Embed Size (px)
Citation preview

Developed by:
Phillip Graham
Captain/Paramedic
Red, White and Blue Fire Protection District
1

Objectives
Describe the incidence of illicit drug abuse
emergencies.
Define the terms substance/drug abuse, drug
dependence/addiction, tolerance, and
withdrawal.
Discuss the role of poison control centers.
Discuss the routes of entry of toxic substances
into the body.
2

Objectives Continued
List the commonly abused street drugs and
toxic substances.
Describe signs and symptoms of street
drug and toxic substances used.
Describe withdrawal effects of typical street
drugs.
Describe treatment options for patients
who are under the influence of street drugs
and toxic substances.
3

Objectives Continued
Describe transport issues regarding the
patient who has overdosed.
Review the reconstitution of glucagon.
Review the use of the MAD device.
Review ventilatory rates using the BVM.
4

Incidence of Illicit Drug Emergencies
There is a high potential for EMS
involvement in illicit drug emergencies
National Institute on Drug Abuse keeps data
14.5 million people use illicit drugs regularly
20 million people have tried cocaine
○ 860,000 people use cocaine weekly
11.6 million people use marijuana regularly
770,000 people use hallucinogens (ie: LSD,
PCP) regularly
2.5 million people have used heroin
5

Illicit Drug Behavior
Substance abusers are 18 times more likely to be involved in criminal activity
Violent crimes and thefts to support drug habits
Drug overdoses
Accidental
Miscalculation of dosing
Changes in strength of drug
Suicide attempt
Polydrug use
Recreational drug use
6

Definition of Terms
Substance/drug abuse Use of pharmacological substances for purposes other than a
medically defined reason
Drug dependence/addiction A craving for the drug, an overwhelming feeling of the need to obtain
and continue to use the drug
Tolerance The need for increasingly higher amounts of the drug to get the same
effects
Withdrawal A psychological or physical reaction when the substance is stopped Most signs and symptoms of withdrawal are the exact opposite of
what exposure to the substance causes
7

Poison Control Centers
Set up to assist in treatment of poison victims
Provides information on new products and
new treatment approaches
Staffed with trained experts 24/7
Information updated regularly
Consultation can assist in determining
potential toxicity to the patient
Can provide definitive treatment information
that should be started
8

Poison Control Center
240per day/7 days per week
9

Routes of Exposure
Ingestion
Can cause immediate or delayed effects
Inhalation
Rapid absorption via alveoli in the lungs
Topical
Entry across the skin or mucous membranes
Injection
Can cause immediate and delayed effects
10
Commonly Abused Depressant Drugs
Alcohol
CNS depressant
Binge drinking equals BAC > 0.08 (80)
○ Men – typically 5+ drinks in 2 hours
○ Women – typically 4+ drinks in 2 hours
Alcohol poisoning
○ Affects the respiratory center in the brain
○ Vomiting leads to aspiration & asphyxiation
Sobering up
○ Need time
○ Caffeine does not help – really!
11

Alcohol Continued
< 0.08 (80) - legal limit in Colorado
0.30 (300) – stupor, passed out, difficult to
awaken
0.35 (350) – typical for coma
0.40 (400) – coma, possibly death due to
respiratory arrest
12

Alcohol Continued
BAC continues to rise even after passing out
Alcohol in the stomach and intestines continues to
enter the blood stream
A fatal dose can be ingested before becoming
unconscious
General signs/symptoms
○ Mental confusion
○ Vomiting
○ Seizures – often related to hypoglycemia
○ Slow/irregular breathing
○ Hypothermia
13

Commonly Abused Depressant Drugs
Narcotics/opiates
CNS depression
○ Heroin
○ Hydromorphine
○ Darvon, Darvocet
Heroin – most abused of the narcotics
○ Physical and psychological dependence
○ Addiction and physical tolerance
○ Mood swings, severe constipation
○ Menstrual irregularities
○ Lung damage, skin infections
○ Seizures, unconsciousness, coma
14

Narcotics
Typical signs and symptoms
Pinpoint pupils
No physical pain; rush of pleasurable feelings
Lethargic, drowsy, slurred speech
Shallow breathing
Sweating, vomiting
Hypothermia
Sleepiness
Loss of appetite
15
16
Heroin: Background
Heroin comes from opium poppy capsules.
Heroin is usually injected, but it can be sniffed,
snorted or smoked.
Typical heroin user injects up to 4 times a day.
Intravenous injection provides greatest intensity
and rapid onset (7-8 seconds).
IM injection produces a slower response (5-8
minutes).

17
Heroin: Background
White powdery substance
Heroin enters the brain, where it is converted to
morphine
Due to needle use, heroin users are at risk for:
HIV
Hepatitis-C
Other bloodborne pathogens
NEW TREND: mixing heroin & fentanyl
Increases number of deaths from respiratory
depression

18
Heroin

19
Treatment of Heroin
Scene Safety
Due to the increased risk for Bloodborne Pathogens,
BSI is extremely important
Be cautious of any needles that may be hidden from
view. This is NOT the patient you want an accidental
stick from!
○ This population has a high incidence of HCV and HIV
ABC’s
IV, O2, & monitor

20
Treatment of Heroin
Watch for pulmonary edema
In some heroin overdoses this can occur
Respiratory support early!
Ventilate at a rate of 10 breaths per minute
○ 1 breath every 6 seconds

21
Treatment of Heroin
Narcan quickly reverses the effects of heroin on
the CNS (usually within 5 minutes)
Generally, these patients are not pleased to have
their “high” wiped out by our Narcan
May cause withdrawal symptoms including seizures
If large doses of heroin were used, there could be
a relapse when the Narcan wears off
Narcan may be shorter acting based on dose of
heroin taken

22
Heroin…
http://youtu.be/Hj6NvwDLjAE
http://youtu.be/6mSq69FT3jM

23
Cocaine: Background
A central nervous system stimulant
Two forms
Powder that can be snorted or dissolved in
water and injected
Crack that comes in a rock crystal form that can
be heated and the vapors smoked
○ Effects occur more rapidly than cocaine
○ Effects more intense than cocaine
○ Effects do not last as long as cocaine

24
Cocaine: Background
Cocaine is the most potent stimulant of natural
origin
One of the oldest identified drugs
Coca leaves (source of cocaine) have been
ingested for thousands of years
Is not used medically today due to high potential
for abuse and addiction
25
Cocaine

26
Crack Cocaine

27
Cocaine: Pathophysiology
Cocaine related dysrhythmic fatalities occur in patients with low or moderate levels of cocaine use
Tachydysrhythmias most common
Hearts of cocaine users are 10% heavier than non-cocaine users
Increase QRS voltage indicative of ventricular enlargement
Conduction delays resulting in widening of the QRS and prolonged QT segment

28
Cocaine: Myocardial Effect
Regular use of cocaine increases risk of AMI
Increased heart rate and B/P results in increased
myocardial O2 demand
Accelerates coronary atherosclerosis process
May also induce coronary artery spasms
During withdrawal, may have increased incidence
of ST elevation indicating acute MI

29
Cocaine: Signs & Symptoms
Dilated pupils
Hyperactivity
Euphoria
Irritability
Anxiety
Excessive talking
Depression or excessive sleeping
Long periods without eating or sleeping
Weight loss
Paranoia
Dry mouth/nose
Tachycardia
Hypertension
Disturbance of heart rhythm
Chest pain
Heart failure
Respiratory failure
Strokes/seizures

30
Cocaine: Agitated/ Excited Delirium
Common in patients dying from cocaine toxicity
Bizarre and violent behavior
Aggression/combativeness
Hyperactivity/unexpected strength
Hyperthermia
Extreme paranoia
Followed by cardiac arrest!

31
Cocaine: Restraints
Restraints have been implicated as a contributing
factor for user deaths during prone restraint
Sudden death appears to have been induced by a
combination of three factors that increases oxygen
demand and decreases oxygen delivery
See next slide

32
The three factors:
1. Cocaine induced state of agitated delirium coupled with police confrontation places stress on the heart
2. Hyperactivity associated with the delirium coupled with the struggling against restraints/police increases oxygen demands
3. The prone position on the cot impairs breathing by inhibiting chest wall and diaphragmatic movement and inhalation of fresh oxygen vs exhaled carbon dioxide

33
Cocaine: Treatment
Make certain the scene is safe
Not only is there potential for your patient to
become violent, but for bystanders that may be
users as well
Establish ABC’s
Oxygen
EKG (12-lead) and monitor continuously
IV of Normal Saline at TKO unless need for
volume is indicated

34
Cocaine: Treatment
Frequent vital signs with temperature levels
Monitor temperature often; may continue to rise
Obtain glucose level
Use Narcan carefully in patients with altered
mental status
If safe to do so, avoid restraints as this could
cause risks associated with hyperthermia

35
Cocaine: Cardiac Arrest Concerns
Epinephrine
Hyper-adrenergic state caused by cocaine
increases myocardial oxygen demand.
○ Epinephrine has the same effect
Cocaine frequently causes acidosis
○ Epinephrine loses much effectiveness in an acidotic
environment
Benzodiazepines
Benzodiazepines (ie: Valium®, Versed®) are used
to control seizure activity

Benzodiazepines
Tranquilizers
Valium®
Librium®
Xanax®
Halcion®
Ativan®
Diazepam (Valium®) may be fatal when mixed with alcohol, opiates, and other depressants
Nearly impossible to take a fatal dose of Valium® when not mixed with any other product, especially alcohol
36

Amphetamines
Stimulant
Benzedrine
Dexedrine
Ritalin
Used by prescription to treat attention deficit
hyperactivity disorder (ADHD)
Ephedrine and pseudoephedrine a component in
cold preparation medications
Used as decongestant
Used for illicit manufacture of methamphetamine
37

Methamphetamine
To control production of methamphetamine from
over-the-counter products, controls in place
Sales of products restricted
○ Limited quantities purchased for every 30 days
○ Must be of a minimum age
○ Must show proper identification
Above controls have contributed to decrease in
meth labs
38

Crystal meth: Background
Dates back to WW II to reduce fatigue and
suppress appetite
Crystal Meth is typically smoked like crack
cocaine
Can also be ingested orally or injected
Easy to make in small clandestine laboratories
Prior to 1990’s was made using ephedrine
Pseudoephedrine became new ingredient
39

40
From a print ad from the Partnership for a Drug Free America

Crystal Meth
41

Crystal Meth: Pathophysiology
Causes vasoconstriction as well as
bronchodilation
May last up to 4 and 6 hours after a small
ingested dose
Effect on the brain is due to norepinephrine
and dopamine
High doses of amphetamine can cause
palpitations and chest pain with a risk of
myocardial infarction
42

Crystal Meth: Signs & Symptoms
Dilated pupils
Dry mouth
Euphoria
Decreased appetite
Rapid speech
Irritability/Argument
Depression
Nasal congestion
Insomnia
Weight loss
Increased HR, BP &
Temperature
Restlessness
No interest in food
or sleep.
Violent
Paranoia
43

Crystal Meth: Treatment
Scene safety
Extra caution needed if there is suspected meth lab
on scene
○ Highly explosive potential for years due to chemicals
used and residue left behind in the environment
Meth lab requires Haz-Mat response
ABC’s
IV, O2, & EKG
Important to monitor EKG continuously due to
potential cardiac issues
44

Meth Lab Recognition
UNUSUAL ODORS – Making meth produces powerful odors that may smell like ammonia or ether. These odors have been compared to the smell of cat urine or rotten eggs
COVERED WINDOWS – Meth makers often blacken or cover windows to prevent outsiders from seeing in
STRANGE VENTILATION – Meth makers often employ unusual ventilation practices to rid themselves of toxic fumes produced by the meth-making process. They may open windows on cold days or at other seemingly inappropriate times, and they may set up fans, furnace blowers, and other unusual ventilation systems.
45

Meth Lab Recognition
ELABORATE SECURITY – Meth makers often set up elaborate security measures, including, for example, "Keep Out" signs, guard dogs, video cameras, or baby monitors placed outside to warn of persons approaching the premises.
DEAD VEGETATION – Meth makers sometimes dump toxic substances in their yards, leaving burn pits, "dead spots" in the grass or vegetation, or other evidence of chemical dumping.
46

Meth Lab Recognition
EXCESSIVE OR UNUSUAL TRASH – Meth makers produce large quantities of unusual waste that may contain, for example:
packaging from cold tablets
lithium batteries that have been torn apart
used coffee filters with colored stains or powdery residue
empty containers – often with puncture holes – of antifreeze, white gas, ether, starting fluids, Freon, lye, drain opener, paint thinner, acetone, alcohol, or other chemicals
plastic soda bottles with holes near the top, often with tubes coming out of the holes
plastic or rubber hoses, duct tape, rubber gloves, or respiratory masks.
47

Meth Labs – A Dangerous Place
Typical products used
Explosive environments
48

Club/Rave/Party Drugs
Very popular in university’s, nightclubs, and party
environments
Ecstasy – MDMA
○ Modified form of methamphetamines
Rohypnol – Date rape drug, roofies
○ Strong benzodiazepine
Often used for sexual purposes
To stimulate and enhance the sexual experience
To sedate and cause amnesia to facilitate raping the
victim
49

Ecstasy/MDMA: Background
Research in animals has shown damage to
specific neurons in the brain
Has stimulant and hallucinogenic properties
Reduces inhibitions, eliminates anxiety and
produces feeling of empathy for others
Enables users to endure all night and
sometimes 2-3 day parties
Suppresses need to eat, drink, or sleep
Effects begin in 30 minutes; last 4 – 6 hours
50

Ecstasy: Background
Is taken orally – pill form with multiple logos
May cause psychological addiction
Polydrug use often involved
Mix of a variety of chemicals simultaneously
taken
Product only manufactured illegally
Can be questionable regarding composition
There are no specific treatments for MDMA
abuse and addiction
In high doses can cause severe hyperthermia
51

Ecstasy
52
Ecstasy: Signs & Symptoms
Dilated pupils
Intense euphoria
Peacefulness
Empathy/sympathy/acceptances
Increased B/P, heart rate
Sweating
Constant motion, excessive talking
Teeth clenching (use pacifiers or cigarettes)
Muscle spasms
53
Ecstasy: Treatment
Normal scene safety precautions
ABC’s
IV, O2, and EKG monitor
Monitor temperature
54
Rohypnol®
Benzodiazepine smuggled into the USA
Best known as “date rape” drug
Placed into alcoholic drink of unsuspecting victim
Removes inhibitions, causes blackouts and memory
loss when mixed with alcohol
Victim incapacitated; has soothing effect
Amnesic to the events
Long-lasting
○ 10 times more powerful than Valium®
55
Synthesized Marijuana
An incense spice sold in Illinois
Labeled “not for human consumption”
But is regularly smoked
Produces a marijuana type high at low doses
Can’t guarantee dosage in the different brands
Popular to use because not traceable in drug
tests
Can increase heart rate, B/P, seizure activity,
hallucinations, and paranoia
56

Treatment of Patients Under the Influence
No specific SOP for “under the influence”
Need to refer to SOP based on assessment and
general impression of patient
SOP’s to consider
Routine Medical or Trauma Care
Altered Mental Status
Tachycardia
Psychological Emergency
Sexual Assault
Seizures
57

Supplemental Oxygen
Delivered to patients when:
Hypoxemia is evident with oxygen saturation <90%
Signs of respiratory distress are evident
Capnography is most accurate method to measure
exhaled carbon dioxide (CO2) levels
Evaluates effectiveness of ventilations
Evaluates effectiveness of CPR
Can determine return of spontaneous circulation
(ROSC) during CPR
58

Transportation of Patients Under the
Influence
Scene Safety – Scene Safety – Scene Safety
Attempt verbal de-escalation Patients fighting mechanical restraints could increase
the adrenalin rush
If patient restrained, document reason why and distal circulation status of the extremities
Monitor airway closely Be prepared for aspiration precautions
○ Suction ready
○ Repositioning of patient
Be prepared to ventilate the patient with depressed respirations
Consider use of Narcan if narcotics suspected
59

Review Equipment
Do you know how to reconstitute Glucagon?
Have you delivered medication via the MAD
device yet?
Do you know the ventilation rate if you have to
support a patient’s ventilations?
60

Glucagon Reconstitution
Glucagon must be reconstituted prior to
administration
Supplied in vials
1 unit of powder generally in compressed form
1 ml of diluting solution
61

Glucagon Administration
Draw up the diluent and add to vial with
powder
Cleanse off vial tops with alcohol wipe
Once the diluent has been added to the
powder, gently roll the vial to mix the contents
Check that all particles have been dissolved
prior to drawing up the medication
Inject glucagon as an IM
Always, always, always aspirate prior to
injecting medications
62

Medication Delivery via MAD
Mucosal atomization device
Tool to deliver medications via nasal route
Medication atomized into tiny particles
Nasal mucosa highly vascular
○ Immediate absorption into bloodstream
○ Maximum volume per nare is 1 ml
○ Use equal divided doses per nares
63

Preparing the Syringe
Variety of ways to prepare the syringe with the
MAD tip
Goal is to deliver a maximum of 1 ml of volume
per nare
Acceptable to use one syringe and deliver half
the dose into one nare, then place the same
MAD tip into the 2nd nare and deliver the
remaining dose from the one syringe
Can prepare 2 equal, separate syringes
64

Attach MAD Tip to Syringe
Suction nasal cavity as needed to clear blood or secretions Clear nasal passages enhance absorption of
medication
Deliver medication in divided doses Maximum of 1 ml per nare
65
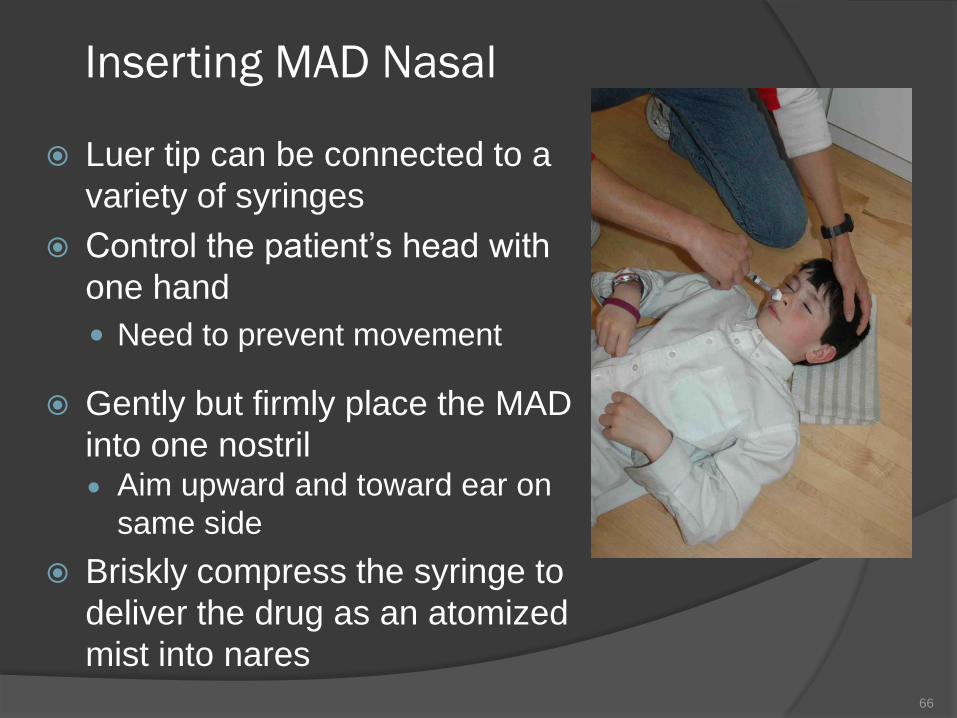
Inserting MAD Nasal
Luer tip can be connected to a
variety of syringes
Control the patient’s head with
one hand
Need to prevent movement
Gently but firmly place the MAD
into one nostril Aim upward and toward ear on
same side
Briskly compress the syringe to
deliver the drug as an atomized
mist into nares
66

Dispensing Mist
Must briskly compress
syringe to convert liquid
drug to a fine atomized
mist
Mist results in broader
mucosal coverage; better
chance of absorption into
the blood stream than
drops that can run straight
back into the throat.
67

Ventilatory Support via BVM
Determine need for ventilatory support
Hypoventilation
Apnea
Shallow respirations
Dropping SpO2 levels
Hypercapnia
○ Excessive levels of carbon dioxide (CO2) from
hypoventilation
○ Best monitored by capnography waveform if available
68

Ventilatory Support
Patient has a pulse, needs ventilatory support
Drug overdose
Stroke
Head injury affecting respiratory center
○ Adult 10 breaths per minute – 1 every 6 seconds
○ Child 20 breaths per minute – 1 every 3 seconds
○ Infant <1 y/o 25 breaths per minute – 1 every 2.5
seconds
69

Hazards of Hyperventilation
Hyperventilation causes excessive exhalation
of carbon dioxide (CO2) creating secondary
injuries
Hypocarbia- low levels of CO2
○ Stimulates vasoconstriction which decreases
blood flow
○ Brain especially sensitive to decreased blood flow
○ Decreased levels of oxygen and glucose
70

Lessons Learned in General
It’s amazing what people will put into their bodies!
Patients under the influence have the potential to
become violent
Be diligent to avoid accidental needle sticks to
yourself in this population
Carefully monitor respiratory status and be
prepared to ventilate this patient
Enough Narcan has been administered when the
patient can resume breathing effectively on their
own
71

Questions??
72