Embed Size (px)
Citation preview
Developing Adult ProfessionAl Psychological services for oncology
January 2015
Dr Julie HighfieldProject Manager Consultant Clinical Psychologist
Applying learning from Arden Psychological Services Scoping Project

2
Acknowledgements 3Foreword 4Executive Summary 5Introduction 6
1.0. Emotional and psychological needs of the oncology population: patients, relatives and carers, workforce 7 1.1. Policy Context 7 1.2. Understanding the need for psychological care 7 1.3. The evidence base for psychological care 9 1.4. Estimated cost-offset of psychological approaches 9
2.0. A best practice model for psychological services in cancer 9 2.1. Summary of best practice service specification 9
2.1.1. Best practice for clinical services provided 10 2.1.2. Best practice for training and supervision 11 2.1.3. Best practice for structure and governance of
psychological services in cancer 11 2.2. Examples of best practice 11 2.2.1. Integrating services 11 2.2.2. Survivorship 11 2.2.3. Self-care: mindfulness group 12 2.2.4. Dimbleby Cancer Care - partnership working 12 2.2.5. Primary care-delivered services 12
3.0. Meeting the need for psychological services 13 3.1. Commissioning in NHS England 13 3.2. Can level 2 services meet need alone? 13
3.3. Providing services within existing mental health services 13 3.3.1. IAPT 13 3.3.2. Secondary mental health 14 3.4. Conclusion to providing services 14
4.0. The Arden Project 14
5.0. Conclusion 15
References 16
Appendices 1. Examples of the impact of psychological interventions 18 2. Psychological assessment and support Levels 1-4 19 3. Typical training pathways for Level 3 and 4 service
professionals 21 4. Understanding what level 3 and 4 professional may offer,
and illustrating the differences between levels 3 and 4 22 5. Psychological services and psycho-oncology individuals
consulted for expert opinion of psychological services in cancer 25
6. Suggested required knowledge and competencies of level 3 and 4 staff 26
7. Outcome measures for a psycho-oncology service 28 8. Mapping tool 29 9. Algorithm for estimating minimum service requirement
at Level 3 and 4 30 10. Service gaps highlighted within the Arden Project,
with considered actions 31
conTents
3
Acknowledgements
This report is based on the findings of the 2014 Macmillan Psychological Services for Cancer Scoping Project for Arden. Several national documents have been referenced throughout this report. In addition several local stakeholders and national experts have been consulted. These are listed in appendices eight and nine.
Special thanks go to:
Macmillan Cancer Support for the funding of this project
Coventry and Warwickshire Partnership Trust and University Hospitals Coventry and Warwickshire NHS Trust for instigating the Arden Project
Dr Alex King, Consultant Clinical Psychologist, at Imperial College Healthcare NHS Trust, who gave key advice regarding estimating the provision of services
Drs Tamily Duggan and James Parker, both local Clinical Psychologists in Coventry and Warwickshire, for their advice regarding local services and their continued support and ideas throughout the project
4
forewordWithin a decade from the seminal 2004 NICE guidance, and driven by tireless campaigning by patient groups as much as by Peer Review standards by experts, psychological care is now firmly and unequivocally embraced within formal specifications for cancer & palliative care services.
Yet, still, we see national cancer patient experience results showing us that about 25-30% of patients do not feel they can discuss their worries and fears with staff; we see such wide variability of provision that doctors & nurses cannot just rely on psychological expertise at their side just as they do for infection control or radiology; and we see the relentless strain on dedicated clinicians who find little scope to do what really brought them into this job – connecting & comforting, not just triaging & discharging.
Clearly, we have a way to go until we get excellent psychological care from the specifications to where it matters: where every clinician is able to offer solid first-line psychological care, and gain the satisfaction of holistic caring; where every person affected by cancer, who finds their thoughts, feelings, reactions and relationships unbearably intense,
can talk to a specialist in the right place, at the right time; where the whole cancer hospital or palliative care centre is thinking, planning and working psychologically.
This report, in its ambitious scope spanning evidence, policy, guidance and case studies, then drilling down to the granular detail of WTEs and KPIs, will certainly help us narrow this gap. It sets a high standard for service development planning, in its scholarship but also its leadership approach to making the effort to talking to all the people who matter, and closing the feedback loop. And finally, it challenges us in psychology, so fascinated by the intricate patterns and processes within minds and relationships, to share fully in the arduous, fractious tasks of shaping systems of care that make a real difference to thousands.
Dr Alex KingConsultant Clinical Psychologist
5
“Although there have been significant improvements in support for people living with and beyond cancer, more needs to be done so that cancer survivors have the care and support they need to live as healthy a life as possible, for as long as possible.” Department of Health 2011, p47
The psychological impacts of cancer are understandable, and distinctively clear impacting the whole system: the individual, families, and the staff who care for them. Many are able to draw on their own resources to cope, however up to 25% of individuals with a cancer diagnosis require a professional intervention from an appropriately trained individual (NICE, 2004). The psychological impacts are not just in terms of distress, but relate to engagement with and utilisation of healthcare, and estimates indicate that having professional psychological services embedded within adult cancer services can save up to 20% of healthcare utilisation costs (Chiles et al, 1999; Carlson & Bultz, 2004). The Department of Health does not currently attach a tariff to Psychological Services in Cancer, leading to variation in how such services are funded and organised, and inequalities of access and service.
In the former Arden Cancer Network, which includes Coventry, Warwickshire, and Worcestershire, such variation has been noted and concerns have been raised for many years. This led to a Macmillan funded project, hosted by Coventry and Warwickshire Partnership Trust in conjunction with University Hospitals Coventry and Warwickshire. The project mapped existing services across the region, and engaged stakeholders in discussions about preferred services. In addition, national experts and guidelines were consulted. This resulted in regional reports to highlight the variations and needs. Local commissioning groups welcomed the reports, and each are considering their position on the development of future services as a result of the project.
The Macmillan Psychological Services Scoping Project for Arden was carried out in 2014, mapping local psychological services for oncology and engaging stakeholders and drawing from national guidance to suggest future workforce developments. This project acts as a case study, as common learning points were noted which were applicable beyond the region. This report represents a summary of such information. It includes information regarding the standards for psychological services for
cancer as documented in several national reports, which suggests offering psychological support and intervention across four levels of complexity to patients, relatives and staff. This includes the role of psychological professionals offering training and supervision to their medical, nursing and allied health professional colleagues, and highlights the need for integration of psychological services within all parts of the cancer care pathway. In addition the mapping tools utilised within the project are summarised, with a view to enable other regions across the UK to develop local psychological services for oncology.
Dr Julie HighfieldConsultant Clinical Psychologist Project Manager
execuTive summary
6
In 2013, a group of clinicians from cancer services and psychology acquired funding from Macmillan for a different kind of project. A Clinical Psychologist was recruited to map psychological services for oncology across Coventry, Warwickshire, and Worcestershire (known as the Arden area). This was done through engaging with local services, stakeholders, service users, and commissioners in addition to compiling evidence from national guidance and leading experts. What resulted was four regional reports delivered to stakeholders and commissioners, and the beginnings of progress towards service development.
However the findings generated interest beyond the region, resulting in the request for this document. Despite multiple reports and articles detailing the psychological impact of cancer, the needs of patients, relatives, and staff, and the workforce required to meet this need, there are still inequities in the provision of psychological services for cancer across the UK.This document attempts to summarise current understanding of the psychological impact of cancer, and the recommendations for psychological services, referring the reader to wider sources where appropriate. It uses the mapping process from the Arden Project as an illustrator of how other services may be able to develop local services.
Throughout this document, such services are referred to “Psychological Services in Cancer”, and this refers to all psychological professionals (e.g. level 2 trained cancer services staff, counsellors, psychotherapists, clinical psychologists, counselling psychologists, and psychiatrists) who may contribute to such services. It is noted that in other documents, these services are also referred to as “Psycho-oncology services” or “Psychological support services”.
introducTion
7
1. Emotional and psychological needs of the oncology population: patients, relatives and carers, workforce
1.1. Policy contextThere are multiple national guidelines and reports that indicate the need for psychological services for cancer patients, their carers, and to support the work of staff in cancer services. Key documents to refer to when considering the development of Psychological Services in Oncology are as follows:
• NICE Guidance in Supportive and Palliative Care (2004) and the associated Improving Outcomes Guidance Manual
• Cancer Reform Strategy (Department of Health, 2007)
• A Model of Care for Cancer (NHS Commissioning Support for London, 2010)
• Improving Outcomes: A Strategy for Cancer (Department of Health, 2011)
• British Psy chological Society, Division of Clinical Psychology - Briefing Paper on Clinical Psychology Services in Oncology (1997)
• National Service Frameworks e.g. Long Term Conditions, 2004
• Cancer Action Team (2007) Holistic Common Assessment of Supportive and Palliative Care Needs for Adults with Cancer: Assessment Guidance. London, Cancer Action Team.
• End of Life Care Strategy (2008)• Report of the All Party Parliamentary Group
on Cancer’s Inquiry into Inequalities in Cancer (All Party Parliamentary Group, 2009).
• London Cancer Alliance (2014) Developing a mental health and psychological support services pathway for adults.
• British Psychological Society, Division of Clinical Psychology - Demonstrating Quality & Outcomes in Psycho-Oncology (in press, 2015)
1.2. Understanding the need for psychological care
The psychological impacts of cancer are significant, yet may be overlooked. In the Macmillan Cancer Support (2006) report “The Emotional Impact of Cancer”, 45% of people cited the emotional effects of cancer as the most difficult to cope with and yet 41% felt unable to get help with this. The National Audit Office, 2005 concluded that over half of cancer patients did not have their psychological needs identified or addressed and a fifth of these patients felt more could have been done to assist with their anxiety or depression. In Macmillan Cancer Support (2006) report, “The Emotional Impact of Cancer”, 45% of people cited the emotional effects of cancer as the most difficult to cope with and yet 41% felt unable to get help with this.
According to the summarised evidence in the Improving Outcomes Guidance (NICE, 2004) up to 25% of cancer patients will require a professional psychological intervention: around the time of diagnosis of early cancer, approximately half of all patients experience anxiety and depression severe enough to affect their quality of life. About a quarter of these patients will continue to do so during
the following six months. Among those whose cancer progresses, the prevalence of anxiety and depression rises to 50%. In the year following diagnosis with early cancer, around 1 in 10 patients will experience symptoms severe enough to warrant interventions by specialist psychological/psychiatric services. Such symptoms are seen in 10-15% of patients with advanced disease. People with cancer are also at increased risk of suicide (Fang et al, 2012; Schairer et al, 2006). Psychological distress is common among people receiving palliative care and although it is an understandable and natural response to a traumatic and threatening situation. Depression does not just impact in terms of distress- in a meta-analysis, Pinquart and Duberstein (2010) drew from 76 studies (176 863 patients) and indicated the relative risk of mortality in cancer patients increased by 17% in patients with depression compared with those without depression.
Recent research indicates a lower prevalence of major depression, however sub-clinical
In Macmillan Cancer Support (2006) report, “The Emotional Impact of Cancer”, 45% of people cited the emotional effects of cancer as the most difficult to cope with and yet 41% felt unable to get help with this.

8
depression may still be higher than those numbers quoted, and many may not admit to symptoms as low mood may be “expected” during cancer treatment. Walker et al (2014) analysed data for 21151 cancer patients. The prevalence of major depression was highest in patients with lung cancer (13·1%), followed by gynaecological cancer (10·9%), breast cancer (9·3%), colorectal cancer (7·0%), and genitourinary cancer (5·6%). Within these cancer groupings, a diagnosis of major depression was more likely in patients who were younger, had worse social deprivation scores, and, for lung cancer and colorectal cancer, and female patients. 73% of patients with depression were not receiving potentially effective treatment.
In addition there are family impacts. For example, in a longitudinal study of caregivers of advanced cancer patients, 13% of caregivers were found to meet DSM-IV criteria for a psychiatric disorder and 25% had accessed treatment for mental health concerns since the patient’s diagnosis. (Vanderwerker, et al., 2005). In addition there are health, social and financial burdens.
The Improving Outcomes Guidance (NICE, 2004), recognises that psychological distress in those living with cancer is associated with a range of harmful outcomes, including amplification of physical symptoms, poorer levels of functioning, adverse impact on carers, an enhanced desire for death, reduced adherence to cancer treatment and probable reduction in life expectancy. It also increases utilisation of healthcare resources. Much of this distress and disorder goes undetected and untreated. This distress is, however, potentially treatable. Expert opinion asserts that ddetecting and actively managing psychological distress and psychiatric disorder leads to safer care, improved clinical outcomes & patient experience, and improved cost effectiveness. However, proving this cost-effectiveness proves difficult.
No Health Without Mental Health (Department of Health, 2011) makes the case for parity of esteem (and parity of provision) between mental health and physical health services. The cost of inadequately addressing the psychological and mental health needs of those with long term conditions, such as cancers, is enormous. The Kings Fund, in its 2012 paper Long Term Conditions and Mental Health: the cost of co-morbidities, point to reduced quality of life, significantly poorer health outcomes (through continued self-damaging behaviours and poor adherence to medical treatment) and additional costs to the NHS of £8-13 billion per annum. Comorbid mental health problems raise total healthcare costs for patients with a long term condition by 45% (Kings Fund, 2012).
Psychological services in cancer exist not just for patients and carers, but for staff too, by providing training and support, and being on-site to consult on complex cases. In local staff surveys as part of the Arden project, staff commented that clinical supervision can improve: levels of stress and ability to self-care, levels of understanding and compassion and is seen as attractive to new staff, impacting upon recruitment and retention of the best staff. This will help to protect against burnout and potential clinical errors and associated mortality.
In a systematic review, Shaller (2007) identified “care for the care givers through a supportive work environment” as one of seven key factors influencing good patient care. Schwartz Rounds were developed in cancer services in USA as a way of reflecting on experience at work and acknowledging the feelings of staff, have been well documented in the USA as impacting positively on teamwork and hospital culture, and these have recently been evaluated with positive results within the UK (Goodrich, The Kings Fund, 2011). Macmillan’s recent report
up to 25% of cancer patients will require a professional psychological intervention
Comorbid mental health problems raise total healthcare costs for patients with a long term condition by 45%
9
on staff experience in 2014, provided evidence of the link between improved staff engagement and better patient experience. The NHS Litigation Authority (NHS LA) Risk Management Standards 2013-14 documentation emphasises the importance of clinical supervision as a key mechanism for reducing emotional exhaustion among clinical staff. The NHS LA states that all organisations must have an approved documented process for managing the risks associated with work-related stress, with the rationale that work-related stress is a major cause of occupational ill health, sickness absence, staff turnover and poor performance.
1.3. The evidence base for psychological intervention
There is a recent trend in mental health research to favour psychological therapies that may be manualised and therefore more easily be subject to randomised controlled trials. However, psychological interventions in more complex cases are more likely to be formulation-driven, and include a multifaceted therapeutic approach. Examples of psychological therapies that have been applied in cancer settings include: counselling, existential psychotherapy, cognitive behavioural approaches for depression and anxiety, and grief therapies. Psychological therapists working in this area may utilise psychological models of adjustment, health beliefs, and effective communication skills .
For an excellent summary of the evidence base for psychological therapies within cancer, please see the London Cancer Alliance’s 2014 publication,
Developing a mental health and psychological support services pathway for adults.
Psychological interventions have impact beyond distress reduction, and appendix 1 gives examples of the impacts of psychological interventions on distress, health outcomes, and healthcare utilisation.
1.4. Estimated cost-offset of psychological approaches
A meta-analysis of psychological interventions on the use of medical services was evaluated by examining the outcome of 91 studies published between 1967 and 1997, and results provided evidence for a medical cost-offset effect, with average savings resulting from implementing psychological interventions was estimated to be about 20% (Chiles, Lambert & Hatch, 1999). In a more recent meta-analysis, Carlson & Bultz (2004) stated: ‘The literature review clearly supports the notion that psychosocial interventions are not only effective, but also economical’ and they refer to the ‘usually overlooked long-term cost savings that may be accrued to overburdened health-care systems’, estimating up to 20% of healthcare costs can be saved in the long term by having trained psychological professionals embedded in cancer services.
Psychological interventions can impact upon healthcare utilisation- for instance individuals with high anxiety or maladaptive health beliefs may stay in hospital for longer or access outpatient
clinics more frequently. Cancer treatment varies from patient to patient, and it is hard to estimate costs accurately, however the average cost of cancer treatment is estimated at £24000, (National Cancer Intelligence Network,2011). Using the meta-analytic research, which suggests a saving of up to 20%, a conservative estimate of savings may suggest up to £4800 per case. Psychological professionals are on agenda for change payscales 5-6 (level 3) and 8a-c (level 4).
For illustration, an 8a Clinical psychologist (current top of A4C 2014 banding / maximum pay is currently £47088) will work with on average 150 patients per year. That Clinical Psychologist would only need to work with 10 cases per year who are using healthcare excessively to offset their direct wage costs.
2.0. A best practice model for psychological services in cancer
The Gold Standard model of services has been compiled using national reports (as listed in section 1.1. Policy Context) in addition to expert opinions sourced as part of this project, listed in appendix five.
2.1. Summary of best practice service specification
A key recommendation refers to levels of psychological care originally detailed in NICE, 2004 and supported by onward reports and guidelines. This is detailed in appendix 2. In summary, psychological care in oncology can

10
be separated into two distinct categories: the care provided by those who have some training in assessment and frontline intervention of psychological problems but who are not mental health or psychological support professionals (level 1 and 2); and that which is provided by trained mental health/psychological support professionals (level 3 and 4). The appropriate professional, and the intervention, will depend on the nature and severity of the person’s psychological problem, their previous psychological morbidity, the quality of social support available, and the status of the cancer. The different level 3 and 4 professionals with training routes are given in appendix 3. As an illustration of the differing skill sets, case illustrations are given in appendix 4.
The key recommendations are:
- Psychological support is offered at all stages of cancer treatment, including end of life and survivorship
- A mix of skills is required, from level 2 trained staff, to level 3 counsellors , psychotherapists and clinical psychologists, to mental health specialists at level 4 such as Clinical Psychologists and Consultant Liaison Psychiatrists.
- During active curative or palliative treatment in hospital (moreso than in remission, survivorship or end-of-life care), it is imperative for psychological services to support patients directly, but also indirectly through working with staff. Having psychological services embedded in cancer services is considered the
optimum way to achieve this.- During survivorship, and when a patient is no
longer under the care of the hospital, some patients may wish to access generic services within primary care, and services should enable this
- Third sector and voluntary services offer additional sources of support, but not necessarily professional psychological intervention. An interface between NHS services and such services where both are communicating with each other and aware of referral criteria may benefit patients and carers. This may enable patients to have access to alternative sources of support
2.1.1. Best practice for clinical services provided • A multi-professional Psychological Care
Team for Oncology might include: liaison psychiatrists, clinical health psychologists, psychotherapists, counsellors, psychosexual therapists and grief therapists.
• Four levels of psychological care are provided, as introduced in NICE 2004
• The psychological needs of all patients and carers are assessed using the Holistic Needs Assessment on a regular basis throughout the patient pathway, with attention given to those points known to be particularly challenging, such as around the time of diagnosis, as treatment ends and at recurrence
• The Holistic Needs Assessment can only be delivered by level 2 trained staff
• Patients and carers are offered psychological support appropriate to their needs, with those experiencing particular distress referred to
professionals with specialist expertise (levels 3 and 4 care).
• 15% are likely to experience mild to moderate problems requiring level 3 input
• 10% are likely to experience problems requiring level 4 input.
• Level 3 approx. 1.6 WTE psychological services staff per 1000 new cancer diagnoses per year (to include palliative care)
• Level 3 and 4 staff should work across a variety of settings, including primary care, hospitals, hospices and the community.
• Level 4 approx. 1.4 WTE per 1000 new cancer diagnoses per year (to include palliative care)
• Where there is no provision for level 3, level 4 services should be increased.
• Level 3 services staff do not have the sufficient training as standard to provided level 4 services
• Level 4 services should include access to Clinical Neuropsychology where services are provided for patients with primary or metastatic brain tumours
• Patients should have access to specialist psychosexual counselling if required
• Psychological services should be integrated and embedded, therefore able to offer on-site consultation and advice
• There should be a Single Point of Entry to psychological services in cancer
• Services should link to mental health and liaison services in the area
• As a general guide, level 3/4 professionals in a full-time clinical position will work with an average of 150 new cases per year; however
11
this may vary widely between specialties e.g. TYA vs Acute Inpatient Oncology and case complexity
• Waiting times should be ideally two weeks, maximum 1 month for outpatients,and ideally 1-2 days to maximum 1 week for inpatients
2.1.2. Best practice for training and supervision• Level 2 training and supervision are provided.• The psychological needs of staff caring
for patients and carers facing difficult circumstances are adequately met (level 2 training and supervision)
• All keyworkers of every cancer MDT (CNS, AHPs) are Level 2 trained and supervised
• The level 2 practitioner(s) should receive a minimum of 1 hours clinical supervision by a level 3 or level 4 practitioner per month
• Sufficient level 2 course capacity to meet local and regional demand- consider running in conjunction with other geographical areas
• 1 level 2 supervision of 1hours per 5-7 level 2 trained staff
• A link to occupational health psychological services for complex staff needs
• Staff should have access to Advanced Communication Skills training
• Schwartz Rounds are a useful way of bringing staff together to reflect on clinical experiences, and supports staff engagement
2.1.3. Best practice for structure and governance of psychological services in cancer
• Psychological Services for cancer should be led by senior psychological care professionals with experience of working within a medical setting
• Outpatient psychological care requires access to few resources other than reliable, good quality accommodation that is conducive to sensitive conversations with people in distress
• Level 3/4 professionals should adhere to all CPD and supervision requirements by their regulatory body (e.g. HCPC, GMC) and/or professional association (e.g. BACP, BPS etc).
• Level 3 and 4 should link to other “level2” style services, such as chaplaincy, service user lead support groups, survivorship programmes, and voluntary sector
• Psychological service providers should meet the minimum training requirements outlined in BPOS-SIGOPAC-BPS 2011, summarised in appendix 6
• Services should gather and report a wide range of data to demonstrate quality & outcomes (cf King 2015, summarised in appendix 7)
• Cross pathway psychological services in the same geographical area should have shared frameworks of governance
• Level 4 services should be involved in generating new evidence and have a university link if possible
• The psychological services should link to other educational needs of staff- e.g. junior doctor and new nurse induction
• Services should attract Trainee Psychologists
and Trainee Counsellors, as well as volunteer counsellors for placements to provide additional staffing
2.2. Examples of best practice2.2.1. Integrating servicesLocally to the Arden Project, South Warwickshire Warwick Hospital has in-house psychological services. Within oncology, there is a 0.8 WTE 8b Clinical Psychologist post, and within Palliative Care there is a 0.6 WTE 8b Clinical Psychology Post. Services are provided to those patients utilising hospital services, however GPs and community clinicians may refer in to the service. The staff also provide in-house training, supervision, and consultation. The team are also funded to provide 0.4 WTE to Myton Hospice. The Myton Hospice Clinical Psychologist works closely with the level 3 hospice counsellors. Therefore, in South Warwickshire, cancer patients, and their relatives, and the cancer services staff have equitable access to a cross pathway psychological service.
2.2.2. Survivorship There are many versions of health & wellbeing, end of treatment, or survivorship groups eg by breast cancer care, those provided by Maggie’s. One example is the “Beyond Cancer Group” run by Clinical Psychologists in Walsall, West Midlands. This group aims to help patients manage the transition from active treatment to ‘survivorship’ in the here and now, which is highlighted as one of the most psychologically demanding phases of the patient pathway (NICE 2004). The group is facilitated by
12
jointly by clinical nurse specialists and the clinical psychologist in oncology and palliative care. The group includes emotional support once active treatment is complete, coming together as a group to normalise feelings and recognise the challenges ahead, sign posting to services that can provide practical help once active treatment is complete. The group aims to provide information on finances, dietary advice, living with cancer, treatment information, complementary therapies and coping with issues such as pain management and breathlessness. The group is based on the principles of Macmillan survivorship programme. It consists of 8 monthly, whole morning sessions.
Patients who have benefitted from the previous groups, have reported improvement in depression and anxiety. The following are some quotes from those who have attended:
“Gives me hope that things will get better, gives me hope that more is being done, shows that I can move on a little. . .”
“It helps me put my feelings into perspective. I tended to think I was over the top with what I am experiencing but it is now apparent that I am not on my own. Other cancer survivors are having the same doubts/fears/feelings”
“I realise I need to take control as things will never change if I don’t say how I am really feeling” .
“I can be honest and everyone in the room can relate to me. People/family doesn’t seem to understand.”
2.2.3. Self-Care: mindfulness groupMindfulness can be defined as ‘paying attention in a particular way: on purpose, in the present moment, and non-judgementally ‘(Jon Kabat- Zinn). Mindfulness Based Cognitive Therapy (MBCT) combines mindfulness meditation practice with techniques from Cognitive Therapy, in an 8-week group programme. Mindfulness Based Cognitive Therapy groups have been piloted in George Eliot Hospital, North Warwickshire for patients who are at the end of/post cancer treatment and are experiencing symptoms of anxiety or low mood/depression and are finding it difficult to cope with the general stresses and challenges presented by their illness. They may have a history of depression and/or anxiety symptoms.
Although open to patients with any cancer diagnosis, the two groups to date have comprised women with a diagnosis of breast cancer and although numbers are small, initial evaluation shows increases in measures of self-compassion, quality of life (physical, social/family, emotional and functional), and facets of mindfulness, along with decreases in le vels of worry. Patients who have attended the programme are then invited to attend a
maintenance group every three months which allows them to continue to practice their mindfulness mediation. This is offered over a period of eighteen months following completion of the programme.
2.2.4. Dimbleby Cancer Care – partnership working
Dimbleby Cancer Care offers psychological care to cancer patients through Guys and St Thomas’s NHS Trust and Kings Health Partners. The service has a skills mix of Clinical Psychologists, Counselling Psychologists, Assistant Psychologists, Counsellors, Existential Psychotherapists and has dedicated input from psychiatry. Cancer patients, their carers , and their children may be referred from anywhere across the pathway of cancer care, including inpatient and end of life care, by anyone treated within Kings Health Partners. It is commissioned across the five local boroughs. In addition level 2 training and supervision is provided to cancer care staff in all tumour groups. The team have a triage system, so that referrers are responded to quickly and more information sought so that the best care can be provided in a timely manner.
2.2.5. Primary Care-delivered servicesIn Swindon and Wiltshire the primary care (IAPT) services deliver services for long term conditions, which may have implications for the role of IAPT in oncology, may be found here:
http://www.nhsiq.nhs.uk/media/2542397/lift_psychological-support.pdf

13
The SMaRT oncology trial- a cancer nurse-led intervention for depression in Scotland, and the Sussex Psychological Support project- a Specialist Cancer Nurse embedded within the cancer centre with a role to improve the psychological approaches of staff may be found here:
http://www.iapt.nhs.uk/silo/files/collaborative-care-report--phase-1--june-2010.pdf
It is worthy of note that both trials suggest the efficacy for having embedded rather than separate psychological services, which poses challenges to the way current primary care psychological services are organised in many parts of the UK.
3.0. Meeting the need for psychological services
3.1. Commissioning in NHS EnglandActive cancer treatments in England are for the most part commissioned directly by NHS England. There is no specific tariff for psychological services. Therefore currently in NHS England it is at the discretion of cancer service providers to allocate a budget to psychological care. This means provision of services varies between Trusts, although many Acute Trusts find the benefits of having embedded psychological services within their teams outweigh the costs.
Mental Health Services in England do not currently, as standard, offer psychological
services to cancer patients, unless that patient meets criteria for mental health problems. In many Mental Health Trusts, this means meeting diagnostic criteria for problems such as Anxiety Disorders, Depressive Disorders, bipolar disorder etc. The presentations of distress in the dynamic context of cancer care may not fit well within mental health diagnostic categories, while the treatment ‘packages’ on offer by community psychological therapy services (e.g. weekly sessions at a set time) may not fit with well within cancer treatment schedules – thus restricting the scope for patients to access such services.
The NHS England Business Plan 2014/15- 15/16 suggests a parity of esteem between mental and physical health, that both should be valued equally. This focusses on the physical health of those with a diagnosed mental health problem. The position on the psychological wellbeing of individuals with physical problems is not clearly considered. The document suggests IAPT services across NHS England should provide services for individuals with long term conditions. However IAPT documentation does not support cancer as a long term condition (IAPT, 2008)
The NHS England Business Plan also considers the rolling out of the 6Cs approach, where nurses are encouraged to have compassion as a focus within care. As there is evidence to suggest that in order to deliver compassionate care, staff self-care, staff engagement and support are key, the psychological training and support of staff is important in rolling out the 6Cs approach.
In the plan’s workforce development related priorities that relate to psychological care within cancer are as follows:
• Enhancing quality of life for people with long term conditions.
• Helping people to recover from episodes of ill health or following injury.
• Ensuring that people have a positive experience of care.
3.2. Can level 2 services meet need alone?The Improving Outcomes Guidance clearly states that 25% of all cancer patients will require level 3 or 4 intervention. Therefore it is not sufficient to provide level 2 interventions by Level 2 trained cancer staff alone. In addition, evidence suggests that without ongoing supervision, level 2 trained individuals will not maintain their skills as this is not their core profession (e.g. Mannix et al 2006).
3.3. Providing services within existing mental health services
3.3.1. IAPTNHS England primary care mental health services since 2005 are often, but not always, referred to as Improving Access to Psychological Therapies ( IAPT) services. There are a number of factors to consider when providing psychological services to cancer patients within IAPT services:
• The provision of such services varies according to what is commissioned locally. Some services have access to Clinical and Counselling Psychologists, so are able to provide level 4
14
interventions, while others do not.• The current model for most IAPT services is
via GP practice and community-based clinics, and therefore does not integrate with acute hospitals, and as such it would be difficult to provide the day to day level 2 training and supervision required to support the holistic needs assessment, the delivery of level 2 psychological care, and offer ad hoc advice and consultation that a more integrated service can offer.
• IAPT are generic services for anxiety and depression. If cancer patients do not reach diagnostic levels of anxiety and depression they may not access all IAPT services. Therefore patients with issues such as problems adjusting, cancer-treatment-specific issues e.g. managing emotional lability on hormonal treatments, anticipatory nausea, post-radiotherapy fatigue, etc, problems engaging with care, thoughts and feelings about ending one’s life in the context of advancing disease, etc, cannot receive the help they require.
• If the patient is within active treatment this can often make the issues and concerns too complex to be managed within IAPT
• IAPT services are generic, and currently IAPT training does not include an understanding of cancer. However, if supported by level 4 experts with experience, IAPT services can provide good services to those patients with anxiety and depression who are not currently in active treatment or palliation (Highfield et al, 2015).
3.3.2 Secondary mental healthUnless service level agreements are in place, Mental Health Trusts do not routinely offer this input, and so cancer patients often fall between gaps in services, or try to access voluntary sector services which differ widely. The Best Practice Standards recommend promoting psychological well-being and preventing the onset of more serious mental ill health. Patients with cancer only access secondary mental health services if they have an active co-morbid mental health problem, which is an appropriate use of dedicated mental health team resources. It is important for teams who provide psychological services in cancer to have good working relationships with secondary mental health teams in case of the escalation of such a need.
3.4. Conclusion to providing servicesThe preferred model is to provide embedded psychological services to those in active treatment or palliation within the settings of the provision of such treatment, such as hospitals and hospices, but with the ability to work with people within the community. Such services sit outside mental health services provision, and currently should be allocated from cancer treatment budgets. However it is the hope that a separate tariff for psychological care related to medical conditions will be developed in the future.For those in survivorship, the choice to return to the cancer services provider or to access IAPT/primary care services should be offered.
4.0. The Arden Project
University Hospitals Coventry and Warwickshire (UHCW) in conjunction with Coventry & Warwickshire Partnership NHS Trust (CWPT) requested investment from Macmillan in a project to review the specialist psychological service provision for cancer patients and their families/carers across the Arden footprint. Currently, there is a wide variation of psychological services provided at levels 3 and 4 across the Arden geographical network, resulting in patient need not being adequately assessed, identified and treated. Models of service delivery vary according to local commissioning arrangements and access to specialist psychological services is not equitable across Coventry, Warwickshire and Worcestershire.
The project identified the existing services throughout Coventry, Warwickshire and Worcestershire with the aim of enabling the development of best practice models and pathways for psychological care for cancer patients. The project draws from scientific research, clinical expertise and recognised quality standards. The aim of the project was to develop links with commissioning leads within the Arden area and ensure that any developments are presented to the commissioners promoting a service that is sustainable and improving services accessible to cancer patients and to ensure standards are met and reduce variation in services.
15
The project stages were as follows:
1. Identify existing services, using the mapping tool developed by the project manager in appendix 8
2. Engagement with stakeholders and service users from each area to discuss their hopes and needs for psychological services
3. Estimating service requirements utilising an algorithm developed by Dr Alex King for the London Cancer Alliance (2014- for the tool see Appendix 9)
4. Of the four regions, three regions were found to be in need of further services
5. Regional reports were produced, and this information was submitted to the local commissioners.
6. Meetings were arranged to discuss the options for development of further services. For a summary, see appendix 10.
The reports were well received across the four main areas. It was noted that developing palliative care services is possible as this is directly funded by local commissioners. However, the way cancer services are funded by NHS England created a barrier to new funds being made available. At this point, it was recommended that psychological services for those cancer patients in active treatment should be provided within the multidisciplinary teams of cancer care. Unfortunately this is a locally
made decision, and continues to promote the regional variation in psychological services for cancer. However, with the evidence within this report, strong cases have been made to have psychological services staff as a key part of the workforce.
5.0 Conclusion
The emotional and psychological impacts of cancer are widely felt, by the patient, their relatives and carers, and the staff caring for them. Most individuals draw from their own
psychological resources, but up to 25% require a professional psychological intervention (NICE, 2004). It is clearly recommended in a number of national reports to have access to psychological support, and there is significant evidence to suggest that having psychological services embedded within cancer services benefits the patients, carers and staff. The Arden Project took this evidence and the opinion of stakeholders to commissioners to help them to develop local psychological services in cancer. However, the different way in which services are commissioned at different points of the cancer journey represents a barrier to developing cross-pathway services.

16
3 Counties Cancer Network (2013) Psychology Project BriefAll Party Parliamentary Group (2009). Report of the All Party Parliamentary Group on Cancer’s Inquiry into Inequalities in CancerArden Cancer Network: Psychological Support Cross Cutting Group (2012) Psychology Service, Baseline Mapping, British Psychological Society Specialist Interest Group in Palliative and Oncology Care (King, 2015): A Framework for Quality & Outcomes in Psycho-Oncology British Psychological Society Specialist Interest Group in Palliative and Oncology Care (2011). Induction to Clinical Practice (psychological support) in Oncology and Palliative CareCancer Action Team (2007) Holistic Common Assessment of Supportive and Palliative Care Needs for Adults with Cancer: Assessment Guidance. London, Cancer Action Team.Carlson LE and Bultz BD. (2004) Efficacy and medical cost offset of psychosocial interventions in cancer care: Making the case of economic analyses. Psycho-Oncology, 13, 837-849Chiles, Jeremy A., Lambert, Michael J. & Hatch, Adrin L. (1999). The Impact of Psychological Interventions on Medical Cost Offset: A Meta-analytic Review. Clinical Psychology: Science and Practice, Vol 6 No. 2 pp 206-220.
Department of Health (2007). Cancer Reform StrategyDepartment of Health (2011) Improving Outcomes: A Strategy for CancerDepartment of Health, (2004). National Service Framework for Long Term Conditions Department of Health (2008). End of Life Care Strategy – Promoting high quality care for all adults at the end of life. Department of Health (2011). No Health Without Mental Health: a cross-government mental health outcomes strategy for people of all ages. Fang F.,Fall, K., Mittleman, M.,et al (2012). Suicide and Cardiovascular Death after a Cancer Diagnosis. New England Journal of medicine, 366, 1310-1318.Highfield, J., Lowe, K et al (2015,submitted). Clinical Psychologists Training and Supervising IAPT therapists to work with Long Term Conditions and Medically Unexplained Symptoms- A Service development Project. Clinical Psychology Forum.Hotopf M., et al. (2002) Depression in advanced disease: a systematic review part 1. Prevalence and case finding. Palliative Medicine 16: 81-97IAPT (2008) Long Term Conditions Positive Practice GuideThe Kings Fund, (2011) Schwartz Center Rounds:
Evaluation of UK PilotsThe Kings Fund (2012) Long Term Conditions and Mental Health: the cost of co-morbiditiesLondon Cancer Alliance (2014), Developing a mental health and psychological support services for adults.Macmillan Cancer Support (2006) Worried sick: the emotional impact of cancer. Macmillan Cancer Support (2014) Dignity Must Not be Denied: How we can support and empower NHS staff to deliver a good experience of care to patients?Mannix, K. A., Blackburn, I. M., Garland, A., Gracie, J., Moorey, S., Reid, B., et al. (2006).Effectiveness of brief training in cognitive behaviour therapy techniques for palliative care practitioners. Palliative Medicine, 20, 579-584.National Audit Office (2005) Tackling Cancer: Improving the Patient Journey. London: The Stationary Office.National Cancer Intelligence Network, (2011) Economics of Cancer accessed at: http://www.ncin.org.uk/news_and_events/economicsNational Cancer Patient Experience Survey 2014 accessed at: https://www.quality-health.co.uk/resources/surveys/national-cancer-experience-survey/2014-national-cancer-patient-experience-survey
references
17
NHS Commissioning Support for London, (2010) A Model of Care for Cancer Services National End of Life Care Intelligence Network. Found at http://www.endoflifecare-intelligence.org.uk/home. Accessed November 2014.NHS England (2014) Business Plan 2014/15- 2015/16NHS Improving Quality (2014) Transforming End of Life Care in Acute Hospitals Programme (Transform Programme)National Institute of Health and Clinical Excellence (2004) Guidance on Cancer Services: Improving Supportive and Palliative Care for Adults with Cancer, The ManualNational Institute of Health and Clinical Excellence (2004) Guidance on Cancer Services. Improving Supportive and Palliative Care for Adults with Cancer. National Institute of Health and Clinical Excellence (2011). Quality Standard for End of Life Care for AdultsNHS Litigation Authority (2013) Risk Management Standards 2013-14Pan Birmingham Cancer Network http://www.birminghamcancer.nhs.uk/staff/clinical-guidelines/psychological%20support
Pinquart, M. and Duberstein, P. R. (2010), Depression and cancer mortality: a meta-analysis. Psychological Medicine, 40(11), 1797-1810Saxby, B. & Svanberg, P. (1998). The Added Value of Psychology to Physical Health Care. British Psychological Society, Division of Clinical Psychology.Schairer, C, Morris Brown, L., Chen, B, Howard, R et al (2006) Suicide After Breast Cancer: an International Population-Based Study of 723 810 Women. Journal of National Cancer Institute 98 (19), 1416-1419.Shaller, D. (2007), Patient centred-care. What does it take? The Commonwealth FundVanderwerker, L. C., Laff, R. E., Kadan-Lottick, N. S., McColl, S., & Prigerson, H. (2005). Psychiatric disorders and mental health service use among caregivers of advanced cancer patients. Journal of Clinical Psychology, 23(28), 1-9.Walker, J., Holm Hansen, C., Martin, P., Symeonides, S., Ramessur, R., Murray, G., & Sharper, M. (2014)Prevalence, associations, and adequacy of treatment of major depression in patients with cancer: a cross-sectional analysis of routinely collected clinical data. Lancet Psychiatry, vol 1 (5), p343–350,
18
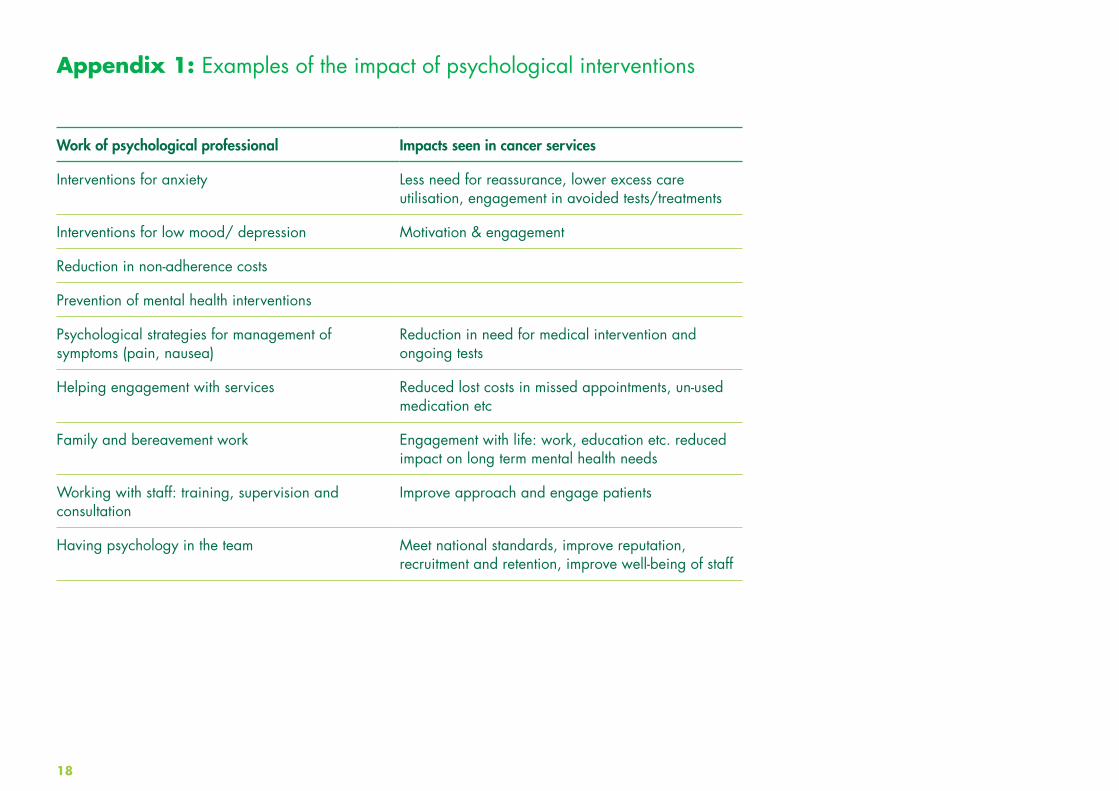
Appendix 1: Examples of the impact of psychological interventions
Work of psychological professional Impacts seen in cancer services
Interventions for anxiety Less need for reassurance, lower excess care utilisation, engagement in avoided tests/treatments
Interventions for low mood/ depression Motivation & engagement
Reduction in non-adherence costs
Prevention of mental health interventions
Psychological strategies for management of symptoms (pain, nausea)
Reduction in need for medical intervention and ongoing tests
Helping engagement with services Reduced lost costs in missed appointments, un-used medication etc
Family and bereavement work Engagement with life: work, education etc. reduced impact on long term mental health needs
Working with staff: training, supervision and consultation
Improve approach and engage patients
Having psychology in the team Meet national standards, improve reputation, recruitment and retention, improve well-being of staff
19
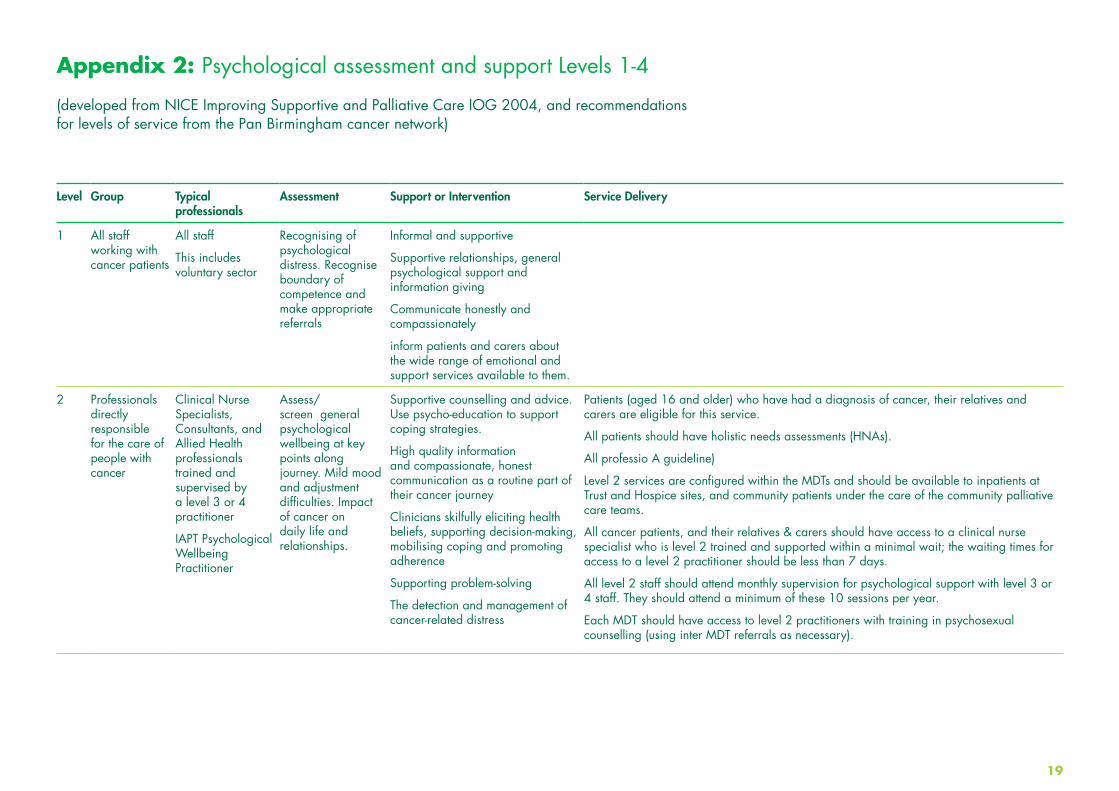
Level Group Typical professionals
Assessment Support or Intervention Service Delivery
1 All staff working with cancer patients
All staff
This includes voluntary sector
Recognising of psychological distress. Recognise boundary of competence and make appropriate referrals
Informal and supportive
Supportive relationships, general psychological support and information giving
Communicate honestly and compassionately
inform patients and carers about the wide range of emotional and support services available to them.
2 Professionals directly responsible for the care of people with cancer
Clinical Nurse Specialists, Consultants, and Allied Health professionals trained and supervised by a level 3 or 4 practitioner
IAPT Psychological Wellbeing Practitioner
Assess/screen general psychological wellbeing at key points along journey. Mild mood and adjustment difficulties. Impact of cancer on daily life and relationships.
Supportive counselling and advice. Use psycho-education to support coping strategies.
High quality information and compassionate, honest communication as a routine part of their cancer journey
Clinicians skilfully eliciting health beliefs, supporting decision-making, mobilising coping and promoting adherence
Supporting problem-solving
The detection and management of cancer-related distress
Patients (aged 16 and older) who have had a diagnosis of cancer, their relatives and carers are eligible for this service.
All patients should have holistic needs assessments (HNAs).
All professio A guideline)
Level 2 services are configured within the MDTs and should be available to inpatients at Trust and Hospice sites, and community patients under the care of the community palliative care teams.
All cancer patients, and their relatives & carers should have access to a clinical nurse specialist who is level 2 trained and supported within a minimal wait; the waiting times for access to a level 2 practitioner should be less than 7 days.
All level 2 staff should attend monthly supervision for psychological support with level 3 or 4 staff. They should attend a minimum of these 10 sessions per year.
Each MDT should have access to level 2 practitioners with training in psychosexual counselling (using inter MDT referrals as necessary).
Appendix 2: Psychological assessment and support Levels 1-4
(developed from NICE Improving Supportive and Palliative Care IOG 2004, and recommendations for levels of service from the Pan Birmingham cancer network)

20
3 Professionals trained and accredited in specific psychological therapies
Counsellor
IAPT High Intensity Therapist
Assess some psychopathology e.g. anxiety, depression, psychosexual problems. Refer those with complex or moderate to severe problems to level 4 services
Psychological interventions according to an explicit theoretical framework e.g. anxiety management and solution-focused therapy
Cancer patients, and their relatives & carers who are significantly distressed to the extent that engagement in treatment, maintenance or resumption of activities of daily living or important relationships are threatened, and this cannot be sufficiently addressed by level 1 or level 2 intervention should be referred for level 3 or 4 psychological support.
The patient feels unable to prepare for treatment because (s)he does not get enough information or does not understand it following level 2 intervention;
The patient does not feel able to establish a relationship of trust with the professionals who treat them;
The patient or family already has (had) other serious problems and stresses in their life that make significant demands on their coping resources;
The patient’s level of distress exceeds their current available support structures and level 2 intervention;
Problems in maintaining daily life functioning (e.g. work, finances, shopping, household tasks, looking after the children) are not addressed;
Significant bereavement reactions are anticipated pre-death.
4 Professionals registered/accredited with a mental health professional body
Clinical Psychologist
Counselling Psychologist
Liaison Psychiatrist
Assessment of complex and severe psychological problems including severe affective disorders, personality disorders, substance misuse and psychotic illness.
Specialist and bespoke psychotherapeutic or psychiatric interventions.
These include severe depression and anxiety, organic brain syndromes, severe inter-personal difficulties (including severe psychosexual problems), alcohol and drug-related problems, personality disorder and psychotic illness
Specialised psychological intervention focused on questions of adjustment, identity and mortality
Coordinating care in complex cases
The care of people with a diagnosis of pre-existing severe mental illness that has been exacerbated by cancer
The expert assessment and management of enduring emotional distress, psychosis , delirium , or cognitive difficulty triggered by cancer or its treatment
Psychological intervention at level 4 should be available for cancer patients, and their relatives & carers with the following additional risk factors
Risk factors in the patient/family: A history of psychiatric disorder Social isolation Dissatisfaction with past medical care Passive coping (i.e. not seeking information/not talking to friends/family)
Risk factors in the cancer: Limitation of daily life activities Disfigurement Poor prognosis/survival rates
Risk factors in the treatment: Disfigurement Isolation (such as in e.g. bone marrow transplant or thyroid radiation therapy) Debilitating or distressing side effects PTSD following surgery/treatment
Patients with primary and metastatic brain tumours frequently have additional cognitive and psychological problems and undergo personality changes.
Psychological assessment and support should therefore be an integral part of the MDT management of these patients.
Providers should ensure that there is access to clinical neuropsychology services for patients who need specialist intervention for cognitive, emotional or behavioural problems.
The provider will make sure that one member of the cancer network MDT (or equivalent) is nominated to maintain links with clinical psychology services.

21
Title Core role Core training Banding Level
Liaison Psychiatrists
Liaison Psychiatrists are medically trained professionals with a role for assessing acute risk and psychiatric morbidity within an acute hospital setting
Medical degree, foundation training plus specialty training. 13 years total.
Not under AfC 4
Clinical Psychologists
Clinical Psychologists are trained mental health professionals, trained within the NHS, with expertise in several modalities of psychological intervention and therapies, and are skilled in the training and supervision of others, and bringing a psychological perspective to systems. Includes a grounding in neuropsychology
6 years minimum training to doctorate level (Bachelors plus Doctorate). Training within NHS.
Minimum of two therapeutic approaches
Recognised by BPS and HCPC.
AfC band 7-9 4
Counselling Psychologists
Counselling psychologists are trained mental health professionals who use psychological theory and research in therapeutic work to help clients with a variety of problems
6 years minimum training to doctorate level (Bachelors plus Doctorate, doctorate pathway post 2012). Usual requirement to have previous counselling training
Trained in one therapeutic model
Trained in NHS or other settings
AfC band 7-9 4
Psychotherapists These are professionals typically focussing upon one specialist area of psychological therapy, including psychosexual therapists who specialise in the psychosexual impacts of cancer
Post graduate diploma recognised by BACP AfC band 6 upwards
3
Counsellors Professionals trained in counselling as a modality of psychological therapy.
BACP accredited one year course full time, two years part time. Diploma level. Choice of person centred, psychodynamic, or integrative approach
AfC band 6 3
High Intensity Therapists (IAPT)
GP based psychological therapists. Typically Cognitive Behavioural therapy or counselling
IAPT accredited one year course AfC band 6 & 7 3
Appendix 3: Typical training pathways for Level 3 and 4 service professionals
22
To illustrate how the differing professionals may work in differing levels of psychological support and intervention, three case studies are given.
Case study one:Susan is recovering following breast cancer. She is a 40 year old, married and has two children. She has been well supported by work. She has requested support with returning to “life as normal” as life feels different now, and it brings her mood down that others seem to have moved on. She has no mental health history but is struggling with existential issues feeling her work has no meaning any longer and no one around her really understands what she has been through.
Case study two:Jane is 70 years old. Her husband John was diagnosed with bowel cancer and is currently under the palliative care team. He is struggling physically. John used to be the more active one in the relationship and does not like his limitations. The team have clearly indicated that John does not have much longer left to live. Jane feels like she is seeing her husband slip away before her, and is very distressed.
Case study three:Andrew is 35, and has been diagnosed with myeloma. Due to lack of treatment response he has a poor prognosis. He has extensive bony disease and lesions which are painful and he feels unsightly, describing himself as looking “like a freak”. He is single and lives alone, and although he gets on with his family he does not feel able to talk with them. He has a history of personal trauma, including being physically bullied by his stepfather. The team are concerned about Andrew as he is often readmitted to the inpatient ward with confusing or difficult to explain symptoms of pain. He describes being angry at his diagnosis and terrified at what might ‘come next’. He has been ruminating recently about thoughts of a bone breaking at any time; thinking he may stretch in the night in bed and break his hip. This has made him fearful of light activity and he is therefore withdrawn and avoiding going out. Andrew admits to excessive alcohol use as his main form of coping. He began drinking heavily at aged 16 to cope with difficult feelings.
Appendix 4: Understanding what level 3 and 4 professional may offer, and illustrating the differences between levels 3 and 4
23
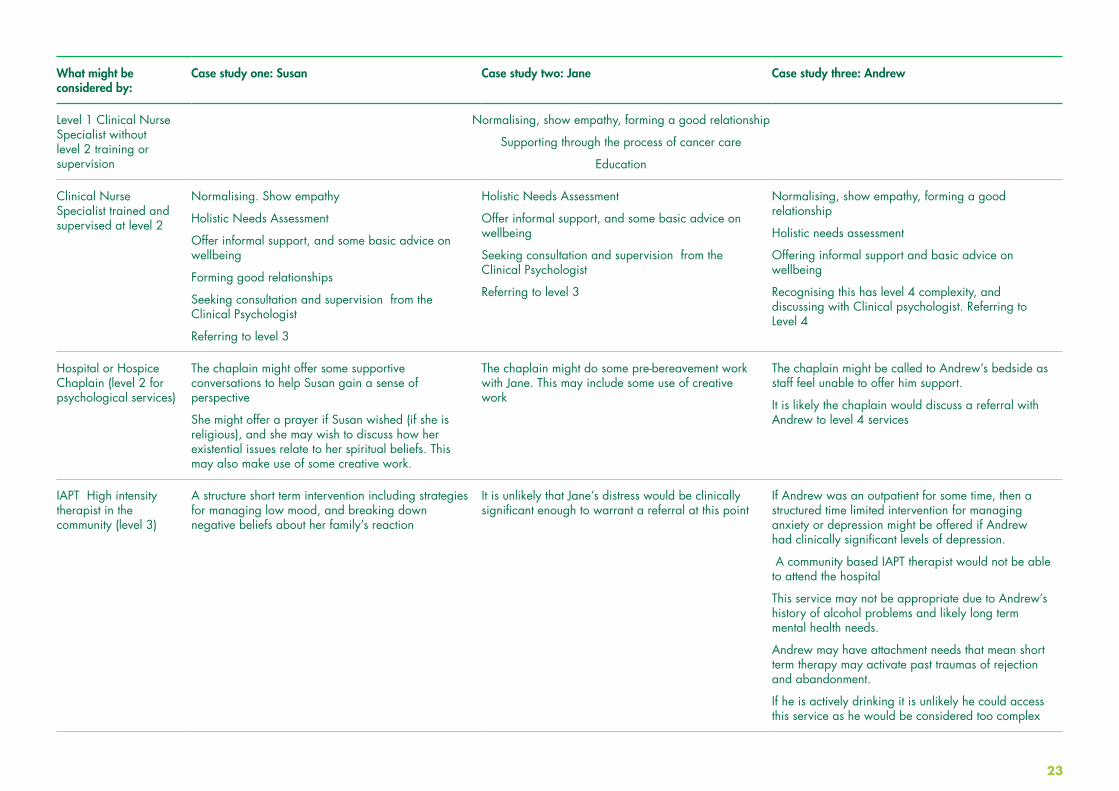
What might be considered by:
Case study one: Susan Case study two: Jane Case study three: Andrew
Level 1 Clinical Nurse Specialist without level 2 training or supervision
Normalising, show empathy, forming a good relationship
Supporting through the process of cancer care
Education
Clinical Nurse Specialist trained and supervised at level 2
Normalising. Show empathy
Holistic Needs Assessment
Offer informal support, and some basic advice on wellbeing
Forming good relationships
Seeking consultation and supervision from the Clinical Psychologist
Referring to level 3
Holistic Needs Assessment
Offer informal support, and some basic advice on wellbeing
Seeking consultation and supervision from the Clinical Psychologist
Referring to level 3
Normalising, show empathy, forming a good relationship
Holistic needs assessment
Offering informal support and basic advice on wellbeing
Recognising this has level 4 complexity, and discussing with Clinical psychologist. Referring to Level 4
Hospital or Hospice Chaplain (level 2 for psychological services)
The chaplain might offer some supportive conversations to help Susan gain a sense of perspective
She might offer a prayer if Susan wished (if she is religious), and she may wish to discuss how her existential issues relate to her spiritual beliefs. This may also make use of some creative work.
The chaplain might do some pre-bereavement work with Jane. This may include some use of creative work
The chaplain might be called to Andrew’s bedside as staff feel unable to offer him support.
It is likely the chaplain would discuss a referral with Andrew to level 4 services
IAPT High intensity therapist in the community (level 3)
A structure short term intervention including strategies for managing low mood, and breaking down negative beliefs about her family’s reaction
It is unlikely that Jane’s distress would be clinically significant enough to warrant a referral at this point
If Andrew was an outpatient for some time, then a structured time limited intervention for managing anxiety or depression might be offered if Andrew had clinically significant levels of depression.
A community based IAPT therapist would not be able to attend the hospital
This service may not be appropriate due to Andrew’s history of alcohol problems and likely long term mental health needs.
Andrew may have attachment needs that mean short term therapy may activate past traumas of rejection and abandonment.
If he is actively drinking it is unlikely he could access this service as he would be considered too complex
24
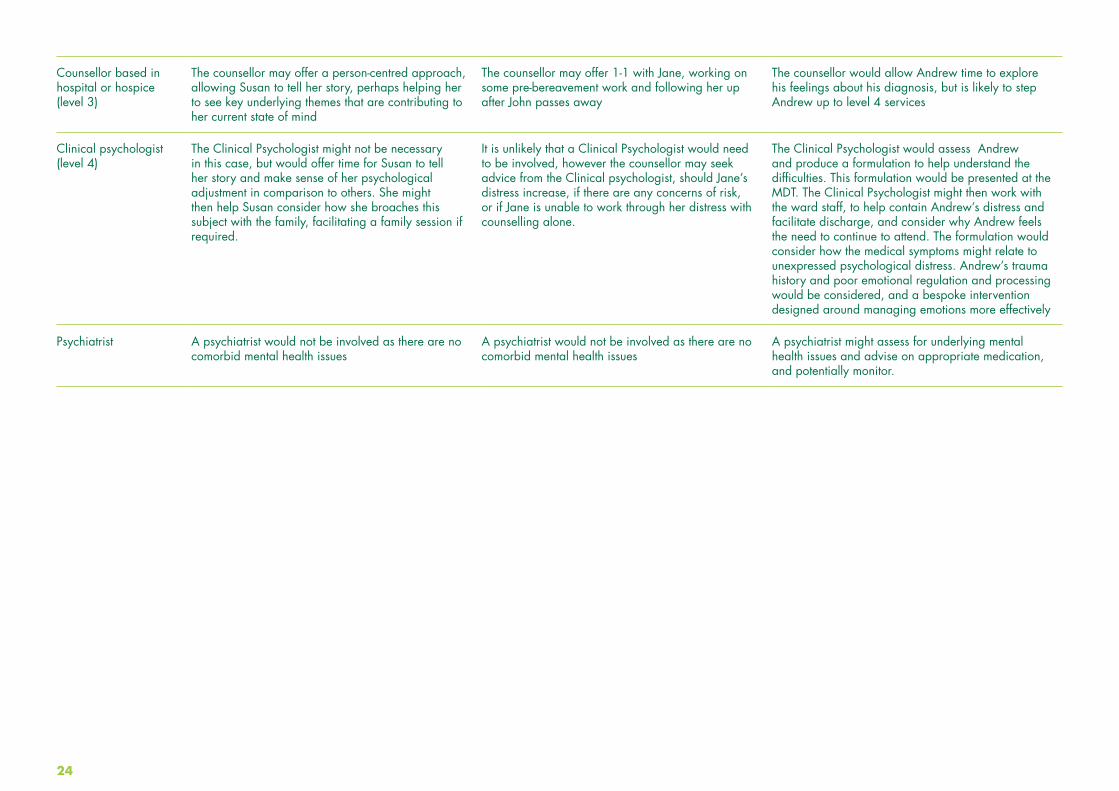
Counsellor based in hospital or hospice (level 3)
The counsellor may offer a person-centred approach, allowing Susan to tell her story, perhaps helping her to see key underlying themes that are contributing to her current state of mind
The counsellor may offer 1-1 with Jane, working on some pre-bereavement work and following her up after John passes away
The counsellor would allow Andrew time to explore his feelings about his diagnosis, but is likely to step Andrew up to level 4 services
Clinical psychologist (level 4)
The Clinical Psychologist might not be necessary in this case, but would offer time for Susan to tell her story and make sense of her psychological adjustment in comparison to others. She might then help Susan consider how she broaches this subject with the family, facilitating a family session if required.
It is unlikely that a Clinical Psychologist would need to be involved, however the counsellor may seek advice from the Clinical psychologist, should Jane’s distress increase, if there are any concerns of risk, or if Jane is unable to work through her distress with counselling alone.
The Clinical Psychologist would assess Andrew and produce a formulation to help understand the difficulties. This formulation would be presented at the MDT. The Clinical Psychologist might then work with the ward staff, to help contain Andrew’s distress and facilitate discharge, and consider why Andrew feels the need to continue to attend. The formulation would consider how the medical symptoms might relate to unexpressed psychological distress. Andrew’s trauma history and poor emotional regulation and processing would be considered, and a bespoke intervention designed around managing emotions more effectively
Psychiatrist A psychiatrist would not be involved as there are no comorbid mental health issues
A psychiatrist would not be involved as there are no comorbid mental health issues
A psychiatrist might assess for underlying mental health issues and advise on appropriate medication, and potentially monitor.
25
Dr James Brennan, Consultant Clinical Psychologist, BristolDr Carolyn Gordon, Clinical Psychologist, WarwickshireSarah Fathers, Bereavement Counsellor, WarwickshireSandy Farley, Psychosexual Counsellor, CoventryJane Fizor, Head and Neck Cancer Counsellor, WorcestershireDr Alex King, Consultant Clinical Psychologist, LondonDr Shradha Lakani, Consultant Clinical Psychologist, WalsallDr Heidi Napier, Consultant Clinical Psychologist, DudleyDr Ray Owen, Consultant Clinical Psychologist, HerefordshireDr James Parker, Clinical Psychologist, WarwickshireDr Louise Price, Consultant Clinical Psychologist, CoventryDr Sue Smith, Consultant Clinical Psychologist, LondonRosalind Talbot, Consultant Clinical Psychologist, WarwickDr Ruth Telfer, Consultant Clinical Psychologist, North WalesDr Inigo Tolosa, Consultant Clinical Psychologist, BirminghamDr Rachel Warren, Clinical Psychologist, Warwickshire
The West Midlands Psychological Services for Cancer Expert Advisory Group
Appendix 5: Psychological services and psycho-oncology individuals consulted for expert opinion of psychological services in cancer

26
A. UNDERPINNING KNOWLEDGE
1. Medical Epidemiology Causes Nature and course of cancer (long term conditions and life limiting illnesses) Treatments and side-effects Follow-up and physical rehabilitation Process of dying (i.e. Liverpool Care pathway for the dying)
2. Theoretical Models A number of clinical and health psychology models may be useful and appropriate in different contexts. For example: An understanding of the bio-psycho-social-spiritual approach to person-centred holistic healthcare Illness Representation Model Social-cognitive models of adjustment Attachment theory Coping theory Models of loss, grief and bereavement
2. Service Context The Multi-disciplinary Team. The roles of professionals whom the patient with cancer is likely to meet, e.g. GPs, surgeons, oncologists, specialist and ward nurses, radiographers, AHPS, Palliative Care Clinical Nurse Specialists (e.g. Macmillan Nurses), hospice staff, etc. Psychological Support services (Levels 3 & 4). The role of psychological support within the MDT and cancer services; face-to-face clinical work (individuals, couples, carers, families, groups); working with in-patients and out-patients; consultation; teaching; staff support and supervision; the role of cancer information and support; communication training, etc.
B. CORE CLINICAL SKILLS
1. Assessment Bio-psycho-social-spiritual approach Expectations of psychological support Understanding problems from within the client’s narrative Client’s understanding of what cancer represents Assessing within time constraints Defining the problem(s) to be addressed Who is the client? (systemic understanding) Personal and socio-cultural context of the client
The client’s strengths and resources and the positive responses they have already made etc. Risk assessments
2. Formulation Using pertinent theoretical models to help understand the client’s problems and distress, and to suggest ways of helping clients overcome them. Negotiating with the client the parameters of the service that can be offered What are reasonable targets for intervention given the possible restraints? (e.g. the illness and its prognosis, ongoing treatment, the distance the client is from the service etc). If the problems predate the cancer or are relatively unconnected with the illness, should the client be offered treatment by psychologists working in the oncology setting or be referred to other services?
3. Intervention Strategies Individuals, couples, carers, families, groups Normalisation Self-management Rehabilitation approaches (e.g. survivorship) Adjustment
Appendix 6: Suggested required knowledge and competencies of level 3 and 4 staff
This is taken directly from Induction to Clinical Practice (psychological support) in Oncology and Palliative Care, BPOS SIGOPAC BPS 2011
27
CBT approaches (e.g. Adjuvant Psychological Therapy) Psycho-educational approaches Systemic ways of working Couple and family therapy Loss and bereavement care Psychodynamic approaches Post-traumatic growth
4. Evaluation Screening methods/tools for identifying client concerns Auditing clinical effectiveness, both individually and across a service Service evaluations, etc. Conducting needs assessments
C. PERSONAL AND PROFESSIONAL SKILLS
Ethics: confidentiality, respecting and working with denial, euthanasia and assisted dying, communication within teams Self-care – impact of working long-term with issues of mortality, grieving for clients, clinical supervision and personal support Spiritual-existential issues (both personal and clinical) Staff support Communication training and other staff training Research – as a balance with clinical work Working with medical agendas
D. TRANSLATING PREVIOUS KNOWLEDGE AND EXPERIENCE
1. Appreciating differing frameworks: Clarifying expectations: differences and similarities Contracting Understanding agendas and expectations of different professionals Clarifying service expectations and remit
2. Recognising and utilising transferable skills: Mix of supervision and ‘on the job’ learning Facilitative aspect
3. Two Levels: Shadow existing Psychological Support Staff recognised as working at Level 3 & 4) Consult other professionals prior to developing service
28
These are taken directly from the British Psychological Society Specialist Interest Group in Palliative and Oncology Care document: A Framework for Quality & Outcomes in Psycho-Oncology (King, 2015), where further detail may be found.
We suggest that the following six domains are considered when evaluating quality & outcomes in a psycho-oncology service:A. Is this service safe?B. Is this service equitable, while also focused on those most in need?C. Is this service timely & responsive?D. Is this service respectful, collaborative and patient-centred?E. Is this service offering effective interventions?F. Is this service contributing to efficient multidisciplinary care?
To address these domains, psycho-oncology services are encouraged to gather and consider multiple, convergent sources of data, including: I. Key Performance Indicators II. Activity LevelsIII. Staff Qualification, Accreditation & RegistrationIV. Quantitative Patient Self-Report Measures V. Qualitative Patient FeedbackVI. Feedback from Professional ColleaguesVII. Additional Data Sources
Appendix 7: Outcome measures for a psycho-oncology service

29
AREA 1 AREA 2
Clinical Commissioning Group- key point of contactPopulation servedAcute TrustHospitalsWhere is the Cancer Centre?HospicesNumber of new cancer diagnoses per yearStaffing numbersWTE Psychological Staffing: level 3 onc & haem
Level 3 palliativeLevel 4 onc & haemLevel 4 PalliativePrimary carePsychiatry
Pathway Diagnostics and active treatmentSurvivorshipPalliationBereavementFamily work
Groups and innovationsLevel 2 trainingLevel 2 SupervisionPeer review compliance: TrainingAt least one clinical core member of the team should have completedL2 TrainingPeer review compliance: Supervision The level 2 practitioner(s) should receive a minimum of 1 hours clinical supervision by a level 3 or level 4 practitioner per monthRISKSNeeds
Appendix 8: Mapping tool
30
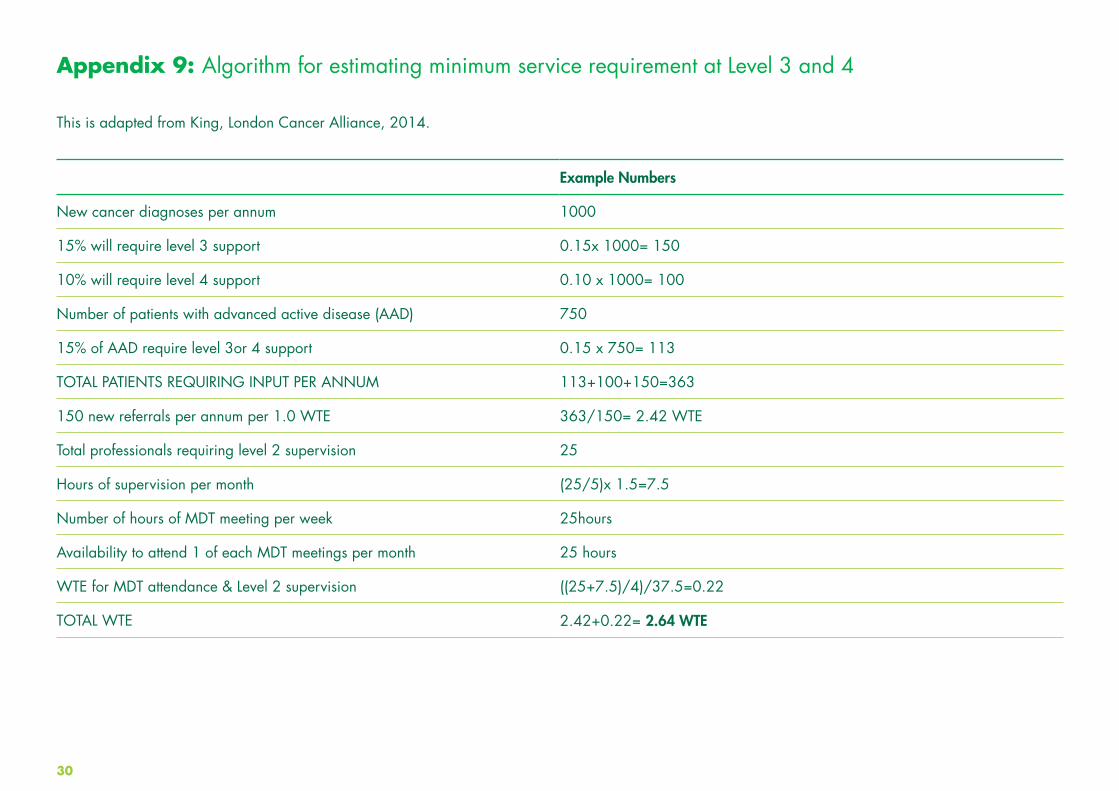
This is adapted from King, London Cancer Alliance, 2014.
Example Numbers
New cancer diagnoses per annum 1000
15% will require level 3 support 0.15x 1000= 150
10% will require level 4 support 0.10 x 1000= 100
Number of patients with advanced active disease (AAD) 750
15% of AAD require level 3or 4 support 0.15 x 750= 113
TOTAL PATIENTS REQUIRING INPUT PER ANNUM 113+100+150=363
150 new referrals per annum per 1.0 WTE 363/150= 2.42 WTE
Total professionals requiring level 2 supervision 25
Hours of supervision per month (25/5)x 1.5=7.5
Number of hours of MDT meeting per week 25hours
Availability to attend 1 of each MDT meetings per month 25 hours
WTE for MDT attendance & Level 2 supervision ((25+7.5)/4)/37.5=0.22
TOTAL WTE 2.42+0.22= 2.64 WTE
Appendix 9: Algorithm for estimating minimum service requirement at Level 3 and 4

31
New cancer diagnoses per annum
Estimated patients with advanced active disease
Estimated numbers requiring L3/4 intervention
Staff who may require level 2 training and supervision
Total WTE psychological services available
Additional psychological workforce required Level 3
Additional workforce required Level 4
Actions for 2015
Coventry and Rugby 2395 1454 744 46 2.22 WTE
(1.4 WTE is non NHS)
2.74 WTE 1.44 WTE 2.0WTE Clinical Psychology posts to be developed, in oncology & palliative care
Warwickshire North 700 586 234 12 0.9 WTE 0.2 WTE 0.6 WTE 0.8WTE Clinical Psychology post to be developed in community palliative care
Warwickshire South 1420 862 441 12 3.33 WTE None. None Maintain services
Worcestershire 3300 1842 1009 65 5.67 WTE
(3.74 is non NHS)
2.7 WTE 2.6 WTE Utilise report in the development of a Clinical Health Psychology/ Long Term Conditions Service
Appendix 10: Service gaps highlighted within the Arden Project, with considered actions
32
When you have cancer, you don’t just worry about what will happen to your body, you worry about what will happen to your life. How to talk to those close to you. What to do about work. How you’ll cope with the extra costs.
At Macmillan, we know how a cancer diagnosis can affect everything. So when you need someone to turn to, we’re here, because no one should face cancer alone. We can help you find answers to questions about your treatment and its effects. We can advise on work and benefits, and we’re always here for emotional support when things get tough.
Right from the moment you’re diagnosed, through your treatment and beyond, we’re a constant source of support to help you feel more in control of your life.
We are millions of supporters, professionals, volunteers, campaigners and people affected by cancer. Together we make sure there’s always someone here for you, to give you the support, energy and inspiration you need to help you feel more like you. We are all Macmillan.
For support, information or if you just want to chat, call us free on 0808 808 00 00 (Monday to Friday, 9am–8pm) or visit macmillan.org.uk
© Macmillan Cancer Support, January 2015. Registered charity in England and Wales (261017), Scotland (SC039907) and the Isle of Man (604).Also operating in Northern Ireland. Printed using sustainable materials. Please recycle.