Embed Size (px)
Citation preview

Determination of left ventricular ejection fraction by visual estimation during real-time two-dimensional echocardiography
It has been shown that the measured reduction in the cross-sectional area of the left ventricle (LV), as viewed in the short axis, closely approximates its ejection fraction (EF). We assessed the reliability of using two-dimensional echocardlography (2DE) to visually estimate the EF during real-time viewing, without the need of dlgltlrers, planimetry, or calculations. Twenty-five adult hospitalized patients with either suspected or known cardiac disease were evaluated prospectively. Each patient also had gated nuclear anglography during the same admission, and 14 had cardiac catheterization with left ventriculography. The EF was determined by 2DE using a visual estimate of the percent area reduction of the LV cavity in the short-axis view at the level of the papillary muscles. All 2 DE studies were read by two or more blinded reviewers, wlth a value for the EF to the nearest 2.5% determined by consensus. These values correlated closely to the values determined in all 25 patients with gated nuclear anglography (I = 0.927) and the 14 patients who had left ventriculography (I = 0.935). We believe that this method of visually estimating the LVEF will enable echocardlographers to easily use 2 DE for a reliable and instantaneous assessment of ventricular function, without the need of sophisticated analytical equipment. (AM HEART J 104:603, 1982.)
Stuart Rich, M.D., Ajazuddin Sheikh, M.D., Jose Gallastegui, M.D., George T. Kondos, M.D., Theresa Mason, M.D., and Wilfred Lam, M.D.Chicugo, Ill.
Two-dimensional echocardiography (2DE) has been shown to be a reliable technique for measuring left ventricular (LV) ejection fraction (EF) using assumptions about the geometry of the LV and applying appropriate mathematical formulas.1-3 The wide utilization of 2DE for this purpose has not been forthcoming, however, because it is a time-consum- ing process that requires tracing the outline of the LV in systole and diastole and then measuring the outlined areas. In addition, by freeze-framing the real-time images for tracing, much of the image quality becomes degraded, making the process even more difficult. We developed a method for evaluat- ing the LVEF during real-time display with 2DE by visual estimation using specific guidelines. We were able to achieve a reliable assessment of LV function while avoiding the need for freeze-framing, planime- try, or using digitized computers.
From the Section of Cardiology, Department of Medicine, Abraham Lincoln School of Medicine. Supported in part by National Heart, Lung and Blood Institute Grant HL 07387.
Received for publication Jan. 25, 1982; accepted Feb. 12, 1982.
Reprint requests: Stuart Rich, M.D., Cardiology Section, University of Illinois Hospital, P.O. Box 6998, Chicago, IL 60680.
0002~8703/82/090603 + 04$00.40/O 0 1982 The C. V. Mosby Co.
METHODS
Patients. Twenty-five hospitalized adult patients who underwent 2DE in our laboratory during July and August, 1981, comprise the study. Patients were unselected con- secutive prospective studies who had technically satisfac- tory echocardiograms and who also had a gated cardiac blood pool image during the same hospitalization. Four- teen of these patients also went on to have cardiac catheterization with left ventriculography. The 25 patients (15 male, 10 female) were between 22 and 68 years of age (mean = 44) and had a variety of cardiac disorders (valvular heart disease (six) coronary artery disease (five), cardiomyopathy (three), primary arrhyth- mic disturbances (three), hypertensive heart disease (one), mitral valve prolapse (one), pericardial effusion (one), and no detectable abnormalities (five).
2DE examination and estimation of LVEF. 2DE was recorded using a commercially available phased array sector scanner (Toshiba SSH-1OA) with a 2.4 MHz trans- ducer. Studies were recorded on a videocassette recorder (Panasonic NV 8200) for later playback and review. All of the patients studied were in a left lateral recumbent position. The echocardiograms were performed using mul- tiple views through the left parasternal and apical win- dows. The determination of LVEF was made solely from the short-axis view of the LV at the level of the papillary muscles. The assessment was made during real-time view- ing, by looking at the repetitive changes in the endocardial
603

604 Rich et al. September, 1982
American Heart Journal
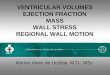
Fig. 1. Two-dimensional echocardiogram of the left ventricle in the short axis at the level of the papillary muscles. Even in this relatively good quality study there is loss of the endocardial outline during freeze-framing (A). The ejection fraction, in this case 55%) was taken as the estimated reduction of the cross-sectional area of the left ventricle. Repetitive viewing during real-time display allows a better determination of these areas. A graphic representation of a measured 55 % area reduction is shown below
outlines between systole and diastole. Two reviewers, blinded to the results of any other cardiac studies, made an estimation of the percent reduction of the intraventri- cular area at that level during systole and diastole, to the nearest 2.5%. When there was disagreement as to the results, an average of the two estimates was taken (Fig. 1).
Radionuclide measurement of LVEF. ECG gated, equi- librium nuclear angiography was performed using an in vivo RBC labeling method with 15 to 25 mCi of techne- cium-99m.’ A large field Anger camera was positioned in the left anterior oblique (LAO) view, chosen for the best visualization of the ventricular septum, with the patient supine. Data were recorded and analyzed in an Informatek Series 3 computer. Acquisition continued until there were 500,000 counts/frame. The LVEF was calculated in a manner previously described,6 using the formula: EF = (end diastolic counts - end systolic counts)/(end diastolic counts) x 100.
Anglographk measurement of LVEF. Fourteen of the 25 patients studied underwent cardiac catheterization during the same hospitalization. Biplane LV angiograms were obtained in each, using a 3bdegree right anterior oblique view, and a 35-degree LAO view with caudal- cranial angulation of 30 degrees. The LV silhouetfe was traced at end-diastole (the largest area) and end-systole
(the smallest area), and the LVEF was calculated using the area-length method.6 Only beats in sinus rhythm not preceded by a premature contraction were used for analy- sis.
Statistical methods. Measurements of EF by 2DE, gated nuclear angiography, and left ventriculography were all made independently. The Pearson product moment correlation coefficient was used to correlate the associa- tions between 2DE, gated nuclear angiography, and left ventriculography.
RESULTS
PDE/RNV LVEF. The ejection fraction in the 25 patients studied as determined by 2DE ranged from 10% to 75% (mean 49.1 + 18.2% SD). The value for the same group of patients as determined by gated nuclear angiography (RNV) ranged between 14% and 79% (mean 51.6 + 19.2% SD). Linear reg’res- sion analysis on the association of EF determined by echocardiography with nuclear angiography re- vealed a correlation coefficient of F = 0.927, with a slope of y = 0.98x + 3.4 (p < 0.001) (Fig. 2).
PDE/contrast angiography LVEF. The ejection fraC- tions of the 14 patients who underwent cardiac catheterization were also compared to the corre-

Volume 104
Number 3 Reliable/practical LVEF estimate by 2DE 605
80
25 0.93 0.98x + 0.0001
3.4
5 60- i= 2 [1I 50- lL
1 IO 20 30 40 50 60 70 80
i/, IO 20 30 40 50 60 70
GATED NUCLEAR EJECTION FRACTION (%) LEFT VENTRICULOGRAM EJECTION FRACTION (%)
Fig. 2. Comparison of left ventricular ejection fraction as estimated using two-dimensional echocardiography vs
Fig. 3. Comparison of left ventricular ejection fraction as
gated nuclear angiography. estimated using two-dimensional echocardiography vs left ventriculography.
sponding results by 2DE. The values for EF by left ventriculography ranged from 15% to 70% (mean 48.8 + 21.2% SD) and by 2DE between 10% and 75% (mean 52.2 + 19.8% SD). Linear regression analysis on the association of the EF determined by these two techniques revealed a correlation coeffi- cient of r = 0.935 with a slope of y = 1.0x - 3.4 (p < 0.001) (Fig. 3).
DISCUSSION
Reliability of calculated LVEF by 2DE. 2DE has been shown to be a reliable technique for measuring the LVEF.~T~ Previous established methods, however, have required that the endocardial outlines of the ventricle be traced in systole and diastole, with the outlined areas then planimeterized and converted to volumes using any of several formulas. The major limitations in these methods have been the time necessary to perform the measurements and the loss of definition in the endocardium from freeze-fram- ing the images. Some investigators have made the process easier by the use of sophisticated computer- ized light pen systems or off-line digital analyzers, but this equipment is not widely available.
Reliability of estimated LVEF by 2DE. We sought to assess the reliability of making a visual estimate of LV function without the need for planimitry or computerized analyzers, so that our method could be utilized widely by most laboratories. Previous inves-
tigators have shown that the calculated reduction in cross-sectional area of the LV as viewed in the short axis closely approximates the EF.? We found that with a short period of training (within 3 months), an echocardiographer could make reliable estimates of the amount of area reduction of the short-axis of the LV when viewed repetitively in real-time. By avoid- ing freeze-framing of the video recorded images, most patients undergoing echocardiography will have echocardiograms of sufficient quality to enable an assessment of cardiac function. In addition, this technique is particularly attractive by the fact that it is neither time-consuming nor does it require accessory computerized equipment, thus allowing an instantaneous assessment of LV function.
Estimated LVEF best expressed as qualitative equiv- alent. In our practice, since the number for the EF determined in this manner is not a calculated value, we feel that it is more appropriate to report the result of an EF as either a range (such as “between 35 % and 40 % “), or as a qualitative equivalent (such as mildly, moderately, or severely diminished). We also recommend that an echocardiographer compare his estimations to other techniques, such as nuclear angiography, before reporting results by this meth- od, to assess his own accuracy and reliability.
Limitations of estimated LVEF technique. Like any echocardiographic study, this technique is limited to those patients in whom the quality of the recorded

Rich et al. September, 1982
American Heart Journal
images is sufficient to permit analysis. In addition, it should be kept in mind that we are overlooking the shortening of the ventricle in the major axis, which on the average contributes 3% to 7% to the actual EF.? The method would also be unreliable in patients with large discrete ventricular aneurysms that are not included in the short-axis view of the ventricle. Our experience in patients with coronary artery disease in general, however, is that the meth- od is useful and reliable.
Conclusions. We found that the percent area reduction of the LV as viewed in the short axis with 2DE closely approximates the actual LVEF, and that this percent change can be reliably estimated by trained echocardiographers. This method obvi- ates the need for planimetry, digitizers, or calcula- tions. In addition, by making the estimates during real-time viewing, an instantaneous assessment of LV function can be made and image quality is preserved, making this technique applicable to most patients who are studied. REFERENCES
1. Carr KW, Engler RL, Forsythe JR, Johnson AD, Gosink B: Measurement of left ventricular ejection fraction by mechan-
2.
3.
4.
5.
6.
7.
ical cross-sectional echocardiography. Circulation 59:1196, 1979. Folland ED, Paris AF, Moynihan PF, Jones DR, Feldman CL, Tow DE: Assessment of left ventricular ejection fraction and volumes by real-time, two-dimensional echocardiogra- phy. Circulation 60:760, 1979. Gueret P, Meerbaum S, Wyatt HL, Uchiyama T, Lang T-W, Corday E: Two-dimensional echocardiographic determina- tion of left ventricular volumes and ejection fraction. Circu- lation 62:1309, 1980. Pave1 DG, Zimmer AM, Patterson UN: In vivo labeling of red blood cells with 99m Tc: A new approach to blood pool visualization. J Nucl Med l&305, 1977. Pave1 DG, Byrom E, Ayres B, Pietras PJ, Bianco JA, Kanakis C: Multifaceted evaluation of left ventricular function by the first transit technique using Anger type cameras and an optimized protocol: Correlation with biplane roentgen angi- ography. In Sorenson JA, editor: Nuclear cardiology: Select- ed computer abstracts. Atlanta, 1978, Society of Nuclear Medicine, pp 129-138. Dodge HT:-Determination of left ventricular volume and mass. Radio1 Clin North Am 9:459. 1971. Quinones MA, Waggoner AD, Reduto LA, Nelson JG, Young JB, Winters WL, Ribeiro LG, Miller RR: A new, simplified and accurate method for determining ejection fraction with two-dimensional echocardiography. Circulation 64:744, 1981.
The calcium-channel blocker, nifediplne, was used as addltional oral therapy to betaudrenergic receptor blockade by the cardtoselective agent, atenolol, in the therapy of 31 pattents with hypertension. Initial studies were directed towards control of assoctated angina pectoris In 15 of the patients, but no effects were found on angina except in two pattents. However, artertal blood pressure was condstently reduced In all pattents. Further studies on 16 patients were therefore directed towards the use of nifedlpine as an antthyperten8ive agent In addttton to atenolol and a thlazide dhtretfc. Nifedtpine (10 mg subtlngualty) acutely dropped blood pressure by about 30120 mm HI) (systolic/diastolic) wlthin 20 minutes. Follow-up studks made after 4 to 8 weeks showed that the lnltlal acute response to nifedipine predlcted the long-term response to oral ntfedtpfne, 10 mg twice daily. Of 31 hypertensive patients tested, only one failed to respond to nlfedtplne. (Au HEART J 104:606, 1982.)
L. H. Opie, L. Jee, and D. White. Cape Town, South Africa
From the Hypertension Clinic, Department of Medicine, Groote Schuur Nifedipine is a calcium antagonist drug which has Hospital and University of Cape Town. been used primarily in the treatment of angina Received for publication Dec. 28, 1981; revision received Apr. 29, 1982; pectoris. The recently described clinical efficacy of accepted May 18, 1982. Reprint requests: Lionel H. Opie, M.D., Dept. of Medicine, Hypertension
n&&pine as an antihypertenaive agent can be
Clinic, Univereity of Cape Town, Medical School, Obeervatmy 7925, Cape ascribed to its direct vascular effect which is medi- Town, South Africa. ated by a decrease in systemic vascular resistance,
606 0002-8703/82/090606 + 07$00.70/O 0 1982 The C. V. Mosby Co.