Embed Size (px)
DESCRIPTION
Best Practice Collection Publication: Reliable information for effective community health plans, programs and policies.
Citation preview

San Gabriel Valley and Metropolitan Service Planning Area Health Office (SPA 3 & 4)
DEVELOPING A COMMUNITY LIAISING PROGRAM IN LOS ANGELES COUNTY
Los Angeles County Department of Public Health
July 2009
SPA 3 & 4 CASE STUDY
San Gabriel Valley and Metropolitan Service Planning Area Health Office (SPA 3 & 4)
SPA 3 & 4 BEST PRACTICE COLLECTIONRELIABLE INFORMATION FOR EFFECTIVE COMMUNITY HEALTH PLANS, PROGRAMS AND POLICIES
M. RICARDO CALDERÓN, SERIES EDITOR
July 2009
1
The SPA 3 & 4 Area Health Office Best Practice Collection fulfilled the DHS local level goal to restructure and improve health services by “establishing and effectively disseminating to all concerned stakeholders comprehensive data and information on the health status, health risks, and health care utilization of Angelinos and definable subpopulations”.1 Since September 2006, when the Los Angeles County Department of Public Health (DPH) became a serperate department from DHS, the SPA 3 & 4 Best Practice Collection continues to provide reliable infromation for the effective development and implementation of community plans, programs and policies. It is a program activity of the SPA 3 & 4 Information Dissemination Initiative created with the following goals in mind:
To highlight lessons learned regarding the design, implementation, management and evaluation of public health programs
To serve as a brief theoretical and practical reference for program planners and managers, community leaders, government officials, community based organizations, health care providers, policy makers and funding agencies regarding health promotion and disease prevention and control
To share information and lessons learned in SPA 3 & 4 for community health planning purposes including adaptation or replication in other SPA’s, counties or states
To advocate a holistic and multidimensional approach to effectively address gaps and disparities in order to improve the health and well-being of populations
The SPA 3 & 4 Information Dissemination Initiative is an adaptation of the Joint United Nations Program on HIV/AIDS (UNAIDS) Best Practice Collection concept. Topics will normally include the following:
1. SPA 3 & 4 Viewpoint: An advocacy document aimed primarily at policy and decision-makers that outlines challenges and problems and proposes options and solutions.
2. SPA 3 & 4 Profile: A technical overview of a topic that provides information and data needed by public, private and personal health care providers for program development, implementation, and/or evaluation.
3. SPA 3 & 4 Case Study: A detailed real-life example of policies, strategies or projects that provide important lessons learned in restructuring health care delivery systems and/or improving the health and well being of populations.
4. SPA 3 & 4 Key Materials: A range of materials designed for educational or training purposes with up-to-date authoritative thinking and know-how on a topic or an example of a best practice.
At a GlanceSAN GABRIEL VALLEY SERVICE PLANNING AREA (SPA 3) METROPOLITAN SERVICE PLANNING AREA (SPA 4)241 North Figueroa Street, Room 312Los Angeles, California 90012
(213) 240-8049
The Best Practice Collection is a publication of the San Gabriel Valley (SPA 3) and Metropolitan Service Planning Area (SPA 4). The opinions expressed herein are those of the editor and writer(s) and do not necessarily reflect the official position or views of the Los Angeles County Department of Public Health (LAC/DPH). Excerpts from this document may be freely reproduced, quoted or translated, in part or in full, acknowledging SPA 3 & 4 as the source.
Internet: http://publichealth.lacounty.gov/spa3/Internet: http://publichealth.lacounty.gov/spa4/Internet: http://mrcalderon.com
LOS ANGELES COUNTY BOARD OF SUPERVISORS
Gloria Molina, First District
Mark Ridley-Thomas, Second District
Zev Yaroslavsky, Third District
Don Knabe, Fourth District Michael D. Antonovich, Fifth District
DEPARTMENT OF PUBLIC HEALTH
Jonathan E. Fielding, MD, MPH, MBA.Director of Public Health and County Health Officer
Jonathan E. FreedmanChief Deputy Director
Deborah Davenport, RN, PHN, MS.Director, Community Health Services
BEST PRACTICE COLLECTION TEAM
M. Ricardo Calderón, MD, MPH, Series Editor.Manuscript Author & SPA 3 & 4 Area Health Officer
Carina Lopez, MPH. Project Manager, Information Dissemination Initiative
COMMUNITY LIAISON REPRESENTATIVES
1
DEVELOPING A COMMUNITY LIAISING PROGRAM IN LOS ANGELES
Philip Perez, BSN, PHN Monica Muñoz, BSN, PHN John Jennings, BSN,PHN Patricia Alexander, BSN, PHN Marie Kreimann, BSN, PHNDavid Caley, BSN, PHN, PHNSYon Silvia Walker, MSN, PHNGrace Lim BSN,PHN Lucille Rayford, BSN, PHN Heidi Behm, BSN, PHN Emily Avilla, BSN, PHN Troy Legaspi, BSN, PHN Betsy Blankfield BSN, PHN Dior Hildebrand BSN, PHN Melanie Donor BSN, PHNReeza Epino, BSN, PHNRosaisela Bernal BSN, PHNDebra Dorst-Porada BSN, PHNWay Wen BSN, PHNIling Wang BSN, PHN Shannon Moody, BSN, PHNJose Escobar, MSN, PHNS

July 2009DEVELOPING A COMMUNITY LIAISING PROGRAM IN LOS ANGELES
DEVELOPING A COMMUNITY LIAISING PROGRAM IN LOS ANGELES
2
EXECUTIVE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 I. DESCRIPTION OF THE INNOVATIVE PROGRAM AND BEST PRACTICE . . . . . . . . . . . . 4
1. PROGRAM BACKGROUND: THE OVERVIEW
2. PROBLEM STATEMENT: THE CHALLENGE
3. PROGRAM APPROACH: THE INNOVATIVE SOLUTION
4. PROGRAM ACCOMPLISIHMENTS: THE OUTCOMES
II. DESCRIPTION OF HOW THE INNOVATION BENEFITS THE COUNTY, THE DEPARTMENT OF PUBLIC HEALTH, AND/OR THE PUBLIC . . . . . . . . . . . . . . . . . . . . . . .13
1. PROGRAM BUDGET: THE SAVINGS AND COST-EFFECTIVENESS
2. PROGRAM SUMMARY: THE BENEFITS
III. APPENDICES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .15
1. CLP CONCEPT PAPER
2. CLP WORKSHOP LEARNING OUTCOMES
3. CLP TRAINING WORKSHOP AGENDA
4. CLP FRAMEWORK
5. LOS ANGELES COUNTY PRODUCTIVIY AND QUALITY AWARD
Table of Contents

DEVELOPING A COMMUNITY LIAISING PROGRAM IN LOS ANGELES July 2009
EXECUTIVE SUMMARY
The Los Angeles County Depart-ment of Health Services (DHS) restructured Public Health Programs and Services in 1998/99 through the implementation of eight Service Planning Area Health Offices. These offices assumed the responsibility to (1) improve the health status of the population, (2) better serve county residents, (3) revitalize the public health system, and (4) move toward more cost-effective services. Since the health status of a population cannot be improved by medical and public health interventions alone, and in view of projected budget deficits and reductions in the work-force, the Metropolitan Los Angeles Service Planning Area Health Office (SPA 4) conceptualized and piloted a Community Liaising Program (Ap-pendix 1). This program redirected DHS resources and utilized commu-nity resources and assets to create a network of alliances and coop-erative agreements to strengthen, expand and diversify public, private, and non-profit health programs. Based on six strategic domains --Community Networking, Commu-nity Mobilization, Strategic Partner-ing, Resource Development, Private Sector Leveraging, and Policy Development-- this unique and unprecedented program changed informal community relations into effective partnerships and imple-mented more than 60 low cost/no-cost initiatives addressing unmet health and social needs during a 10-year period. As a result, status quo approaches inherent in large bureaucratic settings gradually changed into effective value-added interventions that moved public health into the 21st century.
Realizing the vision of healthy people in healthy communities is possible only if all sectors of society are mobilized to engage as authen-tic partners in creating the condi-tions for good health. According to the “2002 Institute of Medicine’s The Future of the Public’s Health in the 21st Century” publication, “we must be led by those who have mastery of the skills to mobilize, coordinate and direct broad collab-orative actions within the complex public health system”. Consequent-ly, the Community Liaising Program is a case story of the vision, leader-ship, culture change, innovation and perseverance required to refine and hone the skills of leaders at every level and, particularly, to utilize a systematic framework of strategies to involve key stakeholders from different industries and sectors of society in health promotion, well-ness and disease prevention and control.
The Community Liaising Program (CLP) was acknowledged at the 2003 17th Annual County of Los Angeles Productivity and Quality Awards Program “Enriching Lives”. It was then presented nationally at the 2003 (Developing a Community
3
Liaising Program in Los Angeles County) and 2006 (Emerging Role of Public Health Nurses as Commu-nity Liaisons in Los Angeles County) American Public Health Association Meetings. In May 2009, CLP was institutionalized in the eight Service Planning Areas of the Department of Public Health (DPH) following a 10-year culture change and innova-tion process. Self-directed SPA-specific, 5 to 10 people work teams for a total of 75 people follow the CLP Framework (Appendix 4) to operationalize the DPH Strategic Plan and support the County of Los Angeles Strategic Goals. More specifically: (a) leadership develop-ment efforts and targeted interven-tions focus on six programmatic areas –non-communicable diseases, injury prevention and control, emer-gency preparedness and response, healthy eating and active communi-ties (HEAC), health promotion, and communicable disease prevention and control, (b) health protection and improvement efforts target the four neighborhood environments in which people are born, live, go to school and work ---built, social, economic and service environments, and (c) expected outcomes aimed to reduce the burden of disease and injury in Los Angeles County by treating disease conditions, reducing risk factors for disease, and focusing on the underlying determinants of health.
The Community Liaising Program has set a new trend and direction for public health practice in the County of Angeles. We trust that the reader will (a) recognize that protecting and improving the health of a population is a shared respon-sibility among all sectors of society, (b) promote and enhance the six
!e Community Liaising Program is a strategic approach aimed to lead, organize or support a concerted public, private and non-pro"t sector e#ort to strengthen, expand and diversify health promotion, wellness, and disease prevention and control.
EXECUTIVE SUMMARY

July 2009DEVELOPING A COMMUNITY LIAISING PROGRAM IN LOS ANGELES
4
PROGRAM BACKGROUND AND PROBLEM STATEMENT
strategic domains of an effec-tive Community Liaising Program, and (c) advocate for a community liaising capacity as a vital part of the health system for identifying population priorities and needs, de-veloping responses and evaluating results, and reducing the burden of disease and injury among individu-als, families and communities.
I. DESCRIPTION OF THE INNOVATIVE PROGRAM AND BEST PRACTICE
1. PROGRAM BACKGROUND: THE OVERVIEW
An innovative public health prac-tice entitled ”Community Liaising Program (CLP)” was created in the fall of 1999 by the Metropolitan Los Angeles Service Planning Area Health Office (SPA 4) as a result of the restructuring and revitaliza-tion efforts of the Department of Health Services (DHS). The program was designed to more effectively protect, maintain and improve the health status of Los Angeles County residents. The initial purpose of CLP was to consolidate public, private and non-profit planning efforts to enhance the quality and quantity of health services and improve the health status of SPA 4 residents. The goals of CLP were to (a) increase awareness of, and generate more support for, health promotion, wellness and disease prevention and control, and (b) identify and secure additional resources --hu-man, material, financial—in order to strengthen, expand and diversify public, personal and private health services. The specific objectives of the program were to (a) implement the “Area Health Office Concept” recommended by the 1977 Breslow
Report, as part of the restructur-ing and revitalization of DHS, (b) develop departmental capabilities in community health improvement, and (c) reduce the burden of disease and injury in Los Angeles County.
The strategic rationale of the Com-munity Liaising Program can be described simply by answering the following “What, Why, Who, How, and When” questions:
WHAT? A strategic approach aimed to lead, organize and/or support a concerted public, private and non-profit sector effort to strengthen, expand and diversify prevention programs and public health services.
WHY? Health promotion, wellness and disease prevention and control are affected by individual, social, economic and environmental factors within and beyond communities that must be addressed comprehen-sively.
WHO? Protecting and improv-ing the health and wellbeing of a population is a shared responsibility among residents, public institutions, private for profit and non-profit organizations, key stakeholders, opinion leaders and policymakers.
HOW? CLP comprises a systematic framework of strategies to involve key stakeholders from different industries and sectors of society in health promotion, wellness and disease prevention and control.
WHEN?
• Phase I: 1999 – 2003: Program Development, SPA 4 Staff Recruit-ment and Training, and Program Implementation.
• Phase II: 2004 – 2006: Program Centralization and Program Consoli-dation at the SPA 3 & 4 Area Health Office.
• Phase: 2007 – 2008: Program Decentralization and Institutional-ization within the SPA 3 & 4 Public Health Nursing Program.
• Phase IV: 2009+: Program Expan-sion, SPA 1 through 8 Staff Recruit-ment and Training, Program Insti-tutionalization within Community Health Services, and County-Wide Program Implementation beginning May 2009.
2. PROBLEM STATEMENT: THE CHALLENGE
The challenges to introduce a new program practice within the Depart-ment of Health Services (DHS), particularly Public Health Programs and Services once they became a separate department from DHS in September 2006, can be appreciat-ed by a discussion of the macro and micro environments, as well as the state of the public health programs, services and workforce at the end of 1999.
2.1. Macro (National) Environ-ment
Health promotion and disease prevention and control are affected by individual, structural, environ-mental and economic factors within
Community Liaising is a approach to link the di#erent stakeholders of a community health system to ful"ll the desired population and health outcomes.

DEVELOPING A COMMUNITY LIAISING PROGRAM IN LOS ANGELES July 2009
and beyond communities that must be viewed comprehensively. Protect-ing and improving the health of a population is a shared responsibility among residents, public institutions, private for profit and non-profit orga-nizations, key stakeholders, opinion leaders and policy makers. Yet, many think that government is the entity responsible for assuring the health status and wellbeing of populations. Governmental actions and agencies constitute the backbone of all efforts to assure the health of the pub-lic. However, governmental public health agencies still suffer from grave under-funding, political neglect, and continued exclusion from the very
6 Strategic Domains of the Community Liaising
forums in which their expertise and leadership are most needed to assure an effective public health system. No single individual or group can assure the conditions needed for health for an entire community or popula-tion. All sectors of society --“public, private and non-profit”-- have a critical role to play and an interest in creating conditions that make good health possible. Also, the health infrastructure and capacity for such approaches must be permanent and sustained by adequate human, material and economic resources. In brief, gov-ernment has a duty to assure the public’s health; government cannot
do it alone; other sectors have a role to play and, thus, there is a need for inter-sectoral engagement.
2.2. Micro (Local) Environment
Los Angeles County is approximately 4,084 square miles and more than 80 miles of coastline. In the late 1990s, the estimated population was close to 10 million residents, a population larger than those of 42 states in the U.S. Over 30% of the adult population did not have medical insurance and 35% had no dental insurance. The population had a low literacy rate reported at 53% and there were over 200,000
STRATEGIC DOMAINS OF THE COMMUNITY LIAISING
5
July 2009DEVELOPING A COMMUNITY LIAISING PROGRAM IN LOS ANGELES
6
people considered homeless, includ-ing an increasing number of women and children. More than 2 ! million people lived in families with income below 125% of the federal poverty level. The percentage of teenag-ers who began prenatal care in the first trimester was much lower than women as a whole, 58% and 69% respectively. The infant mortality ratio was greatest by far in African Americans, next highest in White, followed by Hispanics, and least among Asians. Reported communi-cable disease rates were declining substantially while non-communica-ble disease morbidity and mortality had risen to become the paramount health problems. On the other hand, a great deal of change was seen in the health care system due to a bud-get shortfall within DHS close to $1 billion causing difficult choices to be made, including the closure of clinics, hospitals, emergency departments and trauma centers.
2.3. State of the Public Health Programs and Services (PHPS)
The state of public health in Los Angeles County was summarized in July 1977 by a UCLA School of Public Health Technical Assistance Group in their “Report of Review of Public Health Programs and Services, Los Angeles County Department of Health Services’. This Review Group was headed by Lester Breslow, MD, MPH, Professor & Dean Emeritus and, thus, became known as the Breslow Report. The key findings of this report were the following:
• “Using age-adjusted mortality to crudely indicated health status, Los Angeles County ranks alongside the large California Counties having relatively high death rate; San Diego,
Orange and Santa Clara Counties have lower rates. Within Los Angeles County the large disparities in heath among social and ethnic groups constitute a major public health chal-lenge.
• The public health mission is fulfilling society’s interest in assuring conditions in which people can be healthy.
• Since the 1972 merger of pub-lic health with the personal health services (mainly hospital) side of DHS, and increasingly the past few years, PHPS has been affected by:
o Substantial decline of local ap-propriations for public health, rel-ative both to those in Los Angeles County for disease treatment and to similar appropriations in other jurisdictions throughout the county.
o A series of chaotic reorganiza-tions, especially very recently.
o Severe loss of capacity to perform basic public health func-tions such as health surveillance, disease prevention and commu-nity health activities.
At present PHPS:
• Includes many highly qualified, dedicated staff members, but these are insufficient in numbers and range of competencies for the task.
• Suffers from considerable tension among its elements, with diminished morale.
• Is increasingly dominated by time-limited, categorical state and federal funds for specific aspects of health, with no overall long term program planning based on local needs.
• Maintains poor communication within the agency and with the com-
munities it serves, thereby generating mistrust by the Board of Supervisors as well as others.
• Is hamstrung by many County pro-cedures, especially in personnel and contracting matters”.
The Breslow Report made critical recommendations to restructure and revitalize DHS and strengthen public health programs and services in order to protect and advance the health in the County. These recommendations fell under the following six thematic areas:
o Continue the “Reconstruction of DHS Leadership”, including the appointment of a Director of Public Health and Health Officer.
o Develop and establish and adequate data-information-communication system to identify problems, develop policy, plan and manage services and evaluate their effect.
o Initiate community-oriented-planning for Public Health in appropriate geographic areas to ascertain accurately the commu-nity’s health problems and deal with them.
o Reorganize Public Health Programs and Services including what eventually became eight Service Planning Area Health Offices each with an Area Health Officer.
o Establish an effective training and recruitment program.
o Streamline county procedures and increase the budget.
The Breslow Report contributed to reinvigorate and reorganize the public health priorities and resources
STATE OF PUBLIC HEALTH PROGRAMS AND SERVICES

DEVELOPING A COMMUNITY LIAISING PROGRAM IN LOS ANGELES July 2009
7
PROGRAM APPROACH: THE INNOVATIVE SOLUTION
of DHS with the goal to restore and elevate the status of public health in the Department and Los Angeles County. It also paved the way for the creation of Area Health Offices with delegated tasks and responsibilities to enhance the health status and wellbeing of residents in each Service Planning Area.
3. PROGRAM APPROACH: THE IN-NOVATIVE SOLUTION
3.1. The Community Liaising Concept
The Community Liaising Program is a strategic approach aimed to lead, organize or support a concerted public, private and non-profit sector effort to strengthen, expand and diversify prevention programs and public health services. It was created by M. Ricardo Calderón in the fall of 1999 when he assumed the posi-tion of Area Health Officer for the Metropolitan Service Planning Area (SPA 4) at the Los Angeles County Department of Health Services. The CLP is based on Calderón’s work as Regional Director for Latin America and the Caribbean of the United States Agency for International De-velopment AIDS Control and Preven-tion (AIDSCAP) Project implemented by Family Health International. It draws from the lessons learned and best practice solutions described in his “HIV/AIDS SYNOPSIS Publication Series” along with the realization that: (1) health promotion, wellness, and disease prevention and control are affected by individual, social, economic and environmental factors within and beyond communities that must be addressed comprehensively, and (2) protecting and improving the health and wellbeing of a population is a shared responsibility among resi-
dents, public institutions, private for-profit and non-profit organizations, key stakeholders, opinion leaders and policymakers (see http://www.fhi.org/en/hivaids/pub/archive/handbooks/multidimensionalmodel.htm).
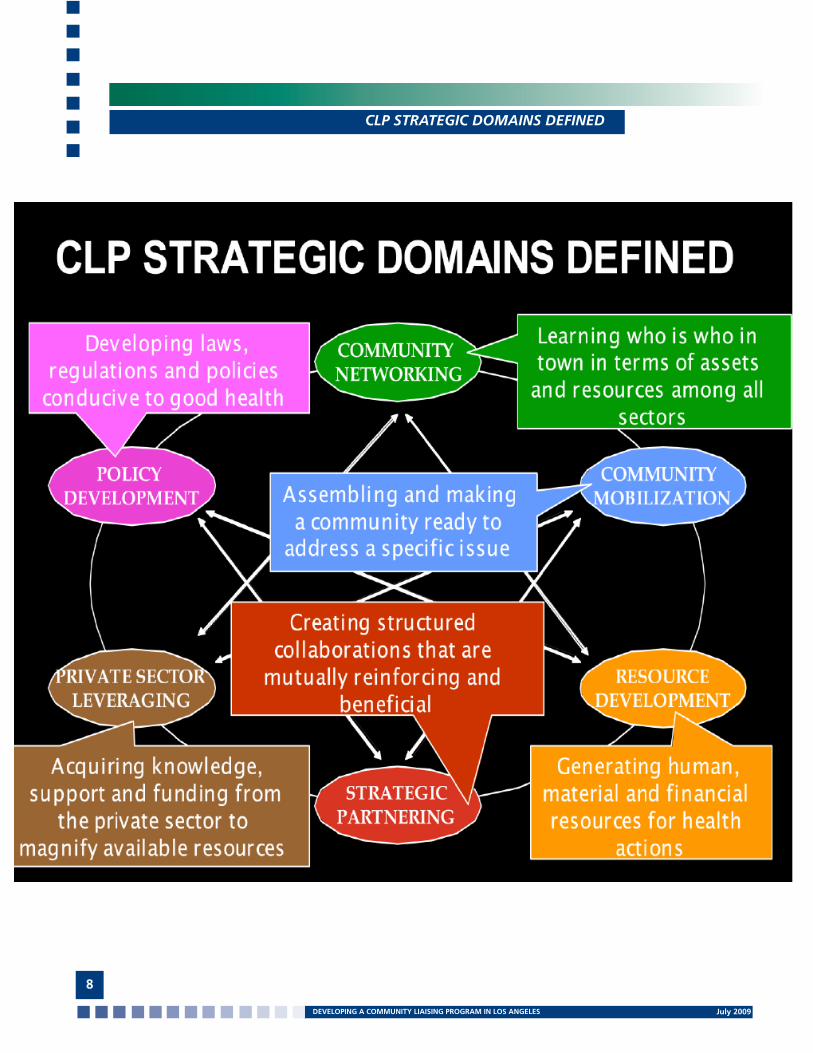
The Community Liaising Program comprises six strategic domains reflecting areas of competence, skills and activity that Area Health Offices must master in order to mobilize, coordinate, and direct broad collab-orative actions within complex public health systems. It is a systematic framework of strategies to involve key stakeholders from different industries and sectors of society in health promotion, wellness and dis-ease prevention and control. As Area Health Offices identify and prioritize health issues, establish goals and objectives, apply evidence-based practices, and develop population and program indicators, the CLP approach can be utilized for success-ful implementation of institutional vision and overall strategy ultimately resulting in increased awareness and resources for health, enhanced Area Health Offices performance, bet-ter health outcomes, and improved health status and wellbeing of indi-viduals, families and communities.
!e Community Liaising Program comprises six strategic domains re$ecting areas of com-petence and skills that that Area Health O%ces must master in order to mobilize, coordinate, and direct broad collaborative actions within complex public health systems.
In the fall of 1999, a Leadership Development Strategy was created to pave the way for the implemen-tation of CLP, change the culture of the SPA 4 public health workforce, bring innovation to the system, de-velop capacities to manage change and, most importantly, develop self-directed work teams and leaders at every level of DHS. The SPA 4 Ad-ministrator was given direct respon-sibility for the traditional “Manage-ment Meetings” that usually take place in bureaucracies like DHS to deal with operational issues. In this way, three-hour Leadership Team Meetings were established twice a month for all staff in supervisory or managerial positions along with the Area Health Office technical staff for health education, nutrition and epi-demiology. Leadership Team Meet-ings focused exclusively on public health leadership development of senior, midlevel and low-level managers and supervisors. This was done through lectures, audiovisual presentations, reading assignments, peer to peer education, problem-solving and trouble-shooting discussions, specific projects and assignments, team development, and practical exercises. Twice a month leadership meetings were held during the first three years (1999 – 2003) of the Area Health Office implementation. Thereafter, three hour meetings continued until today focusing still on leadership development. Currently, the Area Health Office manages the SPA 3 & 4 Service Planning Areas through a 12-member Senior Leadership Team and a 36 to 40 Leadership Team. In order to staff the Community Liaising Program, a reassignment of tasks and responsibilities was conducted within the SPA 3 and 4 nursing program. This enabled the
July 2009DEVELOPING A COMMUNITY LIAISING PROGRAM IN LOS ANGELES
CLP STRATEGIC DOMAINS DEFINED
8

DEVELOPING A COMMUNITY LIAISING PROGRAM IN LOS ANGELES July 2009
COMMUNITY LIAISING DOMAINS
9
Area Health Office to initially re-direct 2 full time public health nurses to pilot CLP efforts assuming the role of Community Liaison Representatives (CLR). These CLRs were supported and assisted by Area Health Office technical and administrative staff uti-lizing a matrix structure and self-di-rected work team approach. In time, two additional nurses were added for a total of 4, two in SPA 3 and two in SPA 4, a Community Liaising Pro-gram Director was appointed, and six additional nurses contributed to the program on a part time basis. Little by little, CLRs were also appointed in other Service Planning Area Health Offices.
As was described in the Section 2: Program Background: The Overview, CLP implementation took place through four phases. The major efforts of Phase I: 1999 – 2003, were Program Development, SPA 4 Staff Recruitment and Training, and Program Implementation. Phase II: 2004 – 2006, focused efforts on Program Centralization and Program Consolidation at the SPA 3 & 4 Area Health Office. Phase III: 2007 – 2008, embarked on the ambitious strategy to conduct Program Decentralization and Institutionalization within the SPA 3 & 4 Public Health Nursing Program. The goal of this particular phase was two-fold, (1) decentralize program
activities, i.e., delegating community liaising tasks, responsibilities and decision-making throughout SPA 3 & 4 relatively away from the central au-thority of the Area Health Officer and Community Liaising Program Director in order to create fewer management tiers within the organizational struc-ture, widen the span of liaising activi-ties, and develop a bottom-to-top flow of decision-effecting ideas, and (2) ensure program institutionaliza-tion, i.e., making the community liais-ing concept, tasks, functions and net-works become embedded within SPA 3 & 4 as an established public health role and activity, particularly within the nursing program. Critical to this

July 2009DEVELOPING A COMMUNITY LIAISING PROGRAM IN LOS ANGELES
THE COMMUNITY LIAISING CONCEPT
10
phase was the integration of four Area Nurse Managers (ANMs) in SPA 3 & 4 as CLP Program Directors based at the Hollywood/Wilshire, Central, Monrovia and Pomona Health Cen-ters (April 2007). The span of control of ANMs had already been expanded in previous years. In addition to their traditional public health nursing re-sponsibilities, ANMs assumed the role of Acting Health Center Directors and Team Leaders for several Community Health Improvement Initiatives. ANMs had already moved, conceptually and in practice within the SPA 3 & 4 Area Health Office, to more empowered, influential and valued leadership posi-tions. They, in turn, had empowered and delegated more responsibilities to their subordinate staff, particularly Pubic Health Nursing Supervisors (PHNS). ANMs assumed the responsi-bility to:
1. Serve as resource and community liaising experts in each of the health centers.
2. Link community liaising efforts to the work of the health center and, particularly, field activities of the nurs-ing and public health investigation programs.
3. Develop a community liaising capacity in each health center by informing, educating, training and engaging other public health staff in community liaising efforts.
4. Coordinate health promotion and disease prevention and control efforts among public, private and non-profit institutions both within the specific geographical coverage of each health center and among other PHN-Community Liaison Representa-tives.
5. Provide support and assistance to the nursing program as a whole including, but not limited to, district public health nursing activities.
6. Provide continuity and follow up to current community liaising activities ensuring nursing program involvement.
7. Perform other duties as described in the PHN-Community Liaison Rep-resentative position description or as needed by the Nursing Program and/or the Area Health Office. The centralized CLP Director position assumed at the same time the role of the first District Public Health Nursing Supervisor/Community Liaison Rep-resentative reporting directly to the Area Nurse Manager at the Monrovia Health Center. This was a pivotal move to decentralize and institution-alize CLP. More specifically, it was an effort to “role-play” as well as to expand the role of the District-Public Health Nurse Supervisor (D-PHNS) positions through community liais-ing functions. Inherent in this move were the Area Health Office efforts to (a) regroup resources, (b) enhance capacity building and widen the span of community liaising efforts, (c) increase the Area Nurse Manager's accountability in community liaising, (d) make D-PHNs true leaders in their communities, (e) reinforce the critical concept of “lateral relationships and influence” instead of a command and control, or top-bottom approach, and (f) model the way, pave the road, and reshape the job of a D-PHNS. These efforts to decentralize, institutional-ize, and widen the span of communi-ty liaising activities took place at three different levels and were carried out by three different staffing structures as follows:
1. PHN-Community Liaison Repre-sentatives working with frontline staff in each and all public health centers in SPA 3 & 4.
2. A District-PHNS/Community Liaison Representative (at Monrovia
Health Center) modeling the way and working with other SPA 3 & 4 D-PHNS as well as D-PHNS colleagues from other Area Health Offices.
3. The SPA 3 & 4 Area Health Officer promoting and advancing community liaising and working with Area Medi-cal Directors and Area Nurse Manag-ers including peers and colleagues from other Area Health Offices.
The appointment of a new Director for Community Health Services in 2008, who had been an Area Nurse Manager in SPA 4 and an Area Health Officer in SPA 1 and 2, brought a renewed vision to strengthen the public health infrastructure to more effectively address 21st century public health threats, be they a result of nat-ural or manmade disasters, emerging infectious diseases, or rising epidem-ics and escalating healthcare costs of chronic diseases. The timing was ideal, therefore, to move into Phase IV: 2009 +: Program Expansion, SPA 1 through 8 Staff Recruitment and Training, Program Institutionalization within Community Health Services, and Countywide Program Implemen-tation beginning May 2009.
The Community Liaising Program was officially launched country-wide in all Service Planning Areas on May 18, 2009 with a one-week intensive training workshop. The overall learn-ing outcome of this workshop aimed to equip Area Health Offices with competencies and skills to mobilize, coordinate and direct broad collab-orative actions to strengthen, expand and diversify prevention programs and public health services (Appendix 2: CLP Training Outcomes and Ap-pendix 3: CLP Training Program). The specific goal was to develop a 70 to 75 CLP workforce comprising Area Health Officers, Area Medical Direc-tors, Area Nurse Managers, Public

DEVELOPING A COMMUNITY LIAISING PROGRAM IN LOS ANGELES July 2009
11
Health Nurse Supervisors, Community Liaison Representatives, Health Educa-tors, Emergency Preparedness Public Health Nurses, Homelessness Coordi-nator, and Senior Staff from Commu-nity Health Services. All-day, monthly follow-up workshops are planned for 12 months to reinforce the knowl-edge and skills gained in the program launch and guide the development of community health improvement net-works and initiatives. A key milestone in program institutionalization is the fact that the cost of the one-week and follow-up training is paid by the Community Liaising Program itself through leveraged funds from one of its grants, the “Healthy Eating, Active Communities Grant” funded by The California Endowment.
4. PROGRAM ACCOMPLISH-MENTS: THE OUTCOMES
A total of 32 Community Health Improvement Initiatives were imple-mented in SPA 3 & 4 during the first 3 years of the program. These initia-tives, ranging from short-term (weeks or months) to long-term projects (6+ years), corresponded to 3 of the 10 nationally recognized Essential Public Health Services (EPHS) as follows:
• Eleven initiatives focused on EPHS #3: Inform, educate and em-power people about health issues.
• Seven initiatives focused on EPHS #4: Mobilize community partnerships and action to identify and solve health problems.
• Fourteen initiatives concen-trated on EPHS #5: Link people to needed personal health services and ensure the provision of health care when otherwise unavailable.
These initiatives were implemented jointly with community-based or-ganizations, academic institutions, faith-based communities, for-profit organizations, and other county and government agencies. They operated at no additional cost to the County. Staff was redirected from nursing to this program as Community Liaison Representatives. They carried out the extensive community work that the Public Health Nurses do not have the time to do, i.e., assess unmet com-munity health and social needs, link people with programs and services, mobilize community leaders and resources, and develop community partnerships.
By 2006, an additional 35 Commu-nity Health Improvement Initiatives were added for a total of 67. These initiatives strengthened, expanded and diversified prevention, healthcare and public services through:
• Additional funding for the health department and communi-ty-based organizations.
• Specific projects and services in the areas of homelessness, built environment, policy change, obe-sity, nutrition and physical activity, emergency preparedness, and
• Representation at local, state and national meetings and confer-ences.
A sample of some of these Commu-nity Health Improvement Initiatives include, but are not limited to, the following key and/or award winning projects:
1. 2004-2003 Mesoamerican Research and Intervention Project: $457,600.00 estimated annual cost avoidance; $136,014.00 estimated annual cost savings; $583,000.00 total estimated benefit.
2. 2002-2003 Community Liaising Program: $583,000.00 estimated an-nual cost avoidance and benefit.
3. 2002-2003 Service Integration Project between Los Angeles Free Clinic and Hollywood/Wilshire Health Center: $74,888.00 estimated annual cost avoidance; $51,250.00 estimat-ed annual cost savings.
4. Healthy Eating and Childhood Obesity Prevention Grant: 2-year $150K program.
5. California Nutrition Network Grant: >$700K to the LAC/DHS Nutri-tion Program.
6. Quality Assurance of Health Care Providers: >$3M cost avoidance.
7. Healthy Eating – Active Commu-nities Grant: $204,000 for the Califor-nia Center for Public Health Advocacy (CCPHA), $125,000 for the Baldwin Park Unified School District (BPUSD), and $125,000 for LAC/DPH per year for 4 years reflecting direct cost sav-ings to LAC/DPH of $500,000. This, plus $1,316,000 awarded to CCPHA and BPUSD, represented an infusion of $1,816,000 in public health and prevention measures for the residents of Baldwin Park. In addition, the grant was renewed for an additional 16 months ending June 2010 at $625,000 for a grand total infusion of $2,441,000 in prevention dollars for Baldwin Park.
8. Breast Health Promotion Taskforce of San Gabriel Valley
• 2008 Hispanic Breast health Conference ($10K)
• 2009 Asian Guard Your Breast Health Conference ($15K)
9. Youth Activism Against Obesity: 2-year $613,261 program.
PROGRAM ACCOMPLISHMENTS
July 2009DEVELOPING A COMMUNITY LIAISING PROGRAM IN LOS ANGELES
CLP STRATEGIC QUESTIONS TO ANSWER
12

DEVELOPING A COMMUNITY LIAISING PROGRAM IN LOS ANGELES July 2009
10. Health and Faith Coalition of San Gabriel Valley
11. SPA 3 & 4 Human Resource De-velopment Initiative
12. Critical input, technical advisory services, meaningful contributions and/or facilitation of the following initiatives and funding:
• Homeless Health Care: $60K + $223K, UHHP
• Homelessness: $20M & $80M, LAC/BOS
• EatWellLiveBetter.org: $50K
• Tobacco Cessation: $25K
• API Obesity Grant: $1M
• Road to Health: >$700K, COPE
• Dental Health Initiative for the Homeless: $70K, Tzu Chi Founda-tion
• Specialty Care Grant: $271,800, Kaiser Permanente
• Hepatitis A and B Vaccina-tion Initiative: Health Christian Foundation, Tzu Chi Foundation El Monte and Tzu Chi Foundation Alhambra. • Student Body Mile Club: $1000, Temple City Elementary School Assistance Grant.• Annual Mobile Healthcare Clinics for the Homesless• Health Care Access and Cancer Survey: $5K, City of Hope
II. DESCRIPTION OF HOW THE IN-NOVATION BENEFITS THE COUN-TY, THE DEPARTMENT OF PUBLIC HEALTH, AND/OR THE PUBLIC:
1. PROGRAM BUDGET: THE SAV-INGS AND COST-EFFECTIVENESS
The SPA 3 and 4 community health improvement initiatives have been
implemented jointly with a variety of stakeholders at no additional cost to the County. As previously described, staff was redirected from the public health nursing program to com-munity liaising. They carry out the extensive community work that Public Health Nurses do not have the time to do. They assess unmet community health and social needs and spend much of their time conceptualizing and linking programs and services, mobilizing community leaders and resources, interacting with and devel-oping community partnerships, and seizing opportunities and capitalizing on existing community assets and resources. SPA 3 & 4 communities have seen an increase in programs and services at non-traditional hours by both traditional and non-traditional providers which, in turn, has improved access to health and social services and empowered them to better (1) care for themselves and their families, (2) help others and their communities, (3) access and under-stand Los Angeles County services, and (4) benefit from new and existing programs and services.
In preparation for the 2003 17th An-nual County of Los Angeles Produc-tivity and Quality Awards Program, a 2002-2003 Cost Avoidance, Cost Savings and Annual Revenue was per-formed. Based on nomination guid-ance from this program, estimates were made as follows:
• Cost Avoidance: 32 initiatives at $1200 per month (cost of field of-fice space, supplies, equipment and utilities) = $384,000.00 per year; 2 Public Health Nurses at $7,083 per month (1.0 FTE salary + 25% benefits = $170,000.00 pr year; 1 Epidemiol-ogy Analyst at $417.00 per month (0.10 FTE salary + 25% benefits) = 5,000.00 per year; 1 Health Educa-tor at $417.00 per month (0.10 FTE salary + 25% benefits) = $5,000.00
per year; 1 Secretary III at $333.00 (0.10 FTE salary + 25% benefits) = $4,000.00 per year; 1 Area Health Officer at $1,250.oo per month (0.10 FTE salary + 25% benefits) = $15,000.00 per year for a Grand Total of $583,000.00.
• Cost Savings: Calculations of cost savings were not made at this time due to lack of population data and a model to assess the impact of prevention efforts and the number and cost of hospital visits averted. It was felt that if these capabilities were available or developed, the estimated savings would far exceed $1 million per year.
• Annual Revenue: No estimate of annual revenue was made for the 17th Annual Productivity and Qual-ity Awards program. However, per Section 4: Program Accomplishments: The Outcomes, the Community Liaising Program enabled an infu-sion of resources for both DPH and community partners in the range of millions of dollars. An accurate financial impact of the Commu-nity Liaising Program is beyond the scope of this publication and, thus, a thorough financial analysis is strongly recommended including the develop-ment of financial models to assess community impact and outcomes. In any event, CLP has (a) contributed over $10,000,000 in cost avoidance, cost savings and annual revenue to the health system as a whole in Los Angeles, (b) enabled the development of critical Board of Supervisor’s home-lessness initiatives ranging from $20 to $80 million and, more importantly, (c) enhance the performance of the health system as a whole, expanded access to healthcare, focused public health efforts on critical 21st cen-tury public health challenges, and increased DPH responsiveness to the expressed priorities and needs of the population.
DESCRIPTION OF HOW THIS INNOVATION BENEFITS LAC DPH
13

July 2009DEVELOPING A COMMUNITY LIAISING PROGRAM IN LOS ANGELES
2. PROGRAM SUMMARY: THE BENEFITS
The Community Liaising Program created in 1999 was "institutional-ized" in 2009 at DPH. Over $30,000 has been spent to date to develop and train the new countywide CLP workforce. Capacity building ex-penditures were paid by the SPA 3 & 4 “Healthy Eating and Active Communities Grant” funded by The California Endowment. A unique, 75-people workforce is now in place utilizing CLP competencies to implement the Department of Public Health Strategic Plan, as well as to support the Los Angeles County Strategic Goals. More importantly, (1) successful interventions from the SPA 3 & 4 Healthy Eating and Active Programs have been integrated as a component of the departmental county-wide programming, (2) the new workforce is strengthening, expanding and diversifying the work and scope of DPH, particularly Com-munity Health Services and Service Planning Area Health Offices, and (3) a departmental capacity is growing and developing to address chronic diseases, the cause of death of 80% of county residents; primarily heart disease, cancers and stroke due to four modifiable behaviors -- alcohol consumption, smoking, poor nutrition and lack of physical activity.
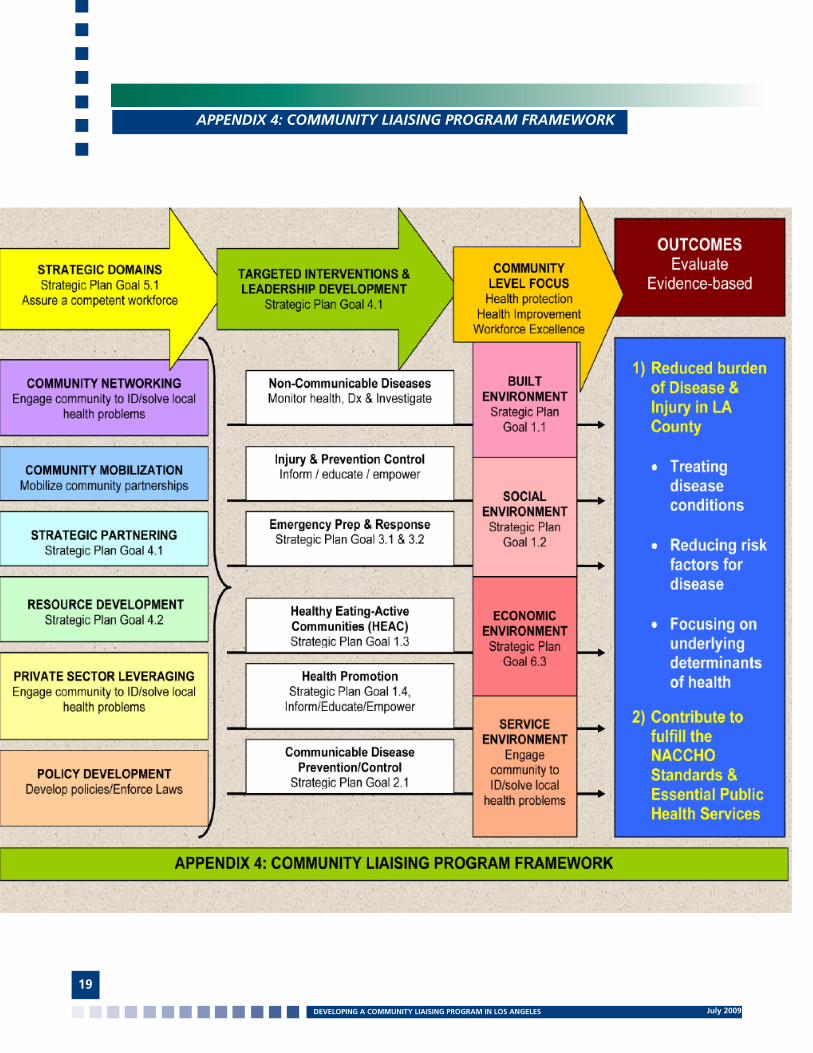
The Community Liaising Program Framework (Appendix #4) has changed public health practice in Los Angeles County setting a new trend and direction, changing the way County did business, and moving sta-tus quo to 21st Century Public Health Interventions by:
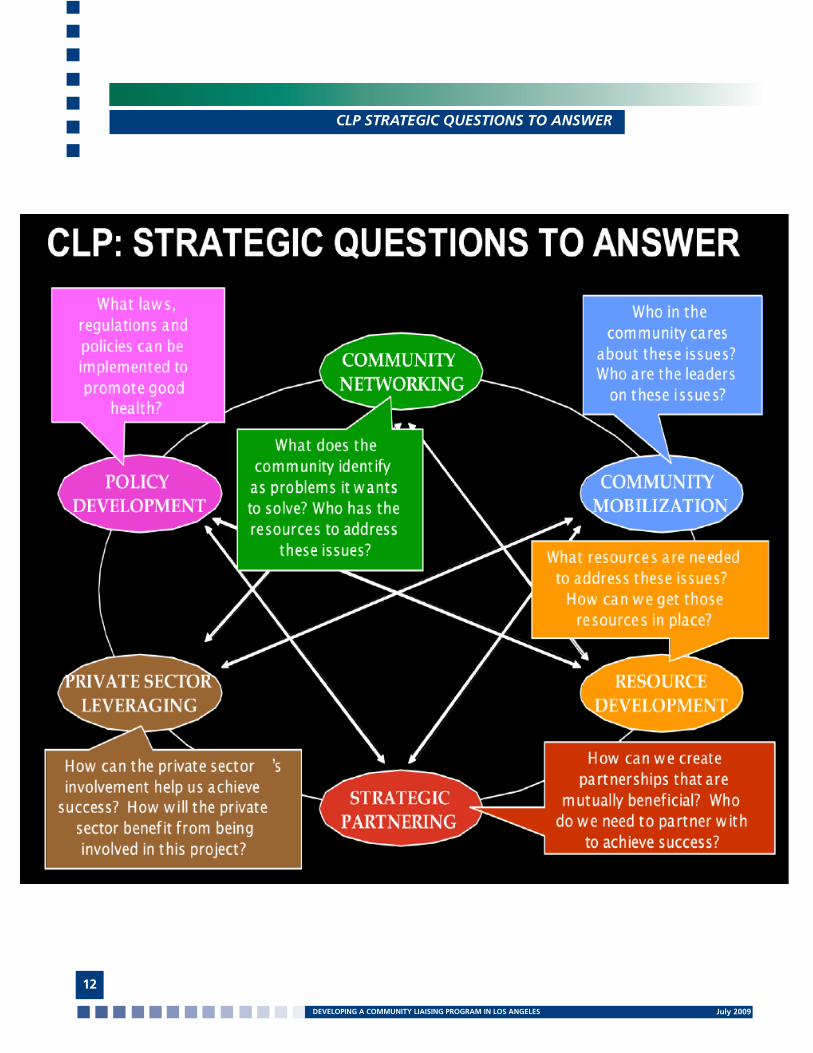
1. Utilizing the six competencies of the CLP Strategic Domains:
a. Community Networkingb. Community Mobilizationc. Strategic Partneringd. Resource Developmente. Private Sector Leveragingf. Policy Development
2. Targeting Leadership Develop-ment and Interventions at five programmatic levels:
a. Non-Communicable Diseasesb. Injury Prevention and Controlc. Health Eating and Active Communitiesd. Prevention and Health Promotione. Communicable Diseases
3. Focusing on four Placed-Based Neighborhood Environments:
a. Built Environmentb. Social Environmentc. Economic Environmentd. Service Environment
4. Reducing the Burden of Dis-ease and Injury by:
a. Treating disease conditionsb. Reducing risk factors for diseasec. Focusing on the underlying determinants of health
In summary, the County of Los Angeles is better positioned today to (a) enhance the performance of the Department of Public Health and the health system as a whole, (b) achieve further extraordinary improvements, (d) not fall short of its potential, and (e) create environments conducive to good health, and (f) develop the most effective health policies, programs and services with available resources. This has, is, and will continue to be reflected through additional human,
DESCRIPTION OF HOW THIS INNOVATION BENEFITS LAC DPH
14
financial and physical resources for health promotion, wellness and dis-ease prevention and control resulting in healthier individuals and families and living longer in healthier com-munities.

DEVELOPING A COMMUNITY LIAISING PROGRAM IN LOS ANGELES July 2009
APPENDIX 1: CONCEPT PAPER
COMMUNITY LIAISING PROGRAM (CLP)*Community Health Services, Los Angeles County Department of Public Health
The Community Liaising Program is a strategic approach aimed to lead, organize and support a concerted public, private and non-profit sector effort to strengthen, expand and diversify prevention programs and public health services. It was created by M. Ricardo Calderón in the fall of 1999 when he assumed the position of Area Health Officer for the Metropolitan Service Planning Area (SPA 4) at the Los Angeles County Department of Health Services. The CLP is based on Calderón’s work as Regional Director for Latin America and the Caribbean of the United States Agency for International Development AIDS Control and Prevention Project implemented by Family Health International. It draws from the lessons learned and best practice solutions described in his “HIV/AIDS SYNOPSIS Publication Series” along with the realization that: (1) health promotion, wellness, and disease prevention and control are affected by individual, social, economic and environmental factors within and beyond communities that must be addressed comprehensively, and (2) protecting and improving the health and wellbeing of a population is a shared responsibility among residents, public institutions, private for-profit and non-profit organizations, key stakeholders, opinion leaders and policymakers (See http://www.fhi.org/en/hivaids/pub/archive/handbooks/multidimensionalmodel.htm).
The Community Liaising Program comprises six strategic domains reflecting areas of competence, skills and activity that Area Health Offices must master in order to mobilize, coordinate, and direct broad collaborative actions within complex public health systems. It is a systematic framework of strategies to involve key stakeholders from different industries and sectors of society in health promotion, wellness and disease prevention and control. As Area Health Offices identify and prioritize health issues, establish goals and objectives, apply evidence-based practices, and develop population and program indicators, the CLP approach can be utilized for successful implementation of institutional vision and overall strategy ultimately resulting in increased awareness and resources for health, enhanced Area Health Offices performance, better health outcomes, and improved health status and wellbeing of individuals, families and communities.
APPENDIX 1
15
July 2009DEVELOPING A COMMUNITY LIAISING PROGRAM IN LOS ANGELES
APPENDIX 2: CLP WORKSHOP LEARNING OUTCOMES
LAC/DPH/CHS - COMMUNITY LIAISING PROGRAM WORKSHOP LEARNING OUTCOMES
May 18, 2009
OVERALL LEARNING OUTCOME: At the completion of this program, Area Health Offices will be equipped with competencies and skills to mobilize, coordinate and direct broad collaborative actions to strengthen, expand and diversify prevention programs and public health services.
SPECIFIC LEARNING OUTCOMES: At the completion of this program, participants will be able to:
1. Describe the CHS strategic vision and new direction in terms of the Community Liaising Program (Deborah Davenport).
2. Describe the six strategic domains of the Community Liaising Program –Community Networking, Community Mobilization, Resource Development, Strategic Partnering, Private Sector Leveraging and Policy Development (M. Ricardo Calderón).
3. Describe principles, models, sample interventions, examples and effective strategies to empower, engage, organize and mobilize communities for local public health efforts (Lourdes Baezconde-Gabarnati).
4. Explain policy advocacy approaches, lessons learned and best practices to address public health challenges including the improvement of children’s health environments by changing public policy (Harold Goldstein, LA Policy Summit).
5. Discuss their leadership and communication styles in terms of their MBTI preferences including an increased commitment to teamwork and performance (Richard Moore).
6. Promote a broader definition of public health including a 3-level approach to improving population health and the critical role of the Community Liaising Program (Jonathan E. Fielding).
7. Discuss how the social determinants of health –social and economic conditions in which people are born, grow, live, work and age, including the health system—determines their health status and wellbeing (M. Ricardo Calderón, Lourdes Baezconde-Gaberrnati, Jonathan E. Fielding).
8. Contribute to create healthy environments that enable residents to make healthy choices about diet, exercise and other habits including the replication or expansion of the Healthy Eating-Active Communities Program (Clara Steimberg).
9. Contribute to enhance the performance of DPH through innovation and change, and cost-effective and quality partnerships and programs leading to the improvement of the health status and wellbeing of LA County residents (All).
10. Recognize that protecting and improving the health of a population is a shared responsibility among all sectors of society (All).
APPENDIX 2
16

DEVELOPING A COMMUNITY LIAISING PROGRAM IN LOS ANGELES July 2009
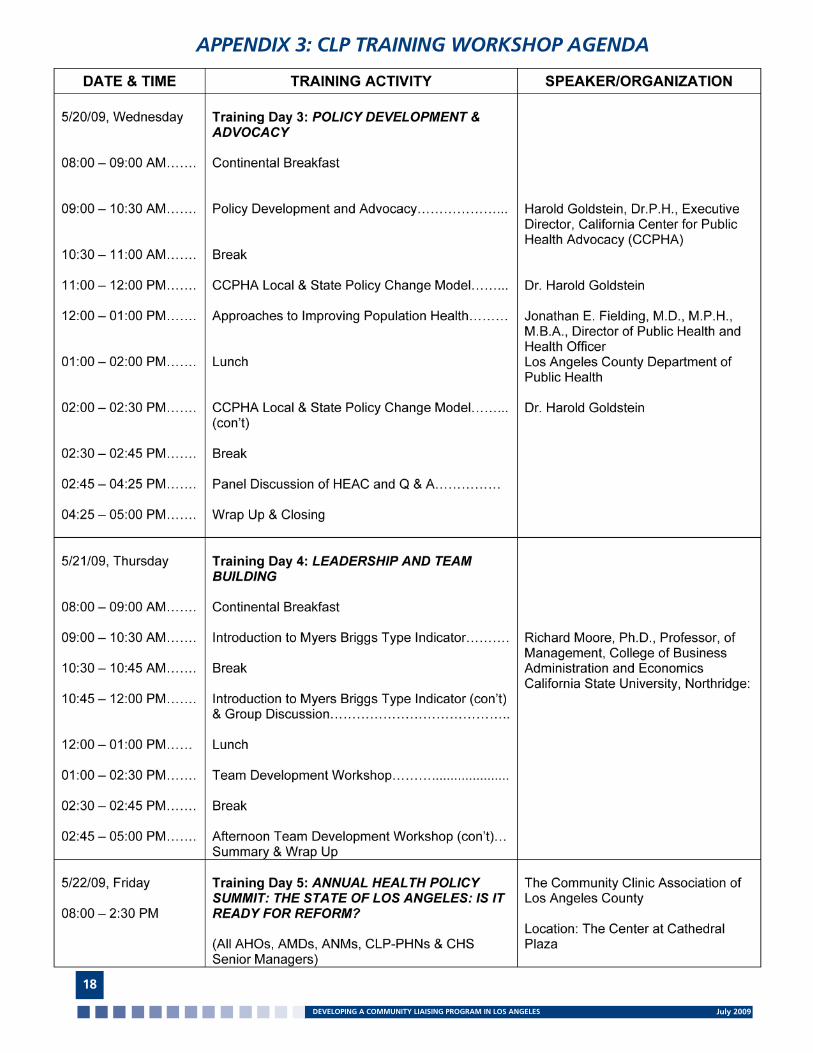
APPENDIX 3: CLP TRAINING WORKSHOP AGENDA
17
July 2009DEVELOPING A COMMUNITY LIAISING PROGRAM IN LOS ANGELES
APPENDIX 3: CLP TRAINING WORKSHOP AGENDA
18
DEVELOPING A COMMUNITY LIAISING PROGRAM IN LOS ANGELES July 2009
APPENDIX 4: COMMUNITY LIAISING PROGRAM FRAMEWORK
19

July 2009DEVELOPING A COMMUNITY LIAISING PROGRAM IN LOS ANGELES
San Gabriel Valley Service Planning Area (SPA 3)Metropolitan Service Planning Area (SPA 4)241 North Figueroa Street, Room 312Los Angeles, California 90012Tel: (213) 240-8049Fax: (213) 202-6096
www.publichealth.lacounty.gov© 2009 SPA 3 & 4