Embed Size (px)
Citation preview

DETECTION OF PNEUMOCOCCUS BY PCR
ANNIKASAUKKORIIPI
Department of Medical Microbiology,University of Oulu
National Public Health Institute,Department of Microbiology
OULU 2003


ANNIKA SAUKKORIIPI
DETECTION OF PNEUMOCOCCUS BY PCR
Academic Dissertation to be presented with the assent ofthe Faculty of Medicine, University of Oulu, for publicdiscussion in the Auditorium of Kastelli Research Center(Aapistie 1), on November 29th, 2003, at 12 noon.
OULUN YLIOPISTO, OULU 2003

Copyright © 2003University of Oulu, 2003
Supervised byProfessor Maija Leinonen
Reviewed byDocent Kirsi LaitinenDocent Simo Nikkari
ISBN 951-42-7211-0 (URL: http://herkules.oulu.fi/isbn9514272110/)
ALSO AVAILABLE IN PRINTED FORMATActa Univ. Oul. D 767, 2003ISBN 951-42-7210-2ISSN 0355-3221 (URL: http://herkules.oulu.fi/issn03553221/)
OULU UNIVERSITY PRESSOULU 2003

Saukkoriipi, Annika, Detection of pneumococcus by PCR Department of Medical Microbiology, University of Oulu, P.O.Box 5000, FIN-90014 University ofOulu, Finland, National Public Health Institute, Department of Microbiology, P.O.Box 310, FIN-90101 Oulu, Finland Oulu, Finland2003
Abstract
New rapid methods for sensitive and specific detection of pneumococci are not only needed toimprove the diagnosis of pneumococcal disease but are also essential for vaccine and carriage studies.The purpose of this study was to develop sensitive PCR methods for the detection and quantificationof S. pneumoniae and to study the applicability of these methods to detecting pneumococci in clinicalsamples.
A previously described PCR method was first developed further by introducing a Europium-labelled hybridisation probe for the detection of amplification products. The hybridisation methodwas easy to use and improved the specificity of the PCR assay. The developed PCR assay wasestablished as a sensitive method for detecting pneumococcal DNA when the presence ofpneumococcal DNA in over 2500 middle ear fluid (MEF) samples of children with acute otitis media(AOM) was studied by using the method. Pneumococcal findings increased by 76% when using PCRdetection in addition to culture, compared to using culture alone. However, the PCR-positive, culture-negative AOM events represented a less severe type of disease compared to the culture-positiveevents. A positive PCR finding seems to indicate the presence of viable, although often non-culturable pneumococci within the middle ear cleft.
To be able to rapidly detect and quantify the initial numbers of pneumococcal genome copies inclinical samples, a real-time PCR method for the detection and quantification of pneumococcal DNAwas developed. In real-time PCR, amplification and detection of amplification products occursimultaneously, which makes it possible to monitor the phase of the reaction at a particular stage orcontinuously. The method developed here was applied to the analysis of MEF samples and toinvestigating the nasopharyngeal carriage of pneumococcus. The sensitivities of bacterial culture andreal-time PCR in detecting pneumococci were also compared. The real-time PCR assay was found tobe rapid and sensitive and to provide information about the differences between the numbers ofbacteria in samples. However, the quantitative results were shown to be dependent on the DNAextraction method applied. The real-time PCR method developed appears to be a good aid in researchwhere an accurate and sensitive pneumococcal diagnosis is needed.
Keywords: bacterial DNA, Europium, nasopharynx, otitis media, pneumolysin, polymerase chainreaction, Streptococcus pneumoniae


Acknowledgements
The present study was carried out at the National Public Health Institute (KTL) Department of Microbiology in Oulu and the Department of Medical Microbiology at the University of Oulu during the years 2000-2003.
I wish to express my deepest gratitude to my supervisor, Professor Maija Leinonen, PhD. Her vast experience, enthusiasm towards research and positive attitude have made it very inspiring to work under her guidance. I am deeply indebted to her for her encouragement and kind support, which have made this thesis possible.
I would like to thank the official reviewers of this thesis, Docent Kirsi Laitinen, PhD, and Docent Simo Nikkari, MD, PhD, for their valuable and constructive criticism. I appreciate their positive attitude and good advice. I am also grateful to Sirkka-Liisa Leinonen, PhL, for efficiently revising the English language of this thesis.
I am grateful to Professor Tapani Hovi, MD, PhD, Head of the Department of Microbiology at KTL, for his interest in this work and for his valuable and encouraging comments on the original manuscripts. I also wish to thank the former Head of the Department of Medical Microbiology at the University of Oulu, Emeritus Professor Pekka Saikku, MD, PhD, for his support and guidance to microbiology in general.
The contributions of all my co-authors and collaborators have been invaluable and I owe my sincere gratitude to them. I wish to thank Docent Elja Herva, MD, PhD, and Docent Terhi Kilpi, MD, PhD, for their friendly guidance and valuable advice. I also thank Academician P. Helena Mäkelä, MD, PhD, for her valuable advice concerning our manuscript. It has been a great privilege to work with her. Special thanks are due to Arto Palmu, MD, PhD, for his hard work with paper V and friendly and encouraging support. I also wish to thank Paula Korhola, PhD, Mika Lahdenkari, MSc, Sanna Rintamäki, MSc, and Docent Aino Takala, MD, PhD. My warm thanks are due to Leena Kuisma, RN, not only for her experience in PCR but also for her friendship and continuous support. Our discussions have been of great value especially when the PCRs have been misbehaving. I am also grateful to Tarja Kaijalainen, MSc, Kristiina Leskelä, BM, and Anu Ojala, RN, for their extensive assistance and friendship.
I am thankful to all the staff at KTL in Oulu, especially my dear friends and colleagues Tiina Sävykoski, PhD, Liisa Törmäkangas, MSc, Leena Erkkilä, MSc, Taina Korhonen,

MSc, and Mika Paldanius, MSc, who have all done PhD research at the same time as I. Our discussions during the lunch and afternoon coffee breaks have been fun and sharing the difficulties of being a researcher with you has made everything a little easier. I would like to thank Anne Jaakkola, RN, for her friendship and for being an excellent opponent at the tennis court. I also wish to acknowledge Aini Bloigu, BSc, for her assistance with the statistical work.
I wish to thank all my friends outside KTL: your friendship, support and never-failing encouragement has meant a lot to me, even if the possibilities to meet with some of you have not always been the best because of the geographical distance.
My warmest thanks go to my family for always being there and for giving me all their support. I thank my parents for their encouragement and belief in me and for letting me do things in my own way. I also wish to thank my big sister for her friendship and support.
This study was financially supported by the Finnish Konkordia Fund, Merck, Aventis Pasteur, and Wyeth Lederle Vaccines.
Oulu, October 2003 Annika Saukkoriipi

Abbreviations
AOM acute otitis media BHI brain heart infusion bp base pair CbpA cholin-binding protein A CFU colony-forming unit CIEP counterimmunoelectrophoresis COA coagglutination CSF cerebrospinal fluid DNA deoxyribonucleic acid dsDNA double-stranded deoxyribonucleic acid EIA enzyme immunoassay FinOM Finnish Otitis Media (Cohort Study, Vaccine Trial) FRET fluorescence resonance energy transfer IC immune complex IgA immunoglobulin A IgG immunoglobulin G kDa kilodalton LA latex agglutination LytA pneumococcal autolysin MEF middle ear fluid mRNA messenger ribonucleic acid OD optical density OME otitis media with effusion PBS phosphate-buffered saline PCR polymerase chain reaction ply pneumolysin PsaA pneumococcal surface adhesin A PspA pneumococcal surface protein A PspC pneumococcal surface protein C RNA ribonucleic acid rRNA ribosomal ribonucleic acid

STGG skimmed milk, tryptone, glucose, glycerol TRF time-resolved fluorescence

List of original publications
The thesis is based on the following articles, which are referred to in the text by their Roman numerals. I Rintamäki S, Saukkoriipi A, Salo P, Takala A, Leinonen M (2002) Detection of
Streptococcus pneumoniae DNA by using polymerase chain reaction and microwell hybridization with Europium-labelled probes. J Microbiol Methods 50: 313-318.
II Saukkoriipi A, Palmu A, Kilpi T, Leinonen M (2002) Real-time quantitative PCR for the detection of Streptococcus pneumoniae in the middle ear fluid of children with acute otitis media. Mol Cell Probes 16:385-390.
III Saukkoriipi A, Kaijalainen T, Kuisma L, Ojala A, Leinonen M (2003) Isolation of pneumococcal DNA from nasopharyngeal samples for real-time, quantitative PCR. Comparison of three methods. Mol Diagn 7:9-15.
IV Saukkoriipi A, Leskelä K, Herva E, Leinonen M. Streptococcus pneumoniae in nasopharyngeal secretions of healthy children: comparison of real-time PCR and culture from STGG-transport medium. Submitted for publication.
V Palmu A, Saukkoriipi A, Lahdenkari M, Kuisma L, Mäkelä PH, Kilpi T, Leinonen M. Does the presence of pneumococcal DNA in the middle ear fluid indicate pneumococcal etiology in acute otitis media? J Infect Dis, in press.
Some previously unpublished data are also presented.
The original articles are reprinted with permission from Elsevier (I, II), Adis International Limited (III), and The University of Chicago, © by the Infectious Diseases Society of America (V).


Contents
Abstract Acknowledgements Abbreviations List of original publications 1 Introduction ...................................................................................................................13 2 Review of the literature .................................................................................................15
2.1 Streptococcus pneumoniae......................................................................................15 2.1.1 Structure and virulence factors ........................................................................15
2.1.1.1 Capsule .....................................................................................................16 2.1.1.2 Pneumococcal proteins .............................................................................19
2.1.2 Pneumococcal carriage ....................................................................................22 2.1.3 Pneumococcal infections .................................................................................23
2.1.3.1 Noninvasive infections .............................................................................23 2.1.3.2 Invasive infections....................................................................................24
2.1.4 Prevention of pneumococcal infections...........................................................25 2.1.4.1 Host defence mechanisms.........................................................................25 2.1.4.2 Vaccines ....................................................................................................26
2.1.5 Diagnosis of pneumococcal infection..............................................................28 2.1.5.1 Culture ......................................................................................................29 2.1.5.2 Antigen detection......................................................................................30 2.1.5.3 Nucleic acid amplification........................................................................31 2.1.5.4 Serology....................................................................................................33
2.2 Real-time PCR........................................................................................................34 2.2.1 Applications.....................................................................................................35
2.2.1.1 Detection of S. pneumoniae......................................................................35 3 Aims of the study...........................................................................................................37 4 Materials and Methods ..................................................................................................38
4.1 Subjects and specimens ..........................................................................................38 4.2 Methods ..................................................................................................................39
4.2.1 Sample treatment and bacterial culture............................................................39 4.2.2 DNA extraction................................................................................................40

4.2.3 Oligonucleotides used for amplification and detection ...................................42 4.2.4 Conventional PCR and microwell hybridisation (I, II, V)...............................43 4.2.5 Real-time quantitative PCR (II- V)..................................................................45 4.2.6 Comparison of the sensitivities of bacterial culture and real-time PCR ..........47 4.2.7 Statistical methods...........................................................................................47
5 Results ...........................................................................................................................48 5.1 Development of methods (I, II) ..............................................................................48
5.1.1 Conventional PCR and microwell hybridisation (I) ........................................48 5.1.2 Real-time quantitative PCR (II).......................................................................49
5.2 Effect of the DNA extraction method on the quantitative real-time PCR results obtained (III)........................................................................52 5.3 Comparison of real-time PCR and pneumococcal culture (III, IV) ........................53 5.4 Detection of pneumococcal DNA in nasopharyngeal swab specimens using real-time PCR (IV)........................................................................................54 5.5 Detection of pneumococcal DNA in MEF samples (V) .........................................56
6 Discussion .....................................................................................................................60 6.1 Methods developed in the study .............................................................................60 6.2 Samples and sample preparation ............................................................................63 6.3 Comparison of PCR and culture findings ...............................................................65 6.4 Presence of pneumococcal DNA in MEF samples (V)...........................................66 6.5 Future research .......................................................................................................68
7 Conclusions ...................................................................................................................70 References

1 Introduction
Streptococcus pneumoniae is a common human pathogen that causes a wide variety of infections, including otitis media, sinusitis, pneumonia, bacteremia and meningitis. The pneumococcus has been extensively studied since its first isolation (reviewed by Austrian 1981), but its virulence mechanisms are still not completely understood (AlonsoDeVelasco et al. 1995). In spite of the availability of safe vaccines and antimicrobial treatment, pneumococcal infections remain an important cause of morbidity an mortality both in children an adults (Obaro et al. 1996b).
S. pneumoniae infections are conventionally diagnosed using bacterial culture combined with biochemical or immunochemical identification tests. Antibiotic treatment prior to the collection of patient specimens or autolysis of S. pneumoniae during the transportation of the specimen may, however, cause negative culture results. Several antigen detection methods for demonstrating pneumococcus in different body fluids have been developed, but the sensitivities of these methods vary (Kalin & Lindberg 1983, Boersma et al. 1991, Perkins et al. 1995). Serological methods for measuring antibodies to various pneumococcal antigens have mainly been used in research settings, as they require paired samples and, thus, cannot be used for rapid diagnosis (Nohynek et al. 1995). The first nucleic acid amplification method for pneumococcus was published in 1993 (Rudolph et al. 1993), and since then, several methods based on the amplification of different targets, including pneumolysin and autolysin-encoding genes have been described. A method based on the amplification of a fragment of the pneumolysin gene was published in 1995 by Salo et al. (1995). Pneumolysin is a species-specific protein toxin produced by virtually all pneumococcal strains isolated from clinical samples (Paton et al. 1983, Kanclerski & Möllby 1987), and the pneumolysin-encoding gene is thus a suitable target to be used in polymerase chain reaction (PCR). The detection of pneumococcal DNA by pneumolysin-based PCR has been shown to be a highly sensitive method, and the percentage of positive specimens detected has been higher than that detected with bacterial culture (Virolainen et al. 1994). However, the conventional PCR methods are often labour-intensive, especially when large numbers of samples need to be analysed. Also, the handling of amplification products, particularly in nested-PCR methods, involves a great risk of contamination of samples with DNA.

14
Real-time PCR, a modification of traditional PCR, was introduced in the late 1990s. In real-time PCR, the amplification products are detected during the process of amplification. Thus, the accumulation of amplification products can be followed. (Wittwer et al. 1997). A large number of real-time PCR applications have been published. For the detection of pneumococcus, four methods have recently been introduced (Kearns et al. 1999, Corless et al. 2001, Greiner et al. 2001, McAvin et al. 2001). However, little is known about the applicability of these methods to large numbers of clinical samples.
New, rapid methods for sensitive and specific detection of pneumcocci are needed to improve the diagnosis of pneumococcal disease, but they are also essential for vaccine and carriage studies. The aim of this study was to develop sensitive PCR methods for the detection and quantification of S. pneumoniae and to study the applicability of these methods to detecting pneumococci in clinical samples. A previously described PCR method (Salo et al. 1995) was further developed by the introduction of a Europium-labelled hybridisation probe for the detection of amplification products. The method was then used to study the presence of DNA in middle ear fluid (MEF) samples. A real-time PCR method was also developed for the detection and quantification of pneumococcal DNA. The method was applied to the analysis of MEF samples and to investigating the nasopharyngeal carriage of pneumococcus. In this study, the sensitivities of bacterial culture and real-time PCR in detecting pneumococci were also compared.

2 Review of the literature
2.1 Streptococcus pneumoniae
Streptococcus pneumoniae or pneumococcus is a species of the genus Streptococcus, which belongs to the family of Streptococcaceae (Lund & Henrichsen 1978). The pneumococcus was first isolated in 1881 independently by Sternberg in the USA and Pasteur in France, who both recovered diplococci from the blood of rabbits injected with human saliva. In 1886, the organism was referred to as Pneumococcus, but in 1920 it was renamed Diplococcus pneumoniae. It was not until 1974 that the pneumococcus received its present name, Streptococcus pneumoniae. (Reviewed by Austrian 1981, Watson et al. 1993).
2.1.1 Structure and virulence factors
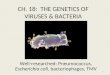
Pneumococci are facultatively anaerobic, Gram-positive, capsulated organisms that usually grow in pairs or short chains (Lund & Henrichsen 1978). Pneumococci are lancet-shaped diplococci with three major surface layers distinguishable: plasma membrane, cell wall and capsule. The innermost layer, the plasma membrane, anchors the pneumococcal F-antigen or lipoteichoic acid (Fig. 1). The pneumococcal cell wall consists of a triple-layered peptidoglycan backbone, to which both the cell wall polysaccharide (C-polysaccharide) and the capsular polysaccharide are anchored (Fig. 1). The C-polysaccharide is a structure common to all pneumococcal serotypes, whereas each of the currently known 90 serotypes has a specific capsular polysaccharide (reviewed by AlonsoDeVelasco et al. 1995, Sørensen 1995). The capsular polysaccharide is the main virulence factor that protects pneumococci against the action of host defence mechanisms (Tomasz 1981, AlonsoDeVelasco et al. 1995, Watson et al. 1995). In addition to capsular polysaccharides, the other factors reported to contribute to pneumococcal virulence include C-polysaccharide, the pneumococcal hemolysin pneumolysin, pneumococcal

16
surface proteins and pneumococcal surface adhesin A. Pneumococcal enzymes, such as autolysin, neuraminidase, hyaluronidase and IgA1 protease, have also been suggested to play a role in the pathogenesis of pneumococcal disease. (Paton et al. 1993, AlonsoDeVelasco et al. 1995, Brooks-Walter et al. 1999).
Fig. 1. Schematic structure of the surface of S. pneumoniae (modified after: Musher 1995).
2.1.1.1 Capsule
When Pasteur published the description of S. pneumoniae in 1880, he already noted the structure that is now known to be the capsular polysaccharide. The capsular substance was isolated as early as 1917 by Dochez and Avery, but because of its immunogenicity, it was thought to be proteinaceous. In 1925, the capsule was demonstrated to consist of polysaccharide. (Reviewed by Paton & Morona 2000). Nearly all fresh clinical isolates of S. pneumoniae are encapsulated (Watson et al. 1995), the capsule forming a 200-400 nm thick, inert outer layer (Sørensen et al. 1988). The chemical structure of the capsular polysaccharide is type-specific, and ninety structurally distinct capsular polysaccharide types are currently known (Henrichsen 1995). At its simplest, the capsular polysaccharide is a linear polymer with repeating units consisting of two or more monosaccharides. More complicated capsular polysaccharides are branched, and the repeat unit backbones consist of one to six monosaccharides and have additional side chains. (Reviewed by Paton & Morona 2000). The capsular polysaccharide appears to be covalently attached to the cell wall peptidoglycan in all serotypes except type 3 (Sørensen et al. 1990). Two nomenclature systems for the pneumococcal capsular serotypes exist: a Danish and an American. The more widely used Danish nomenclature, in which types that possess common capsular antigens compose a group, was first published by Kaufmann et al. in 1940 (reviewed by Lund & Henrichsen 1978, Henrichsen 1999), but has later been extended (Henrichsen 1995). In the American nomenclature, introduced in 1944 by Eddy
PHOSPHOLIPID
LIPOTEICHOIC ACID(F-ANTIGEN)
PEPTIDOGLYCAN
CAPSULAR POLYSACCHARIDE
CELL WALL POLYSACCHARIDE (CELL WALL TEICHOIC ACID)
PLASMA MEMBRANE
CELL WALL

17
et al., different types have consecutive numbers regardless of their antigenic structure (reviewed by Henrichsen 1999).
The capsule is the major virulence factor in S. pneumoniae, but the mechanisms by which it confers to virulence are not completely understood. Purified pneumococcal capsular polysaccharides are not toxic to human or animals, but they are known to have strong antiphagocytic properties in nonimmune hosts (Musher 1992). At biological pH, the majority of pneumococcal serotypes are highly charged, which may disturb the interactions with phagocytes (Lee et al. 1991). The capsule also interferes with the activation of the alternative complement pathway (Silvennoinen-Kassinen & Koskela 1986) and complement components appear to be deposited and degraded on it (Hostetter 1986, Angel et al. 1994). Different pneumococcal serotypes are known to vary in their capacity to resist phagocytosis in vitro (Chudwin et al. 1985, Silvennoinen-Kassinen & Koskela 1986). The ability of serotypes to elicit a humoral immune response also varies (van Dam et al. 1990), and consequently, certain serotypes are more commonly associated with human disease (Austrian 1977). The differences in virulence between the pneumococcal serotypes do not seem to depend merely on the thickness of the capsule (Kim & Weiser 1998), but more importantly, also on the biological properties of the capsular polysaccharide (Paton & Morona 2000, Magee & Yother 2001).
Capsular polysaccharide synthesis requires a complex pathway consisting of synthesis of the component monosaccharides and their activation into nucleotide precursors, sequential transfer of each sugar to form the repeating oligosaccharide and subsequent polymerization, export and attachment to the cell wall (reviewed by Paton & Morona 2000). In the 1990s, cloning and sequencing of the genes encoding the biosynthesis of capsular polysaccharide were first described, the first loci to be completely sequenced being those of the pneumococcal serotypes 3 (Arrecubieta et al. 1995, Dillard et al. 1995) and 19F (Guidolin et al. 1994, Morona et al. 1997a). There are remarkable differences between these two loci, but both are located at the same position, between dexB and aliA, in the chromosome. The capsular polysaccharide of type 3 has a simple structure consisting of a disaccharide repeat unit, and the capsular polysaccharide biosynthesis locus (cps) of type 3, called cps3 or cap3, consists of only three intact genes that are transcribed as a single unit (Arrecubieta et al. 1995, Dillard et al. 1995). The type 3 capsule appears to be synthesized in a distinct way directly from activated monosaccharides by a processive transferase (Arrecubieta et al. 1996). The type 19F capsular polysaccharide is more complex than that of type 3, and the cps19F locus is also more complex, consisting of 15 genes tightly clustered on the chromosome. By comparing the sequence of the cps19F locus to sequence databases and by complementation analysis, functions have been proposed for most of the cps19F gene products. Additionally, a putative biosynthetic pathway for type 19F capsular polysaccharide has been assigned. (Morona et al. 1997a). Recently, sequence data for several other pneumococcal capsular polysaccharide biosynthesis loci, including the types 1, 2, 4, 6B, 8, 9V, 14, 18C, 19A, 19B, 19C, 23F and 33F, have become available (reviewed by Paton & Morona 2000, Jiang et al. 2001, van Selm et al. 2002).
The number of genes comprising the cps loci in different serotypes vary, but the organization of the genes resembles that of the cps locus of type 19F with homologous genes common to all or many capsular polysaccharide types flanking type-specific genes (Kolkman et al. 1997, Munoz et al. 1997, Morona et al. 1999a, Paton & Morona 2000).

18
The conserved 5´ regions of the different cps loci, with the exception of the type 3 locus, encode proteins thought to be involved in the regulation and export of capsular polysaccharide. The central parts of the different cps loci encode glycosyltransferases, the polysaccharide polymerase and the repeat unit transporter. The glycosyltransferases are highly specific in regard to the substrate and form distinct glycosidic linkages, and the putative polysaccharide polymerase and transporter genes are also highly specific. With the exception of type 14, the 3´ regions of the different cps loci encode enzymes for the synthesis of activated monosaccharide precursors. The functions of many of the individual genes in the cps loci of different serotypes, however, await confirmation by conventional biochemical and genetic analysis. (Paton & Morona 2000). The common organization of genes in the cps loci of different serotypes, however, suggests that the mechanism of capsule biosynthesis is common, and that this structure may also allow pneumococci to change their capsule type, as the homologous regions can mediate recombinational exchange (Coffey et al. 1991, Morona et al. 1997b).
Immunologically cross-reactive serotypes presumably share structural similarities in their capsular polysaccharides, and by studying their cps locus, information about the mechanisms of how capsular diversity is generated can be gained. The cps loci of the serotypes comprising group 19 (19F, 19A, 19B, and 19C) have been characterized and compared to each other (Morona et al. 1999b). The arrangement of the genes within the group 19 cps loci was shown to be highly conserved: thirteen genes are common to all four members of the serogroup, and nearly all of the common genes from the types 19F, 19B and 19C are over 95% identical to each other. The genes comprising the type 19A cps locus were found to be more divergent, and the sequence homology between the individual genes of the 19A and 19F cps loci varies from 70 to 99%. The genetic differences that have been identified between the cps loci of the serotypes comprising group 19 are consistent with the polysaccharide structures of each serotype. The capsular polysaccharides of types 19F and 19A are structurally quite similar, as are those of the types 19B and 19C. Transformation studies have shown that the polysaccharide polymerase genes, cps19aI and cps19FI, are likely to be the cause of structural differences between the 19A and 19F capsular polysaccharides. The cps19c locus is almost identical to the cps19b locus, with the exception of an extra gene, cps19cS. This gene has been proposed to encode a glycosyl transferase required for the addition of a glucose side chain present in the 19C capsular polysaccharide. (Morona et al. 1999b, Paton & Morona 2000).
In 1944, Avery, MacLeod and McCarty (1944) showed in their transformation studies that DNA constituted the genetic material responsible for phenotypic changes during transformation. This was the first report on the biologic activity of a nucleic acid ever published. Capsule switching may be relatively common among pneumococci in nature (Coffey et al. 1998a). Modern molecular typing techniques have provided the means to detect otherwise genetically indistinguishable pneumococci that express different capsular types (Coffey et al. 1991, Barnes et al. 1995, Coffey et al. 1998b). In the capsule switching events studied by Coffey et al. (1998a), switching occurred as a consequence of homologous recombination and was shown to involve exchange of large DNA fragments at least 15 kb in size. A good opportunity for exchanging DNA between different serotypes is available in the human nasopharynx, where multiple serotypes of pneumococci are frequently carried, and where capsule switching may provide a

19
mechanism to avoid serotype-specific host immune defences (Paton & Morona 2000). However, the results of a recent study by Meats et al. (2003) suggest that serotype exchange during nasopharyngeal carriage is relatively rare.
2.1.1.2 Pneumococcal proteins
Several proteins have been suggested to be involved in the pathogenesis of S. pneumoniae, pneumolysin being the one most actively studied. More recently, pneumococcal cell surface proteins have also been studied more intensively, and they are likely to be important virulence determinants.
Pneumolysin is a 53-kDa intracellular toxin and a known virulence factor of S. pneumoniae produced by virtually all clinical isolates (Paton et al. 1983, Kanclerski & Möllby 1987, Boulnois et al. 1991, Paton et al. 1993). Direct evidence of the involvement of pneumolysin in pneumococcal pathogenesis was obtained in 1983, when it was shown that mice previously immunized with pneumolysin survived a nasally administered pneumococcal challenge significantly longer than control mice (Paton et al. 1983). Inactivation of the pneumolysin gene has also been shown to reduce pneumococcal virulence significantly, but not to eliminate it completely (Berry et al. 1989, Berry et al. 1992), which indicates that other pneumococcal components are also involved in virulence (Paton et al. 1993). Pneumolysin belongs to the family of thiol-activated cytolysins, which are produced by several Gram-positive bacteria and inactivated by cholesterol (Johnson et al. 1980, Paton 1996). In contrast to the other cytolytic toxins, pneumolysin is not secreted by pneumococci (Johnson 1977, Walker et al. 1987). The thiol-activated toxins presumably act by binding to the target cell membrane via interaction with cholesterol, which results in the insertion of the monomeric toxin into the lipid bilayer. Subsequently, the monomers oligomerize and form transmembrane pores, which cause cell lysis. (Boulnois et al. 1991). In addition to its cytolytic properties, pneumolysin has several effects at lower, sublytic concentrations: it stimulates the production of the pro-inflammatory cytokines tumour necrosis factor α and interleukin-1β by human monocytes (Houldsworth et al. 1994), it has been shown to slow down the ciliary beating of human nasal epithelium cells (Feldman et al. 1990) and to be cytotoxic to pulmonary alveolar epithelial cells (Rubins et al. 1993), it inhibits the proliferation of human lymphocytes in vitro (Ferrante et al. 1984), it decreases the bactericidal activity and migration of human polymorphonuclear leukocytes (Paton & Ferrante 1983), and it is capable of directly activating the classical complement pathway in the absence of specific antibody (Paton et al. 1984). The last-mentioned activity is mediated by the ability of pneumolysin to bind directly to the Fc fragment of human immunoglobulin G (IgG), and it may be unrelated to the cytolytic activity of pneumolysin, since it does not appear to be inhibited in serum by treatment with cholesterol (Paton et al. 1993).
The gene encoding pneumolysin has been cloned and sequenced (Paton et al. 1986, Walker et al. 1987). Thiol-activated toxins share considerable primary amino acid sequence homology, which explains their serological cross-reactivity. The genes encoding

20
these toxins are, however, only weakly homologous, indicating that they have diverged extensively from a common ancestor. (Boulnois et al. 1991). Consistent with the cytoplasmic location of pneumolysin in pneumococcus, the predicted amino acid sequence of pneumolysin showed that it lacks an N-terminal signal sequence that is present in the other thiol-activated toxins (Walker et al. 1987, Boulnois et al. 1991). Interestingly, the pneumolysin shares limited sequence homology with the human C-reactive protein (CRP) (Mitchell et al. 1991), which is an acute-phase protein that activates the classical pathway of complement in an antibody-independent manner through the direct binding of the C1q component to CRP after binding to its ligand (Agrawal et al. 2001). Preliminary data indicate that pneumolysin may also be able to bind C1q directly and thus be able to compete with CRP and abrogate its protective effects (Paton et al. 1993).
The major pneumococcal autolysin (LytA) is a 36-kDa amidase located in the cell envelope (Höltje & Tomasz 1976, Paton et al. 1993). It is believed to be bound to cholin present in the cell membrane lipoteichoic acid (Briese & Hakenbeck 1985). In this form, LytA is inactive but can be activated to cause cellular autolysis when the pneumococcus is in a stationary phase of growth, or when it is treated with antibiotics, such as penicillin. LytA has been suggested to play a role in pneumococcal pathogenesis by generating inflammatory degradation products of a cell wall. It has also been proposed to contribute to pneumococcal virulence by releasing pneumolysin from the cytoplasm. (Paton et al. 1993). Recently, however, it has been shown that the release of pneumolysin to an extracellular location does not require the activity of LytA (Balachandran et al. 2001).
The gene encoding the pneumococcal autolysin protein has been cloned and sequenced (García et al. 1985, García et al. 1986). Autolysin-deficient pneumococcal mutants have been shown to fail to undergo autolysis during the stationary phase of growth and following treatment with penicillin. Interestingly, these mutants also show a tendency to grow as short chains rather than as pairs, which has led to the suggestion that autolysin could also have a function in the daughter-cell separation. (Reviewed by Paton et al. 1993).
Pneumococcal surface protein A (PspA) is a 60 to 200-kDa pneumococcal antigen, which is serologically highly variable (Crain et al. 1990). It is bound to the pneumococcal cell membrane by interactions between the phosphorylcholine of lipoteichoic acid and the C-terminal repeat region of PspA (Yother & White 1994). PspA appears to be present on most of the clinical isolates of S. pneumoniae (Crain et al. 1990), and it seems to be required for full virulence of pneumococcus (McDaniel et al. 1987, Briles et al. 1988). McDaniel et al. (1987) showed that immunization of mice with nonencapsulated pneumococci in which the pspA gene had been inactivated conferred no protection against a challenge with virulent organisms, whereas mice immunized with the corresponding wild-type strain were protected. Intravenous injection of a virulent pneumococcal strain in which the pspA gene had been insertionally inactivated resulted in greater reduction of it in the blood of infected mice compared to an otherwise isogenic wild-type strain (McDaniel et al. 1987). However, the exact mechanisms by which PspA confers virulence are not fully understood. PspA has been shown to inhibit complement activation in vivo (Tu et al. 1999). In that study, infection of mice with pneumococci that lacked PspA caused higher levels of complement activation than infection with an isogenic pneumococcal strain that expressed PspA. The PspA-deficient strain was also

21
cleared more rapidly from the blood than the strain expressing PspA. (Tu et al. 1999). PspA has also been demonstrated to bind human lactoferrin, which is an iron-binding glycoprotein present in mucosal secretions, and neutrophilic leukocytes to the pneumococcal cell surface (Hammerschmidt et al. 1999, Håkansson et al. 2001). Thus, it was suggested that the interaction between lactoferrin and PspA could help pneumococci at mucosal surfaces to acquire the iron necessary for bacterial growth (Hammerschmidt et al. 1999). There is, however, evidence that pneumococci might also use iron sources other than lactoferrin. The interaction between PspA and lactoferrin might provide a way for pneumococci to interfere with host immune functions (Håkansson et al. 2001).
Pneumococcal surface protein C (PspC) is a 59 to 105-kDa pneumococcal protein, whose gene is found in about 75% of pneumococci (Brooks-Walter et al. 1999). PspC possesses strong molecular and serological similarities to PspA, and for this reason, the molecule was designated as PspC by Brooks-Walters et al. (1999). PspC has also been called CbpA (cholin-binding protein A), because it binds phosphorylcholine on the pneumococcal cell surface (Rosenow et al. 1997), and SpsA, because it binds human secretory IgA (Hammerschmidt et al. 1997). PspC elicits cross-reactive antibodies to PspA, which are able to provide protection against pneumococcal bacteremia (Brooks-Walter et al. 1999). PspC also interacts with the human complement pathway by binding to component C3 (Cheng et al. 2000, Balachandran et al. 2002) and factor H (Dave et al. 2001), and it has been shown to mediate the adherence of S. pneumoniae to cytokine-activated human cells (Rosenow et al. 1997). PspC appears to play a major role at mucosal surfaces, and it has been suggested to participate in the pneumococcal colonization of the nasopharynx (Rosenow et al. 1997, Balachandran et al. 2002). In an infant rat model, nasopharyngeal carriage of a pcpC (cbpA)-deficient mutant was reduced 100-fold. No significant difference in virulence was seen between this mutant and the isogenic parent strain in an intraperitoneal model of sepsis (Rosenow et al. 1997). However, Balachandran et al. (2002) showed that, following intravenous infection of mice in a bacteremia model, a strain lacking both PspA and PspC was less virulent and more rapidly cleared from blood than the parent strain or strains lacking only either one of the proteins. Thus, they suggested that PspA and PspC might be able to complement each other in their activities to block the clearance of pneumococci.
The pspC gene is paralogous to the pspA gene. Their gene products both include a highly conserved proline-rich region and a C-terminal cholin-binding repeat domain. (Brooks-Walter et al. 1999). The primary sequences of the N-terminal regions of PspC and PspA are different, but they share common structural features (Rosenow et al. 1997, Brooks-Walter et al. 1999). The structural similarities between PspA and PspC support the suggestion that these two surface proteins may have similar functions (Brooks-Walter et al. 1999).
Pneumococcal surface adhesin A (PsaA) is a 37-kDa metal-binding lipoprotein antigen, which was first described in 1990 (Russell et al. 1990). Immunization of mice with PsaA has been demonstrated to protect them against a challenge with pneumococci (Talkington et al. 1996). Pneumococcal carriage in mice has also been shown to be reduced by intranasal immunization with PsaA (Briles et al. 2000). The gene encoding PsaA has been cloned and sequenced (Sampson et al. 1994) and found to be conserved (Sampson et al. 1997). The psaA gene has been demonstrated in all of the 90 serotypes of S. pneumoniae (Morrison et al. 2000). However, the psaA gene has also been identified in

22
three viridans group streptococcal species and shown to have a high degree of homology with pneumococcal psaA (Jado et al. 2001).
2.1.2 Pneumococcal carriage
S. pneumoniae is often part of the normal nasopharyngeal flora, and most people acquire it for the first time during their first years of life (Gray et al. 1980, Vives et al. 1997, Syrjänen et al. 2001). Nasopharyngeal colonization is particularly rapid in developing countries (Gratten et al. 1986) and in some indigenous populations of developed countries (Leach et al. 1994): in these populations, children often acquire S. pneumoniae by the first few months of life. In industrialized countries, pneumococcus is usually acquired later in life (Aniasson et al. 1992, Leino et al. 2001). In a recent study in Finland, most children (87%) were colonized at least once by the age of 2 years (Syrjänen et al. 2001). Nasopharyngeal carriage of pneumococci constitutes a major reservoir (Austrian 1986), and pneumococci are easily transmitted from person to person through aerosols and by direct contact. Transmission is particularly likely within families (Hendley et al. 1975, Gray et al. 1980, Lloyd-Evans et al. 1996, Vives et al. 1997, Leino et al. 2001, Givon-Lavi et al. 2002, Hoshino et al. 2002), and under crowded conditions, such as in day care centres (Bogaert et al. 2001) and nursing homes (Nuorti et al. 1998). In the studies of Vives et al. (1997), the nasopharyngeal carriage of S. pneumoniae in the mothers of children colonized with pneumococci was low, but the carriage rates in siblings attending day care were high (39.4%). In the recent study of Bogaert et al. (2001) in Amsterdam, the carriage rates for S. pneumoniae were 58% for children attending day care centres and 37% for control children.
Pneumococci may remain in the nasopharynx for several months (Gratten et al. 1986), and children carrying pneumococci are usually asymptomatic. Pneumococcal carriage is not equally common among adults as among children (Lloyd-Evans et al. 1996). Acquisition of S. pneumoniae is associated with the occurrence of respiratory infection (Gray et al. 1980, Faden et al. 1997, Syrjänen et al. 2001). In the study of Syrjänen et al. (2001), nasopharyngeal aspirates obtained during respiratory infection with or without AOM grew pneumococci almost twice as often as nasopharyngeal swab samples collected when the children where healthy. During pneumococcal AOM, the causative serotype is usually found in the nasopharynx or nasal cavity (Gray et al. 1980, Luotonen 1982).
Components required for adherence and colonization have been determined, but very little is still known about the interaction between pneumococci and the host and the transformation of pneumococcus from a commensal to a pathogen. Pneumococcal disease is more likely to occur soon after the acquisition of a new pneumococcal serotype into the nasopharynx than after long carriage (Gray et al. 1980). This suggests that the host’s immune status and the virulence of a particular strain may determine whether or not pneumococci become invasive (reviewed by AlonsoDeVelasco et al. 1995). A relationship between pneumococcal colonial morphology and nasopharyngeal colonization has been found. The pneumococcal colonial morphology spontaneously and

23
reversibly varies from opaque to semitransparent and transparent. In an infant rat model of nasopharyngeal carriage, only pneumococci with the transparent phenotype were able to establish efficient and stable colonization of the nasopharynx. (Weiser et al. 1994). Transparent variants have also been found to adhere to human lung epithelial cells (Cundell et al. 1995). On the other hand, in a mouse model of sepsis following intraperitoneal inoculation, pneumococci with an opaque colony morphology were found to be significantly more virulent than transparent variants. The increased virulence of opaque pneumococci was associated with increased expression of capsular polysaccharide and decreased expression of teichoic acids compared to transparent variants. However, the details of the molecular mechanism that mediates phase variation and regulates the expression of capsular polysaccharide and teichoic acids are not resolved yet. (Kim & Weiser 1998).
2.1.3 Pneumococcal infections
2.1.3.1 Noninvasive infections
Acute otitis media (AOM) is one of the most common diseases of childhood. The disease usually occurs during the first 5 years of life (Teele et al. 1989). In several studies, S. pneumoniae has been found to be the most common bacterial pathogen causing acute otitis media (Luotonen et al. 1981, Bluestone et al. 1992, Kilpi et al. 2001). In the FinOM Cohort Study, in which the children who participated were 2-24 months of age, pneumococci were cultured in 26% of the AOM events. However, Moraxella catarrhalis and Haemophilus influenzae were almost equally common, as both were isolated in 23% of the events. (Kilpi et al. 2001). In the study of Luotonen et al. (1981), in which bacteriological and antigen detection methods were combined, pneumococcus was found to be involved in nearly 60% of the AOM cases. S. pneumoniae has also been found to cause AOM in adults: in a study of Celin et al. (1991), S. pneumoniae was grown in 21% of the middle ear aspirates obtained from 34 adults with AOM. In the FinOM Cohort Study, the incidence of pneumococcal AOM peaked at the age of 12 months. The most frequent pneumococcal serotypes isolated were 19F, 23F, 6A, 6B and 14. (Kilpi et al. 2001). The types causing pneumococcal disease have been found to be similar to the commonly carried serotypes (Gray et al. 1980, Kilpi et al. 2001, Syrjänen et al. 2001). In the study of Gray et al. (1980), otitis media was found to occur mainly during the winter months and to coincide with a peak in the pneumococcal acquisition rate. A relationship between nasopharyngeal colonization and the development of otitis media in children has also been described elsewhere (Faden et al. 1997, Gates 1999).
S. pneumoniae is also one of the most common bacterial causes of sinusitis and bronchitis (Lindbaek et al. 2001, Pfaller et al. 2001).

24
2.1.3.2 Invasive infections
S. pneumoniae is a common cause of invasive infections, and the incidence of pneumococcal disease is highest in children less than 2 years of age and in adults ≥65 years old (Eskola et al. 1992, Butler & Schuchat 1999). In 1983 - 1992, the annual incidence of invasive pneumococcal infections in an adult Finnish population was found to be 9 per 100000 (Sankilampi et al. 1997). Among children less than five years of age, the annual incidence rate in 1985 - 1989 was 24.2 per 100000 (Eskola et al. 1992). According to Eskola et al. (1992), among Finnish children aged 0 to 5 years, the most common clinical entities were bacteremia without focus (69%), pneumonia (15%) and meningitis (11%). The six most common serotypes or serogroups causing 78% of the invasive infections were 14, 6, 19, 7, 18 and 23 (Eskola et al. 1992). In a study of Hausdorff et al. (2000), the pneumococcal serogroups represented in the seven-valent conjugate vaccine (which includes polysaccharides or oligosaccharides derived from the serotypes 4, 6B, 9V, 14, 18C, 19F and 23F) were found to be responsible for 70-88% of the instances of invasive pneumococcal disease in North America, Europe, Africa and Oceania. In Asia, the serogroups that have been found to cause invasive disease are somewhat different (the five most important serogroups are 1, 19, 6, 5 and 14), as the serogroups represented in the seven-valent vaccine were responsible for only 45% of the invasive pneumococcal diseases (Hausdorff et al. 2000).
In industrialized countries, the diagnosis of pneumonia is based on chest radiographs showing infiltrates (Bartlett & Mundy 1995). However, radiographic changes can usually not be used for the differential diagnosis of bacterial and viral pneumonia (Lehtomäki et al. 1988, Bartlett & Mundy 1995). The etiological diagnosis of pneumonia is complicated, and the reported percentages of pneumococcal pneumonia in different studies are dependent on the methods used for searching the etiological agent. In many cases of pneumonia, the etiological agent remains unidentified. In adults, however, pneumococcus is the most common bacterial cause of community-acquired pneumonia leading to hospitalization (Kalin et al. 1983, Kerttula et al. 1987, Kauppinen et al. 1995). In a study among military conscripts in Finland, in which microbiological, serological and clinical laboratory methods were combined, pneumococcal etiology was definitely established in 30% of the patients. In addition, pneumococcal pneumonia was considered to be probable in 20% of the patients. (Lehtomäki et al. 1988). In studies based on serology, pneumococcus has also been found to be the most common cause of childhood pneumonia, being usually found in 20-40% of the cases in Europe and North America (Korppi et al. 1993, Heiskanen-Kosma et al. 1998, Wubbel et al. 1999, Juvén et al. 2000). In a study of Vuori-Holopainen et al. (2002) using lung aspiration, the etiological diagnosis of childhood pneumonia could be disclosed in 59% of the cases of pneumonia, and S. pneumoniae was detected in 30% of these cases. In studies conducted in developing countries, the bacterial culture of lung aspiration has demonstrated S. pneumoniae in 42% of patients (Shann 1986). Mixed bacterial and viral infections are common among children with pneumonia: in the study of Juvén et al. (2000), mixed bacterial-viral infection was demonstrated in 30% of the patients.
Bacterial meningitis is a serious disease affecting the central nervous system. Since the introduction of Haemophilus influenzae type b conjugate vaccines, pneumococcus is

25
often the main pathogen causing meningitis in infants (Musher 1995). S. pneumoniae is estimated to be the cause of 25-45% of the cases of bacterial meningitis among children in the United States and Europe (Schuchat et al. 1997, Hausdorff et al. 2000). When studying the outcome of bacterial meningitis in developed countries, pneumococcal disease has been shown to be associated with higher rates of death and neurologic sequelae than meningitis caused by H. influenzae or N. meningitidis (Baraff et al. 1993). Pneumococcus is also one of the most common causes of bacteremia (Gransden et al. 1985). In a Finnish study among children in 1985-1989, pneumococcus caused 21% of bacteremias without focus (Saarinen et al. 1995). In adults, most cases of bacteremia are due to pneumonia (Musher 1992).
2.1.4 Prevention of pneumococcal infections
2.1.4.1 Host defence mechanisms
Several non-specific and specific defence mechanisms are essential for host defence against S. pneumoniae. Intact respiratory epithelium, mucosal secretion and enzymes participate in non-specific defence and prevent the invasion of pneumococci at the first line. The specific defence mechanisms include antibodies to pneumococcal surface components. (AlonsoDeVelasco et al. 1995).
Pneumococci are extracellular pathogens, which need to be ingested by phagocytic leukocytes to be killed and removed from the host effectively. Phagocytosis occurs most efficiently when serum opsonins, such as specific antibodies to capsular antigens, complement and CRP, are present. (Reviewed by Obaro et al. 1996b). Once the pneumococci have been ingested and trapped in a phagosome, they are readily killed (AlonsoDeVelasco et al. 1995). Pneumococci are able to activate both the classical and the alternative complement pathways in vitro (Winkelstein 1981).
Protection from pneumococcal disease is thought to be mediated mainly by serotype-specific antibodies to capsular antigens (Musher et al. 1986, Gillespie 1989, Bruyn 1992, AlonsoDeVelasco et al. 1995). In the absence of specific antibodies, the clearance of pneumococci may be facilitated by complement activation mediated by CRP or lectins, which are proteins found on liver and spleen macrophages (Ofek & Sharon 1988, Gillespie 1989). Blood-borne pneumococci can be removed effectively by splenic macrophages without opsonising capsular antibodies. This is seen in asplenic patients, who have an increased susceptibility to S. pneumoniae, even though blood-borne pneumococci can also be removed by other cells of the reticuloendothelial system. (Reviewed by Obaro et al. 1996b).

26
2.1.4.2 Vaccines
The first attempts to prevent pneumococcal infection by vaccination were made by Wright and his colleagues in 1911, before the diversity of capsular types was appreciated. They investigated the potential of a vaccine consisting of whole killed pneumococci to prevent pneumococcal pneumonia among South African gold miners. However, these trials did not unequivocally establish the efficacy of vaccination. (Reviewed by Austrian 1977). In the early 1930s, the effect of immunization with a polyvalent pneumococcal vaccine containing killed pneumococci was studied, but the discovery of the immunogenicity of pneumococcal polysaccharides in man by Francis and Tillett led to investigations of the potential of partially purified capsular material as a means of preventing pneumonia. In 1945, it was clearly demonstrated that pneumococcal pneumonia could be prevented by immunization with specific capsular polysaccharides. The vaccine used was tetravalent, containing polysaccharides of the pneumococcal serotypes 1, 2, 5 and 7, and it was shown to be 86 % effective in preventing pneumonia due to vaccine-related types in a military population. Two hexavalent pneumococcal polysaccharide vaccines became commercially available in the late 1940s, but were drawn off the market in the early 1950s already, by which time the introduction of penicillin and other antibiotics had changed the treatment of bacterial infections completely. (Reviewed by Austrian 1981, Bruyn & van Furth 1991). The interest to develop pneumococcal vaccines also diminished, until it was shown that, despite the antibiotics, pneumococci continued to cause serious infections with a high mortality rate (Austrian & Gold 1964). Based on studies where the pneumococcal types most often responsible for bacteremic infections in man were identified, different polyvalent vaccines containing six or twelve to fourteen capsular polysaccharides were developed. The polyvalent pneumococcal capsular polysaccharide vaccines were shown to be safe and antigenic. In trials conducted in South Africa with a 13-valent vaccine, the efficacy was at least 78.5 % in preventing type-specific putative pneumococcal pneumonia and 82.3 % in preventing bacteremic infections caused by vaccine-related pneumococci. (Austrian et al. 1976). As a result, a polyvalent vaccine composed of 14 pneumococcal polysaccharides (1, 2, 3, 4, 6A, 7F, 8, 9N, 12F, 14, 18C, 19F, 23F and 25) was licensed in the USA in 1977 (reviewed by Watson et al. 1993).
In 1983, a 23-valent vaccine replaced the 14-valent vaccine (Robbins et al. 1983). This vaccine includes purified capsular polysaccharide antigens of the pneumococcal serotypes 1, 2, 3, 4, 5, 6B, 7F, 8, 9N, 9V, 10A, 11A, 12F, 14, 15B, 17F, 18C, 19A, 20, 22F, 23F and 33F (Pneumovax®, Aventis-Pasteur MSD, France). The vaccine has been shown to be safe and efficacious in preventing severe pneumococcal disease, its efficacy ranging from 55 % to 65 % (Shapiro et al. 1991). The distribution of S. pneumoniae serotypes varies geographically and over time, which affects the coverage of the vaccine in regard to the disease-causing serotypes. The current 23-valent vaccine covers approximately 85 – 95 % of the disease-causing serotypes in Europe and the United States (Robbins et al. 1983, Parkinson et al. 1994, Hedlund et al. 1995, Sankilampi et al. 1997), but less than 80% in parts of Asia (Lee et al. 1991). Not all vaccinees, however, respond to polysaccharide vaccines: the efficacy of vaccines is much lower in the elderly, in patients with immunodeficiency and hematologic malignancy and, particularly, in

27
young children (reviewed by Bruyn & van Furth 1991). In a recent retrospective study of older adults (≥65 years of age), the pneumococcal polysaccharide vaccine was shown to be effective in preventing bacteremia, but not nonbacteremic pneumonia (Jackson et al. 2003). This has also been seen in other studies (Örtqvist et al. 1998, Honkanen et al. 1999).
The capsular polysaccharide is a T cell-independent antigen, and mature B-lymphocytes are required for a T cell-independent antibody-mediated immune response. Infants do not possess mature B lymphocytes, and many of the polysaccharides included in the 23-valent pneumococcal polysaccharide vaccine are therefore poorly immunogenic in infants and young children. The polysaccharide vaccine has thus not been recommended for children under 2 years of age. Moreover, the polysaccharide vaccine does not reduce mucosal carriage of pneumococcus, and hence fails to protect against mucosal pneumococcal infections or to prevent the spread of pneumococcal strains resistant to antimicrobial drugs. Efforts have therefore been made to develop a pneumococcal vaccine that would be effective in infants and children. The T cell-dependent antibody response appears soon after birth, and by conjugating a protein carrier to the polysaccharide antigen, the immune response can be shifted to be T cell-dependent. T helper cells stimulate polysaccharide-specific B cells to mature into plasma cells, which then produce antibodies, or to develop into memory cells. (Eskola & Anttila 1999). This technique was successfully used with a Haemophilus influenzae type b conjugate vaccine (Eskola et al. 1985), and pneumococcal conjugate vaccines have subsequently been developed by coupling purified capsular polysaccharides with different carrier proteins. The different carrier proteins tested in clinical studies include a meningococcal outer membrane protein complex (PncOMPC conjugate vaccine), a CRM197 protein (a nontoxic mutant of diphtheria toxin) (PncCRM), a diphtheria toxoid (PncD) or tetanus toxoid (PncT) and a mixture with either of these toxoids (PncTD) (Eskola & Anttila 1999). The trials showed that pneumococcal conjugate vaccines were highly immunogenic in human infants and induced immunological memory (Åhman et al. 1996, Rennels et al. 1998, Åhman et al. 1998).
In 2000, a heptavalent pneumococcal conjugate vaccine (PncCRM197, available as Prevenar® or Prevnar®, Wyeth Lederle Vaccines, USA) was licensed in the USA. The serotypes included in this vaccine (4, 6B, 9V, 14, 18C, 19F and 23F) have been shown to cause 80 % of invasive pneumococcal disease in young children in the United States, and the vaccine has been shown to be highly effective (efficacy over 97 %) in preventing invasive pneumococcal disease in young children (Black et al. 2000). The pneumococcal conjugate vaccine is recommended by the American Academy of Pediatrics committee on infectious diseases (2000) for routine use in infants to prevent invasive pneumococcal disease. The conjugate vaccine may also prevent invasive disease in adults, as shown by Whitney et al. (2003). However, Whitney et al. (2003) point out that the reduction in disease burden seen among adults may be due to decreased transmission of pneumococci from children. The heptavalent conjugate vaccine has also been shown to be more immunogenic in infection-prone subjects who do not respond to the pneumococcal polysaccharide vaccine compared to the polysaccharide vaccine (Zielen et al. 2000). In the Finnish Otitis Media (FinOM) Vaccine Trial, in which the efficacy of the PncCRM197 vaccine against AOM was studied, the heptavalent conjugate vaccine reduced the number of AOM episodes due to the serotypes contained in the vaccine by 57%. However, the

28
overall reduction of AOM episodes was only 6%. (Eskola et al. 2001). In the Kaiser Permanente study, the pneumococcal conjugate vaccine was found to provide moderate protection against ear infections (otitis visits reduced by 7.8%). Frequent otitis media and tympanostomy tube placements were also reduced by 10-26% and 24%, respectively. (Fireman et al. 2003).
Initial studies in Israel showed that vaccination with a pneumococcal conjugate vaccine significantly reduced nasopharyngeal carriage of vaccine serotypes (Dagan et al. 1996). In an earlier study with the 14-valent pneumococcal polysaccharide vaccine, a slightly lowered carriage rate of the pneumococcal serotypes present in the vaccine had also been observed (Herva et al. 1980). However, in the Gambia, immunization with a pentavalent pneumococcal conjugate vaccine reduced the carriage of the vaccine-related serotypes, but increased the carriage of non-vaccine serotypes in the children who had recieved the vaccine (77%) compared to controls (43%) (Obaro et al. 1996a). Later, the significantly increased carriage of non-vaccine serotypes was also demonstrated in an Israeli study (Dagan et al. 1999). In the FinOM Trial, AOM episodes due to non-vaccine and non-cross-reactive serotypes increased by 33% (Eskola et al. 2001). The reduction in the carriage of S. pneumoniae and antibiotic-resistant S. pneumoniae of the vaccine serotypes may reduce the spread of the serotypes most commonly associated with pneumococcal disease and antibiotic resistance. On the other hand, in the future, increased pneumococcal disease may be associated with non-vaccine serotypes. It also remains to be seen if antibiotic resistance will spread to the non-vaccine serotypes (Dagan & Fraser 2000, Klugman 2001).
2.1.5 Diagnosis of pneumococcal infection
The first methods by which pneumococcal infections were diagnosed were culture, animal testing and Gram’s stain. The pneumococcus was, in fact, one of the first pathogens observed during the development of Gram’s stain in the 1880s. (Reviewed by Austrian 1981, Watson et al. 1993). Gram’s staining of sputum specimens is an inexpensive and rapid method that is still in use when determining the bacterial cause of pneumonia (Glaister 1991), but the gold standard for diagnosing pneumococcal infections has been and still is bacterial culture. However, if antibiotic treatment has been initiated before the samples for culture are taken, the viability of the bacteria is reduced, which may result in negative culture findings. In these cases, pneumococcal antigens can be searched for in body fluids. In research settings, and when culture and antigen detection fails, antibody assays and assays measuring circulating immune complexes (ICs) have also been used. Despite extensive recent studies, pneumococcal nucleic acid amplification methods have not been standardized yet.

29
2.1.5.1 Culture
Isolation of pneumococci from normally sterile body sites, such as cerebrospinal fluid (CSF) or blood, is considered to be a specific indicator of pneumococcal infection. Bacterial culture is an inexpensive method, which also provides bacterial strains for further studies, such as testing of sensitivity to antimicrobials and molecular epidemiologic studies. Blood culture continues to be the most reliable and specific method for the diagnosis of pneumococcal pneumonia, but the sensitivity of the method is very low. In adults, blood culture is positive in only 10 to 45% of pneumococcal pneumonias (Macfarlane et al. 1982, Kalin & Lindberg 1983, Lehtomäki et al. 1988). In children, the proportion of blood culture-positive pneumococcal pneumonias is less than 10% (Korppi et al. 1993, Clements & Stephenson 1996, Juvén et al. 2000). Larger sample volumes have been shown to improve the results of blood culture (Isaacman et al. 1996). A 10-30 ml sample volume has been recommended for adults and a 1-5 ml sample volume for children (Campos 1989, Weinstein 1996).
For the diagnosis of pneumococcal pneumonia, pneumococci can also be cultured from respiratory samples, such as sputum (Drew 1977, Kalin et al. 1983, Lehtomäki et al. 1988). Sputum culture is a noninvasive method, but it must be performed before the initiation of antimicrobial treatment (Kalin et al. 1983), and it can usually be used in adults only, as young children do not produce sputum. Sputum samples are easily contaminated with bacteria present in the upper respiratory tract, and when culturing sputum, Gram’s stain of the sample should also be performed. In Gram’s stain, the purulence and the degree of contamination can be determined by studying the ratio of leukocytes to squamous epithelial cells. Samples containing ≥5 leukocytes per squamous epithelial cells are considered purulent and can be used for the etiological diagnosis of pneumococcal infection (Kalin & Lindberg 1983, Lehtomäki et al. 1988, Plouffe et al. 1998, Salo & Leinonen 1999). Culture of lung aspirates obtained by lung puncture, transtracheal aspiration or bronchoalveolar lavage could give more reliable results than sputum culture, but these procedures are invasive and may cause complications (Finland 1969, Hughes et al. 1969). Thus, these methods should be used only selectively with severely ill patients. In these cases, they can provide life-saving information (Vuori-Holopainen & Peltola 2001).
In the etiological diagnosis of noninvasive pneumococcal infections, such as otitis media, culture is the most commonly used method. However, when culturing middle ear fluid samples, a large proportion of the specimens remain negative (Luotonen et al. 1981, Kilpi et al. 2001). The culture of nasopharyngeal swab specimens in the diagnosis of respiratory tract infections is complicated by the presence of asymptomatic pneumococcal carriage. The quantification of nasopharyngeal bacteria has been proposed to be of clinical diagnostic value (Söderström et al. 1990).
When studying the nasopharyngeal carriage of S. pneumoniae, nasopharyngeal aspirates have been found to be optimal samples. However, when nasopharyngeal aspirate is not available, it can be replaced by nasopharyngeal swabs for the detection of pneumococcal carriage. (Rapola et al. 1997). Recently, guidelines for the detection of upper respiratory carriage of pneumococcus were published by a WHO working group (O'Brien & Nohynek 2003). The use of a medium containing skim milk, tryptone,

30
glucose and glycerin (STGG) (Gibson & Khoury 1986) in the transport and storage of nasopharyngeal secretions has been recommended because of its ability to preserve pneumococci in short and long term when stored at low temperatures (O'Brien et al. 2001).
Pneumococci are cultured on blood agar and typically grow as round, flat, smooth, translucent colonies with depressions in their centres. The colonies are typically surrounded by narrow zones of α-haemolysis. Capsular polysaccharides often contribute to the mucoidal appearance of these colonies. Nonencapsulated mutant strains that form rough colonies are rarely seen. (Lund & Henrichsen 1978). Pneumococci are differentiated from other α-haemolytic streptococcal species by their sensitivity to optochin (Lund & Henrichsen 1978), bile solubility (Howden 1979, Murray 1979) and capsular reaction with diagnostic pneumococcal sera (Henrichsen 1999). Optochin sensitivity is the most important identification criterion, and it is commonly used in clinical laboratories. However, atypical optochin-resistant pneumococci have also been isolated (Munoz et al. 1990), which has made the definite identification of pneumococci more difficult. A specific nucleic acid probe (AccuProbe®, GEN-PROBE, San Diego, CA) is often used to confirm atypical pneumococci in clinical laboratories. The confirmation of suspected pneumococcal isolates could also be done by demonstrating the presence of a pneumococcal capsule. The most reliable method to demonstrate the presence of a capsule in pneumococcus is the quellung reaction, also known as the capsular reaction test. In the quellung reaction, all capsulated pneumococci can be detected by using a pooled polyvalent antiserum (omniserum). The capsular type or group of the pneumococcal strain can thereafter be determined by using type- or group-specific antisera. (Henrichsen 1999). The quellung reaction gives reliable results of the capsular type of the pneumococcal strain, but it requires experienced personnel to perform it. Other methods for serotyping pneumococcal isolates have also been described, including counterimmunoelectrophoresis (CIEP), coagglutination (COA), latex agglutination (LA), dot blot assay and PCR (Leinonen 1980, Trollfors et al. 1983, Fenoll et al. 1997, Brito et al. 2003, Lawrence et al. 2003).
2.1.5.2 Antigen detection
Antigen detection techniques have been developed as alternatives to pneumococcal culture. The antigens most commonly searched for are the pneumococcal capsular polysaccharides present in sputum (Kalin & Lindberg 1983, Boersma et al. 1991), urine (Macfarlane et al. 1982, Ramsey et al. 1986, Bromberg et al. 1990, Scott et al. 1999), pleural fluid (Macfarlane et al. 1982, Boersma et al. 1993), serum (Ramsey et al. 1986), CSF (Singhal et al. 1996) and middle ear fluid (Leinonen 1980). Pneumococcal C-polysaccharide has been detected in sputum (Holmberg et al. 1985, Krook et al. 1987, Parkinson et al. 1992), CSF (Yolken et al. 1984, Marcos et al. 2001) and urine (Bromberg et al. 1990, Adegbola et al. 2001, Domínguez et al. 2001, Dowell et al. 2001, Marcos et al. 2001, Murdoch et al. 2001, Michelow et al. 2002). The techniques used for the

31
detection of pneumococcal antigens include CIEP, COA, LA, enzyme immunoassay (EIA), radioimmunoassay and immunochromatographic membrane test (ICT).
Detection of pneumococcal antigens in sputum has been shown to be a sensitive indicator of pneumococcal infection. In the study of Boersma et al. (1991), the sensitivity of detecting capsular antigens in patients with community-acquired pneumonia was as high as 94%. Antigens can also be detected after the initiation of antimicrobial therapy (Kalin & Lindberg 1983, Boersma et al. 1991, Holloway et al. 1993a, Scott et al. 1999). The study by Kalin & Lindberg (1983) on patients with acute community-acquired pneumonia showed that, after the initiation of antimicrobial therapy, the detection of pneumococcal capsular polysaccharides from sputum by CIE (56% positive) was a more effective method to demonstrate pneumococcus than bacterial culture from blood (6%), nasopharynx (18%) or sputum (13%). The reliability of antigen detection from sputum is, however, limited by the fact that healthy carriers of pneumococci exist.
Antigen detection from urine during pneumococcal pneumonia has been shown to be sensitive, but its specificity has varied (Domínguez et al. 2001, Michelow et al. 2002). In the study of Domínguez et al. (2001) on patients with bacteremic and non-bacteremic pneumonia, the specificity of the ICT test, which is a new rapid test (15 min) for the demonstration of pneumococcal antigen in urine samples, was found to be as high as 97.2%. The test detected pneumococcal antigen in 80% of patients with pneumococcal pneumonia, the sensitivity being similar in both bacteremic (82%) and non-bacteremic (78%) cases (Domínguez et al. 2001). Pneumococcal antigen detection in CSF and urine of patients with suspected bacterial meningitis has also been found to be sensitive and specific in addition to being more rapid than the conventional diagnostic methods (Marcos et al. 2001). Pneumococcal carriage (Adegbola et al. 2001, Dowell et al. 2001) or infections at sites other than the lungs may cause positive findings in urine (Ramsey et al. 1986).
2.1.5.3 Nucleic acid amplification
The development of polymerase chain reaction (PCR) (Mullis & Faloona 1987) has made it is possible to detect even small amounts of DNA by amplifying a defined sequence more than 106-fold (Saiki et al. 1988). PCR is thus also able to rapidly detect small amounts of pathogens present in clinical samples and to improve the diagnosis of infectious diseases. Since PCR does not depend on the presence of viable, culturable organisms, it may also be used in cases where antimicrobial therapy has been initiated. Several PCR-based assays for detecting S. pneumoniae in clinical samples have been developed, but these methods are usually only used in research settings and not in routine diagnosis of pneumococcus. The PCR methods for detecting pneumococcal DNA are often based on amplification of fragments of the well-conserved pneumolysin or autolysin-encoding genes (Rudolph et al. 1993, Gillespie et al. 1994, Salo et al. 1995). Methods based on the amplification of the penicillin-binding protein 2B-encoding gene (Ubukata et al. 1996, du Plessis et al. 1998), the PsaA-encoding gene (Morrison et al. 2000) and ribosomal RNA genes (Hendolin et al. 1997, Lu et al. 2000, Rantakokko-

32
Jalava et al. 2000, Nikkari et al. 2002) have also been developed. The advantage of broad-range bacterial PCR assays combined with DNA sequencing is that they allow the detection of several other pathogens apart from pneumococci (Kotilainen et al. 1998, Nikkari et al. 2002). PCR methods have been used to detect pneumococcal DNA in whole blood (Zhang et al. 1995, Isaacman et al. 1998) and different fractions of the blood (Dagan et al. 1998, Toikka et al. 1999), blood cultures (Hassan-King et al. 1994), CSF (Cherian et al. 1998, du Plessis et al. 1998, Bäckman et al. 1999), pleural fluid (Falguera et al. 2002, Nikkari et al. 2002), sputum (Gillespie et al. 1994, Lu et al. 2000), lung aspirates (Ruiz-Gonzalez et al. 1997, García et al. 1999, Vuori-Holopainen et al. 2002), urine (Murdoch et al. 2003) and middle ear fluid (Virolainen et al. 1994). In the study of Rudolph et al. (1993), where buffy coat samples of patients with culture-confirmed pneumococcal pneumonia were used, both autolysin and pneumolysin gene-targeted primers were used, and the sensitivities of the nested PCR methods were 75% for pneumolysin primers and 63% for aurolysin primers. However, when whole blood samples were used, the sensitivities were below 40% for both primers (Rudolph et al. 1993). In the study of Salo et al. (1995), serum samples were used and all samples from patients with culture-confirmed pneumonia were positive by the nested PCR method amplifying a fragment of the pneumolysin-encoding gene. In the study of Murdoch et al. (2003), a nested PCR assay targeting the pneumolysin-encoding gene was not found to improve the diagnosis of community-acquired pneumonia caused by S. pneumoniae. The use of whole blood samples or fractions of blood constitutes a problem in PCR, as blood has been found to contain several inhibitors of PCR that are difficult to remove (de Franchis et al. 1988, Abu Al-Soud et al. 2000, Abu Al-Soud & Rådström 2001). Also, the low density of microbial DNA compared to human DNA may cause false negative findings in PCR. However, when the PCR method described by Salo et al. (1995) was used for the detection of pneumococcal bacteremia in mice, the assay was found to be capable of detecting small numbers of bacteria in early-phase bacteremia (Salo et al. 1999). Furthermore, the whole blood fraction seemed to be a better specimen type for PCR than buffy coat or serum.
When a pneumolysin gene-targeting PCR method was used for the detection of pneumococcus in middle ear fluid samples of children with acute otitis media, 91% of the culture-positive samples were positive by PCR (Virolainen et al. 1994). However, the use of PCR increased the amount of positive samples from 18% by culture alone to 30% by culture and PCR. There is evidence that the DNA seen in culture-negative middle ear effusions comes from viable bacteria (Post et al. 1996, Dingman et al. 1998, Rayner et al. 1998). However, it was recently shown that organisms allied to Streptococcus mitis may harbour S. pneumoniae virulence factor-encoding genes and may thus cause false-positive findings in a PCR analysis based on the amplification of fragments of these genes (Whatmore et al. 2000). In the study of Kaijalainen et al. (2002), PCR did not reliably help in the identification of atypical pneumococci, giving partly controversial results compared to a commercial RNA hybridisation test (AccuProbe®). Kearns et al. (2000) have also reported detection of atypical isolates of pneumococci by PCR.
In addition to the PCR methods used to detect pneumococci, PCR assays for the determination of penicillin-resistant pneumococci have been developed. These methods are based on amplification of selected fragments of the genes encoding the pneumococcal

33
penicillin-binding proteins 1A, 2B and 2X (Ubukata et al. 1996, Gillespie et al. 1997, du Plessis et al. 1998, du Plessis et al. 1999).
Two PCR methods for serotyping pneumococci were recently published (Brito et al. 2003, Lawrence et al. 2003). Lawrence et al. (2003) used primers specific for five serotypes (1, 3, 14, 19F and 23F) and three serogroups (6, 19, and 23) in three multiplex PCRs. They used the method to test 93 clinical isolates, of which all the 32 isolates with serotypes among the five serotypes covered by the PCR assay were correctly detected. The serotypes 6A, 6B, 19F and 23F isolates were also correctly assigned to the serogroups 6, 19 and 23, respectively. (Lawrence et al. 2003). Previously, Lawrence et al. (2000) described a PCR method for pneumococcal serotype prediction based on polymorphism detection in the cpsA-cpsB genes. However, these genes do not determine serotype, and although a strong linkage between the cpsA-cpsB polymorphism was found, the method was not absolute (Lawrence et al. 2000). The serotyping method described by Brito et al. (2003) included primers specific for the serotypes 1, 3, 4, 14, 9F, 19A and 23F and the serogroups 6 and 18, combined with seven multiplex PCRs. The primers initially designed for the serotypes 6B and 18C were not able to distinguish between the different serotypes of the same serogroups and were thus serogroup-specific. When 446 pneumococcal isolates were analysed using the method, results concordant with the conventional serotyping technique were obtained. (Brito et al. 2003).
2.1.5.4 Serology
Antibody assays are generally used to demonstrate infections caused by viruses and atypical bacteria, but no sensitive assays for the demonstration of an antibody response to pneumococci are in routine use. The serum response to pneumococcal capsular polysaccharides can be detected around the seventh day during pneumococcal pneumonia in children (Nohynek et al. 1995), and antibody measurements are thus of no major importance for the choice of antimicrobial therapy. In vaccine trials and epidemiological settings, antibody assays could provide a confirmatory method when other assays remain negative. The antibody assays that have been used have measured antibodies against antigens such as type-specific capsular polysaccharides (Russell et al. 1980, Gray et al. 1981, Pedersen & Henrichsen 1982, Kalin & Lindberg 1985, Gray & Dillon 1988, Korppi et al. 1992, Soininen 2001, Soininen et al. 2001), C-polysaccharide (Korppi et al. 1992), pneumolysin (Kalin et al. 1987, Korppi et al. 1992, Nohynek et al. 1995) and pneumococcal surface protein A (Virolainen et al. 2000).
The detection of pneumococcus-specific ICs could be a more specific method than the detection of antibodies, since ICs can be formed only when antigens and antibodies are present in the circulation in optimal concentrations. Thus, this method could be less prone to yielding false-positive results for healthy persons carrying pneumococci. Pneumococcal antibodies in circulating ICs have been demonstrated in several studies (Mellencamp et al. 1987, Leinonen et al. 1990, Holloway et al. 1993b, Korppi & Leinonen 1998, Lankinen et al. 1999). The sensitivity and specificity of the IC assay in the study of Leinonen et al. (1990) on patients with community-acquired pneumonia

34
were 97.8% and 83.4%, respectively. However, the isolation of ICs is difficult, and the methods are not in general use (Leinonen & Mäkelä 2001).
2.2 Real-time PCR
Real-time PCR is a modification of traditional PCR and was first described in the late 1990s. In real-time PCR, the amplification and detection of amplification products occur simultaneously. A microvolume fluorometer is integrated with the termal cycler, thus enabling the detection of amplification products. (Wittwer et al. 1997). Several real-time PCR instruments are currently available, of which the LightCycler (Roche Diagnostics GmbH, Mannheim Germany) and ABI PRISM 7700 sequence detection system (PE Biosystems, Foster City, CA, USA) have been used in most studies published to date. The amplified DNA may be detected using a double-stranded DNA (dsDNA)-binding dye, fluorescent-labelled primers or sequence-specific hybridisation probes. The hybridisation probes available are fluorescence resonance energy transfer (FRET) probes, TaqMan hydrolysis probes, molecular beacons and Scorpion probes. Additionally, there is the Amplifluor Universal Detection System and LUX (light upon extension) primers for the detection of real-time PCR amplification products. (Reviewed by Gloffke 2003).
Double-stranded DNA-specific dyes detect all dsDNA, including undesired products, such as primer dimers. However, when using the dsDNA-specific dye SYBR Green I and measuring the fluorescence continuously through a temperature cycle, the denaturation of product can be seen and DNA melting curves can be plotted. These melting curves can be used for distinguishing amplification products separated by less than 2°C in melting temperature. (Ririe et al. 1997).
In the FRET system, a molecule close to the fluorophore accepts the energy released by the fluorophore after it has been excited. If the acceptor molecule is also a fluorophore, the fluroescence released by it can be measured. The acceptor molecule can also be a quencher molecule that silences the reporter molecule and releases the energy as heat or vibrational energy. In the method developed by Idaho Technology and used in the LightCycler applications, the sequence-specific probes bind adjacent to each other during the annealing step of PCR. One of the probes is labelled at the 3’ end with fluorescein and the other at the 5’ end with Red640 or Red705. The fluorescence of the Red640 or Red705 molecule or both in multiplex applications is then measured after excitation of the fluorescein molecule. (Gloffke 2003).
The TaqMan procedure (Applied Biosystems) utilizes the 5´-3´ exonuclease activity of the Taq polymerase. The TaqMan probe contains a fluorophore at the 5´ end and a quencher, which keeps the molecule non-fluorescent, at the 3´ end. The probe binds to the template DNA sequence. When the polymerase encounters the probe, it removes it nucleotide by nucleotide. Thus, when the fluorophore is released into the solution, it is able to fluoresce. (Gloffke 2003).
The molecular beacon is a hairpin molecule, consisting of a sequence-specific region in the loop and complementary sequences that form the hairpin. The fluorescent dye is at one end of the molecule and the quencher at the other. In solution, the molecule is in the

35
hairpin format, but when the molecule binds the target DNA, it unfolds and frees the fluorophore from the quencher. The Scorpio probes use a stem-loop system. The probes contain a fluorophore at the 5’ end, then a stem-loop structure, a quencher, a PCR blocker preventing read-through by DNA polymerase, and finally the primer at the 3’ end. The specific probe sequence folds back on itself during annealing and binds its complement within the same DNA strand. This opens up the hairpin loop separating the flurophore and the quencher. In duplex Scorpions, the fluorophore-coupled detection segment and the quencher-coupled fragment are on separate, complementary molecules. The Amplifluor Universal detection system also uses a paired flurophore-quencher hairpin structure. An allele-specific tail is incorporated into the 5’ end of the amplicon during the first two cycles of PCR. In the subsequent cycles, UniPrimers that anneal to this new tail system are used. The UniPrimers contain a stem-loop structure at the 5’ end, and when the reverse strand is extended through the UniPrimer sequence, the hairpin opens, enabling fluorescence. The LUX primers are like hairpin probes: they have a stem-loop structure in solution. They do not contain a quencher molecule, but are designed to self-quench based on the sequence context. When they are incorporated into a double-stranded PCR product, the fluorophore is dequenched and emits light strongly. (Gloffke 2003).
The monitoring of PCR product accumulation provides a possibility to perform an absolute or relative quantitative analysis of DNA in the samples studied by using external or internal standards. However, the accuracy of quantification with external standards is dependent on the standards used. (Rasmussen 2001). Since the introduction of real-time PCR, a large number of applications for detecting different microbes have been published (Lee et al. 1999, Schalasta & Schmid 1999, Klaschik et al. 2002, Kuoppa et al. 2002, Reischl et al. 2002, Sloan et al. 2002, Jebbink et al. 2003). Real-time PCR has also been used to determine the penicillin susceptibility of bacteria (Gibson et al. 1999, Kearns et al. 2002). In addition to quantitation, real-time PCR offers a possibility for genotyping and gene mutation detection by analysing the melting curves of amplification products (Bernard et al. 1999, Mangasser-Stephan et al. 1999, Pals et al. 1999).
Sample preparation is one of the most important steps when performing quantitative PCR. The presence of inhibiting substances in the sample may lead to a complete absence of amplification products or have a quantitative effect. (Rasmussen 2001).
2.2.1 Applications
2.2.1.1 Detection of S. pneumoniae
Methods for the detection of pneumococcus using real-time PCR have recently been described (Table 1). Kearns et al. (1999) used real-time PCR for the detection of pneumococcal DNA in 12 CSF specimens. They found that all culture-positive specimens were detected by real-time PCR, and additionally, 2 culture-negative specimens with a positive result in LA assay were detected as positive by real-time PCR. Furthermore, 3

36
samples with negative culture and LA results were positive by real-time PCR. The method of Kearns et al. was targeted to the pneumolysin gene and based on fluorescence resonance energy transfer, although the forward primer was labelled with the acceptor molecule cyanine 5. They reported a sensitivity of the assay of 15 CFUs. (Kearns et al. 1999).
In the study of Corless et al. (2001), S. pneumoniae was simultaneously detected with N. meningitidis and H. influenzae in suspected cases of meningitis and septicemia. When analysing clinical samples (CSF, serum, plasma and whole blood) from culture-confirmed cases, the sensitivity of the assay for pneumococcus was 91.8%. The assay also identified 46 previously undetected cases of pneumococcal disease in an analysis of 4113 culture-negative samples. The data of the study of Corless et al. (2001) suggested that 1% of all meningitis cases were due to more than one pathogen. Traditional laboratory methods, such as bacterial culture, may not always detect multiple pathogens in a sample, which is why organisms other than the predominating pathogen may be underdetected.
In the study of Greiner et al. (2001), pneumococci were detected in nasopharyngeal secretions. The assay used primers specific for the pneumolysin gene and a TaqMan probe. The assay detected DNA in mixtures in which the quantity of DNA was from 1 to 106 cells. The sensitivity and specificity of the assay compared to bacterial culture were 100% and 96%, respectively. When tested for specificity for other alpha-hemolytic streptococci, some amplifications of Streptococcus sanguis strains were observed. (Greiner et al. 2001).
In the study of McAvin et al. (2001), primers amplifying a fragment of the autolysin-encoding gene were used. Also, this assay utilized a TaqMan probe, but it was performed on the LightCycler. The method was evaluated using 70 clinical pneumococcal isolates and 26 negative control clinical isolates, and it detected all isolates correctly. (McAvin et al. 2001).
Table 1. Real-time PCR assays for detecting S. pneumoniae.
Study Group Real-time PCR
instrument
Target gene
Detection format
Specimen type n (culture-pos. + culture-neg.)
Sensitivitya
Kearns et al. 1999
LightCycler ply FRETb probes CSFc 3 + 9 100%
Corless et al. 2001
ABI PRISM 7700
ply TaqMan probe CSFc, plasma, serum, whole
blood
36 + 4113 91.8%
Greiner et al. 2001
ABI PRISM 7700
ply TaqMan probe nasopharyngeal secretion
25 + 170 100%
McAvin et al. 2001
LightCycler lytA TaqMan probe clinical isolates 70 + 26 100%
asensitivity compared to culture, bfluorescence resonance energy transfer, ccerebrospinal fluid

3 Aims of the study
The overall aim of this work was to develop sensitive PCR methods for the detection and quantification of S. pneumoniae and to study the applicability of the methods for detecting pneumococci in clinical samples and in carriers. The specific aims were:
1. to improve the specificity of a previously developed conventional pneumolysin-PCR method by the use of a Europium-labelled hybridisation probe and TRF measurement for the detection of amplification products
2. to develop a real-time PCR method for detecting and quantifying pneumococcal DNA and to study the applicability of the method to MEF samples
3. to investigate the presence of pneumococcal DNA in MEF samples of children with AOM
4. to compare real-time PCR findings in nasopharyngeal swab specimens of healthy children to pneumococcal culture findings
5. to compare the sensitivities of bacterial culture and real-time PCR
6. to study the effects of different DNA extraction methods on the quantification result obtained by real-time PCR

4 Materials and Methods
4.1 Subjects and specimens
The MEF specimens analysed in the studies I, II and V were collected as part of the FinOM studies. The FinOM studies, consisting of the FinOM Cohort Study and the FinOM Vaccine Trial, were conducted in the Tampere region in 1994 to 1997 and in December 1995 to March 1999, respectively. The purpose of the FinOM Cohort Study was to give background data about AOM among Finnish children (Kilpi et al. 2001). In the Cohort Study, 329 children were enrolled and no intervention was given. The FinOM Vaccine Trial evaluated the efficacy of two pneumococcal conjugate vaccines against AOM (Eskola et al. 2001). During the enrolment period, 55% of the total birth cohort in the study area were included in the trial. One third of the children (N = 831) were randomized to receive the HBV vaccine and two thirds either of the two experimental pneumococcal conjugate vaccines. The study protocol of the FinOM vaccine trial was evaluated before the start of the trial by the ethics committee of the National Public Health Institute of Finland, by the National Agency for Medicines, and by the ethics committee and the health board of Tampere and the health boards of Kangasala and Nokia. Informed consent was obtained from the parents or guardians of the children. In study I, 50 MEF samples from the FinOM Cohort study were used in the evaluation of the microwell hybridisation method (Table 2). The real-time PCR method in study II was evaluated by analysing 50 consecutive MEF samples from children participating in the FinOM Vaccine Trial (Table 2). The samples were both from the control group and from the vaccine groups, and some of the samples were taken from the same children. In study V, control subjects in the FinOM Vaccine Trial randomized to receive Hepatitis B virus vaccine were studied. Altogether 2595 MEF samples from 1819 AOM events of 573 children were analysed (Table 2). Additionally, data from the FinOM Cohort Study were used to analyse the relationship between pneumococcal nasopharyngeal carriage and the presence of pneumococcal DNA by PCR in MEF during AOM. In study V, all MEF samples from the FinOM Vaccine Trial were analysed as described later. However, only part of the MEF samples from the FinOM Cohort Study were fully analysed and thus available for subsequent analyses. In study V, the FinOM Vaccine Trial results are

39
presented unless mentioned otherwise. Only descriptive analyses are presented to avoid statistical problems related to the dependence between the data obtained from multiple samples and events from individual children during the follow-up. The results of study V are also mainly presented based on data on individual ears, since the samples from each ear were processed individually. Some data are presented as events, with data on both ears combined.
The nasopharyngeal specimens analysed in the studies III and IV were originally collected as part of the study of Ukkonen et al. (2000), in which the prophylactic effect of an antiadhesive oligosaccharide (NE-1530) on nasopharyngeal carriage of bacteria and on acute otitis media was studied. The ethical permission for the earlier study also covers the ethical permissions for the studies III and IV. The samples used in the studies III and IV were collected in 1999 between January and April from healthy children aged 10 to 24 months. In study III, where three DNA extraction methods were compared, 50 consecutive nasopharyngeal secretions were analysed. In study IV, 400 consecutive nasopharyngeal secretions were tested by real-time PCR (Table 2).
Table 2. Specimens analysed in studies I-V.
Specimens Study N Type
Reference
I 50 middle ear fluid FinOM Cohort Study (Kilpi et al. 2001) II 50 middle ear fluid FinOM Vaccine Trial (Eskola et al. 2001) III 50 Nasopharyngeal swab Ukkonen et al. 2000 IV 400 Nasopharyngeal swab Ukkonen et al. 2000 V 2595 middle ear fluid FinOM Vaccine Trial (Eskola et al. 2001)
4.2 Methods
4.2.1 Sample treatment and bacterial culture
The MEF samples (I, II, V) obtained by aspiration after myringotomy into 0.7 ml (FinOM Vaccine Trial) or 0.5 to 1.0 ml (FinOM Cohort Study) of phosphate-buffered saline (PBS)-LiCl buffer were plated with a 10-µl loop immediately on selective sheep blood agar containing 5 µg/mL gentamicin for the isolation of S. pneumoniae. After incubation overnight, the plates were sent to the bacteriologic laboratory. Identification of S. pneumoniae was based on the optochin test. The numbers of pneumococcal colonies on the culture plates were recorded (Kilpi et al. 2001). Serotyping of pneumococcal isolates was made by CIEP and LA and confirmed by the quellung reaction, when necessary, with antisera obtained from Statens Serum Institut, Copenhagen, Denmark (Kilpi et al. 2001). The remaining MEF sample after bacterial culture was frozen for subsequent analyses.
The nasopharyngeal samples (III, IV) were collected with calcium alginate swabs, immersed at room temperature into 1 ml of STGG transport medium containing 0.5%

40
glucose, 10% glycerol, 3% Oxoid tryptone soya broth and 2% skimmed milk powder (Gibson & Khoury 1986) and frozen at -70°C within two hours. The tubes were transported in dry ice to the bacteriologic laboratory (National Public Health Institute, Oulu, Finland) once a week. The samples were stored at -70°C until thawed for inoculation on sheep blood and chocolate agar plates. S. pneumoniae was identified using standard methods, as described previously by Ukkonen et al. (2000). After plating for culture, the samples were refrozen and stored at -80°C. For comparison with the PCR results, the culture results for S. pneumoniae were obtained from the database compiled by Ukkonen et al. (2000) after the PCR tests had been completed.
4.2.2 DNA extraction
The MEF samples of the studies I, II and V were prepared for PCR by boiling them in water. Forty µl of sample (MEF in PBS-LiCl buffer) and 100 µl of sterile distilled water were mixed and heated at 105°C for 10 min. After boiling, the samples were centrifuged at 14000 rpm for 2 min, and the supernatant was collected and stored at -20°C. A negative control sample containing water was included in every batch of MEF samples. In study I, 20 µl of the supernatant was used in each PCR reaction. In the studies II and V, 11 µl (agarose gel detection) or 13 µl (microwell hybridisation detection) of supernatant was used for each conventional PCR reaction. Additionally, 2 µl of supernatant was used for real-time PCR in study II.
In study V, for real-time PCR of MEF samples that were positive by pneumococcal culture but negative by ply-PCR, DNA was isolated from 50 µl of MEF sample using the QIAamp DNA Mini kit (QIAGEN, Hilden, Germany) in accordance with the Tissue protocol of the manufacturer´s instructions. The purified DNA was eluted in 50 µl of elution buffer, and 8 µl of sample was used for real-time ply-PCR. For a real-time PCR analysis for the presence of PCR inhibitors in MEF samples, selected samples were boiled as above, and 2 µl of supernatant was used for real-time PCR. In study V, Streptococcus group A isolates grown from seven MEF samples were also analysed by real-time ply-PCR. The strains were recultured, colonies were collected from the plate and suspended in 100 µl of sterile distilled water. The bacterial suspensions were heated at 100°C for 10 min and centrifuged at 14000 rpm for 2 min. The supernatant was collected and stored at -20°C. Two µl of supernatant was used for real-time ply-PCR.
In study III, the DNA of each nasopharyngeal sample was extracted by three different methods: the QIAamp® DNA Mini Kit (QIAGEN), the MagNAPure™ LC DNA Isolation Kit II (Tissue) (Roche Diagnostics GmbH, Mannheim, Germany) together with the PickPen™ magnetic particle transfer device (Bio-Nobile, Turku, Finland) and the KingFisher® genomic DNA purification Kit (Thermo Labsystems, Helsinki, Finland) together with the KingFisher® mL instrument (Thermo Labsystems). Fifty nasopharyngeal specimens were thawed, and 100 µl aliquots were placed into three microcentrifuge tubes and stored at -20°C. The aliquots were then thawed right before the DNA extraction. DNA extraction with the QIAamp DNA Mini Kit (QIAGEN) was performed by following the protocol for Tissues in the manufacturer’s instructions, with

41
the following modifications: In the first step, 90 µl of Buffer ATL and 10 µl of Proteinase K –solution were added to 100 µl of nasopharyngeal specimen and incubated overnight at 56°C. In the elution step, the DNA was eluted with 100 µl of Buffer AE. The optional centrifugation step to remove all Buffer AW2 was performed. To detect possible contamination, one negative control sample (water) per 11 clinical samples was taken through the whole QIAGEN extraction procedure. The MagNaPure LC DNA Isolation Kit II (Roche Diagnostics GmbH) was used by following a protocol modified from the manufacturer´s instructions. Instead of the MagNaPure LC instrument, a manual magnetic particle transfer device, the PickPen (Bio-Nobile), with disposable silicon rubber tips for collecting the magnetic particles was used. One hundred µl of Tissue Lysis Buffer and 20 µl of Proteinase K –solution were added to 100 µl of nasopharyngeal sample and mixed. The samples were incubated at 65°C for 10 min, after which they were mixed again and incubated overnight at 65°C. After incubation, 300 µl of Lysis/Binding Buffer was added, the samples were mixed, and 150 µl of Magnetic Glass Particles suspension was added. The samples were incubated at room temperature for 5 min before the beads were collected with the PickPen and transferred to 850 µl of Wash Buffer I. The beads were released into the buffer and mixed gently, after which the beads were similarly collected again, washed in 450 µl of Wash Buffer II, collected and washed in 450 µl of Wash Buffer III. After washing, the beads were collected and transferred to 100 µl of Elution Buffer, which had been heated to 65°C. The purified DNA was eluted from the beads at 65°C for 5 min, after which the beads were collected and removed from the solution. One negative sample (water) per 12 clinical samples went through the whole MagNA Pure-Pick Pen extraction procedure. The KingFisher genomic DNA purification kit (Thermo Labsystems) and the KingFisher mL instrument (Thermo Labsystems) were used according to the following protocol, modified from the Protocol B of the manufacturer´s instructions: Proteinase K and Buffer ATL supplied by QIAGEN were used, as these were not included in the KingFisher kit. Ninety µl of Buffer ATL and 10 µl of Proteinase K solution was added to 100 µl of nasopharyngeal sample, mixed and incubated overnight at +56°C. After incubation, 750 µl of Lysis buffer was added, and the whole mixture was transferred to tube 1 in the tube strips. Washing buffer, ethanol, distilled water and magnetic particles were added to the tubes according to the manufacturer´s instructions. DNA was extracted using the Genomic_DNA_mL_1 program of the KingFisher mL instrument. The extracted DNA was dissolved in 100 µl of water. A negative control sample (water) was extracted in every run with the instrument. All the extracted DNAs were stored at -20°C.
In study IV, genomic DNA was extracted from the 400 nasopharyngeal samples by using a 5% Chelex 100 Resin (Bio-Rad Laboratories, CA, USA) solution. The procedure used was a slightly modified version of that published by Walsh et al. in 1991. The solution was prepared by dissolving 2.5 g of Chelex 100 Resin powder into 50 ml of distilled water and mixing on a magnetic stirrer. While mixing, 200 µl of 5% Chelex solution was pipetted into sterile eppendorf tubes and 50 µl of nasopharyngeal sample was added into the tubes. The mixtures were heated at 56°C for 30 min, vortexed at high speed for 10 s and incubated at 100°C for 8 min. After incubation, the mixtures were vortexed again for 10 s and centrifuged at 15,000 g for 3 min. The supernatant containing the DNA was collected and stored at -20°C.

42
Purified pneumococcal DNA for the external standards used in real-time quantitative PCR and controls in conventional PCR was prepared from cultured pneumococci using the QIAamp DNA Mini Kit (QIAGEN). The amount of purified DNA was measured spectrophotometrically. For real-time PCR, standards containing 5 × 104, 5 × 103, 5 × 102, 5 × 101 and 5 pneumococcal genome equivalents were made based on the S. pneumoniae genome size. In study II, the lowest standard used contained 5 × 101 pneumococcal genome equivalents. In the studies III, IV and V, the standards were prepared in water containing 10 ng/ml MS2 RNA (Roche Diagnostics GmbH) to stabilize the standards and to prevent adsorption to the walls of the tubes.
4.2.3 Oligonucleotides used for amplification and detection
The oligonucleotide sequences for primers and probes used in conventional PCR and real-time PCR are summarized in Table 3. The primers used in conventional PCR (studies I, II, and V) were the same as the IIa and IIb primers described by Salo et al. in 1995, but in this publication the sequence of primer IIa is misspelled. The real-time PCR primers were slightly modified from those published by Salo et al. (1995). The primers were synthesized at the Institute of Biotechnology, Helsinki, Finland (primers IIa [WO 506](Walsh et al. 1991) and IIb) and TIB MOLBIOL, Berlin, Germany (primer LCIIa). One diaminohexane-modified deoxycytidine (modC) was inserted to the 5´end of the WO506 primer for biotinylation. The amplicon product size was 209 bp in conventional PCR and 206 bp in real-time PCR. The Europium-labelled probe was synthesized at the Department of Biochemistry, University of Turku, Turku, Finland. Twenty modC’s were coupled to the 5´end of the oligonucleotide during synthesis for labelling the probe with Europium. The fluorescent-labelled hybridisation probes used in the hybridisation protocol in real-time PCR were designed and synthesised at TIB MOLBIOL, using the sequence for the pneumolysin-encoding gene (Walker et al. 1987).
Table 3. Oligonucleotides used in PCR for the amplification and detection of S. pneumoniae.
Oligonucleotide Sequence (5´→ 3´) Forward primer IIa (WO 506) (biotin-modCa)1 CCCACTCTTCTTGCGGTTGA Forward primer LCIIa ACTCTTCTTGCGGTTGATCG Reverse primer IIb (WO507) TGAGCCGTTATTTTTTCATACTG Eu-labelled probe (Eu-modCa)20 GAGAAAGCTATCGCTACT FLU probe TCTCCAAGTGGAAGACCCCAGCAA-Flub LC probe LCRed640c-CAAGTGTTCGCGGAGCGGTAAAC-pd adiaminohexane-modified deoxycytidine, bfluorescein, cLightCycler Red640, dphosphate

43
4.2.4 Conventional PCR and microwell hybridisation (I, II, V)
Amplification of the 209-bp fragment of the pneumolysin gene was performed using a programmable thermal controller (PerkinElmer GeneAmp PCR System 9600, Applied Biosystems, Foster City, CA, USA) and a "hot start" method, in which one or more reaction components are separated from the others at temperatures where extension of unspecifically paired primers could take place (Erlich et al. 1991). In this application, enzyme and sample were separated from the rest of the reaction mixture by a wax layer (AmpliWax, Applied Biosystems). In study I, the 50-µl reaction mixture contained 50 mM of KCl, 10 mM of Tris-HCl (pH 8,3 at 25°C), 2 mM of MgCl2, 0.2 mM of each deoxyribonucleotide, 25 pmol of biotinylated sense primer WO 506 (Dept. of Biochemistry and Biotechnology, Univeristy of Turku), 25 pmol of antisense primer IIb (Institute of Biotechnology, University of Helsinki, Helsinki, Finland), 1 U of Taq DNA polymerase (HyTest, Turku, Finland) and various amounts of DNA. In the studies II and V, the 25-µl reaction mixture contained 0.2 mM of each deoxyribonucleotide, 30 pmol of each primer, 1 U of Taq DNA polymerase (Promega, Madison, WI), 2 mM MgCl2, 1 x PCR buffer (50 mM KCl, 10 mM Tris-HCl, pH 9.0 at 25°C, 0.1% Triton X-100; Promega) and 11 µl of sample. The wax was transferred onto the lower component consisting of KCl, Tris-HCl, MgCl2, dNTPs and primers with a sterile needle and melted for 5 min at 70°C. The enzyme was mixed with KCl and Tris-HCl buffer and added on the wax layer. Finally, the sample was added. The PCR protocol consisted of an initial denaturation step at 94°C for 5 min, 40 cycles of amplification, each consisting of 30 s of denaturation at 94°C, 30 s of annealing at 55°C and 30 s of elongation at 72°C and, finally, extension at 72°C for 6 min. The tubes were kept at +4°C until electrophoresis and hybridisation were performed. In each series with clinical specimens, a positive control (pneumococcal DNA preparation) and one negative control (sterile distilled water instead of sample) for each set of 5 clinical specimens were included (I). In the studies II and V, two positive controls of pneumococcal DNA preparation were included: one containing approximately 1000 pneumococcal genome equivalents (P1) and a 1:20 dilution of it (P2; containing approximately 50 genome equivalents). One negative control (sterile distilled water instead of sample) for each 6 clinical specimens was also included. Standard precautions against carryover contamination were taken throughout the studies (Kwok & Higuchi 1989).
In study I, agarose gel electrophoresis was used as a reference method for microwell hybridisation. From each PCR reaction, 8 µl aliquots of reaction product were loaded onto a 2 % agarose gel stained with ethidium bromide, and electrophoresis was carried out at 180 V for 60 min. The amplification products were visualized with an UV transilluminator and photographed. A clear-cut band of expected size was considered as a positive result. In the studies II and V, the PCR products were detected first by agarose gel electrophoresis, after which positive findings were reamplified and detected by microwell hybridisation. The PCR was performed as above, except that the forward primer was biotinylated, the sample volume was 13 µl, and all other reaction volumes except enzyme volume were doubled.
The sensitivity of detecting PCR products by microwell hybridisation reaction (I) was evaluated using amplification products made from dilutions of control DNA, which was

44
isolated from pure cultures of pneumococci. The amount of DNA was measured spectrophotometrically, and tenfold dilutions (10-5 -10-9) were made from a DNA sample containing 30 µg DNA/ml. Synthetic biotinylated target DNA (65 base) containing a 18-base-long sequence complementary to the Europium-labelled hybridisation probe (18 base + 20 modC) was used to optimize the hybridisation conditions. Incubation temperatures from +30°C to +55°C were tested to determine the optimum temperature for hybridisation. In all of the hybridisation experiments, 2 ng (about 1011 molecules) of hybridisation probes were used. The sensitivity of hybridisation was studied by measuring the dilution series of the synthetic target DNA. The cut-off level was determined as twice the mean background obtained by hybridisation without the target DNA (I). All the hybridisation measurements were made in triplicate.
Microwell hybridisations were performed as follows: Delfia Assay buffer (PerkinElmer Life Sciences Wallac Oy, Turku, Finland) in a volume of 65 µl (25 mM Tris-HCl pH 7.75, 0.005 % Tween 40, 0.25 % BSA, 0.025 % Bovine globulin, 10 µM diethylenetriaminepentaacetic acid [DTPA], 0.025 % sodium azide) and 10 µl of PCR amplification product (or oligonucleotide standard) were incubated in streptavidin-coated microtitration wells (PerkinElmer Life Sciences Wallac Oy) at room temperature on a plate shaker for 30-45 min, to collect the amplified product (or biotinylated target DNA in optimization assays) onto the surface of the microtitration wells. The wells were then washed twice at room temperature using DELFIA washing solution (10 mM Tris-HCl pH 7.75, 150 mM NaCl, and 0.1 % Tween 20, 0.05 % sodium azide) and an automated plate washer (Autodelfia, PerkinElmer Life Sciences Wallac Oy). To denature the collected amplification products, 150 µl of 50 mM NaOH was added into the microtitration wells, and the plates were incubated for 5 min at room temperature with shaking (the synthetic target DNA is already single-stranded and does not require the denaturation step). After denaturation, the wells were washed twice as described above. Hybridisation was performed by adding 100 µl of hybridisation buffer (Delfia Assay buffer with 1 M NaCl) containing 2 ng of Eu3+-labelled probe and incubating for 3 h (or the time desired) at the optimum hybridisation temperature for the probe. After hybridisation, the wells were washed 6 times using DELFIA washing solution, and 200 µl of DELFIA enhancement solution (PerkinElmer Life Sciences Wallac Oy) was added into the wells and incubated at room temperature for 30 min. Time-resolved fluorescence (TRF) was measured with a DELFIA 1234 research fluorometer (PerkinElmer Life Sciences Wallac Oy) using the program for Eu3+ measurements. To control the efficiency of hybridisation, a series of synthetic target DNA was hybridized on the same plate as the PCR products. All the measurements were made in triplicate. In the studies II and IV, the following modifications of the hybridisation protocol were made: the streptavidin-coated microtitration plates were washed once with DELFIA washing solution before collecting the PCR amplification products onto the surface of the microtitration wells, the PCR products were collected by incubating 60 µl of DELFIA Assay buffer and 10 µl of PCR product in the microtitration wells at room temperature on a plate shaker for 30-45 min, the wells were washed three times at room temperature using DELFIA washing solution both after collection of the PCR products and after denaturation of the products, hybridisation with a Eu3+-labelled probe was performed overnight at +37°C, and after hybridisation, the wells were washed 10 times using DELFIA washing solution. The DELFIA enhancement solution was incubated on a plate shaker at room temperature for

45
30 min before measuring time-resolved fluorescence. The cut-off value for positivity was set at twice the mean of the time-resolved fluorescence of the negative controls included in the run. Thus, the cut-off value differed slightly from one run to another.
To evaluate the applicability of the microwell hybridisation method to clinical samples, 50 randomly selected MEF specimens collected during the FinOM Cohort study were studied (I). The TRF signals produced by culture-positive samples were compared to the number of bacterial colonies. In study II, conventional PCR combined with microwell hybridization was used as a reference method. In study V, all MEF samples from the FinOM Vaccine Trial were analysed using the conventional PCR method.
4.2.5 Real-time quantitative PCR (II- V)
Amplification of a 206-bp fragment of the pneumolysin-encoding gene was performed using the LightCycler Instrument (Roche Diagnostics). The LightCycler FastStart DNA Master SYBR Green Kit (Roche Diagnostics GmbH) was used in the initial optimization of PCR. The LightCycler FastStart DNA Master Hybridisation Probes Kit (Roche Diagnostics GmbH) was used in the analysis of clinical samples. The kit, together with hybridisation probes, is meant for the amplification and sequence-specific detection of DNA fragments. The 20-µl reaction mixture contained 1 × LightCycler FastStart DNA Master Hybridisation Probes reaction mixture (Roche Diagnostics GmbH), 4 mM MgCl2, 1 µM of each primer, 0.2 µM of each probe and 2 µl (II) or 8 µl (III) of extracted sample DNA or standard DNA in appropriate dilution. The amplification was performed in borosilicate glass capillaries (Roche Diagnostics GmbH). The PCR protocol consisted of an initial denaturation step at 95°C for 10 min, 50 cycles of amplification, each consisting of 10 s of denaturation at 95°C, 15 s of annealing at 57°C, and 9 s of elongation at 72°C and, finally, cooling at 40°C for 30 s. The temperature transition rate was 20°C/s, and fluorescence was measured once after each annealing step. In study II, standards containing 5 × 104, 5 × 103, 5 × 102 and 5 × 101 pneumococcal genome equivalents were included in each run with clinical specimens. In the studies III, IV and V, a standard containing 5 genome equivalents was also included. Every seventh specimen was a no-template control (sterile distilled water instead of sample). To prevent carryover contamination, standard precautions were taken, including the preparation of reaction mixture in a clean room separate from the room where the samples and standards were prepared and the room where they were loaded into the capillaries (Kwok & Higuchi 1989).
The fluorescence data gathered during real-time PCR were analysed using the Fit Points method of the Data Analysis program of the LightCycler Software version 3.3 (Roche Diagnostics GmbH) (study II) or the Second derivative maximum method of the LightCycler Data Analysis program version 3.5.28 (Roche Diagnostics GmbH) (studies III, IV, and V).
The applicability of the real-time PCR method to clinical samples was first evaluated by studying 50 MEF samples (II). The patient samples were analysed using both quantitative real-time PCR and the conventional pneumolysin PCR method combined

46
with agarose gel electrophoresis detection of the amplification products. The samples positive in agarose gel electrophoresis were reamplified, and the amplification products were detected and quantified using microwell hybridisation with a Europium-labelled probe and time-resolved fluorescence (TRF) detection.
The average amplification efficiency of samples (II) was studied by analysing the dilution series of one of the samples positive by real-time PCR. The crossing-point (the cycle number where the fluorescence signal first exceeds the threshold level) versus the logarithm of the initial number of genome equivalents was plotted, and the average efficiency was calculated from the slope of the line (Rasmussen 2001). The average efficiency of the standards was calculated from the slope of the standard curves.
In study III, the three different extracts of each sample were amplified in the same PCR run. An external standard curve created from one of the PCR runs was used in the analysis to prevent the possible effect of even minor variations in standards on the quantification results.
The real-time PCR analysis of the nasopharyngeal samples in study IV was done with two different probe concentrations and with two different sample volumes, which affected the quantification done automatically by the fluorimeter of the LightCycler device. The analysis was started with a mixture containing low concentrations of the probes, i.e. 0.15 µM and 0.10 µM of the probes labelled with LCRed640 and fluorescein, respectively, and 2 µl of sample to demonstrate all definitely positive samples. All the samples that yielded a negative or borderline result with this mixture were reanalysed with a mixture that contained more of the probes, i.e. 0.2 µM of both. The samples that still failed to give a clear-cut result – borderline cases from the second analysis and samples with a borderline result from the first analysis and negative with the second probe mixture – were analysed for a third time. In the third mixture, the sample volume was quadrupled to detect the samples containing tiny amounts of S. pneumoniae. Nasopharyngeal samples with culture-positive but real-time PCR-negative results were recultured and bacterial lysates were made. Real-time PCR was performed using 2 µl of the lysate and both of the reagent mixtures containing smaller and larger amounts of probes.
In study V, twenty-three MEF samples positive by pneumococcal culture but negative by ply-PCR and 7 MEF samples growing Group A Streptococcus were reanalysed by using quantitative real-time ply-PCR. In 40 selected MEF samples, including 10 culture-positive samples with high PCR counts, 10 culture-positive samples with low PCR counts, 10 culture-negative samples with high PCR counts and 10 culture-negative samples with low PCR counts, the presence of inhibitors was also tested by adding 1000 pneumococcal genome equivalents to 2µl of boiled MEF sample and by comparing the genome numbers obtained without and with added pneumococcal DNA.

47
4.2.6 Comparison of the sensitivities of bacterial culture and real-time PCR
The sensitivities of real-time ply-PCR and bacterial culture were compared by analysing 10-fold dilutions of a fresh pneumococcal broth culture by both methods (III, IV). The pneumococcal broth culture was prepared by mixing ten colonies of S. pneumoniae strain ATCC 6305, grown on a blood agar plate in 5% CO2 at +37°C overnight, with 4 ml of brain-heart infusion (BHI) broth (Difco 0037-17-8, Detroit, MI) containing 10% horse serum (Gibco 26050-088, Paisley, UK). The suspension was incubated in 5% CO2 at +37°C overnight, after which optical density (OD) at 650 nm was measured. Two hundred µl of the bacterial suspension was transferred into 4 ml of BHI broth (Difco) with 10% horse serum (Gibco), and OD at 650 nm was measured again. The bacteria were grown in 5% CO2 at +37°C, and their growth was followed by measuring the OD values at 650 nm regularly. After 7 h, the bacteria were collected by centrifuging at 2000 × g for 15 min and suspended in 1 ml of phosphate-buffered saline. Tenfold (10-1 – 10-6) dilutions of the suspension were made both in STGG medium and in PBS, and 10 µl of each dilution was immediately spread on blood agar plates. The bacterial cultures of each dilution were made as triplicates. The plates were incubated in 5% CO2 at +37°C, and the number of colonies was recorded after 24 and 48 hours. The rest of the tenfold dilutions of the bacterial suspension were stored at -20°C for PCR. The samples were prepared for PCR by using two methods: the Chelex 100 Resin (Bio-Rad Laboratories) and the QIAamp DNA Mini Kit (QIAGEN). The sample preparations were performed as described above, except that in the QIAamp method, 180 µl of Buffer ATL and 20 µl of Proteinase K solution were added to 200 µl of sample, and DNA was eluted with 200 µl of Buffer AE. The extractions of DNA from the 10-5 and 10-6 dilutions of the pneumococcal suspension were made as triplicates. Real-time PCR was performed as triplicates from all DNA extracts, as described above (sample volume 8 µl).
4.2.7 Statistical methods
The sensitivities of bacterial culture and real-time PCR methods were compared using the Wilcoxon signed-ranks test. Spearman´s correlation was used to evaluate the correlation between the conventional PCR and culture results (I), the real-time PCR and culture results (III, IV) and the conventional PCR and real-time PCR results (II).

5 Results
5.1 Development of methods (I, II)
5.1.1 Conventional PCR and microwell hybridisation (I)
A microwell hybridisation method for the detection of ply-PCR amplification products was developed and optimized. The sensitivity of the assay was 4 x 10-14 - 6 x 10-14 g of purified pneumococcal DNA, corresponding to 17-25 pneumococcal genome equivalents. The same sensitivity was also reached when amplification products were detected by the reference method, i.e. agarose gel electrophoresis.
The measurements of optimal hybridisation time gave an almost linear increase in counts along with the prolongation of hybridisation time. A low hybridisation rate may be due to the formation of secondary structures into a single-stranded target molecule. A sensitivity of 3 x108 target molecules for an individual well was achieved with a 30 min attachment time and a 3 h hybridisation time. The optimal temperature for hybridisation was 35-40°C.
In the hybridisation of PCR products, the cut-off value for positivity was set to be twice the mean value of the negative control samples (10000 cps). Of the 50 MEF samples screened for the presence of pneumococcal DNA by TRF hybridisation, 33 (66 %) were positive. These samples were also all positive by agarose gel electrophoresis. Additionally, six samples that were negative by TRF hybridisation produced multiple bands on the electrophoresis gel and thus remained without definite interpretation. Of the 50 MEF samples, 12 (24 %) were pneumococcal culture-positive. All culture-positive samples were positive by PCR, regardless of the detection method. Thus, the sensitivity of both TRF-based hybridisation and agarose gel electrophoresis compared to bacterial culture was 100 %. Of the pneumococcal culture-negative samples, 21 (55 %) were positive by TRF hybridisation. All these specimens were also positive by agarose gel electrophoresis.

49
The PCR amplification products from pneumococcal culture-positive MEF samples produced distinct cps values never lower than 22500 and varying up to 2.3 million when interacting with the Eu3+-labelled oligonucleotide. In the blanks containing no DNA, generally less than 5000 cps were recorded. The fluorescence intensity of a positive reaction was 4.5 - 460 times higher than that generated by the negatives. There was a correlation (0.669, P < 0.05) between the CFUs obtained by culture and the cps obtained by PCR, although it was not very strong.
The specificity of the PCR primers used had been tested earlier (Salo et al. 1995). The specificity of the TRF method was further tested by using strains of Haemophilus influenzae, Staphylococcus aureus and Chlamydia pneumoniae. No unspecific signals were observed.
5.1.2 Real-time quantitative PCR (II)
A real-time PCR assay for the detection and quantification of pneumococcal DNA was developed (II). The assay was first developed and optimized using a double-stranded DNA-binding dye, which detects DNA regardless of sequence, and standards containing 5 × 10 to 5 × 104 pneumococcal genome equivalents. By studying the melting curves of the standards, the melting temperature of the specific amplification product was found to be close to 84°C (Fig. 2). The real-time PCR assay was further developed by introducing a pair of fluorescent-labelled sequence-specific hybridisation probes for the detection of amplification products. The amplification curves of the standards are shown in Fig. 3. No products were detected in the negative controls after 50 cycles of amplification.

50
Fig. 2. Melting curve analysis of amplification products of tenfold dilutions of purified S. pneumoniae DNA. Detection was done using the double-stranded DNA-binding dye SYBR Green. Neg.: negative control. -d(F1)/dT: the first negative derivative of fluorescence measured at 530 nm.

51
Fig. 3. Amplification of tenfold dilutions of purified S. pneumoniae DNA. Detection was done using sequence-specific hybridisation probes. Neg.: negative control, F2: fluorescence measured at 640 nm, F1: fluorescence measured at 530 nm.
Twenty-six (52%) of the 50 MEF samples analysed by using the real-time PCR assay were positive, including all of the 17 (34%) culture-positive samples and 9 (27%) of the 33 culture-negative samples (Table 4). The sensitivity and specificity of the assay compared to pneumococcal culture were 100% and 73%, respectively. Pneumolysin-PCR and agarose gel detection of amplification products showed 29 (58%) samples to be positive. All positive samples were amplified again and detected using the assay based on a Europium-labelled hybridisation probe and time-resolved fluorescence measurement, resulting in 27 (54%) positive samples. The sensitivity and specificity of the real-time PCR assay compared to conventional PCR with agarose gel and/or TRF detection were 93% and 96%, respectively.
The number of genome equivalents detected by the real-time PCR assay varied from 90 to 88000/µl in culture-positive samples and from 1 to 1200/µl in culture-negative samples (Table 4). The number of genome equivalents exceeded 90/µl in one culture-negative sample only, while the numbers in the remaining eight samples ranged from 1 to 16/µl. The amount of amplified fragments detected by the Eu3+-labelled probe and TRF measurement varied from 30000 to 980000 cps. The correlation between the amount of amplified fragments detected with the PCR-TRF assay and the amount of genome equivalents detected by the real-time PCR assay was 0.827 (Spearman’s correlation coefficient; P < 0.001). Two samples that were positive by conventional PCR were

52
negative by real-time PCR. In these two samples, the lowest cps numbers (30000) were detected. One sample was positive by real-time PCR and negative by conventional PCR. One genome equivalent/µl was detected from this sample.
The average amplification efficiency of real-time PCR with hybridisation probe detection was 1.82 – 1.85 for standards and 1.84 for the sample analysed.
Table 4. Comparison of PCR results obtained when using conventional PCR combined with microwell hybridisation and time-resolved fluorescence (TRF) measurement, and quantitative real-time PCR with a pair of fluorescent-labelled hybridisation probes.
PCR-positive samples
n TRFa, n cpsb , median (range)
qPCRc, n Genomes/µl, median (range)
All MEF samples 50 27 (54%) 510000 (30000 – 980000)
26 (52%) 1000 (1 – 88000)
Culture –d 33 10 (30%) 93000 (30000 – 510000)
9 (27%) 7 (1 – 1200)
Culture +e 17 17 (100%) 640000 (220000 – 980000)
17 (100%) 2100 (90 - 88000)
atime-resolved fluorescence, bcounts per second, cquantitative real-time PCR, dnegative, epositive
5.2 Effect of the DNA extraction method on the quantitative real-time PCR results obtained (III)
Fifty nasopharyngeal secretion samples were analysed by real-time PCR after DNA from the samples had been extracted by three different methods. Twenty-two (44%) of the specimens studied were positive by pneumococcal culture. All culture-positive samples were positive by real-time PCR, regardless of the DNA extraction method used, with the exception of one sample, from which DNA was extracted by the KingFisher method, and which was positive only in a repeatedly test. 71%, 57% and 82% of the culture-negative samples were positive by real-time PCR when DNA was extracted by the QIAamp, MagNAPure-PickPen and KingFisher methods, respectively. Altogether 46 (92%) of the 50 samples were positive by PCR when DNA was extracted with at least one of the three DNA extraction methods used. In eight samples, the PCR amplification curves were low with one or more of the three DNA extracts. To confirm the suspected positive results of these samples, they were reanalysed by PCR. All three extracts of these eight samples were reanalysed at the same time, even though some of them had been clearly negative. Two of these reanalysed DNA extracts, purified by MagNaPure and PickPen, were at first negative, but turned out to be positive in the second analysis. However, their initial results were recorded, as these samples would not have been reanalysed without an unclear positive result in another extract.

53
In the pneumococcal culture-positive samples, the number of genomic equivalents detected by real-time PCR varied from < 1 to 4.8 × 103/µl in QIAamp extraction, from < 1 to 1.7 × 104/µl in MagNAPure and PickPen extraction and from 8 to 2.6 × 104/µl in KingFisher extraction (Table 5). In the culture-negative samples, the number of genome equivalents/µl was below 70 in all but one of the samples. In this sample, the quantification result was of the magnitude of 103 in all the three DNA extracts. The sample was recultured, but remained negative. Otherwise, genome equivalents of the order of 103 and 104 were detected only in the samples from which over 100 colonies had been cultured. Among the 46 samples that were positive by PCR with at least one of the three DNA extraction methods, the highest numbers of genomic equivalents/µl were detected in 9 cases (20%) in the QIAamp extract, in 2 (4%) cases in the MagNaPure and PickPen extract and in 31 cases (67%) in the KingFisher extract. In three cases (7%), the best quantification result was obtained in both the MagNaPure and the QIAamp extracts, and in one case (2%) the quantification result was the same in all the three extracts. Of the PCR-positive samples, the quantification result was < 1 genome equivalent/µl in 16 of the QIAamp DNA extracts, 11 of the MagNaPure and PickPen extracts and 8 of the KingFisher extracts (Table 5).
Table 5. Comparison of the quantitative pneumolysin PCR results obtained from the different DNA extracts with S. pneumoniae culture results
Culture result, number of
Number of samples according to orders of magnitude of genome equivalents/µl
DNA extraction method
colonies neg. <1 100 101 102 103 ≥ 104 QIAamp Negative 8 14 4 1 0 1 0 <10
10-100 >100
0 0 0
1 0 1
2 1 2
1 0 4
0 0 6
0 0 4
0 0 0
MagNAPure + PickPen Negative 12 10 4 1 0 1 0 <10
10-100 >100
0 0 0
1 0 0
3 0 0
0 1 3
0 0
11
0 0 2
0 0 1
KingFisher Negative 5 8 12 2 0 1 0 <10
10-100 >100
1 0 0
0 0 0
2 0 0
1 0 0
0 1 8
0 0 7
0 0 2
5.3 Comparison of real-time PCR and pneumococcal culture (III, IV)
Because of the high PCR positivity rate of culture-negative samples, tenfold dilutions of pneumococcal broth culture were analysed by PCR and pneumococcal culture. The dilutions of the broth culture were made in STGG medium, in which the nasopharyngeal swabs had been stored, and in PBS. For PCR, two different DNA extraction methods, QIAamp and Chelex 100 Resin, were used. When using the Chelex 100 Resin for DNA

54
extraction, the samples were diluted 1:5 during the DNA extraction step. The mean number of colonies growing from the 10-µl samples cultured from the 10-4 STGG dilution of the pneumococcal broth culture was approximately 400, i.e. 40 colonies/µl, whereas by real-time PCR of DNA extracted by using the QIAamp Kit, a ten-fold number, i.e. a mean of 415 genome equivalents/µl, was detected (Table 6). By real-time PCR of the Chelex extracts, a mean of 135 genome equivalents could be detected from the 8-µl samples analysed, corresponding to 84 genome equivalents/µl of the original 10-4 sample. Thus, in this dilution, the number of genome equivalents/µl detected by PCR was two-fold compared to the number of colonies/µl detected by culture. From the 10-5 dilutions, the mean colony number was 5.8 colonies/µl, and by PCR, a 30-fold number of genome equivalents, 180/µl, was found in the QIAamp extracts and a roughly 4-fold number, 23.6/µl, in the Chelex extracts. In the 10-6 STGG dilutions, the corresponding figures were 2.0 colonies/µl and 37 (QIAamp) and 21.8 (Chelex) genome equivalents/µl, respectively. When the quantitative results of bacterial culture and real-time PCR were compared by the Wilcoxon signed-ranks test, real-time PCR was found to detect significantly higher numbers of bacteria (P < 0.001), irrespective of the DNA extraction method used. There was, however, a strong correlation between the results obtained by quantitative culture and real-time PCR (Spearman’s correlations 0.983, P < 0.001[QIAamp]), and 0.922, P < 0.001 [Chelex]).
Table 6. Comparison of pneumococcal culture and real-time PCR results of dilutions of a fresh pneumococcal broth culture.
Dilution STGG PBS Culture
(CFUsa/µl) Real-time PCR (genomes/µl)
Culture (CFUas/µl)
Real-time PCR (genomes/µl)
QIAamp DNA Mini
kit
Chelex100 QIAamp DNA Mini
kit
Chelex100
10-4 40 415 84 43 612 211 10-5 5.8 180 23.6 4.5 47.6 33.6 10-6 2.0 37 21.8 0.4 2.4 4.7 acolony forming units
5.4 Detection of pneumococcal DNA in nasopharyngeal swab specimens using real-time PCR (IV)
Four hundred nasopharyngeal swab samples were analysed by real-time PCR, and 276 (69%) samples were positive (Table 7). Of these, 30 (11%) had amplification curves of non-exponential shapes and were classified as borderline-positive, to distinguish them from the others. One hundred and fifty-eight (40%) of the 400 samples were positive by pneumococcal culture. Real-time PCR was positive in 151 (96%) of the pneumococcal culture-positive samples and in 125 (52%) of the swab samples from which no

55
pneumococci could be cultured. Thus, seven (4%) of the culture-positive samples remained negative by real-time PCR, and 125 (45%) of the PCR-positive samples were negative by pneumococcal culture. When the 7 PCR-negative, culture-positive samples were recultured from STGG tubes, four of them grew pneumococci. The three samples that remained negative had grown only a few colonies (< 10) in the original culture. The pneumococcal isolates from the 4 positive recultured samples were tested for the presence of the ply gene by real-time PCR, and all of them were positive. The corresponding 4 nasopharyngeal samples were therefore further tested for the presence of PCR inhibitors by spiking with pneumococcal DNA. As a result, high genome values were detected in three of the samples, but no amplification occurred in one sample.
Table 7. Detection of Streptococcus pneumoniae in 400 nasopharyngeal swab samples: comparison of the results obtained by real-time PCR and bacterial culture.
Real-time PCR Culture Positive Borderline Negative
Total
Positive 147 4 7 158 (40%) Negative 99 26 117 242 (61%) Total 246 (62%) 30 (8%) 124 (31%) 400
The PCRs of the nasopharyngeal samples were performed using two different probe concentrations and two different sample volumes. The number of samples analysed by using each mixture and the results obtained are shown in Figure 4.
The comparisons of quantitative real-time PCR and culture results of the 400 samples are shown in Table 8. The median orders of magnitude of the genome numbers detected in the clearly PCR-positive nasopharyngeal swab samples were 101 and 103, and the mean was of the order of 101. The borderline cases were categorized into their own order of magnitude, because their genome contents could not be accurately determined. The highest numbers of genome equivalents were detected in the samples from which over 100 colonies had been cultured. In the culture-negative, PCR-positive samples, the genome numbers detected varied mainly within 1-100, the median being of the order of 101. When comparing the quantitative results of the samples that were positive by both culture and PCR, a positive trend could be seen. Within the PCR category of 1 to <10 genome equivalents detected, 6 (75%) samples had a culture result in the smallest order of colonies (<10). The majority, 12 (92%) and 32 (91%), of the samples with PCR results within the categories 101 and 102, respectively, had a culture result of 10-100 colonies or more. Within the PCR results in the categories 103-105, 89% of the culture results also belonged to the highest order of culture colonies (> 100).

56
Fig. 4. Study flow chart showing the outcomes of 400 nasopharyngeal samples stored in STGG transport medium when screened by real-time PCR and culture (IV).
Table 8. Comparison of quantitative results obtained by real-time PCR and culture of 400 nasopharyngeal swab samples.
Real-time PCR, orders of magnitude of genome equivalents detected Culture, number of colonies
Negative Borderline <1 ≥1 <10
101 102 103 104 105 Total
Negative 117 26 3 29 51 12 4 0 0 242 <10 6 4 1 6 1 3 0 0 0 21 10-100 1 0 0 1 8 11 9 1 0 31 >100 0 0 0 1 4 21 51 21 8 106 Total 124 30 4 37 64 47 64 22 8 400
5.5 Detection of pneumococcal DNA in MEF samples (V)
In study V, 1222 (47%) of the 2595 MEF samples analysed were positive by ply-PCR. In 921 (51%) of the 1819 AOM events, ply-PCR was positive. In 686 of the samples positive in ply-PCR, pneumococcal culture was also positive, but in 536 samples (44%), the MEF cultures remained negative for pneumococcus. Pneumococcal findings increased with PCR detection by 76% compared to culture alone.
400samples
+170
+/-43
-187
+25
+/-4
-14
+35
+/-28
-124
-20
133 5
37 20
-
2
-
2 6
- 2
6 28
7
6
2
18
2
117
7
Culture -
Culture +
242
158
Total
Mixture 1
Mixture 2
Mixture 3
+ positive+/- borderline- negative
+6
-2
-8
+2
+8

57
The cps detected by PCR and microwell hybridisation with TRF measurement were considerably higher in the MEF samples that were positive in pneumococcal culture than in those with a negative pneumococcal culture result (geometric mean counts 473000 vs. 127000, Fig. 5). Interestingly, the distribution of PCR counts in the culture-positive samples was bimodal, which raised a hypothesis that PCR inhibitors could be present in the culture-positive samples yielding low PCR counts. However, in a reanalysis of ten culture-positive samples with low PCR counts and ten culture-positive samples with high PCR counts by quantitative real-time PCR, higher numbers of genome equivalents were actually detected in the samples with initially low PCR counts. Six of the 10 samples with low PCR counts contained >200 genome equivalents/µl and 3 samples <5 genomes/µl, whereas only 3 of the 10 samples with high PCR counts contained >200 genomes/µl and 1 sample <5 genomes/µl. Among the culture-negative samples, this phenomenon was not demonstrable: only 2 samples with low PCR counts and 8 with high PCR counts contained >5 genomes/µl. When testing for inhibition by adding 1000 pneumococcal genomes to the samples, clear inhibition (less than 300 genomes detected out of the 1000 added) was seen in one culture-positive sample with high PCR counts and in one with low PCR counts. Thus, the bimodality of the PCR count distribution seen in Figure 5 does not seem to indicate the presence of PCR inhibitors in the culture-positive samples with low PCR counts, but rather, the inhibitory effect caused by the competition between the excessive numbers of amplification products during the microwell hybridisation step.
Twenty-three (3%) of the 709 pneumococcal culture-positive MEF samples were negative by ply-PCR. In these samples, the number of pneumococcal colonies in the MEF culture was considerably lower (median 17) than in the 686 MEF samples positive in ply-PCR (median 150). To assess the potential presence of PCR inhibitors in these 23 MEF samples, the samples were analysed by quantitative real-time ply-PCR using DNA purified from the samples. In this analysis, 20 of the 23 MEF samples were clearly positive. Two samples were negative, and one sample was considered borderline positive because of a low amplification curve, but when reanalysed, they also turned out to be positive. The quantitative result of these three samples was below 5 pneumococcal genome equivalents/µl, and the numbers of pneumococcal colonies in the original culture of these samples were also extremely low (1 to 3). The corresponding pneumococcal isolates of these three samples were also recultured and analysed by real-time PCR, and they were all positive and thus apparently contained the pneumolysin gene.

58
Fig. 5. Distribution of PCR counts in pneumococcal (Pnc) culture-negative and Pnc culture-positive middle ear fluid samples.
Pneumolysin-PCR was positive in 536 pneumococcal culture-negative MEF samples out of 400 events. The factors associated with the sensitivity of bacterial culture, such as concurrent antimicrobial treatment and small sample volume, were first analysed, after which the origin of pneumococcal DNA in these MEF samples was explored.
Current antibiotic treatment was more common in PCR-positive, culture-negative (10%) compared to culture-positive events (4%). Antimicrobial treatment may thus reduce the sensitivity of bacterial culture. However, this would still leave the remaining 90% of PCR-positive, culture-negative samples unexplained. Recent antibiotic treatment (having ended within 1 to 28 days) was equally common in both groups. The MEF volume as assessed by the study physician after the myringotomy procedure turned out to be more often low in PCR-positive, culture-negative cases (21%) compared to culture-positive cases (12%). However, the low MEF volume was most common in PCR-negative, culture-negative samples (37%). The quality of MEF was more commonly mucoid in PCR-positive, culture-negative samples (27%) than in culture-positive samples (14%).
If pneumococcus had been isolated (culture-confirmed pneumococcal otitis) from the same ear previously, 43% of the ears negative by culture were positive by PCR; when pneumococcal culture had been negative, the corresponding figure was 23%. However, the increase was not dependent on the number of previous pneumococcal isolations.

59
Thus, it seems plausible that a positive PCR finding from pneumococcal culture-negative MEF could, at least partly, be explained by a history of previous pneumococcal AOM. The duration of PCR positivity after culture-confirmed pneumococcal AOM, including the subsequent MEF samples from the same child until the next culture-confirmed pneumococcal AOM or PCR-negative AOM event was reached, was assesed, and the results showed that the proportion of PCR-positive, culture-negative samples decreased eventually as a function of time after the initial pneumococcal culture-positive sample, although the rate of decrease after the initial phase was quite low.
Among the bilateral AOM events with both samples available (N = 776), there were 101 events with a unilateral pneumococcal culture finding (the other ear negative by pneumococcal culture). In these events, 62 (61%) of the contralateral ears negative by pneumococcal culture were positive by ply-PCR. This is clearly more than in the ears bilaterally negative by culture (31%, 312/996) or in bilateral events culture-negative for all pathogens (33%, 119/362).
Fifty-three % (282/536) of all PCR-positive, culture-negative samples were derived from children with no documented previous or concurrent culture-confirmed pneumococcal AOM events. Thus, there must also be other mechanisms for PCR positivity except pneumococcus being a bystander in AOM due to other etiologies. Pneumococci or pneumococcal DNA might be brought into the middle ear from the nasopharynx by Eustachian tube reflux with other invading pathogens. The available data from the FinOM Cohort Study (169 MEF samples from ears with AOM) show that 100% of pneumococcal culture-positive MEF samples were associated with concurrent pneumococcal carriage, but only 51% of PCR-positive, culture-negative and 38% of MEF samples with no indication of pneumococcal involvement were associated with concurrent pneumococcal carriage. Thus, concurrent pneumococcal carriage is a prerequisite for pneumococcal isolation from MEF, but it is not a prerequisite for PCR positivity. However, pneumococcal culture-negative MEF samples were more commonly positive by PCR during concurrent pneumococcal carriage (50% ply-PCR-positive) compared to no carriage (38% ply-PCR-positive) based on the data from the FinOM Cohort Study. However, 27% (15/55) of PCR-positive, culture-negative samples of the FinOM Cohort Study could not be explained either by previous pneumococcal AOM or by concurrent pneumococcal carriage.
The proportion of ply-PCR-positive samples was similar in AOM due to Haemophilus influenzae or Moraxella catarrhalis compared to culture-negative AOM events. Thus, these two major AOM pathogens do not seem to increase the reflux of pneumococci into the middle ear cavity or to lead to false-positive PCR findings. Pneumolysin PCR was frequently positive in AOM caused by group A Streptococcus, but the number of isolates was only 7. These seven Streptococcus group A isolates were analysed for the presence of the pneumolysin gene by real-time ply-PCR (without using hybridisation probes and thus producing results comparable to conventional PCR analysis with agarose gel detection), and they were all negative. Thus, the high proportion of ply-PCR positivity refers to pneumococcal involvement, and not to the presence of pneumolysin in Streptococcus group A isolates.

6 Discussion
6.1 Methods developed in the study
In this study, a microwell hybridisation method that utilizes a short Europium-labelled probe was first developed to detect the amplification products of pneumococcal ply-PCR (I). The method turned out to be equally sensitive as the reference method, agarose gel electrophoresis, but proved to have several advantages. Agarose gel electrophoresis is a simple, inexpensive and rapid method for detecting PCR amplification products. However, even in well-optimised PCR systems, fragments of more than one size are occasionally amplified, and the differentiation between positive and negative results is sometimes difficult. The result obtained by agarose gel electrophoresis is also dependent on subjective interpretation. Southern blotting, which applies enzyme- or radiolabelled probes for the final identification of the specific amplification product, is laborious and time-consuming. The microwell hybridisation method is simple with an easy-to-use format for detection, and it yields objective results, as the results are presented as numerical values. In altogether six (12%) of the 50 samples analysed in study I, no definite result concerning the presence of pneumolysin DNA was obtained by agarose gel electrophoresis because of multiple unspecific bands on the gel. Using the TRF-based hybridisation assay, however, a definite negative finding was obtained for all these samples. Thus, the use of microwell hybridisation and TRF measurement improved the specificity of the ply-PCR assay. The TRF technique is easy to introduce in the laboratory. Because at least some of the reaction steps can be automated, large quantities of samples may be processed simultaneously. The detection system displays a high level of sensitivity without the hazards associated with the use of radioactive probes. Unlike radiolabelled probes, Eu3+-labelled probes are very stable and can be stored for at least 12 months without a loss of activity. A fluorometer equipped to measure time-resolved fluorescence is, however, required. The detection limit of the TRF-based assay is directly dependent on the number of Eu3+ molecules in the oligonucleotide. Coupling of several Eu3+ chelates to the DNA molecule enhances sensitivity. In study I, a labelling degree of 15 Eu3+ chelates per oligonucleotide was achieved. The TRF method can also be applied to the detection of several different microbes in the same test tube, as hybridisation

61
probes labelled with different lanthanides can be detected in the same solution after a single hybridisation reaction (Iitiä et al. 1992).
Measurement of TRF of the Eu3+ label enables quantification of the PCR end-product, but does not enable quantification of the initial template concentration. Such factors as competition of the amplification products with primers, decrease of reagent concentrations, instability of the polymerase enzyme and inhibition of products interfere with the exponential amplification and decrease the product concentration. Thus, the initial amount of template cannot be calculated from the amount of reaction end-product. Quantification of the initial amount of template by using standard curves created by stopping PCRs at various points is a laborious procedure, and the dynamic range of the analysis is usually low. In real-time PCR, amplification and detection of amplification products occur simultaneously, which makes it possible to monitor the phase of the reaction at a particular stage or continuously (Wittwer et al. 1997). As a result, the initial template concentration can be calculated based on data obtained in an earlier phase of amplification, where the amount of product still increases exponentially. In addition to being faster and easier to perform, the dynamic range of the real-time quantitative analysis is also larger. In study II, a real-time PCR method for detecting and quantifying pneumococcal DNA was developed. The sensitivity and specificity of the method compared to conventional ply-PCR with agarose gel and microwell hybridisation with TRF measurement were 93% and 96%, respectively (II). In study II, the real-time and conventional PCR classified three of the 50 samples studied divergently as positive or negative. The quantitative analysis of all these three samples produced the lowest values, which may explain the discrepancy in the qualitative PCR results. Although TRF measures the final amount of amplification product, and real-time PCR quantifies the number of initial templates, the correlation between the results obtained by these two detection methods in study II was high (0.827, P < 0.001).
The real-time ply-PCR method developed in this study was found to be rapid and easy to use. If previously extracted DNA is used, the real-time PCR assay takes only about one and a half hour, whereas the conventional ply-PCR assay combined with agarose gel electrophoresis takes about 4 hours. If hybridisation is performed, the assay time for conventional PCR is even longer. In real-time PCR, the risk of contamination is also diminished due to no handling of the amplification products during regular analysis.
The PCR primers published by Salo et al. and used in the conventional PCR assays of this study previously proved to be very specific for S. pneumoniae when tested thoroughly with altogether 55 non-pneumococcal strains (Salo et al. 1995). In the real-time PCR method developed in this study, the forward primer was slightly modified from that used in the conventional PCR assay by moving it three nucleotides forward on the pneumolysin gene. This modification was suggested by the designer and manufacturer of the hybridisation probes to achieve an optimal combination of primers and probes in the real-time PCR analysis. The primers used in real-time PCR were considered to be equally specific as the primers published by Salo et al. (1995), and the detection and quantification of the correct fragment was further ensured by using a pair of sequence specific hybridisation probes.
Since PCR is an extremely sensitive technique, care should be taken to avoid contamination and false-positive results. In this study, guidelines were carefully followed to avoid physical transfer of amplified and unamplified DNA (Kwok & Higuchi 1989).

62
Separate rooms were used for sample preparation, reaction mixture preparation and amplification and amplification product testing. Procedures against contamination included the use of hoods, UV lamps, disposable filter-plugged pipette tips and regular cleaning and desinfection. Negative controls were used during both sample preparation and PCR. In study V, where the number of samples analysed was high and PCR products were handled, the person handling PCR products was not in contact with the MEF samples or PCR reaction mixtures during the same week. In a regular real-time PCR assay with the LightCycler, the capillaries are not opened after they have been sealed for amplification, which diminishes the risk of contamination (Schalasta & Schmid 1999). However, the real-time PCR system is a ”closed” system for only as long as the capillaries containing the amplification products are intact. A broken capillary immediately creates a risk for contamination. Therefore, the real-time PCR analyses of this study were performed in a separate room away from the rooms where the samples and PCR mixtures were prepared and handled. DNA polymerases and the other reagents used in PCR are known to contain bacterial DNA, which causes false-positive results in broad-range bacterial PCR assays (Jalava et al. 2001). However, in this study, no amplification was detected in the negative reagent controls, which shows that the reagents were free of pneumococcal DNA. Because of all the careful procedures described above and the meticulous use of negative controls, contamination in the PCR laboratory is not likely to have caused false-positive PCR results.
When performing quantitative PCR with external standards, the accuracy of quantification is dependent on the standards used (Rasmussen 2001). To minimize variation in the standards in this study, the same pneumococcal DNA extract was used throughout each study, and new dilutions for all other standards except the standard containing the highest DNA concentration were made every day. In study II, the lowest standard used contained 50 pneumococcal genomes and was detected in every run. In the studies III, IV and V, the standards of the real-time PCR analyses were diluted in water containing carrier nucleic acid (MS2 RNA) to stabilize the standards. In these studies, the lowest standard contained 5 pneumococcal genome equivalents and was detected in most, but not all, PCR runs. When studying samples with low copy numbers, random variation due to sampling errors becomes important (Rasmussen 2001) and creates a possibility for false negative findings. Also, if more precise quantification results are needed, the samples containing low copy numbers should be analysed as duplicates or triplicates. Therefore, the quantification results obtained by real-time PCR in this study were generally not taken as absolute values but rather as orders of magnitudes.
In quantitative PCR with external standards, standards and target DNA in samples are assumed to amplify with similar efficiencies. The efficiency of the amplification reaction over a specific range of concentrations can be studied by analysing a dilution series of a sample (Rasmussen 2001). In the studies II and III, the average amplification efficiencies calculated for the samples were similar to those of the standards. However, it should be kept in mind that these are only calculated values and, in reality, the amplification efficiency during a reaction varies and the impact of PCR inhibitors or other factors on the amplification efficiency at a specific stage is unknown.
Real-time PCR is still a relatively new invention, and thus, each specimen type must be optimized separately. In study IV, three reaction mixtures with different probe and sample volumes were used. When 47 (12%) samples were tested with a reaction mixture

63
containing both smaller and larger amounts of probes (data not shown), the differences between the mixtures were seen in the quantification results: the samples containing plenty of bacteria gave much higher values when the lower concentration of hybridisation probes was used. When a sample contained a low number of bacteria, the mixture containing a higher probe concentration was more precise.
Some of the PCR-positive samples in study IV had amplification curves of a non-exponential shape and were classified as borderline-positive. There is no clear explanation for why the shapes of these curves differed from the others. These samples may simply contain very small amounts of target DNA, as the cycle number at which fluorescence exceeded the threshold level was usually high, or the difference could be due to the presence of PCR inhibitors, such as blood, ions and salts, in the samples, which prevent amplification. To evaluate this possibility, 6 samples with borderline results were tested for inhibitors (data not shown). Added pneumococcal DNA could be amplified in each sample without any problems, indicating that the borderline results with atypical amplification curves were not due to the presence of inhibitors in the samples.
6.2 Samples and sample preparation
In the studies I, II and V, MEF samples collected as part of the FinOM studies during the years 1994-1999 from children with AOM were analysed. The samples had been cultured immediately after myringotomy and stored at -70°C for subsequent analyses. Despite storage at -70°C, partial degradation of DNA may have occurred prior to PCR analyses, thus affecting particularly the quantitative real-time PCR results in study II. There is also a possibility that the qualitative PCR result of some samples initially containing very small amounts of pneumococci may have been falsely negative.
The nasopharyngeal samples analysed in the studies III and IV had been collected into STGG transport tubes and cultured more than two years prior to the real-time PCR analyses. After culturing, the samples had been stored at -80°C. The recovery of pneumococcus from nasopharyngeal secretion samples stored in STGG medium by culture has been studied by O’Brien et al. (2001), who showed that the storage of STGG samples at -80°C was favourable, especially for low colony counts. When the survival of S. pneumoniae frozen in STGG medium was studied using semiquantitative cultures, the bacteria were found to remain culturable without obvious loss of colony numbers after 36 months of storage (Kaijalainen et al., In press). On the basis of these findings, the comparison of PCR findings to the culture findings obtained 2 years earlier was considered justifiable. However, despite the storage at -80°C, partial degradation of the pneumococcal DNA present in the nasopharyngeal swab samples of this study might have occurred during the 2 years and may have caused some underestimation of the numbers of pneumococci by real-time PCR. The nasopharyngeal samples were also collected with calcium alginate swabs, which have been reported to inhibit some PCR assays (Wadowsky et al. 1994). In this study, the possible effect of calcium alginate swabs on qualitative and quantitative PCR results was not studied. However, 100% and 96% of the culture-positive samples were positive by real-time PCR in the studies III and IV,

64
respectively. Thus, calcium alginate swabs do not appear to produce false negative results in the culture-positive samples.
Sample preparation is an important step when performing PCR, and particularly when performing quantitative PCR. The boiling method for preparation was tested in study I and based on the findings of that study used in the studies II and V. It is a convenient method for large studies because it is a fast, easy and inexpensive way to release DNA from cells. However, boiling does not remove the possible inhibitors of PCR present in some MEF samples, particularly those containing blood. The presence of inhibiting substances may lead to a complete absence of amplification products, i.e. a false negative result, or have a quantitative effect. The presence of PCR inhibitors in a sample can be studied by amplifying a different endogenous target fragment, by spiking the sample with purified DNA or by running a dilution series on the sample (Rasmussen 2001). In study II, the presence of inhibitors in the boiled MEF samples was studied by spiking four negative samples with purified pneumococcal DNA. In all the four samples, the expected amounts of genome equivalents were detected, indicating that there was no major inhibition of the real-time PCR reaction. However, the amount of PCR inhibitors present in clinical samples may vary, and since only a few samples were tested for inhibitors, the possibility for some false-negative PCR findings in study II cannot be completely excluded. In study V, 23 samples had a positive pneumococcal culture, but negative result in conventional ply-PCR, and they were reanalysed by real-time ply-PCR using DNA purified from the MEF samples. All the 23 samples were positive in real-time ply-PCR, but two of them only after a re-analysis with the real-time PCR method. These 23 MEF samples evidently contained components that inhibited the initial ply-PCR and thus produced negative PCR results. In addition, some of the 23 samples contained a small number of pneumococci, which, together with PCR inhibitors, probably produced repeatedly false negative ply-PCR results.
Extraction of bacterial DNA from clinical samples may be complicated, because the quality of clinical samples varies. Since sample preparation is an important step when performing quantitative PCR, the impact of the DNA extraction method applied to the quantitative results obtained by real-time PCR was studied with 50 nasopharyngeal swab samples (III). All the three DNA extraction methods tested in study III were found to be suitable for sample preparation prior to real-time PCR, but the quantitative results obtained in the different DNA extracts of the same nasopharyngeal samples varied. The extracts prepared by the KingFisher DNA extraction instrument and kit produced the highest number of genome equivalents in 67% of the specimens. The MagNAPure LC instrument was not available in the present study, which probably affected the quantification results obtained by using the MagNAPure kit. When using the MagNA LC instrument, the incubation times may be longer and the washing procedures more effective than those performed manually. However, the PickPen magnetic particle transfer device proved to be good for collecting the magnetic particles and convenient when a small number of samples is studied. The nasopharyngeal samples analysed in study III were a relatively “easy” type of specimen. If blood samples were studied, the sensitivities and differences in quantification results might be completely different, as blood samples contain many inhibitors of PCR reaction (Abu Al-Soud et al. 2000, Abu Al-Soud & Rådström 2001) that may be difficult to remove. The concentration of bacterial DNA is possibly also lower in blood samples than in nasopharyngeal specimens.

65
6.3 Comparison of PCR and culture findings
In the studies I and II, all MEF samples from which pneumococcus was cultured were also positive by ply-PCR, regardless of the method used for the identification of the amplification products. PCR was, however, clearly more sensitive than bacterial culture in the detection of pneumococcus from MEF; 55% and 27% of the culture-negative samples were PCR-positive in the studies I and II, respectively. In study I, the proportion of positive samples increased from 24% by culture to 66% by PCR. In study II, the corresponding percentages were 34 by culture, 52 by real-time PCR and 54 by conventional PCR and TRF detection. Previously, it has been shown that PCR considerably increases the number of positive pneumococcal findings in MEF samples compared to culture: Virolainen et al. (1994) found 18% of MEF samples to be positive by culture and 30% by culture and PCR. Even the detection of pneumococcal capsular antigens in MEF by immunochemical methods has shown increased sensitivity compared to pneumococcal culture (Luotonen et al. 1981).
When the 400 nasopharyngeal swab specimens were analysed in study IV, the percentage of positive samples identified by real-time PCR (69%) was clearly higher than that obtained by culture (40%). Seven of the culture-positive samples were negative by real-time PCR and when these samples were recultured, 3 of them did not grow. Originally, 6 of these 7 samples had had a minimal colony count (<10) and one had had a colony count of less than 100. All of the four recovered pneumococcal strains were positive by real-time PCR, and the lack of the ply gene could thus not be the reason for the negative PCR finding in the culture-positive nasopharyngeal swab samples. When tested for PCR inhibitors by spiking with purified pneumococcal DNA, all but one of the four samples were positive for pneumococcus. The only sample with no amplification at all seems to have contained inhibitors not liable to elimination by the Chelex procedure employed in study IV.
PCR methods based on the amplification of ply or other pneumococcal genes have been shown to be sensitive and reliable in detecting pneumococcus in other specimen types (Rudolph et al. 1993, Virolainen et al. 1994, Salo et al. 1995, Kearns et al. 1999, Greiner et al. 2001) and in the identification of cultured bacteria (McAvin et al. 2001). Kontiokari et al. (2000) investigated the nasopharyngeal carriage of S. pneumoniae in infected rats and found that the number of positive samples increased by about one third when culture and PCR were used simultaneously. The results of the present study are thus in agreement with the earlier studies on this field.
In study II, the lowest number of genome equivalents/µl detected by real-time PCR in culture-positive MEF samples was 90. The number of genomes detected in culture-negative MEF samples was below this in all but one of the nine samples. In study III, the quantification results in pneumococcal culture-positive nasopharyngeal swab samples varied from below 1 to 2.2 × 103 genome equivalents/µl. In culture-negative samples, below 70 genome equivalents/µl were detected in all but one of the samples. In this exceptional sample, the quantification result was of the order of 103 in all the three DNA extracts tested. The results indicate that PCR-positive samples from which pneumococci were not found by culture generally contain small numbers of bacteria. The results also suggest that real-time PCR is more sensitive than culture in detecting pneumococcus in

66
MEF and nasopharyngeal swab samples. The comparison of quantitative results obtained by real-time PCR and culture analysis of 10-fold dilutions of a pneumococcal broth culture in STGG medium showed that when the DNA was purified using a DNA extraction kit (QIAamp, QIAGEN), at least ten-fold numbers of pneumococcal genomes could be detected by real-time PCR compared to the number of colonies detected by quantitative culture on plates (III). When the same 10-fold dilutions of the broth culture in STGG medium were treated for PCR by boiling in a 5% Chelex 100 solution, real-time PCR detected 2- to 10-fold numbers of pneumococcal genomes compared to the colonies detected by culture. One explanation for the discrepancy between the real-time PCR and culture results might be that PCR is also able to detect dead bacteria – autolysis is a typical feature for pneumococcus – and bacteria with impaired viability are possibly present in samples. In addition, pneumococci grow in pairs and short chains, and more than one bacterium could therefore contribute to the formation of a colony. PCR, on the other hand, detects DNA from each bacterium separately.
The high percentage of samples positive by PCR could be due to the presence of the pneumolysin gene in other α-haemolytic streptococci, which are common colonisers of the respiratory tract. Alpha-haemolytic streptococci have been shown to harbor the pneumolysin gene occasionally and thus to form a potential source for false positive findings in PCR based on the detection of the pneumolysin gene (Whatmore et al. 2000). Greiner et al. (2001) recently described a real-time PCR method for the demonstration and quantification of S. pneumoniae, and when they tested the specificity of the assay with ten non-pneumococcal strains, they detected minor amplification of the DNA of α-haemolytic streptococci. However, in MEF samples obtained during AOM, other α-haemolytic streptococci are not commonly found: in the FinOM Cohort Study, α-haemolytic streptococci were isolated in less than 2% of MEF samples (Kilpi et al. 2001). Thus, α−haemolytic streptococci cannot be responsible for a significant proportion of positive PCR results in MEF samples. As mainly small numbers of genome equivalents were present in culture-negative, PCR-positive MEF and nasopharyngeal swab samples, a lower sensitivity of culture compared to PCR rather than the presence of other bacteria containing the pneumolysin gene could be the reason for the discrepant findings.
6.4 Presence of pneumococcal DNA in MEF samples (V)
In study V, where over 2500 MEF samples were analysed, ply-PCR was confirmed to be a sensitive method in detecting pneumococcal DNA. Pneumococcal findings during AOM increased with PCR detection by 76% compared to culture alone. In an earlier study of Virolainen et al. (1994), the increase was quite similar, 64%. In otitis media with effusion (OME), the number of pneumococcal findings has also been found to increase several-fold when PCR was used compared to culture (Post et al. 1995, Jero et al. 1996).
In study V, the PCR-positive, culture-negative AOM events represented a less severe type of disease compared to culture-positive events. The PCR-positive, culture-negative findings could, at least partly, be explained by the presence of non-culturable pneumococci remaining in the middle ear after previous AOM events. The persistence of

67
ply-PCR positivity was shown to be time-dependent and to wane gradually. In addition, concurrent nasopharyngeal carriage, antibiotic treatment and MEF dilution (MEF samples collected to 0.7 ml of buffer) could all contribute to PCR positivity in culture-negative samples.
To avoid false-positive PCR findings due to subjective interpretation, the agarose gel results of study V were interpreted and recorded by two laboratory technicians. Samples with a positive result were reamplified and analysed using microwell hybridisation with Europium-labelled probes. In study V, the cut-off value for positivity was set as twice the mean of the time-resolved fluorescence counts of the negative controls included in each run. The computer-controlled fluorometer automatically subtracted the background of all samples and negative and positive controls.
In the FinOM studies, a special emphasis was placed on the optimal isolation of S. pneumoniae from MEF samples (Kilpi et al. 2001). However, even in the most optimal circumstances, the sensitivity of pneumococcal culture is not perfect. Antibiotic treatment decreases the yield of conventional culture methods. In study V, current antibiotic treatment was associated with an increased proportion of PCR-positive, culture-negative samples. Interestingly, no association was found with the previous antibiotic treatment, suggesting that dead bacteria are efficiently removed from the middle ear cavity. The number of samples remaining culture-negative due to antibiotic treatment was low and, thus, not enough to explain the high number of PCR-positive, culture-negative samples.
Pneumolysin is produced by virtually all pneumococcal isolates (Kanclerski & Möllby 1987). Gram-positive bacteria producing thiol-activated cytolysins structurally related to pneumolysin (Billington et al. 2000) could yield positive results in ply-PCR analyses, although the primers used in the current PCRs have turned out to be highly specific (Salo et al. 1995). In study V, five of the seven MEF samples with a pure Streptococcus group A culture finding were positive for pneumolysin by PCR. Group A Streptococcus produces streptolysin O with high sequence homology with pneumolysin (Kehoe et al. 1987); however, none of the Streptococcus group A isolates cultured from the MEF samples of study V were positive in ply-PCR.
In a chinchilla model, it has been shown that DNA from dead bacteria does not remain detectable in MEF. In this study by Post et al. (1996), ears inoculated with purified DNA from pneumococcus and H. influenzae or with killed M. catarrhalis turned PCR-negative after three days. However, when ears were inoculated with living pneumococcus or H. influenzae, PCR remained positive for up to 3 weeks despite antimicrobial treatment and the presence of culture-negative effusions after three days (Post et al. 1996). In study V, the PCR positivity rate of MEF samples decreased over time after a culture-confirmed pneumococcal AOM. The MEF samples – culture-negative for pneumococcus - included in the analysis were not obtained systematically but for clinical reasons. It is possible that these MEF samples were from more severe cases, e.g. those prone to recurrent AOM. Even so, the decreasing trend in DNA positivity suggests that DNA remnants are removed from the middle ear cavity after the resolution of the otitis episode. Although non-viable bacteria and isolated DNA do survive in the middle ear longer than for a few days, it is still possible that their continuous entry from the nasopharynx may produce positive results in PCR.
Although PCR is able to detect both dead and viable bacteria, PCR-positive, culture-negative otitis events have, in some cases, been shown to be caused by metabolically

68
active bacteria: messenger RNA (mRNA) that has a half-life of seconds to a few minutes of H. influenzae has been detected by reverse transcriptase-PCR in PCR-positive, culture-negative samples from ears with chronic otitis media with effusion (Rayner et al. 1998). However, it has also been suggested that the middle ear effusion could possess nuclease-inhibiting activity, which could allow both DNA and mRNA to persist longer in MEF than previously anticipated (Peizhong et al. 2000).
The presence of bacterial biofilms on mucosal membranes has been proposed as an explanation for cases positive by PCR, yet negative by culture (Post 2001, Ehrlich et al. 2002). In a biofilm, the bacteria may form a complex bacterial community attached to the middle ear epithelium and covered by a protective polysaccharide matrix. These biofilms are resistant to antimicrobials and immune defence mechanisms. While in the biofilm phenotype, the bacteria are less active regarding their interactions with the environment and more difficult to isolate in culture. The bacteria may survive in the middle ear as biofilms for long periods. The results of this study support the biofilm theory, since dormant pneumococci after culture-positive AOM may reside in the middle ear and be detected by PCR but not by culture. On the other hand, a high proportion of samples were PCR-positive and culture-negative in the absence of documented previous culture-confirmed pneumococcal AOM or even in the absence of any previous documented AOM. At present, nothing is known about the kinetics of biofilm formation, and it is thus naturally possible that biofilms have already developed before the first MEF sample was taken. Other types of mechanisms may also explain this phenomenon. The less severe clinical disease could be associated with the biofilm formation and insidious onset of the disease, but also with the theory of ascending non-replicating pneumococci from the nasopharynx as secondary invaders.
6.5 Future research
The quantitative real-time PCR method developed in this study could be further improved by introducing an internal control into the real-time method (Rosenstraus et al. 1998, Stöcher et al. 2003). The LightCycler instrument allows the sequence-specific detection of two separate DNA targets, and the internal control could thus be amplified simultaneously with the specific target. This would enable testing for inhibitors in all samples. However, amplification of multiple targets simultaneously may decrease the sensitivity of PCR. Therefore, the introduction of an internal control to the real-time ply-PCR assay requires careful planning and optimization for finding the right concentration of internal control needed for optimal results. An internal control could also be introduced in the microwell hybridisation method described in study I, since hybridisation probes labelled with different lanthanides can be detected in the same solution after a single hybridisation reaction (Iitiä et al. 1992).
The real-time PCR method developed in this study for detecting pneumococci from MEF and nasopharyngeal swab samples should also be tested with other specimen types. The use of the method for detecting pneumococcal DNA in blood or other samples of patients suffering from invasive pneumococcal disease, such as pneumonia, should be

69
studied. Quantification may offer new possibilities to distinguish between carriers of pneumococci and people suffering from pneumococcal disease.
The possibility of false positive ply-PCR findings due to α-haemolytic streptococci harbouring the pneumolysin gene needs to be studied further. Preliminary results suggest that, at least in some cases, α-hemolytic streptococci giving positive PCR findings for pneumolysin can be distinguished from pneumococcus by analysing the melting curves of amplification products in real-time PCR: they seem to contain a slightly modified form of the target fragment of the pneumolysin encoding gene (Kaijalainen et al., manuscript in preparation). To exclude the possibility that the positive PCR findings in culture-negative samples are due to the presence of the ply gene in other α-hemolytic streptococci, quantitative real-time PCR methods to demonstrate the presence of capsular genes of the most common serotypes (those present in 7- and 11-valent conjugate vaccines) are under development.
S. pneumoniae is part of the normal flora of the human nasopharynx. It has been shown that most children become colonized before their second birthday (Gray et al. 1980, Syrjänen et al. 2001). The frequency and significance of multiple carriage of different pneumococcal serotypes are not well known, at least partly due to the laborious and expensive culturing and serotyping methods (Huebner et al. 2000). As soon as specific primers and probes for different pneumococcal serotypes have been designed and optimized, real-time PCR may also be used to demonstrate and quantify the carriage of multiple serotypes.
To elucidate both the pathogenetic mechanism and the clinical significance of PCR diagnosis, further studies both in animal models and in clinical samples, using quantitative, real-time PCR for the demonstration of pneumococcal DNA and mRNA during acute otitis media are needed.

7 Conclusions
With the real-time PCR method developed in this study, pneumococci could be rapidly detected and quantified directly from patient samples. The assay provides information about the differences between the numbers of bacteria in samples and is a good aid in research where an accurate and sensitive pneumococcal diagnosis is needed. The fastness and sensitivity of real-time PCR speaks for its use in the demonstration of S. pneumoniae both in carriers and in clinical samples. Real-time PCR may even provide a new rapid and sensitive tool for the diagnosis of severe, invasive pneumococcal infection.
Real-time PCR based on the amplification of a pneumolysin gene fragment was more sensitive than culture in the demonstration of pneumococcus in nasopharyngeal samples regardless of the DNA extraction method used. However, the quantitative results were shown to be dependent on the DNA extraction method applied. Thus, when performing quantitative PCR experiments, the DNA extraction method used should be evaluated carefully. It should also be remembered that the numbers of genome equivalents reported in quantitative PCR should not be considered as absolute values because of possible differences in amplification efficiency between samples and standards and because of random variation particularly in samples containing small copy numbers of target DNA.
Conventional ply-PCR combined with microwell hybridisation was found to be a highly sensitive method for detecting pneumococcal DNA in middle ear fluid samples. A positive finding seems to indicate the presence of viable, although often non-culturable pneumococci within the middle ear cleft. Positive PCR findings may be derived from a previous pneumococcal infection remaining in the middle ear probably as a biofilm phenotype. Other mechanisms are also possible because PCR findings are commonly obtained from MEF of children with no previous documented pneumococcal AOM. The PCR-positive AOM clearly represents a clinically less active pneumococcal disease compared to the culture-positive cases.

References
Abu Al-Soud W, Jönsson LJ & Rådström P (2000) Identification and characterization of immunoglobulin G in blood as a major inhibitor of diagnostic PCR. J Clin Microbiol 38: 345-350.
Abu Al-Soud W & Rådström P (2001) Purification and characterization of PCR-inhibitory components in blood cells. J Clin Microbiol 39: 485-493.
Adegbola RA, Obaro SK, Biney E & Greenwood BM (2001) Evaluation of Binax NOW Streptococcus pneumoniae urinary antigen test in children in a community with a high carriage rate of pneumococcus. Ped Infect Dis J 20: 718-719.
Agrawal A, Shrive AK, Greenhough TJ & Volanakis JE (2001) Topology and structure of the C1q-binding site on C-reactive protein. J Immunol 166: 3998-4004.
AlonsoDeVelasco E, Verheul AFM, Verhoef J & Snippe H (1995) Streptococcus pneumoniae: virulence factors, pathogenesis, and vaccines. Microbiol Rev 59: 591-603.
American Academy of Pediatrics, Committee on Infectious Diseases (2000) Policy statement: recommendations for the prevention of pneumococcal infections, including the use of pneumococcal conjugate vaccine (Prevnar), pneumococcal polysaccharide vaccine, and antibiotic prophylaxis. Pediatrics 106: 362-366.
Angel CS, Ruzek M & Hostetter MK (1994) Degradation of C3 by Streptococcus pneumoniae. J Infect Dis 170: 600-608.
Aniasson G, Alm B, Andersson B, Larsson P, Nylén O, Peterson H, Rignér P, Svanborg M & Svanborg C (1992) Nasopharyngeal colonization during the first years of life. J Infect Dis 165: S38-42.
Arrecubieta C, Garcia E & Lopez R (1995) Sequence and transcriptional analysis of a DNA region involved in the production of capsular polysaccharide in Streptococcus pneumoniae type 3. Gene 167: 1-7.
Arrecubieta C, Lopez R & Garcia E (1996) Type 3-specific synthase of Streptococcus pneumoniae (Cap3B) directs type 3 polysaccharide biosynthesis in Escherichia coli and in pneumococcal strains of different serotypes. J Exp Med 184: 449-455.
Austrian R (1977) Prevention of pneumococcal infection by immunization with capsular polysaccharides of Streptococcus pneumoniae: current status of polyvalent vaccines. J Infect Dis 136 Suppl: S38-42.
Austrian R (1981) Pneumococcus: the first one hundred years. Rev Infect Dis 3: 183-189. Austrian R (1986) Some aspects of the pneumococcal carrier state. J Antimicr Chemother 18: 35-
45. Austrian R, Douglas RM, Schiffman G, Coetzee AM, Koornhof HJ, Hayden-Smith S & Reid RD
(1976) Prevention of pneumococcal pneumonia by vaccination. Trans Assoc Am Physicians 89: 184-194.

72Austrian R & Gold J (1964) Pneumococcal bacteremia with especial reference to bacteremic
pneumococcal pneumonia. Ann Intern Med 60: 759-776. Avery OT, MacLeod CM & McCarty M (1944) Studies on the chemical nature of the substance
inducing transformation of pneumococcal types. Induction of transformation by a desoxyribonucleic acid fraction isolated from pneumococcus type III. J Exp Med 5: 137-157.
Balachandran P, Brooks-Walter A, Virolainen-Julkunen A, Hollingshead SK & Briles DE (2002) Role of pneumococcal surface protein C in nasopharyngeal carriage and pneumonia and its ability to elicit protection against carriage of Streptococcus pneumoniae. Infect Immun 70: 2526-2534.
Balachandran P, Hollingshead SK, Paton JC & Briles DE (2001) The autolytic enzyme LytA of Streptococcus pneumoniae is not responsible for releasing pneumolysin. J Bacteriol 183: 3108-3116.
Baraff LJ, Lee SI & Schriger DL (1993) Outcomes of bacterial meningitis in children: a meta-analysis. Pediatr Infect Dis J 12: 389-394.
Barnes DM, Whittier S, Gilligan PH, Soares S, Tomasz A & Henderson FW (1995) Transmission of multidrug-resistant serotype 23F Streptococcus pneumoniae in group day care: evidence suggesting capsular transformation of the resistant strain in vivo. J Infect Dis 171: 890-896.
Bartlett JG & Mundy LM (1995) Community-acquired pneumonia. N Engl J Med 333: 1618-1624. Bernard PS, Pritham GH & Wittwer CT (1999) Color multiplexing hybridization probes using the
apolipoprotein E locus as a model system for genotyping. Anal Biochem 273: 221-228. Berry AM, Paton JC & Hansman D (1992) Effect of insertional inactivation of the genes encoding
pneumolysin and autolysin on the virulence of Streptococcus pneumoniae type 3. Microb Pathog 12: 87-93.
Berry AM, Yother J, Briles DE, Hansman D & Paton JC (1989) Reduced virulence of a defined pneumolysin-negative mutant of Streptococcus pneumoniae. Infect Immun 57: 2037-2042.
Billington SJ, Jost BH & Songer JG (2000) Thiol-activated cytolysins: structure, function and role in pathogenesis. FEMS Microbiol Lett 182: 197-205.
Black S, Shinefield H, Fireman B, Lewis E, Ray P, Hansen JR, Elvin L, Ensor KM, Hackell J, Siber G, Malinoski F, Madore D, Chang I, Kohberger R, Watson W, Austrian R & Edwards K (2000) Efficacy, safety and immunogenicity of heptavalent pneumococcal conjugate vaccine in children. Northern California Kaiser Permanente Vaccine Study Center Group. Pediatr Infect Dis J 19: 187-195.
Bluestone CD, Stephenson JS & Martin LM (1992) Ten-year review of otitis media pathogens. Pediatr Infect Dis J 11: S7-11.
Boersma WG, Löwenberg A, Holloway Y, Kuttschrütter H, Snijder JAM & Koëter GH (1991) Pneumococcal capsular antigen detection and pneumococcal serology in patients with community acquired pneumonia. Thorax 46: 902-906.
Boersma WG, Löwenberg A, Holloway Y, Kuttschrütter H, Snijder JAM & Koëter GH (1993) Rapid detection of pneumococcal antigen in pleural fluid of patients with community acquired pneumonia. Thorax 42: 160-162.
Bogaert D, Engelen MN, Timmers-Reker AJ, Elzenaar KP, Peerbooms PG, Coutinho RA, de Groot R & Hermans PW (2001) Pneumococcal carriage in children in The Netherlands: a molecular epidemiological study. J Clin Microbiol 39: 3316-3320.
Boulnois GJ, Paton JC, Mitchell TJ & Andrew PW (1991) Structure and function of pneumolysin, the multifunctional, thiol-activated toxin of Streptococcus pneumoniae. Molecular Microbiol 5: 2511-2516.
Briese T & Hakenbeck R (1985) Interaction of the pneumococcal amidase with lipoteichoic acid and choline. Eur J Biochem 146: 417-427.
Briles DE, Ades E, Paton JC, Sampson JS, Carlone GM, Huebner RC, Virolainen A, Swiatlo E & Hollingshead SK (2000) Intranasal immunization of mice with a mixture of the pneumococcal proteins PsaA and PspA is highly protective against nasopharyngeal carriage of Streptococcus pneumoniae. Infect Immun 68: 796-800.
Briles DE, Yother J & McDaniel LS (1988) Role of pneumococcal surface protein A in the virulence of Streptococcus pneumoniae. Rev Infect Dis 10: S372-374.

73Brito DA, Ramirez M & de Lencastre H (2003) Serotyping Streptococcus pneumoniae by multiplex
PCR. J Clin Microbiol 41: 2378-2384. Bromberg K, Tannis G & Rodgers A (1990) Pneumococcal C and type polysaccharide detection in
the concentrated urine of patients with bacteremia. Med Microbiol Immunol 179: 335-338. Brooks-Walter A, Briles DE & Hollingshead SK (1999) Thr pspC gene of Streptococcus
pneumoniae encodes a polymorphic protein, PspC, which elicits cross reactive antibodies to PspA and provides immunity to pneumococcal bacteremia. Infect Immun 67: 6533-6542.
Bruyn GAW (1992) Mechanisms of host defence against infection with Streptococcus pneumoniae. Clin Infect Dis 14: 251-262.
Bruyn GAW & van Furth R (1991) Pneumococcal polysaccharide vaccines: indications, efficacy and recommendations. Eur J Clin Microbiol Infect Dis 10: 897-910.
Butler JC & Schuchat A (1999) Epidemiology of pneumococcal infections in the elderly. Drugs Aging 15 Suppl 1: 11-19.
Bäckman A, Lantz P, Rådström P & Olcén P (1999) Evaluation of an extended diagnostic PCR assay for detection and verification of the common causes of bacterial meningitis in CSF and other biological samples. Mol Cell Probes 13: 49-60.
Campos JM (1989) Detection of bloodstream infections in children. Eur J Clin Microbiol Infect Dis 8: 815-824.
Celin SE, Bluestone CD, Stephenson J, Yilmaz HM & Collins JJ (1991) Bacteriology of acute otitis media in adults. JAMA 266: 2249-2252.
Cheng Q, Finkel D & Hostetter MK (2000) Novel purification scheme and functions for a C3-binding protein from Streptococcus pneumoniae. Biochemistry 39: 5450-5457.
Cherian T, Lalitha MK, Manoharan A, Thomas K, Yolken RH & Steinhoff MC (1998) PCR-Enzyme immunoassay for detection of Streptococcus pneumoniae DNA in cerebrospinal fluid samples from patients with culture-negative meningitis. J Clin Microbiol 36: 3605-3608.
Chudwin DS, Artrip SG, Korenblit A, Schiffman G & Rao S (1985) Correlation of serum opsonins with in vitro phagocytosis of Streptococcus pneumoniae. Infect Immun 50: 213-217.
Clements H & Stephenson TJ (1996) Blood culture is poor method of confirming pneumococcus as cause of childhood pneumonia. BMJ 313: 757.
Coffey TJ, Dowson CG, Daniels M, Zhou J, Martin C, Spratt BG & Musser JM (1991) Horizontal transfer of multiple penicillin-binding protein genes, and capsular biosynthetic genes, in natural populations of Streptococcus pneumoniae. Mol Microbiol 5: 2255-2260.
Coffey TJ, Enright MC, Daniels M, Morona JK, Morona R, Hryniewicz W, Paton JC & Spratt BG (1998a) Recombinational exchanges at the capsular polysaccharide biosynthetic locus lead to frequent serotype changes among natural isolates of Streptococcus pneumoniae. Mol Microbiol 27: 73-83.
Coffey TJ, Enright MC, Daniels M, Wilkinson P, Berron S, Fenoll A & Spratt BG (1998b) Serotype 19A variants of the Spanish serotype 23F multiresistant clone of Streptococcus pneumoniae. Microb Drug Resist 4: 51-55.
Corless CE, Guiver M, Borrow R, Edwards-Jones V, Fox AJ & Kaczmarski EB (2001) Simultaneous detection of Neisseria meningitidis, Haemophilus influenzae, and Streptococcus pneumoniae in suspected cases of meningitis and septicemia using real-time PCR. J Clin Microbiol 39: 1553-1558.
Crain MJ, Waltman WD, 2nd, Turner JS, Yother J, Talkington DF, McDaniel LS, Gray BM & Briles DE (1990) Pneumococcal surface protein A (PspA) is serologically highly variable and is expressed by all clinically important capsular serotypes of Streptococcus pneumoniae. Infect Immun 58: 3293-3299.
Cundell DR, Weiser JN, Shen J, Young A & Tuomanen EI (1995) Relationship between colonial morphology and adherence of Streptococcus pneumoniae. Infect Immun 63: 757-761.
Dagan R & Fraser D (2000) Conjugate pneumococcal vaccine and antibiotic-resistant Streptococcus pneumoniae: herd immunity and reduction of otitis morbidity. Pediatr Infect Dis J 19: S79-87; discussion S88.
Dagan R, Fraser D, Givon N & Yagupsky P (1999) Carriage of resistant pneumococci by children in southern Israel and impact of conjugate vaccines on carriage. Clin Microbiol Infect 5 Suppl 4: S29-S37.

74Dagan R, Melamed R, Muallem M, Piglansky L, Greenberg D, Abramson O, Mendelman PM,
Bohidar N & Yagupsky P (1996) Reduction of nasopharyngeal carriage of pneumococci during the second year of life by a heptavalent conjugate pneumococcal vaccine. J Infect Dis 174: 1271-1278.
Dagan R, Shriker O, Hazan I, Leibovitz E, Greenberg D, Schlaeffer F & Levy R (1998) Prospective study to determine clinical relevance of detection of pneumococcal DNA in sera of children by PCR. J Clin Microbiol 36: 669-673.
van Dam JEG, Fleer A & Snippe H (1990) Immunogenicity and immunochemistry of Streptococcus pneumoniae capsular polysaccharides. Antonie van Leeuvenhoek 58: 1-47.
Dave S, Brooks-Walter A, Pangburn MK & McDaniel LS (2001) PspC, a pneumococcal surface protein, binds human factor H. Infect Immun 69: 3435-3437.
de Franchis R, Cross NC, Foulkes NS & Cox TM (1988) A potent inhibitor of Taq polymerase copurifies with human genomic DNA. Nucleic Acids Res 16: 10355.
Dillard JP, Vandersea MW & Yother J (1995) Characterization of the cassette containing genes for type 3 capsular polysaccharide biosynthesis in Streptococcus pneumoniae. J Exp Med 181: 973-983.
Dingman JR, Rayner MG, Mishra S, Zhang Y, Ehrlich MD, Post JC & Ehrlich GD (1998) Correlation between presence of viable bacteria and presence of endotoxin in middle-ear effusions. J Clin Microbiol 36: 3417-3419.
Domínguez J, Galí N, Blanco S, Pedroso P, Prat C, Matas L & Ausina V (2001) Detection of Streptococcus pneumoniae antigen by rapid immunochromatographic assay in urine samples. Chest 119: 243-249.
Dowell SF, Garman RL, Liu G, Levine OS & Yang YH (2001) Evaluation of Binax NOW, an assay for the detection of pneumococcal antigen in urine sampels, performed among pediatric patients. Clin Infect Dis 32: 824-825.
Drew WL (1977) Value of sputum culture in diagnosis of pneumococcal pneumonia. J Clin Microbiol 6: 62-65.
du Plessis M, Smith AM & Klugman KP (1998) Rapid detection of penicillin-resistant Streptococcus pneumoniae in cerebrospinal fluid by a seminested-PCR strategy. J Clin Microbiol 36: 453-457.
du Plessis M, Smith AM & Klugman KP (1999) Application of pbp1A PCR in identification of penicillin-resistant Streptococcus pneumoniae. J Clin Microbiol 37: 628-632.
Ehrlich GD, Veeh R, Wang X, Costerton JW, Hayes JD, Hu FZ, Daigle BJ, Ehrlich MD & Post JC (2002) Mucosal biofilm formation on middle-ear mucosa in the chinchilla model of otitis media. JAMA 287: 1710-1715.
Erlich HA, Gelfand D & Sninsky JJ (1991) Recent advances in the polymerase chain reaction. Science 252: 1643-1651.
Eskola J & Anttila M (1999) Pneumococcal conjugate vaccines. Pediatr Infect Dis J 18: 543-551. Eskola J, Kilpi T, Palmu A, Jokinen J, Haapakoski J, Herva E, Takala A, Käyhty H, Karma P,
Kohberger R, Siber G, Mäkelä PH & Group. atFOMFS (2001) Efficacy of a pneumococcal conjugate vaccine against acute otitis media. N Engl J Med 344: 403-409.
Eskola J, Käyhty H, Peltola H, Karanko V, Mäkelä PH, Samuelson J & Gordon LK (1985) Antibody levels achieved in infants by course of Haemophilus influenzae type b polysaccharide/diphtheria toxoid conjugate vaccine. Lancet 1: 1184-1186.
Eskola J, Takala AK, Kela E, Pekkanen E, Kalliokoski R & Leinonen M (1992) Epidemiology of invasive pneumococcal infections in children in Finland. JAMA 268: 3323-3327.
Faden H, Duffy L, Wasielewski R, Wolf J, Krystofik D, Tung Y & Pediatrics TW (1997) Relationship between nasopharyngeal colonization and the development of otitis media in children. J Infect Dis 175: 1440-1445.
Falguera M, Lopez A, Nogues A, Porcel JM & Rubio-Caballero M (2002) Evaluation of the polymerase chain reaction method for detection of Streptococcus pneumoniae DNA in pleural fluid samples. Chest 122: 2212-2216.
Feldman C, Mitchell TJ, Andrew PW, Boulnois GJ, Read RC, Todd HC, Cole PJ & Wilson R (1990) The effect of Streptococcus pneumoniae pneumolysin on human respiratory epithelium in vitro. Microb Pathog 9: 275-284.

75Fenoll A, Jado I, Vicioso D & Casal J (1997) Dot blot assay for the serotyping of pneumococci. J
Clin Microbiol 35: 764-766. Ferrante A, Rowan-Kelly B & Paton JC (1984) Inhibition of in vitro human lymphocyte response
by the pneumococcal toxin pneumolysin. Infect Immun 46: 585-589. Finland M (1969) Diagnostic lung puncture [editorial]. Pediatrics 44: 471-473. Fireman B, Black SB, Shinefield HR, Lee J, Lewis E & Ray P (2003) Impact of the pneumococcal
conjugate vaccine on otitis media. Pediatr Infect Dis J 22: 10-16. García A, Rosón B, Pérez JL, Verdaguer R, Dorca J, Carratalà J, Casanova A, Manresa F & Gudiol
F (1999) Usefulness of PCR and antigen latex agglutination test with samples obtained by transthoracic needle aspiration for diagnosis of pneumococcal pneumonia. J Clin Microbiol 37: 709-714.
García E, García JL, Ronda C, García P & López R (1985) Cloning and expression of the pneumococcal autolysin gene in Escherichia coli. Mol Gen Genet 201: 225-230.
García P, García JL, García E & López R (1986) Nucleotide sequence and expression of the pneumococcal autolysin gene from its own promoter in Escherichia coli. Gene 43: 265-272.
Gates GA (1999) Otitis media--the pharyngeal connection. JAMA 282: 987-989. Gibson JR, Saunders NA, Burke B & Owen RJ (1999) Novel method for rapid determination of
clarithromycin sensitivity in Helicobacter pylori. J Clin Microbiol 37: 3746-3748. Gibson LF & Khoury JT (1986) Storage and survival of bacteria by ultra-freeze. Letts Appl
Microbiol 3: 127-129. Gillespie SH (1989) Aspects of pneumococcal infection including bacterial virulence, host response
and vaccination. J Med Microbiol 28: 237-248. Gillespie SH, McHugh TD, Hughes JE, Dickens A, Kyi MS & Kelsey M (1997) An outbreak of
penicillin resistant Streptococcus pneumoniae investigated by a polymerase chain reaction based genotyping method. J Clin Pathol 50: 847-851.
Gillespie SH, Ullman C, Smith MD & Emery V (1994) Detection of Streptococcus pneumoniae in sputum samples by PCR. J Clin Microbiol 32: 1308-1311.
Givon-Lavi N, Fraser D, Porat N & Dagan R (2002) Spread of Streptococcus pneumoniae and antibiotic-resistant S. pneumoniae from day-care center attendees to their younger siblings. J Infect Dis 186: 1608-1614.
Glaister D (1991) Early detection of lower respiratory tract infection: the value of the Gram-stained sputum smear. Med Lab Sci 48: 175-177.
Gloffke W (2003) Quantitative PCR update. Reviewing the latest trends and applications in quantitative, real-time PCR. The Scientist 17: 41-43.
Gransden WR, Eykyn SJ & Phillips I (1985) Pneumococcal bacteraemia: 325 episodes diagnosed at St. Thomas’s Hospital. Br Med J (Clin Res Ed) 290: 505-508.
Gratten M, Gratten H, Poli A, Carrad E & Raymer M (1986) Colonisation of Haemophilus influenzae and Streptococcus pneumoniae in the upper respiratory tract of neonates in Papua New Guinea: Primary acquisition, duration of carriage, and relationship to carriage in mothers. Biol Neonate 50: 114-120.
Gray BM, Converse GM, Huhta N, Johnston RB, Pichichero ME, Schiffmann G & Dillon HC (1981) Epidemiologic studies of Streptococcus pneumoniae in infants: antibody response to nasopharyngeal carriage of types 3, 19, and 23. J Infect Dis 144: 312-318.
Gray BM, Converse GMI & Dillon Jr HC (1980) Epidemiologic studies of Streptococcus pneumoniae in infants: acquisition, carriage, and infection during the first 24 months of life. J Infect Dis 142: 923-933.
Gray BM & Dillon HC (1988) Epidemiological studies of Streptococcus pneumoniae in infants: antibody to types 3, 6, 14, and 23 in the first two years of life. J Infect Dis 158: 948-955.
Greiner O, Day PJ, Bosshard PP, Imeri F, Altwegg M & Nadal D (2001) Quantitative detection of Streptococcus pneumoniae in nasopharyngeal secretions by real-time PCR. J Clin Microbiol 39: 3129-3134.
Guidolin A, Morona JK, Morona R, Hansman D & Paton JC (1994) Nucleotide sequence analysis of genes essential for capsular polysaccharide biosynthesis in Streptococcus pneumoniae type 19F. Infect Immun 62: 5384-5396.

76Hammerschmidt S, Bethe G, Remane PH & Chhatwal GS (1999) Identification of pneumococcal
surface protein A as a lactoferrin-binding protein of Streptococcus pneumoniae. Infect Immun 67: 1683-1687.
Hammerschmidt S, Talay SR, Brandtzaeg P & Chhatwal GS (1997) SpsA, a novel pneumococcal surface protein with specific binding to secretory immunoglobulin A and secretory component. Mol Microbiol 25: 1113-1124.
Hassan-King M, Baldeh I, Secka O, Falade A & Greenwood B (1994) Detection of Streptococcus pneumoniae DNA in bood cultures by PCR. J Clin Microbiol 32: 1721-1724.
Hausdorff WP, Bryant J, Paradiso PR & Siber GR (2000) Which pneumococcal serogroups cause the most invasive disease: implications for conjugate vaccine formulation and use, part I. Clin Infect Dis 30: 100-121.
Hedlund J, Svenson SB, Kalin M, Henrichsen J, Olsson-Liljequist B, Möllerberg G & Källenius G (1995) Incidence, capsular types, and antibiotic susceptibility of invasive Streptococcus pneumoniae in Sweden. Clin Infect Dis 21: 948-953.
Heiskanen-Kosma T, Korppi M, Jokinen C, Kurki S, Heiskanen L, Juvonen H, Kallinen S, Stén M, Tarkiainen A, Rönnberg P-R, Kleemola M, Mäkelä PH & Leinonen M (1998) Etiology of childhood pneumonia: serologic results of a prospective, population-based study. Pediatr Infect Dis J 17: 986-991.
Hendley JO, Sande MA, Stewart PM & Gwaltney Jr. JM (1975) Spread of Streptococcus pneumoniae in families. I. Carriage rates and distribution of types. J Infect Dis 132: 55-61.
Hendolin PH, Markkanen A, Ylikoski J & Wahlfors JJ (1997) Use of multiplex PCR for simultaneous detection of four bacterial species in middle ear effusions. J Clin Microbiol 35: 2854-2858.
Henrichsen J (1995) Six newly recognized types of Streptococcus pneumoniae. J Clin Microbiol 33: 2759-2762.
Henrichsen J (1999) Typing of Streptococcus pneumoniae: past, present, and future. Am J Med 107: 50S-54S.
Herva E, Luotonen J, Timonen M, Sibakov M, Karma P & Mäkelä PH (1980) The effect of polyvalent pneumococcal polysaccharide vaccine on nasopharyngeal and nasal carriage of Streptococcus pneumoniae. Scand J Infect Dis 12: 97-100.
Holloway Y, Boersma WG, Kuttschrütter H & Snijder JAM (1993a) Detection of pneumococcal capsular antigen in the presence of penicillin in vitro. Scand J Infect Dis 25: 317-322.
Holloway Y, Snijder JA & Boersma WG (1993b) Demonstration of circulating pneumococcal immunoglogulin G immune complexes in patients with community-acquired pneumonia by means of an enzyme-linked immunosorbent assay. J Clin Microbiol 31: 3247-3254.
Holmberg H, Holme T, Krook A, Olsson T, Sjöberg L & Sjögren A-M (1985) Detection of C polysaccharide in Streptococcus pneumoniae in the sputa of pneumonia patients by an enzyme-linked immunosorbent assay. J Clin Microbiol 22: 111-115.
Honkanen PO, Keistinen T, Miettinen L, Herva E, Sankilampi U, Läärä E, Leinonen M, Kivelä S-L & P.H. M (1999) Incremental effectiveness of pneumococcal vaccine on simultaneously administered influenza vaccine in preventing pneumonia and pneumococcal pneumonia among persons aged 65 years or older. Vaccine 17: 2493-2500.
Hoshino K, Watanabe H, Sugita R, Asoh N, Ntabaguzi SA, Watanabe K, Oishi K & Nagatake T (2002) High rate of transmission of penicillin-resistant Streptococcus pneumoniae between parents and children. J Clin Microbiol 40: 4357-4359.
Hostetter MK (1986) Serotypic variations among virulent pneumococci in deposition and degradation of covalently bound C3b: implications for phagocytosis and antibody production. J Infect Dis 153: 682-693.
Houldsworth S, Andrew PW & Mitchell TJ (1994) Pneumolysin stimulates production of tumor necrosis factor alpha and interleukin-1 beta by human mononuclear phagocytes. Infect Immun 62: 1501-1503.
Howden R (1979) A rapid bile solubility test for pneumococci. J Clin Pathol 32: 1293-1294. Huebner RE, Dagan R, Porath N, Wasas AD & Klugman KP (2000) Lack of utility of serotyping
multiple colonies for detection of simultaneous nasopharyngeal carriage of different pneumococcal serotypes. Pediatr Infect Dis J 19: 1017-1020.

77Hughes JR, Sinha DP, Cooper MR, Shah KV & Bose SK (1969) Lung tap in childhood: bacteria,
viruses, and mycoplasmas in acute lower respiratory tract infections. Pediatrics 44: 477-485. Håkansson A, Roche H, Mirza S, McDaniel LS, Brooks-Walter A & Briles DE (2001)
Characterization of binding of human lactoferrin to pneumococcal surface protein A. Infect Immun 69: 3372-3381.
Höltje JV & Tomasz A (1976) Purification of the pneumococcal N-acetylmuramyl-L-alanine amidase to biochemical homogeneity. J Biol Chem 251: 4199-4207.
Iitiä A, Liukkonen L & Siitari H (1992) Simultaneous detection of two cystic fibrosis alleles using dual-label time-resolved fluorometry. Mol Cell Probes 6: 505-512.
Isaacman DJ, Karasic RB, Reynolds EA & Kost SI (1996) Effect of number of blood cultures and volume of blood on detection of bacteremia in children. J Pediatr 128: 190-195.
Isaacman DJ, Zhang Y, Reynolds E & Ehrlich G (1998) Accuracy of a polymerase chain reaction-based assay for detection of pneumococcal bacteremia in children. Pediatrics 101: 813-816.
Jackson LA, Neuzil KM, Yu O, Benson P, Barlow WE, Adams AL, Hanson CA, Mahoney LD, Shay DK & Thompson WW (2003) Effectiveness of pneumococcal polysaccharide vaccine in older adults. N Engl J Med 348: 1747-1755.
Jado I, Fenoll A, Casal J & Perez A (2001) Identification of the psaA gene, coding for pneumococcal surface adhesin A, in viridans group streptococci other than Streptococcus pneumoniae. Clin Diagn Lab Immunol 8: 895-898.
Jalava J, Skurnik M, Toivanen A, Toivanen P & Eerola E (2001) Bacterial PCR in the diagnosis of joint infection. Ann Rheum Dis 60: 287-289.
Jebbink J, Bai X, Rogers BB, Dawson DB, Scheuermann RH & Domiati-Saad R (2003) Development of real-time PCR assays for the quantitative detection of Epstein-Barr virus and cytomegalovirus, comparison of TaqMan probes, and molecular beacons. J Mol Diagn 5: 15-20.
Jero J, Virolainen A, Salo P, Leinonen M, Eskola J & Karma P (1996) PCR assay for detecting Streptococcus pneumoniae in the middle ear of children with otitis media with effusion. Acta Otolaryngol (Stockh) 116: 288-292.
Jiang SM, Wang L & Reeves PR (2001) Molecular characterization of Streptococcus pneumoniae type 4, 6B, 8, and 18C capsular polysaccharide gene clusters. Infect Immun 69: 1244-1255.
Johnson MK (1977) Cellular location of pneumolysin. FEMS Microbiol Lett 2: 243-245. Johnson MK, Geoffroy C & Alouf JE (1980) Binding of cholesterol by sulfhydryl-activated
cytolysins. Infect Immun 27: 97-101. Juvén T, Mertsola J, Waris M, Leinonen M, Meurman O, Roivainen M, Eskola J, Saikku P &
Ruuskanen O (2000) Etiology of community-acquired pneumonia in 254 hospitalised children. Pediatr Infect Dis J 19: 293-298.
Kaijalainen T, Rintamäki S, Herva E & Leinonen M (2002) Evaluation of gene-technological and conventional methods in the identification of Streptococcus pneumoniae. J Microbiol Methods 51: 111-118.
Kaijalainen T, Ruokokoski E, Ukkonen P & Herva E Survival of Streptococcus pneumoniae, Haemophilus influenzae and Moraxella catarrhalis frozen in STGG medium. J Clin Microbiol In Press.
Kalin M, Kanclerski K, Granström M & Möllby R (1987) Diagnosis of pneumococcal pneumonia by enzyme-linked immunosorbent assay of antibodies to pneumococcal hemolysin (pneumolysin). J Clin Microbiol 25: 226-229.
Kalin M & Lindberg AA (1983) Diagnosis of pneumococcal pneumonia: a comparison between microsopic examination of expectorate, antigen detection and cultural procedures. Scand J Infect Dis 15: 247-255.
Kalin M & Lindberg AA (1985) Antibody response against the type specific capsular polysaccharide in pneumococcal pneumonia measured by enzyme linked immunosorbent assay. Scand J Infect Dis 17: 25-32.
Kalin M, Lindberg AA & Tunevall G (1983) Etiological diagnosis of bacterial pneumonia by Gram stain and quantitative culture of expectorates. Scand J Infect Dis 15: 153-160.
Kanclerski K & Möllby R (1987) Production and purification of Streptococcus pneumoniae hemolysin (pneumolysin). J Clin Microbiol 25: 222-225.

78Kauppinen MT, Herva E, Kujala P, Leinonen M, Saikku P & Syrjälä H (1995) The etiology of
community-acquired pneumonia among hospitalized patients during a Chlamydia pneumoniae epidemic in Finland. J Infect Dis 172: 1330-1335.
Kearns AM, Freeman R, Murphy OM, Seiders PR, Steward M & Wheeler J (1999) Rapid PCR-based detection of Streptococcus pneumoniae DNA in cerebrospinal fluid [letter]. J Clin Microbiol 37: 3434.
Kearns AM, Graham C, Burdess D, Heatherington J & Freeman R (2002) Rapid real-time PCR for determination of penicillin susceptibility in pneumococcal meningitis, including culture-negative cases. J Clin Microbiol 40: 682-684.
Kearns AM, Wheeler J, Freeman R, Seiders PR, Perry J, Whatmore AM & Dowson CG (2000) Pneumolysin detection identifies atypical isolates of Streptococcus pneumoniae. J Clin Microbiol 38: 1309-1310.
Kehoe MA, Miller L, Walker JA & Boulnois GJ (1987) Nucleotide sequence of the streptolysin O (SLO) gene: structural homologies between SLO and other membrane-damaging, thiol-activated toxins. Infect Immun 55: 3228-3232.
Kerttula Y, Leinonen M, Koskela M & Mäkelä PH (1987) The aetiology of pneumonia. Application of bacterial serology and basic laboratory methods. J Infect 14: 21-30.
Kilpi T, Herva E, Kaijalainen T, Syrjänen R & Takala AK (2001) Bacteriology of acute otitis media in a cohort of Finnish children followed for the first two years of life. Pediatr Infect Dis J 20: 654-662.
Kim JO & Weiser JN (1998) Association of intrastrain phase variation in quantity of capsular polysaccharide and teichoic acid with the virulence of Streptococcus pneumoniae. J Infect Dis 177: 368-377.
Klaschik S, Lehmann LE, Raadts A, Book M, Hoeft A & Stuber F (2002) Real-time PCR for detection and differentiation of gram-positive and gram-negative bacteria. J Clin Microbiol 40: 4304-4307.
Klugman KP (2001) Efficacy of pneumococcal conjugate vaccines and their effect on carriage and antimicrobial resistance. Lancet Infect Dis 1: 85-91.
Kolkman MA, Wakarchuk W, Nuijten PJ & van der Zeijst BA (1997) Capsular polysaccharide synthesis in Streptococcus pneumoniae serotype 14: molecular analysis of the complete cps locus and identification of genes encoding glycosyltransferases required for the biosynthesis of the tetrasaccharide subunit. Mol Microbiol 26: 197-208.
Kontiokari T, Renko M, Kaijalainen T, Kuisma L & Leinonen M (2000) Comparison of nasal swab culture, quantitative culture of nasal mucosal tissue and PCR in detecting Streptococcus pneumoniae carriage in rats. APMIS 108: 734-738.
Korppi M, Heiskanen-Kosma T, Jalonen E, Saikku P, Leinonen M, Halonen P & Mäkelä PH (1993) Aetiology of community-acquired pneumonia in children treated in hospital. Eur J Pediatr 152: 24-30.
Korppi M, Koskela M, Jalonen E & Leinonen M (1992) Serologically indicated pneumoccal respiratory infection in children. Scand J Infect Dis 24: 437-443.
Korppi M & Leinonen M (1998) Pneumococcal immune complexes in the diagnosis of lower respiratory infections in children. Pediatr Infect Dis J 17: 992-995.
Kotilainen P, Jalava J, Meurman O, Lehtonen OP, Rintala E, Seppala OP, Eerola E & Nikkari S (1998) Diagnosis of meningococcal meningitis by broad-range bacterial PCR with cerebrospinal fluid. J Clin Microbiol 36: 2205-2209.
Krook A, Holmberg H & Sjögren AM (1987) A new coagglutination test for detecting pneumococcal C-polysaccharide. Eur J Clin Microbiol 6: 68-69.
Kuoppa Y, Boman J, Scott L, Kumlin U, Eriksson I & Allard A (2002) Quantitative detection of respiratory Chlamydia pneumoniae infection by real-time PCR. J Clin Microbiol 40: 2273-2274.
Kwok S & Higuchi R (1989) Avoiding false positives with PCR. Nature (London) 339: 237-238. Lankinen KS, Ruutu P, Nohynek H, Lucero M, Paton JC & Leinonen M (1999) Pneumococcal
pneumonia diagnosis by demonstration of pneumolysin antibodies in precipitated immune complexes: a study in 350 philippine children with acute lower respiratory infections. Scand J Infect Dis 31: 155-161.

79Lawrence ER, Arias CA, Duke B, Beste D, Broughton K, Efstratiou A, George RC & Hall LM
(2000) Evaluation of serotype prediction by cpsA-cpsB gene polymorphism in Streptococcus pneumoniae. J Clin Microbiol 38: 1319-1323.
Lawrence ER, Griffiths DB, Martin SA, George RC & Hall LM (2003) Evaluation of semiautomated multiplex PCR assay for determination of Streptococcus pneumoniae serotypes and serogroups. J Clin Microbiol 41: 601-607.
Leach AJ, Boswell JB, Asche V, Nienhuys TG & Mathews JD (1994) Bacterial colonization of the nasopharynx predicts very early onset and persistence of otitis media in Australia Aboriginal infants. Pediatr Infect Dis J 13: 983-989.
Lee CJ, Banks SD & Li JP (1991) Virulence, immunity, and vaccine related to Streptococcus pneumoniae. Crit Rev Microbiol 18: 89-114.
Lee MA, Brightwell G, Leslie D, Bird H & Hamilton A (1999) Fluorescent detection techniques for real-time multiplex strand specific detection of Bacillus anthracis using rapid PCR. J Appl Microbiol 87: 218-223.
Lehtomäki K, Leinonen M, Takala A, Hovi T, Herva E & Koskela M (1988) Etiological diagnosis of pneumonia in military conscripts by combined use of bacterial culture and serological methods. Eur J Clin Microbiol Infect Dis 7: 348-354.
Leino T, Auranen K, Jokinen J, Leinonen M, Tervonen P & Takala AK (2001) Pneumococcal carriage in chidren during their first two years: important role of family exposure. Pediatr Infect Dis J 20: 1022-1027.
Leinonen M (1980) Detection of pneumococcal capsular polysaccharide antigens by latex agglutination, counterimmunoelectrophoresis, and radioimmunoassay in middle ear exudates in acute otitis media. J Clin Microbiol 11: 135-140.
Leinonen M & Mäkelä PH (2001) Diagnosis of pneumococcal pneumonia. Clin Infect Dis 33: 1440-1441.
Leinonen M, Syrjälä H, Jalonen E, Kujala P & Herva E (1990) Demonstration of pneumolysin antibodies in circulating immune complexes – a new diagnostic method for pneumococcal pneumonia. Serodiagn Immunother Infect Dis 4: 451-458.
Lindbaek M, Melby KK, Schoyen R & Hjortdahl P (2001) Bacteriological findings in nasopharynx specimens from patients with a clinical diagnosis of acute sinusitis. Scand J Prim Health Care 19: 126-130.
Lloyd-Evans N, O’Dempsey TJD, Baldeh i, Secka O, Demba E, Todd JE, McArdle TF, Banya WS & Greenwood BM (1996) Nasopharyngeal carriage of pneumococci in Gambian children and in their families. Pediatr Infect Dis J 15: 866-871.
Lu JJ, Perng CL, Lee SY & Wan CC (2000) Use of PCR with universal primers and restriction endonuclease digestions for detection and identification of common bacterial pathogens in cerebrospinal fluid. J Clin Microbiol 38: 2076-2080.
Lund E & Henrichsen J (1978) Laboratory diagnosis, serology and epidemiology of Streptococcus pneumoniae. In: Norris, JR (ed) Methods in microbiology. Academic Press, London, 241-262.
Luotonen J (1982) Streptococcus pneumoniae and Haemophilus influenzae in nasal cultures during acute otitis media. Acta Otolaryngol (Stockh) 93: 295-299.
Luotonen J, Herva E, Karma P, Timonen M, Leinonen M & Mäkelä PH (1981) The bacteriology of acute otitis media in children: with special reference to Streptococcus pneumoniae as studied by bacteriological and antigen methods. Scand J Infect Dis 13: 177-183.
Macfarlane JT, Ward MJ, Finch RG & Macrae AD (1982) Hospital study of adult community-acquired pneumonia. Lancet: 255-258.
Magee AD & Yother J (2001) Requirement for capsule in colonization by Streptococcus pneumoniae. Infect Immun 69: 3755-3761.
Mangasser-Stephan K, Tag C, Reiser A & Gressner AM (1999) Rapid genotyping of hemochromatosis gene mutations on the LightCycler with fluorescent hybridization probes. Clin Chem 45: 1875-1878.
Marcos MA, Martinez E, Almela M, Mensa J & Jimenez de Anta MT (2001) New rapid antigen test for diagnosis of pneumococcal meningitis. Lancet 357: 1499-1500.

80McAvin JC, Reilly PA, Roudabush RM, Barnes WJ, Salmen A, Jackson GW, Beninga KK,
Astorga A, McCleskey FK, Huff WB, Niemeyer D & Lohman KL (2001) Sensitive and specific method for rapid identification of Streptococcus pneumoniae using real-time fluorescence PCR. J Clin Microbiol 39: 3446-3451.
McDaniel LS, Yother J, Vijayakumar M, McGarry L, Guild WR & Briles DE (1987) Use of insertional inactivation to facilitate studies of biological properties of pneumococcal surface protein A (PspA). J Exp Med 165: 381-394.
Meats E, Brueggemann AB, Enright MC, Sleeman K, Griffiths DT, Crook DW & Spratt BG (2003) Stability of serotypes during nasopharyngeal carriage of Streptococcus pneumoniae. J Clin Microbiol 41: 386-392.
Mellencamp MA, Preheim LC & McDonald TL (1987) Isolation and characterization of circulating immune complexes from patients with pneumococcal pneumonia. Infect Immun 55: 1737-1742.
Michelow IC, Lozano J, Olsen K, Goto C, Rollins NK, Ghaffar F, Rodriguez-Cerrato V, Leinonen M & McCracken GH (2002) Diagnosis of Streptococcus pneumoniae lower respiratory infection in hospitalizes children by culture, polymerase chain reaction, serological testing and urinary antigen detection. Clin Infect Dis 34: e1-11.
Mitchell TJ, Andrew PW, Saunders FK, Smith AN & Boulnois GJ (1991) Complement activation and antibody binding by pneumolysin via a region of the toxin homologous to a human acute-phase protein. Mol Microbiol 5: 1883-1888.
Morona JK, Miller DC, Coffey TJ, Vindurampulle CJ, Spratt BG, Morona R & Paton JC (1999a) Molecular and genetic characterization of the capsule biosynthesis locus of Streptococcus pneumoniae type 23F. Microbiology 145 ( Pt 4): 781-789.
Morona JK, Morona R & Paton JC (1997a) Characterization of the locus encoding the Streptococcus pneumoniae type 19F capsular polysaccharide biosynthetic pathway. Mol Microbiol 23: 751-763.
Morona JK, Morona R & Paton JC (1997b) Molecular and genetic characterization of the capsule biosynthesis locus of Streptococcus pneumoniae type 19B. J Bacteriol 179: 4953-4958.
Morona JK, Morona R & Paton JC (1999b) Comparative genetics of capsular polysaccharide biosynthesis in Streptococcus pneumoniae types belonging to serogroup 19. J Bacteriol 181: 5355-5364.
Morrison KE, Lake D, Crook J, Carlone GM, Ades E, Facklam R & Sampson JS (2000) Confirmation of psaA in all 90 serotypes of Streptococcus pneumoniae by PCR and potential of this assay for identification and diagnosis. J Clin Microbiol 38: 434-437.
Mullis KB & Faloona FA (1987) Specific synthesis of DNA in vitro via a polymerase-catalyzed chain reaction. Methods Enzymol 155: 335-350.
Munoz R, Fenoll A, Vicioso D & Casal J (1990) Optochin-resistant variants of Streptococcus pneumoniae. Diagn Microbiol Infect Dis 13: 63-66.
Munoz R, Mollerach M, Lopez R & Garcia E (1997) Molecular organization of the genes required for the synthesis of type 1 capsular polysaccharide of Streptococcus pneumoniae: formation of binary encapsulated pneumococci and identification of cryptic dTDP-rhamnose biosynthesis genes. Mol Microbiol 25: 79-92.
Murdoch DR, Anderson TP, Beynon KA, Chua A, Fleming AM, Laing RT, Town GI, Mills GD, Chambers ST & Jennings LC (2003) Evaluation of a PCR assay for detection of Streptococcus pneumoniae in respiratory and nonrespiratory samples from adults with community-acquired pneumonia. J Clin Microbiol 41: 63-66.
Murdoch DR, Laing RTR, Mills GD, Karalus NC, Town GI, Mirrett S & Reller LB (2001) Evaluation of a rapid immunochromatographic test for detection of Streptococcus pneumoniae antigen in urine samples from adults with community-acquired pneumonia. J Clin Microbiol 39: 3495-3498.
Murray PR (1979) Modification of the bile solubility test for rapid identification of Streptococcus pneumoniae. J Clin Microbiol 9: 290-291.
Musher DM (1992) Infections caused by Streptococcus pneumoniae: clinical spectrum, pathogenesis, immunity and treatment. Clin Infect Dis 14: 801-809.
Musher DM (1995) Streptococcus pneumoniae. In: Dolin, R (ed) Priciples and practice of infectious diseases, 4th edition. Churchill Livingstone, New York, 1811-1826.

81Musher DM, Chapman AJ, Goree A, Jonsson S, Briles D & Baughn RE (1986) Natural and
vaccine-related immunity to Streptococcus pneumoniae. J Infect Dis 154: 245-256. Nikkari S, Lopez FA, Lepp PW, Cieslak PR, Ladd-Wilson S, Passaro D, Danila R & Relman DA
(2002) Broad-range bacterial detection and the analysis of unexplained death and critical illness. Emerg Infect Dis 8: 188-194.
Nohynek H, Eskola J, Kleemola M, Jalonen E, Saikku P & Leinonen M (1995) Bacterial antibody assays in the diagnosis of acute lower respiratory tract infection in children. Pediatr Infect Dis J 14: 478-484.
Nuorti JP, Butler JC, Crutcher JM, Guevara R, Welch D, Holder P & Elliott JA (1998) An outbreak of multidrug-resistant pneumococcal pneumonia and bacteremia among unvaccinated nursing home residents. N Engl J Med 338: 1861-1868.
Obaro SK, Adegbola RA, Banya WA & Greenwood BM (1996a) Carriage of pneumococci after pneumococcal vaccination [letter]. Lancet 348: 271-272.
Obaro SK, Monteil MA & Henderson DC (1996b) The pneumococcal problem. Bmj 312: 1521-1525.
O'Brien KL, Bronsdon MA, Dagan R, Yagupsky P, Janco J, Elliott J, Whitney CG, Yang YH, Robinson LG, Schwartz B & Carlone GM (2001) Evaluation of a medium (STGG) for transport and optimal recovery of Streptococcus pneumoniae from nasopharyngeal secretions collected during field studies. J Clin Microbiol 39: 1021-1024.
O'Brien KL & Nohynek H (2003) and the Pneumococcal Vaccine Trials Carriage Working Group. Report from a WHO Working Group: standard method for detecting upper respiratory carriage of Streptococcus pneumoniae. Pediatr Infect Dis J 22: 133-140.
Ofek I & Sharon N (1988) Lectinophagocytosis: a molecular mechanism of recognition between cell surface sugars and lectins in the phagocytosis of bacteria. Infect Immun 56: 539-547.
Pals G, Pindolia K & Worsham MJ (1999) A rapid and sensitive approach to mutation detection using real-time polymerase chain reaction and melting curve analyses, using BRCA1 as an example. Mol Diagn 4: 241-246.
Parkinson AJ, Davidson M, Fitzgerald MA, Bulkow LR & Parks DJ (1994) Serotype distribution and antimicrobial resistance patterns of invasive isolates of Streptococcus pneumoniae: Alaska 1986-1990. J Infect Dis 170: 461-464.
Parkinson AJ, Rabiego ME, Sepulveda C, Davidson M & Johnson C (1992) Quantitation of pneumococcal C polysaccharide in sputum samples from patients with presumptive pneumoccal pneumonia by enzyme immunoassay. J Clin Microbiol 30: 318-322.
Paton JC (1996) The contribution of pneumolysin to the pathogenicity of Streptococcus pneumoniae. [Review]. Trends Microbiol 4: 103-106.
Paton JC, Andrew PW, Boulnois GJ & Mitchell TJ (1993) Molecular analysis of the pathogenicity of Streptococcus pneumoniae: the role of pneumococcal proteins. Ann Rev Microbiol 47: 89-115.
Paton JC, Berry AM, Lock RA, Hansman D & Manning PA (1986) Cloning and expression in Escherichia coli of the Streptococcus pneumoniae gene encoding pneumolysin. Infect Immun 54: 50-55.
Paton JC & Ferrante A (1983) Inhibition of human polymorphonuclear leukocyte respiratory burst, bactericidal activity, and migration by pneumolysin. Infect Immun 41: 1212-1216.
Paton JC, Lock RA & Hansman DJ (1983) Effect of immunization with pneumolysin on survival time of mice challenged with Streptococcus pneumoniae. Infect Immun 40: 548-552.
Paton JC & Morona JK (2000) Streptococcus pneumoniae capsular polysaccharide. In: Rood, JI (ed) Gram-positive pathogens. American Society for Microbiology, Washington, D.C., 201-213.
Paton JC, Rowan-Kelly B & Ferrante A (1984) Activation of human complement by the pneumococcal toxin pneumolysin. Infect Immun 43: 1085-1087.
Pedersen FK & Henrichsen J (1982) Detection of antibodies to pneumococcal capsular polysaccharides by enzyme-linked immunosorbent assay. J Clin Microbiol 15: 372-378.
Peizhong L, Whatmough K, Birchall JP, Wilson JA & Pearson JP (2000) Does the bacterial DNA found in middle ear effusions come from viable bacteria? Clin Otolaryngol 25: 570-576.
Perkins MD, Mirrett S & Reller LB (1995) Rapid bacterial antigen detection is not clinically useful. J Clin Microbiol 33: 1486-1491.

82Pfaller MA, Ehrhardt AF & Jones RN (2001) Frequency of pathogen occurrence and antimicrobial
susceptibility among community-acquired respiratory tract infections in the respiratory surveillance program study: microbiology from the medical office practice environment. Am J Med 111 Suppl 9A: 4S-12S; discussion 36S-38S.
Plouffe JF, McNally C & File TMJ (1998) Value of noninvasive studies in community-acquired pneumonia. Inf Dis Clin N Amer 12: 689-699.
Post JC (2001) Direct evidence of bacterial biofilms in otitis media. Laryngoscope 111: 2083-2094. Post JC, Aul JJ, White GJ, Wadowsky RM, Zavoral T, Tabari R, Kerber B, Doyle WJ & Ehrlich
GD (1996) PCR-based detection of bacterial DNA after antimicrobial treatment is indicative of persistent, viable bacteria in the chinchilla model of otitis media. Am J Otolaryngol 17: 106-111.
Post JC, Preston RA, Aul JJ, Larkins-Pettigrew M, Rydquist-White J, Anderson KW, Wadowsky RM, Reagan DR, Walker ES, Kingsley LA, Magit AE & Ehrlich GD (1995) Molecular analysis of bacterial pathogens in otitis media with effusion. JAMA 273: 1598-1604.
Ramsey BW, Marcuse EK, Foy HM, Cooney MK, Allan I, Brewer D & Smith AL (1986) Use of bacterial antigen detection in the diagnosis of pediatric lower respiratory tract infections. Pediatrics 78: 1-9.
Rantakokko-Jalava K, Nikkari S, Jalava J, Eerola E, Skurnik M, Meurman O, Ruuskanen O, Alanen A, Kotilainen E, Toivanen P & Kotilainen P (2000) Direct amplification of rRNA genes in diagnosis of bacterial infections. J Clin Microbiol 38: 32-39.
Rapola S, Salo E, Kiiski P, Leinonen M & Takala AK (1997) Comparison of four different sampling methods for detecting pharyngeal carriage of Streptococcus pneumoniae and Haemophilus influenzae in children. J Clin Microbiol 35: 1077-1079.
Rasmussen R (2001) Quantification on the LightCycler. In: Meuer, S, Wittwer, C., Nakagawara, K. (ed) Rapid cycle real-time PCR. Methods and applications. Springer Verlag, Berlin Heidelberg, 21-34.
Rayner MG, Zhang Y, Gorry MC, Chen Y, Post JC & Ehrlich GD (1998) Evidence of bacterial metabolic activity in culture-negative otitis media with effusion. Jama 279: 296-299.
Reischl U, Linde HJ, Lehn N, Landt O, Barratt K & Wellinghausen N (2002) Direct detection and differentiation of Legionella spp. and Legionella pneumophila in clinical specimens by dual-color real-time PCR and melting curve analysis. J Clin Microbiol 40: 3814-3817.
Rennels MB, Edwards KM, Keyserling HL, Reisinger KS, Hogerman DA, Madore DV, Chang I, Paradiso PR, Malinoski FJ & Kimura A (1998) Safety and immunogenicity of heptavalent pneumococcal vaccine conjugated to CRM197 in United States infants. Pediatrics 101: 604-611.
Ririe KM, Rasmussen RP & Wittwer CT (1997) Product differentiation by analysis of DNA melting curves during the polymerase chain reaction. Anal Biochem 245: 154-160.
Robbins JB, Austrian R, Lee C-J, Rastogu SC, Schiffman G, Henrichsen J, Mäkelä PH, Broome CV, Facklam RR, Tiesjema RH & Parke Jr. JC (1983) Considerations for formulating the second-generation pneumococcal capsular polysaccharide vaccine with emphasis on the cross-reactive types within groups. J Infect Dis 148: 1136-1159.
Rosenow C, Ryan P, Weiser JN, Johnson S, Fontan P, Örtqvist Å & Masure HR (1997) Contribution of novel choline-binding proteins to adherence, colonization and immunogenicity of Streptococcus pneumoniae. Molecular Microbiol 25: 819-829.
Rosenstraus M, Wang Z, Chang SY, DeBonville D & Spadoro JP (1998) An internal control for routine diagnostic PCR: design, properties, and effect on clinical performance. J Clin Microbiol 36: 191-197.
Rubins JB, Duane PG, Clawson D, Charboneau D, Young J & Niewoehner DE (1993) Toxicity of pneumolysin to pulmonary alveolar epithelial cells. Infect Immun 61: 1352-1358.
Rudolph KM, Parkinson AJ, Black CM & Mayer LW (1993) Evaluation of polymerase chain reaction for diagnosis of pneumoccal pneumonia. J Clin Microbiol 31: 2661-2666.
Ruiz-Gonzalez A, Nogues A, Falguera M, Porcel JM, Huelin E & Rubio-Caballero M (1997) Rapid detection of pneumococcal antigen in lung aspirates: comparison with culture and PCR technique. Respirat Med 91: 201-206.

83Russell H, Edwards LR, Wortham EW & Facklam RR (1980) Enzyme-linked immunosorbent
assay for detection of antibodies against Streptococcus pneumoniae capsular polysaccharides. J Clin Microbiol 11: 198-199.
Russell H, Tharpe JA, Wells DE, White EH & Johnson JE (1990) Monoclonal antibody recognizing a species-specific protein from Streptococcus pneumoniae. J Clin Microbiol 28: 2191-2195.
Saarinen M, Takala AK, Koskenniemi E, Kela E, Ronnberg PR, Pekkanen E, Kiiski P & Eskola J (1995) Spectrum of 2,836 cases of invasive bacterial or fungal infections in children: results of prospective nationwide five-year surveillance in Finland. Finnish Pediatric Invasive Infection Study Group. Clin Infect Dis 21: 1134-1144.
Saiki RK, Gelfand DH, Stoffel S, Scharf SJ, Higuchi R, Horn GT, Mullis KB & Erlich HA (1988) Primer-directed enzymatic amplification of DNA with a thermostable DNA polymerase. Science 239: 487-491.
Salo P, Laitinen K & Leinonen M (1999) Detection of pneumococcus from whole blood, buffy coat and serum samples by PCR during bacteremia in mice. APMIS 107: 601-605.
Salo P & Leinonen M (1999) Microbiological investigations. Semin Respirat Infect 14: 128-134. Salo P, Örtqvist Å & Leinonen M (1995) Diagnosis of bacteremic pneumococcal pneumonia by
amplification of pneumolysin gene fragment in serum. J Infect Dis 171: 479-482. Sampson JS, Furlow Z, Whitney AM, Williams D, Facklam R & Carlone GM (1997) Limited
diversity of Streptococcus pneumoniae psaA among pneumococcal vaccine serotypes. Infect Immun 65: 1967-1971.
Sampson JS, O'Connor SP, Stinson AR, Tharpe JA & Russell H (1994) Cloning and nucleotide sequence analysis of psaA, the Streptococcus pneumoniae gene encoding a 37-kilodalton protein homologous to previously reported Streptococcus sp. adhesins. Infect Immun 62: 319-324.
Sankilampi U, Herva E, Haikala R, Liimatainen O, Renkonen OV & Leinonen M (1997) Epidemiology of invasive Streptococcus pneumoniae infections in adults in Finland. Epidemiol Infect 118: 7-15.
Schalasta G & Schmid M (1999) Ultrarapid and semiautomated real-time PCR - a breakthrough in nucleic acid analysis. Clin Lab 45: 661-663.
Schuchat A, Robinson K, Wenger JD, Harrison LH, Farley M, Reingold AL, Lefkowitz L & Perkins BA (1997) Bacterial meningitis in the United States in 1995. Active Surveillance Team. N Engl J Med 337: 970-976.
Scott JAG, Hannington A, Marsh K & Hall AJ (1999) Diagnosis of pneumococcal pneumonia in epidemiological studies: evaluation in Kenyan adults of a serotype-specific urine latex agglutination assay. Clin Infect Dis 28: 764-769.
van Selm S, Kolkman MA, van der Zeijst BA, Zwaagstra KA, Gaastra W & van Putten JP (2002) Organization and characterization of the capsule biosynthesis locus of Streptococcus pneumoniae serotype 9V. Microbiology 148: 1747-1755.
Shann F (1986) Etiology of severe pneumonia in children in developing countries. Pediatr Infect Dis 5: 247-252.
Shapiro ED, Berg AT, Austrian R, Schroeder D, Parcells V, Margolis A, Adair RK & Clemens CD (1991) The protective efficacy of polyvalent pneumococcal polysaccharide vaccine. N Engl J Med 325: 1453-1460.
Silvennoinen-Kassinen S & Koskela M (1986) Optimal conditions for the opsonophagocytosis test with Streptococcus pneumoniae serotypes 3, 6A, 7F and 19F and human granulocytes. Acta Pathol Microbiol Immunol Scand [C] 94: 105-111.
Singhal A, Lalitha MK, Jacob John t, Thomas K, Raghupathy P, Jacob S & Steinhoff MC (1996) Modified latex agglutination test for rapid detection of Streptococcus pneumoniae and Haemophilus influenzae in cerebrospinal fluid and direct serotyping of Streptococcus pneumoniae. Eur J Clin Microbiol Infect Dis 15: 472-477.
Sloan LM, Hopkins MK, Mitchell PS, Vetter EA, Rosenblatt JE, Harmsen WS, Cockerill FR & Patel R (2002) Multiplex LightCycler PCR assay for detection and differentiation of Bordetella pertussis and Bordetella parapertussis in nasopharyngeal specimens. J Clin Microbiol 40: 96-100.

84Soininen A (2001) Antibodies to capsular polysaccharides of Streptococcus pneumoniae in
children: acquisition and measurement. Helsinki: University of Helsinki, pp. 72. Soininen A, Pursiainen H, Kilpi T & Käyhty H (2001) Natural development of antibodies to
pneumococcal capsular polysaccharides depends on the serotype: association with pneumococcal carriage and acute otitis media in children. J Infect Dis 184: 569-576.
Stöcher M, Leb V & Berg J (2003) A convenient approach to the generation of multiple internal control DNA for a panel of real-time PCR assays. J Virol Methods 108: 1-8.
Syrjänen RK, Kilpi TM, Kaijalainen TH, Herva EE & Takala AK (2001) Nasopharyngeal carriage of Streptococcus pneumoniae in Finnish children younger than 2 years old. J Infect Dis 184: 451-459.
Söderström M, Hovelius B, Prellner K & Schalen C (1990) Quantification of nasopharyngeal bacteria for diagnosis of respiratory tract infection in children. Scand J Infect Dis 22: 333-337.
Sørensen UB, Henrichsen J, Chen HC & Szu SC (1990) Covalent linkage between the capsular polysaccharide and the cell wall peptidoglycan of Streptococcus pneumoniae revealed by immunochemical methods. Microb Pathog 8: 325-334.
Sørensen UBS (1995) Pneumococcal polysaccaride antigens: capsules and C-polysaccaride. Danish Med Bull 42: 47-53.
Sørensen UBS, Blom J, Birch-Andersen A & Henrichsen J (1988) Ultrastructural localization of capsules, cell wall polysaccharide, cell wall proteins, and F antigen in pneumococci. Infect Immun 56: 1890-1896.
Talkington DF, Brown BG, Thrape JA, Koenig A & Russell H (1996) Protection of mice against fatal pneumococcal challenge by immunization with pneumococcal surface adhesin A (PsaA). Microbial Pathogen 21: 17-22.
Teele DW, Klein JO & Rosner B (1989) Epidemiology of otitis media during the first seven years of life in children in greater Boston: a prospective, cohort study. J Infect Dis 160: 83-94.
Toikka P, Nikkari S, Ruuskanen O, Leinonen M & Mertsola J (1999) Pneumolysin PCR-based diagnosis of invasive pneumococcal infection in children. J Clin Microbiol 37: 633-637.
Tomasz A (1981) Surface components of Streptococcus pneumoniae. Rev Infect Dis 3: 190-211. Trollfors B, Burman L, Dannetun E, Llompart J & Norrby R (1983) Serotyping of Streptococcus
pneumoniae strains by coagglutination and counterimmunoelectrophoresis. J Clin Microbiol 18: 978-980.
Tu AH, Fulgham RL, McCrory MA, Briles DE & Szalai AJ (1999) Pneumococcal surface protein A inhibits complement activation by Streptococcus pneumoniae. Infect Immun 67: 4720-4724.
Ubukata K, Asahi Y, Yamane A & Konno M (1996) Combinational detection of autolysin and penicillin-binding protein 2B genes of Streptococcus pneumoniae by PCR. J Clin Microbiol 34: 592-596.
Ukkonen P, Varis K, Jernfors M, Herva E, Jokinen J, Ruokokoski E, Zopf D & Kilpi T (2000) Treatment of acute otitis media with an antiadhesive oligosaccharide: a randomised, double-blind, placebo-controlled trial. Lancet 356: 1398-1402.
Virolainen A, Russell W, Crain MJ, Rapola S, Käyhty H & Briles DE (2000) Human antibodies to pneumococcal surface protein A in health and disease. Pediatr Infect Dis J 19: 134-138.
Virolainen A, Salo P, Jero J, Karma P, Eskola J & Leinonen M (1994) Comparison of PCR assay with bacterial culture for detecting Streptococcus pneumoniae in middle ear fluid of children with acute otitis media. J Clin Microbiol 32: 2667-2670.
Vives M, Garcia ME, Saentz P, Mora M, Mata L, Sabharwal H & Svanborg C (1997) Nasopharyngeal colonization in Costa Rican children during the first year of life. Pediatr Infect Dis J 16: 852-858.
Vuori-Holopainen E & Peltola H (2001) Reappraisal of lung tap: review of an old method for better etiologic diagnosis of childhood pneumonia. Clin Infect Dis 32: 715-726.
Vuori-Holopainen E, Salo E, Saxen H, Hedman K, Hyypia T, Lahdenpera R, Leinonen M, Tarkka E, Vaara M & Peltola H (2002) Etiological diagnosis of childhood pneumonia by use of transthoracic needle aspiration and modern microbiological methods. Clinical Infectious Diseases 34: 583-590.

85Wadowsky RM, Laus S, Libert T, States SJ & Ehrlich GD (1994) Inhibition of PCR-based assay
for Bordetella pertussis by using calcium alginate fiber and aluminum shaft components of a nasopharyngeal swab. J Clin Microbiol 32: 1054-1057.
Walker JA, Allen RL, Falmagne P, Johnson MK & Boulnois GJ (1987) Molecular cloning, characterization and complete nucleotide sequence of the gene for pneumolysin, the sulfhydryl-activated toxin of Streptococcus pneumoniae. Infect Immun 55: 1184-1189.
Walsh PS, Metzger DA & Higuchi R (1991) Chelex 100 as a medium for simple extraction of DNA for PCR-based typing from forensic material. Biotechniques 10: 506-513.
Watson DA, Musher DM, Jacobson JW & Verhoef J (1993) A brief history of the pneumococcus in biomedical research: a panoply of scientific discovery. Clin Infect Dis 17: 913-924.
Watson DA, Musher DM & Verhoef J (1995) Pneumococcal virulence factors and host immune responces to them. Eur J Clin Microbiol Infect Dis 14: 479-490.
Weinstein MP (1996) Current blood culture methods and systems: clinical concepts, technology, and interpretation of results. Clin Infect Dis 23: 40-46.
Weiser JN, Austrian R, Sreenivasan PK & Masure HR (1994) Phase variation in pneumococcal opacity: relationship between colonial morphology and nasopharyngeal colonization. Infect Immun 62: 2582-2589.
Whatmore AM, Efstratiou A, Pickerill AP, Broughton K, Woodard G, Sturgeon D, George R & Dowson CG (2000) Genetic relationships between clinical isolates of Streptococcus pneumoniae, Streptococcus oralis, and Streptococcus mitis: characterization of "atypical" pneumococci and organisms allied to S. mitis harboring S. pneumoniae virulence factor-encoding genes. Infect Immun 68: 1374-1382.
Whitney CG, Farley MM, Hadler J, Harrison LH, Bennett NM, Lynfield R, Reingold A, Cieslak PR, Pilishvili T, Jackson D, Facklam RR, Jorgensen JH & Schuchat A (2003) Decline in invasive pneumococcal disease after the introduction of protein-polysaccharide conjugate vaccine. N Engl J Med 348: 1737-1746.
Winkelstein JA (1981) The role of complement in the host’s defence against Streptococcus pneumoniae. Rev Infect Dis 3: 289-298.
Wittwer CT, Ririe KM, Andrew RV, David DA, Gundry RA & Balis UJ (1997) The LightCyclerTM: a microvolume multisample fluorimeter with rapid temperature control. Biotechniques 22: 176-181.
Wubbel L, Muniz L, Ahmed A, Trujillo M, Carubelli C, McCoig C, Abramo T, Leinonen M & McCracken GH, Jr. (1999) Etiology and treatment of community-acquired pneumonia in ambulatory children. Pediatr Infect Dis J 18: 98-104.
Yolken RH, Davis D, Winkelstein J, Russell H & Sippel JE (1984) Enzyme immunoassay for detection on pneumococcal antigen in cerebrospinal fluid. J Clin Microbiol 20: 802-805.
Yother J & White JM (1994) Novel surface attachment mechanism of the Streptococcus pneumoniae protein PspA. J Bacteriol 176: 2976-2985.
Zhang Y, Isaacman DJ, Wadowsky RM, Rydquist-White J, Post JC & Ehrlich GD (1995) Detection of Streptococcus pneumoniae in whole blood by PCR. J Clin Microbiol 33: 596-601.
Zielen S, Buhring I, Strnad N, Reichenbach J & Hofmann D (2000) Immunogenicity and tolerance of a 7-valent pneumococcal conjugate vaccine in nonresponders to the 23-valent pneumococcal vaccine. Infect Immun 68: 1435-1440.
Åhman H, Käyhty H, Lehtonen H, Leroy O, J. F & Eskola J (1998) Streptococcus pneumoniae capsular polysaccharide-diphtheria toxoid conjugate vaccine is immunogenic in early infancy and able to induce immunologic memory. Pediatr Infect Dis J 17: 211-216.
Åhman H, Käyhty H, Tamminen P, Vuorela A, Malinoski F & Eskola J (1996) Pentavalent pneumococcal oligosaccharide conjugate vaccine PncCRM is well-tolerated and able to induce an antibody response in infants. Pediatr Infect Dis J 15: 134-139.
Örtqvist Å, Hedlund J, Burman L-Å, Elbel E, Höfer M, Leinonen M, Lindblad I, Sundelöf B, Kalin M & Group aSPVS (1998) Randomised trial of 23-valent pneumococcal capsular polysaccharide vaccine in prevention of pneumonia in middle-aged and elderly people. Lancet 351: 399-403.