Embed Size (px)
Citation preview
1
Determine When Skin Testing, Test Doses and Desensitization
are Appropriate
David A. Khan, MD Professor of Medicine
Allergy & Immunology Program Director Division of Allergy & Immunology
Disclosures
Research Grants NIH, Vanberg Family Fund
Speaker Honoraria Merck, Genentech, Viropharma, Baxter
Organizations: Joint Task Force on Practice Parameters
Objectives
Be able to identify patients appropriate for drug skin testing
Be able to identify patients appropriate for drug challenges
Be able to identify patients appropriate for drug desensitization
Case 1
The Role of Drug Skin Testing
Drug Skin Testing
Penicillin is only drug with well-validated outcomes
Skin testing with platinum-based chemotherapeutics of value
Skin testing for drug-induced anaphylaxis may be helpful
Skin testing for most other drugs and other reaction types of unclear benefit
5
Penicillin Skin Testing
Penicillin skin testing using PRE-PEN and PCN-G has good negative predictive value (96-99%) in excluding penicillin allergy
Some of these studies may have excluded penicillin anaphylaxis
Macy E et al. JACI In Practice 2013;1:258-63. Solensky R, Khan DA et al. Ann Allergy Asthma Immunol 2010;105:273e1-e78. delReal GA, et al. Ann Allergy Asthma Immunol 2007;98:355-9. Green GR, et al. J Allergy Clin Immunol1977;60:339-45. Brown BC, et al. JAMA1964;189:599-604.
PRE-PEN & PCN-G 500 patients with history of PCN allergy
Rash (40%), hives/AE (34%), unknown (14%), other (8%), anaphylaxis (2.8%)
Mean time since reaction 20 years
496 negative skin tests underwent amoxicillin challenge 15/496 had subjective symptoms (e.g.
itching) with amoxicillin challenge 4/496 had urticaria within 1 hr with
amoxicillin challenge
NPV=96-99.1% Macy E et al. JACI In Practice 2013;1:258-63.
Drug-Induced Anaphylaxis Case
40 year old woman with history of recurrent urinary tract infection developed confusion, nausea, dyspnea, chest pain, sensation of throat closure, facial swelling, generalized erythema, pruritus, and collapse within 20 minutes after the first dose of co-trimoxazole and an energy drink.
Treated with epinephrine 0.3mg IM x 2 at pediatric ED and transferred to a nearby adult emergency department where BP was 87/46 mmHg
Resolution of hypotension after 3rd dose of epinephrine and IV fluids
Drug-Induced Anaphylaxis Case
Patient remains unconvinced that sulfonamide antibiotic was the cause of her anaphylaxis
Skin testing to TMP/SMX performed using a nonirritating dose
Skin testing for Antibiotics
There are no validated diagnostic tests for evaluation of IgE-mediated allergy to non-penicillin antibiotics
Skin testing with non-irritating concentrations of non-penicillin antibiotics established for 15 commonly used antibiotics
A negative skin test result does not rule out the possibility of an immediate-type allergy
Positive skin test results to a drug concentration known to be nonirritating suggests the presence of drug-specific IgE
Empedrad R et al. J Allergy Clin Immunology 2003;112:629.
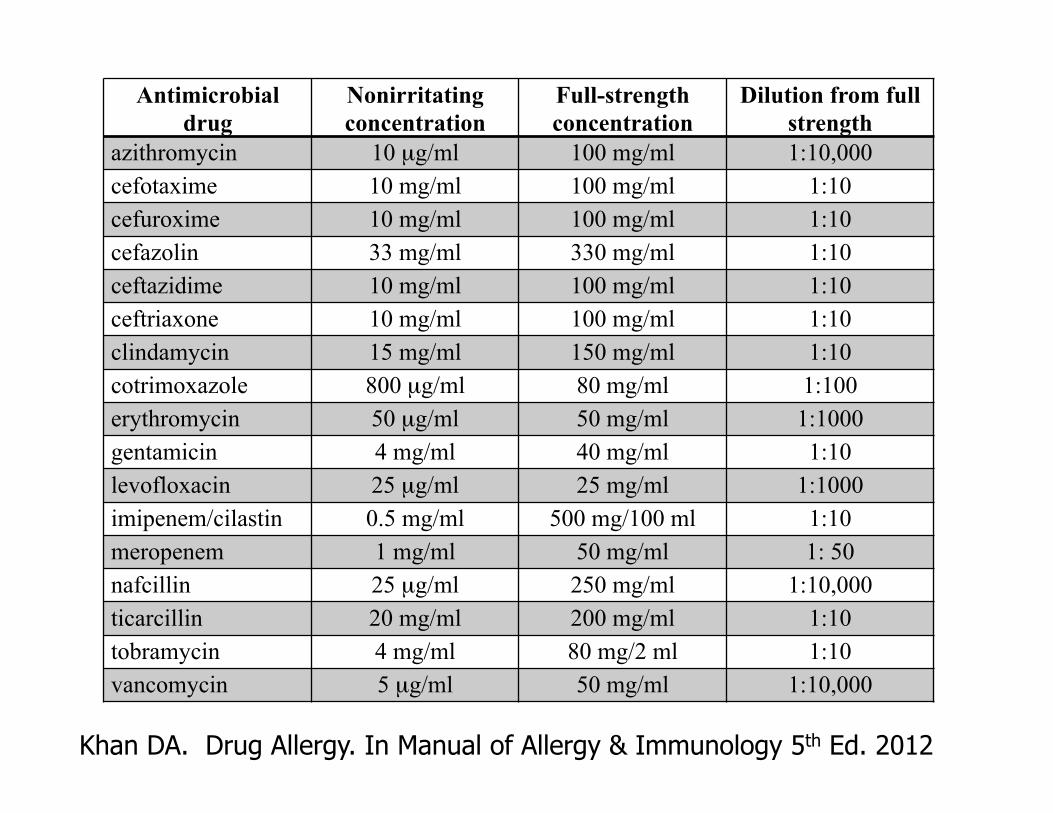
Antimicrobial drug
Nonirritating concentration
Full-strength concentration
Dilution from full strength
azithromycin 10 µg/ml 100 mg/ml 1:10,000 cefotaxime 10 mg/ml 100 mg/ml 1:10 cefuroxime 10 mg/ml 100 mg/ml 1:10 cefazolin 33 mg/ml 330 mg/ml 1:10 ceftazidime 10 mg/ml 100 mg/ml 1:10 ceftriaxone 10 mg/ml 100 mg/ml 1:10 clindamycin 15 mg/ml 150 mg/ml 1:10 cotrimoxazole 800 µg/ml 80 mg/ml 1:100 erythromycin 50 µg/ml 50 mg/ml 1:1000 gentamicin 4 mg/ml 40 mg/ml 1:10 levofloxacin 25 µg/ml 25 mg/ml 1:1000 imipenem/cilastin 0.5 mg/ml 500 mg/100 ml 1:10 meropenem 1 mg/ml 50 mg/ml 1: 50 nafcillin 25 µg/ml 250 mg/ml 1:10,000 ticarcillin 20 mg/ml 200 mg/ml 1:10 tobramycin 4 mg/ml 80 mg/2 ml 1:10 vancomycin 5 µg/ml 50 mg/ml 1:10,000
Khan DA. Drug Allergy. In Manual of Allergy & Immunology 5th Ed. 2012
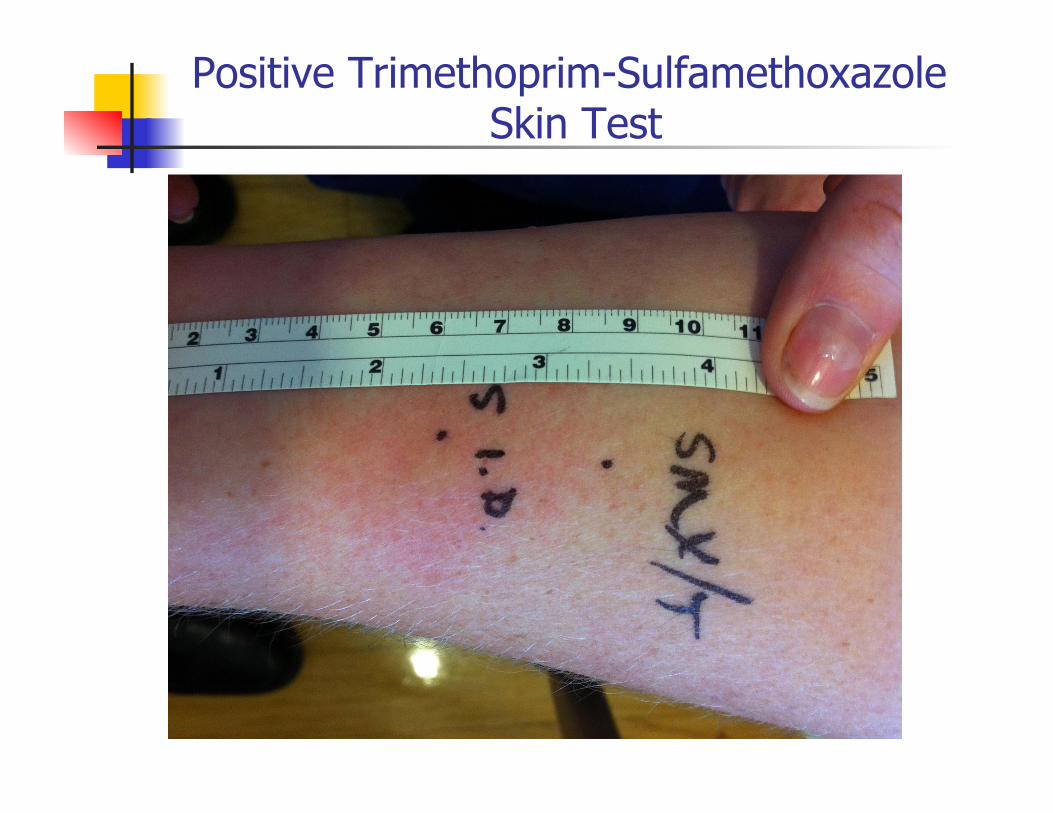
Positive Trimethoprim-Sulfamethoxazole Skin Test
Case 2
The Role of Drug Challenge
Terminology
Drug Challenge Test dosing Drug provocation test Graded dose challenge Incremental challenge
Definition of Drug Challenge
The intention of a drug challenge is to verify that a patient will not experience an adverse reaction to a given drug
Intended for patients who are unlikely to be allergic to the given drug
Graded challenge or test dosing describes administration of progressively increasing doses of a medication until a full dose is reached
Some test doses may be full therapeutic doses
Solensky R, Khan DA et al. Ann Allergy Asthma Immunol 2010;105:273e1-e78.
Multiple Drug Allergy Case 38 yo woman with multiple drug-induced
anaphylaxis Listed Drug Allergies
RhoGAM Ciprofloxacin Ceftriaxone Amoxicillin
Also reports episodes of crawling skin, nasal congestion, few non-pruritic skin lesions, throat tightness Treated with prednisone (up to 400 mg/d) for months at
a time
Symptoms with Drug Reactions
RhoGAM After 15 minutes, urticaria, throat tightness, BP
90/50 mm Hg, dyspnea, sense of impending doom
Subsequent drug reactions: Usually within minutes of 1st dose Itching, tingling lips, throat tightness,
dysphonia, cough
Other triggers Certain toothpastes, perfumes
Multiple Drug Allergy Case
Skin testing with non-irritating concentration of ceftriaxone negative
Penicillin skin tests negative What would you recommend now?
A. Continued avoidance of all listed drugs due to anaphylactic history
B. Drug desensitization if listed antibiotic required
C. Graded challenge D. Full therapeutic dose challenge
Drug “Anaphylaxis” Case Due to doubtful reaction history patient given full
therapeutic dose of ciprofloxacin 12 minutes later had itching of palms, lip
numbness, and mild throat tightness BP 133/83, P 132
Over next 5 minutes symptoms more severe, with worsening throat tightness BP 142/96, P 142
Laryngoscopy performed and revealed VCD with arytenoids completely adducting with inspiration
Symptoms resolved with reassurance and relaxation
Drug-Induced Vocal Cord Dysfunction (VCD)
Often mistaken for anaphylaxis Primary and most severe symptom is
isolated throat tightness Often have histories of multiple drug “anaphylaxis” from structurally-unrelated drugs
Lack objective angioedema elsewhere
Khan DA. Ann Allergy Asthma Immunol 110 (2013) 2-6.
Role of Drug Challenges
Drug challenges are an important tool in diagnosis and management of drug allergic patients
With careful assessment of patients and appropriately designed protocols, drug challenges can be safely performed in your office
Patients with > 10 listed allergies and subjective symptoms at higher risk for subjective symptoms with drug challenge
Kao L et al. Ann Allergy Asthma Immunol 110 (2013) 86e91.
Benefit of Drug Challenges
The real benefit of drug challenges is that it answers the question (Is the patient allergic to the drug?)
Avoids unnecessary repeated “empiric desensitizations”
Great service the practicing allergist can provide to patients and referring physicians
New Code for Oral Challenge
95076 Ingestion Challenge Higher RVUs Minimum of 61 minutes required Likely requires a graded challenge
Stay tuned on this No E&M should be billed in conjunction
with this code
Case 3
Drug Desensitization
Case of Macrolide Allergy
A 68-year-old woman developed urticaria and shortness of breath six days into a course of clarithromycin for Mycobacterium avium intracellulare infection
Her pulmonologist advised her to take a “test” dose of azithromycin 250 mg. Within an hour she developed urticaria, shortness of breath, and throat tightness resulting in an emergency department visit.
Swamy N et al. Ann Allergy Asthma Immunol 2010;105:489-90.
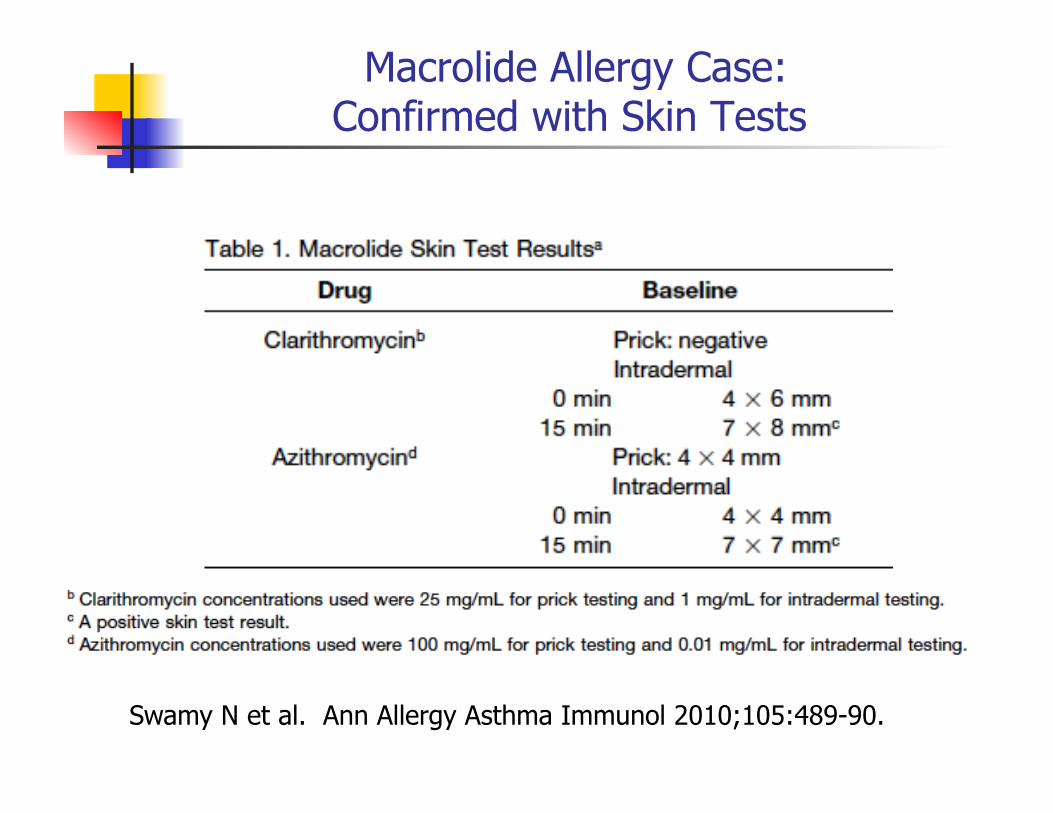
Macrolide Allergy Case: Confirmed with Skin Tests
Swamy N et al. Ann Allergy Asthma Immunol 2010;105:489-90.
Role of Drug Desensitization
Penicillin and chemotherapy desensitization protocols have been studied the most
Similar desensitization principles can be used for other drugs
Most drug desensitizations associated with ~ 1/3 risk of reactions during desensitizations severe anaphylactic reactions are rare
Choice of location depends on treatment facilities, experience, drug, and patient factors
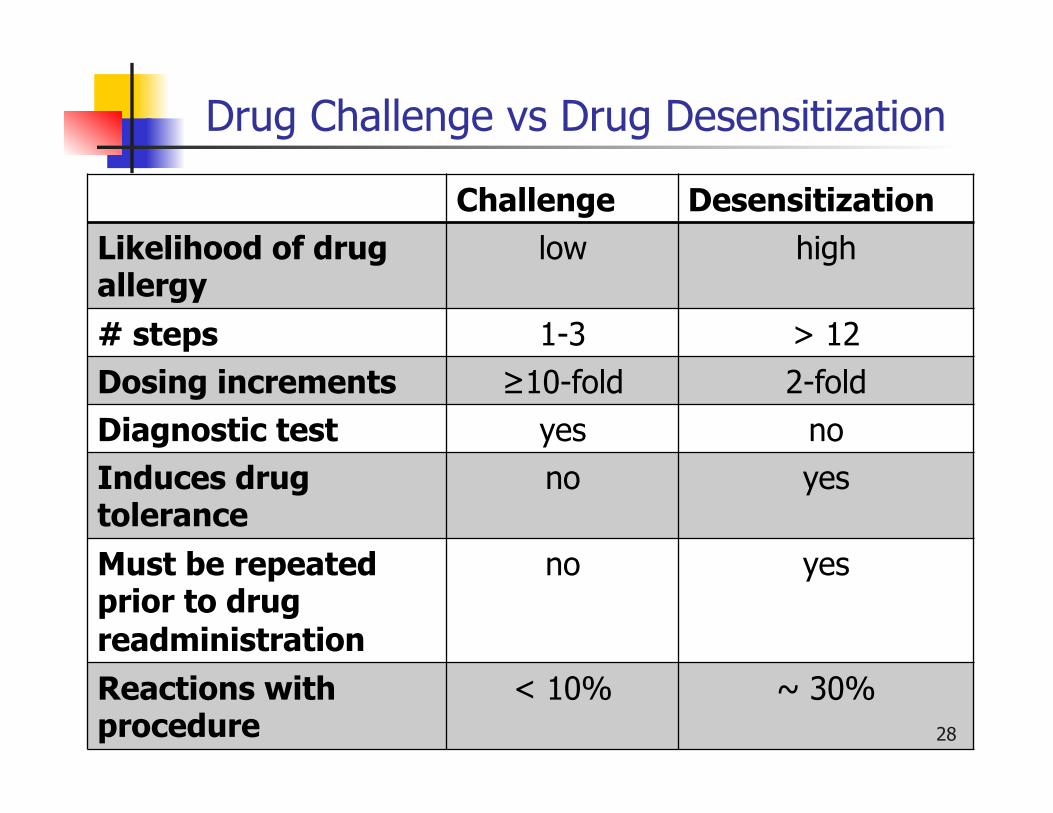
Drug Challenge vs Drug Desensitization
Challenge Desensitization Likelihood of drug allergy
low high
# steps 1-3 > 12 Dosing increments ≥10-fold 2-fold Diagnostic test yes no Induces drug tolerance
no yes
Must be repeated prior to drug readministration
no yes
Reactions with procedure
< 10% ~ 30% 28
Drug Desensitizations
Indicated for patients with: High likelihood or confirmed drug
allergy e.g. + skin test
In need of culprit drug where no therapeutic alternative exists
Basic Template of Drug Desensitization Protocols
Typical starting dose is 1/10,000th of target therapeutic dose
Can also use calculated dose from skin test as starting point
Further dosage increases are typically double the previous dose
Administered at 15-20 minute intervals until therapeutic dosage achieved
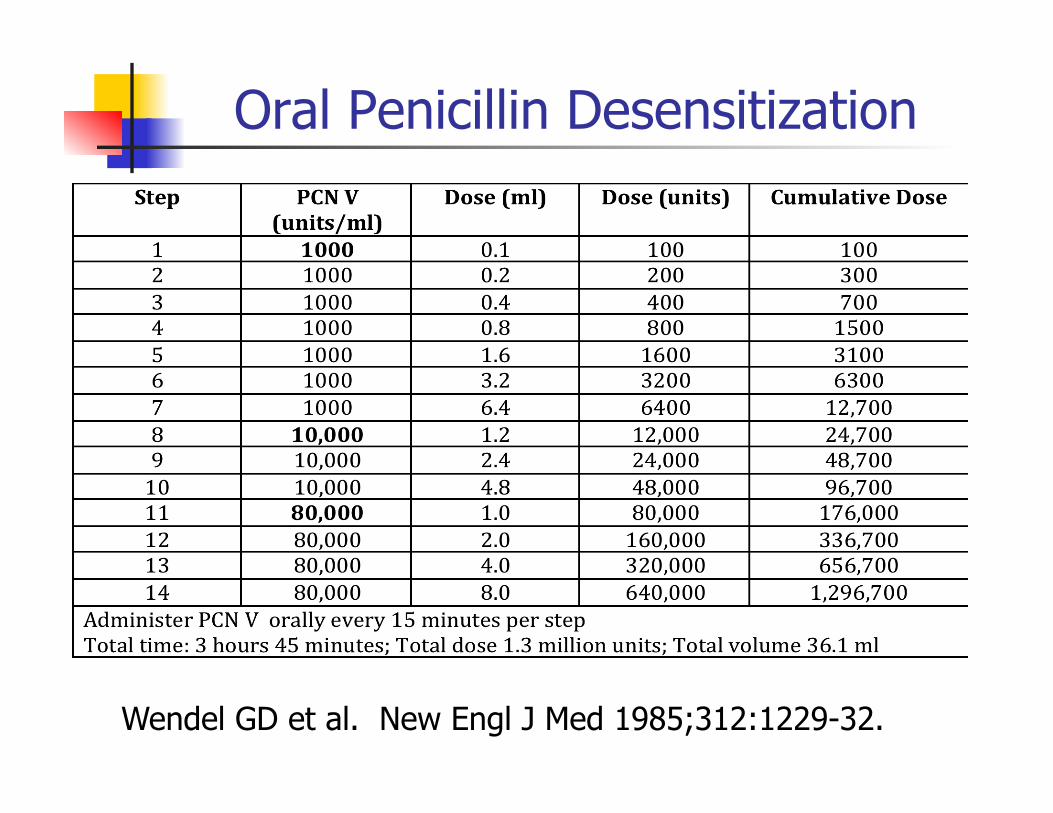
Oral Penicillin Desensitization
Wendel GD et al. New Engl J Med 1985;312:1229-32.
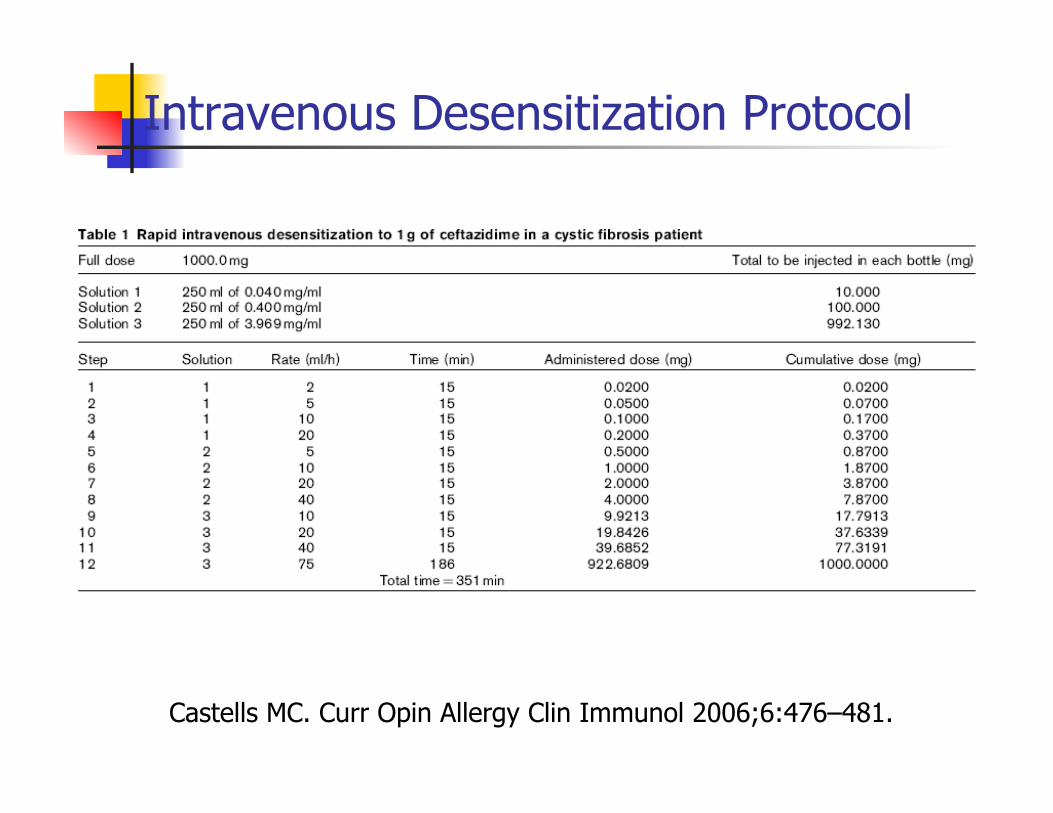
Castells MC. Curr Opin Allergy Clin Immunol 2006;6:476–481.
Intravenous Desensitization Protocol
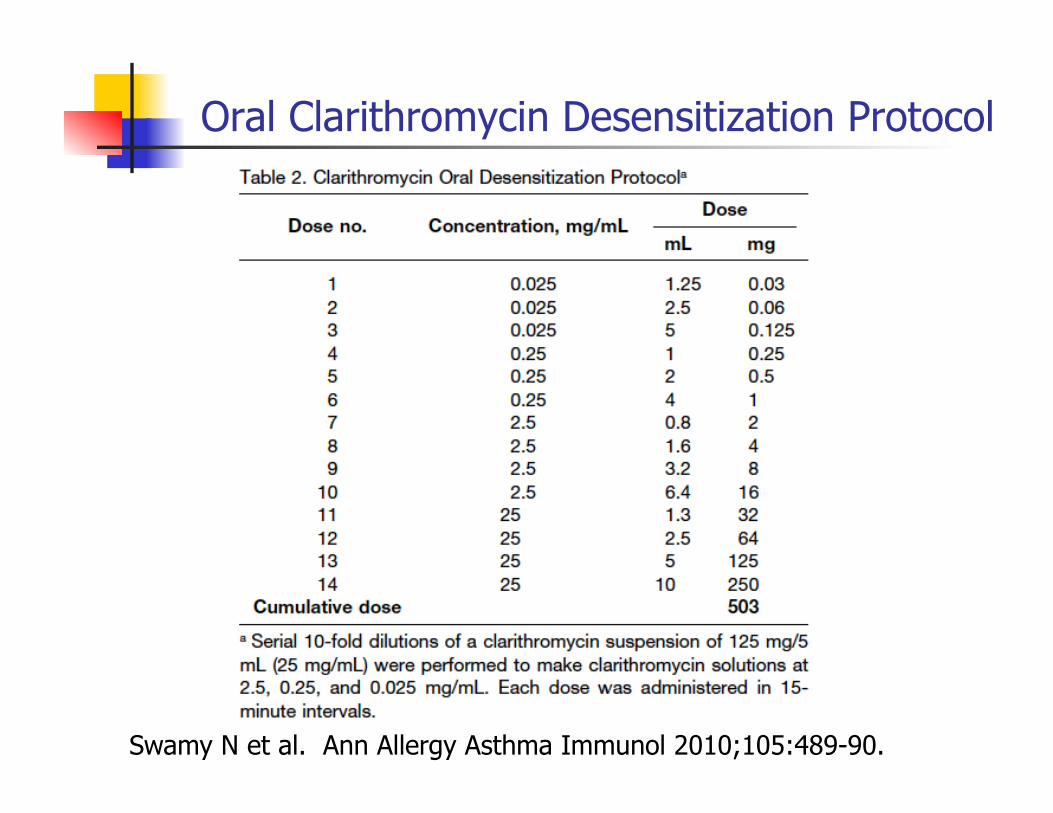
Oral Clarithromycin Desensitization Protocol
Swamy N et al. Ann Allergy Asthma Immunol 2010;105:489-90.
Back to the Case
Clarithromycin desensitization performed in the office
No adverse reactions developed during the desensitization
After the desensitization she began routine administration of clarithromycin 500 mg twice a day and received this dose over the following three months
She tolerated the treatment course without any adverse effects, and had resolution of her respiratory symptoms
Conclusions
Other than penicillin skin testing, drug skin testing has a limited utility when negative, but when positive can be helpful
Drug challenges are an underutilized tool and with careful selection of patients, can be done safely in the office
Drug desensitizations are effective when used appropriately but are often over utilized instead of performing a drug challenge



















![Review Article Supplements and Foods with Potential ... · Garlic mg doses of mg x weeks Sphyg SBP ± versus ± DBP ± versus ± Mizushima et al. [] M/ Hypertensives ± years Milk](https://img.pdfslide.us/doc/110x75/612d802f1ecc515869423a8e/review-article-supplements-and-foods-with-potential-garlic-mg-doses-of-mg-x.jpg)









