Embed Size (px)
Citation preview

Developing and testing models for the investigation of barriers
to effective HIV / AIDS prevention in the USA
Dr Anatole S Menon-JohanssonDrs Jean McGuire & Harvey Makadon
Harvard School of Public Health
Harkness / Health Foundation Fellow 2006Orlando June, 2007

Outline• Measuring AIDS prevention performance
• Describe how AIDS prevention differs between men & women
• Highlight correlations with AIDS prevention
• Predicting AIDS prevention performance
• Policy implications

HIV > AIDS > DeathViral transmission
Acute retroviral syndrome
Recovery + seroconversion
Chronic HIV infection
Symptomatic HIV infection / AIDS
Death
2-3 weeks
2-3 weeks
2-4 weeks
~ 8 years
~ 1.3 years
HIV+
AIDS
HIV Rx
PREVENTION
1o
2/3o

HIV vs AIDS data• HIV data available from 28 states in 1995
and 36 in 2004
• ? HIV data reliability– HIV ≤ AIDS diagnoses for some states
• Estimated 25% HIV+ persons do not know their ‘serostatus’
• AIDS = notifiable disease since late 1980’s and disease definition set in 1993

Changes in AIDS cases over time
Data: Center for Disease Control and Prevention (CDC) 1995-2004

AIDS prevention by gender
Data: CDC 1995-2004

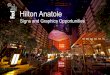
AIDS prevention in men (1995-2004)
COLOUR
Average AIDS
change / year (%)
- 15-25%
- 10-15%
- 5-10%
- 0-5%
+ 0-5%
+ 5%

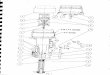
AIDS prevention in women (1995-2004)
COLOUR
Average AIDS
change / year (%)
- 15-25%
- 10-15%
- 5-10%
- 0-5%
+ 0-5%
+ 5%

Relationships with known prevention strategies
• How does AIDS prevention relate to:– Demographics– Economics– Prevention strategies
• Primary• Secondary / Tertiary
• Linear regression was used to compare AIDS prevention with the above variables

Demographics
Data: US Census Bureau 2004

Income / Poverty & AIDS prevention
Data: US Census Bureau 2004

Primary prevention
Data: Kaiser Family Foundation, Office of Applied Studies, CDC

Women’s Health
Data: American Cancer Society 2004, CDC 2004, NARAL Pro-choice America 2006

The uninsured and state to state disparity in provision
• KFF / NASTAD ADAP reports– 25% of HIV+ people on Rx use ADAP– ADAP formulary varies by state– Waiting lists are used for cost control– Variation in eligibility criterion
• Kaiser Daily HIV / AIDS reports– August 29th, 2003– “Three people with HIV / AIDS die while on West
Virginia ADAP waiting list”

Health care provision
Data: US Census Bureau 2004

Secondary / Tertiary prevention
Data: KFF / NASTAD ADAP reports 1997-2004, AMA 2004, US Census Bureau 2004

Impact of sodomy laws
Data: CDC 1995-2003, US Supreme Court

Impact of Syringe Exchange Program (SEP) authorization laws
Data: Beasley School of Law, Temple University

Summary
• State AIDS prevention can be accurately evaluated using this model
• Less effective state AIDS prevention is associated with :– Women (Reduced reproductive health)– Poverty (Black)– Poor STD control– History sodomy laws– No SEP authorization laws

Prediction AIDS prevention success
• Key variables:– Poverty– Gonorrhoea rate– Not having a SEP authorization law
• Properties of predictive model:– Sensitivity 83%– Specificity 79%

Policy implications
AIDS prevention could be improved by:
• Standardization of SEP authorization laws
• Improving sexual and reproductive health
• Poverty alleviation

Acknowledgements
• Commonwealth Fund
• Health Foundation
• Ellison-Cliffe Travelling Fellowship
• Senta Foulkes Travelling Fellowship
• Avni Patel (KFF)
• Drs Sullivan and Campsmith (CDC)
• Professors and students at HSPH