Embed Size (px)
Citation preview
Development of a Score and Probability Estimate forDetecting Angle Closure Based on Anterior Segment
Optical Coherence Tomography
MONISHA E. NONGPIUR, BENJAMIN A. HAALAND, SHAMIRA A. PERERA, DAVID S. FRIEDMAN,MINGGUANG HE, LISANDRO M. SAKATA, MANI BASKARAN, AND TIN AUNG
� PURPOSE: To develop a score along with an estimatedprobability of disease for detecting angle closure based onanterior segment optical coherence tomography (AS OCT)imaging.� DESIGN: Cross-sectional study.� METHODS: A total of 2047 subjects 50 years of age andolder were recruited from a community polyclinic inSingapore. All subjects underwent standardized ocularexamination including gonioscopy and imaging by ASOCT (Carl Zeiss Meditec). Customized software (Zhong-shan Angle Assessment Program) was used to measureAS OCT parameters. Complete data were available for1368 subjects. Data from the right eyes were used foranalysis. A stepwise logistic regression model withAkaike information criterion was used to generate a scorethat then was converted to an estimated probability of thepresence of gonioscopic angle closure, defined as theinability to visualize the posterior trabecular meshworkfor at least 180 degrees on nonindentation gonioscopy.� RESULTS: Of the 1368 subjects, 295 (21.6%) hadgonioscopic angle closure. The angle closure score wascalculated from the shifted linear combination of the ASOCT parameters. The score can be converted to an esti-mated probability of having angle closure using the rela-tionship: estimated probability [ escore/(1 D escore),where e is the natural exponential. The score performedwell in a second independent sample of 178 angle-closuresubjects and 301 normal controls, with an area under thereceiver operating characteristic curve of 0.94.
Accepted for publication Sep 11, 2013.From the Singapore Eye Research Institute and Singapore National Eye
Center, Singapore, Republic of Singapore (M.E.N., S.A.P., L.M.S., M.B.,T.A.); the Centre for Quantitative Medicine, Office of Clinical SciencesDuke-NUS Graduate Medical School, Singapore, Republic of Singapore(M.E.N., B.A.H.); Department of Statistics and Applied Probability,National University of Singapore, Singapore, Republic of Singapore(B.A.H.); Wilmer Eye Institute, Dana Center for PreventiveOphthalmology, Johns Hopkins University, Baltimore, Maryland(D.S.F.); the State Key Laboratory of Ophthalmology, ZhongshanOphthalmic Center, Sun Yat-sen University, Guangzhou, China(M.H.); and the Yong Loo Lin School of Medicine, National Universityof Singapore, Singapore, Republic of Singapore (T.A.).
Lisandro M. Sakata is now affiliated with the Federal University ofParana, Curitiba, Brazil.
Inquiries to Tin Aung, Singapore National Eye Center, 11 ThirdHospital Avenue, Singapore 168751, Republic of Singapore; e-mail:[email protected]
32 � 2014 BY ELSEVIER INC.
� CONCLUSIONS: A score derived from a single AS OCTimage, coupled with an estimated probability, provides anobjective platform for detection of angle closure. (Am JOphthalmol 2014;157:32–38. � 2014 by Elsevier Inc.All rights reserved.)
PRIMARY ANGLE-CLOSURE GLAUCOMA ACCOUNTS
for approximately 50% of people with bilateralglaucoma blindness worldwide,1,2 with significant
impact on individuals, societies, and health care systems.Identifying people with the early asymptomatic stages ofthe disease may allow for prophylactic treatment by laseriridotomy to prevent visual loss. Therefore, it is desirableto augment the efficiency and effectiveness of screeningpractices above and beyond the current approaches.3–6
Anterior segment optical coherence tomography (ASOCT) technology enables the acquisition and visualizationof high-resolution images of the anterior segment (AS) struc-tures in vivo.7 Recently, several novel AS OCT parametershave been associated with angle closure, including smalleranterior chamber width, area, and volume8,9; greater iristhickness, curvature, and area10; and a larger lens vault.11,12
In addition to their individual association with angleclosure, it was shown recently that more than 80% of thevariation in angle width is explained by these newlyidentified risk factors, with lens vault, anterior chamberarea, and volume being the most important determinants.13
We recently evaluated the diagnostic ability of a range ofbiometric, demographic, and AS OCT-based parameters todetect angle closure. A stepwise logistic regression modelwith a variable set consisting of just 6 AS OCT-derivedparameters—namely, lens vault; anterior chamber width,area, and volume; iris thickness; and iris area—had a highdiagnostic capability with an area under the receiver oper-ating characteristic curve (AUC) of more than 0.95 in iden-tifying eyeswith gonioscopic angle closure.14Webelieve thatthese findings can be useful in developing a feasible, imaging-based tool for the detection of eyes with angle closure.The purpose of this study was to develop an angle-closure
score and probability estimate based on AS OCT imagingthat would allow for objective identification of eyes withgonioscopic angle closure. As a secondary aim, we wantedto dissect out the contribution of the various anatomicfactors imaged by AS OCT to identify the likely mecha-nism(s) contributing to angle closure.
0002-9394/$36.00http://dx.doi.org/10.1016/j.ajo.2013.09.012
ALL RIGHTS RESERVED.

METHODS
APPROVAL FOR THE STUDY WAS GRANTED BY THE
Singapore Eye Research Institute Institutional ReviewBoard. The study was conducted in accordance with thetenets of the Declaration of Helsinki, and written informedconsent was obtained from all subjects before enrolmentinto the study. Analysis was performed on data collectedfrom a community-based cross-sectional study performedin Singapore, the details of which have been described pre-viously.6 In brief, the subjects for the study were recruitedfrom a government-run community-based clinic facilitythat provides primary health care services for local resi-dents. The study participants were 50 years of age and older.
� EXAMINATION AND DEFINITION OF GONIOSCOPICANGLE CLOSURE: All study participants underwent a stan-dardized eye examination that included measurements ofvisual acuity using a logarithm of the minimal angle of reso-lution chart (Lighthouse, Inc, Long Island,NewYork,USA),slit-lamp examination (Model BQ 900; Haag-Streit, Bern,Switzerland), stereoscopic optic disc examination with a78-diopter lens (Volk Optical, Inc, Mentor, Ohio), measure-ment of intraocular pressure by Goldmann applanationtonometry (Haag-Streit, Koniz, Switzerland), and gonio-scopy performed in the dark using a Goldmann 2-mirrorlens at high magnification (316) by a single examiner.
An eye was considered to have gonioscopic angle closureif the posterior pigmented trabecular meshwork was notvisible for at least 180 degrees on nonindentation gonio-scopy with the eye in the primary position. Axial lengthand anterior chamber depth (ACD) were measured usingpartial coherence laser interferometry by IOLMaster(Carl Zeiss Meditec, Dublin, California, USA).
� ANTERIORSEGMENTOPTICALCOHERENCETOMOGRAPHYIMAGING: ASOCTimageswere acquired fromall participantsin dark room conditions by a single operator. Each scan wascentered on the pupil, and a single cross-sectional horizontalscan (nasal-temporal angles at 0 degrees and 180 degrees)was evaluated for each subject. The best-quality imageswere obtained by adjusting the saturation and noise and byoptimizing the polarization for each scan during the examina-tion.Acustomized software, the ZhongshanAngleAssessmentProgram15 (Guangzhou, China), was used to process the ASOCT images. For each image, the only observer input was todetermine the location of the 2 scleral spurs, which is describedas the inwardprotrusionof the sclerawithachange incurvatureof its inner surface. The algorithm then automatically calcu-lated the various AS parameters. The reproducibility ofthe AS parameters was excellent, with the intraclass correla-tion coefficient ranging from 0.88 to 0.97.8,10,12
� DEFINITIONOFANTERIORSEGMENTOPTICALCOHERENCETOMOGRAPHYPARAMETERS: The parameters as measured byASOCT (Figure 1) were defined as follows. Anterior chamberwidthwas defined as the horizontal scleral spur-to-spur distance
VOL. 157, NO. 1 AN AUTOMATED SCORE FOR DE
(inmillimeters),8 and lens vault11 was the perpendicular dis-tance between the anterior pole of the crystalline lens andthe horizontal line joining the 2 scleral spurs (inmicrometers). The iris thickness was measured at 750 and2000mm from the scleral spur.10 The iris area was calculatedas the cross-sectional area of the full length (from spur topupil) of the iris (in square millimeters). To determine iriscurvature, the software draws a line from themost peripheralto the most central points of the iris pigment epithelium. Aperpendicular line then is extended from this line to the irispigment epithelium at the point of greatest convexity. Thelength of this perpendicular line is a measure of the iris cur-vature (in millimeters).10 The anterior chamber area wasdefined as the cross-sectional area (in square millimeters)ofAS bounded by the corneal endothelium, the anterior sur-face of the iris, and the anterior surface of the lens (withinthe pupil).9 To assess anterior chamber volume, the algo-rithm first plots a vertical axis through themidpoint (center)of the anterior chamber area, and by rotating the anteriorchamber area 360 degrees around this vertical axis, the ante-rior chamber volume9 was calculated (in cubedmillimeters).
� STATISTICAL ANALYSIS: Development of the angle closurescore and estimated probability. Data from right eyes wereused for analysis. After an evaluation of the diagnostic accu-racy of several classification algorithms to detect gonioscopicangle closure, we found that the stepwise logistic regressionmodel with Akaike information criterion consisting of only6 AS OCT parameters was both the most accurate and leastvariable.14 Akaike information criterion measures both theaccuracy and complexity of a model, and in the context ofa given problem, a model with lower Akaike informationcriterion often will have better generalizability. Stepwiselogistic regression was begun with none of the 6 variablesin the model. At each stage, the possibilities of (1) addingeach variable not yet included, (2) removing each of thecurrently included variables, and (3) leaving the modelunchanged were considered in turn. The action withminimum Akaike information criterion was taken with thealgorithm terminating when leaving the model unchangedhad minimum Akaike information criterion. The logisticregression yields a score that is a shifted linear combinationof the selected variables. This score can be converted toan estimated probability of angle closure using therelationship: estimated probability ¼ escore/(1 þ escore),where e is the natural exponential.
Determination of the relative contributions of the anteriorsegment optical coherence tomography parameters and theirgraphical representation. An assessment of the relative con-tributions of the variables to the angle closure score for agiven subject was achieved first by standardizing each ofthe variables, so that each had a mean of 0 and a standarddeviation of 1. This was achieved by subtracting each vari-able’s mean and then dividing each variable by its standarddeviation. Then, the shifted linear combination of selected
33TECTION OF ANGLE CLOSURE
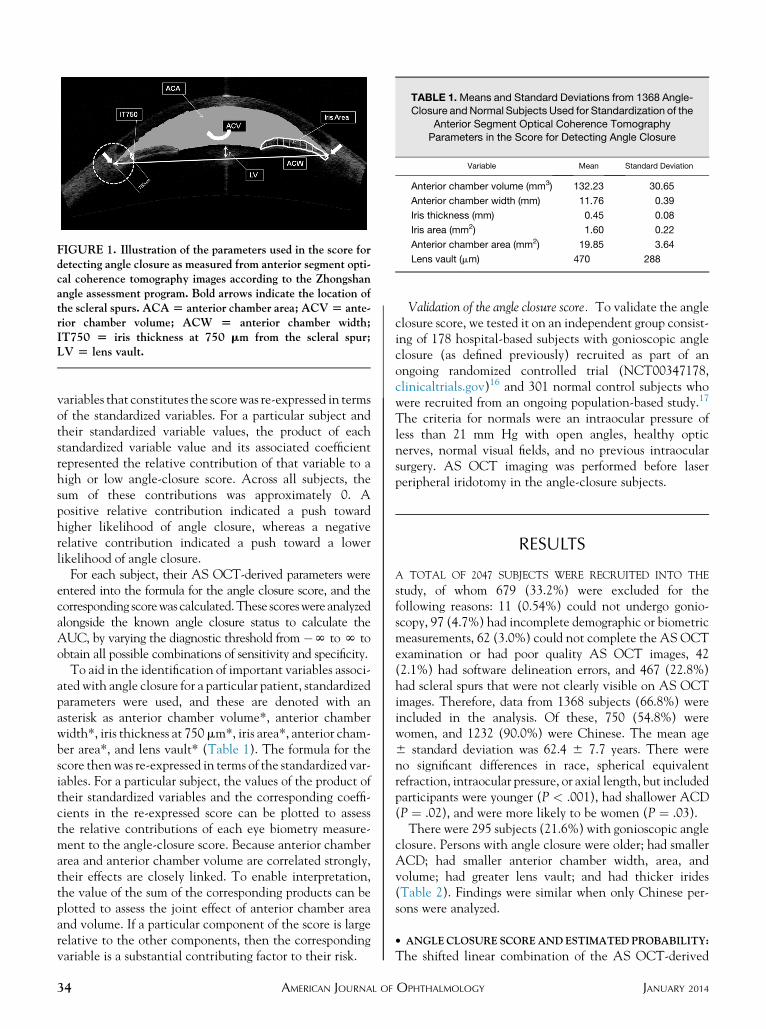
TABLE 1.Means and Standard Deviations from 1368 Angle-Closure andNormal Subjects Used for Standardization of the
Anterior Segment Optical Coherence Tomography
Parameters in the Score for Detecting Angle Closure
Variable Mean Standard Deviation
Anterior chamber volume (mm3) 132.23 30.65
Anterior chamber width (mm) 11.76 0.39
Iris thickness (mm) 0.45 0.08
Iris area (mm2) 1.60 0.22
Anterior chamber area (mm2) 19.85 3.64
Lens vault (mm) 470 288FIGURE 1. Illustration of the parameters used in the score fordetecting angle closure as measured from anterior segment opti-cal coherence tomography images according to the Zhongshanangle assessment program. Bold arrows indicate the location ofthe scleral spurs. ACA[ anterior chamber area; ACV[ ante-rior chamber volume; ACW [ anterior chamber width;IT750 [ iris thickness at 750 mm from the scleral spur;LV [ lens vault.
variables that constitutes the scorewas re-expressed in termsof the standardized variables. For a particular subject andtheir standardized variable values, the product of eachstandardized variable value and its associated coefficientrepresented the relative contribution of that variable to ahigh or low angle-closure score. Across all subjects, thesum of these contributions was approximately 0. Apositive relative contribution indicated a push towardhigher likelihood of angle closure, whereas a negativerelative contribution indicated a push toward a lowerlikelihood of angle closure.
For each subject, their AS OCT-derived parameters wereentered into the formula for the angle closure score, and thecorresponding scorewas calculated.These scoreswere analyzedalongside the known angle closure status to calculate theAUC, by varying the diagnostic threshold from �N toN toobtain all possible combinations of sensitivity and specificity.
To aid in the identification of important variables associ-ated with angle closure for a particular patient, standardizedparameters were used, and these are denoted with anasterisk as anterior chamber volume*, anterior chamberwidth*, iris thickness at 750mm*, iris area*, anterior cham-ber area*, and lens vault* (Table 1). The formula for thescore thenwas re-expressed in terms of the standardized var-iables. For a particular subject, the values of the product oftheir standardized variables and the corresponding coeffi-cients in the re-expressed score can be plotted to assessthe relative contributions of each eye biometry measure-ment to the angle-closure score. Because anterior chamberarea and anterior chamber volume are correlated strongly,their effects are closely linked. To enable interpretation,the value of the sum of the corresponding products can beplotted to assess the joint effect of anterior chamber areaand volume. If a particular component of the score is largerelative to the other components, then the correspondingvariable is a substantial contributing factor to their risk.
34 AMERICAN JOURNAL OF
Validation of the angle closure score. To validate the angleclosure score, we tested it on an independent group consist-ing of 178 hospital-based subjects with gonioscopic angleclosure (as defined previously) recruited as part of anongoing randomized controlled trial (NCT00347178,clinicaltrials.gov)16 and 301 normal control subjects whowere recruited from an ongoing population-based study.17
The criteria for normals were an intraocular pressure ofless than 21 mm Hg with open angles, healthy opticnerves, normal visual fields, and no previous intraocularsurgery. AS OCT imaging was performed before laserperipheral iridotomy in the angle-closure subjects.
RESULTS
A TOTAL OF 2047 SUBJECTS WERE RECRUITED INTO THE
study, of whom 679 (33.2%) were excluded for thefollowing reasons: 11 (0.54%) could not undergo gonio-scopy, 97 (4.7%) had incomplete demographic or biometricmeasurements, 62 (3.0%) could not complete the AS OCTexamination or had poor quality AS OCT images, 42(2.1%) had software delineation errors, and 467 (22.8%)had scleral spurs that were not clearly visible on AS OCTimages. Therefore, data from 1368 subjects (66.8%) wereincluded in the analysis. Of these, 750 (54.8%) werewomen, and 1232 (90.0%) were Chinese. The mean age6 standard deviation was 62.4 6 7.7 years. There wereno significant differences in race, spherical equivalentrefraction, intraocular pressure, or axial length, but includedparticipants were younger (P < .001), had shallower ACD(P ¼ .02), and were more likely to be women (P ¼ .03).There were 295 subjects (21.6%) with gonioscopic angle
closure. Persons with angle closure were older; had smallerACD; had smaller anterior chamber width, area, andvolume; had greater lens vault; and had thicker irides(Table 2). Findings were similar when only Chinese per-sons were analyzed.
� ANGLECLOSURE SCOREANDESTIMATED PROBABILITY:
The shifted linear combination of the AS OCT-derived
JANUARY 2014OPHTHALMOLOGY
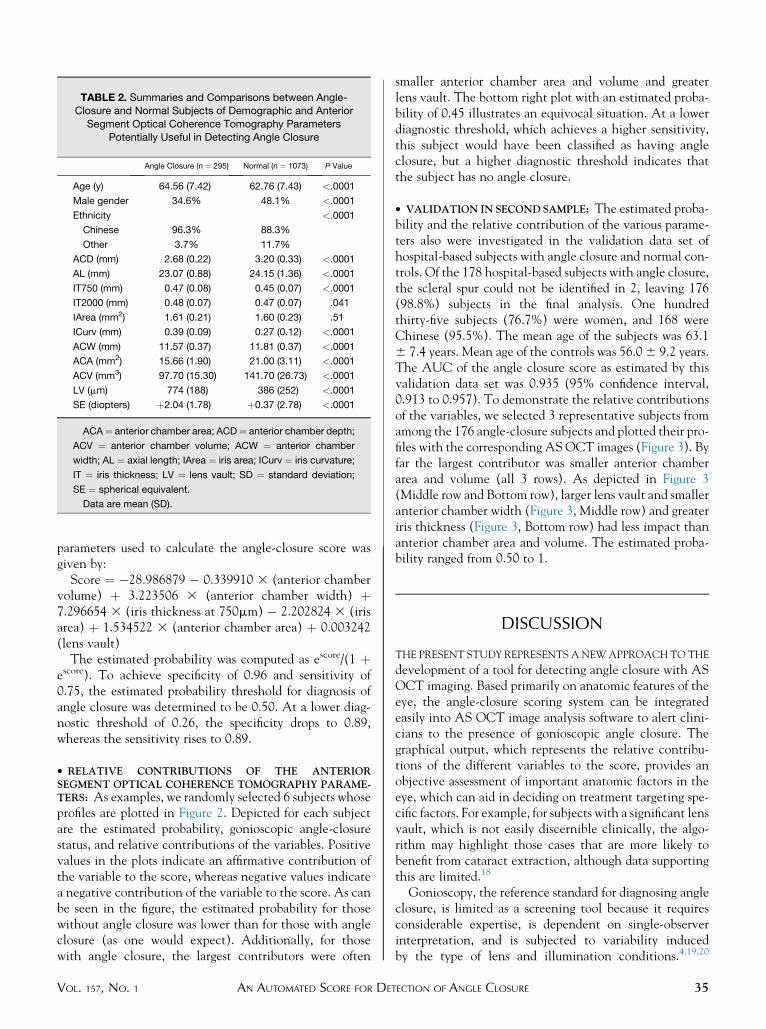
TABLE 2. Summaries and Comparisons between Angle-Closure and Normal Subjects of Demographic and Anterior
Segment Optical Coherence Tomography Parameters
Potentially Useful in Detecting Angle Closure
Angle Closure (n ¼ 295) Normal (n ¼ 1073) P Value
Age (y) 64.56 (7.42) 62.76 (7.43) <.0001
Male gender 34.6% 48.1% <.0001
Ethnicity <.0001
Chinese 96.3% 88.3%
Other 3.7% 11.7%
ACD (mm) 2.68 (0.22) 3.20 (0.33) <.0001
AL (mm) 23.07 (0.88) 24.15 (1.36) <.0001
IT750 (mm) 0.47 (0.08) 0.45 (0.07) <.0001
IT2000 (mm) 0.48 (0.07) 0.47 (0.07) .041
IArea (mm2) 1.61 (0.21) 1.60 (0.23) .51
ICurv (mm) 0.39 (0.09) 0.27 (0.12) <.0001
ACW (mm) 11.57 (0.37) 11.81 (0.37) <.0001
ACA (mm2) 15.66 (1.90) 21.00 (3.11) <.0001
ACV (mm3) 97.70 (15.30) 141.70 (26.73) <.0001
LV (mm) 774 (188) 386 (252) <.0001
SE (diopters) þ2.04 (1.78) þ0.37 (2.78) <.0001
ACA¼ anterior chamber area; ACD¼ anterior chamber depth;
ACV ¼ anterior chamber volume; ACW ¼ anterior chamber
width; AL ¼ axial length; IArea ¼ iris area; ICurv ¼ iris curvature;
IT ¼ iris thickness; LV ¼ lens vault; SD ¼ standard deviation;
SE ¼ spherical equivalent.
Data are mean (SD).
parameters used to calculate the angle-closure score wasgiven by:
Score ¼ �28.986879 � 0.339910 3 (anterior chambervolume) þ 3.223506 3 (anterior chamber width) þ7.296654 3 (iris thickness at 750mm) � 2.202824 3 (irisarea) þ 1.534522 3 (anterior chamber area) þ 0.003242(lens vault)
The estimated probability was computed as escore/(1 þescore). To achieve specificity of 0.96 and sensitivity of0.75, the estimated probability threshold for diagnosis ofangle closure was determined to be 0.50. At a lower diag-nostic threshold of 0.26, the specificity drops to 0.89,whereas the sensitivity rises to 0.89.
� RELATIVE CONTRIBUTIONS OF THE ANTERIORSEGMENT OPTICAL COHERENCE TOMOGRAPHY PARAME-TERS: As examples, we randomly selected 6 subjects whoseprofiles are plotted in Figure 2. Depicted for each subjectare the estimated probability, gonioscopic angle-closurestatus, and relative contributions of the variables. Positivevalues in the plots indicate an affirmative contribution ofthe variable to the score, whereas negative values indicatea negative contribution of the variable to the score. As canbe seen in the figure, the estimated probability for thosewithout angle closure was lower than for those with angleclosure (as one would expect). Additionally, for thosewith angle closure, the largest contributors were often
VOL. 157, NO. 1 AN AUTOMATED SCORE FOR DE
smaller anterior chamber area and volume and greaterlens vault. The bottom right plot with an estimated proba-bility of 0.45 illustrates an equivocal situation. At a lowerdiagnostic threshold, which achieves a higher sensitivity,this subject would have been classified as having angleclosure, but a higher diagnostic threshold indicates thatthe subject has no angle closure.
� VALIDATION IN SECONDSAMPLE: The estimated proba-bility and the relative contribution of the various parame-ters also were investigated in the validation data set ofhospital-based subjects with angle closure and normal con-trols. Of the 178 hospital-based subjects with angle closure,the scleral spur could not be identified in 2, leaving 176(98.8%) subjects in the final analysis. One hundredthirty-five subjects (76.7%) were women, and 168 wereChinese (95.5%). The mean age of the subjects was 63.16 7.4 years. Mean age of the controls was 56.06 9.2 years.The AUC of the angle closure score as estimated by thisvalidation data set was 0.935 (95% confidence interval,0.913 to 0.957). To demonstrate the relative contributionsof the variables, we selected 3 representative subjects fromamong the 176 angle-closure subjects and plotted their pro-files with the corresponding ASOCT images (Figure 3). Byfar the largest contributor was smaller anterior chamberarea and volume (all 3 rows). As depicted in Figure 3(Middle row and Bottom row), larger lens vault and smalleranterior chamber width (Figure 3, Middle row) and greateriris thickness (Figure 3, Bottom row) had less impact thananterior chamber area and volume. The estimated proba-bility ranged from 0.50 to 1.
DISCUSSION
THE PRESENT STUDY REPRESENTS ANEWAPPROACHTO THE
development of a tool for detecting angle closure with ASOCT imaging. Based primarily on anatomic features of theeye, the angle-closure scoring system can be integratedeasily into AS OCT image analysis software to alert clini-cians to the presence of gonioscopic angle closure. Thegraphical output, which represents the relative contribu-tions of the different variables to the score, provides anobjective assessment of important anatomic factors in theeye, which can aid in deciding on treatment targeting spe-cific factors. For example, for subjects with a significant lensvault, which is not easily discernible clinically, the algo-rithm may highlight those cases that are more likely tobenefit from cataract extraction, although data supportingthis are limited.18
Gonioscopy, the reference standard for diagnosing angleclosure, is limited as a screening tool because it requiresconsiderable expertise, is dependent on single-observerinterpretation, and is subjected to variability inducedby the type of lens and illumination conditions.4,19,20
35TECTION OF ANGLE CLOSURE
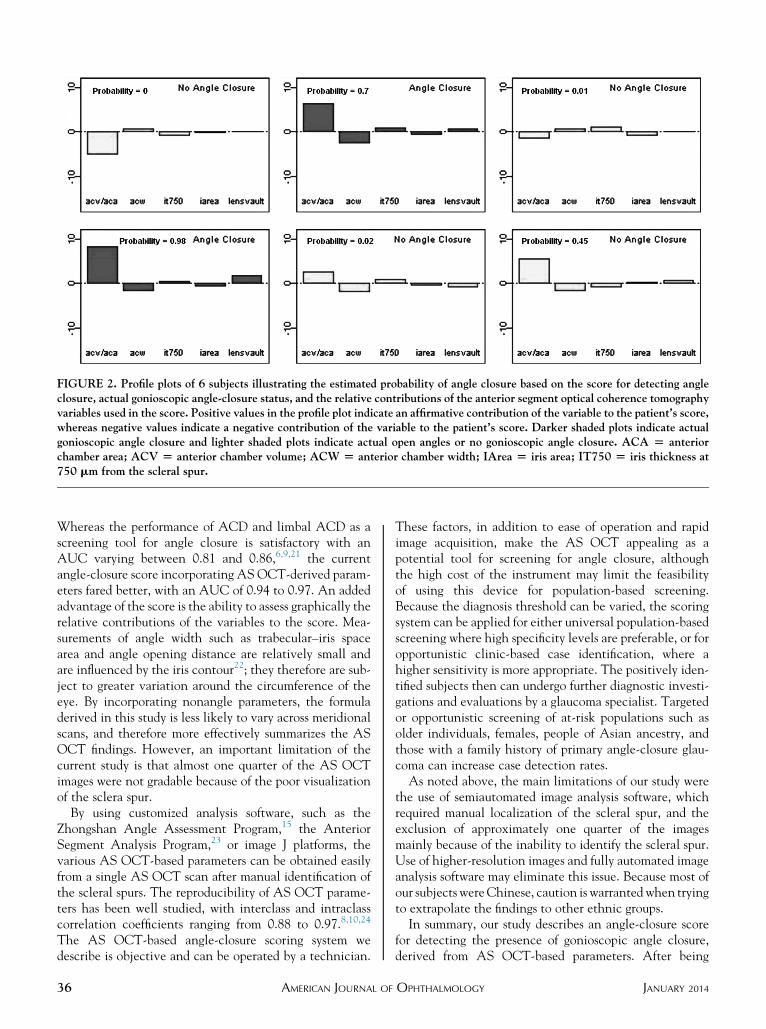
FIGURE 2. Profile plots of 6 subjects illustrating the estimated probability of angle closure based on the score for detecting angleclosure, actual gonioscopic angle-closure status, and the relative contributions of the anterior segment optical coherence tomographyvariables used in the score. Positive values in the profile plot indicate an affirmative contribution of the variable to the patient’s score,whereas negative values indicate a negative contribution of the variable to the patient’s score. Darker shaded plots indicate actualgonioscopic angle closure and lighter shaded plots indicate actual open angles or no gonioscopic angle closure. ACA [ anteriorchamber area; ACV [ anterior chamber volume; ACW [ anterior chamber width; IArea [ iris area; IT750 [ iris thickness at750 mm from the scleral spur.
Whereas the performance of ACD and limbal ACD as ascreening tool for angle closure is satisfactory with anAUC varying between 0.81 and 0.86,6,9,21 the currentangle-closure score incorporating AS OCT-derived param-eters fared better, with an AUC of 0.94 to 0.97. An addedadvantage of the score is the ability to assess graphically therelative contributions of the variables to the score. Mea-surements of angle width such as trabecular–iris spacearea and angle opening distance are relatively small andare influenced by the iris contour22; they therefore are sub-ject to greater variation around the circumference of theeye. By incorporating nonangle parameters, the formuladerived in this study is less likely to vary across meridionalscans, and therefore more effectively summarizes the ASOCT findings. However, an important limitation of thecurrent study is that almost one quarter of the AS OCTimages were not gradable because of the poor visualizationof the sclera spur.
By using customized analysis software, such as theZhongshan Angle Assessment Program,15 the AnteriorSegment Analysis Program,23 or image J platforms, thevarious AS OCT-based parameters can be obtained easilyfrom a single AS OCT scan after manual identification ofthe scleral spurs. The reproducibility of AS OCT parame-ters has been well studied, with interclass and intraclasscorrelation coefficients ranging from 0.88 to 0.97.8,10,24
The AS OCT-based angle-closure scoring system wedescribe is objective and can be operated by a technician.
36 AMERICAN JOURNAL OF
These factors, in addition to ease of operation and rapidimage acquisition, make the AS OCT appealing as apotential tool for screening for angle closure, althoughthe high cost of the instrument may limit the feasibilityof using this device for population-based screening.Because the diagnosis threshold can be varied, the scoringsystem can be applied for either universal population-basedscreening where high specificity levels are preferable, or foropportunistic clinic-based case identification, where ahigher sensitivity is more appropriate. The positively iden-tified subjects then can undergo further diagnostic investi-gations and evaluations by a glaucoma specialist. Targetedor opportunistic screening of at-risk populations such asolder individuals, females, people of Asian ancestry, andthose with a family history of primary angle-closure glau-coma can increase case detection rates.As noted above, the main limitations of our study were
the use of semiautomated image analysis software, whichrequired manual localization of the scleral spur, and theexclusion of approximately one quarter of the imagesmainly because of the inability to identify the scleral spur.Use of higher-resolution images and fully automated imageanalysis software may eliminate this issue. Because most ofour subjects wereChinese, caution is warranted when tryingto extrapolate the findings to other ethnic groups.In summary, our study describes an angle-closure score
for detecting the presence of gonioscopic angle closure,derived from AS OCT-based parameters. After being
JANUARY 2014OPHTHALMOLOGY
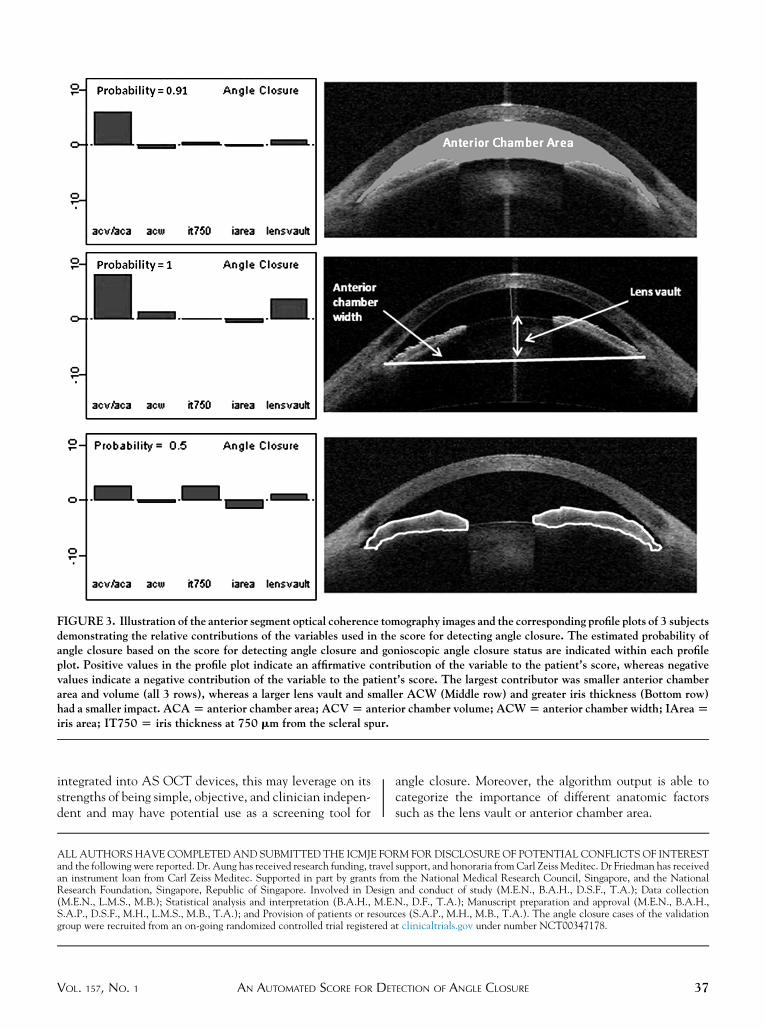
FIGURE 3. Illustration of the anterior segment optical coherence tomography images and the corresponding profile plots of 3 subjectsdemonstrating the relative contributions of the variables used in the score for detecting angle closure. The estimated probability ofangle closure based on the score for detecting angle closure and gonioscopic angle closure status are indicated within each profileplot. Positive values in the profile plot indicate an affirmative contribution of the variable to the patient’s score, whereas negativevalues indicate a negative contribution of the variable to the patient’s score. The largest contributor was smaller anterior chamberarea and volume (all 3 rows), whereas a larger lens vault and smaller ACW (Middle row) and greater iris thickness (Bottom row)had a smaller impact. ACA[ anterior chamber area; ACV[ anterior chamber volume; ACW[ anterior chamber width; IArea[iris area; IT750 [ iris thickness at 750 mm from the scleral spur.
integrated into AS OCT devices, this may leverage on itsstrengths of being simple, objective, and clinician indepen-dent and may have potential use as a screening tool for
VOL. 157, NO. 1 AN AUTOMATED SCORE FOR DE
angle closure. Moreover, the algorithm output is able tocategorize the importance of different anatomic factorssuch as the lens vault or anterior chamber area.
ALL AUTHORS HAVE COMPLETED AND SUBMITTED THE ICMJE FORM FOR DISCLOSURE OF POTENTIAL CONFLICTS OF INTERESTand the following were reported. Dr. Aung has received research funding, travel support, and honoraria from Carl Zeiss Meditec. Dr Friedman has receivedan instrument loan from Carl Zeiss Meditec. Supported in part by grants from the National Medical Research Council, Singapore, and the NationalResearch Foundation, Singapore, Republic of Singapore. Involved in Design and conduct of study (M.E.N., B.A.H., D.S.F., T.A.); Data collection(M.E.N., L.M.S., M.B.); Statistical analysis and interpretation (B.A.H., M.E.N., D.F., T.A.); Manuscript preparation and approval (M.E.N., B.A.H.,S.A.P., D.S.F., M.H., L.M.S., M.B., T.A.); and Provision of patients or resources (S.A.P., M.H., M.B., T.A.). The angle closure cases of the validationgroup were recruited from an on-going randomized controlled trial registered at clinicaltrials.gov under number NCT00347178.
37TECTION OF ANGLE CLOSURE
REFERENCES
1. Quigley HA, Broman AT. The number of people with glau-coma worldwide in 2010 and 2020. Br J Ophthalmol 2006;90(3):262–267.
2. Hu Z, Zhao ZL, Dong FT. An epidemiological investigation ofglaucoma in Beijing and Shun-Yi county. Chin J Ophthalmol1989;25:115–118.
3. Congdon NG, Quigley HA, Hung PT, Wang TH, Ho TC.Screening techniques for angle-closure glaucoma in ruralTaiwan. Acta Ophthalmol Scand 1996;74(2):113–119.
4. Foster PJ, Devereux JG, Alsbirk PH, et al. Detection of gonio-scopically occludable angles and primary angle closure glau-coma by estimation of limbal chamber depth in Asians:modified grading scheme.Br JOphthalmol 2000;84(2):186–192.
5. Devereux JG, Foster PJ, Baasanhu J, et al. Anterior chamber depthmeasurement as a screening tool for primary angle-closure glaucomainanEastAsianpopulation.ArchOphthalmol2000;118(2):257–263.
6. Lavanya R, Foster PJ, Sakata LM, et al. Screening for narrowangles in the Singapore population: evaluation of new noncon-tact screeningmethods.Ophthalmology2008;115(10):1720–1727.
7. Radhakrishnan S, Rollins AM, Roth JE, et al. Real-timeoptical coherence tomography of the anterior segment at1310 nm. Arch Ophthalmol 2001;119(8):1179–1185.
8. Nongpiur ME, Sakata LM, Friedman DS, et al. Novel associ-ation of smaller anterior chamber width with angle closure inSingaporeans. Ophthalmology 2010;117(10):1967–1973.
9. Wu RY, Nongpiur ME, He MG, et al. Association of narrowangles with anterior chamber area and volume measuredwith anterior segment optical coherence tomography. ArchOphthalmol 2011;129(5):569–574.
10. Wang BS, Sakata LM, Friedman DS, et al. Quantitative irisparameters and association with narrow angles. Ophthal-
mology 2010;117(1):11–17.11. Nongpiur ME, He MG, Amerasinghe N, et al. Lens vault,
thickness and position in Chinese subjects with angle closure.Ophthalmology 2011;118(3):474–479.
12. TanGS, HeM, ZhaoW, et al. Determinants of lens vault andassociation with narrow angles in patients from Singapore.Am J Ophthalmol 2012;154(1):39–46.
13. Foo LL, Nongpiur ME, Allen JC, et al. Determinants of anglewidth in Chinese Singaporeans. Ophthalmology 2012;119(2):278–282.
38 AMERICAN JOURNAL OF
14. Nongpiur ME, Haaland BA, Friedman DS, et al. Classifica-tion algorithms based on anterior segment optical coherencetomography measurements for detection of angle closure.Ophthalmology 2013;120(1):48–54.
15. Console JW, Sakata LM, Aung T, Friedman DS, He M.Quantitative analysis of anterior segment optical coherencetomography images: the Zhongshan Angle AssessmentProgram. Br J Ophthalmol 2008;92(12):1612–1616.
16. How AC, Baskaran M, He M, et al. Changes in anteriorsegment morphology after laser peripheral iridotomy: ananterior segment optical coherence tomography study.Ophthalmology 2012;119(7):1383–1387.
17. Lavanya R, Jeganathan VS, Zheng Y, et al. Methodology ofthe Singapore Indian Chinese Cohort (SICC) eye study:quantifying ethnic variations in the epidemiology of eye dis-eases in Asians. Ophthalmic Epidemiol 2009;16(6):325–336.
18. Azuara-Blanco A, Burr JM, Cochran C, et al. Effectiveness inAngle-closure Glaucoma of Lens Extraction (EAGLE) StudyGroup. The effectiveness of early lens extraction with intra-ocular lens implantation for the treatment of primary angle-closure glaucoma (EAGLE): study protocol for a randomizedcontrolled trial. Trials 2011;12:133.
19. Foster PJ, Oen FT, Machin D, et al. The prevalence of glau-coma in Chinese residents of Singapore: a cross-sectionalpopulation survey of the Tanjong Pagar district. ArchOphthalmol 2000;118(8):1105–1111.
20. HeM, Foster PJ, Ge J, et al. Gonioscopy in adult Chinese: theLiwan Eye Study. Invest Ophthalmol Vis Sci 2006;47(11):4772–4779.
21. Nolan WP, Aung T, Machin D, et al. Detection of narrowangles and established angle closure in Chinese residents ofSingapore: potential screening tests. Am J Ophthalmol 2006;141(5):896–901.
22. Radhakrishnan S, Huang D, Smith SD. Optical coherencetomography imaging of the anterior chamber angle. Ophthal-mol Clin North Am 2005;18(3):375–381, vi.
23. Zheng C, Cheung CY, Narayanaswamy A, et al. Pupildynamics in Chinese subjects with angle closure. GraefesArch Clin Exp Ophthalmol 2012;250(9):1353–1359.
24. Muller M, Dahmen G, Porksen E, et al. Anterior chamberangle measurement with optical coherence tomography:intraobserver and interobserver variability. J Cataract RefractSurg 2006;32(11):1803–1808.
JANUARY 2014OPHTHALMOLOGY
Biosketch
Monisha Esther Nongpiur, MD is a Senior Clinical Research Fellow at the Singapore Eye Research Institute. She completed
her Ophthalmology residency training at the All India Institute of Medical Sciences (AIIMS), New Delhi, India. She has
authored several clinical research papers in the field of glaucoma and her research interests include ocular imaging and
ophthalmic genetics.
VOL. 157, NO. 1 38.e1AN AUTOMATED SCORE FOR DETECTION OF ANGLE CLOSURE