II error) were designated in this
study. The sample size were 72 subjects that calculated by using program of G power.
Then, attribution rate 15 % was included in this study because the long period of study
might have the drop out of participants. Therefore, total participants were 82 mother-
preterm infant dyads. The process of data collection found that 10 participants were
dropped out because preterm infants discharged before complete the intervention
(one case of experimental group and three cases of control group), and preterm infant
had a severe illness and referred to admit at NICU (four cases of the experimental
group and two cases of the control group).
Sampling method: the research assistants selected 82 mother-preterm infant
dyads who meet the inclusion criteria that were eligible to be invited in this study, of
which 41 were in the experimental group and participated in the EMPAC program
conducted by the researcher while the other 41 were in the control group and
participated in routine care.
When each qualified subject has been identified, the research assistants
informed the subject of the purpose, methods, and participation in the research for the
study. Voluntary participants were invited over for questions or concerns, then signing
the consent form. After that, the flipping coin method was performed to randomly
assign participants into experimental and control group. All participants with “Head”
side were assigned to experimental group whereas participants with “Tail” side were
assigned to the control group.
56
Setting of the study
The setting of conducting the research was the nursery unit where
participants stayed and follow-up at Nakhon Phanom hospital. This hospital is a
general hospital or secondary hospital in Thailand. It is a SAIYAIRUK hospital. This
nursery unit admitted the preterm infant who did not need the ventilator which waiting
to gain weight until 2,000 grams, neonate who has the problem such as infection,
hyperbilirubinemia, cleft lip & cleft palate and other. This unit has a room for mothers
to stay with newborn who is not caring in incubator. Nurses in nursery unit oriented
the mother about the rules in this unit, encouraging for breast feeding for her infant,
presentation the progress of illness, and the way to keep breast milk for her preterm
infant. In addition, nursery unit has the area for mother to sit behind the incubator of
preterm infant. These units are focused on breast feeding and physical health of
preterm infant. There have a breast milk nurse for suggesting to mothers about how
the success of breast feeding for preterm infant. Some of nurses encourage mothers to
touch and skin to skin contact with preterm infants. When preterm infant plan to
discharge, nurses provided information for mother about the way to observe the
severe clinical sign of preterm infant, infant rearing at home that use the handout of
fullterm infant, and the follow-up day for mother. However, professional nurses did
not teach mothers to understand preterm infant’s cue and behavior, and inconsistency
care to promote attachment between mothers with preterm infants.
Instrumentations
The instruments in this study consist of instruments for 2 phases. The first
phase includes 2 parts of instrument. These instruments compose of general
information questionnaire of mothers, pediatricians and nurses, and an interview guide
of participants' perception. The second phase is including 2 parts of instruments.
These instruments comprise of general information questionnaires of preterm infant
and mother, instrument for measuring outcomes of maternal stress, maternal
attachment and mother-preterm infant attachment.
Phase I: Intervention development
Instruments of intervention development phase consist of 2 parts of
instrument that follow:
57
1. General information questionnaires
1.1 Mother’s general information questionnaire. It contains a checklist of
demographic characteristics of the father, mother, and other attachment figure in
families. These include age, current marital status, education, occupation, monthly
income, intention to plan pregnancy, antenatal care, complications in pregnancy, type
of delivery, separation time, number of child, experience of preterm infant care, and
significant person.
1.2 Pediatrician's general information questionnaire. It contains a
checklist of demographic characteristics of the pediatrician. These include gender,
age, education, and time of experiencein NICU or Nursery unit.
1.3 Nurse's general information questionnaire. It contains a checklist of
demographic characteristics of the nurse. These include gender, age, education, and
time of experience in NICU or Nursery unit.
2. An interview guide of participants' perception
The interview guide was developed based on mother-infant attachment,
attachment theory, and review of literature regarding enhancing attachment for
preterm infant. It explored the mother’s feeling, knowledge, needs, beliefs, and
competency for attachment with preterm infant. For the nurses and pediatrician
explored their the thinking, knowledge, skills, and routine care for they provided to
promote attachment in NICU and nursery unit of hospital. They were semi-structured
interviews. The interview data will be collected for analysis of the current situation of
attachment. Each interview with the audio record taped about 30 minutes per case,
then complete writing of transcriptions immediately after the interviews.
Phase II: Examining new intervention
Instruments for examining the new intervention phase consist of 2 parts of
instrument. They are general information questionnaire, and instruments for
measuring outcome that follows:
1. General information questionnaires
1.1 Preterm infant’s general information questionnaire. It contains a
checklist of demographic characteristics of preterm infant. These are gestational age,
gender, birth weight, type of feeding, diagnosis and complication.

58
1.2 Mother’s general information questionnaire. It contains a checklist of
demographic characteristics of the father, mother, other attachment figures in families.
These include age, current marital status, education, occupation, monthly income,
intention to plan pregnancy, antenatal care, complication in pregnancy, type of
delivery, separation time, number of child, experience of preterm infant care, and
significant person.
2. Instrument for measuring outcome
2.1 Parent stress scale: NICU [PSS: NICU] (Miles et al., 1993) was used
to assess maternal stress in hospital. The questionnaire was a tool to evaluate the
stressors experienced by parents in NICU. It was originally adapted from the parental
stressor scale: pediatric ICU [PSS: PICU]. The instrument was altered to reflect
stressors in four major areas: a) those associated with the appearance and behavior of
a preterm infant, b) changes in the parental role that differ for parents of sick infants,
c) differences in the routines and environment of the NICU, and d) parental
relationships with staff on the unit. It consists of 34 items that includes three scales for
identifying parental role alterations (11 items), sights and sound of the unit (6 items),
and infant behavior and appearance (17 items). The scale of stressfulness is a rating
scale. Each rating is on a 5-point Likert type scale from 1 (not at all stressful) to 5
(extremely stressful). Total scores are obtained by summing responses to all 34 items;
higher scores represented more maternal stress in hospital. This instrument will
measure mothers’ stress when they visit their preterm infant the second time, and on
the discharge day of preterm infant.
The psychometric properties of the PSS: NICU were evaluated by Miles
et al. (1993) who determined internal consistency reliability, inter scale correlation,
and construction validity. One hundred ninety parents (115 mothers and 75 fathers)
from the Midwestern and Southeastern regions of the United States and from two
neonatal intensive care units located in Canada participated in the study. Parents were
contacted within the first week of their infant’s admission into the NICU. Internal
consistency reliability was determined for all three subscales and for the total
instrument using Cronbach’s alpha coefficient. For the entire scale they were .94 and
.89 for metrics 1 (stress occurrence level) and 2 (overall stress level). Inter-scale
correlations between metric 1 and metric 2 found that both of the metrics were highly
59
correlation (r = .88 to .96). To establish constructed validity of the test, a Pearson
correlation performed between each of the subscale scores for both of the metrics and
for the state anxiety scores [SAS]. It was observed that the strongest correlation
existed between the metrics and anxiety regarding the infants’ appearance (r = .44 and
.41 for metrics 1 and 2 respectively), parental role alteration (r = .44 and .40) and for
the total score (r = .45). In addition, Shah (2010) studied about parental stress in the
NICU in India. She tested the psychometrics on 190 parents (115 mothers and 75
fathers). The internal consistency reliability was determined for all three subscales and
for the total instrument using Cronbach's alpha coefficient. For metric 1, Cronbach’s
alpha coefficient was .92 for the infant appearance, .90 for parental role alteration, .80
for sight and sounds, and .94 for the total score. For metric 2, Cronbach’s alpha
coefficient was .83 for the infant’s appearance, .83 for parent role alterations, .73 for
sight and sounds and .89 for the total score. The internal consistencies for the entire
scale (.94 and .89, for metric 1 and metric 2, respectively) were found to be good. The
Cronbach alpha of PSS: NICU in this study was .96.
2.2 Parenting stress index-short form [PSI-SF] (Abidin, 1990, 1995) was
used to assess mother’s stress at home. It has three components that include parental
distress, difficult child characteristics, and dysfunctional parent-child interaction.
Parental distress includes items related to the mother’s lack of confidence in her role
as a parent, role restriction, depression, lack of social support and conflict with her
partner/ spouse. Difficult child characteristics includes items that reflected the
characteristics of a difficult child. Finally, dysfunctional parent-child interaction
includes items reflecting interactions with the child that are not reinforcing and the
child’s inability to meet parental expectations. The scale contains 36 items (12 items
in each subscale), each rate on a 5-point Likert type scale from 2 (strongly agree) to -2
(strongly disagree). Total scores are obtained by summing responses to all 36 items;
high scores represent more maternal stress at home. This instrument will measure
mother’s stress when the preterm infants are 1 and 2 months corrected age.
In Thailand, Wacharasin, Thienpichet, and Deoisres (2011) translated it in to Thai
language, and evaluated content validity by three experts. Then, they revised
according to suggestion from experts. After that, this instrument has been backward
translation to English language by two bilingual persons, and compared the meaning

60
with the original version for ensuring of equivalence meaning. They used the PSI-SF
to evaluated maternal stress of mothers having children aged 0-3 years in Thailand
that had alpha coefficient .85 (Wacharasin et al., 2011). The Cronbach alpha of PSI-
SF in this study was 98.
2.3 Maternal attachment inventory [MAI] (Muller, 1994) was used to
assess maternal attachment. The questionnaire contents assessed maternal affectionate
attachment to the infant at 1 months corrected age of preterm infant. This 26-item
scale asks mothers to indicate how they generally feel in relation to thoughts (e.g. ‘My
thoughts are full of my baby’), feelings (e.g. ‘I feel love for my baby’) and situations
(e.g. ‘I watch my baby sleep’) new mothers may experience. Responses are scored on
a 4-point scale ranging from 1 (almost never) to 4 (almost always). Summing
responses to items creates a total score ranging from 26 to 104. Higher scores
represent more maternal attachment.
Muller (1994) reported the MAI as having an adequate level of reliability
from 207 mothers, with coefficient alpha .85 and .76 for 1 and 4 months after the birth
of the infant respectively. In Thailand, Jongpranee (1997) translated it in to Thai
language, and it was tested for content validity by five experts. After receiving
recommendations from those experts, the instrument was modified according to the
experts’ suggestions to improve the clarity of the questions that was to provide a more
appropriate order to the questions, and to ensure appropriate language. She evaluated
the reliability of the Thai version with 20 adolescent mothers and found that the alpha
coefficient was .92, and which was also .92 in a confirmatory research study with 100
adolescent mothers. In addition, Charoensir (2002) administered the MAI to 40
mothers of preterm infant. Its Cronbach’s alpha coefficient was .87. The Cronbach
alpha in this study was .80.
2.4 Mother-infant attachment tool (MIAT) was used to observationally
assess mother-preterm infant attachment. It is adapted from the mother-infant
screening tool [MIST] of Reiser (1981), and literature review. The MIST was
measured four aspects of mother-infant attachment that include tactile (holding and
touching), visual (eye to eye contact and facial expression), auditory (language), and
feeding (during, and after feeding). It focuses equally on the mother’s behavior and
infant’s reaction when mother is feeding her infant. There is a four rating scale of
61
behavior that is labeled A-B-C-D. The very attentive mother and responsive infant
would be under A (score 3), and at the other extreme, the non-attentive mother and
unresponsive infant would be under D (score 0). Summing responses to items creates
a total score ranging from 0 to 48. Higher scores represent higher mother-infant
attachment.
Sunsaneeyanon (1965) applied the MIST (Reiser, 1981) for measuring
mother-infant attachment for assessing attachment between mother and preterm infant
at 2 months of preterm infant age in Thailand. She translated MIST to Thai language
by two bilingual persons, and it was tested for content validity by three experts. Then,
she revised MIST following the suggestion of experts in order to ensure that all of
questions were precise and appropriate questions. She evaluated the reliability with 20
mother-preterm infant dyads that found the alpha coefficient was .91.
However, when using this instrument with the preterm infant, it is difficult to
classify the preterm infant’s reaction to each label. Moreover, some of items were not
appropriate with the development of preterm infant. Therefore, this instrument was
changed to a three rating scale of behavior that is label A-B-C. The very attentive
mother and responsive infant would be under A (score 3), and at the other extreme,
the non-attentive mother and unresponsive infant would be under C (score 1).
Summed total scores was rank from 16 to 48. A high score represents high mother-
preterm infant attachment. The inter-rater reliability of MIAT in this study was .90.
The instrument of MIAT is an observation instrument. Researcher trained
research assistants B for using the MIAT. Researcher described the meaning of each
item and gave the manual for administration of this instrument for research assistant
B. Then, researcher and research assistant B saw the video records about the
attachment behavior between preterm infants and their mothers in the feeding time,
and testing the inter-rater between researcher and research assistant B that was
performed until giving the score .90 that for protecting interpretation bias.
Validity and reliability
Validity
The content validity for all instruments was approved by five experts that
consist of one pediatrician, two pediatric nursing instructors, and two pediatric nurses.
Each item of the instruments was assessed for relevancy and accuracy on a score of 1
62
(not relevant), 2 (somewhat relevant), 3 (quite relevant), and 4 (very relevant). The
content validity index [CVI] of this study was 0.92.
Reliability
Reliability of this study has 2 types of reliability base on the kind of
instrument that include reliability for all questionnaires, and reliability for observation
instrument. The questionnaires of this study consist of parent stress scale [PSS:
NICU], parent stress index-short form [PSI-SF], and maternal attachment inventory
[MAI]. The reliability of all questionnaires were trialed with 30 mothers of preterm
infant. The Cronbach’s alpha of PSS: NICU, PSI-SF, and MAI were .96, .98, and .80
respectively.
The observation instrument of this study is mother-infant attachment tool
[MIAT]. This study tested inter-rater reliability [IRR] between 4 research assistants
for 10 participants for confirmation of the agreement or consistency among scores
from all research assistants. The intraclass correlation coefficient for testing inter-rater
reliability of MIAT was .90.
Description of intervention
The EMPAC program was revised from the perspective of mothers, nurses,
and pediatricians. Then, pilot study was applied for testing the possibility and
acceptability of the intervention for modification.
The EMPAC program conducted for experimental group over 10 days.
The EMPAC program offered three sessions. The first session started the second time
for the mother visiting preterm infants. The second session was conducted in day 5
after the first session. The third session was conducted in day 10 after the first session.
The EMPAC program consists of five stages that presented in table 3-1 as follow:
Stage 1 Creating trusting relationship
Creating trusting relationship has two components that consist of building
relationship and non-hierarchal relationship. In this stage, building the relationship
between coach (researcher) with coachee (mother) was started with introducing each
other and informing the objective of the discussion and period of meeting. It is
important that the coach makes eye contact, faces the coachee directly and expresses
emotions honestly. The coach invited the coachee to tell her feelings, beliefs and
needs related to the care for her preterm infant. The coach show respect, fully present,
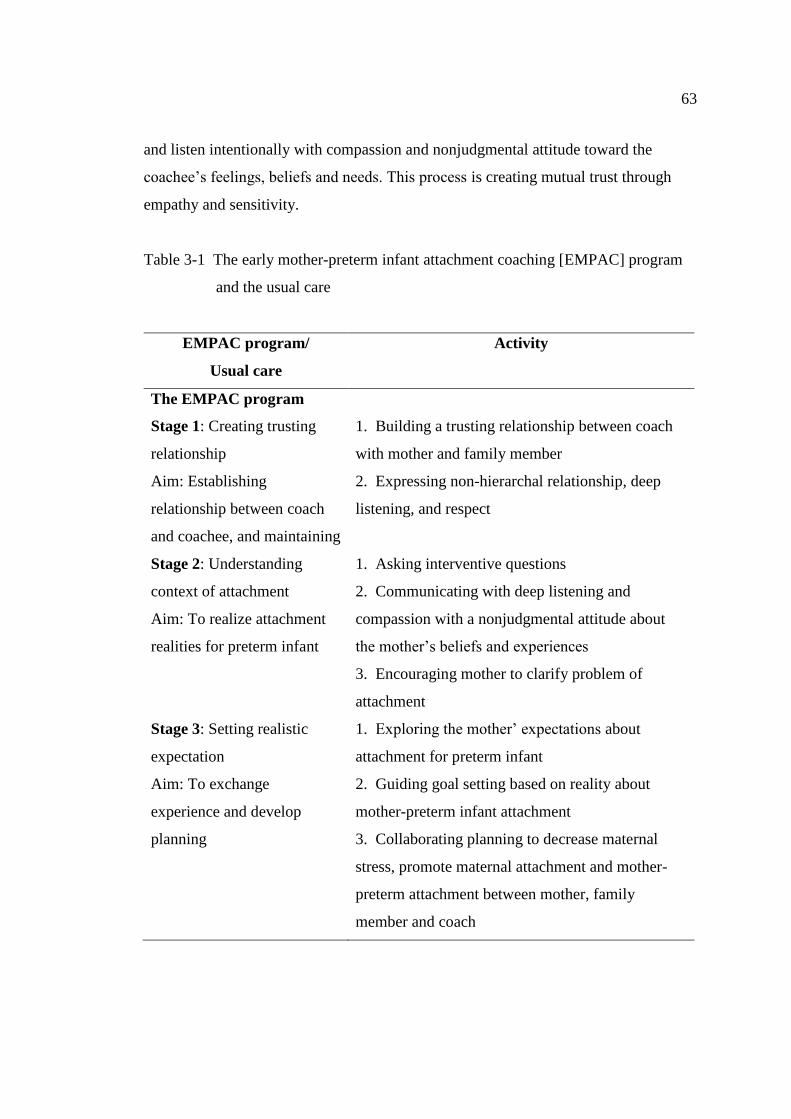
63
and listen intentionally with compassion and nonjudgmental attitude toward the
coachee’s feelings, beliefs and needs. This process is creating mutual trust through
empathy and sensitivity.
Table 3-1 The early mother-preterm infant attachment coaching [EMPAC] program
and the usual care
EMPAC program/
Usual care
Activity
The EMPAC program
Stage 1: Creating trusting
relationship
Aim: Establishing
relationship between coach
and coachee, and maintaining
1. Building a trusting relationship between coach
with mother and family member
2. Expressing non-hierarchal relationship, deep
listening, and respect
Stage 2: Understanding
context of attachment
Aim: To realize attachment
realities for preterm infant
1. Asking interventive questions
2. Communicating with deep listening and
compassion with a nonjudgmental attitude about
the mother’s beliefs and experiences
3. Encouraging mother to clarify problem of
attachment
Stage 3: Setting realistic
expectation
Aim: To exchange
experience and develop
planning
1. Exploring the mother’ expectations about
attachment for preterm infant
2. Guiding goal setting based on reality about
mother-preterm infant attachment
3. Collaborating planning to decrease maternal
stress, promote maternal attachment and mother-
preterm attachment between mother, family
member and coach
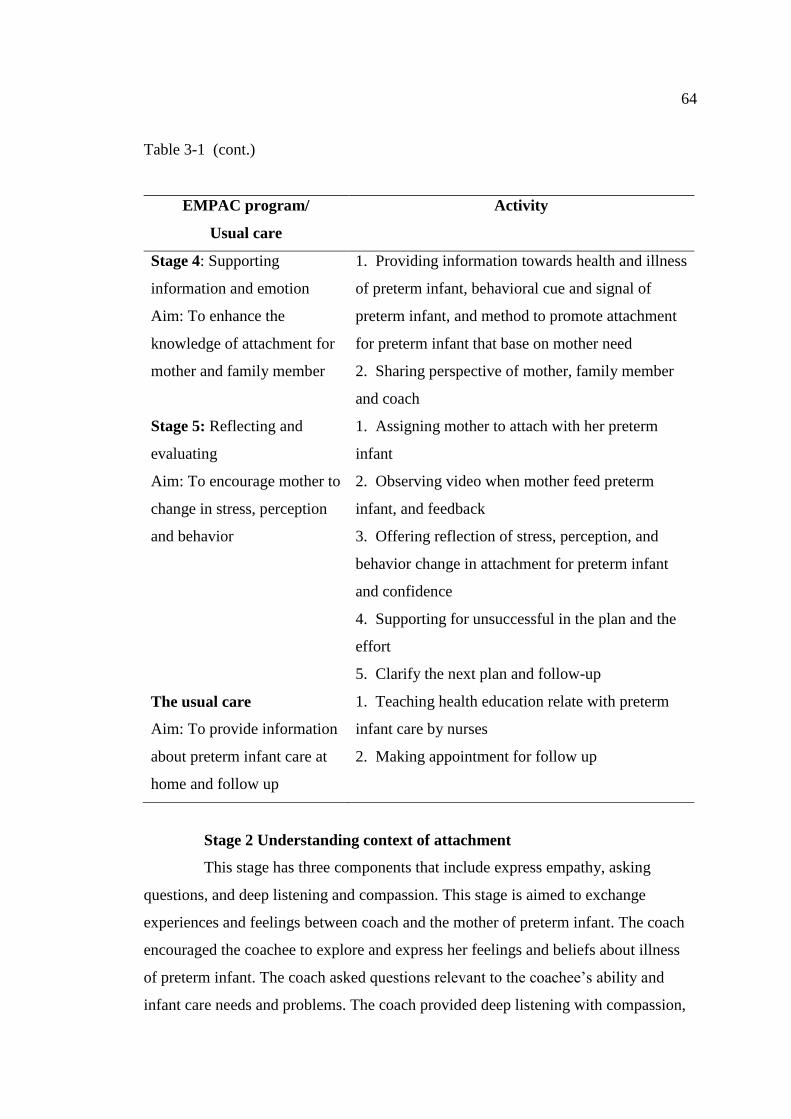
64
Table 3-1 (cont.)
EMPAC program/
Usual care
Activity
Stage 4: Supporting
information and emotion
Aim: To enhance the
knowledge of attachment for
mother and family member
1. Providing information towards health and illness
of preterm infant, behavioral cue and signal of
preterm infant, and method to promote attachment
for preterm infant that base on mother need
2. Sharing perspective of mother, family member
and coach
Stage 5: Reflecting and
evaluating
Aim: To encourage mother to
change in stress, perception
and behavior
1. Assigning mother to attach with her preterm
infant
2. Observing video when mother feed preterm
infant, and feedback
3. Offering reflection of stress, perception, and
behavior change in attachment for preterm infant
and confidence
4. Supporting for unsuccessful in the plan and the
effort
5. Clarify the next plan and follow-up
The usual care
Aim: To provide information
about preterm infant care at
home and follow up
1. Teaching health education relate with preterm
infant care by nurses
2. Making appointment for follow up
Stage 2 Understanding context of attachment
This stage has three components that include express empathy, asking
questions, and deep listening and compassion. This stage is aimed to exchange
experiences and feelings between coach and the mother of preterm infant. The coach
encouraged the coachee to explore and express her feelings and beliefs about illness
of preterm infant. The coach asked questions relevant to the coachee’s ability and
infant care needs and problems. The coach provided deep listening with compassion,
65
and respecting belief and ability of mother. The coach clarified the problems of
attachment to preterm infant and transform the agenda in to an action step through
listening intently, asking powerful questions, and serving as catalyst in moving
mother toward to taking attachment and achieving desired solution. The coach had
a facilitator role of providing important updated information and research findings
related to preterm infant attachment behaviors. Importantly, the coach praise or
commend the coachee for any positive issues.
Stage 3 Setting realistic expectations
This stage has three components that comprise being purposeful and
positive, collaborating planning, family and social support. This stage is a guide for
goal setting based on reality about mother-preterm infant attachment. The coach
encouraged coachee to make a commitment to achieving goal for promoting
attachment for her preterm infant. Coach was empowered mother toward solution of
attachment in preterm infant, and to focus on what the mother wants. The mother was
response for bringing the planning. The coach encouraged family such as father or
grandmother involvement to help mother to develop an action plan for enhancing
attachment for her preterm infant. A mother with father or grandmother provided
feedback to the coach regarding what was work well and what was not, and
participating actively to set the agenda of mother-preterm infant attachment.
Stage 4 Supporting information and emotion
This stage has three components that encompass providing information base
on mother’s need, guidance strategies to achieve goals, and sharing perspectives.
This stage was provided updated information and research evidences about strategies
to promote attachment for preterm infant depending on the needs of mothers, assisted
mother to develop appropriate strategies to achieve the goals, and shared perspectives
about interaction between mothers and preterm infants. This stage was coached
mother to learn about preterm infant’s cues and behavioral states from her own infant,
and sharing perspectives to enhance attachment.
Stage 5 Reflecting and evaluating
This stage has three components that cover requesting cognitive, affective
and behavior changing, assignment mother to attach with her preterm infant, and
clarify the plan and follow-up. This stage was encouraged mother for reflection about
66
sessions and evaluation about the change related to affective, cognitive, and behavior
of her attachment for preterm infant. This stage was requested mothers to clarify
behavior changes, the plan, and follow-up. The coach became a partner behind
coachee when she interacts with her preterm infant. The coach must provide mental
support for uplifting the mothers or make sure that the mother will be successful in the
plan and the effort. It could be valuable for the coach to connect with the mother at
critical points to provide commendation and positive affirmation when mother can
progress in attachment for her preterm infant. It is about being clear that the coachee
can do whatever they have set out to accomplishfor attachment with her preterm
infant.The coach in this stage observed, gave positive reinforcement and feedback
about the attachment from mother to her preterm infant. In addition, coach encouraged
coachee to interact with her preterm infant and feedback herself about her feelings,
perceptions, and behavior changings to attach her preterm infant.
Moreover, this study had the chart desktop of mother-preterm infant
attachment that developed from research evidences and literature review. It had a
concept of CARE attachment (correct attachment, appropriate attachment, right time
attachment, and early attachment) that is important content to promote the process of
relationship creation between the mother and the infant during postpartum period. It
was given to mother at the first session and used it every session depending on the
need of mother. The chart desktop is covers topics to help mother to establish
attachment with preterm infant, namely: knowledge of preterm infant's cues, preterm
infant's needs, behavioral state, and sensory stimulations (touching, talking, massage,
eye-to-eye contact, and holding).
Control threat of internal and external validity
1. Threat of maturation may occur because preterm infants are improving
the development and attachment overtime. In addition, maternal sensitivity is
increased overtime when mothers contact with their children. It is difficult to evaluate
the impact of the intervention in the one group design. The threat of maturation can be
prevented by inclusion of a control group, where maturation is similar between the
intervention group and the control group.
2. Threat of mortality may occur because the period of the data collection is
around 2 months corrected age of preterm infant which was considered a very long
67
time. Therefore, there is high possibility for the dropouts from the research. Thus,
good relationship with participants should take place from the beginning before data
collecting. The researcher should come up with strategies such as gift giving to
reinforce and motivate mothers to participate until the end of the research for both
groups.
3. Threat of data contamination may occur because participants of the
control and experimental groups are admitting to the same setting. They can see and
may communicate about the intervention each received from the researcher.
Moreover, nurses in this setting may observe the intervention and applied some of
intervention to the control group. This will affect the outcome of the study. The threat
of data contamination can be prevented by separating the implementation area in the
private room for the experimental group.
4. Threat of resentful demoralization may occur because the control group
may felt that they did not have the similar nursing care same the experimental group.
The threat of demoralization can prevented by providing the information before
random assignment to experimental and control group. The control group will be
perceived as valuable of routine care that is a standard care, while the experimental
group adds some of program that did not know the beneficial outcome. It made all of
participant from both group felt equally of nursing care. Therefore, participants of this
study did not decline in their participation.
Protection of human rights
Prior to conducting the study, the study proposal and the research
instruments are reviewed and approved by the research ethic committee of Faculty of
Nursing, Burapha University for protection of human subjects. In addition, permission
for data collection was obtained from the administrator of the Nakhon Phanom
hospital.
The researcher informed mothers of preterm infants, nurses, and physicians
about the research purposes, process, and benefits of this study. If they were willing to
participate in the study, they signed consent forms. The researcher also provided
contact address and telephone number to all subjects so they can directly contact the
researcher if they needed further information about the study. Participants who are
68
mothers of preterm infants, pediatricians and nurses have the right to refuse to
participate or withdraw from this study at any time. And, if mothers do so, the care
and treatment was not affected. Confidentiality of the participants were assured that
personal information was kept strictly confidential and reported only as group data.
Moreover, all data was stored in a secure place and utilized only for the purpose of
research.
Data collection
The data collection of this study was presented in the two phases that
congruence with the research design as follows:
Phase I Qualitative data was collected by the researcher in order to gain an
understanding of the situation with the key informants that follow:
1. First week of data collection, in-depth interview was performed to collect
data from two physicians and five nurses in nursery unit concerning the strategies for
promoting mother-preterm infant attachment that uses in-depth interview guide.
2. First month of data collection, in-depth interview was used to collect data
from eight mothers about feelings, knowledge, needs, beliefs, and competency of
attachment for preterm infant that is using an interview guide. The researcher had
conducted face-to-face, audiotape, and semi-structured interviews. Each participant’s
interview lasted between 20-25 minutes. The face-to-face interviews are usually
conducted to offer the researcher the opportunity to interpret the non-verbal cues
through the observation of body language such as facial expression and eye contact,
whereby it enhanced the interviewers’ understanding of what was being said. To this
end, it permits the researcher to probe and explore the meanings and understanding
(Ryan, Coughlan, & Cronin, 2009). The questions were generated based on the
purpose of this phase. In addition, field notes were used to supplement other forms of
data collection that were written after in-depth interview in the ward. Researcher spent
five to six hours on the ward each day to be familiar with the nurses in order to
perform subsequent observations of attachment behavior of mothers. Moreover,
documentary data sources consist of nurses’ notes and other records used to support
data.

69
3. Synthesize new intervention to promote attachment for preterm infant
based on data from EMPAC program, mothers' perspective, and nurses’ and
physicians’ experiences. As a result, the EMPAC program had involved family
members in every process of intervention because mothers had a high confidence to
attach their preterm infants when family members join in caring of preterm infants.
Moreover, intervener gave the chart desktop of mother-preterm infant attachment for
mother at the first time when starting the intervention.
4. Pilot study before examining the new intervention to confirm feasibility,
acceptability, and a beneficial outcome. This step used qualitative and quantitative
data for shaping the intervention and confirmation about the feasibility and
acceptability (Thabane et al., 2010). This step starts with the selecting 20 mother-
preterm infant dyads (Melnyk & Morrison-Beedy, 2012) in nursery at Nakhon
Phanom hospital for enrolling to receive the EMPAC program. Then, researcher uses
in-depth interview with participants about the opinion of feasibility and acceptability
for this program after finishing this intervention. In addition, researcher tested the
effectiveness of EMPAC program on maternal stress and maternal attachment at
discharge day compare with pre-intervention. Last step, researcher revised the
EMPAC program.
The results of pilot study showed that the admission period of preterm
infants in nursery unit was 7-33 days. Most of the preterm infants were admitted in
nursery unit less than 18 days. Therefore, the time period of EMPAC program should
be completed before two weeks. Every participant accepted and was satisfied with the
EMPAC program; however, problems of program implementation were reported that
participants rejected the flip chart for recording the maternal attachment (diary record
for mother that record about the attachment behavior of mother) because they could
not managed the time to do it. In addition, the effectiveness of EMPAC program on
maternal stress between before and after intervention presented the effect size was
0.89, and the effectiveness of EMPAC program on maternal attachment between
before and after intervention presented the effect size was 1.12 (Appendix L).
Finally, the EMPAC program had revised the program to three sessions
based on the admission period time of preterm infants in nursery unit at Nakhon
Phanom hospital, and the suggestion of participants. The first session started in the
70
second time of mother visiting preterm infants of mothers. The second session was
conducted in day 5 after the first session. The third session was conducted in day 10
after the first session. In addition, the program cut-out the flip chart of maternal
attachment in this study because it was not appropriate for participants. Moreover,
intervener gave the chart desktop of mother-preterm infant attachment at the first time
when starting the intervention. Future more, the program involved family members in
every process of intervention because mothers had a high confidence to attach their
preterm infants when family members joined in caring for preterm infants.
Phase II Experimental phase collected data by research assistants. It
prevented bias in this study. Besides, research assistants B who collected the data
were also blind for group assignment. Therefore, this study has a single blind. The
procedures of data collection are preparation stage and experimental stage as follows:
Preparation stage:
1. The researcher explained the purpose of the research to the director of
Nakhon Phanom hospital, and the head of nursery unit in Nakhon Phanom hospital
before starting to collect data. It is beneficial for getting permission for data
collection.
2. The researcher prepared the room and materials for mothers and preterm
infants such as video, chart desktop of mother-preterm infant attachment.
3. Researcher trained research assistants B for using the instrument of PSI:
NICU, PSI, MAI, and MIAT. The questionnaires of PSI: NICU, PSI, MAI described
a meaning of each item, and the time for assessment. In addition, the instrument of
MIAT is an observation instrument. Research described the meaning of each item and
gave the manual for administration for this instrument for research assistant B. Then,
researcher and research assistant B saw the video records about the attachment
behavior between preterm infants and their mothers in the feeding time, and testing
the inter-rater between researcher and research assistant B that was performed until
giving the score .90.
4. The research assistant A selected the sample group following inclusion
criteria from their hospital chart. The research assistant A met the mothers when first
time of mother to visit her preterm infant that is for introducing research objectives to
them with a request for participation. When they agreed to participate in this study,
71
the research assistant A ensure them of their human rights and to sign the inform
consent. Then, research assistant A randomly assigned the participants to
experimental group (41 cases) and control group (41 cases) that used simple random
sampling by flipping coin method.
Experimental stage:
1. The research assistants B assesses maternal stress by PSS: NICU,
maternal attachment and as well as other demographic characteristics of mother and
preterm infant dyads (Appendix C) at second time of visiting her preterm infant.
2. In the control group, mother-preterm infant dyads received routine
nursing care till they were discharged one by one. In the experimental group, mother-
preterm infant dyads received routine nursing care in the same way, in conjunction
with the EMPAC program by researcher one by one.
2.1 Control group received routine care. It consists of orientating the
mother about the rules in this unit, encouraging for breast feeding for her infant,
presentation the progress of illness, and the way to keep breast milk for her preterm
infant. When preterm infant plan to discharge, nurses taught them about the way to
observe the severe clinical sign of preterm infant, infant rearing at home that used the
handout of fullterm infant by Ministry of Public Health, and the follow-up day for
mother.
2.2 Experimental group received the EMPAC program. This intervention
has a 3 sessions over 10 day that had the 5 stages as follow:
2.2.1 Stage1: Creating trusting relationship (5 minutes)
The coach started with creating trusting relationship in the second time
visiting preterm infant of mother. Coach had been non hierarchal relationship that
consist of good eye contact, face the coachee directly, be emotionally honest, and
deep listening with compassion and caring. Listening deeply demonstrates respect and
builds mutual trust through empathy and sensitivity. The aim of this stage needs to
develop trust for mother and her family member.
2.2.2 Stage 2: Understanding context of attachment (10 minutes)
The coach will encourage the coachee to explore and express her
feelings and beliefs about illness of preterm infant. The coach will ask questions
relevant to the coachee’s ability and infant care needs and problems, and applied
72
technique of one question question (Wright & Bell, 2009) that will help mother
understanding her emotion and perception when her interact with preterm infant. The
coach will deep listening with compassion, and respecting belief and feeling of
mother. Coach encourage family member supported mother together.
2.2.3 Stage 3: Setting realistic expectation (5 minutes)
The coach offered mother and her family to set the goal and agenda for
reducing stress, increasing perception of attachment, and promoting attachment for
preterm infant. The mother will responsible for bringing the planning. The coach
encouraged family such as father or grandmother involvement to help mother to
develop an action plan for enhancing attachment for her preterm infant. The coach
must provided mental support to uplifting the mothers or make sure that the mother
will be successful in the plan and the effort.
2.2.4 Stage 4: Supporting information and emotion (10 minutes)
This stage had been coached mother to learn about nature of preterm
infant (growth and development) preterm infant’s cue, behavioral state of preterm
infant, preterm infant’s need and how to response to preterm infant’s signals (multi-
modalities sensory stimulation) for mother from her own infant, by using chart
desktop of mother-preterm infant attachment, and demonstration that depending on
need and perception of mother. Coach supported emotional and data for helping
mother understanding situation of attachment in preterm infant. In addition, coach
encourage family member supported mother together.
2.2.5 Stage 5: Reflecting and evaluating (15 minutes)
The coach stimulated mother to interact with preterm infant when
bathing time with recording her behavior by video. Then, coach, mother, and family
member saw the video. Coach encouraged mother reflect on her feelings, perceptions
and behaviors of attachment for preterm infant changing. The coach and family
member provided mental support to uplifting the mothers or make sure that the
mother will be successful in the plan and the effort. The coach gave a positive
affirmation when mother can progress of coping to stress, had more perception of
attachment, and improving attachment skill for preterm infant.
3. On discharge day, the research assistant B assesses maternal stress by
PSS: NICU, and maternal attachment by MAI in both control and experimental
73
groups. In addition, researcher will make appointment for follow-up at dad & mom
clinic with mother, when preterm infant is a 1 month corrected age.
4. Follow-up at dad & mom clinic when preterm infant is a 1 and 2 month
corrected age. Research assistant B assessed maternal stress at home by PSI, maternal
attachment by MAI, and mother-preterm infant attachment by MIAT in both control
and experimental groups. In addition, researcher was record video when preterm
infant had a breast feeding in breast feeding room. Then, researcher send the file of
video record for researcher assistant B for evaluating the score of MIAT.
A summary of the data collection process is show in figure 3-2.
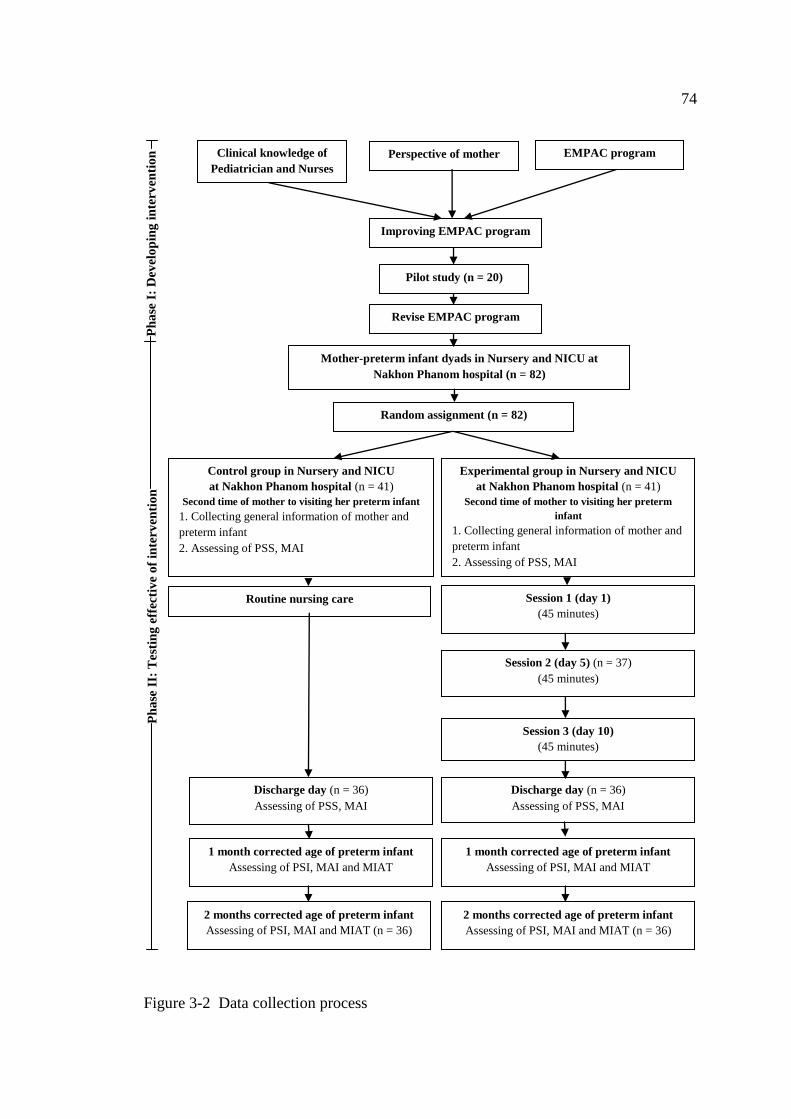
74
Figure 3-2 Data collection process
Mother-preterm infant dyads in Nursery and NICU at
Nakhon Phanom hospital (n = 82)
Random assignment (n = 82)
Control group in Nursery and NICU
at Nakhon Phanom hospital (n = 41)
Second time of mother to visiting her preterm infant
1. Collecting general information of mother and
preterm infant
2. Assessing of PSS, MAI
Experimental group in Nursery and NICU
at Nakhon Phanom hospital (n = 41)
Second time of mother to visiting her preterm
infant
1. Collecting general information of mother and
preterm infant
2. Assessing of PSS, MAI
Routine nursing care
Session 1 (day 1)
(45 minutes)
Discharge day (n = 36)
Assessing of PSS, MAI
Discharge day (n = 36)
Assessing of PSS, MAI
1 month corrected age of preterm infant
Assessing of PSI, MAI and MIAT
1 month corrected age of preterm infant
Assessing of PSI, MAI and MIAT
2 months corrected age of preterm infant
Assessing of PSI, MAI and MIAT (n = 36)
2 months corrected age of preterm infant
Assessing of PSI, MAI and MIAT (n = 36)
Ph
ase
I:
Dev
elo
pin
g i
nte
rven
tio
n
EMPAC program Perspective of mother Clinical knowledge of
Pediatrician and Nurses
Improving EMPAC program
Pilot study (n = 20)
Revise EMPAC program
Ph
ase
II:
Test
ing
eff
ecti
ve
of
inte
rven
tio
n
Session 2 (day 5) (n = 37)
(45 minutes)
Session 3 (day 10)
(45 minutes)
75
Data analysis
The data analysis procedures utilized according to type of data and aims of
study. All of statistic had been tested the assumption before application it. The details
for data analysis were summarizing as follow:
1. Qualitative data analyzed by analytic procedures of Marshall and
Rossman (2006). The analytic procedures fall into seven phases that consist of
a) organizing the data, b) immersion in the data, c) generating categories and themes,
d) coding the data, e) offering interpretations through analytic memos, f) searching for
alternative understandings, and g) writing the report or other format for presenting the
study.
The researcher transcribed the tape-recorded from the interview data. Then,
the data were read, reread line by line and extracted the essential data for coding. The
lists of codes must relate to the research questions. After coding, researchers reviewed
all the codings. The categories were generated by classifying the patterns according to
their similarity and differences, thereafter, the characteristics codings were assigned.
Finally, the themes were emerged by grouping categories to the answers of the
research questions.
Categorization involves identifying codes with similar characteristics and
grouping these together into meaningful categories. Conceptualization involves in
considering the relationship among these categories, and views the data as a whole.
2. Demographic characteristics of preterm infants, mother, pediatricians,
and nurses was analyzed that using descriptive statistics such as frequency,
percentage, mean and standard deviation.
3. Testing similarity between the experimental and the control group used
t-test (parametric test) and chi-square test (non-parametric test) to compare in terms of
demographic data, maternal stress, and maternal attachment at pre-intervention
(second time visiting preterm infant of mother).
4. Testing hypotheses used t-test to compare the mean score of maternal
stress at hospital between experimental and control group at discharge day of preterm
infant.
5. Testing hypotheses used t-test to compare the mean score of maternal
stress at home between experimental and control group at 1 month corrected age of
76
preterm infant. In addition, testing hypotheses use t-test to compare mean score
difference of maternal stress at home between experimental and control group from
1 month to 2 months corrected age of preterm infant.
6. Testing hypotheses used a repeated measures ANOVA to compare the
mean score of maternal attachment between experimental and control group over time
at pre-intervention, discharge day of preterm infant, and at 1 months and 2 months
corrected age of preterm infant.
7. Testing hypotheses used t-test to compare the mean score of mother-
preterm infant attachment between experimental and control group at 1 month
corrected age of preterm infant. In addition, testing hypotheses use t-test to compare
mean score difference of mother-preterm infant attachment between experimental and
control group from 1 month to 2 months corrected age of preterm infant.
77
CHAPTER 4
RESULTS
This chapter presents the research findings concerning the development of
early mother-preterm infant attachment coaching [EMPAC] program for mothers and
preterm infants in Nakhon Phanom Province, Thailand. The research results include
two parts; the development of EMPAC program and the verification the EMPAC
program on maternal stress, maternal attachment, and mother-preterm infant
attachment.
Part 1: Development of EMPAC program
The results of this section are presented in four parts: 1) perspective of
mothers towards attachment for preterm infants, 2) perspective of health care
providers towards clinical knowledge and practice of promoting attachment for
mothers and preterm infants, 3) improving EMPAC program, and 4) pilot study for
revising and testing effectiveness of EMPAC program.
1. Perspective of mothers towards attachment for preterm infants
This part focuses on understanding current situation of attachment from the
perspectives of eight mothers having preterm infants by using in-depth interview.
The average age of mothers who had preterm infants was 28 (SD = 2.56)
years. Most of mothers finished lower than bachelor degree (62.5 %) and 37.5 % of
them were labor occupation. The average families income was 14,127.25 (SD =
9.276.44) baht per month. All mothers were married. Most of them had extended
family (87.5 %), first order of infant (75 %), and had maternal support (75 %). Half of
them had planned for pregnancy and normal labor. Every mother had a complete
antenatal care, and non-experience of preterm infant birth.
The results of this content analysis are described as follows:
The theme expressed in the overall temporal meaning of attachment with
preterm infants was “maternal attachment uncertainty”
Mothers explained “maternal attachment uncertainty” at early state (0-10
days) after birth as uncertainty since the mother had feeling of both promoting and
78
inhibiting maternal attachment of attachment in the same time. The promoting
maternal attachment starts with the affection of mothers that is a root of attachment.
Mothers show their affection, and close attention to care for preterm infant. Mothers
felt pity for their preterm infants. The affection of mothers invited them to visit and
interact with preterm infants. In addition, it also stimulated mothers to seek a way to
attach with their preterm infants. Mothers believed the nurse could coach them in
order to increase the knowledge and skill relevant to attachment with their preterm
infants. Moreover, fathers were facilitated and involved in caring for their preterm
infants. Grandmothers planned to help mothers care for preterm infants at home.
On the other hand, attachment for preterm infants also had inhibiting maternal
attachment because mothers were delaying visiting preterm infants. As the mothers
separated with preterm infants after birth (1-5 days), bonding and attachment between
mothers and preterm infants will be delayed. Besides, mothers were afraid to touch
their preterm infants, anxiety about illness of their preterm infants, and felt sad, shock
and guilt at the same time. When mothers visited preterm infants, most of them could
not interact with their preterm infants, they would only stand behind the incubators.
They feared the interaction will damage their preterm infants because preterm infants
were very small and have illnesses. Accordingly, mothers had a low confidence to
attach with preterm infants. All of these were an inhibiting maternal attachment for
preterm infants.
This theme had been generated from the 5 categories that consist of
“affection of mothers was a root of attachment”, “mothers needed early help from
nurses to promote attachment with preterm infants”, “family support enhanced
maternal confidence to attach preterm infants”, “delay visits affected delay
attachment, and ”mothers felt afraid to attach with preterm infants”.
Affection of mothers was a root of attachment. Mothers absolutely loved
their preterm infants. They also needed to have close attention for caring of preterm
infants because they felt pity for their babies. Moreover, mothers concerned with the
health problem of preterm infants, and miss them when they were in the period of
separation (1-5 days after delivery), some mother expressed that:
“Even I have not seen my baby I still miss him every day” (28 year old
mothers)
79
“I am so sad that he gets sick and has to be in the incubator” (24 year old
mothers)
“It is uncomfortable for him. Every time I see him stay alone in the
incubator” (25 year old mothers)
Mothers needed early help from nurses to promote attachment with preterm
infants. Mothers required the early coaching from nurses to clarify about the
attachment for preterm infants. Mothers didn’t understand the behavior of preterm
infants, and the method to promote positive interaction with their preterm infants.
Moreover, mothers required information related to the progress of preterm infant’s
health. They need to interact with their preterm infants, nevertheless they did not want
to interrupt the sleep of their babies or hurt them, and some mothers stated that:
“I would like some nurses to teach me, how to understand the behavior of
my baby, and how to create the right and no-harmful relationship with my baby in
nursery unit. Later, we can continue doing at home” (22 year old mother)
“It would be the best if we have a nurse coach us at the first week in nursery
unit. Because I don’t know how to take care our baby. ….I am afraid if any problem
occurs” (22 year old mother)
“I need some data about the progress in the health of my babies from
pediatricians and nurses. I don’t need to make something harm, and interrupt the sleep
of my babies. Just only seeing and know the progress is OK.” (30 year old mother)
Family support enhanced maternal confidence to attach preterm infants.
Mothers felt warm when their husband visited the baby with them at
hospital. Moreover, most of the grandmothers plan to help the mothers care for
preterm infants at home that would increase self-confidence of mothers to attach with
preterm infants and decrease maternal stress, some mothers addressed that:
“It makes me feel comfortable when my husband come to visit our baby
along with me every time” (25 year old mother)
“My mother will help me to care my baby when I go home. So, I don’t
worry about that” (23 year old mother)
Delay visit affected delay attachment. Mothers and preterm infants were
separated at the early state after birth for caring preterm infants in the intensive care
unit or nursery unit, caring the suture of mothers, or mother went back home to work.
80
Mothers had no early bonding after birth, and preterm infants had no early attach with
mothers immediately after birth, as some mothers stated that:
“I cannot visit my baby earlier because I need to care the wound first”
(29 year old mother)
“I did not see my baby after birth. I did not know what happen with my
baby” (28 year old mother)
Mothers felt afraid to attach with preterm infants. Mother felt scared, afraid,
fear, as illustrated in some mothers’ responses, especially in NICU because preterm
infants had many types of medical equipment on the body, small size, and less
responsiveness. In addition, mothers felt guilt, sadness, and shock when they knew
their babies were preterm infants that made them uncertain to attach preterm infants,
some mothers expressed that:
“I am not sure how to create the right attachment with my baby. When he
cries, I don’t know what he wants and what I should do” (25 year old mother)
“The preterm infant is too little, so I scare to disturb him because I am afraid
that it will hurt him” (26 year old mother)
“He is very small and skinny…when I look at him I feel unhappy and I feel
sorry for him. I don’t want to see him for long time, it make me unhappy” (23 year old
mother)
“When I open the shutter the air will come inside the incubator and will
make him get cold, and have less air to breathe. I don’t want to stay for long time,
it will dangerous for him” (28 year old mother)
“When I see him in the incubator with many types of equipment in his body,
I’m very sad. I want to hold him but I cannot, it will make him hurt” (30 year old
mother)
2. Perspective of health care providers
This part focuses on understanding current situation about clinical
knowledge and practice of promoting attachment for mothers and preterm infantsin
perspective of health care providers that include five nurses and two pediatricians by
using in-depth interview. The average age of nurses was 36 (SD = 7) years. Most
nurses finished bachelor degree of nursing science (60 %), and had experienced in
nursery unit/ NICU 5-10 years (60 %). The average age of pediatricians was 33
81
(SD = 2) years. Every pediatrician finished residency of pediatric, and had
experienced in nursery unit/ NICU 5-10 years.
The researchers had conducted face-to-face, audiotape, and semi-structured
interviews. Each participant’s interview lasted between 20-25 minutes. The questions
were generated based on the purpose of this phase (Appendix B) that described about
their belief, knowledge, skill, and routine care for promoting attachment between
mothers and preterm infants.
The results of this part are described as follows:
The theme was expressed in the overall temporal meaning of attachment
with preterm infant in perspective of health care providers at Nakhon Phanom
Hospital. This theme was “promoting attachment was important &ambiguous”
Promoting attachment was important. Health care providers are concerned
that promoting mother-preterm infant attachment is very important in order to
enhance the development, especially psycho-social development for preterm infants.
Most of them promoted attachment between mothers and preterm infants at nursery
unit/ neonatal intensive care unit.
Promoting attachment was ambiguous. Nursing care for promoting maternal-
preterm infant attachment was inconsistent. No guideline aimed to make mothers
understand behavioral cues of preterm infant, and the attachment security for preterm
infants. They promoted attachment between mothers and preterm infants by their own
experiences, some nurses and Pediatricians state that:
“Maternal-infant attachment is the most important in creating the
relationship between mothers and preterm infants such feeding and touching. Indeed,
it should be better, if nursing service has the proper guidelines for promoting
attachment. …Besides, we do not have if now. So, nurses will do this nursing care
inconsistently” (pediatrician)
“We promoted attachment between mothers with preterm infants by
encouraging mothers to visit their babies, gave breast milk to babies, touching, and set
the bed for mothers to stay in this unit for taking care of their babies. Now, we did not
have guidelines, everyone promoted attachment by using their own experiences”.
(Nurse)
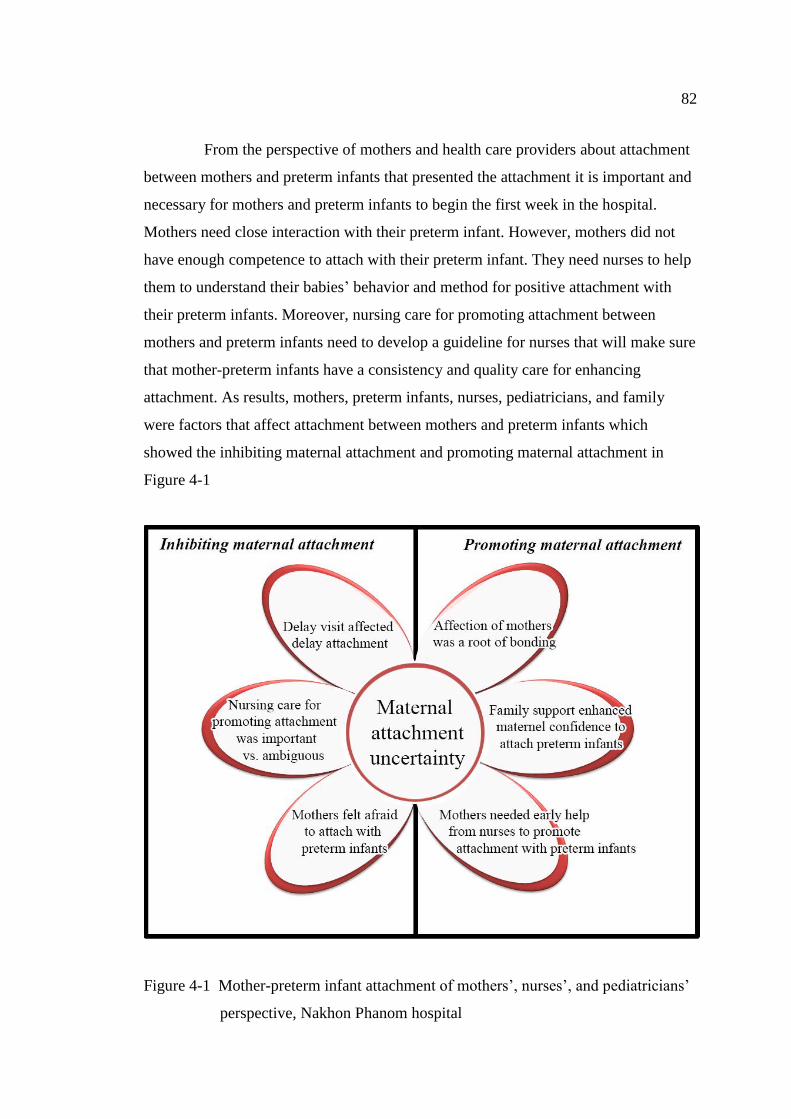
82
From the perspective of mothers and health care providers about attachment
between mothers and preterm infants that presented the attachment it is important and
necessary for mothers and preterm infants to begin the first week in the hospital.
Mothers need close interaction with their preterm infant. However, mothers did not
have enough competence to attach with their preterm infant. They need nurses to help
them to understand their babies’ behavior and method for positive attachment with
their preterm infants. Moreover, nursing care for promoting attachment between
mothers and preterm infants need to develop a guideline for nurses that will make sure
that mother-preterm infants have a consistency and quality care for enhancing
attachment. As results, mothers, preterm infants, nurses, pediatricians, and family
were factors that affect attachment between mothers and preterm infants which
showed the inhibiting maternal attachment and promoting maternal attachment in
Figure 4-1
Figure 4-1 Mother-preterm infant attachment of mothers’, nurses’, and pediatricians’
perspective, Nakhon Phanom hospital
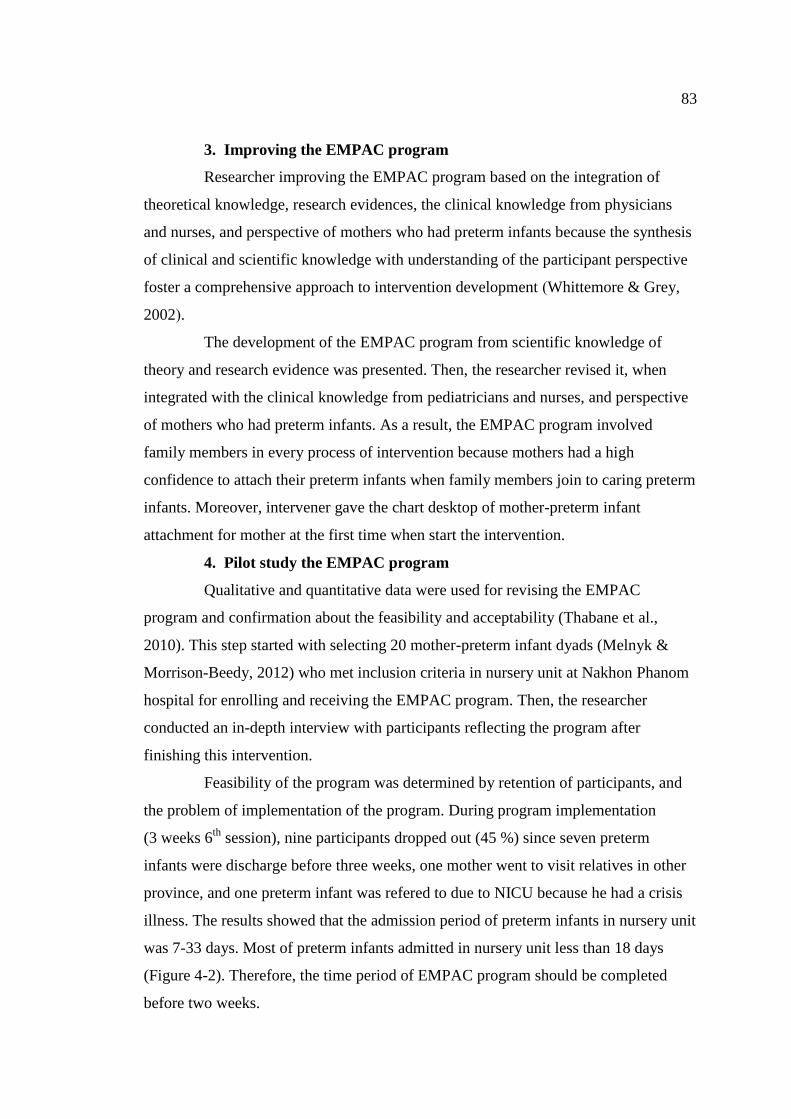
83
3. Improving the EMPAC program
Researcher improving the EMPAC program based on the integration of
theoretical knowledge, research evidences, the clinical knowledge from physicians
and nurses, and perspective of mothers who had preterm infants because the synthesis
of clinical and scientific knowledge with understanding of the participant perspective
foster a comprehensive approach to intervention development (Whittemore & Grey,
2002).
The development of the EMPAC program from scientific knowledge of
theory and research evidence was presented. Then, the researcher revised it, when
integrated with the clinical knowledge from pediatricians and nurses, and perspective
of mothers who had preterm infants. As a result, the EMPAC program involved
family members in every process of intervention because mothers had a high
confidence to attach their preterm infants when family members join to caring preterm
infants. Moreover, intervener gave the chart desktop of mother-preterm infant
attachment for mother at the first time when start the intervention.
4. Pilot study the EMPAC program
Qualitative and quantitative data were used for revising the EMPAC
program and confirmation about the feasibility and acceptability (Thabane et al.,
2010). This step started with selecting 20 mother-preterm infant dyads (Melnyk &
Morrison-Beedy, 2012) who met inclusion criteria in nursery unit at Nakhon Phanom
hospital for enrolling and receiving the EMPAC program. Then, the researcher
conducted an in-depth interview with participants reflecting the program after
finishing this intervention.
Feasibility of the program was determined by retention of participants, and
the problem of implementation of the program. During program implementation
(3 weeks 6th
session), nine participants dropped out (45 %) since seven preterm
infants were discharge before three weeks, one mother went to visit relatives in other
province, and one preterm infant was refered to due to NICU because he had a crisis
illness. The results showed that the admission period of preterm infants in nursery unit
was 7-33 days. Most of preterm infants admitted in nursery unit less than 18 days
(Figure 4-2). Therefore, the time period of EMPAC program should be completed
before two weeks.
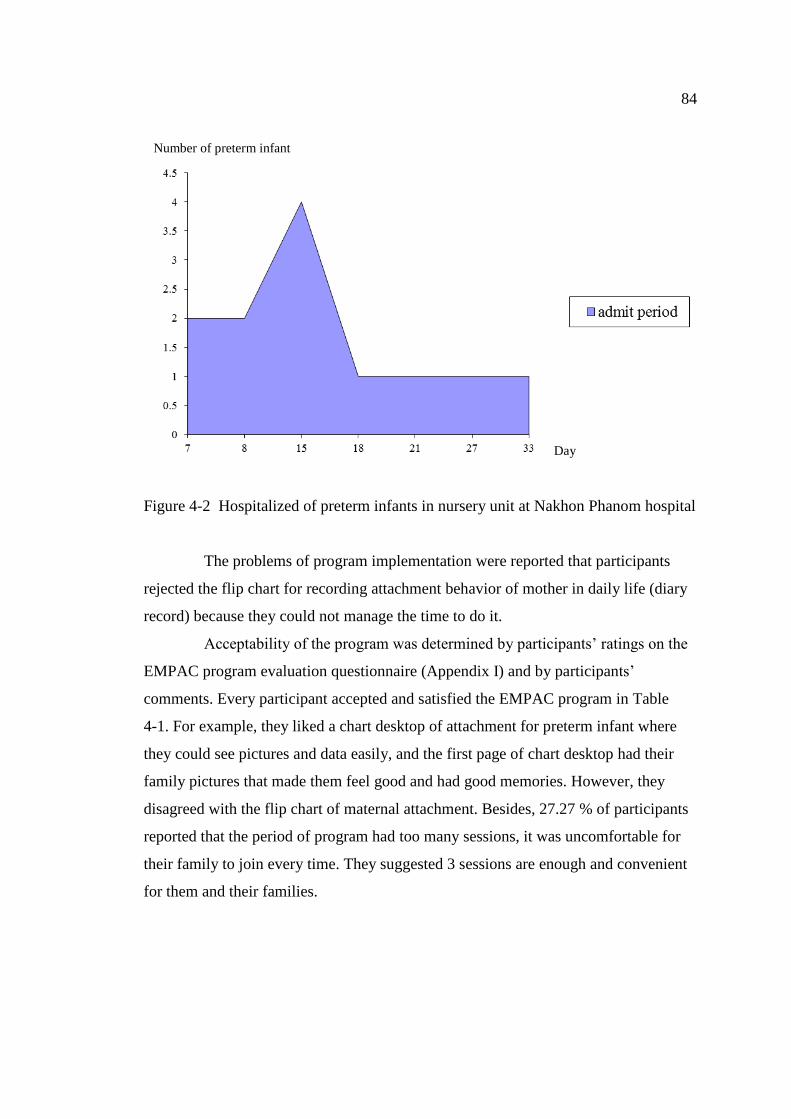
84
Figure 4-2 Hospitalized of preterm infants in nursery unit at Nakhon Phanom hospital
The problems of program implementation were reported that participants
rejected the flip chart for recording attachment behavior of mother in daily life (diary
record) because they could not manage the time to do it.
Acceptability of the program was determined by participants’ ratings on the
EMPAC program evaluation questionnaire (Appendix I) and by participants’
comments. Every participant accepted and satisfied the EMPAC program in Table
4-1. For example, they liked a chart desktop of attachment for preterm infant where
they could see pictures and data easily, and the first page of chart desktop had their
family pictures that made them feel good and had good memories. However, they
disagreed with the flip chart of maternal attachment. Besides, 27.27 % of participants
reported that the period of program had too many sessions, it was uncomfortable for
their family to join every time. They suggested 3 sessions are enough and convenient
for them and their families.
Number of preterm infant
Day
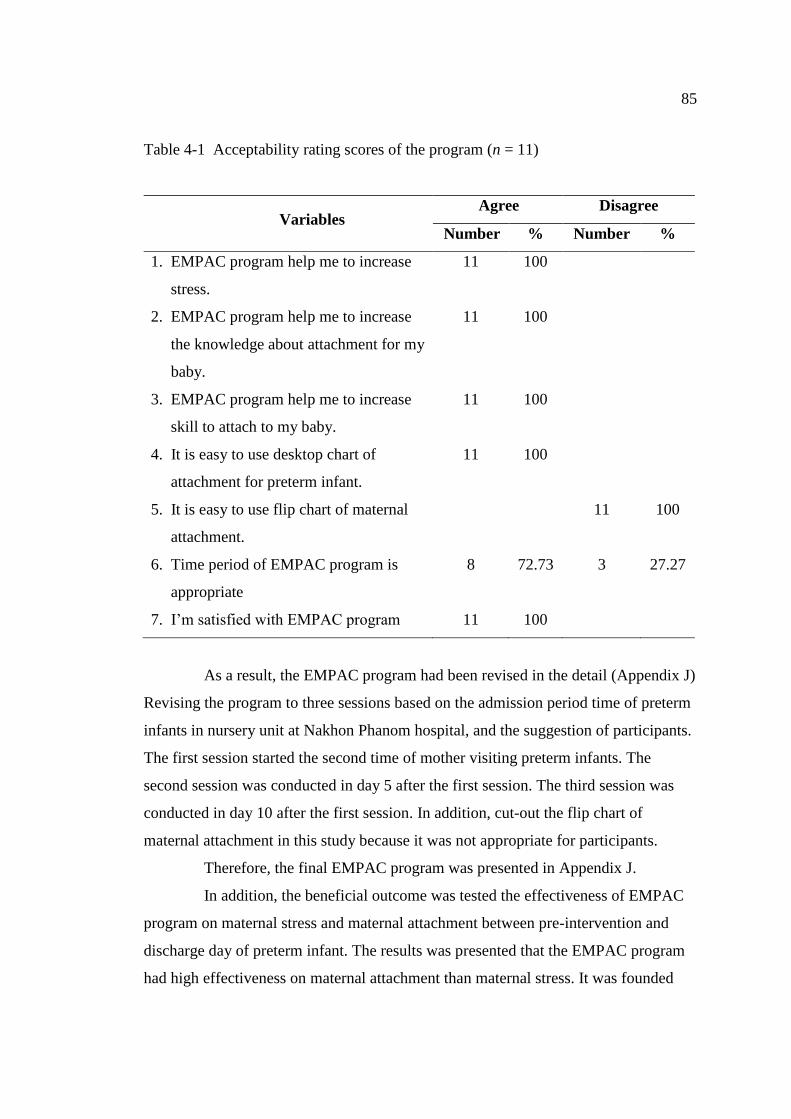
85
Table 4-1 Acceptability rating scores of the program (n = 11)
Variables Agree Disagree
Number % Number %
1. EMPAC program help me to increase
stress.
11 100
2. EMPAC program help me to increase
the knowledge about attachment for my
baby.
11 100
3. EMPAC program help me to increase
skill to attach to my baby.
11 100
4. It is easy to use desktop chart of
attachment for preterm infant.
11 100
5. It is easy to use flip chart of maternal
attachment.
11 100
6. Time period of EMPAC program is
appropriate
8 72.73 3 27.27
7. I’m satisfied with EMPAC program 11 100
As a result, the EMPAC program had been revised in the detail (Appendix J)
Revising the program to three sessions based on the admission period time of preterm
infants in nursery unit at Nakhon Phanom hospital, and the suggestion of participants.
The first session started the second time of mother visiting preterm infants. The
second session was conducted in day 5 after the first session. The third session was
conducted in day 10 after the first session. In addition, cut-out the flip chart of
maternal attachment in this study because it was not appropriate for participants.
Therefore, the final EMPAC program was presented in Appendix J.
In addition, the beneficial outcome was tested the effectiveness of EMPAC
program on maternal stress and maternal attachment between pre-intervention and
discharge day of preterm infant. The results was presented that the EMPAC program
had high effectiveness on maternal attachment than maternal stress. It was founded
86
the effect size of EMPAC program on maternal attachment was 1.12, and the effect
size of EMPAC program on maternal stress was 0.89 (Appendix L).
Part 2: Verification the EMPAC program on maternal stress,
maternal attachment, and mother-preterm infant attachment
The results of this section are presented in three parts: 1) characteristic of
participants in the intervention and control groups, 2) descriptive statistics of maternal
stress, maternal attachment, and mother-preterm infant attachment between the
intervention and control group, and 3) examine the effectiveness of EMPAC program
on maternal stress, maternal attachment, and mother-preterm infant attachment.
1. Characteristic of participants in the intervention and control groups
This study had 82 eligible participants. All of them were invited to
participate and sign the inform consents. The process of data collection found that 10
participants were dropped out because preterm infants discharged before complete the
intervention (one case of experimental group and three cases of control group), and
preterm infant had a severe illness and referred to admit at NICU (four cases of the
experimental group and two cases of the control group). Therefore, the participants of
this study were 72 mother-preterm infant dyads.
1.1 Mother characteristics
In the control group, there were 36 mothers with their mean age of 27.53
years old (SD = 4.35), and average of family income was 19,944 bath/ month
(SD = 10,348). Most of them completed primary school (36.1 %), and bachelor degree
(36.1 %). More than one half of families were extended families (58.3 %), had no
children in the family (63.9 %). Most of mothers planed to get pregnant (66.7 %), and
had grandmother for supporting to care preterm infant at home (61.1 %). Separation
time after birth between mother and preterm infant was 2 days and 4.81 hours
(SD = 35.08). The average time to visit preterm infants of mother was 5.97 days/ week
(SD = 1.40).
In intervention group, there were 36 mothers with their mean age of 29 years
old (SD = 6.81), and average of family income was 22,639 bath/ months
(SD = 17,930). Most of them finished secondary school (44.4 %). More than on half
of families were extended families (69.4 %). Most of mothers planed to get pregnant
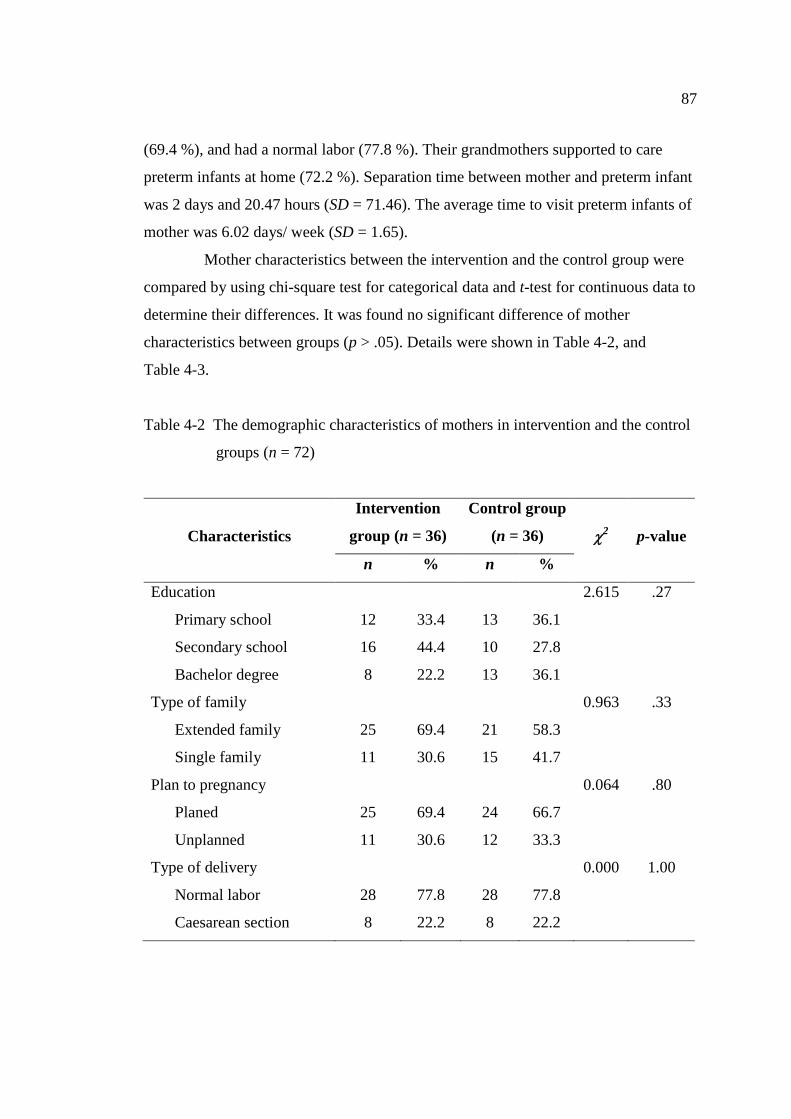
87
(69.4 %), and had a normal labor (77.8 %). Their grandmothers supported to care
preterm infants at home (72.2 %). Separation time between mother and preterm infant
was 2 days and 20.47 hours (SD = 71.46). The average time to visit preterm infants of
mother was 6.02 days/ week (SD = 1.65).
Mother characteristics between the intervention and the control group were
compared by using chi-square test for categorical data and t-test for continuous data to
determine their differences. It was found no significant difference of mother
characteristics between groups (p > .05). Details were shown in Table 4-2, and
Table 4-3.
Table 4-2 The demographic characteristics of mothers in intervention and the control
groups (n = 72)
Characteristics
Intervention
group (n = 36)
Control group
(n = 36) 2 p-value
n % n %
Education
Primary school
Secondary school
Bachelor degree
Type of family
Extended family
Single family
Plan to pregnancy
Planed
Unplanned
Type of delivery
Normal labor
Caesarean section
12
16
8
25
11
25
11
28
8
33.4
44.4
22.2
69.4
30.6
69.4
30.6
77.8
22.2
13
10
13
21
15
24
12
28
8
36.1
27.8
36.1
58.3
41.7
66.7
33.3
77.8
22.2
2.615
0.963
0.064
0.000
.27
.33
.80
1.00
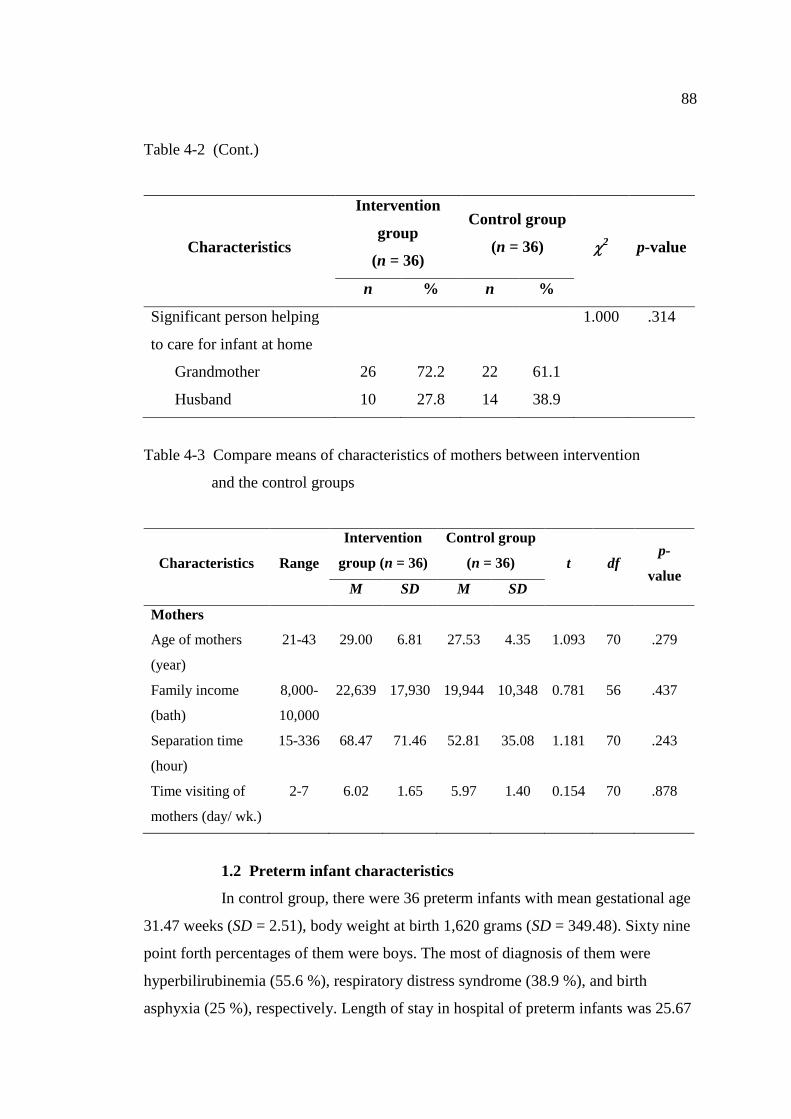
88
Table 4-2 (Cont.)
Characteristics
Intervention
group
(n = 36)
Control group
(n = 36) 2 p-value
n % n %
Significant person helping
to care for infant at home
Grandmother
Husband
26
10
72.2
27.8
22
14
61.1
38.9
1.000 .314
Table 4-3 Compare means of characteristics of mothers between intervention
and the control groups
Characteristics Range
Intervention
group (n = 36)
Control group
(n = 36) t
df p-
value M SD M SD
Mothers
Age of mothers
(year)
21-43
29.00
6.81
27.53
4.35
1.093
70
.279
Family income
(bath)
8,000-
10,000
22,639
17,930
19,944
10,348
0.781
56
.437
Separation time
(hour)
15-336
68.47
71.46
52.81
35.08
1.181 70
.243
Time visiting of
mothers (day/ wk.)
2-7
6.02 1.65
5.97
1.40
0.154
70
.878
1.2 Preterm infant characteristics
In control group, there were 36 preterm infants with mean gestational age
31.47 weeks (SD = 2.51), body weight at birth 1,620 grams (SD = 349.48). Sixty nine
point forth percentages of them were boys. The most of diagnosis of them were
hyperbilirubinemia (55.6 %), respiratory distress syndrome (38.9 %), and birth
asphyxia (25 %), respectively. Length of stay in hospital of preterm infants was 25.67
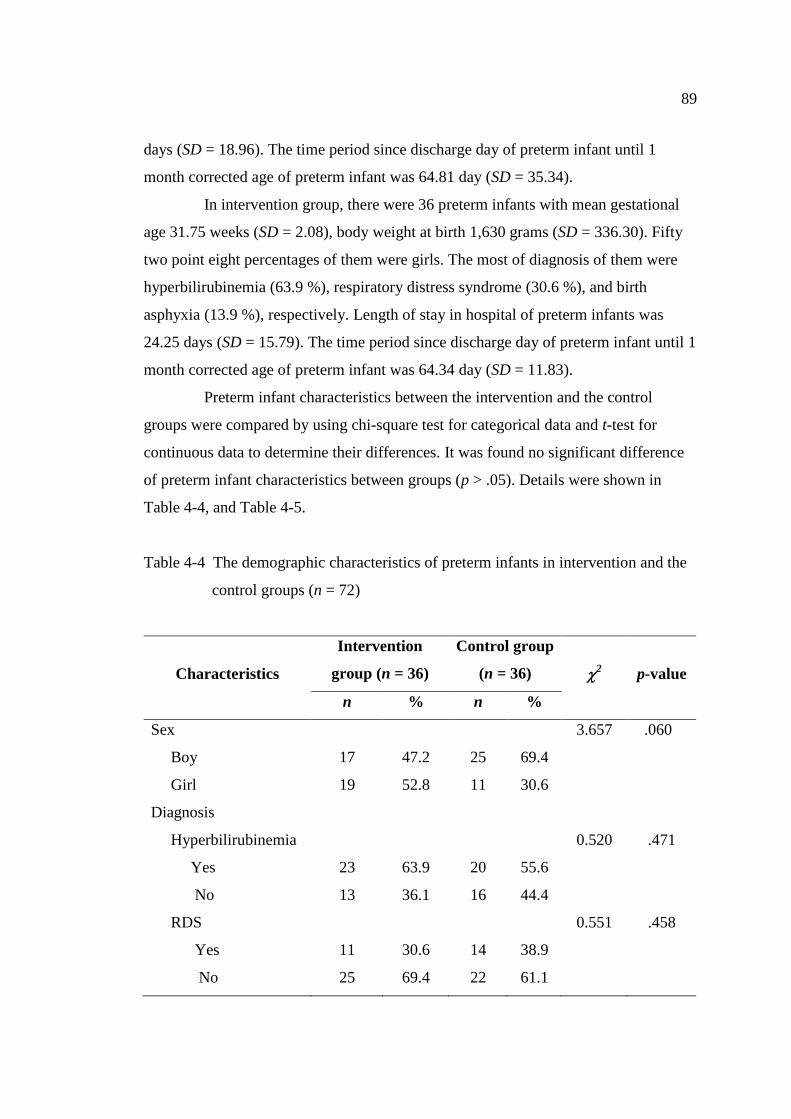
89
days (SD = 18.96). The time period since discharge day of preterm infant until 1
month corrected age of preterm infant was 64.81 day (SD = 35.34).
In intervention group, there were 36 preterm infants with mean gestational
age 31.75 weeks (SD = 2.08), body weight at birth 1,630 grams (SD = 336.30). Fifty
two point eight percentages of them were girls. The most of diagnosis of them were
hyperbilirubinemia (63.9 %), respiratory distress syndrome (30.6 %), and birth
asphyxia (13.9 %), respectively. Length of stay in hospital of preterm infants was
24.25 days (SD = 15.79). The time period since discharge day of preterm infant until 1
month corrected age of preterm infant was 64.34 day (SD = 11.83).
Preterm infant characteristics between the intervention and the control
groups were compared by using chi-square test for categorical data and t-test for
continuous data to determine their differences. It was found no significant difference
of preterm infant characteristics between groups (p > .05). Details were shown in
Table 4-4, and Table 4-5.
Table 4-4 The demographic characteristics of preterm infants in intervention and the
control groups (n = 72)
Characteristics
Intervention
group (n = 36)
Control group
(n = 36) 2 p-value
n % n %
Sex
Boy
Girl
Diagnosis
Hyperbilirubinemia
Yes
No
RDS
Yes
No
17
19
23
13
11
25
47.2
52.8
63.9
36.1
30.6
69.4
25
11
20
16
14
22
69.4
30.6
55.6
44.4
38.9
61.1
3.657
0.520
0.551
.060
.471
.458
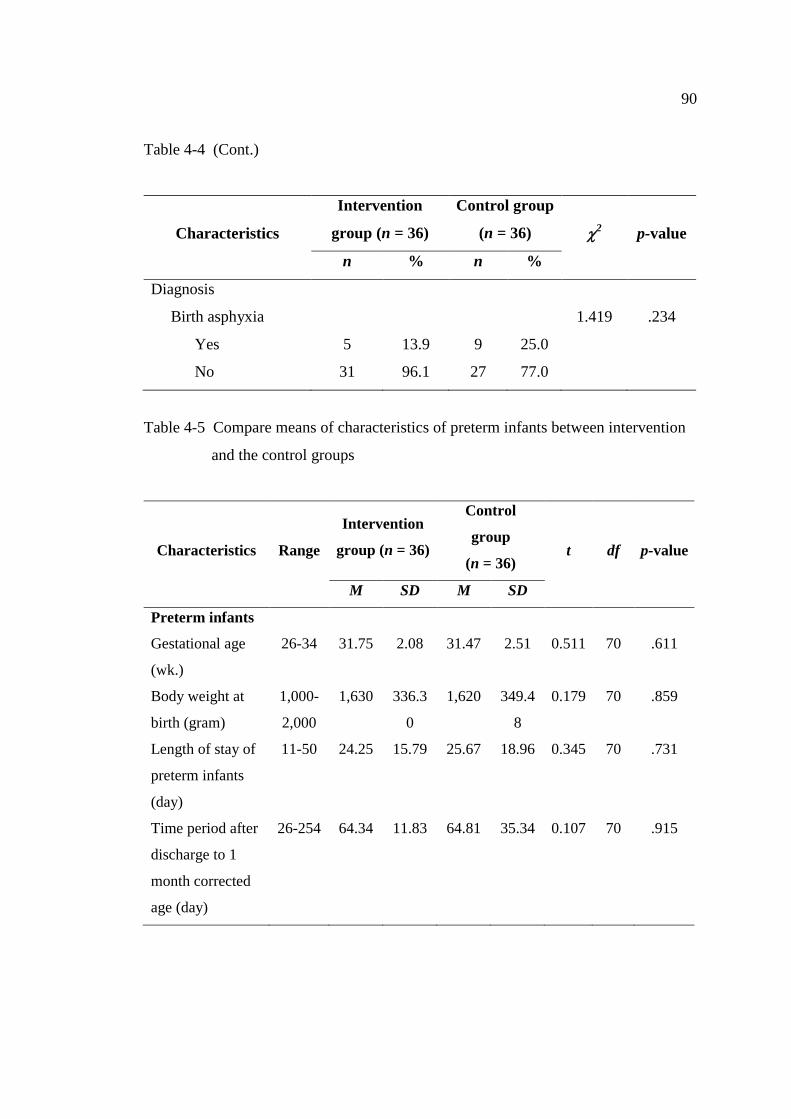
90
Table 4-4 (Cont.)
Characteristics
Intervention
group (n = 36)
Control group
(n = 36) 2 p-value
n % n %
Diagnosis
Birth asphyxia
Yes
No
5
31
13.9
96.1
9
27
25.0
77.0
1.419
.234
Table 4-5 Compare means of characteristics of preterm infants between intervention
and the control groups
Characteristics Range
Intervention
group (n = 36)
Control
group
(n = 36) t df p-value
M SD M SD
Preterm infants
Gestational age
(wk.)
26-34
31.75
2.08
31.47
2.51
0.511
70
.611
Body weight at
birth (gram)
1,000-
2,000
1,630 336.3
0
1,620 349.4
8
0.179 70 .859
Length of stay of
preterm infants
(day)
Time period after
discharge to 1
month corrected
age (day)
11-50
26-254
24.25
64.34
15.79
11.83
25.67
64.81
18.96
35.34
0.345
0.107
70
70
.731
.915
91
2. Description statistics of outcome variables
In this study, outcome variables consisted of maternal stress, maternal
attachment, and mother-preterm infant attachment. Means and standard deviations
were used to describe these variables.
2.1 Maternal stress
This study evaluated maternal stress in two periods that was maternal
stress which occurred during preterm infants stay at hospital and maternal stress
which occurred after preterm infants discharge at home.
For the control group, means scores of maternal stress at hospital at
pre-intervention (baseline) and at discharge day of preterm infants, as measured by
PSS: NICU, were 87.89 (SD = 22.72) and 67.36 (SD = 23.20), respectively. Mean
score differences between pre-intervention and discharge day of preterm infants of
maternal stress at hospital was 20.53 (SD = 19.69). Mean scores of its three subscale
of two times measurement were also calculated. The mean scores of maternal stress
towards sight and sounds were 15.06 (SD = 8.29) and 10.97 (SD = 3.82). The mean
scores of maternal stress towards baby looks and behaves were 54.72 (SD = 20.16)
and 37.31 (SD = 13.50). Maternal stress towards relationship had mean scores of 28
(SD = 12.84) and 19.08 (SD = 7.74), respectively. Besides, maternal stress at 1 month,
and 2 months corrected age of preterm infant at home, as measured by PSI, were
118.78 (SD = 15.49) and 102.47 (SD = 12.71), respectively. Mean score differences
between 1 month and 2 months corrected age of preterm infants of maternal stress at
home was 16.31 (SD = 7.99).
For the intervention group, means scores of maternal stress at hospital at
pre-intervention (baseline) and at discharge day of preterm infants, as measured by
PSS: NICU, were 87.81 (SD = 22.72) and 43.81 (SD = 6.55), respectively. Mean score
differences between pre-intervention and discharge day of preterm infants of maternal
stress at hospital was 44 (SD = 21.44). Mean scores of its 3 subscale of 2 times
measurement were also calculated. The mean scores of maternal stress towards sight
and sounds were 16.33 (SD = 7.80) and 7.19 (SD = 1.19). The mean scores of
maternal stress towards baby looks and behaves were 59.72 (SD = 18.88) and 22.31
(SD = 3.46). Maternal stress towards relationship had mean scores of 29.14
(SD = 10.41) and 14.31 (SD = 3.00), respectively. Besides, maternal stress at 1 month,

92
and 2 months corrected age of preterm infant at home, as measured by PSI, were
98.41 (SD = 13.07) and 86.58 (SD = 9.01), respectively. Mean score differences
between 1 month and 2 months corrected age of preterm infants of maternal stress at
home was 11.83 (SD = 9.28). It showed the stresses of mothers in both groups were
decreased from baseline. (Table 4-6)
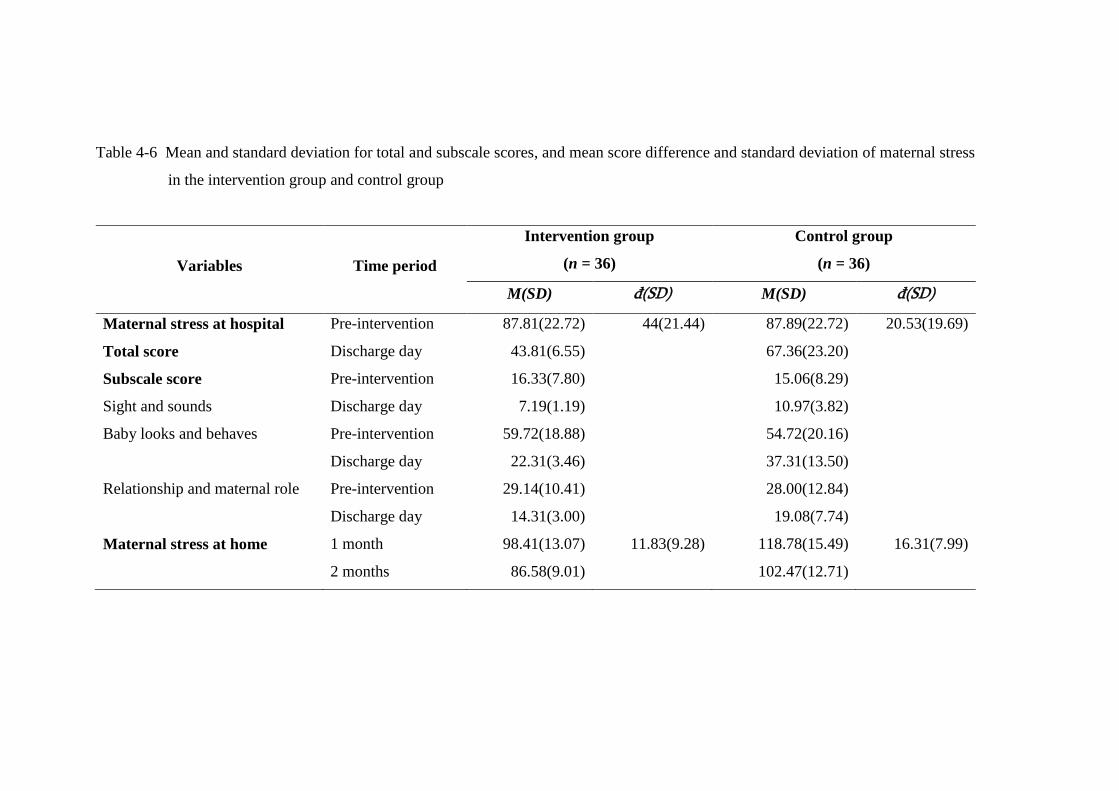
77
Table 4-6 Mean and standard deviation for total and subscale scores, and mean score difference and standard deviation of maternal stress
in the intervention group and control group
Variables Time period
Intervention group
(n = 36)
Control group
(n = 36)
M(SD) đ(SD) M(SD) đ(SD)
Maternal stress at hospital
Total score
Pre-intervention
Discharge day
87.81(22.72)
43.81(6.55)
44(21.44)
87.89(22.72)
67.36(23.20)
20.53(19.69)
Subscale score
Sight and sounds
Pre-intervention
Discharge day
16.33(7.80)
7.19(1.19)
15.06(8.29)
10.97(3.82)
Baby looks and behaves Pre-intervention
Discharge day
59.72(18.88)
22.31(3.46)
54.72(20.16)
37.31(13.50)
Relationship and maternal role Pre-intervention
Discharge day
29.14(10.41)
14.31(3.00)
28.00(12.84)
19.08(7.74)
Maternal stress at home 1 month
2 months
98.41(13.07)
86.58(9.01)
11.83(9.28) 118.78(15.49)
102.47(12.71)
16.31(7.99)
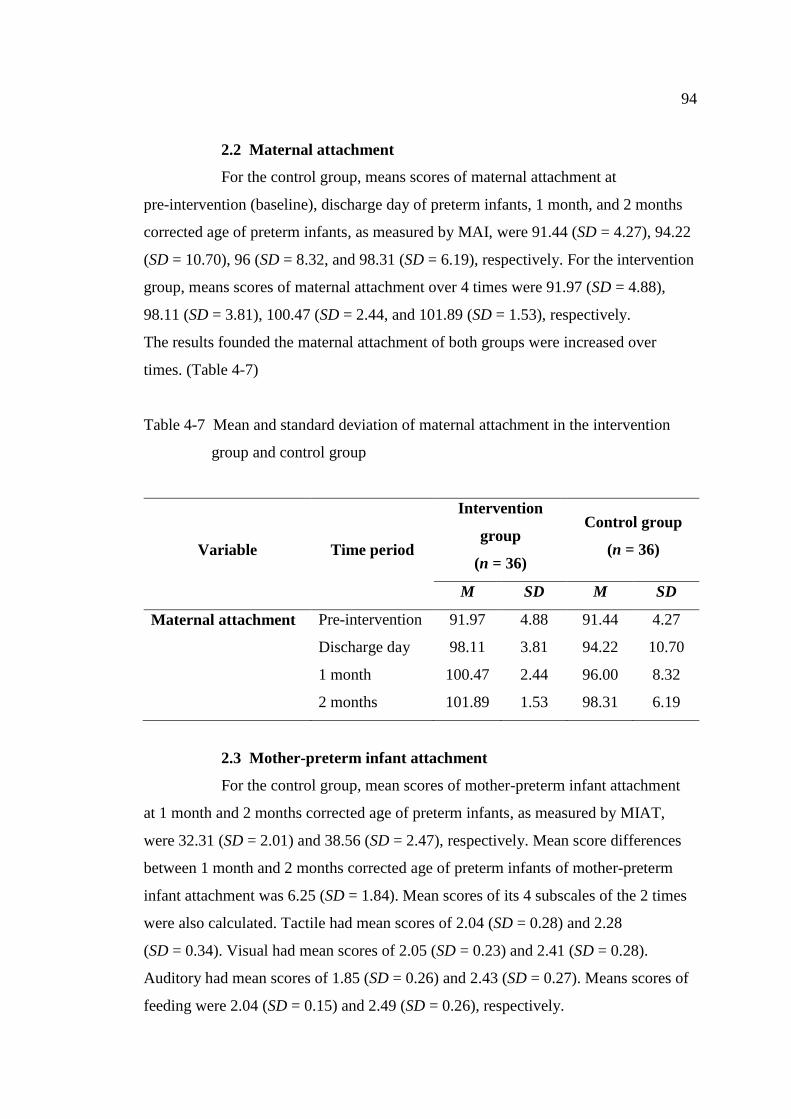
94
2.2 Maternal attachment
For the control group, means scores of maternal attachment at
pre-intervention (baseline), discharge day of preterm infants, 1 month, and 2 months
corrected age of preterm infants, as measured by MAI, were 91.44 (SD = 4.27), 94.22
(SD = 10.70), 96 (SD = 8.32, and 98.31 (SD = 6.19), respectively. For the intervention
group, means scores of maternal attachment over 4 times were 91.97 (SD = 4.88),
98.11 (SD = 3.81), 100.47 (SD = 2.44, and 101.89 (SD = 1.53), respectively.
The results founded the maternal attachment of both groups were increased over
times. (Table 4-7)
Table 4-7 Mean and standard deviation of maternal attachment in the intervention
group and control group
Variable Time period
Intervention
group
(n = 36)
Control group
(n = 36)
M SD M SD
Maternal attachment
Pre-intervention
Discharge day
1 month
2 months
91.97
98.11
100.47
101.89
4.88
3.81
2.44
1.53
91.44
94.22
96.00
98.31
4.27
10.70
8.32
6.19
2.3 Mother-preterm infant attachment
For the control group, mean scores of mother-preterm infant attachment
at 1 month and 2 months corrected age of preterm infants, as measured by MIAT,
were 32.31 (SD = 2.01) and 38.56 (SD = 2.47), respectively. Mean score differences
between 1 month and 2 months corrected age of preterm infants of mother-preterm
infant attachment was 6.25 (SD = 1.84). Mean scores of its 4 subscales of the 2 times
were also calculated. Tactile had mean scores of 2.04 (SD = 0.28) and 2.28
(SD = 0.34). Visual had mean scores of 2.05 (SD = 0.23) and 2.41 (SD = 0.28).
Auditory had mean scores of 1.85 (SD = 0.26) and 2.43 (SD = 0.27). Means scores of
feeding were 2.04 (SD = 0.15) and 2.49 (SD = 0.26), respectively.
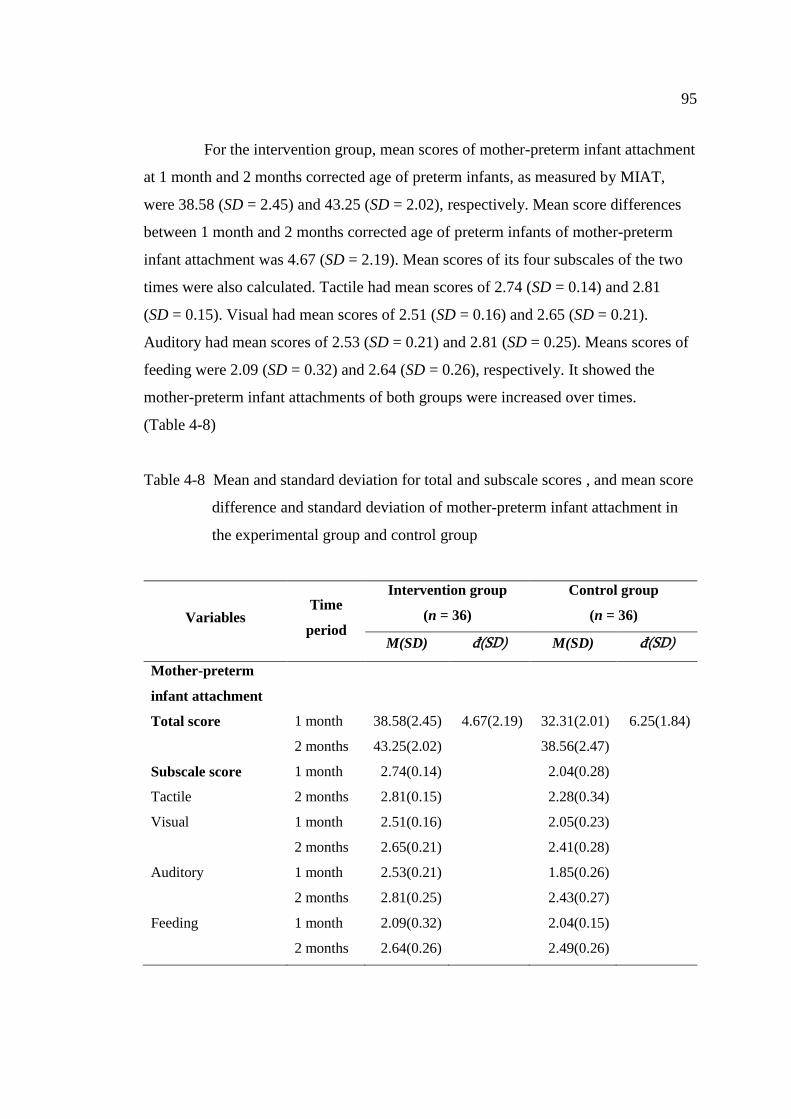
95
For the intervention group, mean scores of mother-preterm infant attachment
at 1 month and 2 months corrected age of preterm infants, as measured by MIAT,
were 38.58 (SD = 2.45) and 43.25 (SD = 2.02), respectively. Mean score differences
between 1 month and 2 months corrected age of preterm infants of mother-preterm
infant attachment was 4.67 (SD = 2.19). Mean scores of its four subscales of the two
times were also calculated. Tactile had mean scores of 2.74 (SD = 0.14) and 2.81
(SD = 0.15). Visual had mean scores of 2.51 (SD = 0.16) and 2.65 (SD = 0.21).
Auditory had mean scores of 2.53 (SD = 0.21) and 2.81 (SD = 0.25). Means scores of
feeding were 2.09 (SD = 0.32) and 2.64 (SD = 0.26), respectively. It showed the
mother-preterm infant attachments of both groups were increased over times.
(Table 4-8)
Table 4-8 Mean and standard deviation for total and subscale scores , and mean score
difference and standard deviation of mother-preterm infant attachment in
the experimental group and control group
Variables Time
period
Intervention group
(n = 36)
Control group
(n = 36)
M(SD) đ(SD) M(SD) đ(SD)
Mother-preterm
infant attachment
Total score
1 month
2 months
38.58(2.45)
43.25(2.02)
4.67(2.19)
32.31(2.01)
38.56(2.47)
6.25(1.84)
Subscale score
Tactile
1 month
2 months
2.74(0.14)
2.81(0.15)
2.04(0.28)
2.28(0.34)
Visual
1 month
2 months
2.51(0.16)
2.65(0.21)
2.05(0.23)
2.41(0.28)
Auditory
1 month
2 months
2.53(0.21)
2.81(0.25)
1.85(0.26)
2.43(0.27)
Feeding
1 month
2 months
2.09(0.32)
2.64(0.26)
2.04(0.15)
2.49(0.26)
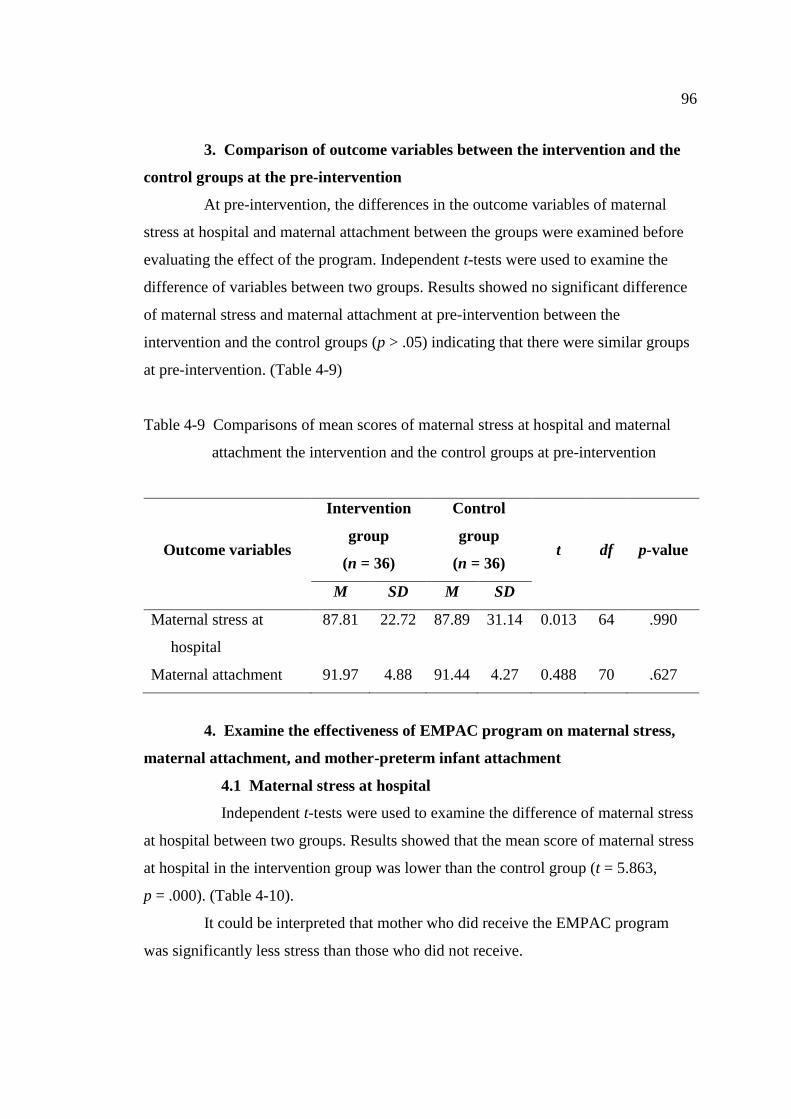
96
3. Comparison of outcome variables between the intervention and the
control groups at the pre-intervention
At pre-intervention, the differences in the outcome variables of maternal
stress at hospital and maternal attachment between the groups were examined before
evaluating the effect of the program. Independent t-tests were used to examine the
difference of variables between two groups. Results showed no significant difference
of maternal stress and maternal attachment at pre-intervention between the
intervention and the control groups (p > .05) indicating that there were similar groups
at pre-intervention. (Table 4-9)
Table 4-9 Comparisons of mean scores of maternal stress at hospital and maternal
attachment the intervention and the control groups at pre-intervention
Outcome variables
Intervention
group
(n = 36)
Control
group
(n = 36) t df p-value
M SD M SD
Maternal stress at
hospital
Maternal attachment
87.81
91.97
22.72
4.88
87.89
91.44
31.14
4.27
0.013
0.488
64
70
.990
.627
4. Examine the effectiveness of EMPAC program on maternal stress,
maternal attachment, and mother-preterm infant attachment
4.1 Maternal stress at hospital
Independent t-tests were used to examine the difference of maternal stress
at hospital between two groups. Results showed that the mean score of maternal stress
at hospital in the intervention group was lower than the control group (t = 5.863,
p = .000). (Table 4-10).
It could be interpreted that mother who did receive the EMPAC program
was significantly less stress than those who did not receive.
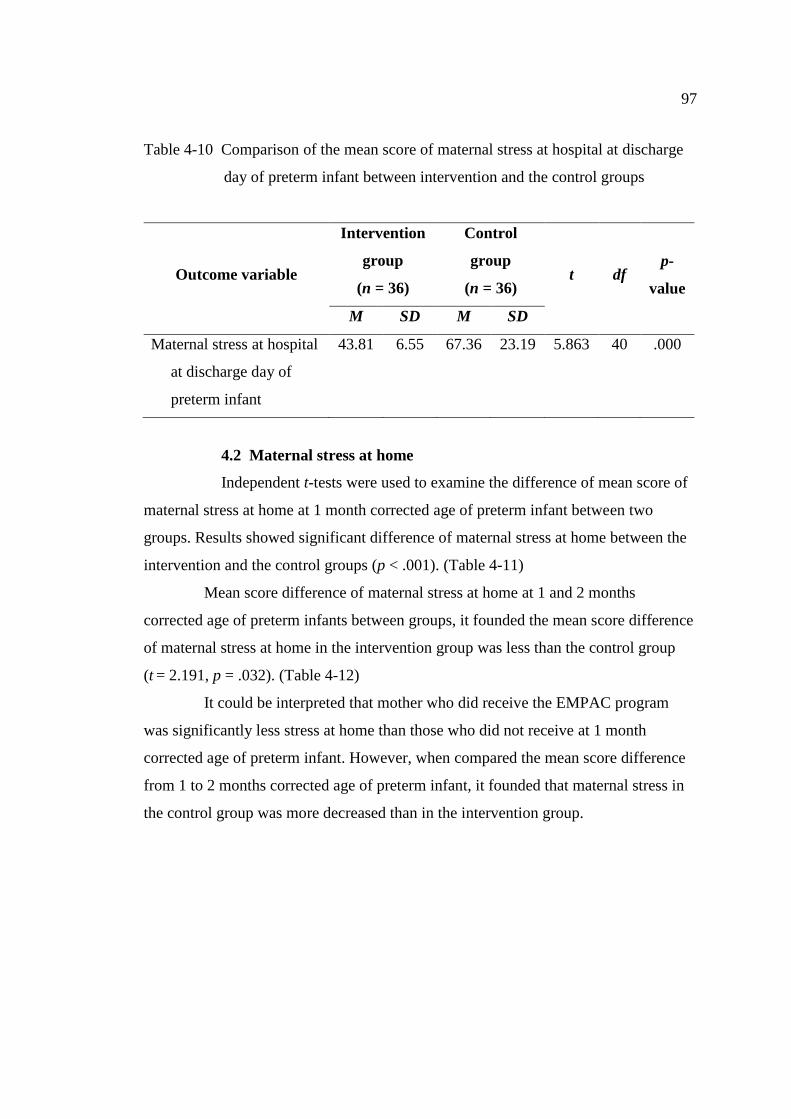
97
Table 4-10 Comparison of the mean score of maternal stress at hospital at discharge
day of preterm infant between intervention and the control groups
Outcome variable
Intervention
group
(n = 36)
Control
group
(n = 36) t df
p-
value
M SD M SD
Maternal stress at hospital
at discharge day of
preterm infant
43.81
6.55
67.36
23.19
5.863
40 .000
4.2 Maternal stress at home
Independent t-tests were used to examine the difference of mean score of
maternal stress at home at 1 month corrected age of preterm infant between two
groups. Results showed significant difference of maternal stress at home between the
intervention and the control groups (p < .001). (Table 4-11)
Mean score difference of maternal stress at home at 1 and 2 months
corrected age of preterm infants between groups, it founded the mean score difference
of maternal stress at home in the intervention group was less than the control group
(t = 2.191, p = .032). (Table 4-12)
It could be interpreted that mother who did receive the EMPAC program
was significantly less stress at home than those who did not receive at 1 month
corrected age of preterm infant. However, when compared the mean score difference
from 1 to 2 months corrected age of preterm infant, it founded that maternal stress in
the control group was more decreased than in the intervention group.
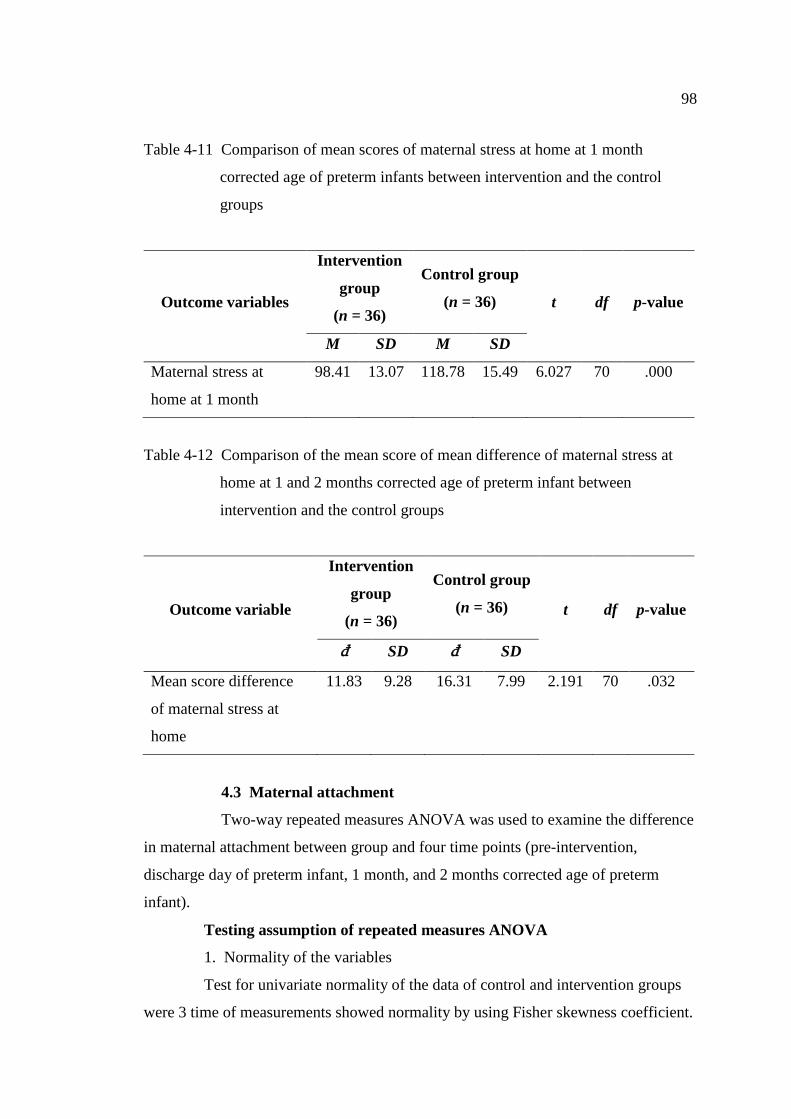
98
Table 4-11 Comparison of mean scores of maternal stress at home at 1 month
corrected age of preterm infants between intervention and the control
groups
Outcome variables
Intervention
group
(n = 36)
Control group
(n = 36) t df p-value
M SD M SD
Maternal stress at
home at 1 month
98.41 13.07 118.78 15.49 6.027 70 .000
Table 4-12 Comparison of the mean score of mean difference of maternal stress at
home at 1 and 2 months corrected age of preterm infant between
intervention and the control groups
Outcome variable
Intervention
group
(n = 36)
Control group
(n = 36) t df p-value
đ SD đ SD
Mean score difference
of maternal stress at
home
11.83 9.28 16.31 7.99 2.191 70 .032
4.3 Maternal attachment
Two-way repeated measures ANOVA was used to examine the difference
in maternal attachment between group and four time points (pre-intervention,
discharge day of preterm infant, 1 month, and 2 months corrected age of preterm
infant).
Testing assumption of repeated measures ANOVA
1. Normality of the variables
Test for univariate normality of the data of control and intervention groups
were 3 time of measurements showed normality by using Fisher skewness coefficient.
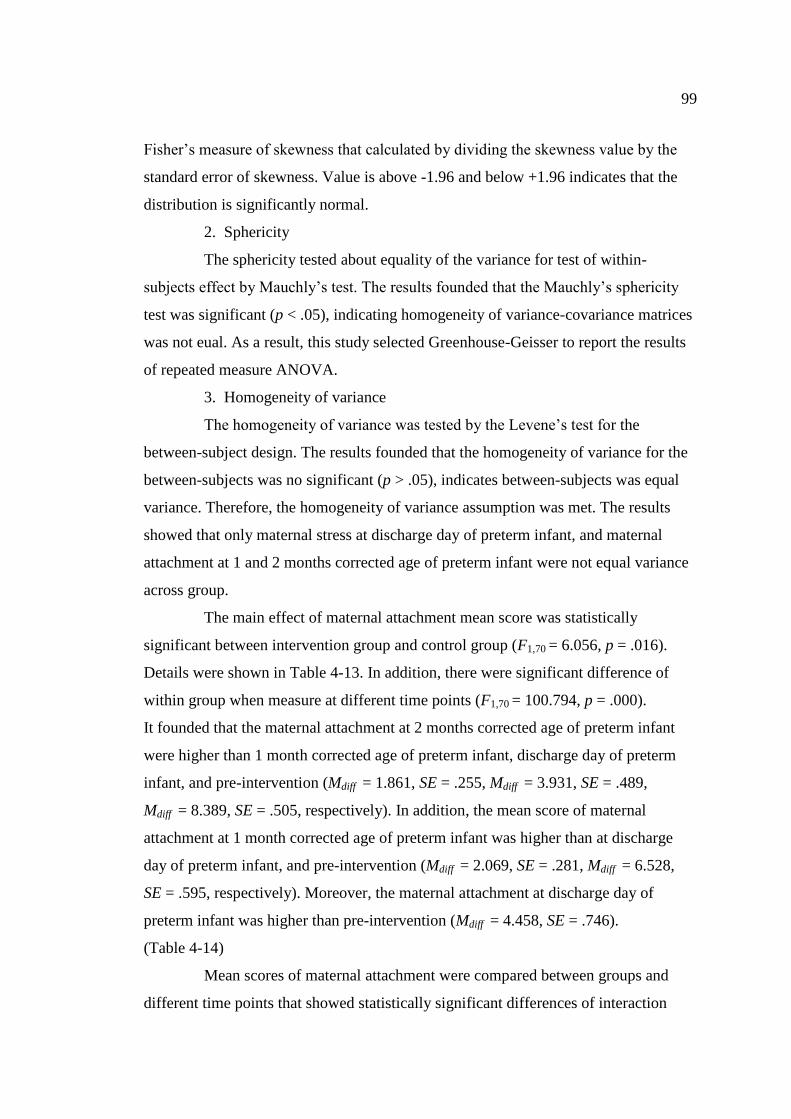
99
Fisher’s measure of skewness that calculated by dividing the skewness value by the
standard error of skewness. Value is above -1.96 and below +1.96 indicates that the
distribution is significantly normal.
2. Sphericity
The sphericity tested about equality of the variance for test of within-
subjects effect by Mauchly’s test. The results founded that the Mauchly’s sphericity
test was significant (p < .05), indicating homogeneity of variance-covariance matrices
was not eual. As a result, this study selected Greenhouse-Geisser to report the results
of repeated measure ANOVA.
3. Homogeneity of variance
The homogeneity of variance was tested by the Levene’s test for the
between-subject design. The results founded that the homogeneity of variance for the
between-subjects was no significant (p > .05), indicates between-subjects was equal
variance. Therefore, the homogeneity of variance assumption was met. The results
showed that only maternal stress at discharge day of preterm infant, and maternal
attachment at 1 and 2 months corrected age of preterm infant were not equal variance
across group.
The main effect of maternal attachment mean score was statistically
significant between intervention group and control group (F1,70 = 6.056, p = .016).
Details were shown in Table 4-13. In addition, there were significant difference of
within group when measure at different time points (F1,70 = 100.794, p = .000).
It founded that the maternal attachment at 2 months corrected age of preterm infant
were higher than 1 month corrected age of preterm infant, discharge day of preterm
infant, and pre-intervention (Mdiff = 1.861, SE = .255, Mdiff = 3.931, SE = .489,
Mdiff = 8.389, SE = .505, respectively). In addition, the mean score of maternal
attachment at 1 month corrected age of preterm infant was higher than at discharge
day of preterm infant, and pre-intervention (Mdiff = 2.069, SE = .281, Mdiff = 6.528,
SE = .595, respectively). Moreover, the maternal attachment at discharge day of
preterm infant was higher than pre-intervention (Mdiff = 4.458, SE = .746).
(Table 4-14)
Mean scores of maternal attachment were compared between groups and
different time points that showed statistically significant differences of interaction
100
effect (F1,17 = 6.042, P = .007, partial Eta square = .064), indicating the mean scores of
maternal attachment between intervention and control group was different over time.
(Table 4-13)
It could be interpreted that mother who received the EMPAC program was
significantly increased maternal attachment better than those who did not received.
In addition, within the intervention group, when the time change, the EMPAC
program could increase maternal attachment at 2 months corrected age of preterm
infant that was significantly higher than those at 1 months corrected age of preterm
infant.
Table 4-13 Comparison the score of maternal attachment between experimental and
control group overtime at pre-intervention, discharge day of preterm
infant, 1 month corrected age, and 2 months corrected age of preterm
infant
Source SS df MS F SE p-value
Within subject
Time
Time*Group
Error time
Between subject
Group
Error
2809.038
168.372
1950.840
700.003
8090.965
1.528
1.525
106.731
1
70
1842.324
110.427
18.278
700.003
115.585
100.794
6.042
6.056
.59
.079
.08
.000
.007
.016
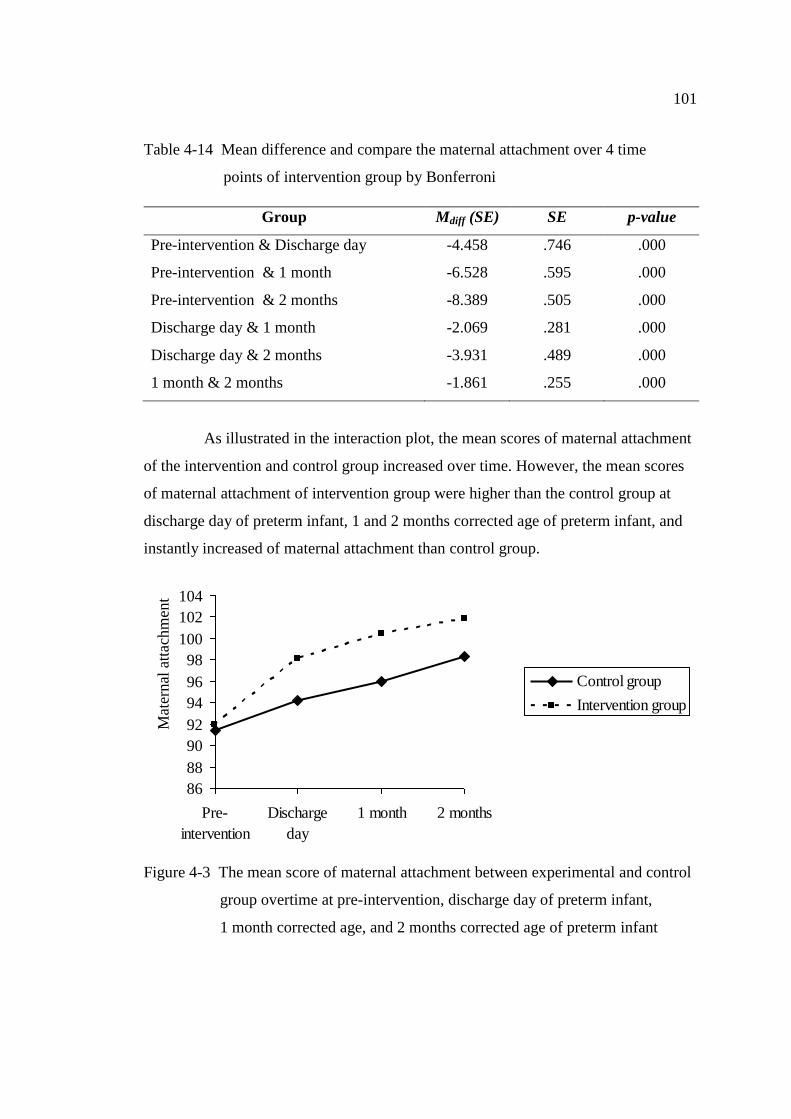
101
Table 4-14 Mean difference and compare the maternal attachment over 4 time
points of intervention group by Bonferroni
Group Mdiff (SE) SE p-value
Pre-intervention & Discharge day
Pre-intervention & 1 month
Pre-intervention & 2 months
Discharge day & 1 month
Discharge day & 2 months
1 month & 2 months
-4.458
-6.528
-8.389
-2.069
-3.931
-1.861
.746
.595
.505
.281
.489
.255
.000
.000
.000
.000
.000
.000
As illustrated in the interaction plot, the mean scores of maternal attachment
of the intervention and control group increased over time. However, the mean scores
of maternal attachment of intervention group were higher than the control group at
discharge day of preterm infant, 1 and 2 months corrected age of preterm infant, and
instantly increased of maternal attachment than control group.
86
88
90
92
94
96
98
100
102
104
Pre-
intervention
Discharge
day
1 month 2 months
Control group
Intervention group
Figure 4-3 The mean score of maternal attachment between experimental and control
group overtime at pre-intervention, discharge day of preterm infant,
1 month corrected age, and 2 months corrected age of preterm infant
Mat
ernal
att
achm
ent

102
4.4 Mother-preterm infant attachment
Independent t tests were used to examine the difference of mean score of
mother-preterm infant attachment at 1 month corrected age of preterm infant between
two groups. Results showed significant difference of mother-preterm infant
attachment between the intervention and the control groups (p < .001). (Table 4-15)
When compared the mean score difference of mother-preterm infant
attachment at 1 and 2 months corrected age of preterm infants between groups,
it founded the mean score difference mother-preterm infant attachment in the
intervention group was lower than the control group (t = 3.319, p = .001).
(Table 4-16)
It could be interpreted that mother who did receive the EMPAC program
was significantly high mother-preterm infant attachment than those who did not
receive at 1 month corrected age of preterm infant. However, when compared the
mean score difference from 1 to 2 months corrected age of preterm infant, it founded
that mother-preterm infant attachment in the control group was more increased than in
the intervention group.
Table 4-15 Comparison of mean scores of mother-preterm infant attachment at
1 month corrected age of preterm infants between intervention and the
control groups
Outcome variable
Intervention
group
(n = 36)
Control
group
(n = 36) t df p-value
M SD M SD
Mother-preterm infant
attachment at 1 month
38.58
2.45
32.31
2.01 11.871
70 .000
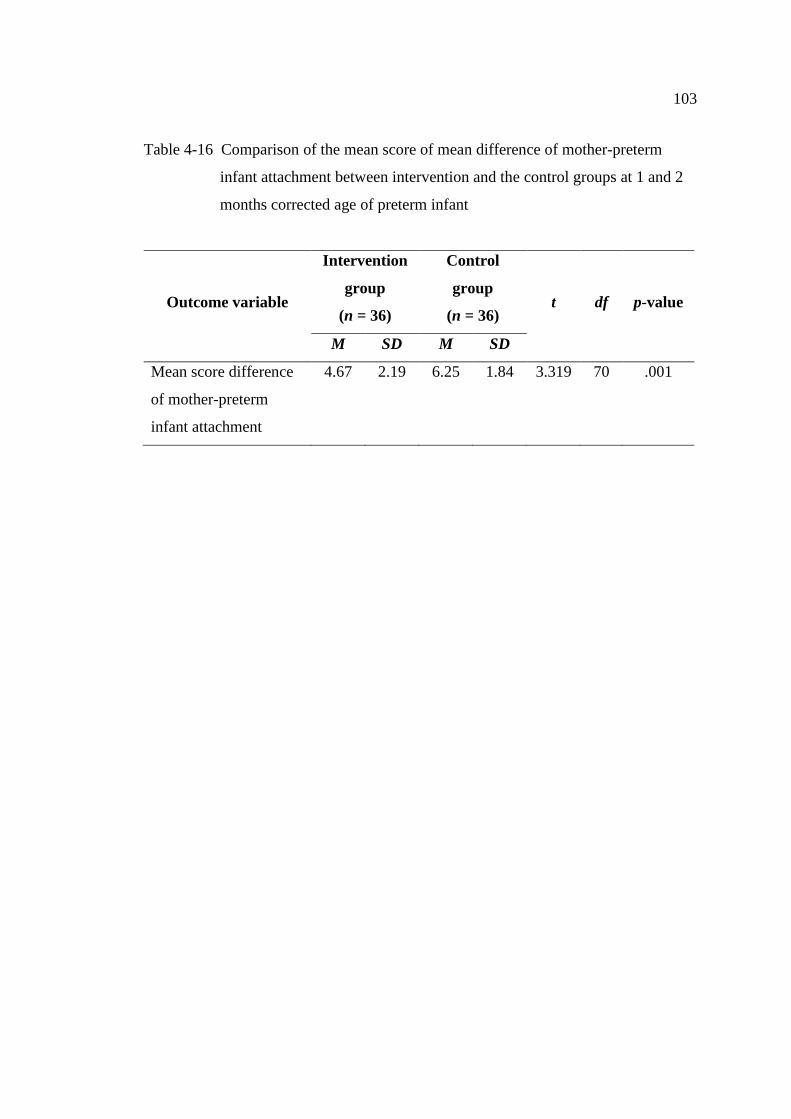
103
Table 4-16 Comparison of the mean score of mean difference of mother-preterm
infant attachment between intervention and the control groups at 1 and 2
months corrected age of preterm infant
Outcome variable
Intervention
group
(n = 36)
Control
group
(n = 36) t df p-value
M SD M SD
Mean score difference
of mother-preterm
infant attachment
4.67
2.19
6.25
1.84
3.319
70 .001

CHAPTER 5
CONCLUSION AND DISCUSSION
This chapter is presented in five parts. Firstly, a summary of the study that
included the developmental EMPAC program part and the examination the EMPAC
program on maternal stress, maternal attachment, and mother-preterm infant
attachment part. Secondly, discussion of the research findings will be presented.
Thirdly, strengths and limitations will be described. Fourthly, the implications for
nursing will be presented. Finally, the recommendations for future studies were be
presented.
Summary of the study
This study aimed to develop the maternal-preterm attachment intervention
and examine the effectiveness of the EMPAC program by comparing maternal stress,
maternal attachment, and maternal-preterm infant attachment between the control and
the intervention groups. A mixed method (embedded experimental model) was
employed to develop an intervention of the EMPAC program and test its effect on
maternal stress, maternal attachment, and mother-preterm infant attachment. The
study developed the intervention based on the theory of coaching and maternal infant
attachment, research evidences, clinical knowledge from 2 pediatricians and 5 nurses,
and 8 perspective of mothers in the context of families in Nakhon Phanom province,
Thailand. In addition, a pilot study was conducted to revise the intervention. After
that, this study tested the effective of the intervention by randomized control trial.
The effectiveness of the EMPAC program was verified at the pre-intervention,
discharge day of preterm infants, and 1 and 2 months corrected age of preterm infant.
The samples were 36 and 36 mother-preterm infant dyads in the control and the
intervention groups that were recruited who met the inclusion criteria, and the flipping
coin method was performed to randomly assign participants into control and
experimental group. Control group received the routine care; on the other hand,
experimental group received the EMPAC program.
Measurements were collected in both the control and intervention group by
using the parent stress scale [PSS: NICU] at pre-intervention, and discharge day of
105
preterm infant, parenting stress index-short form [PSI-SF] at 1 and 2 months corrected
age of preterm infant, maternal attachment inventory [MAI] at pre-intervention and
discharge day of preterm infant and 1 and 2 months corrected age of preterm infant,
and mother-infant attachment tool (MIAT) at 1 and 2 months corrected age of preterm
infant. The Cronbach alphas of PSS, PSI-SF, and MAI were .96, .98, and .80
respectively. The inter-rater reliability of MIAT was .90.
Testing similarity between the experimental and the control group used
independent t-test and chi-square test to compare in terms of demographic data,
maternal stress, and maternal attachment at pre-intervention. The examination of the
EMPAC program on maternal stress at hospital at pre-intervention, discharge day of
preterm infant, and maternal stress at home and mother-preterm infant attachment at
1 and 2 months corrected age of preterm infant used independent t-test to compare
between experimental and control group. The examination of the EMPAC program on
maternal attachment at pre-intervention, discharge day of preterm infant, and 1 and
2 months corrected age of preterm infant used repeated measures ANOVA to compare
between experimental and control group over time.
The research findings:
Part I: Developmental EMPAC program
This part is focused on the revising of the EMPAC program. Revisions were
made based on the perspective of mothers, nurses, and pediatricians. Then, a pilot
study was completed to test the feasibility, and acceptability of the intervention.
From the perspective of mothers and health care providers about attachment
between mothers and preterm infants that presented the attachment is important and
necessary for mothers and preterm infants since the first week in hospital. Mothers
need close interaction with their preterm infant. They need nurses to help them to
understand their infant’s behavior and how to attach to their preterm infants.
Moreover, nursing care for promoting attachment between mothers and preterm
infants needs to develop guidelines of nurses that will make sure that mother-preterm
infants have consistent and quality care for enhancing attachment. As results, mothers,
preterm infants, nurses, pediatricians, and family were factors that affect attachment
between mothers and preterm infants which showed the promoting and inhibiting
maternal attachment. “maternal attachment uncertainty” was expressed in the overall
106
temporal meaning of attachment with preterm infants. This theme had been
formulated from the six categories that consist of ‘affection of mothers as a root of
attachment’, ‘mothers need early help from nurses to promote attachment with
preterm infants’, ‘family support enhanced maternal confidence to attach preterm
infants’, ‘delay attachment, ‘mothers felt afraid to attach with preterm infants’, and
‘promoting attachment is important vs. ambiguous’.
The results of the pilot study showed that the admission period of preterm
infants in nursery unit was 7-33 days. Most of the preterm infants were admitted in the
nursery unit for less than 18 days. Therefore, the time period of the EMPAC program
should be completed before 2 weeks. Every participant accepted and was satisfied
with the EMPAC program; however, problems of program implementation were
reported that participants rejected the flip chart for recording maternal attachment
because they could not manage the time to do it.
As a result, the EMPAC program was revised to three sessions based on the
admission period time of preterm infants in nursery unit at Nakhon Phanom hospital,
and the suggestion of participants. The first session started on the second time of
mother visiting preterm infants. The second session was conducted on day 5 after the
first session. The third session was conducted on day 10 after the first session. In
addition, the program eliminated the flip chart of maternal attachment in this study
because it was not appropriate for participants. Moreover, the intervener gave the
chart desktop of mother-preterm infant attachment to mother at the first time when
start the intervention. Furthermore, the program involved family members in every
process of intervention because mothers had a high confidence to attach their preterm
infants when family members joined them in caring for their preterm infants.
Part II: Examination the effectiveness of EMPAC program
Mother and preterm infant characteristics between the control and the
experimental group were compared by using chi-square test for categorical data and
independent t-test for continuous data to determine their differences. No significant
differences were found between groups at pre-intervention. Then, two-way repeated
measures ANOVA was used to test hypotheses. The results showed that:
1. Mothers who received the EMPAC program have significantly lower
mean scores of the maternal stress at hospital on the discharge day than those who did

107
not received. The EMPAC program could decrease maternal stress in hospital.
2. Mothers who received the EMPAC program have significantly lower
mean scores of the maternal stress at home on 1 month corrected age of preterm
infants than those who did not received. The EMPAC program could decrease
maternal stress on 1 month corrected age of preterm infant. However, when compared
the mean score difference from 1 to 2 months corrected age of preterm infant,
it founded that maternal stress in the control group was faster decreased than in the
intervention group. It represented the effect of EMPAC program maintained to
decrease maternal stress until 1 months corrected age of preterm infants when they
came back to home.
3. Mothers who received the EMPAC program have significantly higher
mean scores of the maternal attachment overtime on the discharge day, and 1 and
2 months corrected age of preterm infants than those who did not received.
The EMPAC program could enhance maternal attachment at hospital, and maintain to
increase maternal attachment until 2 months corrected age of preterm infant.
4. Mothers who received the EMPAC program have significantly higher
mean scores of the maternal-preterm infant attachment on 1 month corrected age of
preterm infants than those who did not received. However, when compared the mean
score difference from 1 to 2 months corrected age of preterm infant, it founded that
mother-preterm infant attachment in the control group was faster increased than in the
intervention group.
Discussion of the research findings
The study findings of the effectiveness of the program will be discussed on
each outcome variable (maternal stress, maternal attachment, and mother-preterm
infant attachment) as follows:
Maternal stress
Maternal stress occurs when mother can not cope with a perceive threat of
preterm infant birth (Howland, 2007). Maternal stress is an important factor inhibiting
attachment process (Schenk et al., 2005). Mothers of preterm infants indicated lights
and sounds in the NICU and nursery unit, the preterm infant’s appearance, her
relationship with her preterm infant, and the enactment of her maternal role were
108
related to feeling of stress (Miles et al., 1993). Inability to read the preterm infant’s
cues, fear of medical equipments and the uncertain environment in the hospital
increased maternal stress (Miles et al., 1993; Shin et al., 2008). All of these conditions
of the hospitalization of preterm infants are the stressful situation for mothers (Engler,
2005). Mothers reported high levels of stress from preterm infant birth because they
had high level of suffering (Howland, 2007). In addition, the delivery of a preterm
infant may place the family at significant risk for chronic stress arousal (Howland,
2007). Mother needed to receive emotional support (Walker, 1992).
The results of this study showed that mothers who received the EMPAC
program could decrease maternal stress in hospital better than those who received
only the routine care. The results founded the mean of time lap between the end of the
intervention and discharge day in this sample was 12 days. However, the maternal
stress in hospital of the intervention group steadily decreased after the intervention at
discharge day of preterm infant from before intervention. On the other hand, the mean
score of maternal stress in hospital of control group slowly decreased. Although
maternal stress score can decrease over time like the control group, the intervention
group decline faster decreased than control group.
The EMPAC program started with the step of creating a trusting relationship
from first time mothers were visited. This step built mutual trust with the mother that
will make mother relaxation and open mind with nurse. Mutual trust between nurse
and patient is beginning with a positive mind set, and demonstrating thoughtful and
kindness that demonstrate the importance of the relationship (Kowalski & Casper,
2007). Second step understood the context of attachment. The nurse encouraged the
mother to express her feelings about situation of her preterm infant to help mother
understand her feelings and her problems in this situation. Nurse had a deep listening
and compassion with a nonjudgmental attitude about the mother belief and experience
that will make nurse understanding this situation of maternal stress. In the process of
this step founded that most of mother stress about the health and illness (H) of preterm
infants, and equipment (E) in unit in first session. Then, most of them stress about the
behavior (B) of preterm infant in session 2. In session 3, most of them stress about the
method to enhance positive attachment (A) with preterm infants. Therefore, total
stresses of mother are HEAB. Third step was setting realistic expectation. This step
109
will encourage mother to set the goal and plan for solving the problem in step 2.
Fourth step was supporting information and emotion. The teaching mothers about
recognizing infant’s disorganization/ stress cues, responding to infant’s cues, principle
during care, and interaction at hospital for promoting attachment that can decreased
maternal stress (Newnham et al., 2009). Mother will learn and clear understanding
about the kind of stress in hospital (HEAB) that made them understand and declining
the stress. The last step was reflecting & evaluating. This step will give the positive
reinforcement when mother feedback her changing of stress. Most of mothers stated
that they are understand this situation of HEAB in preterm infant and decreasing
stress about it.
When preterm infants came back home, maternal stress at home between
groups were significantly different at 1 month corrected age of preterm infant.
The results found that mothers who received the EMPAC program had lower score of
maternal stress at home than those who did not receive. However, when compared the
mean score difference from 1 to 2 months corrected age of preterm infant, it founded
that maternal stress in the control group was faster decreased than in the intervention
group. It represented the effect of EMPAC program maintained to decrease maternal
stress until 1 months corrected age of preterm infants when they came back to home.
In addition, the EMPAC program involved fathers or grandfathers in every
process of the program that decreased the maternal stress because the family support
is a one social support that may act directly to promote health regardless of person's
level of stress by protecting persons from the effects of stress (Walker, 1992). Family
support could be decreased maternal stress of mothers who had preterm infants in post
partum period because mothers felt warm when their husband visited baby with them
at hospital. Moreover, half of the Thai children are cared by the extended family with
whom they share a home (Chaimongkol, 2012). Results from phase I founded that
most of grandmothers planned to help the mothers care for their preterm infants at
home. This type of support may increase self-confidence of mothers to attach with
preterm infants and decreasing maternal stress. It’s verifying that EMPAC program
has effectiveness to decrease maternal stress.
110
Maternal attachment
Maternal attachment refers to the perception of affection tie that a mother
feels toward her infant. This was reflected a developing growth of positive feelings on
the part of the mother toward her infant, and included such dimensions as wanting to
possess, to prolong, or to seek contact, and to be proud of and to love her infant that
developed through their interactions (Carson & Virden, 1984; Gottlieb, 1978). Klaus
and Kennell (1982) found that the immediate contact after birth and the contact at the
first three postpartum days are associated with the increase score of maternal
attachment. The results founded that separation time between mothers with preterm
infants after birth was two days and 10 hours in the intervention group, and two days
and five hours in the control group. As both groups did not contact at the first three
post partum days, the maternal attachment will difficult to increasing.
The results showed that mothers who received the EMPAC program
reported stronger maternal attachment than those who did not receive. In addition,
the maternal attachment in the intervention group increased steadily from the
pre-intervention to 2 months corrected age of preterm infant. Moreover, the EMPAC
program could increased maternal attachment at 2 months corrected age of preterm
infants was higher than those at 1 month corrected age of preterm infant, discharge
day of preterm infant, and pre-intervention, respectively. It represented that the effect
of EMPAC program maintained to increased maternal attachment until 2 months
corrected age of preterm infants.
The EMPAC program encouraged mothers to interacted (eye contact &
speak & touch [EST]) with preterm infants when preterm infants are in a state of alert
behavior. Mother learned about the preterm infant’ cures, behavioral state when
preterm infant expressed the signal. In addition, mother learned the appropriate
strategies to response her preterm infant’s cue when she interact with her preterm
infant. It represented that maternal-infant interaction included promoting the process
of relationship creation between the mother and the infant during the postpartum
period (Trisayaluk, 1999) that help mother to develop her caregiver system (George &
Solomon, 1999). Mother learn to develop her caregiver system when her interact with
her child which consider a balance between her need to protect and care for her child
(George & Solomon, 1999). This process to develop caregiver system of mother could

111
especially important component to enhance maternal attachment for mother of
preterm infant. If mothers have more positive interaction with preterm infants, they
will have more maternal attachment (Bowlby, 1969; Klaus & Kennell, 1982).
Mother-preterm infant attachment
Mother-infant attachment is a reciprocal process that occurs mutually
between mother and infant. The infant receives warmth, feeding, and security from
the mother’s behavior. The mother accepts the responsibility for the infant’s care and
responds to the child’s need. In return, she receives enjoyment and establishes her
identity as a mother. Both benefit from the formation of an irreplaceable linkage
continuing long after the child ceases to be dependent (Murray & McKinney, 2010).
Therefore, the mother-infant attachment process is a development of attachment
between mother with infant since post-partum and gradually develops throughout the
time and last long in people's life.
The results found that mothers who received the EMPAC program had
higher scores of mother-preterm infant attachment than those who did not receive at
1 and 2 months corrected age of preterm infant. However, when compared the mean
score difference from 1 to 2 months corrected age of preterm infant, it founded that
mother-preterm infant attachment in the control group was faster increased than in the
intervention group. It represented the effect of EMPAC program could maintain to
increase mother-preterm infant attachment until 1 months corrected age of preterm
infants when they came back to home.
The EMPAC program prepared mothers to understand preterm infant
behavior and trained to promote attachment for preterm infant since the second time
visiting her preterm infant at hospital. Therefore, when mothers took care for preterm
infants at home, they had a ready to attach her preterm infant in the positive
attachment. Besides, preterm infants received the positive attachment from their
mother since they admitted in nursery unit that will make them learn to attach
mothers. It’s a reciprocal way that occurs in both directions between the mother and
the infant that is mother-preterm attachment (Murray & McKinney, 2010).
In addition, giving information and responding the question that depends on need of
the mother will help the mother learning and understanding the preterm infant’s cues,
behavioral state, attachment for the preterm infant (Charoensri, 2002; Newnham et al.,
112
2009; Trisayaluk, 1999). As a result, the mother-preterm attachment in the
intervention group has a higher score more than control group.
In addition, the last step of EMPAC program in every session (3 times)
applied video-feedback to facilitate mother’ sense of self as a good caregiver, and
understanding of her preterm infant behavior. The video-feedback helped mother to
improve her attachment behavior during interact with preterm infant since it made her
understand her changing of attachment behavior. In addition, when the mother saw the
video-feedback her will learn towards the preterm infant’s cues and how to respond
preterm infant’s cues as well. It confirms that the video-feedback could promote
maternal sensitivity that led to improve mother-preterm infant attachment
(Kalinauskiene et al., 2009). Besides, maternal sensitivity contributed to predict of
infant attachment as well (Chaimongkol, 2012). Moreover, most of mothers said that
the chart desktop of attachment for preterm infants help them to remember towards
attachment for their preterm infants, and stimulate them when they sew this chart
desktop. It affected their behaviors. When they attached preterm infant every day,
it automatically engaged to the daily life. It seem chart desktop could remind the
mothers to attachment mother with her preterm infants, and how to connect with their
babies in atypical environment. Furthermore, the family member was invited to join in
every step of the EMPAC program. This study founded that most of family member
who join this program was father that enhances the relationship between couple.
Marital relationship was significant predictor of the maternal-infant attachment. It
could predict 13.3 % of variance in maternal-infant attachment (Soakeaw, 2007).
This could explain that marital relationship might help the mother feel that they were
loved and cared to their preterm infant (Soakeaw, 2007). Thus, they could extend their
love and care to their preterm infant. It was congruent with Klaus and Kennell (1982).
They stated the most important factor that affects the maternal-infant attachment was
marital relationship because spouse was the best supporter.
According to the nursing coaching model the nurse coach-patient
relationship shifts expected pattern of patient as “passive” to patient as “dynamic.”
In a coaching paradigm, researcher coach acknowledges the patient as the expert
(Hess et al., 2013). Researcher coaches transition from directing, anticipating, fixing,
and controlling to appreciating and facilitate. Researcher is not qualified to determine

113
the next best step for mothers. Researcher become adept at staying in the moment,
relinquishing any illusion of control, become comfortable with not knowing, and trust
that self-selected goals and actions of mothers are integral to their self-development
and learning. As the researcher recedes into a supporting role, the mothers can shift
into the expert role (Bark & Conrad, 2015) which outcome can change thoughts,
feeling, and behavior (Kowalski & Casper, 2007). Also, when the mother of a preterm
infant understand this situation, self-selecting goal, planning and implementing the
strategies to promote attachment by herself, and evaluating and understanding her
attachment behavior and infant’s cues that will made mother learn and improve self-
development of attachment role. In addition, the chart desktop of mother-preterm
infant attachment has a concept of CARE attachment (correct attachment, appropriate
attachment, right time attachment, and early attachment) with is important content to
promote the process of relationship creation between the mother and the infant during
postpartum period. The chart desktop shows the interaction of both the mother to the
child (touch, eye-to-eye contact, high-pitched voice, entrainment, and heat), and the
infant to the mother (eye-to-eye contact, cry, entrainment). The quality interaction
between mothers with preterm infant will enhance maternal attachment and mother-
preterm infant attachment (Klaus & Kennell, 1982). If mother and preterm infant have
more positive interaction, they will increase attachment overtime.
Strengths and limitations
The strengths of this study should acknowledge three essential points.
Firstly, the EMPAC program was developed based on the scientific knowledge
(theories and research evidences), clinical knowledge (perspective of health care
providers), and belief and experience of participant perspective (perspective of
mothers). The EMPAC program was effective for decreasing maternal stress, and
increasing mother-preterm infant attachment until 1 month corrected age of preterm
infant. In addition, the EMPAC program could enhance maternal attachment overtime
up to 2 months corrected age of preterm infants. Because it was congruent with
beliefs, competency, and context of mothers. Therefore, the EMPAC program is
efficacious, effective, participant-focused, and appropriate to health service delivery
process (Whittemore & Grey, 2002). Secondly, this study applied the randomized
114
control trial [RCT] or a true experiment to test the effectiveness of the EMPAC
program. This design is the strongest type of the intervention study for testing cause
and effect relationships. This study applied the three components required in the true
experiment that consisted of an intervention or treatment, a comparison or control
group for prevention threat of maturation, and random assignment of participants to
experimental or control group for prevention threat of history, and threat of selection
(Melnyk & Morrison-Beedy, 2012). Thirdly, this study had a single blind from the
research assistances who collected the data. They were not exposed to any
intervention components and function. Thus, they did not know participants who
received the EMPAC program versus who did not receive. This helps for protecting
the bias. It showed that this study had a design to address threats to internal validity.
It will be better equipped to design and conducted degree of confidence in
scientifically rigorous intervention study (Melnyk & Morrison-Beedy, 2012).
Limitation of this study was treat of data contamination may be occurred
because some cases of participants of both groups were visiting preterm infants at the
same time. Although researcher separate the mother of experiment group in the
separating room when implement the EMPAC program, the communication between
both groups might. In addition, nurses might saw these techniques, and could have
used these techniques with the control group mothers.
Suggestions and recommendations
The EMPAC program is an appropriate early nursing intervention for
mothers having preterm infants that can decrease maternal stress in hospital, and still
decrease maternal stress at home and enhance mother-preterm infant attachment until
1 month corrected age of preterm infant. Moreover, it can enhance maternal
attachment until 2 months corrected age of preterm infant. Additionally, the findings
will serve to affirm results of the experiment with EMPAC program which represents
a new, innovative, and effective approach to changing attachment feeling and
perception of mother, and attachment behavior of mothers and preterm infants.
Therefore, this study gains more knowledge about promoting attachment between
mothers and preterm infants. Moreover, this study confirms that the best intervention
should be created not only from theory or research evidence, but also integrate with
115
perspective of health care providers, belief, and experience, and competency of
participants that will be appropriate with the setting and real situation, and effective
for changing the outcomes.
Implication for nursing practice
The EMPAC program can decrease maternal stress, and enhance maternal
attachment and mother-preterm infant attachment. Also, the EMPAC program can
maintain effect until 2 months corrected age of preterm infants for maternal
attachment, and maintain effect until 1 month corrected age of preterm infants for
maternal stress and mother-preterm infant attachment. Therefore, this program should
be implemented for decreasing maternal stress and enhancing maternal attachment
and mother-preterm infant attachment in hospital and intermediately time at home.
Nurse professional can apply EMPAC program for caring mothers and their preterm
infants in the nursery unit or sick newborn unit in the early state after preterm infant
birth. It will benefit for mothers and preterm infants to develop better attachment and
may benefit for maternal confident, attachment security, and development of preterm
infants continuously.
The EMPAC program conducted three sessions per 10 days. The first
session started on mothers’ second visit to their preterm infants. The program was not
done on the first visit because mothers needed to get to know and experience their
preterm infant before starting the intervention. Therefore, the first visit was a
preparation time for mothers. The second session was conducted 5 days after the first
session. The Third session was conducted 10 days after the first session. There were
five stages in each session which were presented in Appendix 10. The followings
were necessary components and features to apply EMPAC program.
1. First session was very important to open mothers and their family’s mind.
Nurses should express their emotion honestly, respectfully, friendly, and
compassionately. Besides, nurses should keep the emotional expression through all
stages of EMPAC program.
2. Techniques to develop a quick trust with mothers were to remember their
names, their husbands’, their babies’, and communicate with their native languages or
dialects. In this setting, most of participants communicated in Thai-Lao language
which was one of the ethnic group languages in the setting area.
116
3. At stage 2, nurses should use the close-ended questions mixing with the
open-ended questions to help mothers understand the situation of preterm birth in
view of Thai culture. If nurses used only open-ended questions, nurses would find that
mothers could not answer anything. It was difficult for them to ask any questions
because most of them had not had experience or did not know what situation they
were being in. In addition, the situation of preterm infant made it difficult for mothers
to express their fears and concern about the current conditions, and the future
development of the preterm infant (Sannino et al., 2011)
4. At stage 3 (setting realistic expectation) and stage 5 (reflecting and
evaluating), fathers were key persons to help mothers set the goal and plan to attach
with their preterm infants. Nurses should facilitate involvement of the fathers in
caring for their preterm infants. This study found that the fathers were the persons
who prepared for all appliances for preterm infant care such as food and beverages for
mothers. They also helped mother out with the infants when she was tired. On top of
that, they handled all documents of and for the hospital. Moreover, when dads and
moms took care of the preterm infants together, they would advise each other and that
was the best development of building attachment with their babies. This constructed
self-development in roles of mothers and fathers.
5. At stage 4, supporting information and emotion. Nurse should play a role
of the informational and emotional supporters to support the mothers. Each mother
had different needs. It required an individual approach for giving information and
emotional support to mother. However, nurse should support information using chart
desktop of mother-preterm infant attachment because it was made easy for mothers to
understand.
6. The appropriate time to apply EMPAC program into each session was
after bathing time because it was an active and alert state of preterm infants. It was the
best and easiest time for mothers to learn and interact with their preterm infants.
Nurses could help complete each session in a short time to have benefit outcome.
7. Technique of video records. Before asking mothers to sign consent forms
for clear understandings, nurse should allow mothers to record video of themselves
and their babies when they were together in nursery unit. Nurse should do a long
video record, then selected some good shots of interaction between mothers and their

117
preterm infants for discussion with mothers and their families in stage 5. Doing so,
nurse would get natural and real interaction from them. In this study, the researcher
set up a video record of 1 hour before bathing time until 1 hour after bathing time.
Furthermore, if nursery unit had a close circuit camera, it would be easy to select the
shot of interactions between mothers and their babies.
Implication for nursing research
The further researchers should to monitor the response of attachment
behavior between mothers and preterm infants over 6 and 12 months in order to
examine the sustainable effects of the EMPAC program. In addition, the EMPAC
program could guide to modify for promoting attachment, and test in other kinds of
infants. Furthermore, the future researches should examine the EMPAC program in
other setting in other parts of Thailand or other countries for confirmation that
EMPAC program can be generalized in difference cultures.
REFERENCES
Abidin, R. R. (1990). Parenting stress index-short form: Test manual.
Charlottesville, Virginia: Pediatric Psychology Press.
Abidin, R. R. (1995). Parenting stress index (3rd
ed.). Odessa, Florida: Psychological
Assessment Resources.
Ainsworth, M., Blehar, M., Waters, E., & Wall, S. (1978). Patterns of attachment.
New Jersey: Erlbaum.
Als, H. (1982). Toward a synactive theory of development: Promise for the
assessment and support of infant individuality. Infant Mental Health
Journal, 3(4), 229-243.
Apichaiyawat, S., Lamchang, S., & Yenbut, J. (2010). Effects of coaching on care
practices among parents of children with pneumonia. Nursing Journal,
37(3), 49-61.
Bakermans-Kranenburg, M. J., van IJzendoorn, M. H., & Kroonenberg, P. M.
(2004). Differences in attachment security between African-American and
white children: Ethnicity or socio-economic status?. Infant Behavior &
Development, 27, 417-433.
Bark, L., & Conrad, S. (2015). Nurse coaching is not what I do: It informs who I am.
Beginnings, 35(4), 18-20.
Barnard, K. E., & Kang, R. (1987). State modulation. In N. Johnson-Crowley, &
G. A. Sumner (Eds.), Concept manual: Nursing system toward effective
parenting-preterm (pp. 61-88). Seattle, Washington: NCAST.
Belsky, J. (1993). Etioligy of child maltreatment: A developmental ecological
analysis. Psychological Bulletin, 114(3), 413-434.
Belsky, J. (1999). Interactional and contextual determinants of attachment security.
In J. Cassidy, & P. R. Shaver (Eds.), Handbook of attachment: Theory,
research, and clinical applications (pp. 249-264). New York: The Guilford
press.
Bialoskurski, M., Cox, C., & Hayes, J. A. (1999). The Nature of attachment in a
neonatal intensive care unit. The Journal of Perinatal and Neonatal
Nursing, 13(1), 66-77.
119
Borghini, A., Pierrehumbert, B., Miljkovitch, R., Muller-Nix, C., Forcada-Guex, M.,
& Ansermet, F. (2006). Mother’s attachment representations of their
premature infant at 6 and 18 months after birth. Infant Mental Health
Journal, 27(5), 494-508.
Bowlby, J. (1969). Attachment. New York: Basic book.
Bowlby, J. (1982). Attachment and loss: Volume 1 attachment (2nd
ed.). New York:
Basic Books.
Browne, J. V. (2003). New perspectives on premature infants and their parents. Zero
to Three, 24(2), 4-12.
Burn, N., & Grove, S. (2005). The practice of nursing research: Conduct, critique,
and utilization (5th
ed.). Missouri: Elsevier Saunders.
Carson, K., & Virden, S. (1984). Can prenatal teaching promote maternal
attachment? Practicing nurses test Carter-Jessop's prenatal attachment
intervention. Health Care for Women International, 5, 355-369.
Cassidy, J., & Shaver, P. R. (1999). Handbook of attachment: Theory, research, and
clinical applications. New York: The Guilford press.
Chaimongkol, N. (2012). Mother-child attachment in Thailand: A review article.
Journal of Science, Technology, and Humanities, 10(2), 73-79.
Charoensri, P. (2002). Effects of multi-modalities sensory stimulation program on
the growth of premature infants and maternal infant attachment. Master's
thesis, Pediatric Nursing, Faculty of Graduate Studies, Mahidol
University.
Chawaphanth, S. (2006). Effects of cycled lighting on heart rate in preterm infants:
Comparing the use of standard and individual heart rate criteria.
International Journal for Human Caring, 10(2), 25.
Chiu, S. H., & Anderson, G. C. (2009). Effect of early skin-to-skin contact on
mother-preterm infant interaction through 18 months: Randomized
controlled trial. International Journal of Nursing Studies, 46, 1168-1180.
Christensen, L. B. (2007). Experimental methodology (10th
ed.). Boston: Pearson.
Cohen, J. (1998). Statistical power analysis for the behavioral sciences (2nd
ed.).
Hillsdale, NJ: Erlbaum.
120
Cook, M. J., & Poole, L. (2011). Effective coaching (2nd
ed.). New York: McGraw-
Hill.
Corriveau, K. H., Harris, P. L., Meins, E., Fernyhough, C., Arnott, B., Elliott, L.,
Liddle, B., Hearn, A., Vittorini, L., & Rosnay, M. D. (2009). Young
children’s trust in their mother’s claim: Longitudinal links with attachment
security in infancy. Child Development, 80(3), 750-761.
Creswell, J. W., & Plano Clark, V. P. (2007). Designing and conducting: Mixed
methods research. Thousand Oaks: Sage.
Creswell, J. W., & Plano Clark, V. P. (2011). Designing and conducting: Mixed
methods research. Los Angeles: SAGE.
Danerek, M., & Dykes, A. K. (2008). A theoretical model of parents’ experiences of
threat of preterm birth in Sweden. Midwifery, 24(4), 416-424.
DeCasper, A. J., & Fifer, W. P. (1980). Of human bonding: Newborns prefer their
mothers voices. Science, 208, 1173-1176.
Di Lorio, C. K. (2005). Measurement in health behavior: Methods for research and
education. San Francisco: Jossey-Bass A Wiley imprint.
DiVitto, B., & Goldberg, S. (1979). The effects of newborn medical status on early
parent-infant interaction . In T. Field, A. Sostek, S. Goldberg, &
H. Shuman (Eds.), Infant born at risk (pp. 311-332). New Delhi: SAGE.
Engler, A. J. (2005). Maternal stress and the white coat syndrome: A case study.
Pediatric Nursing, 31(6), 470-473.
Feldman, R., Weller, A., Sirota, L., & Eidelman, AI. (2003). Testing a family
intervention hypothesis: The contribution of mother-infant skin-to-skin
contact (kangaroo care) to family interaction, proximity and touch.
Journal of Family Psychology, 17(1), 94-107.
Fish, H., & Stifter, C. A. (1995). Patterns of mother-infant interaction and
attachment: A cluster-analytic approach. Infant Behavior & Development,
18, 435-446.
Ford-Gilboe, M., Campbell, J., & Berman, H. (1995). Stories and numbers:
Coexistence without compromise. Advances in Nursing Science, 18(1),
14-26.
121
George, C., & Solomon, J. (1999). Attachment and caregiving: The caregiving
behavioral system. In J. Cassidy, & P. R. Shaver (Eds.), Handbook of
attachment: Theory, research, and clinical applications (pp. 649-670).
New York: The Guilford press.
Goldberg, S. (2000). Attachment and development. London: Arnold.
Gottlieb, L. (1978). Maternal attachment in primiparas. Journal of Obstetric,
Gynecologic, and Neonatal Nursing, 7, 39-44.
Goulet, C., Bell, L., Tribble, D. S., Paul, D., & Lang A. (1998). A Concept analysis
of parent-infant attachment. Journal of Advanced Nursing, 28(5), 213-218.
Guba, E. C. (1990). The paradigm dialog. California: SAGE.
Haney, P., & Durlak, J. A. (1998). Changing self-esteem in children and
adolescents: A meta-analytical review. Journal of clinical Child
Psychology, 27(4), 423-433.
Heinicke, C. M., & Guthrie, D. (1992). Stability and change in husband-wife
adaptation and the development of the positive parent-child relationship.
Infant Behavior and Development, 15, 109-127.
Hess, D. R., Dossey, B. M., Southard, M. E., Luck, $., Schaub, B. G., & Bark, L.
(2013). The art and science of nurse coaching: A provider’s guide to
coaching scope and competencies. Maryland: Silver Spring. Howland, L. C. (2007). Preterm birth: Implications for family stress and coping.
Newborn and Infant Nursing Review, 7(1), 14-19.
Inwongwan, C., Lamchang, S., & Thanasuwan, W. (2008). Stressors among mothers
of premature infants in transition period from hospital to home. Nursing
Journal, 35(4), 98-107.
Johnson, S., Whitelaw, A., Glazebrook, C., Israel, C., Tumer, R., White, I. R.,
Croudace, T., Davenport, F., & Marlow, N. (2009). Randomized trial of
a parenting intervention for very preterm infants: Outcome at 2 years.
The Journal of Pediatrics, 155(4), 488-494.
Johnson-Crowley, N., & Sumner, G. A. (1987). Nursing systems toward effective
parenting-preterm. Seattle, WA: NCAST.
122
Jongkae, J., Thaiyapirom, N., & Soontornchai, P. (2008). Effect of information and
emotional support on uncertainty in illness of mothers with premature
Infant. Nursing Journal, 35(1), 56-67.
Jongpranee, P. (1997). Selected factors, social support and maternal newborn
attachment in adolescent mothers. Master's thesis, Maternity and Newborn
Nursing, Faculty of Graduate Studies, Mahidol University.
Kalinauskiene, L., Cekuoliene, D., Van IJzendoorn, M. H., Bakermans-Kranenburg,
M. J., Juffer, F., & Kusakovskafa, I. (2009). Supporting insensitive
mothers: The Vilnius randomized control trial of video-feedback
intervention to promote maternal sensitiviry and infant attachment security.
Child: Care, Health and Development, 35(5), 613-623.
Kinsey, C. B., & Hupcey, J. E. (2013). State of the science of maternal-infant
bonding: A principle-based concept analysis. Midwifery, 29(12), 1-14.
Klaus, M. H. (2009). Commentary: An early, short, and useful sensitive period in the
human infant. Birth, 36(2), 110-112.
Klaus, M. H., & Kennell, J. H. (1982). Parent-infant bonding. St. Louis: The C. V.
Mosby.
Korja, R., Maunu, J., Kirjavainen, J., Savonlahti, E., Haataja, L., Lapinleimu, H.,
Manninen, H., Piha, J., & Lehtonen, L. (2008). Mother-infant interaction is
influenced by the amount of holding in preterm infants. Early Human
Development, 84(4), 257-267.
Korja, R., Savonlahti, E., Haataja, L., Lapinleimu, H., Manninen, H., Piha, J., &
Lehtonen, L. (2009). Attachment representations in mothers of preterm
infants. Infant Behavior & Development, 32(3), 305-311.
Korja, R., Ahlqvist-Bjorkroth, S., Savonlahti, E., Stolt, S., Haataja, L., Lapinleimu,
H., Piha, J., & Lehtonen, L. (2010). Relations between maternal attachment
representations and the quality of mother-infant interaction in preterm and
full-term infants. Infant Behavior & Development, 33(3), 330-336.
Kowalski, K., & Casper, C. (2007). The Coaching process: An effective tool for
professional development. Nursing Administration Quarterly, 31(2),
171-179.
123
Littleton, L. Y., & Engebretson, J. C. (2005). Maternity nursing care (2nd
ed.). New
York: Delmar Cengage Learning.
Lokham, C. (2003). The effect of mother providing premature infant massage
program on attachment and bonding between mother and preterm infants.
Master’s thesis, Public Health Nursing, Faculty of Graduate Studies,
Mahidol University.
Malekpour, M. (2007). Effects of attachment on early and later development.
The British Journal of Developmental Disabilities, 53(105), 81-95.
Mangelsdorf, S. C., Plunkett, J. W., & Dedrick, C. F., Berlin, M., Meisels, S. J.,
McHale, J. L, & Dichtellmiller, M. (1996). Attachment security in very low
birth weight infants. Development Psychology, 32(5), 914-920.
Mantymaa, M., Puura, K., Luoma, I., Salmelin, R., Davis, H., Tsiantis, J., Ispanovic-
Radojkovic, V., Paradisiotou, A., & Tamminen, T. (2003). Infant-motor
interaction as a predictor of child's chronic health problems. Child: Care,
Health and Development, 29(3), 181-191.
Marshall, C., & Rossman, G. B. (2006). Designing qualitative research (4th
ed.).
Thousand Oaks: Sage.
Marvin, R. S., & Brittner, P. A. (1999). Normative development: The ontogeny of
attachment. In J. Cassidy, & P. R. Shaver (Eds.), Handbook of attachment:
Theory, research, and clinical applications (pp. 44-67).New York:
Guilford Press.
Meijssen, D., Wolf, M-J., van Bakel, H., Koldewijn, K. K., Kok, J., & van Baar, A.
(2011). Maternal attachment representations after very preterm birth and
the effect of early intervention. Infant behavior & Development, 34(1),
72-80.
Melnyk, B. M., & Morrison-Beedy, D. (2012). Intervention research: Designing,
conducting, analyzing, and funding. New York: Springer.
Mercer, R. T. (2004). Becoming a mother versus maternal role attainment. Journal
of Nursing Scholarship, 36(3), 226-232.
Mercer, R. T., & Ferketich, S, L. (1994). Matenal infant attachment of experienced
and inexperienced mothers during infancy. Nursing Research, 43(6),
344-351.
124
Miles, S. M., Funk, S. G., & Carlson, J. (1993). Parental stressor scale: Neonatal
intensive care unit. Nursing Research, 42(3), 148-152.
Ministry of Public Health. (2011). Public health statistic. Retrieved from
http://bps.ops.moph.go.th/Healthinformation/statistic54/2.1.5_54.pdf
Muller, M. E. (1994). A questionnaire to measure mother-to-infant attachment.
Journal of Nursing Measurement, 2(2), 129-141.
Muller, M. E. (1996). Prenatal and postnatal attachment: Model correction. Journal
of Gynecology and Neonatal Nursing, 25, 161-166.
Murray, S. M., & McKinney, E. S. (2010). Foundations of maternal newborn and
women’s health nursing (5th
ed.). Missouri: Elsevier.
Nakhon Phanom hospital. (2011). Medical record. Nakhon Phanom: Nakhon
Phanom hospital.
Newman, M. A. (1992). Prevailing paradigms in nursing. Nursing Outlook, 40(1),
10-32.
Newnham, C. A., Milgrom, J., & Skouteris, H. (2009). Effectiveness of a modified
mother-infant transaction program on outcomes for preterm infants from 3
to 24 months of age. Infant Behavior & Development, 32, 17-26.
Orapiriyakul, R., Jirapaet, V., & Rodcumdee, B. (2007). Struggling to get connected:
The process of maternal attachment to the preterm infant in the neonatal
intensive care unit. Thai Journal Nursing Research, 11(4), 251-264.
Page, M., Wilhelm, M. S., Gamble, W.W., & Card, N. A. (2010). A comparison of
maternal sensitivity and verbal stimulation as unique predictors of infant
social-emotional and cognitive development. Infant Behavior &
Development, 33, 101-110.
Palmer, S., Tubbs, I., & Whybrow, A. (2003). Health coaching to facilitate the
promotion of healthy behaviour and achievement of health-related goals.
International Journal of Health Promotion & Education, 41(3), 91-93.
Performance Coaching International. (2012). History of coaching. Retrieved
from http://www.performancecoachinginternational.com/resources/articles/
historyofcoaching.php
125
Phatthanasiriwethin, S. (2001). Attachment behaviors in mothers of premature
infant: A case study in Thai mothers. Master’s thesis, Maternal and Child
Nursing, Faculty of Graduate studies, Mahidol University.
Polit, D. F., & Beck, C. T. (2010). Essentials of nursing research: Appraising
evidence for nursing practice (7th
ed.). Philadelphia: Lippincott Williams &
Wilkins.
Price, A. (2009). Using coaching interventions to develop clinical skill. Nursing
Standard, 23(44), 48-55.
Reiser, S. L. (1981). A tool to facilitate mother-infant attachment. JOGN Nursing,
10(4), 294-297.
Rugolo, L. M. (2005). Growth and developmental outcomes of the extremely
preterm infant. Journal de Pediatric, 81(1), 101-110.
Ryan, F. Coughlan, M., & Cronin, P. (2009) Interviewing in qualitative research: the
one-to-one interview. International Journal of Therapy and Rehabilitation,
16(6), 309-314.
Sannino, P., Plevani, L., Bezze, E., & Cornalba, C. (2011). The ‘broken’ attachment
between parents and preterm infant: How and when to intervene. Early
Human Development, 875, 581-582.
Schenk, L. K., Kelley, J. H., & Schenk, M. P. (2005). Model of maternal-infant
attachment: A role for nurses. Pediatric Nursing, 31(6), 514-517.
Seaward, B. L. (2011). Essentials of managing stress. Boston: Jones and Bartlett.
Shadish, W. R., Cook, T. D., & Campbell, D. T. (2002). Experimental and quasi-
experimental designs for generalized causal inference. Boston: Houghton
Mifflin.
Shah, A. K. (2010). Parental stress in the neonatal intensive care unit in India.
Master’s thesis, Rehabilitation Science, Faculty of the Graduate School,
State University .
Shin, H., Park, Y.-J., & Kim, M. J. (2006). Predictors of maternal sensitivity during
the early postpartum period. Journal of Advanced Nursing, 55(4), 425-434.
Shin, H., Park, Y.-J., Ryu, H., & Seomun, G. A. (2008). Maternal sensitivity:
A concept analysis. Journal of Advanced Nursing, 64(3), 304-314.
126
Sitanon, T. (2009). Thai parents’ experiences of parenting preterm infants during
hospitalization in the neonatal intensive care unit. Doctoral dissertation,
Nursing Science, University of Washington.
Soakeaw, S. (2007). The influence of marital relationship, complications during
pregnancy, and separation time on maternal-newborn attachment in
postpartum mothers. Master’s thesis, Maternal and Newborn Nursing,
Faculty of Graduate studies, Mahidol University.
Suksawat, S., Lamchang, S., & Jintrawet, U. (2012). Effect of coaching on care
practice among parents. Nursing Journal, 39(4), 1-12.
Sunsaneeyanon, P. (1965). Health of preterm infant, knowledge, attitude and
behavior of child rearing of mother for preterm infant 0-6 months.
Master’s thesis, Maternal and Newborn Nursing, Faculty of Graduate
studies, Mahidol University.
Talmi, A., & Harmon, R. J. (2003). Relationships between preterm infants and their
parents: Disruption and development. Zero to Three, 24(2), 13-20.
Thabane, L., Ma, J., Rong, C., Cheng, J., Ismaila, A., Rios, L. P., Robson, R.,
Thabane, M., Giangregorio, L., & Goldsmith, C. (2010). A tutorial on pilot
studies: The what, why and how. BMC Medical Research Methodology,
10(1), 1-10.
Tiden, V. P. (1985). Issues of conceptualization and measurement of social support
in the construction of nursing theory. Research in Nursing and Health, 5,
199-206.
Tilokskulchai, F., Phatthanasiriwethin, S., Vichitsukon, K., & Serisathien, Y. (2002).
Attachment behaviors in mothers of preterm infants: A descriptive study in
Thai mothers. Journal of Perinatal and Neonatal Nursing, 16(3), 69-83.
Trisayaluk, T. (1999). Effects of maternal-infant interaction on maternal-infant
attachment and growth of premature infant. Master’s thesis, Maternal and
Newborn Nursing, Faculty of Graduate studies, Mahidol University.
Troy, N. W. (1995). The time first holding the infant and maternal self-esteem
related to felling of maternal attachment. Women and Health, 22(3), 59-72.
VandenBerg, K. A., & Hanson, M. J. (2013). Coming home from the NICU.
Maryland: Paul H. Brookes.
127
Vincent, A. E., & Birkhead, A. C. S. (2013). Evaluation of the effectiveness of nurse
coaching in improving health outcomes in chronic condition. Holistic
Nursing Practice, 27(3), 148-161.
Wacharasin, C., Thienpichet, S., & Deoisres, W. (2011). Predicting maternal stress
of mothers having children age 0-3 years. The Public Health Journal of
Burapha University, 6(1), 31-41.
Walker, L. O. (1992). Parent-infant nursing science: Paragigms, phenomena,
method. Philadelphia: F. A. Davis.
Whitmore, J. (2002). Coaching for performance: Growing people, performance and
purpose. London: Nicholas Brealey Publishing.
Whittemore, R. & Grey, M. (2002). The systematic development of nursing
interventions. Journal of Nursing Scholarship, 34(2), 115-120.
Whittemore, R., Melkus, G. D. E., Sullivan, A., & Grey, M. (2004). A nurse-
coaching intervention for women with type 2 diabetes. The Diabetes
Educator, 30(5), 795-804.
Wilinger, U., Diendorfer-Radner, Wilnauer, R., Jorgl, G., & Hager, V. (2005).
Parenting stress and parental bonding. Behavioral Medicine, 31(2), 63-72.
Wolke, D., Eryigit-Madzwamuse, S., & Gutbrod, T. (2014). Very preterm/ very low
birthweight infants’ attachment: Infant and maternal characteristics.
Archives of Disease in Childhood Fetal and Neonatal Edition, 99,
F70-F71.
Wong, D. L., Perry, S. E., Hockenberry, M. J., & Lowdermilk, D. L. (2006).
Maternal child nursing care. St. Louis: Mosby.
Woodhouse, S.S. (2010). Dyadic interactions as precursors to attachment security:
Implications for intervention and research. Attachment and Human
Development, 12(1-2), 151-157.
Wright L. M., & Bell J. M. (2009). Beliefs and illness: A model for healing. Calgary,
Alberta: 4th
Floor Press.
Wu, C-H. (2009). The relationship between attachment style and self-concept
clarity: The mediation effect of self-esteem. Personality and Individual
Differences, 47, 42-46.

128
Zeus, P., & Skiffington, S. (2005). The coaching at work toolkit: A complete guide
to techniques and practice. Sydney: McGraw-Hill.
APPENDICES

130
APPENDIX A
General information and interview guild about attachment
for mother of preterm infant
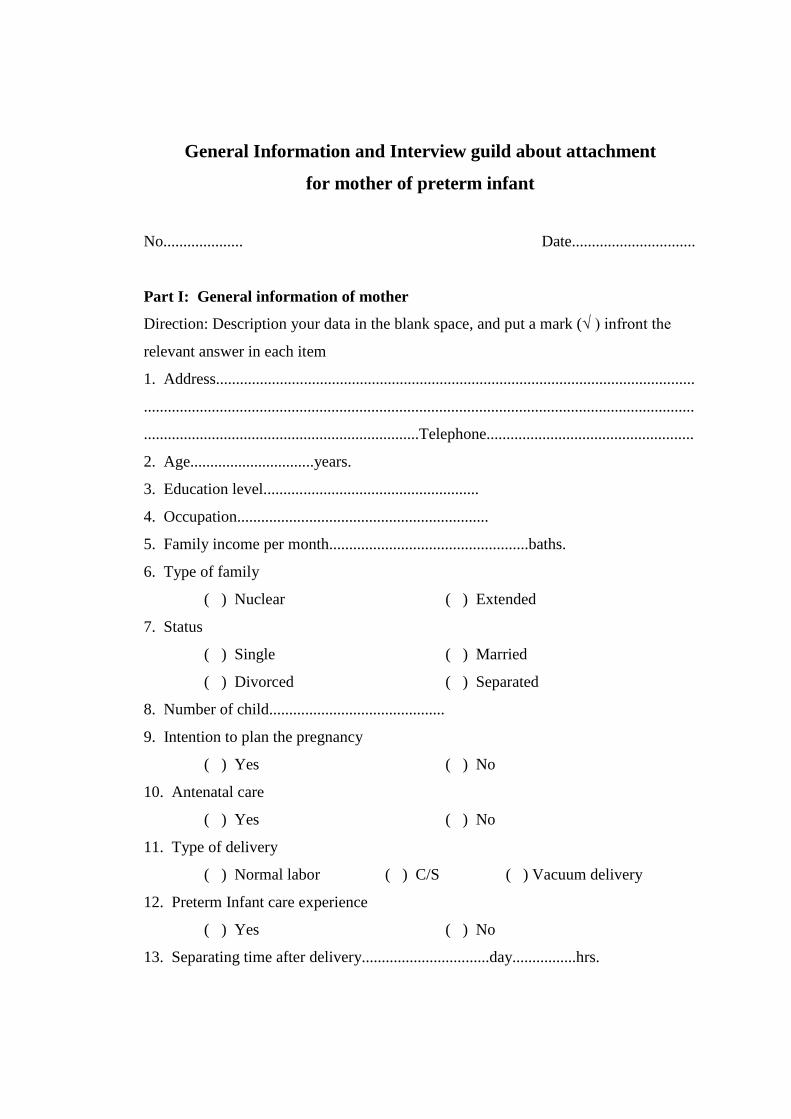
131
General Information and Interview guild about attachment
for mother of preterm infant
No.................... Date...............................
Part I: General information of mother
Direction: Description your data in the blank space, and put a mark (√ ) infront the
relevant answer in each item
1. Address........................................................................................................................
..........................................................................................................................................
.....................................................................Telephone....................................................
2. Age...............................years.
3. Education level......................................................
4. Occupation...............................................................
5. Family income per month..................................................baths.
6. Type of family
( ) Nuclear ( ) Extended
7. Status
( ) Single ( ) Married
( ) Divorced ( ) Separated
8. Number of child............................................
9. Intention to plan the pregnancy
( ) Yes ( ) No
10. Antenatal care
( ) Yes ( ) No
11. Type of delivery
( ) Normal labor ( ) C/S ( ) Vacuum delivery
12. Preterm Infant care experience
( ) Yes ( ) No
13. Separating time after delivery................................day................hrs.
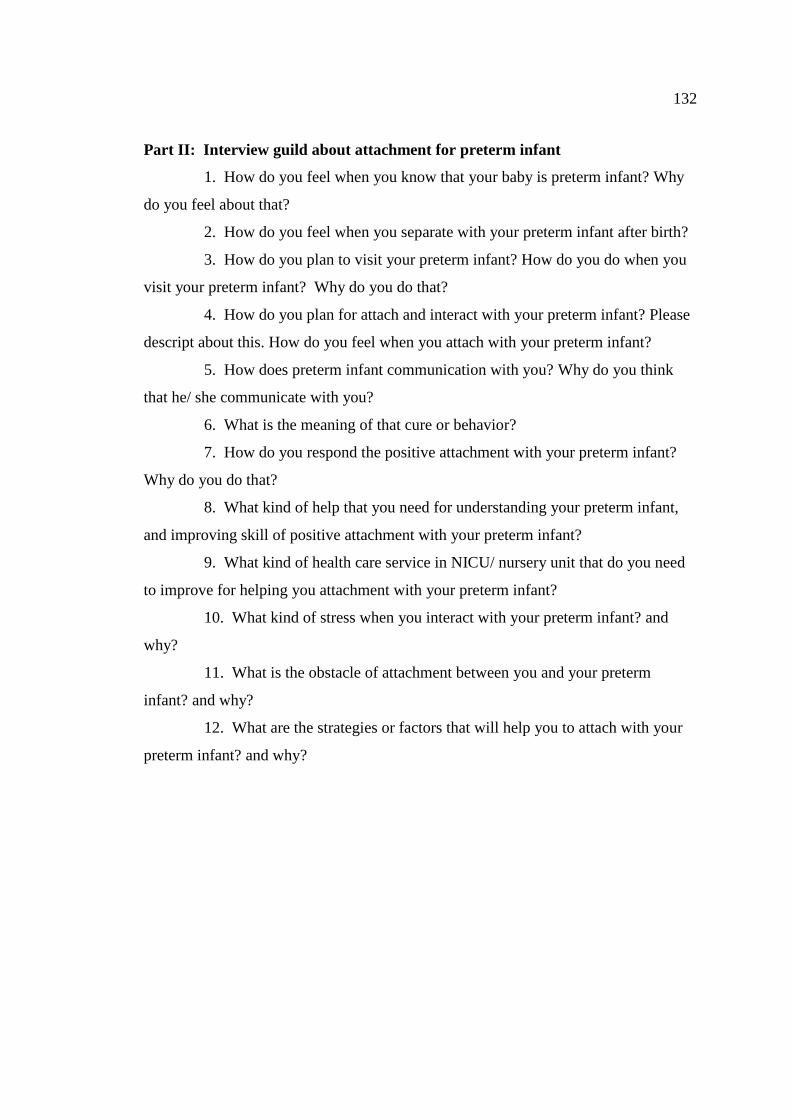
132
Part II: Interview guild about attachment for preterm infant
1. How do you feel when you know that your baby is preterm infant? Why
do you feel about that?
2. How do you feel when you separate with your preterm infant after birth?
3. How do you plan to visit your preterm infant? How do you do when you
visit your preterm infant? Why do you do that?
4. How do you plan for attach and interact with your preterm infant? Please
descript about this. How do you feel when you attach with your preterm infant?
5. How does preterm infant communication with you? Why do you think
that he/ she communicate with you?
6. What is the meaning of that cure or behavior?
7. How do you respond the positive attachment with your preterm infant?
Why do you do that?
8. What kind of help that you need for understanding your preterm infant,
and improving skill of positive attachment with your preterm infant?
9. What kind of health care service in NICU/ nursery unit that do you need
to improve for helping you attachment with your preterm infant?
10. What kind of stress when you interact with your preterm infant? and
why?
11. What is the obstacle of attachment between you and your preterm
infant? and why?
12. What are the strategies or factors that will help you to attach with your
preterm infant? and why?

APPENDIX B
General information and interview guild about attachment for nurses
in NICU & nursery, and pediatrician
134
General Information and Interview guild about attachment
for nurses in NICU or nursery unit
No.................... Date...............................
Part I: General information of nurses
Direction: Description your data in the blank space, and put a mark (√) in front the
relevant answer in each item.
1. Age............................years.
2. Education level...........................................................................
3. Period of experience of work in NICU and nursery unit
( ) < 5 years
( ) 5-10 years
( ) > 10 years
Part II: Interview guild for nurses about mother-preterm infant attachment
1. How do you think about attachment between mothers with preterm
infants.
2. What is nursing intervention from your experience that you use to
promote mother-preterm infant attachment?
3. How do you plan to improve nursing intervention for enhancing mother-
preterm infant attachment?
4. What are the important factors that can promote mother-preterm infant?
and why?
5. What are the important factors that can inhibit mother-preterm infant?
and why?
135
General Information and Interview guild about attachment
for pediatrician
No.................... Date...............................
Part I: General information of pediatrician
Direction: Description your data in the blank space, and put a mark (√ ) in front the
relevant answer in each item.
1. Age............................years.
2. Education level...........................................................................
3. Period of experience of work in NICU and nursery unit
( ) < 5 years
( ) 5 - 10 years
( ) > 10 years
Part II: Interview guild for pediatrician about mother-preterm infant
attachment
1. How do you think about attachment between mothers with preterm
infants.
2. What is nursing intervention from your experience that you use to
promote mother-preterm infant attachment?
3. How do you plan to improve nursing intervention for enhancing mother-
preterm infant attachment?
4. What are the important factors that can promote mother-preterm infant?
and why?
5. What are the important factors that can inhibit mother-preterm infant?
and why?

APPENDIX C
Mother and preterm infant's general information questionnaire
137
Mother and preterm infant's general information questionnaire
No.................... Date...............................
Part I: General information of mother
Direction: Description your data in the blank space, and put a mark (√ ) infront the
relevant answer in each item
1. Address........................................................................................................................
..........................................................................................................................................
.....................................................................Telephone....................................................
2. Age...............................years.
3. Education level......................................................
4. Occupation...............................................................
5. Family income per month..................................................baths.
6. Type of family
( ) Nuclear ( ) Extended
7. Status
( ) Single ( ) Married
( ) Divorced ( ) Separated
8. Number of child............................................
9. Intention to plan the pregnancy
( ) Yes ( ) No
10. Antenatal care
( ) Yes ( ) No
11. Type of delivery
( ) Normal labor ( ) C/S ( ) Vacuum delivery
12. Preterm Infant care experience
( ) Yes ( ) No
13. Separating time after delivery................................day................hrs.
14. The person who significant for your life that helps you to caring your preterm
infant..............................................................................................................................
138
Part I: General information of preterm infant
1. Date of birth..................................................Time....................................................
Sex................................................................Apgar score..........................................
Gestational age..............................................week........................day
2. Diagnosis..................................................................................................................
3. Growth
3.1 Birth
Body weight........................................grams
Length.................................................cms
Head circumference............................cms
3.2 Date of study
Age of study........................................days
Body weight........................................grams
Length.................................................cms
Head circumference............................cms
4. Length of stay......................................days
APPENDIX D
Parent stress scale: NICU
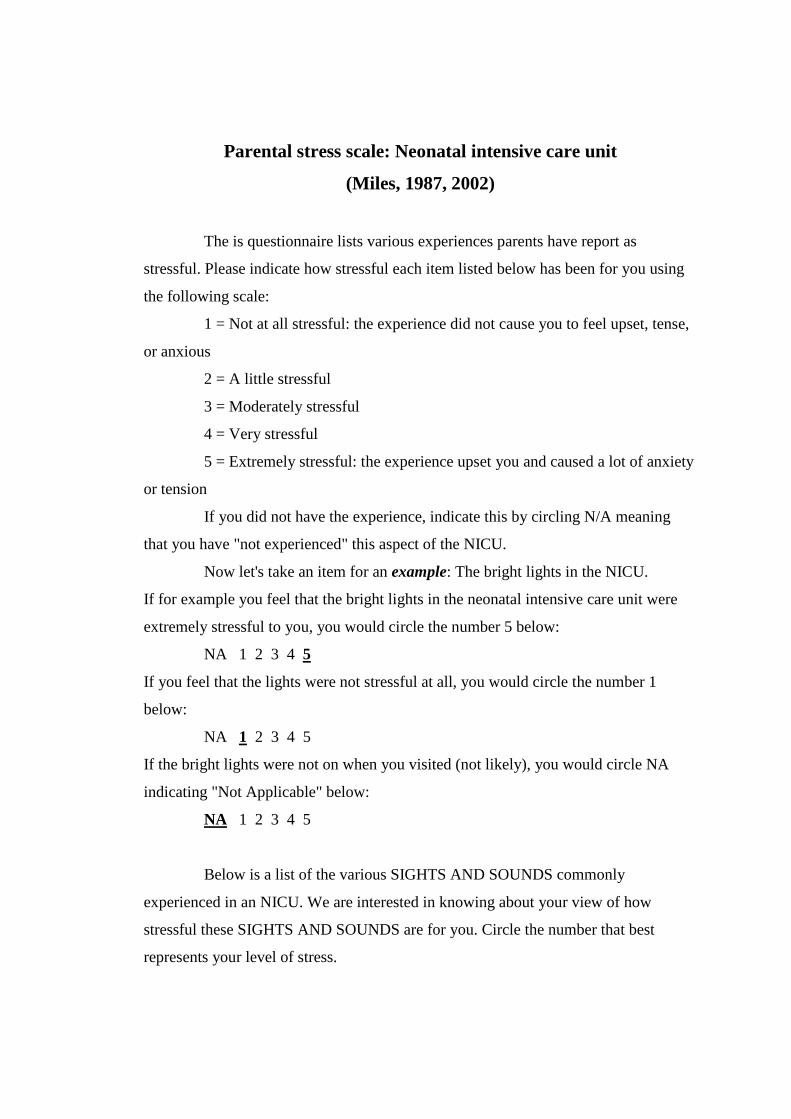
140
Parental stress scale: Neonatal intensive care unit
(Miles, 1987, 2002)
The is questionnaire lists various experiences parents have report as
stressful. Please indicate how stressful each item listed below has been for you using
the following scale:
1 = Not at all stressful: the experience did not cause you to feel upset, tense,
or anxious
2 = A little stressful
3 = Moderately stressful
4 = Very stressful
5 = Extremely stressful: the experience upset you and caused a lot of anxiety
or tension
If you did not have the experience, indicate this by circling N/A meaning
that you have "not experienced" this aspect of the NICU.
Now let's take an item for an example: The bright lights in the NICU.
If for example you feel that the bright lights in the neonatal intensive care unit were
extremely stressful to you, you would circle the number 5 below:
NA 1 2 3 4 5
If you feel that the lights were not stressful at all, you would circle the number 1
below:
NA 1 2 3 4 5
If the bright lights were not on when you visited (not likely), you would circle NA
indicating "Not Applicable" below:
NA 1 2 3 4 5
Below is a list of the various SIGHTS AND SOUNDS commonly
experienced in an NICU. We are interested in knowing about your view of how
stressful these SIGHTS AND SOUNDS are for you. Circle the number that best
represents your level of stress.
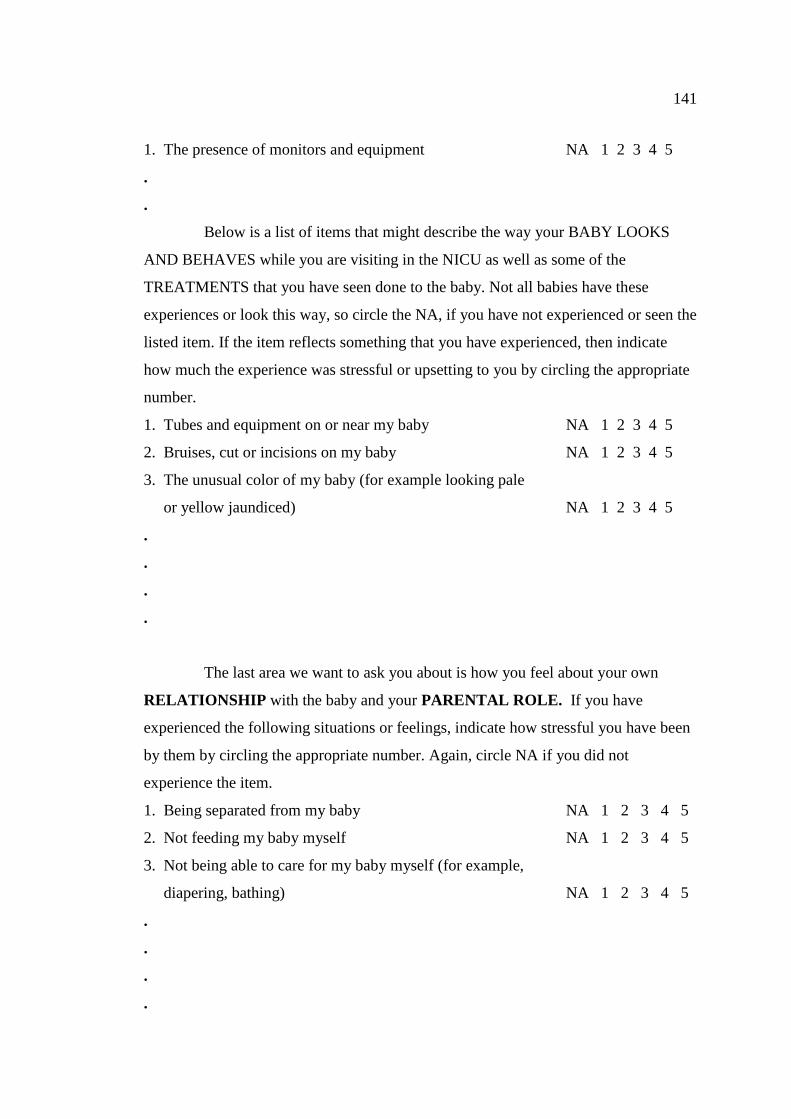
141
1. The presence of monitors and equipment NA 1 2 3 4 5
.
.
Below is a list of items that might describe the way your BABY LOOKS
AND BEHAVES while you are visiting in the NICU as well as some of the
TREATMENTS that you have seen done to the baby. Not all babies have these
experiences or look this way, so circle the NA, if you have not experienced or seen the
listed item. If the item reflects something that you have experienced, then indicate
how much the experience was stressful or upsetting to you by circling the appropriate
number.
1. Tubes and equipment on or near my baby NA 1 2 3 4 5
2. Bruises, cut or incisions on my baby NA 1 2 3 4 5
3. The unusual color of my baby (for example looking pale
or yellow jaundiced) NA 1 2 3 4 5
.
.
.
.
The last area we want to ask you about is how you feel about your own
RELATIONSHIP with the baby and your PARENTAL ROLE. If you have
experienced the following situations or feelings, indicate how stressful you have been
by them by circling the appropriate number. Again, circle NA if you did not
experience the item.
1. Being separated from my baby NA 1 2 3 4 5
2. Not feeding my baby myself NA 1 2 3 4 5
3. Not being able to care for my baby myself (for example,
diapering, bathing) NA 1 2 3 4 5
.
.
.
.

APPENDIX E
Parent stress index (PSI)
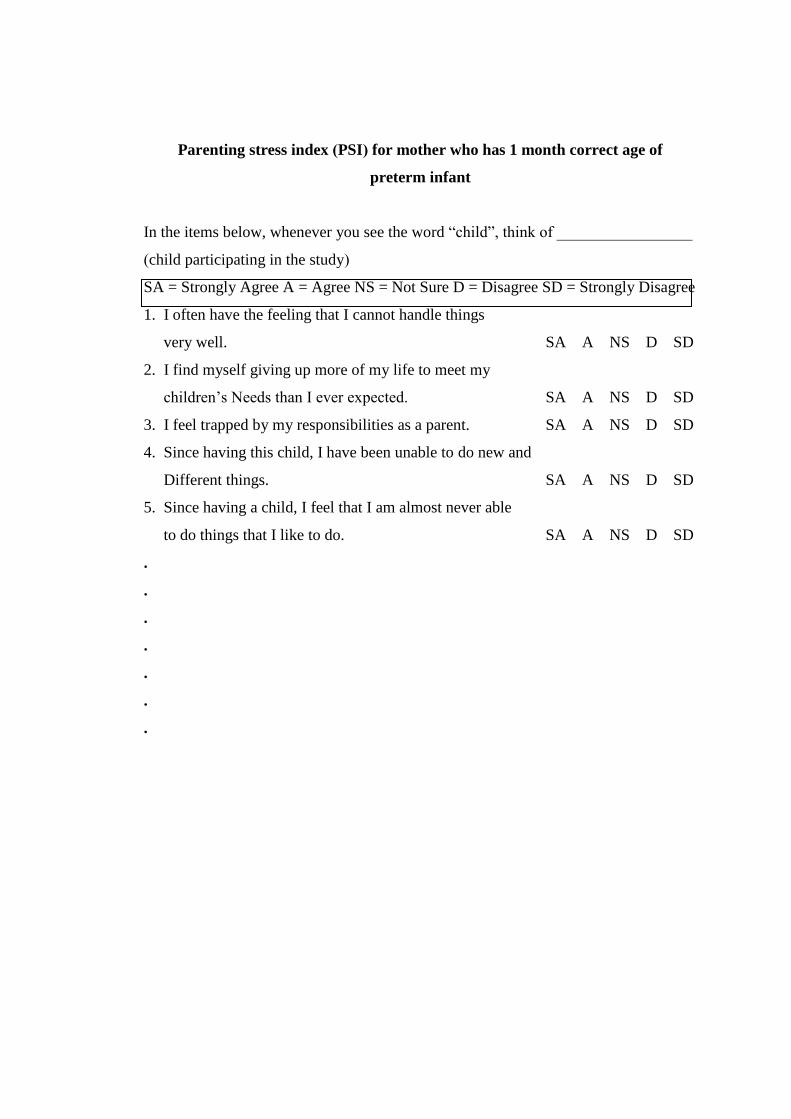
143
Parenting stress index (PSI) for mother who has 1 month correct age of
preterm infant
In the items below, whenever you see the word “child”, think of _________________
(child participating in the study)
SA = Strongly Agree A = Agree NS = Not Sure D = Disagree SD = Strongly Disagree
1. I often have the feeling that I cannot handle things
very well. SA A NS D SD
2. I find myself giving up more of my life to meet my
children’s Needs than I ever expected. SA A NS D SD
3. I feel trapped by my responsibilities as a parent. SA A NS D SD
4. Since having this child, I have been unable to do new and
Different things. SA A NS D SD
5. Since having a child, I feel that I am almost never able
to do things that I like to do. SA A NS D SD
.
.
.
.
.
.
.
144
APPENDIX F
Maternal attachment inventory (MAI)

145
Maternal attachment inventory (MAI)
The following sentences describe thoughts, feelings, and situations mothers
of preterm infant may experience. Checklist the letter under the word that is applies to
you.
Almost
always
Often Some
time
Almost
never
1. I feel love for my baby
2. I feel warm and happy with my baby
3. I want to spend special time with my
baby
4. I look forward to being with my baby
5. Just seeing my baby makes me feel good
.
.
.
.
.
.
.

146
APPENDIX G
Mother-infant attachment tool
147
MANUAL FOR ADMINISTRATION OF THE MOTHER-INFANT
ATTACHMENT TOOL (MIAT)
Introduction
The Mother-Infant Attachment Tool (MIAT) is a 16-items observational that
measure of the quality of mother-infant attachment among preterm infants. In
addition, there is an 8-items assessment of attachment from mother to infant, and 8-
items assessment of attachment from infant to mother. The MIAT measures four
aspects of the mother-infant attachment that include tactile, visual, auditory, and
feeding.
What is the purpose of the MIAT?
The MIAT is designed to measure mother-infant attachment among preterm
infant at 1 and 2 months corrected age. The instrument categorizes areas of mother
and preterm infant attachment strength and areas in which their require support to
achieve effective attachment.
Why was the instrument developed?
The MIAT was developed to assessment the mother-infant attachment that is
especially in preterm infants for the intervention research. The MIAT grew from the
need to describe attachment behavior of mothers and preterm infants during feeding
time. There was also need to generate a common language to communicate with other
nurses concerning mother and preterm infant attachment.
What does the Mother-Infant Attachment Tool offer?
- Identifies domains of attachment that are areas of strength and those that
are most in require of supportive interventions.
- Establishes a common language/point of reference about mother and
preterm infant attachment to aid communication between nurses.
- Provides a research instrument for attachment assessment between mother
with preterm infant or full term infant. It can be used as an antecedent condition, and
outcome of an intervention, or the target of the intervention itself.
148
How was the MIAT developed?
The MIAT was applied from Mother-Infant Screening Tool (MIST) by
Reiser (1981). She developed this instrument that was most crucial in facilitating
attachment between mother and full term infant while the mother was feeding her
infant since the one week old infant. However, some of items didn’t vigorous for
preterm infant attachment. Therefore, the MIAT will be developed for justification
attachment between mother and preterm infant.
How is the MIAT scaled and scored?
There are three distinct columns of behavior label A-B-C. The very attentive
mother and responsive infant would be under A, and at the other extreme, the
nonattentive mother and unresponsive infant would be under C. Label A have a 2
scores, B have a 1 score, and C have a 0 score. Therefore, the score will be between
0-32 scores. If the score more that mean + SD, it mean they have high level of
mother-infant attachment. On the other hand, if the score less than mean + SD, it
mean they have low level of mother-infant attachment. In addition, if the score be
equal to mean + SD, it mean they have medium level of mother-infant attachment.
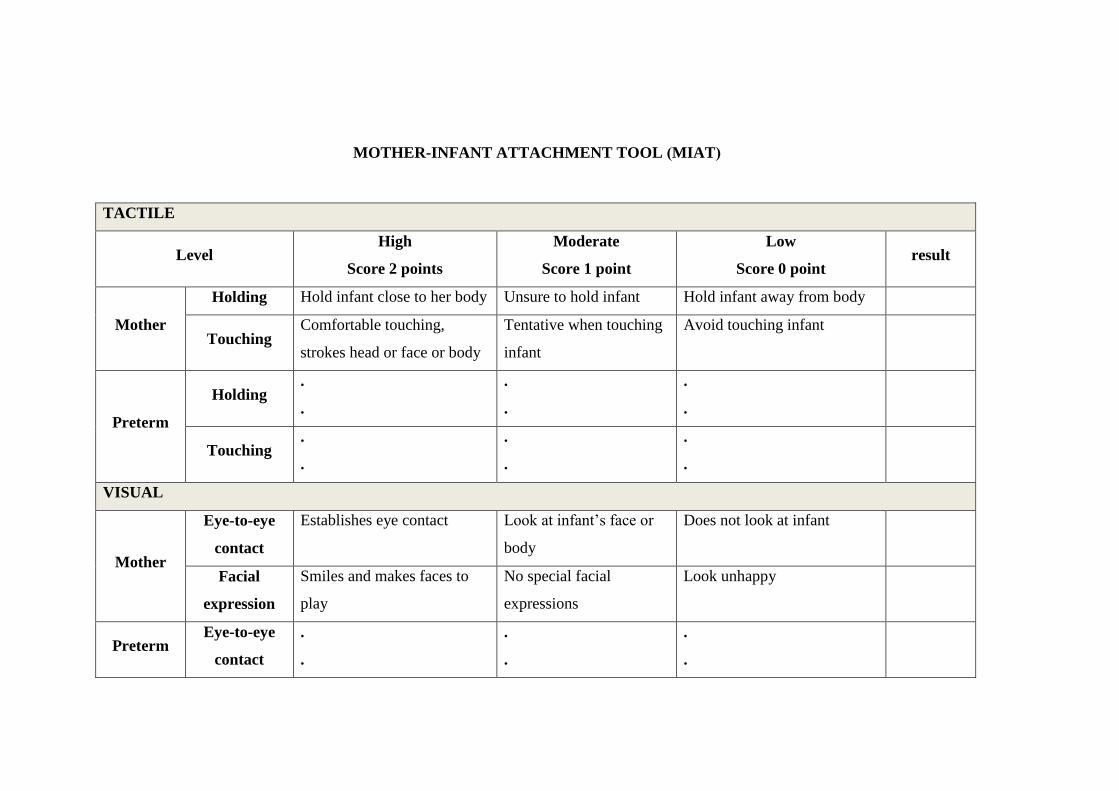
147
MOTHER-INFANT ATTACHMENT TOOL (MIAT)
TACTILE
Level High
Score 2 points
Moderate
Score 1 point
Low
Score 0 point result
Mother
Holding Hold infant close to her body Unsure to hold infant Hold infant away from body
Touching Comfortable touching,
strokes head or face or body
Tentative when touching
infant
Avoid touching infant
Preterm
Holding .
.
.
.
.
.
Touching .
.
.
.
.
.
VISUAL
Mother
Eye-to-eye
contact
Establishes eye contact Look at infant’s face or
body
Does not look at infant
Facial
expression
Smiles and makes faces to
play
No special facial
expressions
Look unhappy
Preterm Eye-to-eye
contact
.
.
.
.
.
.
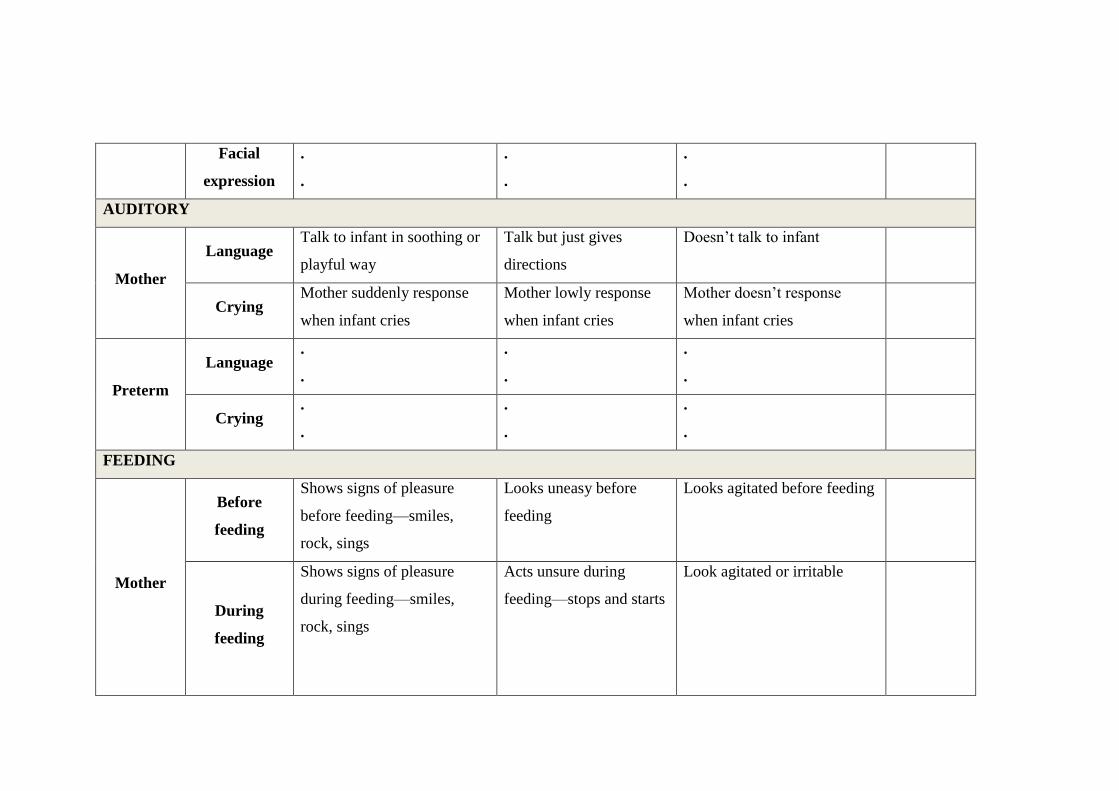
148
Facial
expression
.
.
.
.
.
.
AUDITORY
Mother
Language Talk to infant in soothing or
playful way
Talk but just gives
directions
Doesn’t talk to infant
Crying Mother suddenly response
when infant cries
Mother lowly response
when infant cries
Mother doesn’t response
when infant cries
Preterm
Language .
.
.
.
.
.
Crying .
.
.
.
.
.
FEEDING
Mother
Before
feeding
Shows signs of pleasure
before feeding—smiles,
rock, sings
Looks uneasy before
feeding
Looks agitated before feeding
During
feeding
Shows signs of pleasure
during feeding—smiles,
rock, sings
Acts unsure during
feeding—stops and starts
Look agitated or irritable
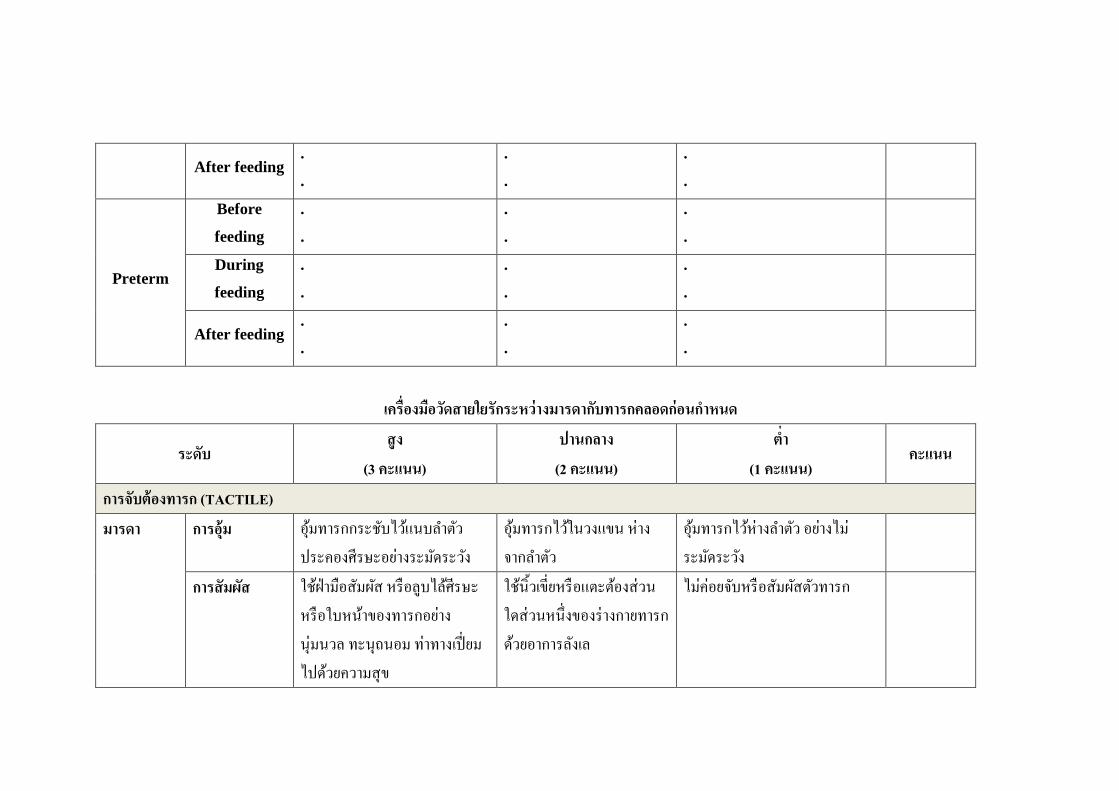
149
After feeding .
.
.
.
.
.
Preterm
Before
feeding
.
.
.
.
.
.
During
feeding
.
.
.
.
.
.
After feeding .
.
.
.
.
.
เครองมอวดสายใยรกระหวางมารดากบทารกคลอดกอนก าหนด
ระดบ สง
(3 คะแนน) ปานกลาง (2 คะแนน)
ต า (1 คะแนน)
คะแนน
การจบตองทารก (TACTILE)
มารดา การอม อมทารกกระชบไวแนบล าตว ประคองศรษะอยางระมดระวง
อมทารกไวในวงแขน หางจากล าตว
อมทารกไวหางล าตว อยางไมระมดระวง
การสมผส ใชฝามอสมผส หรอลบไลศรษะหรอใบหนาของทารกอยางนมนวล ทะนถนอม ทาทางเปยมไปดวยความสข
ใชนวเขยหรอแตะตองสวนใดสวนหนงของรางกายทารกดวยอาการลงเล
ไมคอยจบหรอสมผสตวทารก
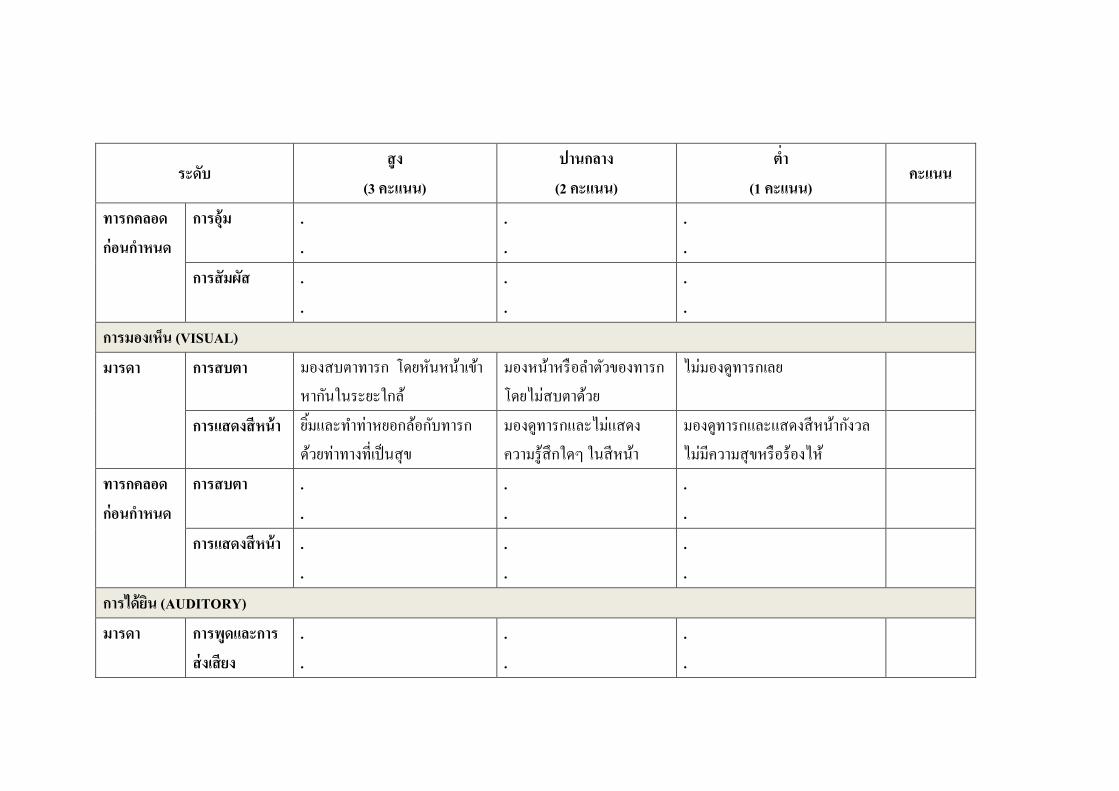
150
ระดบ สง
(3 คะแนน) ปานกลาง (2 คะแนน)
ต า (1 คะแนน)
คะแนน
ทารกคลอดกอนก าหนด
การอม . .
.
. . .
การสมผส . .
.
. . .
การมองเหน (VISUAL)
มารดา การสบตา มองสบตาทารก โดยหนหนาเขาหากนในระยะใกล
มองหนาหรอล าตวของทารก โดยไมสบตาดวย
ไมมองดทารกเลย
การแสดงสหนา ยมและท าทาหยอกลอกบทารกดวยทาทางทเปนสข
มองดทารกและไมแสดงความรสกใดๆ ในสหนา
มองดทารกและแสดงสหนากงวล ไมมความสขหรอรองไห
ทารกคลอดกอนก าหนด
การสบตา . .
.
. . .
การแสดงสหนา . .
.
. . .
การไดยน (AUDITORY)
มารดา การพดและการสงเสยง
.
. . .
.
.
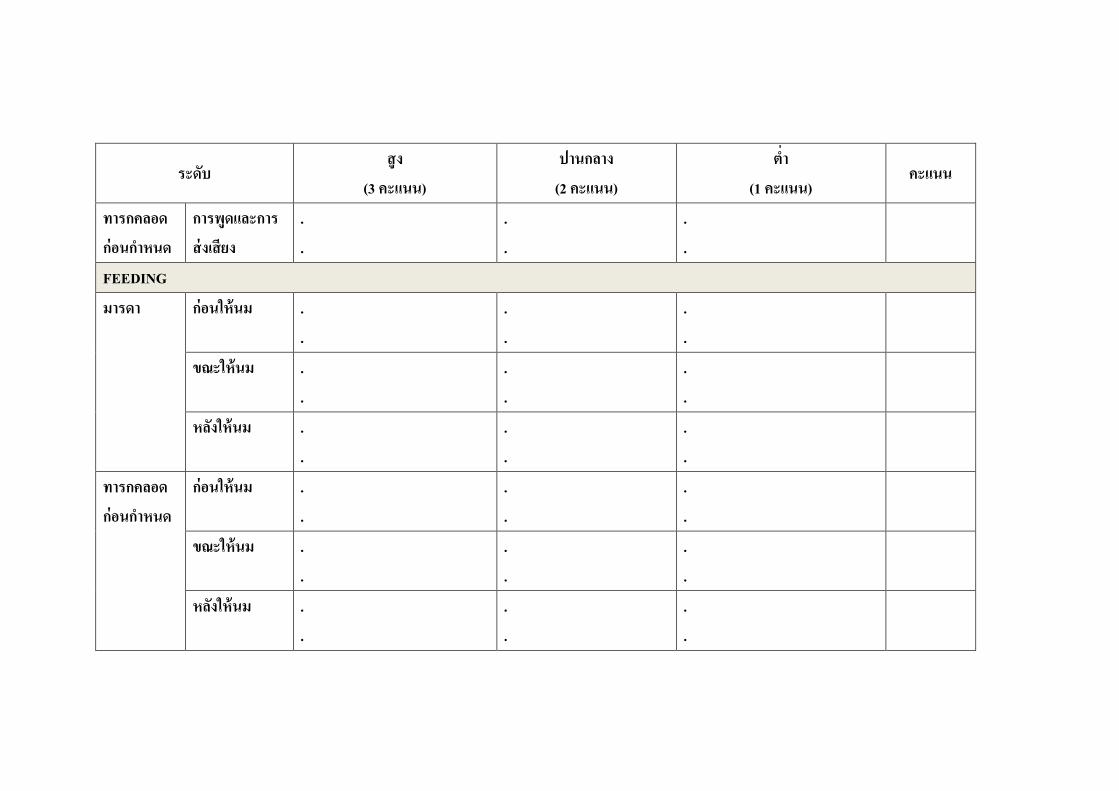
151
ระดบ สง
(3 คะแนน) ปานกลาง (2 คะแนน)
ต า (1 คะแนน)
คะแนน
ทารกคลอดกอนก าหนด
การพดและการสงเสยง
.
. . .
.
.
FEEDING
มารดา
กอนใหนม . .
.
. . .
ขณะใหนม . .
.
. . .
หลงใหนม . .
.
. . .
ทารกคลอดกอนก าหนด
กอนใหนม . .
.
. . .
ขณะใหนม . .
.
. . .
หลงใหนม . .
.
. . .
154
APPENDIX H
The table of modifed EMPAC program
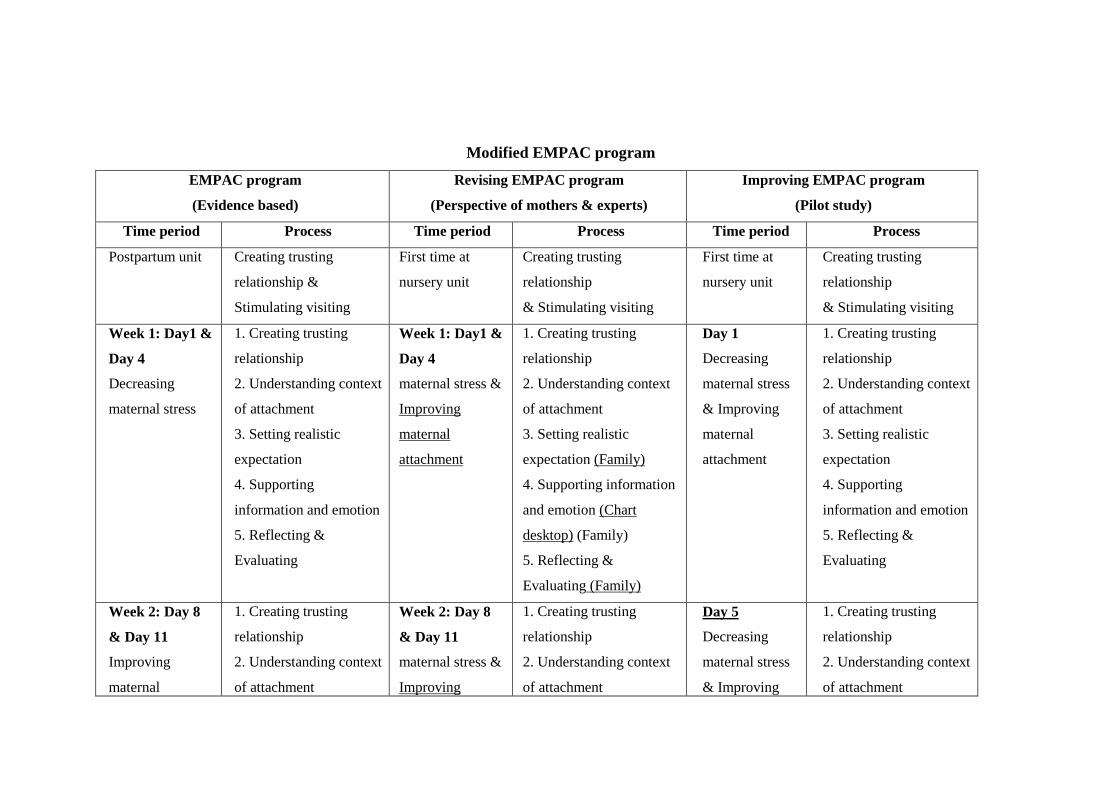
155
Modified EMPAC program
EMPAC program
(Evidence based)
Revising EMPAC program
(Perspective of mothers & experts)
Improving EMPAC program
(Pilot study)
Time period Process Time period Process Time period Process
Postpartum unit Creating trusting
relationship &
Stimulating visiting
First time at
nursery unit
Creating trusting
relationship
& Stimulating visiting
First time at
nursery unit
Creating trusting
relationship
& Stimulating visiting
Week 1: Day1 &
Day 4
Decreasing
maternal stress
1. Creating trusting
relationship
2. Understanding context
of attachment
3. Setting realistic
expectation
4. Supporting
information and emotion
5. Reflecting &
Evaluating
Week 1: Day1 &
Day 4
maternal stress &
Improving
maternal
attachment
1. Creating trusting
relationship
2. Understanding context
of attachment
3. Setting realistic
expectation (Family)
4. Supporting information
and emotion (Chart
desktop) (Family)
5. Reflecting &
Evaluating (Family)
Day 1
Decreasing
maternal stress
& Improving
maternal
attachment
1. Creating trusting
relationship
2. Understanding context
of attachment
3. Setting realistic
expectation
4. Supporting
information and emotion
5. Reflecting &
Evaluating
Week 2: Day 8
& Day 11
Improving
maternal
1. Creating trusting
relationship
2. Understanding context
of attachment
Week 2: Day 8
& Day 11
maternal stress &
Improving
1. Creating trusting
relationship
2. Understanding context
of attachment
Day 5
Decreasing
maternal stress
& Improving
1. Creating trusting
relationship
2. Understanding context
of attachment
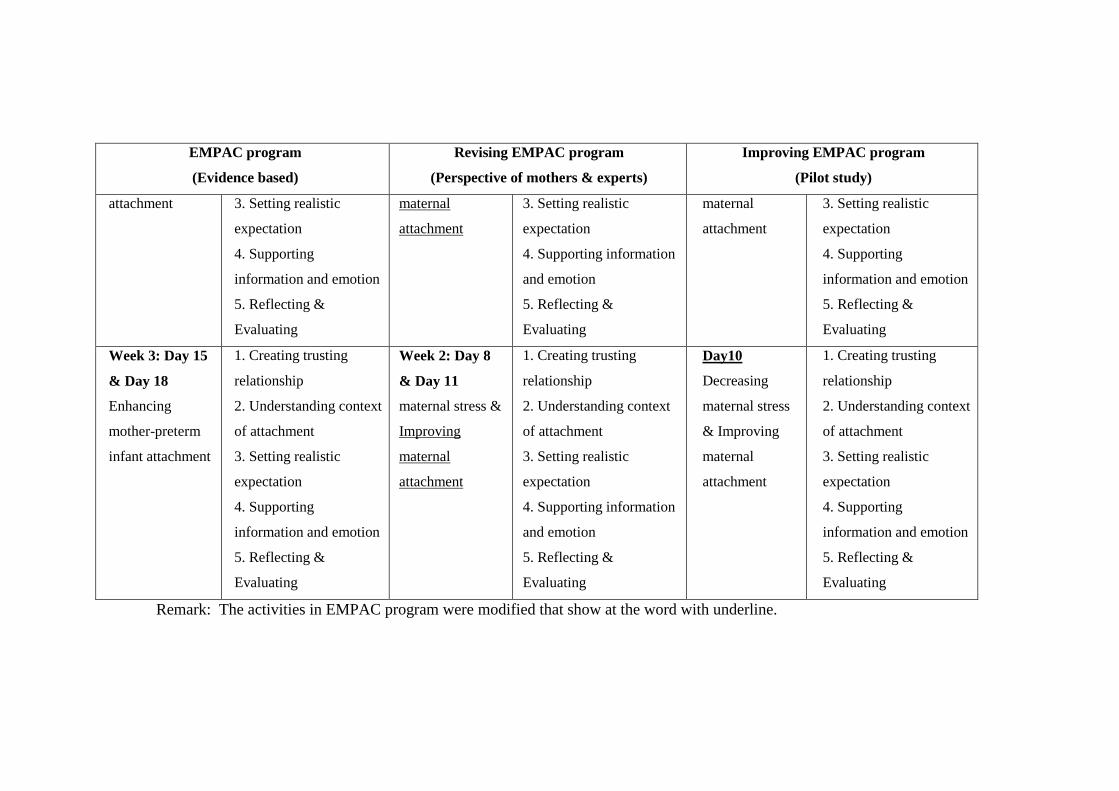
156
EMPAC program
(Evidence based)
Revising EMPAC program
(Perspective of mothers & experts)
Improving EMPAC program
(Pilot study)
attachment 3. Setting realistic
expectation
4. Supporting
information and emotion
5. Reflecting &
Evaluating
maternal
attachment
3. Setting realistic
expectation
4. Supporting information
and emotion
5. Reflecting &
Evaluating
maternal
attachment
3. Setting realistic
expectation
4. Supporting
information and emotion
5. Reflecting &
Evaluating
Week 3: Day 15
& Day 18
Enhancing
mother-preterm
infant attachment
1. Creating trusting
relationship
2. Understanding context
of attachment
3. Setting realistic
expectation
4. Supporting
information and emotion
5. Reflecting &
Evaluating
Week 2: Day 8
& Day 11
maternal stress &
Improving
maternal
attachment
1. Creating trusting
relationship
2. Understanding context
of attachment
3. Setting realistic
expectation
4. Supporting information
and emotion
5. Reflecting &
Evaluating
Day10
Decreasing
maternal stress
& Improving
maternal
attachment
1. Creating trusting
relationship
2. Understanding context
of attachment
3. Setting realistic
expectation
4. Supporting
information and emotion
5. Reflecting &
Evaluating
Remark: The activities in EMPAC program were modified that show at the word with underline.

157
APPENDIX I
Program evaluation questionnaire
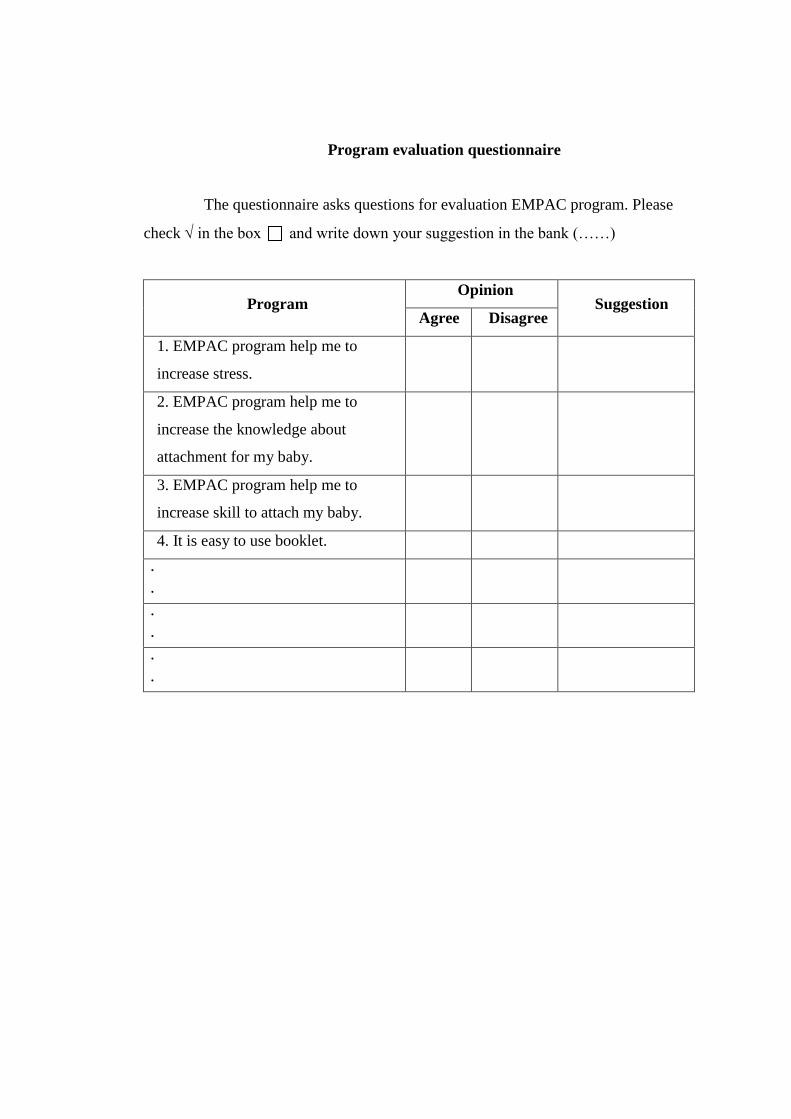
158
Program evaluation questionnaire
The questionnaire asks questions for evaluation EMPAC program. Please
check in the box and write down your suggestion in the bank (……)
Program Opinion
Suggestion Agree Disagree
1. EMPAC program help me to
increase stress.
2. EMPAC program help me to
increase the knowledge about
attachment for my baby.
3. EMPAC program help me to
increase skill to attach my baby.
4. It is easy to use booklet.
.
.
.
.
.
.
159
APPENDIX J
The early mother-preterm infant attachment coaching (EMPAC) program
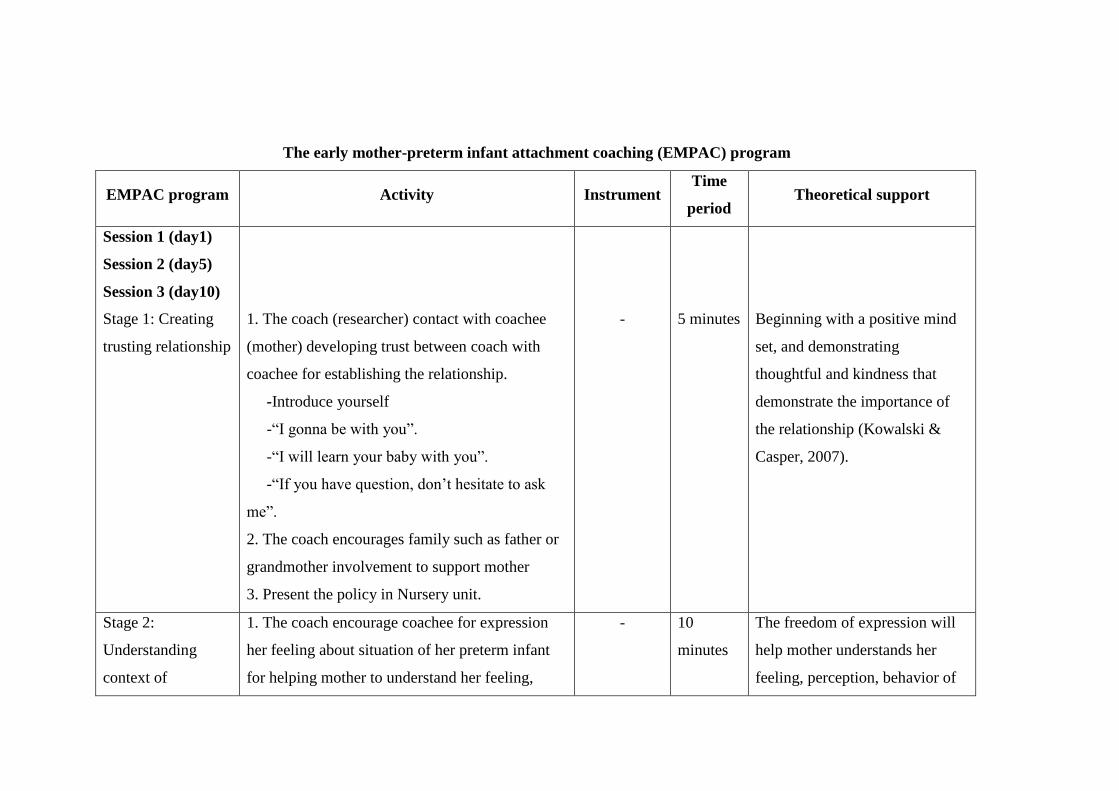
147
The early mother-preterm infant attachment coaching (EMPAC) program
EMPAC program Activity Instrument Time
period Theoretical support
Session 1 (day1)
Session 2 (day5)
Session 3 (day10)
Stage 1: Creating
trusting relationship
1. The coach (researcher) contact with coachee
(mother) developing trust between coach with
coachee for establishing the relationship.
-Introduce yourself
-“I gonna be with you”.
-“I will learn your baby with you”.
-“If you have question, don’t hesitate to ask
me”.
2. The coach encourages family such as father or
grandmother involvement to support mother
3. Present the policy in Nursery unit.
-
5 minutes
Beginning with a positive mind
set, and demonstrating
thoughtful and kindness that
demonstrate the importance of
the relationship (Kowalski &
Casper, 2007).
Stage 2:
Understanding
context of
1. The coach encourage coachee for expression
her feeling about situation of her preterm infant
for helping mother to understand her feeling,
- 10
minutes
The freedom of expression will
help mother understands her
feeling, perception, behavior of
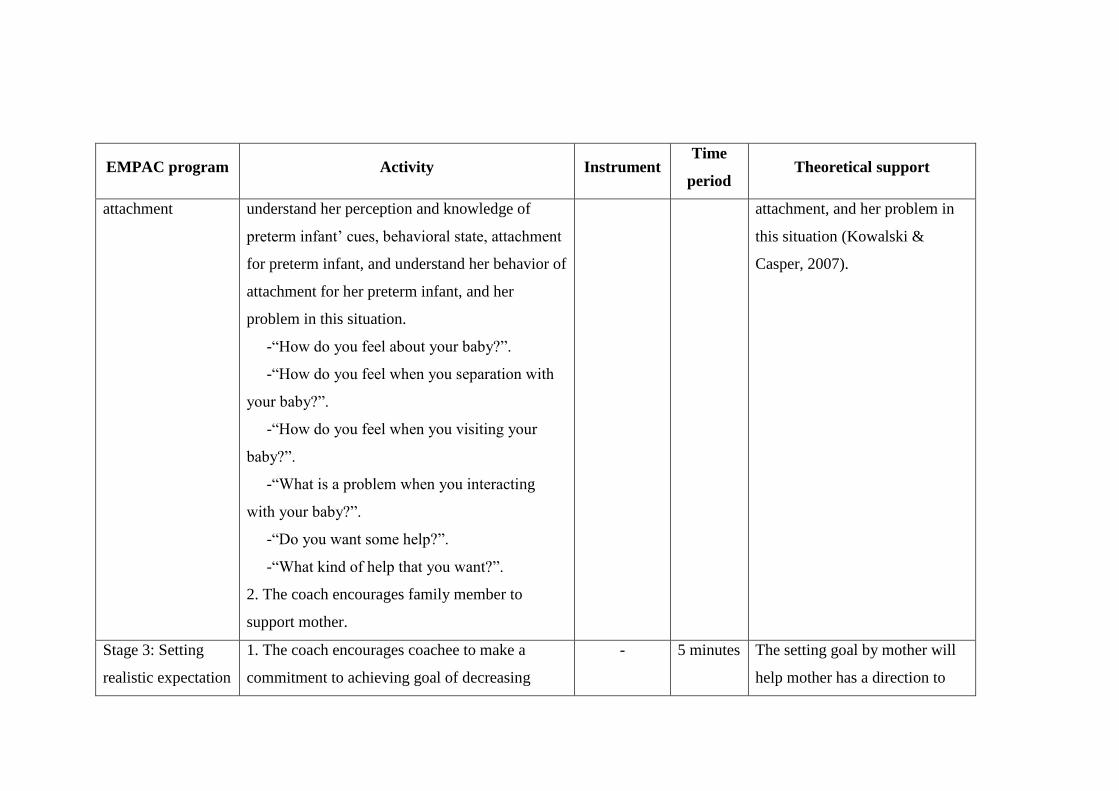
148
EMPAC program Activity Instrument Time
period Theoretical support
attachment understand her perception and knowledge of
preterm infant’ cues, behavioral state, attachment
for preterm infant, and understand her behavior of
attachment for her preterm infant, and her
problem in this situation.
-“How do you feel about your baby?”.
-“How do you feel when you separation with
your baby?”.
-“How do you feel when you visiting your
baby?”.
-“What is a problem when you interacting
with your baby?”.
-“Do you want some help?”.
-“What kind of help that you want?”.
2. The coach encourages family member to
support mother.
attachment, and her problem in
this situation (Kowalski &
Casper, 2007).
Stage 3: Setting
realistic expectation
1. The coach encourages coachee to make a
commitment to achieving goal of decreasing
- 5 minutes The setting goal by mother will
help mother has a direction to
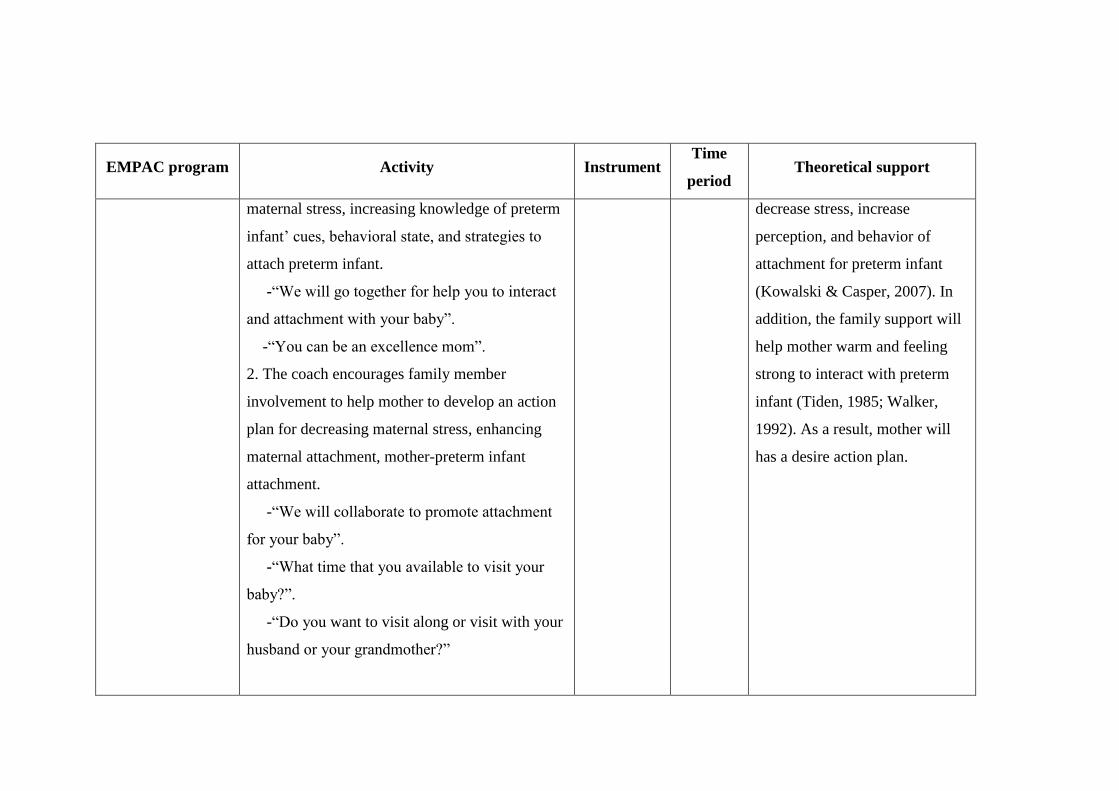
149
EMPAC program Activity Instrument Time
period Theoretical support
maternal stress, increasing knowledge of preterm
infant’ cues, behavioral state, and strategies to
attach preterm infant.
-“We will go together for help you to interact
and attachment with your baby”.
-“You can be an excellence mom”.
2. The coach encourages family member
involvement to help mother to develop an action
plan for decreasing maternal stress, enhancing
maternal attachment, mother-preterm infant
attachment.
-“We will collaborate to promote attachment
for your baby”.
-“What time that you available to visit your
baby?”.
-“Do you want to visit along or visit with your
husband or your grandmother?”
decrease stress, increase
perception, and behavior of
attachment for preterm infant
(Kowalski & Casper, 2007). In
addition, the family support will
help mother warm and feeling
strong to interact with preterm
infant (Tiden, 1985; Walker,
1992). As a result, mother will
has a desire action plan.
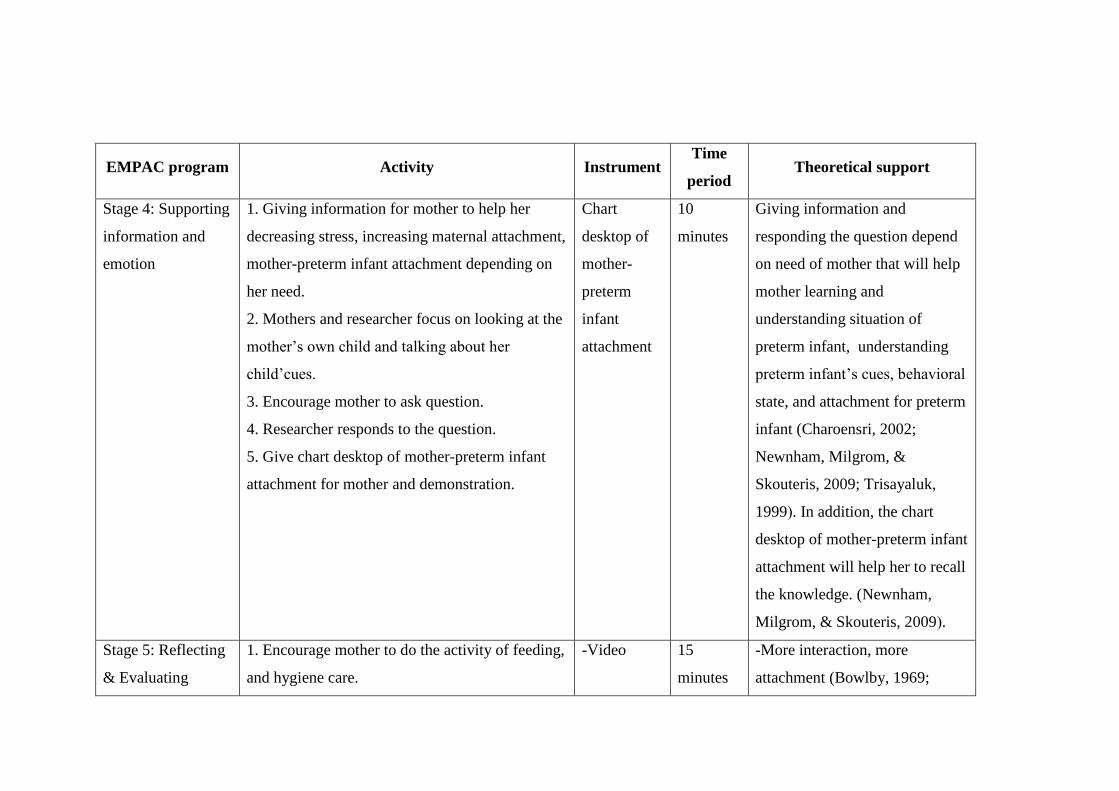
150
EMPAC program Activity Instrument Time
period Theoretical support
Stage 4: Supporting
information and
emotion
1. Giving information for mother to help her
decreasing stress, increasing maternal attachment,
mother-preterm infant attachment depending on
her need.
2. Mothers and researcher focus on looking at the
mother’s own child and talking about her
child’cues.
3. Encourage mother to ask question.
4. Researcher responds to the question.
5. Give chart desktop of mother-preterm infant
attachment for mother and demonstration.
Chart
desktop of
mother-
preterm
infant
attachment
10
minutes
Giving information and
responding the question depend
on need of mother that will help
mother learning and
understanding situation of
preterm infant, understanding
preterm infant’s cues, behavioral
state, and attachment for preterm
infant (Charoensri, 2002;
Newnham, Milgrom, &
Skouteris, 2009; Trisayaluk,
1999). In addition, the chart
desktop of mother-preterm infant
attachment will help her to recall
the knowledge. (Newnham,
Milgrom, & Skouteris, 2009).
Stage 5: Reflecting
& Evaluating
1. Encourage mother to do the activity of feeding,
and hygiene care.
-Video
15
minutes
-More interaction, more
attachment (Bowlby, 1969;
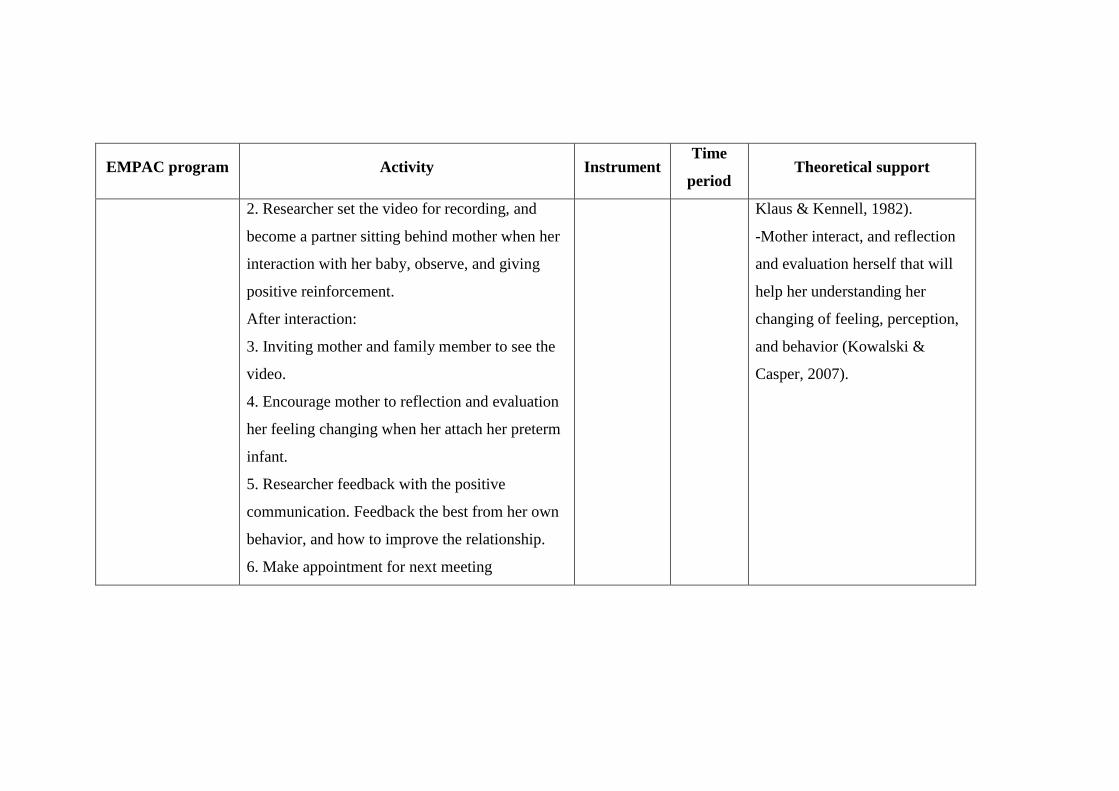
151
EMPAC program Activity Instrument Time
period Theoretical support
2. Researcher set the video for recording, and
become a partner sitting behind mother when her
interaction with her baby, observe, and giving
positive reinforcement.
After interaction:
3. Inviting mother and family member to see the
video.
4. Encourage mother to reflection and evaluation
her feeling changing when her attach her preterm
infant.
5. Researcher feedback with the positive
communication. Feedback the best from her own
behavior, and how to improve the relationship.
6. Make appointment for next meeting
Klaus & Kennell, 1982).
-Mother interact, and reflection
and evaluation herself that will
help her understanding her
changing of feeling, perception,
and behavior (Kowalski &
Casper, 2007).

165
APPENDIX K
Chart desktop of mother-preterm infant attachment
166
Chart desktop of mother-preterm infant attachment

167
APPENDIX L
Effect size calculation
Corrected age of preterm infant calculation
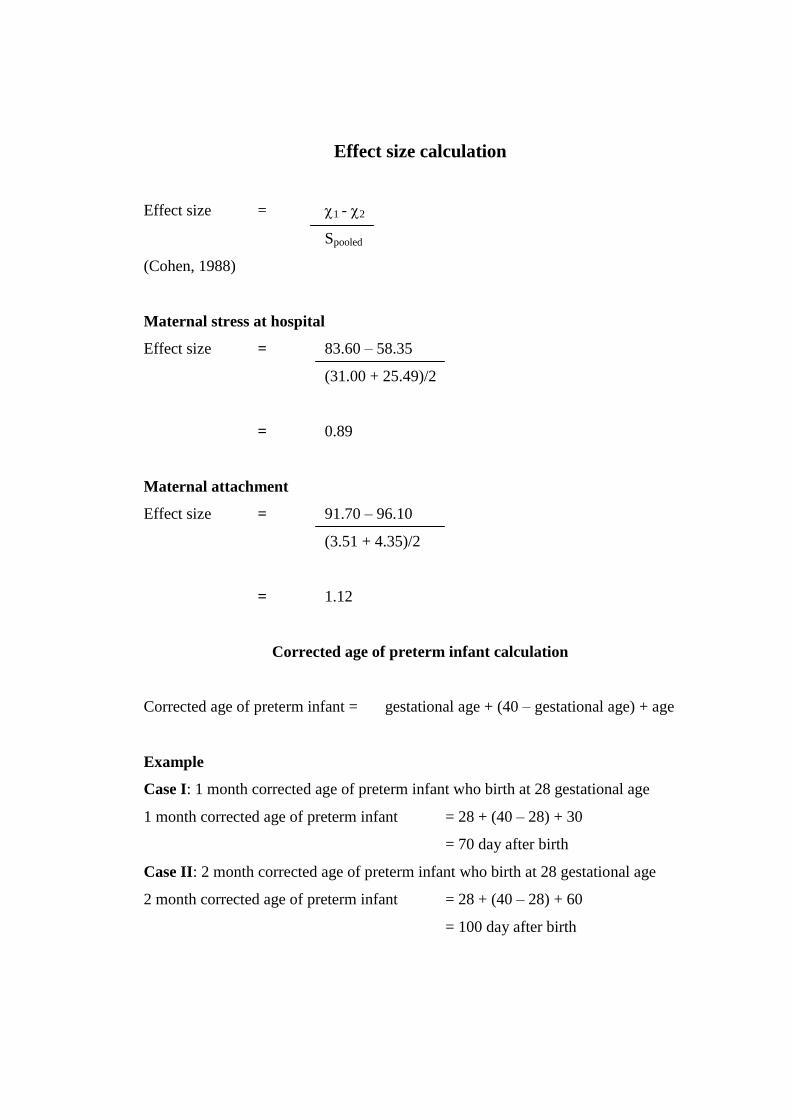
168
Effect size calculation
Effect size = 1 - 2
Spooled
(Cohen, 1988)
Maternal stress at hospital
Effect size = 83.60 – 58.35
(31.00 + 25.49)/2
= 0.89
Maternal attachment
Effect size = 91.70 – 96.10
(3.51 + 4.35)/2
= 1.12
Corrected age of preterm infant calculation
Corrected age of preterm infant = gestational age + (40 – gestational age) + age
Example
Case I: 1 month corrected age of preterm infant who birth at 28 gestational age
1 month corrected age of preterm infant = 28 + (40 – 28) + 30
= 70 day after birth
Case II: 2 month corrected age of preterm infant who birth at 28 gestational age
2 month corrected age of preterm infant = 28 + (40 – 28) + 60
= 100 day after birth

169
APPENDIX M
The IRB approval
170
171
BIOGRAPHY
Name Mrs. Runglawon Eamkusolkit
Date of birth August 31, 1974
Place of birth Muang, Nakhon Phanom
Present address 71/ 1 M. 4 Nitayo Road, Nongyad Subdistrict,
Muang, Nakhon Phanom province 48000
Position
1996-present Lecturer
Boromarajonani College of Nursing,
Nakhon Phamom University
Education
1992-1996 Bachelor of Nursing Science
(Nursing and Midwifery)
Boromarajonani College of Nursing, Saraburi
1998-2000 Master of Nursing Science
(Pediatric Nursing)
Khon Khan University
2010-2016 Doctor of Philosophy (Nursing Science)
International program,
Burapha University





























