Embed Size (px)
Citation preview

http://cre.sagepub.com/Clinical Rehabilitation
http://cre.sagepub.com/content/16/6/630The online version of this article can be found at:
DOI: 10.1191/0269215502cr532oa
2002 16: 630Clin RehabilRuth M Dannenbaum, Stella M Michaelsen, Johanne Desrosiers and Mindy F Levin
strokeDevelopment and validation of two new sensory tests of the hand for patients with
Published by:
http://www.sagepublications.com
can be found at:Clinical RehabilitationAdditional services and information for
http://cre.sagepub.com/cgi/alertsEmail Alerts:
http://cre.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://cre.sagepub.com/content/16/6/630.refs.htmlCitations:
What is This?
- Jun 1, 2002Version of Record >>
at National Dong Hwa University on March 25, 2014cre.sagepub.comDownloaded from at National Dong Hwa University on March 25, 2014cre.sagepub.comDownloaded from

Clinical Rehabilitation 2002; 16: 630–639
© Arnold 2002 10.1191/0269215502cr532oa
Address for correspondence: Ruth Dannenbaum, CRIR,Institut de réadaptation de Montréal, 6300 Darlington,Montréal, Québec H3S 2J4. e-mail: [email protected]
Development and validation of two new sensorytests of the hand for patients with strokeRuth M Dannenbaum Centre de recherche interdisciplinaire en réadaptation, Institut de réadaptation de Montréal,Stella M Michaelsen Centre de recherche interdisciplinaire en réadaptation, Institut de réadaptation de Montréal, Écolede réadaptation, Université de Montréal, Johanne Desrosiers Centre de recherche en gérontologie et gériatrie, Institutuniversitaire de gériatrie de Sherbrooke and Université de Sherbrooke, Faculté de Medecine Québec and Mindy F LevinCentre de recherche interdisciplinaire en réadaptation, Institut de réadaptation de Montréal; École de réadaptation,Université de Montréal, Montréal, Québec, Canada
Received 22nd January 2001; returned for revisions 13th March 2001; revised manuscript accepted 24th May 2001.
Objective: To establish validity and reliability of two new sensory testsevaluating moving (MTP) and sustained (STP) touch-pressure and theirrelationship to hand function for patients with stroke. The STP had fourcomponents in which a light or heavy ball was applied passively or heldactively.Participants: Twenty-eight participants with hemiparesis (1–109 months) fromrehabilitation hospitals or outpatient programmes.Design: Content validity was established. Then reliability and concurrent andconstruct validity were determined. Sensation was compared with handfunctional ability using the Modi�ed Moberg recognition task, the Box andBlock test and one task of the TEMPA test. Results: Reliability: Both types of reliability were signi�cant for MTP (ICC =0.92) and all components of STP (ICC = 0.62 to 0.92). Concurrent validity:MTP and STP correlated signi�cantly (r = –0.39 to –0.83) with theSemmes–Weinstein Mono�lament test used as a ‘gold standard’ comparison.Construct validity: MTP was signi�cantly related to Moberg (r = 0.49). Three offour components of STP correlated with TEMPA (r = 0.49–0.53) and Moberg(0.45–0.71). Only STP (heavy ball) correlated with Box and Block (0.42–0.48).Of the four components of STP, only the passive STP (light ball) was notrelated to hand function.Conclusion: The new sensory tests of moving, and three components ofsustained touch-pressure were reliable. The passive STP (light ball) wasdiscarded. All but this test were relevant to the two functional roles ofsensation: exploration for MTP and dexterity during holding for STP.
at National Dong Hwa University on March 25, 2014cre.sagepub.comDownloaded from

New sensory tests for stroke 631
Introduction
Stroke, with an incidence of 600 000 new casesper year in the United States,1 is one of the lead-ing causes of impairment and disability in NorthAmerica. Among stroke survivors, there is oftena major loss of upper limb motor function. A con-tributing factor to hand impairment relates to dis-turbances of sensation in approximately 60% ofpatients.2 Stroke-related brain damage may resultin different degrees of impairment in sensory dis-criminative modalities in the hand such as stere-ognosis and texture recognition.3,4 Aside frominstrumented tests used for research, current clin-ical evaluation of hand sensation has not beenstandardized in stroke. Furthermore, no test, clin-ical or otherwise, has been related to manualfunctional de�cits in this population.2 There isclearly a need for standardized, reliable and validtests that re�ect the importance of sensoryde�cits to hand dysfunction.
Two of the main functional roles of cutaneoussensation in the hand are to provide informationabout the environment during exploration tasksand to provide feedback for �ne precision skillsduring holding and manipulation tasks. The �rstrole, exploratory function, has been de�ned asthe ability to identify and discriminate sensoryfeatures of the environment.5 Usually, cutaneousinformation from the tips of the �ngers are the�rst signals allowing a person to appreciate andinterpret the environment. For example, the �n-gertips and �nger pads provide crucial informa-tion to search for and remove a coin from apocket. Information provided by the �ngertips isused to appreciate the differences of material,shape and size of the coin from its surroundingenvironment, then to localize it on the appropri-ate skin surfaces of the thumb and index inpreparation for grasping and removing the coinfrom the pocket.
The second role of cutaneous sensation relatesto dexterity during holding tasks. Many activitiesof daily living require precise grasping to hold anobject during manipulation. For example, whenholding a fork, the ability to maintain a uniformgrip is important. During holding, small correc-tions of the skin surface in contact with the objectand �ne adjustments of the amount of forceapplied by the �ngers occur in response to cuta-
neous feedback. Such afferent signals guidemotor responses in goal-directed grasping andobject manipulation.6
Several techniques to measure sensory func-tion in neurological patients have been described.The most commonly used method is the standardneurological evaluation. In this test of light touchappreciation, the patient reports on the similar-ity of the intensities of sensations evoked by thetouch of a cotton ball on different skin surfacesof the involved and uninvolved side of the body.7
This evaluation provides crude information andis useful as a screening technique but its rele-vance to hand motor dysfunction has not beendocumented.
Evaluation of the threshold for touch pressureappreciation, performed mainly in research stud-ies, uses Semmes–Weinstein mono�laments.8 Thethreshold for touch pressure sensitivity is deter-mined on the relevant skin surfaces. Similarly, norelationship between this test and function hasbeen shown for holding tasks.
Although it is possible in the clinic to deter-mine the presence or absence of cutaneous sen-sation, valid and reliable sensory tests evaluatingthe intensity of the sensory experience that arealso related to functional ability have not beendescribed for neurological patients. The purposeof this study was to develop two new sensory teststhat have the potential to measure the intensityof cutaneous sensation and to relate sensoryde�cits to the functional ability of the hand inadults who have had a stroke to help provide afocus for rehabilitation.
The tests were developed in consultation withclinical experts and their test–retest, inter-raterreliability as well as validity were evaluated.
Methods
Phase 1: development of the testsAs a �rst step in the development of the new
sensory tests, physical and occupational thera-pists from 20 different neurology departments inthe Montreal area were surveyed by writtenquestionnaire about the frequency and type oftests administered to evaluate sensory functionand functional ability of the hand in strokepatients. Individuals from all departments replied
at National Dong Hwa University on March 25, 2014cre.sagepub.comDownloaded from

632 RM Dannenbaum et al.
of a 2-cm proximal to distal sweeping movementof the brush held at a 30° angle to the skin sur-face. The force applied by the examiner was suf-�cient to just de�ect the brush hairs. Each of thethree brush stimuli was administered six times tothe palmar surface of the distal phalanx of theindex �nger according to a randomization table.Testing was �rst done on the less involved sideand then on the involved side. Several (2–5) prac-tice trials with each brush were given �rst withthe eyes open, then testing was done with eyesclosed or the hands screened from view. Thescore represented the number of correctresponses out of 18 expressed in per cent: 0%indicating no correct responses and 100% indi-cating all responses were correct.
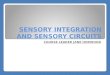
Our second hypothesis was that STP evaluatedthe ability to perceive a sustained touch-pressureinput over time. In a previous study, Dannen-baum and Dykes10 applied four different cylin-drical weights ranging from 23 to 350 g passivelyto the palmar surface of the index �nger for aperiod of 20 seconds. The 20-second period wasused to assess the ability to perceive the sustainedinput over time, a necessary prerequisite for �nemotor adjustments during holding tasks. The testwas modi�ed for this project. Two balls of dif-ferent weights were used instead of cylindricalweights. These were applied passively to thehypothenar surface of the hand (Figure 1B) oractively held by the participant between thumband index �nger. The latter component wasadded since active holding is more closely relatedto function. The light ball was a ping-pong ballweighing 2.14 g and the heavy ball was a golf ballweighing 45.72 g. Thus, the STP had four com-ponents, two passive and two active which alsotook not more than 15 minutes to apply. For thepassive components of STP, each ball was low-ered by a string onto the hand, where it remainedfor a period of 20 seconds. For the active com-ponents, the therapist placed each ball betweenthe participant’s thumb and index �nger. All testswere done without vision by asking participantsto close their eyes. For each test, the participantreported the intensity of the sensation feltaccording to a numerical scale of zero to ten,immediately after the ball was placed on the hand(T1), and then at time intervals of 5, 10, 15 and20 seconds. The intensity was recorded on the
and a total of 55 therapists’ responses were com-piled. The survey revealed that 73% (40) regu-larly tested sensation and that 25% (14) did soonly sometimes. However, 84% (46) of those sur-veyed reported that they used the standard neu-rological evaluation, a test that has no uniformmethod of application and has not been relatedto functional ability. This con�rmed that forstroke patients there is an unanswered need forclinical tests that provide a quanti�able measureof sensation re�ecting the in�uence of sensationon hand functional ability.
The second step consisted of a consensus meet-ing with occupational and physical therapistsworking at the Institut de réadaptation de Mon-tréal and specializing in stroke rehabilitation. Theoutcome of these discussions was that there wasa need for an evaluation, not only of the abilityto feel an object, but of the ability to discrimi-nate its features and to continue to appreciate amaintained sensation over a prolonged period oftime without the sensation fading. This supporteda need to develop measures of moving and sus-tained touch-pressure appreciation.
Two tests were thus developed: The movingtouch-pressure (MTP) test and the sustainedtouch-pressure (STP) test. The MTP test is a tac-tile intensity estimation task using brushes of dif-ferent textures taking a maximum of 15 minutesto complete (Figure 1A). This evaluation wasmodi�ed from the tactile magnitude estimationtask developed for spinal cord-injured patients bySaddiki-Traki et al.9 In that study, testing con-sisted of subjects estimating the magnitude of atactile stimulus on a 10-point scale after the appli-cation of one of three brushes. In the presentstudy, we simpli�ed the testing so that partici-pants only had to indicate either verbally or non-verbally, which brush contacted the skin. Thispermitted patients with communication disordersto participate. Our hypothesis was that MTPevaluated the capacity to discriminate betweensensations generated by brushing movements.The brush hairs (1 cm wide and 2.5 cm long) weresuch that in a healthy population, the lightest wasbarely felt (the soft, Isabey 6236 no. 4), the sec-ond was readily felt as light pressure (themedium, Heinz-Jordan 10B no. 6) and the thirdwas felt as strong but not painful (the hard,Heinz-Jordan 940B no. 6). The stimulus consisted
at National Dong Hwa University on March 25, 2014cre.sagepub.comDownloaded from

New sensory tests for stroke 633
same 10-point scale at the end of 20 seconds (T2).The tests evaluated whether the perception of thesensation faded with time. To determine if theperception had faded during the 20-second
period, T2 was subtracted from T1 and the resul-tant ratio was multiplied by 100 to obtain a per-centage score.
Phase 2: establishment of reliability and validityParticipants
Twenty-eight participants with hemiparesiswere included in the study (Table 1): 17 men(mean age (SD) = 64.8 (13.2) years; range 44–84years); and 11 women (76.3 (7.3) years, range68–91 years.). Sixteen participants had a strokesix months or less prior to the evaluation, while12 had a stroke from 6 to 109 months previously.All participants had been discharged from acutecare facilities. They were recruited from rehabil-itation hospitals and stroke outpatient physio-therapy programmes in the Montreal area.Testing was done by trained physiotherapistsinvolved in the study (RD and SM). Prior to test-ing in each institution, approval was obtainedfrom the institution ethics committee and partic-ipants signed a consent form. All participantswere screened to determine the motor impair-ment level of their hand using the Chedoke–McMaster Stroke Assessment Scale.11 This validand reliable scale rates manual motor perfor-mance on a categorical scale. Participants mustcomplete two of three tasks outlined for eachlevel without assistance to obtain a grade from 1(no hand function) to 7 (normal hand function).The distribution of hand impairment for our par-ticipants is listed in Table 1.
ReliabilityFor reliability testing, MTP and STP were done
three times and by two different raters. Testingprocedures were demonstrated to the ratersbefore they administered them. The �rst rater(RD) tested the same patients twice (R1 andR1a) separated by a one-week interval or less. Insome cases, participants with more chronic stroke(>1 year) were tested up to three weeks apartsince it was unlikely that their sensory statuswould change in this time frame. The secondrater (SM) administered the test once (R2) onthe second testing day. Comparisons between R1and R1a were used to evaluate test–retest relia-bility. The inter-rater reliability was assessed bycomparing results from R1a and R2. Generally,raters required only 1–3 practice trials with each
Figure 1 (A) Moving touch-pressure test (MTP). Thestimulus consisted of a 2-cm proximal-to-distal sweepingmovement of one of three brushes. The brush was heldat a 30° angle to the surface of the skin and applied bythe examiner with a force just suf�cient to de�ect thehairs of the brush. Each brush stimulus was administeredsix times to the distal phalanx of the index �nger in arandomized order. The participant indicated verbally bysaying 1, 2 or 3, which brush was applied. (B) Sustainedtouch-pressure test (STP, passive component). Each oftwo balls was lowered by a string onto the hypothenarsurface of the hand. The intensity of the sensoryexperience was rated by the participant on a scale of 1 to10 after initial contact of the ball with the skin and after20 s to evaluate if the intensity faded. Both MTP and STPwere done with eyes closed. The active component ofthe STP is not shown.
A
B
at National Dong Hwa University on March 25, 2014cre.sagepub.comDownloaded from

634 RM Dannenbaum et al.
test to achieve pro�ciency in testing. The orderof testing on the second day was randomized.
Concurrent validity The Semmes–Weinstein8 test, a standardized
test commonly used in research and sensory eval-uation of peripheral nerve lesions, was used as a‘gold standard’ of touch-pressure thresholdappreciation against which the results of the twonew sensory tests were compared in order toevaluate concurrent validity. This test was usedsince there is currently no comparable clinicaltest for evaluation of sensory dysfunction inpatients with brain lesions. Nylon �laments of dif-ferent diameters were applied perpendicularly tothe palmar surface of the affected index �ngeruntil the �lament bent. The threshold was deter-mined by the method of limits as the mean of the�lament value last perceived in a descendingseries and the �rst perceived in an ascendingseries. A verbal cue to alert the patient that astimulus was about to be applied was providedbefore each stimulus. The testing protocolincluded ‘catch-trials’ in which no stimuluswas presented to control for the effects ofguessing.
Construct validityThree functional tests were used to determine
the construct validity of the new sensorytests. The �rst functional test was the Modi�edMoberg recognition task12 measuring stereogno-sis. The test was performed with the eyes closed.Participants had to locate and identify everydayobjects as they were picked up. The number ofobjects identi�ed within 60 seconds was recorded.Only eight of the ten objects de�ned by Dellon12
were used as two of the objects (small bolt andwasher) were unfamiliar to many participants.The objects included were a screw, nail, wingnut, large bolt, dime and nickel coins, safety pin,paper clip. All of these items were made ofsimilar material to prevent cues of texture ortemperature. Each series was �rst performedusing the uninvolved hand and then the involvedone.
The second functional test, the Box and Blocktest13 is a test of gross manual dexterity. The taskwas to move as many 1-cm3 wooden blocks aspossible from one side of the box to the other,over a 15.2-cm-high partition in 60 seconds. Thenumber of blocks moved was recorded. The taskwas done twice with the uninvolved hand andthen twice with the involved hand. Blocks weremoved from the side of the box nearest the hand
Table 1 Demographic characteristics of the participants and their scores obtained with the scales (n = 28)
Continuous variables:Mean (SD) Range
Age (years) 69.3 (12.5) 34–91Time since the stroke (months) 23.5 (3.1) 1–109TEMPA 8 8.7 (6.8) 0–15Moberg – identify (number of objects) 3.7 (3.9) 0–8Box and Block Test (number of blocks/min) 21.9 (18.8) 0–55Semmes–Weinstein Mono�laments (number of) 4.24 (1.24) 2.83–6.45
Categorical variables:Frequency (%)
GenderWomen 11 (39.3)Men 17 (60.7)
Side of the strokeRight 15 (53.6)Left 13 (46.4)
Chedoke–McMaster Stroke AssessmentHand: 2–3 9 (32.1)
4–5 4 (14.3)6–7 15 (53.6)
at National Dong Hwa University on March 25, 2014cre.sagepub.comDownloaded from

New sensory tests for stroke 635
At the same time, the experimenter requestedthe needed response.
Data analysis and statisticsReliability for MTP and STP was analysed
using intraclass correlation coef�cients (ICC) andtheir 95% con�dence intervals (CI). Fortest–retest reliability, the ICC was based on aone-way random effects analysis of variance17
(SPSS 9.0). For inter-rater reliability, a two-waymixed model with absolute agreement was used.Paired t-tests on the differences in the scoresobtained at time 1 and time 2 or by R1 and R2were used to test the presence of a bias betweenmeasurements.
To determine concurrent validity, the scores ofeach of the new sensory tests were correlated tothe criterion Semmes–Weinstein measure usingSpearman rank-order correlation coef�cients. Asigni�cance level of p < 0.05 was used for all tests.Spearman rank-order correlations between thenew sensory tests and tests of hand functionalability (Moberg, Box and Blocks, TEMPA 8)were calculated to determine the construct valid-ity examining the role of sensation in hand func-tion. We hypothesized that there would be arelationship between the MTP and the functionaltask, Modi�ed Moberg recognition task, sincesuccess on the Moberg test requires the ability toexplore, �nd and appreciate object features inorder to identify it using moving touch-pressureinputs. The MTP was not expected to be relatedto holding tasks (Box and Block and TEMPA 8).On the other hand, we expected the STP to berelated to the TEMPA 8, a task which uses sus-tained cutaneous feedback while holding andhandling coins. This test was not expected to cor-relate with Box and Blocks, which is a grossmotor task in which sensory loss can be com-pensated for by vision.
Results
Reliability The test–retest reliability for rater 1 was sig-
ni�cant for MTP and all four components ofthe STP. The ICC for MTP was 0.92 and rangedfrom 0.62 to 0.88 for STP. The passive STP: lightball was the weakest with an ICC of 0.62 and
to the opposite side so that movements werealways made from the ipsilateral to the con-tralateral direction.
Finally, the third functional test, the TEMPAUpper Extremity Performance Test for theElderly,14 was used to evaluate functional abilityon nine tasks that represent skills needed in dailylife. Five of the tasks are bilateral and four areunilateral. Only one unilateral task (Task 8;TEMPA 8) was used for analysis. In this task, theparticipant had to pick up four coins of differentsizes from a table and place them, one at a time,in a vertical slot at approximately eye level. Thistask was chosen since it is a �ne motor manipu-lative task presumably requiring cutaneous feed-back from the �ngertips.14 Performance wasmeasured on a task analysis scale and on a func-tional scale. The task analysis scale quanti�es thedegree of dif�culty to perform the task on four-point scales measuring amplitude of movement,force, precision of gross and �ne movement andprehension, taking into account movement speed.The functional scale assesses performance of thetask according to four levels where 0 indicatessuccessful completion without hesitation or dif�-culty, as instructed or demonstrated; 1 indicatesthat the task was executed completely, but withsome hesitation or dif�culty; 2 denotes that thetask was partially executed (more than 25%) orcertain steps were executed with major dif�cul-ties necessitating repeated efforts; and 3 indicatesthat only up to 25% of the task could be per-formed. Scores for each section were addedtogether with higher scores indicating better per-formance. The TEMPA has good test–retest(intraclass correlation coef�cient (ICC) 0.70–1)and inter-rater (ICC varying from 0.75 to 1) reli-ability.15 In addition, concomitant criteria andconstruct validity studies have con�rmed itsvalidity.16
Testing paradigmOn the �rst testing day, in addition to the MTP
and STP, the Semmes–Weinstein and two func-tional tests (Moberg and Box and Blocks) wereadministered by rater 1. On the second day, theMTP, STP and the TEMPA 8 were administered.All testing was done in a quiet environment withthe participant seated in front of a table. All testswere done without vision and with verbal cueing.
at National Dong Hwa University on March 25, 2014cre.sagepub.comDownloaded from

636 RM Dannenbaum et al.
The MTP had a correlation of –0.83, and for STPthe values ranged from –0.39 (passive STP: lightball) to –0.80 (active STP: heavy ball) (Table 4).
Construct validityMTP and STP scores were examined to analyse
their relationship to the three functional tasks.The relationship between MTP and exploratoryfunction, as measured by the Moberg, was sig-ni�cant (r = 0.49; p < 0.01) but, as anticipated,there was no relationship between this sensorytest and the other two functional measures(Table 4). On the other hand, three of the fourcomponents of STP (except for the passive STP:light ball) correlated with TEMPA 8 and Moberg
large 95% con�dence limits (0.34–0.80) (Table 2).The inter-rater reliability was signi�cant for
the MTP and all four components of the STP(Table 3). The ICC for MTP was 0.92 and forSTP, it ranged from 0.66 to 0.94. Again, the pas-sive STP: light ball had the weakest correlationwith an ICC of 0.66 (95% CI 0.40–0.82). For bothtypes of reliability, paired t-tests indicated thatthere was no signi�cant bias between sessions orraters.
Validity Concurrent validity
Both the new sensory tests were signi�cantlyinversely correlated with the Semmes–Weinstein.
Table 2 Mean (SD) scores for rater 1 on two test days and test–retest reliability for the moving touch-pressure (MTP)and four components of the sustained touch-pressure (STP) tests (n = 28)
T1 T2 T2–T1 Test–retestMean (SD) Mean (SD) Mean (SD) ICC
p-valuea (95% CI)
MTP 65.5 (33.3) 66.8 (34.4) –1.3 (14.1) 0.92–0.62 0.83–0.96
STP – passive heavy ball 58.7 (43.3) 59.3 (42.9) –0.6 (21.8) 0.88–0.88 0.75–0.94
STP – passive light ball 45.8 (42.6) 46.0 (41.9) –0.2 (37.3) 0.62–0.98 0.34–0.80
STP – active heavy ball 70.3 (42.8) 63.7 (43.1) –6.6 (24.0) 0.84–0.15 0.69–0.92
STP – active light ball 65.0 (44.2) 64.3 (44.6) –0.8 (23.7) 0.86–0.86 0.73–0.93
aPaired t–test.
Table 3 Mean (SD) scores for raters 1 and 2 on the same test day and inter-rater reliability of the moving touch-pressure (MTP) and four components of the sustained touch-pressure (STP) tests
Rater 1 Rater 2 R1–R2 Inter-raterMean (SD) Mean (SD) Mean (SD) ICC
p-valuea (95% CI)
MTP 66.8 (34.4) 63.8 (32.2) –3.1 (12.6) 0.92–0.16 0.85–0.96
STP – passive heavy ball 59.3 (42.9) 59.9 (43.3) –0.6 (15.5) 0.94–0.84 0.87–0.97
STP – passive light ball 46.0 (41.9) 51.8 (45.7) –5.7 (36.2) 0.66–0.40 0.40–0.82
STP – active heavy ball 63.7 (43.1) 63.8 (41.9) –0.04 (15.7) 0.94–0.99 0.86–0.97
STP – active light ball 64.3 (44.6) 66.1 (42.4) –1.8 (22.3) 0.87–0.66 0.75–0.94
aPaired t–test.
at National Dong Hwa University on March 25, 2014cre.sagepub.comDownloaded from

New sensory tests for stroke 637
the ability to discriminate three different movingtouch-pressure inputs while the STP evaluatedthe time course of the sensory adaptation, in par-ticular, the fading of sensory appreciation duringsustained touch during a holding task.
The lowest reliability scores were found for thepassive STP performed with the light ball, sug-gesting that this component of the STP shouldnot be included in the testing battery. The weakreliability may be due to the fact that the lightweight of the ball was near or at the thresholdfor perception in individuals with decreased sen-sation. If the intensity of the stimulus on the handwas just appreciable on �rst contact, estimationof the change in sensation over time may nothave been possible.
Our results showed high inter-rater reliabilityfor both tests when two different raters evaluatedsensation in the same patients on the same day.Since rater 1’s scores had good test–retest relia-bility, it is assumed that a similar inter-observerreliability would also be calculated between datafrom different raters on different days, a situa-tion often occurring in the clinic. To ensure reli-ability of the two tests, it is necessary to ensurethat all therapists perform the tests in exactly thesame manner. To ensure consistency of applica-tion, written guidelines outlining test proceduresare available. In addition, some variables in testapplication should be controlled. For the MTP,variability in measurement may be related to dif-ferences in the size of the skin surface stimulatedby the brush (the area on the �ngertip), theamount of pressure applied to each brush and thespeed of stimulus application. For the STP, mea-surement variability may also be in�uenced byintensity and duration of the stimulus. On exam-
and only two components (STP: heavy ball,active and passive) correlated with the Box andBlock. The Box and Block had lower overall cor-relation scores with both MTP and STP.
Discussion
The two new tests of sensation, moving touch-pressure and sustained touch-pressure, weredeveloped for the clinical environment to evalu-ate hand sensation speci�cally for patients withstroke. These tests needed to be developed asmost tests currently used to evaluate sensationstudy sensory recovery in patients with periph-eral nerve lesions.12,18 Such tests are used todetermine the severity of the nerve lesion and therate of recovery of modality speci�c nerve types.These are not the key concerns in evaluation ofsensation in patients with brain lesions. Rather,the focus is on the ability to perceive, appreciateand interpret sensory events. The MTP related to
Clinical messages
� Moving touch-pressure and sustained touch-pressure can be assessed using balls andbrushes.
� Tests show these to be reasonably reliable.� Tests show good concurrent validity and
moderate construct validity.� This is a �rst step in relating the two roles
of sensation to functional de�cits in thehand in patients with stroke.
� Responsiveness has yet to be determined.
Table 4 Correlation between moving touch-pressure (MTP) and sustained touch-pressure (STP) test scores andmeasures of functional ability in the hand (n = 28)
Test SW MI BBT TEMPA 8
MTP –0.83*** 0.49** 0.25 –0.34STP – passive heavy ball –0.58*** 0.45* 0.42* –0.53**STP – passive light ball –0.39 * 0.21 0.17 –0.35STP – active heavy ball –0.80*** 0.71*** 0.48** –0.50*STP – active light ball –0.67*** 0.54** 0.37 –0.49*
***p < 0.001; **0.001 < p < 0.01; *0.01 < p < 0.05.SW, Semmes–Weinstein test; MI, Modi�ed Moberg recognition task; BBT, Box and Block Test; TEMPA 8: TEMPAUpper Extremity Performance Test for the Elderly, handling coins.
at National Dong Hwa University on March 25, 2014cre.sagepub.comDownloaded from

638 RM Dannenbaum et al.
to guide holding during precision skills. However,despite signi�cant correlations between thesevariables, the explained variance of the associa-tions was only around 25%. This suggests that thenew tests should be adapted to improve theirconstruct validity or, more likely, functionalde�cits in the hand may not be only related tode�cits in the two sensory modalities that wemeasured.
As a next step in the development of the tests,it is necessary to examine their construct validitybefore studying their responsiveness to changesin sensory ability with recovery.
Acknowledgements The authors would like to thank Dr RW
Dykes, Dr CE Chapman and Lois Finch for theirassistance and comments on the manuscript.Thanks are also extended to staff and patients atthe Julius Richardson Rehabilitation Hospitaland at the Stroke Group at Temple EmanuelBeth Shalom, Montreal, Quebec. We gratefullyacknowledge funding support from the MedicalResearch Council of Canada.
References
1 Galski T, Bruno RL, Zorowitz R, Walker A.Predicting length of stay, functional outcome, andaftercare in the rehabilitation of stroke patients.Stroke 1993; 24: 1794–800.
2 Winward CE, Halligan PW, Wade DT. Currentpractise and clinical relevance of somatosensoryassessment after stroke. Clin Rehabil 1999; 13:48–55.
3 Lincoln NB, Jackson JM, Adams SA. Reliabilityand revision of the Nottingham Sensory Assessmentfor stroke patients. Physiotherapy 1998; 84:358–65.
4 Bassetti C, Bogousslavsky J, Regli F. Sensorysyndromes in parietal stroke. Neurology 1993; 43:1942–49.
5 Carey LM, Matyas TA, Oke LE. Sensory loss instroke patients: effective training in tactile andproprioceptive discrimination. Arch Phys MedRehabil 1993; 74: 602–11.
6 Johansson RS, Cole KJ. Sensory-motor coordinationduring grasping and manipulative actions. Curr OpinNeurobiol 1992; 2: 815–23.
7 Kunesch E, Binkofski F, Steinmetz H, Freund H.The pattern of motor de�cits in relation to the siteof stroke lesions. Eur Neurol 1995; 35: 20–26.
8 Bell-Krotowski J, Tomancik E. The repeatability of
ining the raw data, the STP began to fade afterapproximately 15 seconds in several participantswith sensory de�cits and continued to fade after20 seconds. It is possible that our testing periodwas too short to measure the full extent of fad-ing. Thus, it may be advisable to extend the test-ing period to 30 seconds or longer.
Another variable to control in the STP is theintensity and variability of the force exerted bythe �ngers on the ball during the active holdingtask. This force may not be steadily maintainedthroughout the 20-second period. Studies haveshown that subjects with experimentally inducedsensory de�cits vary the amount of force appliedto the �ngers during grip to compensate slippageof the object on the skin surface.19 It was possi-ble that if sensation had begun to fade, then thepatient may have compensated by increasing thepressure of the �ngers on the ball or by makingsmall to-and-fro movements of the ball. Thiswould result in an increase in the amount of pres-sure of the object against the skin, the stimula-tion of a different skin surface and/or a changein the sense of effort exerted to maintain theobject between the �ngers. These factors, onlyassociated with active holding, would have beenindistinguishable and may have been a source ofvariability in the participant’s report of the levelof sensation. This variability may be reduced bymore careful instructions on how to perform thetests. In addition, it is important to considersources of variability due to individual �uctua-tions in psychological factors such as stress orphysical factors such as fatigue.
Clinically, the most interesting aspect of thenew tests is that they examine the relationshipbetween sensory discriminative functions: explo-ration for identi�cation of objects and �ne coor-dination for the provision of ongoing cutaneousfeedback during holding tasks, and two majorroles of sensation: moving and sustained touch-pressure. Indeed, the modest correlation betweenthe MTP and the Modi�ed Moberg recognitiontest suggests that some relationship existsbetween de�cits in appreciation of moving touch-pressure sensation and the ability to �nd anobject and discriminate its features. Similarly, therelationship between the sensory tests and thetasks of manipulating objects suggests that theseaspects of sustained touch-pressure are important
at National Dong Hwa University on March 25, 2014cre.sagepub.comDownloaded from

New sensory tests for stroke 639
(TEMPA): Normative data and correlates withsensorimotor parameters. Arch Phys Med Rehabil1995; 76: 1125–29.
15 Desrosiers J, Hébert R, Dutil E, Bravo G.Development and reliability of an upper extremityfunction test for the elderly: the TEMPA. Can JOccup Ther 1993; 60: 9–16.
16 Desrosiers J, Hébert R, Dutil E, Bravo G, MercierL. Validity of a measurement instrument for upperextremity performance: the TEMPA. Occup Ther JRes 1994; 14: 267–81.
17 Streiner DL, Norman GR. Health measurementscales. A practical guide to their development anduse, second edition. Oxford: Oxford UniversityPress, 1995.
18 Van Boven RW, Johnson KO. A psychophysicalstudy of the mechanisms of sensory recoveryfollowing nerve injury in humans. Brain 1994; 117:149–67.
19 Johansson RS, Hager C, Backstrom L.Somatosensory control of precision grip duringunpredictable pulling loads. Exp Brain Res 1992; 89:204–13.
testing with Semmes–Weinstein mono�laments. JHand Surg 1987; 12A: 155–61.
9 Saddiki-Traki F, Tremblay N, Dykes RW, Derraz S,El-Khamlichi A. Differences between the tactilesensitivity on the anterior torso of normalindividuals and those having suffered completetransection of the spinal cord. Somatosens Mot Res1999; 16: 263–73.
10 Dannenbaum RM, Dykes RW. Evaluating sustainedtouch-pressure in severe sensory de�cits: meeting anunanswered need. Arch Phys Med Rehabil 1990; 71:455–59.
11 Gowland C, Stratford P, Ward M et al. Measuringphysical impairment and disability with theChedoke-McMaster Stroke Assessment. Stroke 1993;24: 58–63.
12 Dellon AL. Evaluation of sensibility and re-educationof sensation of the hand. Baltimore: Williams andWilkins, 1981.
13 Mathiowetz V, Volland G, Kashman N, Weber K.Adult norms for the Box and Block Test of manualdexterity. Am J Occup Ther 1985; 36: 386–91.
14 Desrosiers J, Hébert R, Bravo G, Dutil E. Upperextremity performance test for the elderly
at National Dong Hwa University on March 25, 2014cre.sagepub.comDownloaded from






![Interventionsforsensoryimpairmentintheupperlimbafter ...206782/UQ206782_OA.pdf · [Intervention Review] Interventions for sensory impairment in the upper limb after stroke Susan Doyle1,](https://img.pdfslide.us/doc/110x75/5f61d7f3216c8e387b5bac19/interventionsforsensoryimpairmentintheupperlimbafter-206782uq206782oapdf.jpg)