Embed Size (px)
Citation preview

Developing Scheduled &
routines that WorkCreating a
Culture of Change for People Living
with Cognitive ChangesIts not a Nursing Home or FacilityIt’s a HOME where nursing care is
given

Design Each Day
8 am – coffee circle 8:30 – songs of joy9 am – time to ‘go’9:15 – take a hike – walk’n’roll10 am – cool down & stretch10:30 – watering hole 11 am - ‘use your brains’ games11:30 - time to ‘go’ – wash up11:45 – ‘set-‘em up’ crew12 noon – let’s eat12:30 – clean up crew1 pm – music and meditation1:30 – coupons clipping2 pm – time to ‘go’2:15 – let’s dance
Make a schedule and follow it
Be structured BUT allow flexibility
Create a FLOW for the day
Build up and then slow down
Circadian rhythms
Offer a variety of activities every day
Leisure, work, rest, self-care,
groups and 1:1, passive and
active
Create Group schedules
BUT also build individual schedules
Not everything is for everybody!
Build a Foundation of Familiar and Favorite
Activities
Add a fewspecial events and something
different

Understand Activities
Modify and Structure the Activity for Success
Change the materials, the complexity, the setting, the help offered, the task demands, or
the purpose of the activity
Analyze the Activity…
What do you need to do
it?What skills,
abilities, interests?
What is the activity all
about?
Doing something
or making
something?
What type of activity is it???Self-care, leisure, work, rest…
Spiritual, social, physical, cognitive, passive, active, solitary
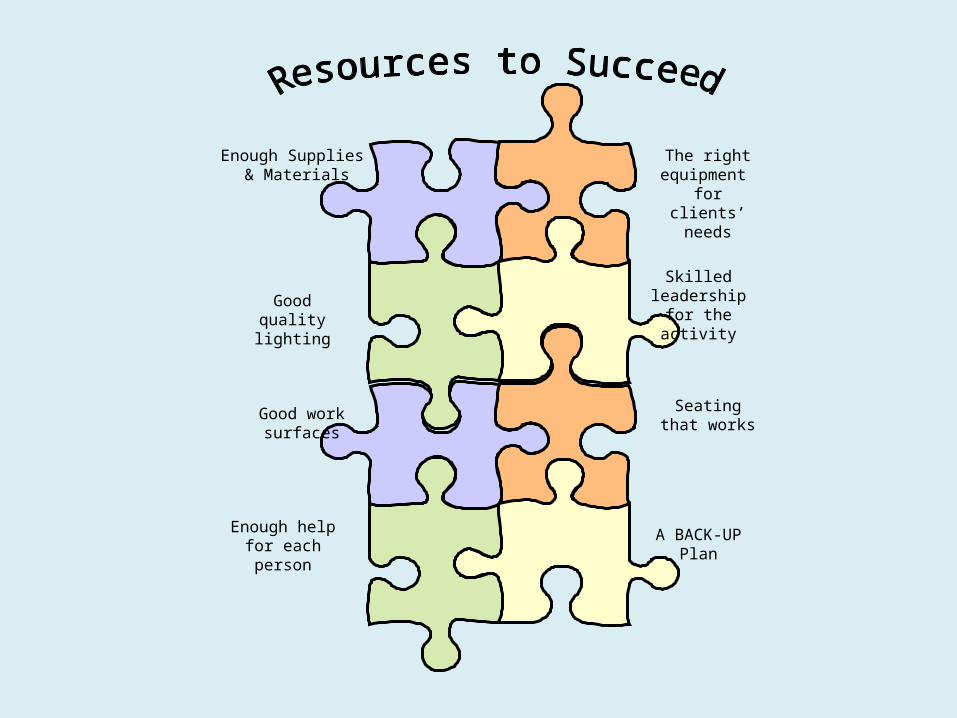
Enough Supplies & Materials
The right equipment for clients’ needs
Good quality lighting
Skilled leadership for
the activity
Good work surfaces
Seating that works
Enough help for each person
A BACK-UP Plan

Traditional Facility Care
• Run by administrators & nurses• Organized around staffing • Work shared among 3 shifts of staff• Safety and health care issues TOP
PRIORITY• Medical model • Organized by departments – task specific• You are sick – you need care for your
diagnosis• Father knows best!

What’s Wrong with this Model?
• Who wants to live in a hospital?• Who wants to do everything you are
supposed to?• Who wants to have someone else
telling what to do and when to do it?• Who wants to have to talk to three
different people to get something done?
• Who wants to live in a nursing home?

For People with Changes in Health and Abilities
• Need for help• Need for equipment• Need for changes in routines & habits• Need to match needs with availability
of help• Need to ‘anticipate’ when and where
you will do things, need things

Cognitive Changes with Aging
• slowed processing • less flexibility• more difficulty with new learning• more rehearsals needed• benign forgetfulness – immediate
recall goes first

Emotional Changes with Aging
• increased incidence of depression• increased incidence of anxiety• with stress – mood swings• with some drugs – emotional side
effects
What Does Having Cognitive Abilities Do To This Whole
System of Care?
• Changes in memory & thinking• Changes in understanding &
speaking• Changes in impulsivity & initiation• Changes in abilities & processing

So Let’s Figure YOU Out…
• What time do you wake up?
• How do you wake up?• What do you do when
you wake up?• When do you eat
breakfast? • What do you eat for
breakfast?• How do you get ‘clean’?• When do you get clean?
• When do you toilet?• What do you do for work?• What do you do for fun?• What do you do when
you are stressed?• ID two people you love…• Where are you from?• What is your favorite
food?• What do you HATE to
eat?

Questions
• How would you DO living in your community?
• What would it be like if you had physical changes?
• What about cognitive impairments?
• How would you do on someone else schedule?
• What would NOT be OK?
• What if it was the rest of your life?
• What would you want?

What is Veteran-Centered Care?
Combination of…• Person’s wants• Person’s needs• Still can do• Can’t do• Can do with support• Individual good• Common good• Family needs• Family wants
Balanced with…• Staff skills• Staff availability• Private space• Public space• People resources• Equipment resources• Safety & Security• Rules & regulations• Others needs and wants

Personal Preferences & Values
• Who have you been?• What did you value?• Who are you now?• What do you value now?• Why does it matter?• Who gets a ‘say’?• Who gets to set the priorities?

Who Matters?
All of UsEach of Us

What Matters – When Illnesses Are Present?
• Safety – Environmental modifications• Access - Availability• Timeliness of help• Flexibility in timing• Structure & predictability• Privacy and respect• Preservation of SELF

Key Steps
• Connect• Gather Information• Share Information• Use Information• Review Information• Make Changes

What About Medical Conditions?
What is essential?• Good care is delivered• The person is
receiving the care they need and want
• Conditions are assessed
• Decisions are made based on good info
• There is agreement on what to do and what NOT to do…
What is optional?• When it is done• Where it is done• Who does it• How often it is done• How strictly it is
followed• It depends on the
person & their situation

What are the Different Care Approaches to Consider?
• Health Promotion• Curative• Restorative - Rehabilitative• Maintenance• Compensatory• Palliative

Health Promotion
• Check Ups• Annual vaccinations• Lower the numbers• Increase activity level• Eat well – moderately• Monitor all conditions for careful control• DO WHAT YOU SHOULD to be the BEST
YOU CAN BE!

Curative
• Fix what is wrong• Test to figure out what is happening
then DO SOMETHING ABOUT IT:– Surgery– Medications– Treatment
• Full recovery of function – GOOD as NEW!
Restorative
• Recovery of SOME degree of function or ability
• Focuses on the PERSON regaining skills and abilities with help– Rehab personnel– Special equipment– New techniques
• Not perfect, but BACK to a Higher level of Function

Maintenance
• Maintaining the Status Quo – Keepin’ ON
• Not losing ground• Depends on:
– Physical environment not changing– Caregiver consistency– Sustained abilities of the person– All other things staying the same
• It’s HARD WORK … SO…– ‘IS what I have worth keeping???’

Compensatory
• Providing what the person can’t do to ‘fill in the gaps so that LIFE GOES ON….
• Supportive – Physical environment changes– Caregiver cueing and helping changes– Expectations change– Schedules and routines change to
accommodate
• End Point is the Same – – How we get there Changes

Palliative• Comfort Care• TOP PRIORITY –
– Honor personal preferences and choices– Manage Pain, Distress, Anxiety, Fear,
Discomfort
• Identify & seek to meet social, physical, psychological, and spiritual needs
• Let go of FIXING and MOVE ON to Comforting

The GOAL?
• Build a schedule and care routine that helps the person:– Be the way they want to– Do what they are able– Feel good about themselves– Feel OK about where they are– Enjoy the people who are there to help
them– Get what they need

Who Needs to Buy In?
• Residents• Families• Front line staff• Managers• Community leader• Regulators• Public• Reimbursors

So… What Do We Need from Staff & Families?
• Awareness of the process• Participation in planning• Sharing about the past• Time to learn & try something new• Willingness to listen• Willingness to advocate AND negotiate• Flexibility as we figure this out





























